Embed Size (px)
Citation preview

Gut 1996; 38: 454-458
Acute liver damage and ecstasy ingestion
A J Ellis, J A Wendon, B Portmann, Roger Williams
AbstractEight cases of ecstasy related acute liverdamage referred to a specialised liverunit are described. Two patients pre-sented after collapse within six hours ofecstasy ingestion with hyperthermia,hypotension, fitting, and subsequentlydisseminated intravascular coagulationwith rhabdomyolysis together with bio-chemical evidence ofsevere hepatic dam-age. One patient recovered and the otherwith evidence of hyperacute liver failurewas transplanted but subsequently died,histological examination showing wide-spread microvesicular fatty change. Fourpatients presented with acute liver failurewithout hyperthermia. All four fulfilledcriteria for transplantation, one patientsurvived after transplantation, one diedbefore a donor organ became available,and two died within one month post-transplantation of overwhelming sepsis.Histological examination showed sub-massive lobular collapse. Two patientspresented with abdominal pain and jaun-dice and recovered over a period of threeweeks; histological examination showed alobular hepatitis with cholestasis.Patients developing jaundice or with evi-dence of hepatic failure particularlyencephalopathy and prolongation of theinternational normalised ratio, or both,whether or not preceded by hyperther-mia, should be referred to a specialisedliver unit as liver transplantationprobably provides the only chance ofrecovery.(Gut 1996; 38: 454-458)
Keywords: ecstasy, acute liver failure, transplantation,hepatitis, 3,4, methylenedioxymethamphetamine,MDMA.
The social use of 3,4 methyldioxymetham-phetamine (MDMA), otherwise known as'ecstasy', and other drugs with similar effectssuch as 3,4-methylenedioxyamphetamine(MDA) and 3,4-methylenedioxyethampheta-mine (MDEA) is widespread in the UnitedKingdom and Europe. Ecstasy is taken at'rave-parties' for its amphetamine-like stimula-tory effect allowing users to dance for pro-longed periods with increased energy andreduced awareness of fatigue. Publications todate have brought attention to patients col-lapsing with hyperthermia complicatedwith disseminated intravascular coagulationand rhabdomyolysis.' 2 Other complicationsreported include cerebral haemorrhage, hypo-natraemia, and cardiac arrhythmias.3-5 Sevencases of ecstasy related hepatotoxicity werereported in a study of telephone referrals toThe National Poisons Information Service,two of which were subsequently described inmore detail in correspondence columns assingle cases with liver dysfunction.6-8 Sixfurther cases have been described as single casereports9 12 making 13 possible cases in total(Table).
This paper describes eight patients referredto a single centre with evidence of acute liverdamage temporally related to the ingestion ofecstasy, two cases presenting with hyper-thermia and six with an acute hepatitic illness.Five patients developed encephalopathy andsevere coagulopathy sufficient to merit listingfor transplantation.
Case histories
Case 1A 21 year old woman collapsed after a convul-sion having taken both ecstasy and LSD at aparty six hours earlier. On admission she was
Clinical data available from 10 previous cases of ecstasy related hepatotoxicity
Case Alkaline Time tono Clinical AST phosphatase GGT INR APTT Last ecstasy resolution of(re]) Age Sex course Hepatomegaly Bilirubin (pmol/l) (IU/l) (IU/l) (IU/l) (secs) use (days) LFTs (days) Outcome
17 27 F Hepatitis 3 cm 471 1717 439 50 N 10 21 Survived28 20 M Hepatitis None 131 2050 201 1 5 1 Survived
(max 330)39 32 F Hyperthermia None 6 1820 107 PT 37-9 28 28 Survived
(max 130)410 23 M Hyperthermia 77 2659 3-6 >115 1 Survived56 29 M Hepatitis 'Jaundiced' >90 Survived66 19 M Hepatitis 170 1509 369 103 21 > 14 Survived76 19 M Acute liver 400 Liver transplant Survived
failure86 20 M Hepatitis Yes 40 Regular use Survived96 19 M Hepatitis 181 659 276 Regular use 'Slow resolution' Survived
1011 18 F Acute liver No 480 1025 30 208 2-7 Regular use >50 Survivedfailure
1 12 24 M Hepatitis No 346 950 251 Single exposure1212 22 M Hepatitis Yes 137 748 216 Single exposure
APTT=activated partial thromboplastin time.
The Institute of LiverStudies, King's CollegeHospital and King'sCollege School ofMedicine andDentistry, LondonA J EllisJ A WendonB PortmannRoger Williams
Correspondence to:Professor Roger WilliamsCBE, Institute of LiverStudies, King's CollegeHospital School of Medicineand Dentistry, BessemerRoad, London SE5 9RS.Accepted for publication7 September 1995
454
on Septem
ber 4, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.38.3.454 on 1 March 1996. D
ownloaded from

Acute liver damage and ecstasy ingestion
deeply unconscious with sluggish and dilatedpupils, hypertonic limbs, and no response topain. Axillary temperature was 41°C, bloodpressure 170/100 mm Hg, and pulse 180.Blood investigations showed a creatine kinase4710 IU/1, pH 7-27, arterial bicarbonate(HCO3) 15, bilirubin 25 ,umoI/l, aspartateaminotransaminase (AST) 3940 lU/1, alkalinephosphatase 38 lU/1, y-glutamyltransferase(GGT) 62 lUl1. Further convulsions necessi-tated ventilation, paralysis, and sedation.Computed tomography showed diffuse brainswelling and within 24 hours she developed asevere coagulopathy with an international nor-malised ratio (INR) >15, thrombin time 86seconds (control 17 seconds), and fibrin degra-dation products of 2 pumol/l (N=<0 5 ,umolIl)consistent with disseminated intravascularcoagulation. Continuous veno-venous haemo-diafiltration was started for developing renalfailure. Cardiac output rose to 18 I/min anddespite use of fresh frozen plasma and cryopre-cipitate, the INR remained grossly prolongedat 8.4. Toxicology showed serum MDMA0-1 1 mg/1, urine MDMA 0 04 mg/l.A diagnosis of hyperacute liver failure was
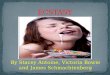
made with criteria for transplantation fulfilled,and a donor organ became available on thefourth day of admission. Postoperativelycardiovascular stability improved and graftfunction was good but she remained feverish.Despite treatment with broad spectrum anti-biotics and systemic antifungal treatment shedied of sepsis on day 13 post-transplant.Examination of the explanted liver showed apale liver on cut section with light microscopyshowing enlarged and ballooned hepatocytesresulting from microvesicular fatty infiltration.Scattered eosinophilic single cell necrosis wasevident with small foci of collapse due to celldrop out. Inflammation was minimal (Fig 1).
Case 2An 18 year old girl noted progressive jaundiceover a four week period with malaise, palestools, and dark urine. She took ecstasy on aregular basis and continued to do so after theappearance of jaundice. Blood tests performedby her doctor showed a serum bilirubin of 277gmol/l and an AST of 1575 IU/1. Three weekslater she became confused and by this time theserum bilirubin was 452 gumoi/i, AST 3160IU/1, and INR 4.0. On arrival she wasencephalopathic (grade II) and haemodynami-cally stable. Renal function was good with aserum creatinine 91 pumol/1, urine output >50ml/h. Her encephalopathy worsened within 24hours necessitating paralysis, ventilation, andsedation. Repeat liver blood tests showed albu-min 34 g/dl, bilirubin 397 pumol/1, AST 974IU/1, alkaline phosphatase 235 lU/1, GGT 71IU/1, and an INR of 4. Serological testsexcluded known hepatotropic viruses includ-ing hepatitis C. Abdominal ultrasound showeda small liver of normal reflectivity. A diagnosisof ecstasy induced acute liver failure was madeand she was listed for urgent transplantation.Her INR became more prolonged (>15) andshe developed signs of raised intracranial
Figure 1: Liver histology in case 1 showing extensiveballooning and cytoplasmic vacuolation of hepatocytes andfrequent mitoses in the absence of significant inflammation.
pressure. Despite treatment with broad spec-trum antibiotics and intravenous antifungalagents she became profoundly septic with acardiac output of 18 1/min and died before adonor organ became available.
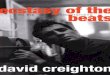
Case 3A 36 year old woman presented to hospitalwith a six day illness characterised by nauseaand lower back pain with vomiting and thedevelopment of jaundice. Ten days before thisillness she had taken a single capsule of ecstasy.She was admitted to the local hospital and after10 days developed encephalopathy and wastransferred to King's College Hospital. Onadmission ascites was detectable clinically andinvestigations showed a white cell count11.7X109/l, INR 6.5, urea 7.4 mmol/1, creati-nine 163 pumol/I, amylase 23 IU/i, serum albu-min 37 g/dl, bilirubin 406 gumol/l, AST 828IU/1, alkaline phosphatase 90 IU/1, and GGT78 IU/1. Abdominal ultrasound was unremark-able and serological tests excluded knownhepatotropic viruses including hepatitis C. Shewas ventilated and with criteria for liver trans-plantation fulfilled was listed for urgent ortho-topic liver transplantation, which was carriedout on day 5 after admission. After surgery shedeveloped fluctuating increases of AST(119-820 IU/1). Rejection was excluded byliver biopsy and there were no features of graftreinfection with virus. Angiography showedpatent recipient vessels. Despite appropriateantibiotics she continued to deteriorate anddied 25 days post-transplantation of over-whelming sepsis. Histological examination ofthe explanted liver showed widespread cell losswith islands of surviving cells composed ofvesiculated or ballooned hepatocytes (Fig 2).
Case 4A 21 year old woman with a four month historyof taking up to five ecstasy tablets at weekendswas admitted with right upper quadrant pain.Six weeks before admission she experienced a'flu-like' illness followed by general malaiseand continuous pain associated with vomitingand pale stools. On admission she was notencephalopathic and examination was un-remarkable apart from abdominal tenderness.Initial investigations showed a white cell countof 5'7X 109/i, INR 0-93, creatinine 63 jimolll,
455
on Septem
ber 4, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.38.3.454 on 1 March 1996. D
ownloaded from

Ellis, Wendon, Portmann, Williams
Figure 2: Liver histology in case 3 with confluentparenchymal collapse with clusters ofsurviving,considerably enlarged hepatocytes.
total protein 65 g/l, albumin 42 g/l, bilirubin 44pumoVl, AST 760 IU/1, alkaline phosphatase149 1U/1, GGT 94 1U/1. Ultrasound examina-tion showed stones in the gall bladder and anormal biliary tree. She was referred to theLiver Unit, King's College Hospital for furtherinvestigations and over a two week period as aninpatient her AST settled and she was dis-charged well. Serological tests excluded knownhepatotropic viruses including hepatitis C.Liver biopsy showed a lobular hepatitis withscattered single cell necrosis, acidophilicbodies, and sparse mixed inflammatory cellsand occasional pigmented macrophages. Theportal tracts appeared lightly infiltrated bymixed inflammatory cells including eosinophilswith mild cell spill over at the margin.
Case 5A 19 year old man, a regular user of ecstasy,was found unconscious at a party having takenthree tablets. No fitting was witnessed. Onarrival to his local hospital he was hyper-thermic (42°C), unresponsive (tolerating anairway), and hypotensive with a systolic bloodpressure of 90 mm Hg. He required ventilationand aggressive rehydration with administrationof dantrolene (total dose 3 mg/kg bodyweightover two hours) to reduce body temperature.Investigations showed a white cell count14.8X 109/1, platelets 130X 109/1, prothrombintime 24 seconds (control 20 seconds), urea 5.2mmolI, creatinine 175 pumol/, bilirubin 120,umolI1, AST 80 lU/l, creatinine kinase 22918IU/1. Toxicological tests on serum showedMDMA 0.38 mg/l, MDA 0.03 mg/l. Twelvehours later a repeat coagulation screen showedan activated partial thromboplastin time of> 120 seconds (control 35 seconds), pro-thrombin time > 120 seconds (control 17seconds), platelets 38 X 109/1. Serum AST hadrisen to >5000 1U/1. A diagnosis of dis-seminated intravascular coagulation andhypoxic/heat induced acute liver damage wasmade, and he was transferred to King'sCollege Hospital. After admission fluidbalance was optimised and urine output main-tained at > 100 mV/h with crystalloid andNaHCO3 (1.4%) to reduce the risk of renalfailure secondary to myoglobinuria. Heremained ventilated for six days with initiallysigns of fitting and during this time his coagu-lopathy normalised (INR fell from 5 to 1 1),
Figure 3: Acute hepatitis in case 6 with the portal areabeing infiltrated by lymphocytes, neutrophils, andeosinophils.
platelet count increased from 37 to 219 X 1 09.Serum bilirubin peaked at 287 pumoYl onday 3. Having required ventilation for six dayshe was discharged home on day 15, the serumbilirubin having fallen to 56 pumol/l.
Case 6A 22 year old man presented to his localhospital with a seven day history of malaise,nausea, pale stools, and dark urine and wasimmediately referred to King's CollegeHospital. He was a regular user of ecstasy andamphetamine up to the appearance of jaun-dice. On arrival investigations showed a whitecell count of 7-8X 109/1, INR 1. 1, creatinine99 ,umol/l, albumin 51 g/l, bilirubin 311[Lmol/l, alkaline phosphatase 173 IU/1, AST1191 IU/1, and GGT 169 IU/l. Over a threeday period he required 10% dextrose to main-tain his blood sugar. All known causes of acutehepatitis were excluded and an ultrasound wasunremarkable. Liver biopsy showed ballooningof hepatocytes and some acidophilic bodies.Both the sinusoids and portal tracts showedmild to moderate inflammatory infiltrates con-sisting of lymphocytes, neutrophils, andeosinophils. Cholestasis was evident and over-all findings were consistent with a drug relatedhepatitis (Fig 3).
Case 7A 22 year old woman with a six month historyof ecstasy use was admitted to her localhospital with a three week history of worseningjaundice associated with nausea and vomiting.Initial investigations showed a serum bilirubinof 129 ,mol/l and an INR of 2. Two weekslater on referral to King's College Hospital herbilirubin had risen to 343 Rmol/l and the INRhad become more prolonged to 2.9 in associa-tion with grade II encephalopathy. Withworsening encephalopathy, an INR of 4 1 andher general condition but with the possibility ofnative liver regeneration, it was decided toproceed to an auxiliary left partial orthotopictransplant. In this procedure the left laterallobe from the donor organ is implanted in anormal anatomical position following excisionof the native left lobe. Her initial postoperativerecovery was good but she developed worsen-ing sepsis and died 30 days post-transplant.Histological samples from the excised left lobe
456
on Septem
ber 4, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.38.3.454 on 1 March 1996. D
ownloaded from

Acute liver damage and ecstasy ingestion
showed extensive collapse with small areas ofregeneration. Biopsy specimens taken in thepostoperative period from both donor andnative livers showed severe cholestasis com-patible with sepsis.
Case 8A 24 year old woman presented to casualty ingrade III encephalopathy having recentlyarrived in England after a two month holidayin the Caribbean. She had been seen one weekearlier at a local hospital with a non-specificillness and jaundice. There was no hepato-splenomegaly and investigations showed awhite cell count of 18 X 109/1, INR >15, urea0.5 mmol/l, creatinine 52 ,umol/l, glucose 1.2mmol/l, albumin 37 g/l, bilirubin 407 ,umol/l,alkaline phosphatase 295 lUl1, AST 721 lU/1,GGT 123 IU/1. Fulfilling criteria for transplan-tation she was placed on the urgent list and aliver became available after 48 hours. Becauseof a mismatch in size between donor andrecipient she received a reduced graft. In thepostoperative phase there were no episodes ofrejection and she was discharged home wellafter five weeks. All tests for known causes ofacute liver failure were negative and in a subse-quent outpatient visit she admitted to havingtaken two to four tablets of ecstasy in the sixweeks prior to her admission. Histologicalexamination showed a small shrunken liverwith diffusely collapsed parenchyma. Com-plete cell drop out was evident with a wide-spread mixed cell infiltrate, denser in theperiportal areas. The findings were consistentwith drug or viral induced fulminant hepatitis.
DiscussionReferrals to our unit with acute liver failure anda history of ecstasy use are increasing. Fivecases were referred in 1994 and 1993 withprior to that only single cases in 1989 and 1991respectively. Ecstasy was the sole agent thatcould be incriminated in causing the liverdamage in eight patients, the other four havingalso taken a paracetamol overdose with aclinical picture and biochemical changesappropriate to paracetamol ingestion. Of theeight cases with ecstasy as the sole aetiologicalagent, two had presented with hyperthermia,hypotension, and collapse, four with evidenceof acute liver failure without preceding hyper-thermia, and two with a less severe hepatitis.On the basis of the patterns of liver damagedescribed, the 13 cases previously reported canbe classified similarly with two cases of hyper-thermia with liver injury,9 10 two reports ofacute liver failure without hyperthermia,6 11
and nine cases of apparent drug relatedhepatitis.6-8 12The clinical features of those cases present-
ing with hyperthermia are similar to thosepreviously reported in heatstroke, namelyhypotension, coagulopathy, renal impairment,and evidence of severe liver injury.13-15 Ecstasyusers may be at an increased risk of heatstrokebecause of the direct effect of MDMA onthermoregulation via central serotinergic nerve
terminals in addition to high exercise levels,inadequate fluid replacement, and the highambient temperatures often found at'raves'.16 17 Clinical features include cerebraloedema, hypotension, and tissue hypoxia withimpaired myocardial contractility secondary tothermal injury, as are seen in acute liver failure.The coagulopathy arises from a combinationof hepatic necrosis, endothelial cell damage,and thermal inactivation of clotting factors,platelets, and megakaryocytes.
Survival in patients with heatstroke present-ing with a core temperature above 42°C ispoor2 18 and severe hepatic necrosis has beenreported in such patients.'9 20 Patients devel-oping acute liver failure may benefit fromtransplantation but identification of whichcases should be selected is complicated by theoverlap between the clinical and biochemicalchanges in heatstroke and those of acute liverfailure. We have considered as possible candi-dates patients with a core temperature of>41 'C along with biochemical changescompatible with the worst prognosis afterparacetamol overdose, namely systemicacidosis (pH <7.3) or renal failure (serumcreatinine >300 Rumol/l), grade III encephalo-pathy and an INR >7.21 In the only other casereport of liver transplantation after heatstrokeinjury, the patient died after 41 days.22 Thehistological findings of diffuse microvesicularfatty infiltration in case 1, although consistentwith a mitochondrial defect (such as in Reye'ssyndrome), have also been reported in youngmilitary recruits with fatal heatstroke.23Whether ecstasy is directly hepatotoxic in thesecases or results in liver injury over and abovethat resulting from the hyperthermia is difficultto determine.Of the remaining six cases, four had severe
liver damage progressing to acute liver failurein the absence of a hyperthermic episode.All other causes of acute liver failure wereexcluded including hepatitis A, B, C, E, herpesviruses, autoimmune disease, Wilsons'sdisease, and other potentially hepatotoxicdrugs. The illness was characterised bymalaise, nausea and vomiting, hyperbiliru-binaemia, and progressive coagulopathy fol-lowed by the development of encephalopathyand sepsis. One patient survived after trans-plantation, one died of cerebral oedema beforea donor organ became available, and the othertwo died as a result of continuing sepsisbetween three and four weeks post-transplan-tation. The survival rate after transplantation(one of three, 33%) in this group is similar tothat of other reported series of drug inducedacute liver failure and most probably reflectsthe duration of illness before transplantationand a combination of poor nutrition andsepsis. The remaining two cases presented witha milder illness consistent with a less severeprocess of hepatic damage and recovered spon-taneously over a period of three weeks withoutdeveloping severe coagulopathy or encephalo-pathy. In those cases with acute liver damagewithout heatstroke, the development of coagu-lopathy may lead to further deteriorationand referral to a centre with facilities for liver
457
on Septem
ber 4, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.38.3.454 on 1 March 1996. D
ownloaded from

458 Ellis, Wendon, Portmann, Williams
transplantation should be made earlierrather than later as once encephalopathy hasdeveloped, deterioration beyond this is rapid.However, to date there is only one case notedwith a successful result after transplantation.6The mechanism ofMDMA induced hepatic
injury is unclear but a spectrum of severityseems to exist as assessed with histologicalchanges varying from a mild to moderatelobular hepatitis to features of massive hepaticparenchymal collapse with areas of nodularregeneration. The severity of liver damage doesnot seem to correlate with either the amount orfrequency of MDMA ingested suggesting anidiosyncratic type of reaction. Individual sus-ceptibility toMDMA hepatotoxicity is possibleas a single case of recurrent hepatitis afterexposure has been reported.7 Except after anacute collapse with hyperthermia, MDMA willnot be detectable in the urine or blood becauseof the short half life of the drug and the usualinterval between ingestion and presentation. Itis therefore important to include a comprehen-sive drug history, both oral and intravenous, inyoung patients presenting with an unexplainedhepatitis and care should be exercised in followup with the risks of progression to acute liverfailure.
1 Chadwick IS, Curry PD, Linsley A, Freemont AJ,Doran B. Ecstasy, 3-4 methylenedioxymethamphetamine(MDMA), a fatality associated with coagulopathy andhyperthermia. Jf R Soc Med 1991; 84: 371.
2 Tehan B, Hardern R, Bodenham A. Hyperthermia associ-ated with 3,4-methylenedioxyethamphetamine ('Eve').Anaesthesia 1993; 48: 507-10.
3 Manchanda S, Connolly MJ. Cerebral infarction in associa-tion with Ecstasy abuse. Postgrad Med _J 1993; 69: 874-5.
4 Kessel B. Hyponatraemia after ingestion of ecstasy [Letter].BMJ 1994; 308: 414.
5 Dowling GP, McDonough E, Bost RO, 'Eve' and 'Ecstasy'.
A report of five deaths associated with the use ofMDEAand MDMA.JAMA 1987; 257: 1615-7.
6 Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from3,4-methylenedioxymethamphetamine ('ecstasy'). Lancet1992; 340: 384-7.
7 Shearman JD, Chapman RW, Satsangi J, Ryley NG,Weatherhead S. Misuse of ecstasy [Letter]. BMJ 1992;305: 309.
8 Gorard DA, Davies SE, Clark ML. Misuse of ecstasy[Letter]. BMJ 1992; 305: 301.
9 Brown C, Osterloh J. Multiple severe complications fromrecreational ingestion of MDMA ('Ecstasy') [Letter].JAMA 1987; 258: 780-1.
10 Fahal IH, Sallomi DF, Yaqoob M, Bell GM. Acute renalfailure after ecstasy. BMJ 1992; 305: 348.
11 deMan RA, Wilson JH, Tjen HS. Acute liver failure causedby methylenedioxymethamphetamine ('ecstasy'). NedTijdschr Geneeskd 1993; 137: 727-9.
12 Dykhuizen RS, Brunt PW, Atkinson P, Simpson JG, SmithGC. Ecstasy induced hepatitis mimicking viral hepatitis.Gut 1995; 36: 939-41.
13 Shibolet S, Coll R, Gilat T, Sohar E. Heatstroke: its clinicalpicture and mechanism in 36 cases. Q Jf Med 1967; 36:525-48.
14 O'Donnell TF. Acute heatstroke. Epidemiological, bio-chemical, renal and coagulation studies. JAMA 1975;234: 824-8.
15 Olson KR, Benowitz NL. Environmental and drug inducedhyperthermia. Pathophysiology, recognition and manage-ment. Emerg Med Clin North Am 1984; 2: 459-74.
16 Schmidt CJ, Black CK, Abbate GM, Taylor VL. MDMA-induced hyperthermia and neurotoxicity are indepen-dently mediated by 5-HT2 receptors. Brain Res 1990;529: 85-90.
17 Gordon CJ, Watkinson WP, O'Callaghan JP, Miller DB.Effects of 3,4-methylenedioxymethamphetamine on auto-nomic thermo-regulatory responses of the rat. PharmacolBiochem Behav 1991; 38: 339-44.
18 Logan AS, Stickle B, O'Keefe N, Hewitson H. Survivalfollowing 'Ecstasy' ingestion with a peak temperature of42 degrees C [Letter]. Anaesthesia 1993; 48: 1017-8.
19 Kim RC, Collins GH, Cho C, Ichikawa K, Givelber H.Heatstroke: report on three fatal cases with emphasis onfindings in smooth muscle. Pathol Lab Med 1980; 104:345-59.
20 Fidler S, Fagan EA, Williams R, Dewhurst I, Cory CE.Heatstroke and rhabdomyolysis presenting as fulminanthepatic failure. Postgrad MedJ 1988; 64: 157-9.
21 O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Earlyindicators of prognosis in fulminant hepatic failure.Gastroenterology 1989; 97: 439-45.
22 Hassanein T, Perper JA, Tepperman L, Starzl TE, VanThiel DH. Liver occurring as a component of exertionalheatstroke. Gastroenterology 1991; 100: 1442-7.
23 Rubel LR, Ischak KG. The liver in fatal heat stroke. Liver1983; 3: 249-60.
on Septem
ber 4, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.38.3.454 on 1 March 1996. D
ownloaded from