Embed Size (px)
Citation preview

GGuuiiddeelliinneess oonn tthheeMMaannaaggeemmeenntt ooff DDiiaabbeetteess
October 2010

Walsall Guidelineson the Management of Diabetes
These guidelines replace all earlier versions
Objective
Of the estimated 16,500 patients with diabetes in Walsall about 14,500 are looked afterentirely in Primary Care. These guidelines have been produced by a multi-disciplinary teamof professionals with an interest in diabetes to ensure that people with diabetes receive aquality service.
These guidelines have been approved by the Diabetes Local Implementation Team and willbe used to monitor the quality of services and the delivery of the National Service Frame-work in Walsall.
The guidelines will be reviewed on an annual basis by professionals working across thespectrum of diabetes care and, in the event of significant changes resulting from newresearch findings and other best practice guidance, will be updated. It is anticipated thatrevised guidelines will be produced every two years.
Guidelines are meant to guide and inform and should not be rigorously applied in allclinical circumstances. Good clinical practice always involves weighing the advantages anddisadvantages of a clinical intervention depending on individual circumstances.
Chairman of LITDr Andrew Askey
Diabetes Team
Dr Diana RaskauskieneConsultant DiabetologistWalsall Hospitals Trust
Dr Noushad PadinjakaraConsultant DiabetologistWalsall Hospitals Trust
Dr Andrew HartlandClinical PathologistWalsall Hospitals Trust
Helen BladonDiabetes Lead Walsall Community Heath
Joe MyattClinical Nurse Specialist- Diabetes Walsall Community Heath
Sheila PageClinical Nurse Specialist- Diabetes Walsall Community Heath
Marie MaturiClinical Nurse Specialist- Diabetes Walsall Community Heath
Mandy ProffittDiabetes Specialist NurseWalsall Hospitals Trust
Karen GnosillDiabetes Specialist NurseWalsall Hospitals Trust
Emma CunninghamDiabetes DietitianWalsall Hospitals Trust
Samantha BrownDiabetes DietitianWalsall Hospitals Trust
Ian TarrExtended Scope Podiatrist - DiabetesWalsall Community Heath
Zara ShaikhEducational SupportWorker (minority communities)Walsall Community Heath
Paediatrics
Dr B J MuhammedConsultant PaediatricianWalsall Hospitals Trust
Debbie McCauslandDiabetes Specialist NurseWalsall Hospitals Trust
Craig CotterillDiabetes Nurse Walsall Community Heath

Contents
Diabetes - Service Redesign 1
Overview of Management 2
Diagnosis of Suspected Type 1 Diabetes 3
Diagnosis of Type 2 Diabetes 4
Management of Type 2 Diabetes 5
Oral Hypoglycaemic Drugs 7
Insulin in Type 2 Diabetes 8
Titrating Basal Insulin 9
Titrating BD (twice daily) Insulin 10
Ongoing Review of Diabetes 11
The Prevention and Management of Renal Diseasein Adult Patients with Diabetes 12
Hypertension Management in Diabetes 13
Blood Glucose Monitoring Guidelines 14
Diabetic Foot Referral to Podiatry Department 16
Management of Pregnancy in Diabetes 18
Patient Held Record 19
Education 20

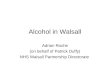
Diabetes - Service Redesign
The Diabetes Local Implementation Team in collaboration with Practice Based Commissionersand local stakeholders outlined a vision for diabetes care in Walsall. The aim: To develop aprimary care led, culturally sensitive service for patients with diabetes. Delivery of the visionwill see that more care is able to be provided to diabetic patients in a community settingthrough a locally enhanced service.
A tiered approach has been adopted to represent the care pathway, with patients receivingtimely care within the appropriate tier. Education for both patients and health care workerswill continue to be provided primarily by the Specialist Community Diabetes Team.
The project plan is currently being rolled out.
1
Tier 1GP
Tier 2aAWP with specialism in
diabetes
Tier 2bConsultant led MD community clinics
Tier 3Hospital based
MD Clinics
Patientpresentsat Tier 1
Patientremainsat Tier 1
Completegenericreferral
and referral
template
Patient referred to Tier 2a as per criteria
Advice/treatmentrecommen-
dation
Prescribeandtreat
Patientreturns
to originalreferrer
Patient remains at
Tier 2a
Patientreturns
to originalreferrer
Patientreturns
to originalreferrer
Escalateto Tier 3
Episode of carefor specific needie: pump start/
foot wound
Patient referred to Tier 2b as per criteria
Patientreferred to
Tier 3 asper criteria
Episode ofcare for
specific needie: duringpregnancy
Patient remains at
Tier 3

Overviewof Management
2
Make the correct diagnosisSymptoms (thirst, polyuria, weight loss) + an abnormal glucoseORNo symptoms but 2 abnormal fasting or random blood glucose results ondifferent daysRandom plasma glucose 11.1 mmol/mol or more.Fasting plasma glucose 7.0 mmol/mol or more.Two-hour plasma glucose 11.1 mmol/mol or more during an oral glucosetolerance test.
Initial assessmentInform the patient of the result as appropriate. Discuss:
provide with ‘my diabetes’ information packinitial dietary adjustments and advice on physical activity to include alcohol and smoking cessation if required patients' thoughts and fears about having been diagnosed with diabetes.Refer to DESMOND ecucation programme, if non English speaking, refer todietitian management plan check Weight, BMI, BP, HbA1c, ACR, Lipids, U&E
Organise follow-up appointment in 4-6 weeks.
Second appointment• Check on dietary change and physical activity. Make further suggestions
where appropriate• blood glucose• weight and BMI• blood pressure• smoking, alcohol and exercise levels• Discuss risks and complications
- feet- eyes- cardiovascular system - kidneys
• Discuss importance of correct self-management with support of surgery team,consider treatment with OHAs if HbA1c > 8% (64mmol/mol)
Make next appointment in 3 months
Agreed by DiabetesLIT 2007
Targets to bereviewed every 3-6 months
Targets to beachievedHbA1c < 7%Fasting glucose 4 –7mmol/lPostprandial< 8 mmol/mol
If targets areachieved, continue:• Diet• Regular exercise• Smoking advice• Moderate alcohol• Education• Monitoring
Review regularly:• Quality of life• Understanding
of condition • Complications• Blood pressure• Lipids• Smoking habits
Lifestyle LinkSupport for smoking cessation and/or support with healthy eating and increasing excerse and activity:01922 444044
Third appointment• Check HbA1c, if not reducing, discuss possibility of treatment by oraltherapy and the implications - explain how control deteriorates with time i.e.progression of condition necessitating changes in treatment
• Discuss results from blood test along with cardiovascular risk factors
• Target HbA1c ≤ 7% (58mmol/mol)
Agree next appointment

Yes
Yes
Yes
No
Yes
No
No
No
Diagnosis of Suspected Type 1 Diabetes
3
Symptoms
� Thirst� tiredness� polyuria� weight loss
Typical symptoms and a diagnostic blood glucose (random > 11.1 mmol/mol or fasting> 7.0 mmol/mol)
Is the patient ill (vomiting or semiconscious)? Admit
Is there moderate / heavy ketonuria?(> 3mmol/L blood test or > ++ urine test)and blood glucose > 15mmol/L
Indication forinsulin. If childrefer immediatleyto PAU
Is the patient under 30 years of age?
No immediate need for insulin.
Dietary advice based on healthy eating principles
First degree relative ondiet or oralmedication fordiabetesFew symptoms/Overweight BMI> 25/No ketonuria/ketonaemia
No immediate need forinsulinConsider non-urgentreferral (see below)
Are the following present?
• Severe symptoms (nocturia x 3-4)• Short history (weeks)• Marked weight loss (irrespective of
absolute weight)• A first degree relative with Type 1 diabetes• A personal history of autoimmune disease• Age less than 40 years
Two or more are anindication for insulin
Contact telephone numbers for advice
Diabetes ReceptionWalsall Manor Hospital 01922 656543
Consultant Diabetologist 01922 656030
Community Diabetes Team Sina Health Centre 01922 406057
Paediatric Assessment Unit (PAU) 01922 656888
Yes

Diagnosis of Type 2 DiabetesScreening for Diabetes
4
Reinforce diet and lifestyle changes.Optimise treatment for cardiovascular risk factorsRepeat fasting glucose or GTT in one year
Random blood test results such as those carriedout at randomscreening may be difficult to interpret andshould not beused to diagnose diabetes.
The use of HbA1cas a diagnostictool for diabetes is currently underreview.
Finger Prick Blood Glucose >5.5
Check Fasting Venous Plasma Glucose
Fasting venous plasmaglucose > 7.0 mmol/mol If asymptomatictwo separate occasions
Fasting venousplasma glucose < 5.6 mmol/mol
Fasting venousplasma glucose5.6 - 6.9 mmol/mol
DIABETES CONFIRMED Consider annualcheck + assess CVSrisk factors.
ARRANGE GTT
Fasting venous plasmaglucose > 7.0 mmol/molOR2-hour venous plasmaglucose
> 11.1 mmol/mol
DIABETES CONFIRMED
Fasting venousplasma glucose < 7.0 mmol/molAND2-hour venousplasma glucose7.8-11.0 mmol/mol
ImpairedGlucoseTolerance
Fasting venousplasma glucose5.6-6.9 mmol/molAND2-hour venousplasma glucose< 7.8 mmol/mol
IMPAIRED FASTING GLYCAEMIA
People who should be screened for diabetes include:Caucasians aged over 40 years Black, Asian and Minority ethnic groups aged over 25 with one or more of the following:BMI > 27, waist circumference females > 80cm (31.5 inches)South Asian males > 89cm (35 inches), other males > 94cm(37 inches)Ischaemic heart diseaseVascular diseaseHypertensionGlycosuria on routine screeningFirst degree family history of diabetesHistory gestational diabetes or Polycystic Ovary Syndrome (PCO)(Then annually)
Symptoms oftenabsent butmay be
• Polydipsia• Polyuria• Nocturia• Lethargy• Weight Loss• Pruritis Vulvae• Balanitis• Blurred Vision• Recurrent
sepsis

HbA1c ≥ 7.5%(a)
(58mmol/mol)
HbA1c < 6.5%(a)
(48mmol/mol) Monitor for deterioration
Add insulin(b,h) particularly if person ismarkedly hyperglycaemic
Insulin + Metformin + Sulphonylurea(d)
HbA1c ≥ 7.5%(a)
(58mmol/mol)
HbA1c < 6.5%(a)
(48mmol/mol) Monitor for deterioration
Metformin + sulphonylurea(d)
Management ofType 2 Diabetes
5
Consider Statin(Simvastatin 40 mg)if aged >40 and totalcholesterol > 3.5mmol/molor if 10- year risk CVD >20%
Consider high intensive statin ie: Simvastatin 80mg or Atorvastatin 40mg in patients with a known history of CVD.
Recheck cholesterol if between 4 - 4.5mmol/Lsee intranet link forinitiating Statins.Click on departmentsthen medicinesmanagement, then quick access to formulary.
NICE care pathway for blood-glucose-lowering therapy.
HbA1c ≥ 6.5% (48mmol/mol) refer toDESMOND (within three months of
diagnosis). After trial of lifestyle interventions
Metformin(b)
Increase insulin dose and intensify regimenover time.Consider pioglitazone with insulin if• A thiazolidinedione has previously had
a marked glucose-lowering effect, or • Blood glucose control is inadequate
with high dose insulin.
HbA1c ≥ 6.5%(a)
(48mmol/mol)
HbA1c < 6.5%(a)
(48mmol/mol) Monitor for deterioration
Consider sulphonylurea here if:• Not overweight (tailor the assessment
of body-weight-associated risk according to ethnic groupc) or
• Metformin is not tolerated or is contraindicated, or
• A rapid therapeutic response is required because of hyperglycaemic symptoms.
Consider rapid-acting insulin secretagoguefor people with erratic lifestyles.
Consider substituting a DPP-4 inhibitori or a thiazolidinedionej for the sulphonylurea if there is significant risk of hypoglycaemia(or its consequences) or a sulphonylurea iscontraindicated or not tolerated.
Consider adding a DPP-4 inhibitor or a thiazolidinedionej instead of insulin if insulin is unacceptable (because of employment, social, recreational or otherpersonal issues or obesity).Consider adding exenatide to metforminand sulphonylurea if:• BMI > 35kg/m2 in people of European
descent and there are problems associated with high weight or
• BMI < 35kg/m2 and insulin is unacceptable because of occupational implications or weight loss would benefit other co-morbidities.
Keya. Or individually agreed targetb. With active dose titrationc. See the NICE clinical guidance on obesity
(www.nice.org.uk/CG43)d. Offer once-daily sulphonylurea if
adherence is a probleme. Only continue DPP-4 inhibitor or
thiazolidinedione if reduction in HbA1c of at least 0.5 percentage in six months
f. Only continue exenatide if reduction in HbA1cof at least 1 percentage point and weight loss of at least 3% of initial body weight at six months.

6
Consider adding a DPP-4 inhibitor(i) or a thiazolidinedione(j) if metformin contraindicated
or not tolerated.
HbA1c < 6.5%(a)
(48mmol/mol) Monitor for deterioration
Sulphonylurea(d)
HbA1c ≥ 6.5%(a)
(48mmol/mol)
HbA1c ≥ 7.5%(a)
(58mmol/mol)
Metformin(b) + sulphonylurea(d) + sitagliptin,(e)
Or metformin(b) + sulphonylurea(d) + a thiazolidinedione(e),j or metformin(b) +
sulphonylurea(d) + exenatide(f)
HbA1c < 7.5%(a)
(58mmol/mol) Monitor for deterioration
Metformin(b) + DPP-4 inhibitor(e,i) or a thiazolidinedione(j)
HbA1c < 7.5%(a)
(58mmol/mol) Monitor for deterioration
Sulphonylurea(d) + DPP-4 inhibitor(e,i)
or a thiazolidinedione(e,j)
HbA1c ≥ 7.5%(a)
(58mmol/mol)
HbA1c < 7.5%(a)
(58mmol/mol) Monitor for deterioration
HbA1c ≥ 7.5%(a)
(58mmol/mol)
HbA1c < 7.5%(a)
(58mmol/mol) Monitor for deterioration
HbA1c ≥ 7.5%(a)
(58mmol/mol) Start insulin(b,h)
g. Only continue DPP-4 inhibitor or thiazolidinedione if reduction in HbA1c of at least 0.5 percentage in six months with adjustment for other ethnic groups
h. Only continue DPP-4 inhibitor or thiazolidinedione if reduction in HbA1c of at least 0.5 percentage in six monthsContinue with metformin and sulphonylurea
(and acarbose, if used) but only continue with other drugs that are licensed for use with insulin.Review the use of sulphonylurea if hypoglycaemia occurs.
i. DPP-4 inhibitor refers to sitagliptin, vildagliptinand saxaliptin
j. Thiazolidinedione refers to pioglitazone
NICE guideline 87 May 2009

7
Oral Hypoglycaemic Drugs
Metformin
• Start with 500mg daily (standard release)for 1-2 weeks.
• Titrate every 1-2 weeks to max dose of1.5g BD.
• GI disturbance may be prevented bygradually increasing the dose over time.
• Take with or immediately after a meal.• Modified release metformin should be
considered in patients who cannottolerate standard release. Maximum doseof modified release is 2g daily (available in1gm tablets. Metformin also in powderform for those unable to swallow largetablets).
• Not associated with weight gain.
CONTRAINDICATED in patients with • creatinine > 150 µmol/L, eGFR < 30• severe heart failure/COPD • severe liver disease (ALT > 3 x normal level)
Metformin should be stopped 48 hoursbefore and after any radiological procedureneeding intravenous contrast.
GGlliippttiinnss
These are dipeptidyl peptidase - IV (DPP-4)inhibitors, and therefore slow the breakdownof incretin hormones produced in the gut.These hormones play an important part inglucose regulation including stimulation ofinsulin synthesis, inhibition of glucagon secretion, delay in gastric emptying, andpromotion of satiety. These drugs haveshown to be weight neutral and are generally well tolerated however GI disturbance may occure.
Drugs include: • Sitagliptin and• Vildagliptin.
Sulphonylureas
• Gliclazide 40-80 mg OD, titrate every4-6 weeks until max 160mg BD orGlimepiride 1mg OD titrate every4-6 weeks until max 6mg OD.
• Tablets should be taken before meals.• Weight gain is a recognised side effect.• Educate on management of
hypoglycaemia. • Educate regarding need to inform DVLA
and insurance.• AVOID Glibenclamide in patients over
70 years and in those with poor renalfunction
Thiazolidinedione(Pioglitazone)
Current NICE recommends combinationwith either metformin (preferably) orsulphonylurea, however are frequently usedwith both when glycaemic control is notsatisfactory with one agent.
The use of this class of drug should
be carefully considered as there is anestablished risk of weight gain along withheart failure, oedema. There is also a riskof fractures occuring in women. Patientsshould be carefully assessed forcardiovascular risk prior to its use.
GLP - 1 Mimetics
These drugs mimic the action of incretinhormones and are resistant to the effects of DDP-4. The are given by sub-cutaneousinjection once or twice daily. They havebeen shown to help with weight reduction.However, may cause some GI side effects,particularly nausea; this usually improvesafter 4-5 days.
Drugs include: • Exenatide and• Liraglutide (awaiting NICE guidance due
in October 2010)• Recommend discontinue if patient has
not achieved a 1% reduction in HbA1cand 3% reduction in weight at six months.

Insulin inType 2 Diabetes
8
Caution: Insulin therapy should only be initiated in practices where thenecessary skills and experience is in place to do so effectively and safely.
Patient on maximum tolerated oral combination therapy, with poor glycaemic controlHbA1c > 7.5% (58mmol/mol)
Insulin appropriate on clinical grounds and patient happy to use insulin
Patient performing home blood glucose monitoring?
Teach home bloodglucose monitoring
Once daily insulin
Initiate glargine/detemir
Check HbA1c and reviewtherapy every 3-6 months
Control remains poor Refer to specialist services
Twice daily pre-mixed insulin
30/70 mix or 50/50 mix
Review oral hypoglycaemic agents asapplicable:
Continue Metformin and consider ifother anti-hyperglycemic medicationshould continue or should be stopped
Decide on most appropriate insulin regime:(particulary if HbA1c > 8%(64mmol/L))Either once daily insulin glargine/detemir(see NICE guidance)or twice daily pre-mixed standard or analogue insulin
NoYes
YesNo

9
Titrating Basal InsulinScheme for Insulin Glargine or Detemir once daily
Start basal insulin 10 units daily
Reduce topreviousdoseimmediatelyif glucoseless than4mmol/L onany day
Refer tospecialistservices
Increase dose every 4 days as per chart(if fasting glucose higher than target on2 consecutive days prior to expecteddose change)
Check HbA1c 3 months after stable insulin dose and6 monthly thereafter
HbA1c above target, hypoglycemia or othermanagement problems
Caution: Insulin therapy should only be initiated in practices where thenecessary skills and experience is in place to do so effectively and safely.
Algorithm for Insulin Dose TitrationAfter consideration of changes in diet/activity
Less than 4 Reduce insulin to previous dose
4 - 6 No change
Greater than 6 Increase dose by 2 units
Fasting Blood Glucose (mmol/mol) Insulin Dose Change (units)
Note:Glargine orDetemir should begiven at approxsame time eachday. (Taking insulinin an evening is thepreferred option)
Target:Fasting glucose < 6mmol/lHbA1c < 7.5%(58mmol/mol)
Start daily fasting (pre-breakfast) glucosemonitoring (additional glucose tests onlyif patient feels unwell)

Titrating BD (twice daily) InsulinScheme for Biphasic pre-mixed Insulin
10
Note:Dose Timing: Biphasic immediately no longer than 5-10 minutes prior to food.Morning Insulin affects pre-lunch and pre-tea levelsEvening Insulin affects bedtime and fasting glucose levelsReduce Insulin to previous dose immediately if glucose less than 4mmol/l on any day.Dose titration schedules are a guide and can be modified as necessary.
Pre-teaglucose
Dosechange
Pre-lunchglucose
Less than 4
Between 4-7
Between 4-7
Greaterthan 10
Less than 4 Reduce toprevious
Between 4-7
Between 7-10
No change
Greaterthan 10
Increase by2 units
Adjustment of morning insulin dose:After consideration of changes in diet/activity
Pre-breakfastglucose
Dosechange
Pre-bedglucose
Less than 6
Between 6-10
Between 6-10
Greaterthan 10
Less than 4 Reduce toprevious
Between 4-7
Greater than 7
No change
Greaterthan 7
Increase by2 units
Adjustment of evening insulin dose:After consideration of changes in diet/activity
Target:Premeal Glucose:4-7mmol/LBedtime Glucose:6-10 mmol/molHbA1c < 7.5%(58mmol/mol)
Start Insulin 12 units before breakfast and8 units before evening meal
Refer tospecialistservices
HbA1c >target/othermanagementproblems
Increase dose every 4 days as algorithm(if glucose higher than target on2 consecutive days prior to expecteddose change)
Difficulty in dose titration, hypoglycemia
Check HbA1c 3 months after stable insulindose, and 6 monthly thereafter (reducefrequency of home glucose monitoringwhen on stable insulin doses)
Start 2 times daily (fasting, pre-lunch,pre-tea and bedtime) Blood glucosemonitoring
Titrating Basal InsulinScheme for Insulin Glargine or Detemir once daily

11
Ongoing Reviewof Diabetes
Plans should be made in conjunction with the patient, and recorded in the Patient HeldRecord for:Hyperglycaemia, hypertension, hyperlipidaemiaConsider Statin (Simvastatin 40 mg) if aged > 40 and total cholesterol > 3.5mmol/L. For further information see NICE clinical guidance 87. Type 2 diabetes. May 2009.
Renal
• Blood pressure• Microalbuminuria • Creatinine
Vascular
• Discuss to stopsmoking
• Diet review• Advise on exercise• Lipids• BP
Retinopathy
• Retinal screeningprogramme usingdigital photography
• Screening not requiredif attending hospitalOphthalmologyservices
Foot Care
• Deformity/callus• Check dorsalis pedis
and posterior tibialfoot pulses
• Vibration perception• 10g Seimes-Weinstein
monofilament(if available)
• Active foot ulcers
On-going review is an essential part of the planned management of people withdiabetes. The following should be covered during the annual review process:
Weight/BMI, BPPatient’s monitoring recordsSymptoms of hyperglycaemiaEpisodes of hypoglycaemiaProblems with medicationInjection sites for lipohypertrophyProblems with eyesight, parasthesia,erectile dysfunctionMacrovascular disease - angina, TIA,claudication
Bloods forHbA1cCreatinineLipids (see page 5)
(Target total cholesterol ≤ 4.0mmol/L,
LDL ≤ 2.0mmol/L. For more details seeNICE guidance Lipid modification No.67 May 2008)
Urine forAlbumin/creatinine ratio
Renal :See page 12

Walsall Manor Hospital Biochemistry Department/Walsall Diabetes NSF Local ImplementationTeam/Wolverhampton Renal Unit. For further information contact: Dr PD Giles, ConsultantChemical Pathologist, Manor Hospital, Walsall: [email protected] with acknowledgement to David Crothers, Biochemistry, Walsall Manor Hospital.
The Prevention and Management of RenalDisease in adult Patients with Diabetes
12
Review complications and risk factors for renal disease on diagnosis of diabetes in adults and at least on an annual basis as follows:
Measure urine albumin:creatinineratio. Use a first morning urine sample where practicable
Repeat urine test twice within1 Month. Use a first morningurine sample where practicable
Lower RiskMaintain good bloodglucose control.HbA1c below 7.5% according to individual’starget and good bloodpressure control target130/180mm Hg
Review use of MetforminIf eGFR 45-59 and stable continuemetformin as before;If eGFR 30-44, or if eGFR 45-59and worsening, consider reducingmetformin dose; If eGFR below 30 stop metformin.
Are 2 out of 3 tests abnormal?ie: in the microalbuminuric or proteinuric range?
Assess glomerular filtration.Measure serum creatinine; estimateeGFR by modified MDRD formula
Is Microalbuminuria or Proteinuria present?Microalbuminuria Albumin: creatinine ratio>2.5mg/mmol (men) or >3.5mg/mmol (women)Proteinuria Albumin: creatinine ration ≥30mg/mmol
Is glomerular filtration impaired?ie: is eGFR < 60ml/min/1.73m2?
And
No
Yes Yes
Yes YesHigher Risk: Albuminuric and/or Impaired Glomerular Filtration
Consider Referral to Nephrologist
1. Consider the possibility of non-diabetic renaldisease: History, examination, urinalysis (including microscopy and culture),renal ultrasound, other investigations as appropriate.
2. Begin/optimise therapy with ACE inhibitor. Test eGFR (or creatinine) and serum potassium before ACEI (or ARB) initiation, repeat after 1-2 weeks of treatment and after each dose increase. Titrate ACEI to maximum tolerated therapeutic dose before adding second line hypertensive.
3. Target blood pressure below 130/80(SBP range 120-129mm Hg) Combination therapy likely in most patients.
4. Tight blood glucose control: Target HbA1c below 7.5%
5. Avoid nephrotoxins, including NSAIDs 6. Lipid-lowering in diabetics with significantly impaired. GFR is of unknown effectivenessPatients should be treated in accordance with JointBritish Societies Guidelines or offered entry into an appropriate trial.
7. General Health Measures Smoking cessation advice. Control body weight, and alcohol and salt intake. Immunisation against influenza and pneumococcus
1. Severe deterioration in glomerular filtration rate. either - e-GFR less than 30ml/min/1.73m2 or - significantly declining eGFR (over 5ml/min/1.73m2
in 1 year or over 10/ml/min/1.73 m2 within 5 years) in a patient with eGFR in the range 30-59ml/min/1.73m2
3. Suspected renal artery stenosis
2. More severe albuminuriaUrine albumin: creatinine ratio > 70 mg/mmolIndicative of worse prognosis and/or non-diabeticnephropathy
4. Non-diabetic renal disease suspected e.g. patients with combined haematuria & proteinuriaor evidence of multisystem disease or diabetes ofshort duration and/or without retinopathy
8. Annual (more frequent if unstable) measurements of: Haemoglobin. Serum U&E, creatinine, albumin. Urine albumin: creatinine ratio
ReferencesType 2 Diabetes - National Institute forClinical Excellence2008.Chronic Kidney Disease- National Institute forHealth and Clinical Excellence 2008.The National ServiceFramework for RenalServicesPart one: Dialysis andTransplatation 2004Part two: Chronic Kidney Disease, AcuteRenal Failure and Endof Life Care 2005Department of Health
5. Hyperkalaemia i.e. serum K > 6 mmol/mol After addressing exacerbating factors e.g. spironolactone, ACEI / ARBs, beta blockers, NSAIDs

13
HypertensionManagement in Diabetes
BP > 130/80
ACE Inhibitor e.g. Ramipril 2.5-10 mg, Lisinopril 10-40mg, Enalapril 5-40mgIf generally unable to tolerate consider A2RB eg. Losartan 25-100mg, Irbesartan 150-300mg, or Candesartan 8-32mg
Uncontrolled (BP > 130/80, sustained over at least 3 readings)consider 2nd line agentdiuretic eg Bendroflumethiazide 2.5mg
Uncontrolled (BP > 130/80, sustained over at least 3 readings) check complianceConsider 3rd line agentCalcium chanel blocker eg Felodipine 2.5-10mg, Amlodipine 5-10mg,Diltiazem 180-360mg
Uncontrolled on 3 classes of drugs (BP > 130/80) Consider referral to tier 2 or 3Consider 4th line agentCardioselective betablocker eg Bisoprolol 2.5-10mg, Atenolol 25-50mgAlpha blocker eg Doxazosin 2 - 16mg(A2RB eg Losartan 25-100mg or Irbesartan 150-300mg)
Lowering of BP in Type 2 diabetes is associated not just with a reduction in the risk of CVD but also eye and kidney microvascular complications. A BP-lowering strategy is thusparticularly effective and cost effective in those with diabetes kidney,eye or cerebrovasculardamage, with interventional thresholds and targets of 130/80mm/Hg in those people and140/80mm/Hg in all others. Strategy should include lifestyle advice, medications if lifestyleadvice does not achieve targets, and monitoring every one to two months with intensificationof medication if not to target.

Blood GlucoseMonitoring Guidelines
14
Who should Test?
The following is general guidance on thefrequency of blood glucose testing indiabetics. This should be discussed with thepatient and the frequency of testing agreedwith the patient, taking into account his/hercircumstances at the time.
Diet alone
Type 2 Diabetes, controlled with diet alone Ifpatient is stable, probably does not need tomonitor blood glucose at home.Recommend 3-4 monthly HbA1c.
Oral medication
Type 2 Diabetes, on diet plus oralhypoglycaemic treatment.If the patient is stable, there is littleevidence to support routine home bloodglucose testing in patients who are not oninsulin treatment. It is acknowledged,however, that home blood glucosemonitoring may be appropriate for patientson diet/oral hypoglycaemics in certain clinicalcircumstances, for example:• To aid education in newly diagnosed
patients or patients with poor glycaemic control
• In patients suspected of experiencinghypoglycaemic episodes onsulphonylurea/metformin
• In patients already established ona regime of home blood glucosemonitoring which is significantlycontributing to glycaemic control.
• During ante-natal assessment In these circumstances the aims ofhome blood glucose testing should bediscussed with the patient. Frequencyof testing will be determined by clinicalcircumstances.
Recommend 3-4 monthly HbA1c.
Insulin
Blood glucose monitoring is important inpatients treated with insulin to ensure thatthe dose of insulin is appropriate. One ortwo multipoint profiles per week are theminimum accepted frequency, for example,before breakfast, 1-2 hours after breakfast,before evening meal and after evening meal.
Where patients adjust the dose of insulinaccording to their blood glucose level thenthis should be taken prior to insulin injection.The exact frequency of monitoring for thesepatients should be appropriate to thelifestyle of the patient.
Blood glucose testing may need to increasewhere there are significant changes inlifestyle or the patient is unwell. Othersituations where more frequent bloodglucose testing may be appropriate include:• Suspected hypoglycaemic episodes, to
assist patients to achieve better control, until good control is achieved
• HbA1c high: symptoms of hyperglycaemia,until good control is achieved
• Short-term need to monitor blood glucosemore frequently. e.g. during intercurrent illness; diabetes in pregnancy.
• Recent change in treatment, until patient is stabilised
General Advice about blood glucosemonitoring
Single readings are of relatively limited valueexcept to confirm or exclude the possibilityof acute hypoglycaemia.Multipoint profiles are preferred.
Choice of meters
A wide choice of meters are available.Patients should be guided to choose a meterthat they are able to use. They should thenuse the testing strips appropriate to thatmachine. It is useful for practices to keep anote of the blood glucose meter thatpatients use and ensure that patients keepthis information updated. Patients should bereminded of the importance of regularcalibration and cleaning.
It is essential that patients are taught clearlyhow to take their blood glucose level usingthe meter and test strip that they havechosen. 50% of self-monitored bloodglucose measurements are inaccurate,usually due to operator error, for exampleforgetting to wash hands.
Patients should understand clearly why theyare testing their blood glucose.It should not be considered a stand-aloneactivity. Diabetics should be recommended

15
to record their blood glucose results (withdate and time) along with any symptoms ofdiabetic problems to provide a cumulativerecord. Along with HbA1c, this can thenform the basis of treatment modifications atdiabetic review.
Patients purchasing meters should beencouraged to see the practice nurse forguidance on blood testing. Local communitypharmacists should also be advised toforward such patients to their practice nurse.
Advice on repeat prescriptions of bloodglucose monitoring strips.
There is significant wastage of blood glucosemonitoring strips through over prescribing,over-ordering by patients and unnecessaryblood glucose testing. There are a number ofways to reduce unnecessary prescriptionsincluding:• Only prescribing blood glucose tests on
acute prescriptions thereby making it easierto monitor and control the supply of blood testing strips in line with patient needs
• Including on the prescription thenormal directions for use, enabling better compliance checks to be made by practice staff
• Reviewing use of lancets and aligning the quantity prescribed with that of testing strips.
NB It may also be useful including in anydiabetic review the question “How oftendo you test?”
Urine testingUrine testing for glucose is not recommendedfor routine monitoring of glycaemic control.It is noted, however, that urine testing doesform part of the DESMOND educationprogramme for patients with Type 2 diabetesand so may be useful as part of thisprogramme.
Testing for ketonesBlood or Urine testing for ketones is useful indetecting early onset Diabetic Ketoacidosis inType 1 diabetes. We recommend all patientswith Type 1 diabetes have the facility to test
for ketones (either blood or urine test) duringtimes of illness or when a rise in ketonelevels is suspected.

Diabetic Foot ReferralPodiatry Department
16
Diabetes specialist foot care is located at Sina Health Centre,230 Coppice Farm Way, Willenhall WV12 5XZ.Telephone: 01922 406057 Fax: 01922 404327.
Podiatry department based at Lichfield House Telephone: 0845 1130607.
Chronic
Acute
Red or swollen area on footor early stages of ulceration
FFOOOOTT UULLCCEERRNon-healing ulcer:ie shown nosign of major improvementwithin 4 weeks
Foot problems needing vascularassessment but not requiring urgent action.
Chronic painful neuropathy
Charcot Joint AlertHot swollen, neuropathic, diabeticfoot - no signs of infection - Suspect Charcot Arthropathy
Severe Infection abscess or pus
Severe Infectionin non-healing ulcer, spreading cellulites
Acute/Critical IschaemiaFeatures include the following:• Discoloration of toes; pale,
dusky, black• Signs of necrosis• Pain at rest, often at night• Cold• Dimnished/absent pulses• If in doubt, refer for admission,
assessment or urgent vascular appointment
Communitycare initially, GP, nurse, podiatryantibiotics. If not improving:
Community FootProtection Team
All Patients Designated asHigh Risk:• Ongoing review
by advanced diabetes podiatry service
• Follow-up by Diabetes Centre if appropriate, including long-term risk factors, eg; smoking, lipids
• Information given about future foot care, how to access services in an emergency, and how to contact DNS
• Once healed refer to orthotics for footwear
Recommendedantibiotics
Flucloxacillin250-500mg QDS
co-amoxiclav625mg TDS
If allergy to penicillin Erythromycin500mg QDS
Metronidazole (inthe presence ofanaerobes)400mg TDS
Accident andEmergency
MAU DiabeticFoot DVT teamensure vascularassessmentwithin 24 hoursand refer to vascular team,Manor Hospitalif appropriate.Telephone:721172 ext 7763
For treatment of painful diabetic neuropathy see NICE clinical guideline 96 (neuropathic pain march 2010)

17
ErectileDysfunction
Patient known to have diabetes experiencing Erectile Dysfunction
Total Testosterone (taken before 10.00am)> 12nmol/L - does not require treatment< 8nmol/L - will usually require treaatment8 - 12nmol/L - repeating the measurementof total testosterone and calculating freetestosterone may be helful. Considerreferral to consultant endocrinologist(before testosterone therapy is commencedprolactin, LH, FSH should be checked.
Check testosterone
Sildenafil 50mg or 100mg
Vardenafil10mg or 20mg
Combination Therapy
M.U.S.E. Intra cavernosalInjection
Vacuum Pump
Tadalifil 10mg or 20mg
HbA1c, TSH,Lipid profile
Normal Limits
Taking Oral Nitrates
Refer to ED clinic (GU MED Dept)
Treat asnecessaryto optimise
• Testosterone therapy Testogel 5g gel od for3 months, if ED improves consider continuing.
• If long-term maintenance dose required, consider Depo injection.
• Prior to therapy with testosterone risk of prostate cancers must be assessed using a minimum digital rectal exam (DRE) and determination of serum Prostate Specific Antigen (PSA)haemotocrit and LFT’s.
• Repeat at 3-4 months and again at 12 months, then annually.
Low testosterone
YesNo
Abnormal
OR
OR
Approx. 50% efficiency in patients with diabetes. Durationof action 6-7 hours. Side effectsincude headache, facial flushing,possible visual disturbances.
Approx. 50% efficiency inpatients with diabetes.Duration of action 24 hours.Side effects incude headache,back pain and facial flushing.
Approx. 70% efficiency in patients with diabetes.Duration of action 6-8 hours.Side effects incude headacheand facial flushing.

Management ofPregnancy in Diabetes
18
Pre pregnancy1. All women (of child bearing age) should
receive pregnancy advice at each visit (this should be documented in case notes) highlighting:a) The benefits of pre conception
glycaemic controlb) The importance of planning
pregnancy and avoiding unplanned conception
c) Contraceptive advice
2. If planning pregnancy:a) Ensure good glycaemic control
(HbA1c < 6.5% (48mmol/mol), ideallyHbA1c < 6.1% ((43mmol/L) is safe) before stopping contraception. If HbA1c is >10 (86mmol/L) advise to avoid pregnancy
b) Advice regarding hypoglycaemia and hypoglycaemia awareness
c) Encourage diet and exercise and weight management (to BMI < 27 kg)
d) Start Folic Acid 5 mg ode) Review ongoing medications (stop
ACE, AII, consider alternative for blood pressure, e.g. Labetalol, Methyldopa, stop Statins)
f) Make sure screening forcomplications is up to date:-
• Retinal photos (do not offer rapidoptimisation of glycaemic control until after retinal assessment and treatments are completed)
• Urine ACR, U & E (refer if ACR is positive or serum creatinine is > 120 or GFR is < 45)g) Refer to specialist diabetes service if
requiredh) Refer to combined diabetes antenatal
clinic immediately after pregnancy is confirmed
Safety of Medications Beforeand During Pregnancy 1. Stop oral hypoglycaemic agents apart
from Metformin as soon as pregnancy confirmed and consider insulin
2. Stop ACE and ARBs IMMEDIATELY and consider alternative anti-hypertensives,e.g. Methyldopa or Labetalol
3. Stop STATINS4. Refer to combined diabetes antenatal
clinic.
Gestational Diabetes(In liaison with Community Midwives)1. Risk factor for gestational diabetes:
a) BMI > 30b) Previous macrosomic baby 4.5 kg or
more
c) Previous gestational diabetesd) Family origin with high prevalence of
diabetes - South Asians, Black Caribbean Middle Eastern
2. If any of above risk factors (except c - see point 3 below) perform oral glucosetolerance test (OGTT) at 24-28 weeks gestation.
NB Do not use fasting glucose, randomglucose or urinalysis for screening
3. If previous gestational diabetes:Eithera) Early BM monitoring starting at
16-18 weeks (refer to combinedantenatal clinic) or
b) Organised glucose tolerance test at 16-18 weeks, if OGTT negativerepeat a 24-28 weeks
c) Information and advice before screening. Advise that:
1. There is a small risk of birth complications if gestational diabetes is not controlled
2. Gestational diabetes will respond to diet and exercise in most women
3. Oral hypoglycaemic agents or insulininjections may be needed if diet andexercise do not control blood glucoselevels
4. Extra monitoring and care may be needed during pregnancy and labourd) Refer to combined antenatal diabetic
clinic if screening positive.
Post Natal Care1. Women with diabetes who are breast
feeding to continue to avoid drugs that were discontinued for safety reasonsduring or pre pregnancy
2. Risk of hypoglycaemia, especially while breast feeding (to have food availablebefore and during breast feeding)
3. Metformin and Glibenclamide can be taken during breast feeding BUT NOT any other oral hypoglycaemic agent (see NICE Guidelines)
2. Women with gestational diabetes:a) Advise on risk of diabetes (35-50%
risk of developing type II diabetes)b) Increase risk of gestational diabetes
in further pregnancyc) Importance of weight control, diet,
exercise and healthy lifed) Fasting blood glucose at six weeks
post natal then annually to screen for type II diabetes, to be carried out by GP.

19
My Diabetes Informationand Resource Pack
All patients shall be given a copy of theWalsall ‘My Diabetes Information andResource Pack’ which includes the hand held record for:
• Patient Information• Medications record• Management chart• Diabetes review sheet• Treatment goals• Education checklist
All patients with diabetes should be giventhe Patient Record by their GP practice alongwith an explaination of how this should beused. The record should be brought withthem when attending appointments withany relevant HCP. The record is an essentialpart of diabetes management and shouldbe completed following consultation with aHCP, it will serve as a valuable tool, for boththe patient and HCP, aiding a partnershipapproach to diabetes management.
The education section of the handheldrecord card should be used in conjunctionwith the Walsall Diabetes Education Plan.
Patient leaflets supporting this plan are available on the intranet.

Education
20
DESMOND
DESMOND stands for: Diabetes Educationand Self Management for Ongoing andNewly Diagnosed.
This is a nationally accredited formaleducation programme for people withnewly diagnosed Type 2 diabetes.
This programme commenced in Walsall inJune 2006.
All English speaking patients newly diagnosed with Type 2 diabetes within 12 weeks of diagnosis should be offeredthe opportunity to attend the educationprogramme. In order to do this a referralform should be fully completed and sent to the DESMOND co-ordinator community diabetes team at Sina Health Centre. The individual will then be contacted with a list of dates and venues to choose from.
This programme consists of six hours of education. The individual can choosewhether to attend an all day session or two half day sessions.
Walsall DiabetesEducation Plan
Having completed discussion on aneducation topic the health care professionaland the patient should sign the diabeteseducation list in the hand held record and a copy should be kept in the notes of thehealth care professional. All discussionsshould be supported with literature.
Discussion of topics on educationchecklist includes:
What is Diabetes?
• How blood glucose is controlled before diabetes.
• What happens to glucose control indiabetes.
• Types of Diabetes, contributing factors.• Causes of signs of diabetes.• Outline of treatment of diabetes.• Progressive nature of diabetes.
Lifestyle Issues
Significance and implications of a diagnosisof diabetes re.travel, sex, smoking, driving.
Diet
• Diet principles/healthy eating and drinking.• Assess current diet including cultural/
religious needs eg. fasting.• Changes in diet, meal planning and
cooking needed to follow healthy eating principles.
• Effect of alcohol.• Effects of diet on weight and weight on
blood glucose control.• Benefits of strategies for weight
management if required.
Activity and Exercise
• Effect of physical activity on bloodglucose level, blood pressure and weight.
• Importance of physical activity.• Need to consider pre existing health
problems before embarking on increased activity.
• Risk of hypoglycaemia/preventing/treating hypoglycaemia.
• Inform of support available/contactnumber for One Call for All Activity Services.
Driving DVLA Insurance
• If on tablets or insulin treatment, need to inform the DVLA and insurance company.
• Importance of avoiding hypoglycaemia whilst driving.
• Implications of diabetes regardingvocational licences.
• Medical checks to expect, (see the lowblood sugar leaflet).
Smoking
• Effect of smoking.• Benefits of stopping.• Advise on support available, supply
telephone numbers, enter whether or notwish to stop smoking in comments box.
Pregnancy/Gestational Diabetes -
Remember to refer to the Diabetes NurseSpecialist when considering pregnancy for:
• Use of contraception until glycaemic control targets acheived (HbA1c 6.5% (48mmol/mol)
• Preconception advice: the importance of

21
good control at the time of conception as well as during pregnancy.
• Pregnancy: support and examinationsto expect, dietary and treatmentmodifications.
• Relationship between blood glucosecontrol and pregnancy outcomes.
• Risk of maternal and fetal complications.• For gestational diabetes: diet advice,
discuss insulin treatment if applicable, and reducing the risk of developing diabetes after pregnancy.
Insulin and Injection Technique• Discuss insulin regimens and types of
insulin.• Injection sites and technique.• Duration of action of prescribed insulin,
and timing of injections.• Storage of insulin.• Disposal of sharps.• Insulin dose adjustment.• Relationship between diet, exercise and
insulin.• How to manage changes from usual
routine.
Medicines
• Name, dose, timing, side effects ofprescribed medicine.
• How the prescribed medication works.• Relationship between diet, activity and
medication.• How to manage changes in usual routine
eg. fasting.
Low Blood Glucose(Hypoglycaemia)
• Causes.• Signs and symptoms, (how I will feel,
how I will appear to others).• Treatment.• Prevention.• Reducing the risk, planning for extra
activity, including sex.• Implications for driving, working at
heights.• When to seek advice.• Indications for changing treatment.• Need to carry identification and source of
glucose.
High Blood Glucose(Hyperglycaemia)
• Causes.• Signs and symptoms, (what you may
notice).• Action to take.• Indications for changing treatment.• When to seek advice.
Illness
• Effect of illness on diabetes.• Continuing medication.• Increasing monitoring - indications for
increasing treatment.• Increasing fluids.• Food replacement.• Signs, symptoms and action to take
re: Ketones.• Signs, symptoms and action to take
re: Hyperosmolar non ketotic coma.• When to seek advice.• Immunisations, (flu, pneumonia), to
reduce risk of illness.
Monitoring Glucose Level
• Significance of glucose control.• Targets for glucose control.• How/when to monitor (home testing and
clinic tests).• Technique for home monitoring method
selected.• Significance of the results.• When action on results is required.
Annual Review
• Outline chronic complications, (macrovascular, microvascular and neuropathic) andthe place of ongoing review to screen for/detect complications and monitor the effect of current treatment.
• Risk factors associated with chroniccomplications eg. Hypertension,hyperglycaemia, smoking, inactivity,BMI 26 and above.
• Importance of regular review and what this should include.
• Targets for glucose, lipid and bloodpressure control.
Foot Care• Factors that increase the risk of foot
problems in diabetes.

• Importance of daily foot examination todetect problems promptly.
• Importance of daily foot care routine to promote the integrity of the skin.
• Signs/symptoms indicating the need for prompt medical assessment.
• Importance of foot assessment as part of annual review.
• Ensure only consult state registeredchiropodists.
• Inform when/how to access podiatry.
Eye Checks• Outline reasons for eye screening.• What retinal screening includes.• Inform how to access eye screening.• Inform that annual eye screening is free
of charge.
Diabetes UKInform of charity for people with diabetes.Details in handbook.
Prescription ExemptionCertificate
• Ensure aware of entitlement to freeprescriptions if prescribed oral diabetes medication or insulin.
• Inform how to obtain the exemptioncertificate.
DAFNEDose Adjustment For Normal Eating.This is a nationally accredited formaleducation programme for people withType 1 diabetes.
This is a five day course run by speciallytrained diabetes nurses, dietitans and consultants.
PPuummpp TThheerraappyy
Insulin pumps are available to a small selectgroup of patients with Type 1 diabetes inWalsall who should meet the followingcriteria.
1. All adults should fulfil the criteria in theNICE guidelines.
a. They are using a MDI with a glargine/Detemir insulin regime.
b. They continue to have poor control despitethe above.
2. They are motivated, as demonstrated byregular contact with the diabetes team.
3. Diligent hospital attendance.4. They are doing a minimum of 4 Blood
Glucose Tests per day.5. They can demonstrate good dietary
knowledge, e.g. carbohydrate value 6. They have a good understanding of the
physiology of diabetes.7. The adult wishes to improve their control
not just their carers8. They and their carers are prepared to
undertake and complete the training programme.
9. They agree to comply with instructionand direction after pump therapy has started.
10. Pump therapy is not suitable for allpeople and the decision to initiatepump therapy remains the prerogativeof the diabetes team.
11. The pump remains the property ofWalsall Hospitals NHS Trust.
12. They agree to ensure the pump isinsured as part of their householdcontents and provide evidence of this tothe diabetes team.
13. They keep the pump safe and use itappropriately.
14. They are responsible for the safe keepingof the pump, if it is lost, stolen, or brokenthey are responsible for it’s replacementor reimbursement to Walsall HospitalsNHS Trust.
15. Walsall Hospitals NHS Trust will notprovide a second pump.
16. If the pump is not being used or controland/or quality of life does not improvethe pump will be returned to WalsallHospitals NHS Trust promptly.
Contraindications
1.Those patients who are not motivated.2.Those who do not perform a minimum
of 4 daily blood glucose Tests.3.Those who cannot achieve the
competencies required.
Caution
1. Those who have proliferative or preproliferative retinopathy as pump therapymay temporarily make this worse.
Relative Contraindications
1. Severe or end stage diabetes.2. Blindness.3. Lack of support from friends and or family.
Education

Notes