Embed Size (px)
Citation preview

SQUAMOUS CELL CARCINOMAIt is the eighth most common cancer in males and
the fifteenth most common in femalesApproximately 94% of all oral malignancies are squamous cell carcinomaAs with so many carcinomas, the risk of intraoral cancer increases with increasing age, especially for males

عوامل خارجیتنباکوالکل
سیفیلیسنورخورشیدویروس ها
عوامل داخلیسوءتغذیهکم خونی فقرآهن
کمبودایمنیسندرم های
ژنتیکی
سرطان اتیولوژیدهان


CLINICAL FEATURES
most often older men who have been aware of an alteration in anoral cancer site for 4 to 8 months before seeking professional helpOral squamous cell carcinoma has a varied clinical presentation, including:♦ Exophytic (mass-forming; fungating, papillary,verruciform)♦ Endophytic (invasive, burrowing, ulcerated)♦ Leukoplakic (white patch)♦ Erythroplakic (red patch)♦ Erythroleukoplakic (combined red-and-whitepatch)

Destruction of underlying bone, when present, may be painful or completely painless, and it appears on radiographs as a "moth-eaten" radiolucency with ill-defined or ragged margins (an appearance similar to osteomyelitis)
Lip vermilion carcinomaIntraoral carcinomaCarcinoma of the tongueCarcinoma of the oral floorGingival and alveolar carcinomasOropharyngeal carcinoma

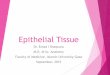
Squamous cell carcinoma. An exophytic lesion of the posterior lateral tongue demonstrates surface nodularity and
minimal surface keratin production. It is painless and indurated

Squamous cell carcinoma An exophytic buccal
lesion shows a roughened and irregular surface with areas of
erythemaadmixed with small areas of white
keratosis. Surface ulcerationis eviden

Squamous cell carcinoma .A posterior lateral
tongue lesion is exophytic but also demonstrates extensive surfaceulceration and nodularity. Such
lesions are sometimesreferred to as "fungating" carcinomas

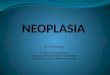
Squamous cell carcinoma An ulcerated or
endophytic lesion of the hard palate demonstrates rolled borders
and a necrotic ulcer bed. This cancer was painless, although it had
partially destroyed underlying palatal bone

Squamous cell carcinomaBone involvement is
characterized by an irregular, "moth-eaten" radiolucency with
ragged margins—an appearance similar to that of osteomyelitis

Squamous cell carcinomaSmall, crusted ulcer of
the lower lip vermilion

Squamous cell carcinomaUlcerated mass of
the lower lip vermilion

Squamous cell carcinomaPatient neglect can
result in extensive involvement, even in a readily visible site such
as the lip vermilion. This ulcerating lesion of the lower lip had
been present for more than 1 year before diagnosis

Squamous cell carcinomaUlcerated lesion with
surrounding leukoplakia on the posterior lateral and ventral
tongue.

Squamous cell carcinomaUlcerated, exophytic
mass of the posterior lateral border of the tongue

Squamous cell carcinomaOral floor lesions are
typically ulcerated or present as an admixed red-and-white,
pebbled-surface change

Squamous cell carcinomaAn exophytic lesion with
an irregular and pebbled surface has a linear indentation along its
facial aspect resulting from pressure from the patient's lower
denture. Underlying alveolar bone was extensively destroyed

Squamous cell carcinoma Large fungating
tumor of the maxillary alveolar ridge and hard palate

Squamous cell carcinomaAn innocuous pebbledsurface
change of the attached and marginal gingiva was interpreted
as an inflammatory change until multifocal white keratoses
occurred.

Squamous cell carcinoma. Large, ulcerated
lesion of the right lateral soft palate

Metastasis
The metastatic spread of oral squamous cell carcinoma is largely through the lymphatics to the ipsilateral cervical lymph nodesA cervical lymph node that contains a metastatic deposit of carcinoma is usually firm to stony hard, nontender, and enlargedThe most common sites of distant metastasis are the lungs, liver, and bones

Staging
Tumor size and the extent of metastatic spread of oralsquamous cell carcinoma are the best indicators of thepatient's prognosisQuantifying these clinical parameters is called staging the diseaseTNM

HISTOPATHOLOGIC FEATURESSquamous cell carcinoma arises from dysplastic surfaceepithelium and is characterized histopathologically by invasive islands and cords of malignant squamous epithelial cellsInvasion is represented by irregular extension of lesional epithelium through the basement membrane and into subepithelial connective tissueIndividual squamous cells and sheets or islands of cells are seen to be thriving as independent entities within the connective tissues, without attachment to the surface epithelium


Histopathologic evaluation of the degree to which these tumors resemble their parent tissue (squamous epithelium) and produce their normal product (keratin) is called gradingLesions are graded on a three-point (grades Ito III) or a four-point (grades Ito IV) scale
To a certain extent, the grading of squamous cell carcinomais a subjective process, depending on the area of the tumor sampled and the individual pathologist's criteriafor evaluation. Moreover, clinical staging seems to correlate much better with the prognosis than microscopic grading

Treatmt and prognosisSurgical exisionRadiotherapychemotherapy

VERRUCOUS CARCINOMA (SNUFF DIPPER'SCANCER; ACKERMAN'S TUMOR)
Verrucous carcinoma is a low-grade variant of oral squamous cell carcinomaReported first by Ackerman in 1948 as a spit tobacco-associated malignancyTypically in the area where the tobacco is habitually Placed
Clinical Features:men older than 55 years of agemandibular vestibule, the buccal mucosa, and the hard PalateThe lesion appears as a diffuse, well-demarcated,painless, thick plaque with papillary or verruciform surfaceLesions are typically white but also may appear erythematous or pinkVerrucous carcinoma is a lesion that may develop from the highriskprecancer, proliferative verrucous leukoplakia (PVL)



HISTOPATHOLOGIC FEATURES
wide and elongated rete ridges that appear to "push" into the underlying connective tissueParakeratin typically fills the numerous clefts or crypts (parakeratin plugs) between the surface projectionsThe lesional epithelial cells generally show a normal maturation pattern with no significant degree of cellular atypiaThere is frequently an intense infiltrate of chronic inflammatory cells in the subjacent connectiveTissue aAdequate sampling also is important because as many as 20% of these lesions have a routine squamous cell carcinoma developing concurrently within the verrucous carcinoma

TREATMENT AND PROGNOSIS
Because metastasis is an extremely rare event in verrucouscarcinoma, the treatment of choice is surgicalExcision without radical neck dissection

با تشکر از توجه شما







![Pancreatic Cytopathology Cystic Lesions Cytol… · Cystic Lesions Cystic Lesions Of The Pancreas [Practical Issues] ... 1-2% of all pancreatic tumors LMP epithelial tumor of uncertain](https://img.dokumen.tips/doc/110x75/5f6d9c61a7374f61f46d815c/pancreatic-cytopathology-cystic-lesions-cytol-cystic-lesions-cystic-lesions-of.jpg)