Embed Size (px)
Citation preview

2/23/20
1
Stacy Goergen
Head, Obstetric MRI Program and Obstetric ImagingMonash Imaging, Monash Health
Professor, Medical Imaging, Monash University School of Clinical SciencesMelbourne, Australia
From Images to Genes: the Role of
Prenatal MRI in Fetal PhenotypingTOP
Request?review
committee
SecondOpinion
T2 Ultrasound
Cell FreeDNA
?TOP
MicroarrayTertiary
Ultrasound
T1 Ultrasound
Multi -disciplinary
Team
Fetal Therapy
Follow up
T2 Ultrasound
Chromosome Testing
Diagnosis, prognostication, recurrence prediction for fetal CNS anomalies is multidisciplinary in
2019
Information Obtained at
Initial Screening
Additional Information Obtained at
FDU
Counseling and
Management Decision
MRI
Image: Courtesy Dr. Mark Teoh
2014 ISUOG Survey of 60 international fetal diagnosis / MFM centres
When would you perform fetal MRI ?
Fetal MRI for Suspected CNS abnormality
Funded by Medicare Australia from 1 May 2019
Apparently isolated VM• Ganglionic eminences• Sulcation / opercularisation• Subependymal heterotpia• Polymicrogyria
Absent septal leaflets• Perforation vs failed formation
The small cerebellum / posterior fossa “cyst”• Brainstem and cerebellar size and shape
Accurate Fetal Phenotyping with MR:Diagnosis, Prognosis, Recurrence
Isolated severe ventriculomegaly 36/40 neurosonogram
PVNH due to X linked Filamin A mutation

2/23/20
2
CLICK TO EDIT MASTER TITLE STYLEIsolated bilateral >15mm VM at 32 weeks
neurosonogramPVNH – Filamin A mutation
Filamin A mutation – Mother of affected female child
23.5/40 – Posterior fossa cyst? Abn cerebellum?
US: Mega cisterna magna or Posterior fossa arachnoid cyst
cyst?Filamin A mutation

2/23/20
3
• Diagnosis: Filamin A (FLNA) genetic variant
• Prognosis: Epilepsy/ aortic dissection / intracranial aneurysms / cardiac valvular dysplasia – monitoring and BP control important
• Recurrence: 50% in females50% in utero fatality in males, 50% unaffected
• Other:• Head MRI of mother – 50% denovo mutation, 50% inherited• If mother carrier – risk of same cardiovascular complications as fetus• Preimplantation diagnosis possible
Both pregnancies continued based on change of counselling from “severe VM” and PF abnormality” to specific diagnosis
Severe VM
22+2 G3P0 – 40 y.o. IVF pregnancySevere bilateral ventriculomegaly
?Intraventricular mass - haemorrhage?
22+2w Ultrasound15mm bilateral VM
Reduced TCD, Thin CC – hypogenetic?Thin CC
Normal 23/40 DWI
Enlarged GEunderopercularisation DWI
Lissencephaly – which one?
23/40 MRI
CC too thin – hypogenesisGE too large
Normal 23/40

2/23/20
4
TCD 20mm: – 3SD below mean for 23/40 25/40 Follow upPersistent enlarged GE
No opercularisation
Normal 25 / 40
25/40 Cerebellar biometry still - 3SD
Hypogenesis of CC + cerebellar hypoplasia + lissencephaly
Prenatal Dx = tubulinopathy
TOP – selective genetic testing for tubulin gene variantsDiagnosis – Tubulinopathy due to
c.74G>T (p.Cys25Phe) in exon 2 of TUBA1A gene
Severe VM + callosal hypogenesis + cerebellar hypoplasia• Diagnosis – Tubulinopathy
• Prognosis – severe neurodevelopmental abnormality, seizures
• Recurrence – de novo mutation – likelihood of recurrence very low

2/23/20
5
23yoG1P0
External tertiary neurosonogram 28/40Isolated fetal ventriculomegaly 14 mm
BPD, HC, AC > 99th centile
Mild (12mm) VMCerebral Hemispheres and TCD +6 SD > mean for GA
Source: Kline – Fath, Fetal Imaging, Wolter – Kluwers 2016
Enlarged GE, Abnormal opercularisation
Normal 28 week DWI
Abnormal opercularisationBilateral perisylvian polymicrogyria
Normal 28 / 40
US same day as MRI
Courtesy Dr. Lufee Wong
Postaxial polydactyly

2/23/20
6
Provisional Diagnosis – Megalencephaly, polydactyly, polymicrogyria hydrocephalus (MPPH) syndrome
TOPPathogenic PI3K variant on WES
Ventriculomegaly + Head >99th centileDiagnosis : MPPH
Prognosis: Very poor prognosisSeizuresMajor developmental delay
Recurrence:• De novo somatic mutation in majority – no recurrence• Small risk of germline mutation with N parental phenotype• Preimplantation Dx possible
32yoG2P1
P1 macrosomicNormal 20/40 morphology G2
T3 US for growth assessment @32/40
“Incidental” US findings on T3 growth scan
• EFW 9th centile • HC, AC, FL 13th – 19th centile• 15mm, 11mm atria – otherwise N brain• Echogenic enlarged kidneys – 1 cyst 3mm• Talipes
Abnormal opercularisation @33 weeksFrontal lobes smaller than temporal
àPerisylvian PMG, temporal lobe overgrowth in FGFR mutations (Apert’s, thanatophoric dysplasia)
perisylvian polymicrogyria
Talipes Enlarged kidneys
Perisylvian PMG + cystic kidneys + growth restriction = Zellweger syndrome
2/23/20
7
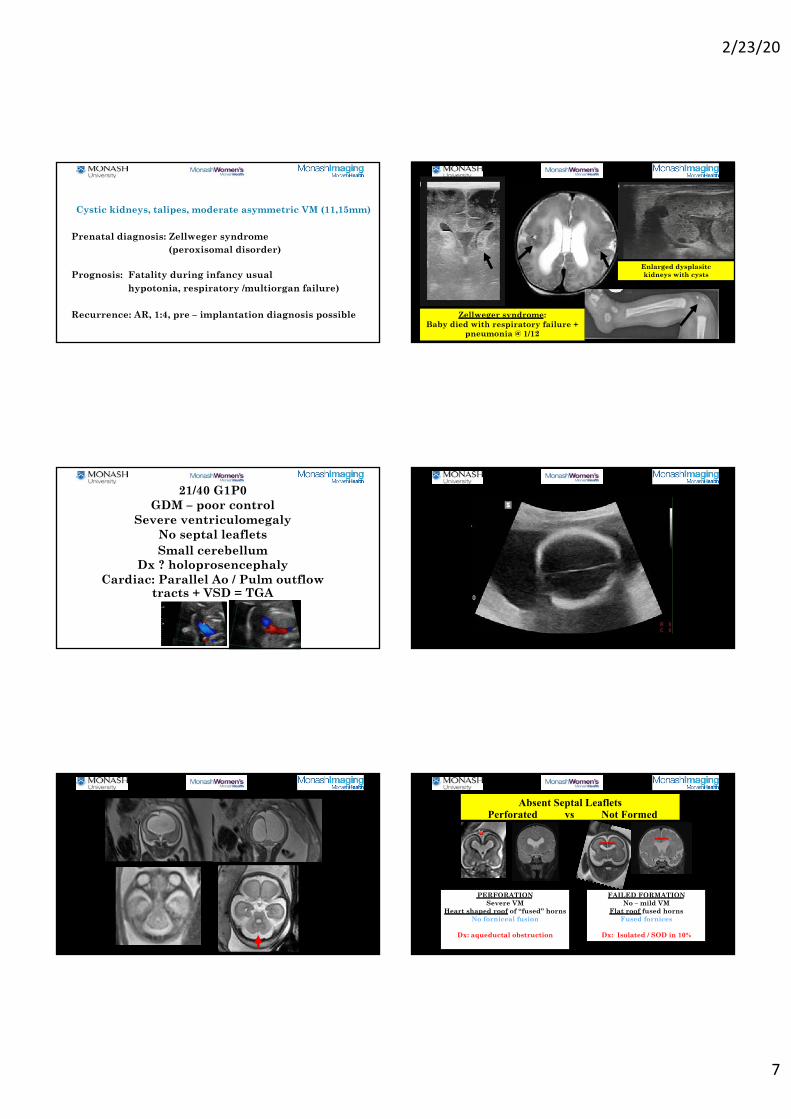
Cystic kidneys, talipes, moderate asymmetric VM (11,15mm)
Prenatal diagnosis: Zellweger syndrome (peroxisomal disorder)
Prognosis: Fatality during infancy usualhypotonia, respiratory /multiorgan failure)
Recurrence: AR, 1:4, pre – implantation diagnosis possible Zellweger syndrome: Baby died with respiratory failure +
pneumonia @ 1/12
Enlarged dysplasitckidneys with cysts
21/40 G1P0GDM – poor control
Severe ventriculomegalyNo septal leaflets Small cerebellum
Dx ? holoprosencephalyCardiac: Parallel Ao / Pulm outflow
tracts + VSD = TGA
Absent Septal LeafletsPerforated vs Not Formed
PERFORATIONSevere VM
Heart shaped roof of “fused” hornsNo forniceal fusion
Dx: aqueductal obstruction
FAILED FORMATIONNo – mild VM
Flat roof fused hornsFused fornices
Dx: Isolated / SOD in 10%
❤

2/23/20
8
9 % of all paediatric cases of aqueductal stenosis have RESRES associations: VACTERL, poorly controlled GDM
Severe VM, no septal leaflets ?HPE, cerebellar hypoplasia
Diagnosis: RES with AS due to VACTERL sequence associated with poor GDM control
Prognosis: Variable and dependent on • severity of AS• presence of Gomez Lopez Hernandez syndrome
Recurrence: Unlikely with good control of GDM
*Tan TY, McGillivray G, Goergen SK, White SM. Prenatal magnetic resonance imaging in Gomez-Lopez-Hernandez syndrome and review of the literature. American Journal of Medical Genetics Part A. 2005 Nov 1;138(4):369-73
US 22/40 – Dandy Walker Malformation? The most likely diagnosis is:
1. Dandy – Walker malformation2. Persistent Blake’s pouch cyst3. PHACE(S)4. Isolated vermian hypoplasia5. Cerebellar hemispheric infarction
Leibowitz et al 2018 Eur J Paediatric Neurol“tilted telephone receiver sign”
PHACE(S) – Neurocutaneous disorderPosterior fossa malformations
Dandy – WalkerUnilateral hemispheric hypoplasia
Haemangioma (facial +/- neck, chest, limbs) – typically not be present antenatally / early newborn
Arterial anomalies (head and neck stenoses, occlusions, moya moya, dural AVF, aneurysms)
Cardiac (aortic coarctation, anomalous great vessels, septal defects, tetralogy of Fallot, dextrocardia)
Eye (1/3 have one or more coloboma, buphthalmos / microphthalmia, glaucoma, morning glory on fundoscopy / many ophthalmoplegia, other clinical eye abnormalities)
Sternal cleft (prenatal US), supraumbilical raphe

2/23/20
9
Leibowitz et al 2018 Eur J Paediatric Neurol –“tilted telephone receiver sign” pathognomonic for
PHACE(S) = 11/11 cases
Day 20
Day 4
PHACE syndrome
MR and US working together in fetal neurology can be a marriage made in heaven
• Contemporary diagnosis of fetal cerebral anomalies is multidisciplinary
• Knowledge of obstetric US, paediatricneuroradiology, genetics needs to be integrated
• Close interdisciplinary co-operation and communication are challenging but essential





























