Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry 1990;53:1080-1083
Grading white matter lesions on CT and MRI:a simple scale
J C van Swieten, A Hijdra, P J Koudstaal, J van Gijn
AbstractWe developed and tested a simple three-point scale for grading white matterlesions in anterior and posterior regionsof the brain. Twenty four CT scans and24 MRI scans were separately judged by11 and five observers, respectively, onthe presence and severity of whitematter lesions. The observers wereradiologists and neurologists. For CTscans, these periventricular changeswere graded according to their extent asabsent, or partly involving the whitematter, or extending up to the sub-cortical region. The MRI lesions weregraded as no lesion or only a single one,multiple focal lesions, and multipleconfluent lesions. The pairwiseagreements of all possible combinationsof observers for each scan were cor-rected for chance (kappa statistics;maximal agreement 1-0). The weightedkappa value, for anterior and posteriorregions combined, was 0-63 for CT scans,and 078 for MRI scans. This three-pointscale for two separate regions seemssuitable as a basis for cross-sectional orlongitudinal studies of large series ofpatients.
Department ofNeurology, UniversityHospital, UtrechtJ C van SwietenJ van GijnDepartment ofNeurology, AcademicMedical Centre,AmsterdamA HijdraDepartment ofNeurology, UniversityHospital Dijkzigt,Rotterdam, TheNetherlandsP J KoudstaalCorrespondence to:Dr van Swieten,Department of Neurology,University Hospital,Heidelberglaan 100,3584 CX Utrecht,The Netherlands.
Received 31 May 1989and in revised form9 February 1990.Accepted 3 April 1990
Periventricular leukoencephalopathy is a more
or less symmetrically diminished density ofthe white matter on CT scans of elderlyindividuals.`' The frontal and the parieto-occipital white matter are most often affected,although not always to equal degrees,6frequently in association with ventricularenlargement. Magnetic resonance imaging(MRI) has proved more sensitive in detectingwhite matter lesions than CT.7' Thehypodense lesions on CT correspond withareas of increased signal intensity in T2weighted MRI. They are most often foundin patients with stroke, hypertension or
dementia.'s-6 Neuropathological studies haveshown that these lesions on CT or MRIcorrespond with demyelination, astrocyticgliosis, arteriolosclerosis, or dilated peri-vascular spaces, and are often associated withlacunar infarcts.17 18
Further studies of the incidence, causes andprognosis of periventricular white matterlesions are impeded by the lack of reliablecriteria for the presence and severity of theselesions. The presence of white matterlucencies on CT has in some cases beenquantified in Hounsfield units,2" but in most
previous studies a subjective assessment wasmade of the extent or degree of attenuation ofthese lesions at one site, compared with thesurrounding brain.'01217 19 20 Other CT studieshave distinguished different types accordingto the anatomical distribution of white matterlesions, but did not take account of theseverity.' 3
In MRI studies, a variety of scales has beenused for measuring the severity of whitematter lesions. In most cases two categories oflesions were distinguished that often occurtogether, that is, periventricular lesions andfocal lesions. 1416 21-26 Sometimes these lesionshave been separately graded2224 and elsewherethey were taken together.212325 The extent ofthe periventricular lesions in the white mattermay range from narrow rims around thefrontal horns to thick bands extending deep inthe white matter, and focal lesions may besingle, multiple or confluent.Whether these white matter lesions imply
functional impairment is not entirely clear.Studies about cognitive functions in patientswith white matter lesions on CT or MRI havegiven conflicting results.9 20 228 Although thismay have been caused by differences inpatient selection, another and perhaps neglec-ted factor may be the severity of the lesions inthe frontal or parieto-occipital white matter.In future studies in which periventricularleukoencephalopathy is related to function orto future events, white matter lesions on CTor MRI should be graded according to boththe anatomical pattern and the severity.An ideal rating scale for white matter
lesions on CT or MRI should meet the foll-owing requirements. First, it should includethe anatomical distribution as well as theseverity of white matter lesions, with cleardefinitions for the different categories.Secondly, the scale should be simple. Finally,the reliability of the scale should be assessedin an inter-observer study. One such studyhas been reported, but without mention of thetype of scale or the actual measure ofagreement.29 In this study, we have developeda scale for CT and another for MRI, consist-ing of similar categories for anterior andposterior regions, but with different defini-tions for the kind of lesions on CT or MRI.We determined the extent of agreementamong different observers by means of kappastatistics, which accounts for chanceagreement.
MethodsA method for systematic evaluation of the
1080
on May 16, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.12.1080 on 1 D
ecember 1990. D
ownloaded from

Grading white matter lesions on CT and MRI: a simple scale
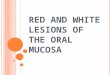
Figure I The severity ofwhite matter lesions isgraded as 0, 1 or 2for theanterior white matter inthe slice through thechoroid plexus (left) andthe slice through the cellamedia (centre), andforthe posterior white matterin the slice through thecella media (middle) andthe slice through thecentrum semiovale (right),for instance, Ao P, or A2P2.
white matter lesions on CT and MRI wasgradually developed in small and repeatedinterobserver studies; the results with a moresensitive scale (four grades for differentregions) have not been included in this report,because of considerable disagreement. Wefinally distinguished two regions that are mostfrequently affected: one region around theanterior horns of the lateral ventricles, andanother consisting of the white matter aroundthe posterior part of the cella media and theposterior part of the centrum semiovale. Whitematter lesions in these two regions of interestwere separately evaluated on three subsequentCT or MRI slices: one through the choroidplexus of the posterior horns, one through thecella media, and one through the centrumsemiovale (fig 1). These three levels can beconsidered representative of the total whitematter, since they include the largest cross-sectional areas.
CT scan assessmentCT scans of 24 patients were obtained from thefile of the Dutch TIA-trial.'0 Patients areeligible for this trial when they have suffered atransient ischaemic attack or a non-disablingstroke (Rankin-scale grade 3 or less).3' CTscans were selected according to the presenceand degree of white matter lucencies, withapproximately equal proportions betweennormal white matter, slight involvement andsevere involvement in one or more regions. Toavoid overrepresentation ofgood quality scans,second generation scans of eight patients wereincluded, together with third generation scansin sixteen patients. Hard-copy images had beenmade, at a window width of 75 Hounsfield in 11patients, and of 100 units in 13 patients. Alacunar infarct, defined as a sharply marginatedlow density lesion without mass effect, andwithin a recognised arterial territory, waspresent in nine scans, and an infarct of thecortical type in three.Leukoencephalopathy on CT was distingui-
shed from infarction by its ill-defined borders.The severity of hypodensity, if present, wasexpressed in one of two degrees for each of thetwo regions. In grade 1 the abnormality wasrestricted to the region adjoining the ventricles,in grade 2 the increased hypodensity involvedthe entire region from lateral ventricle to the
cortex. Eleven observers, six neurologists andfive radiologists, were instructed and sub-sequently asked to grade any abnormality ofthewhite matter for each of the two regions incomplete sets of all 24 CT scans. The degree ofradiolucency was not explicitly graded. Whenasymmetric hypodensities were found, themost severely affected side was taken intoaccount. Since the two regions almost make upthe total white matter, the grades given to theregions can be added together, to give anoverall value between 0 and 4.
MRI assessmentTwenty four MRIs, obtained from a study ofelderly hypertensive patients, were selected torepresent an even distribution according to theseverity of white matter lesions, judged byincreased signal-intensity on T2-weightedimages. All MRI were performed with a 1 5 TPhilips gyroscan. Multiple slice spin-echo (SE)sequences were performed with a repetitiontime (TR) of 2000 ms and an echo time (TE) of50 and 100 ms, producing a T2-weightedimage. A heavily Ti -weighted image wasproduced with a TR of 1500 ms, an inversiontime (TI) of 575 ms, and a TE of 30 ms. Fiveobservers were asked to grade the severity ofthe white matter lesions in the same slices as forCT assessment, again separately for theanterior and posterior region, in one of threecategories. Focal lesions were judged presentwhen the diameter was 1 mm or more on thehard copy images (true dimensions approxi-mately 2 mm). The severity of the lesions wasgraded according to their number and con-figuration: grade 0, no lesion or only a singleone; grade 1, multiple focal lesions; grade 2,multiple confluent lesions scattered through-out the white matter. Since periventricularlesions nearly always accompanied focal orconfluent lesions, we did not grade theseseparately. The grades for the two regions wereconsidered separately as well as added together.
Statistical analysisThe degree of agreement among manyobservers was expressed by means of kappastatistics." Kappa values were calculated foreach CT or MRI, and for all possible combina-tions of the 11 and five observers, respec-tively.3 For the grades with both regions added
1081
on May 16, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.12.1080 on 1 D
ecember 1990. D
ownloaded from

van Swieten, Hiidra, Koudstaal. van Gijn
...
*u 1)1 .'N. .;!i. hr
'..
together, kappa values were corrected by takingthe degree of disagreement into account(weighted kappa).34 In doing so, we attributedtwice as much weight to a difference of twogrades as to a difference ofone grade, and threetimes as much weight to a difference of threegrades (linear disagreement weights). Kappavalues range between 0 (only chanceagreement) and 1 (perfect agreement).
ResultsCT assessmentWith 11 observers, each set of scans of onepatient gives rise to 55 pairwise comparisons,and with 24 scans the total number ofcomparisons is 1320. The kappa value for theanterior region alone was 0 51, and for theposterior region 0 57. When the grades of bothregions were added together, the overall kappavalue was 0-42, with a weighted kappa of 0-63(table). One region was considered more affec-ted than the other in 104 of 264 assessments.On separate analysis of CT images made
with the third generation scanners, the weigh-ted kappa values were similar to those of thetotal series. In a further study with the same 24CT scans, five of 11 observers were explicitlyinstructed to give separate grades for theanatomical extent of hypodensity and for thedegree of radiolucency of the white matter;subsequently, they were asked to combine bothfeatures by attributing one grade. The interob-server agreement for the degree of radiolucency
Table Kappa values for the severity of white matterlesions in anterior and posterior regions on CT and MRI
CT Kappa (K.) 95% confidence limits
Anterior region 0-51 0-47-055Posterior region 0 57 0-53-0 60Both regions together 0-42 (0-63) 0 39-0-46 (0-61-066)
MRIAnterior region 0-68 060-076Posterior region 0-65 0-57-073Both regions together 0-60 (0 78) 0-52-067 (0-73-0-83)
was equal to that of the anatomical extent, andthe combination of these separate features didnot lead to better agreement than in the firstround.
MRI assessmentWith five observers and 24 scans, the numberof comparisons was 240. Perfect agreement forwhite matter lesions existed in 190 of these forthe anterior region, and in 183 for the posteriorregion. The kappa value for the anterior regionwas 0-68, and for the posterior region 065.When the two grades were added together, theoverall kappa value was 0 60, and the weightedkappa 0-78. One region was graded as moreseverely affected than the other in 34 of 120assessments.
DiscussionThe reliability in measuring the severity ofwhite matter lesions on CT and MRI hasreceived little attention so far. An unequivocalgrading scale is necessary for quantifying thisabnormality, particularly in clinical andradiological studies involving large numbers ofsubjects, with cross-sectional or longitudinaldesign. The kappa values for assessments of thetwo regions with MRI (0 68 and 0 65) werehigher than those for CT assessments of thesame regions (0-51 and 0 57). The weightedagreements with the CT and MRI scale were0-63 and 0-78, respectively, and these valuescan be considered good."That inter-observer agreement is lower for
CT than for MRI may be mainly caused by theill-defined margins ofhypodensity on CT scan,which often makes the differences with normalwhite matter small. Another complicating fac-tor with CT are partial volume effects withcerebrospinal fluid or grey matter.36 Finally,lacunar infarcts often occurred in our series, asin other reports,37 and these are sometimesdifficult to distinguish from diffuse leuko-encephalopathy, if the lacunes are only faintlyseen on CT.
1082
:. .1 ...
on May 16, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.12.1080 on 1 D
ecember 1990. D
ownloaded from

Grading white matter lesions on CT and MRI: a simple scale
The severity of white matter lesions on MRIshowed considerable variation. The greaterimage contrast of these lesions with thesurrounding normal brain allows more reliableassessment. Moreover, exact measurement ofthe size of these lesions is possible. In tworecent small series of patients,24 26 the diameterof these lesions has been measured and addedtogether. The three standardised axial levelsfor assessment in this study also offer theopportunity of measuring the cross-sectionalareas of MRI lesions, and of detecting changesin longitudinal studies.We found that the lesions in anterior or
posterior white matter were not equally severein about a third of the CTs and MRIs in ourseries. Also, the involvement of certain deepsubregions, such as the internal or externalcapsule, is a conspicious feature in some cases.In two CT studies, the extent of abnormallucencies were assessed in several regions,resulting in a very sensitive summed score.7 12In one MRI study, the size of the lesions hasbeen measured in four regions and addedtogether.26 However, this method results ingreater interobserver disagreement, and itmakes the scale impractical for use in largeseries of patients. It is unknown whether thedistribution of lesions between anterior andposterior regions is only a matter of chance orwhether it has pathogenetic significance. Inview of the conflicting results about the exis-tence of neuropsychological impairment inpatients with white matter lesions, the distinc-tion in anterior and posterior regions may behelpful.
In conclusion, the use of the three-pointscale for white matter lesions on CT and MRIis suitable for analysing large series of patients.The three-point rating scale for MRI lesions intwo regions has already been fruitfully appliedin a recently completed study of elderly hyper-tensive patients.
We gratefully acknowledge the cooperation of neurologists andradiologists from the University Hospital, Utrecht, and ofradiologists from the Academic Medical Centre, Amsterdam,from the Dijkzigt Hospital and St Franciscus Hospital,Rotterdam.
1 Valentine AR, Moseley IF, Kendall BE. White matterabnormality in cerebral atrophy: clinicoradiologicalcorrelations. J Neurol Neurosurg Psychiatry 1980;43:139-42.
2 Zeumer H, Schonsky B, Sturm KW. Predominant whitematter involvement in subcortical arteriosclerotic ence-phalopathy (Binswanger disease). JComput Assist Tomogr1980;1 :39-48.
3 Goto K, Ishii N, Fukasawa H. Diffuse white matter diseasein geriatric population. Radiology 1981;141:687-95.
4 Brott Th, Mouradin M, Uhtman B. Dementia, ventricularenlargement, and hypertension associated with periven-tricular hypodensity by computed tomography. AnnNeurol 1986;20:129-30.
5 Loizou LA, Kendall BE, Marshall J. Subcortical arterio-sclerotic encephalopathy: clinical and radiological inves-tigation. JNeurol Neurosurg Psychiatry 1981;44:294-304.
6 Derix MMA, Hijdra A, Verbeeten BWJ. Mental changes insubcortical arteriosclerotic encephalopathy. Clin NeurolNeurosurg 1987;89:71-78.
7 Erkinjuntti T, Ketonen L, Sulkava R, Sipponen J,Vuorialho M, Iivianen M. Do white matter changes onMRI and CT differentiate vascular dementia from Alz-heimer's disease? J Neurol Neurosurg Psychiatry 1987;50:37-42.
8 Johnson KA, Davis KR, Buonanno FS, Brady ThJ, Rosen J,
Growdon JH. Comparison of magnetic resonance androentgen ray computed tomography in dementia. ArchNeurol 1987;44:1075-80.
9 George AE, de Leon MJ, Kalnin A, Rosner L, Goodgold A,Chase N. Leukoencephalopathy in normal and pathologicaging: 2. MRI of brain lucencies. AJNR 1986;7:567-70.
10 George AE, de Leon MJ, Gentes CI, et al. Leukoence-phalopathy in normal and pathological aging 1. CT ofbrain lucencies. AJNR 1986;7:561-6.
11 Steingart A, Hachinski VC, Lau C, et al. Cognitive andneurologic findings in demented patients with diffusewhite matter lucencies on computed tomographic scan
(Leuko-araiosis). Arch Neurol 1987;44:36-9.12 Rezek DL, Morris JC, Fullnig KH, Gado MH. Periven-
tricular white matter lucencies in senile dementia ofAlzheimer type and in normal aging. Neurology1987;37: 1365-8.
13 Inzitari D, Diaz F, Fox A, et al. Vascular risk factors andleuko-araiosis. Arch Neurol 1987;44:42-7.
14 Awad IA, Spetzler RF, Hodak JA, Awad CA, Carey R.Incidental subcortical lesions identified on magneticresonance imaging in the elderly. 1. Correlation with ageand cerebrovascular risk factors. Stroke 1986;17:1084-9.
15 Gerard G, Weisberg LA. MRI periventricular lesions inadults. Neurology 1986;36:998-1001.
16 Lechner H, Schmidt R, Bertha G, Justich E, Offenbacher H,Schneider G. Nuclear magnetic resonance image whitematter lesions and risk factors for stroke in normalindividuals. Stroke 1988;19:263-5.
17 Lotz PR, Ballinger WE, Quisling RG. Subcortical arterio-sclerotic encephalopathy: CT spectrum and correlation.AJNR 1986;7:817-22.
18 Awad IA, Johnson PC, Spetzler RF. Incidental subcorticallesions on magnetic resonance imaging in the elderly. 2.Postmortem pathological correlations. Stroke 1986;17:1090-7.
19 Aharon-Peretz J, Cummings JL, Hill MA. Vascular demen-tia and dementia of the Alzheimer type. Cognition,ventricular size, and leuko-araiosis. Arch Neurol 1988;5:719-21.
20 Gupta SR, Naheedy MH, Young JC, Ghobrial M, RubinoFA, Hindo W. Periventricular white matter changes anddementia. Clinical, neuropsychological, radiological andpathological correlation. Arch Neurol 1988;45:637-41.
21 Kinkel WQR, Jacobs L, Polachini I, Bates V, Heffner RR.Subcortical arteriosclerotic encephalopathy (Binswan-ger's disease). Arch Neurol 1985;42:951-9.
22 Kertesz A, Black SE, Tokar G, Benke Th, Carr T, Nichol-son L. Periventricular and subcortical hyperintensities onmagnetic resonance imaging "Rims, caps and unidentifiedbright objects". Arch Neurol 1988;45:404-8.
23 Hershey LA, Modic MT, Greenough PG, Jaffe DF. Mag-netic resonance imaging in vascular dementia. Neurology1987;37:29-35.
24 Rao SM, Mittenberg W, Bernardin L, Haughton V, Leo GJ.Neuropsychological test findings in subjects with leuko-araiosis. Arch Neurol 1989;46:40-4.
25 Hendrie HC, Farlow MR, Guerriero Austrom M, EdwardsMK, Williams MA. Foci of increased T2 signal intensityon brain scans of healthy elderly subjects. AJNR 1989;10:703-7.
26 Hunt AL, Orrison WW, Yeo RA, et al. Clinical significanceof MRI white matter lesions in the elderly. Neurology1989;39: 1470-4.
27 Steingart A, Hachinski V, Lau C, Fox AJ, et al. Cognitiveand neurologic findings in subjects with diffuse whitematter lucencies on computed tomographic scan (leuko-araiosis). Arch Neurol 1987;44:32-5.
28 Lee A, Yu YL, Tsoi M, Woo E, Chang CM. Subcorticalarteriosclerotic encephalopathy-a controlled psycho-metric study. Clin Neurol Neurosurg 1989;91:235-40.
29 Lee D, Fox A, Vinuela F, Pelz D, Lau C, Donald A, Me:skeyH. Interobserver variation in computed tomography ofthe brain. Arch Neurol 1987;44:30-1.
30 The Dutch TIA study group. The Dutch TIA trial: theprotective effect of low dose aspirin and atenolol inpatients with transient ischemic attacks or non-disablingstroke. Stroke 1988;19:512-17.
31 van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJA,van Gijn J. Interobserver agreement for the assessment ofhandicap in stroke patients. Stroke 1988;19:604-7.
32 Longstreth WT, Koepsell TD, van Belle G. Clinicalneuroepidemiology 1. diagnosis. Arch Neurol 1987;44:1091-499.
33 Schouten HJA. Measuring pairwise interobserveragreement when all subjects are judged by the sameobservers. Statist Neerland 1982;36:45-61.
34 Cohen J. Weighted kappa: nominal scale agreement withprovision for scaled disagreement or partial credit. PsycholBull 1976;70:213-20.
35 Landis JR, Koch GG. The measurement of observeragreement for categorical data. Biometrics 1977;33:159-74.
36 Schwartz M, Creasey H, Grady CL, DeLeo JM, Frederick-son HA, Cutler NR, Rapoport SI. Computed tomo-graphic analysis of brain morphometrics in 30 healthymen, aged 21 to 81 years. Ann Neurol 1985;17:146-57.
37 Bogousslavsky J, Regli F, Uske A. Leukoencephalopathy inpatients with ischemic stroke. Stroke 1987;18:896-9.
1083
on May 16, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.12.1080 on 1 D
ecember 1990. D
ownloaded from