Embed Size (px)
Citation preview
9/20/2013
1
Stephen Pittenger, DVM, DABVP
As shown in the graphic to the right, there is often a trade off: speed vs. flexibility. Although some may type much faster than the write, it is assumed in this model that the doctor is not a proficient typist.
Dictation or transcription is not a usual and standard mode of data entry in veterinary medicine at present, but voice recognition systems are now readily available and do represent an additional choice.
Expert systems involve the use of complex prompting algorithms and are usually set up by the programmer. Although this may speed data entry, you may be forced to practice medicine and document your cases in a style that does not agree with your philosophy.
Template driven records are the most common implementation in veterinary electronic medical records.
There is wide variation in the speed and flexibility here due to the inherent flexibility here due to the inherent simplicity or complexity of the presenting case.
Your template designed for the typical fleabite dermatitis may serve you well in a typical case, but you may compromise a little speed or flexibility when using it for a slightly atypical presentation.
Doctors treat many similar cases each week. These frequent cases not only comprise the bulk of our routine caseload, but they also hold the majority of our errors and omissions.
We are less likely to overlook something when we are treating the “fascinoma”, as we leave no stone unturned in our hunt for knowledge and understanding of new, complex and rare diseases we may encounter.
Since these cases are so rare, it is unlikely we will need this data entry “automated” in the future
The common cases, however, are where we tend to concentrate or i d ff O time and efforts. Once decision trees and templates are created for these common presentations, our data entry speed increases dramatically.

9/20/2013
2
Many cases may be very similar (parallel findings, but new conclusions) and require
l i d t ti t th only minor adaptations to the created template. If this type of case should become very common in presentation, then a modified template could be created and saved for this as well.
As the Venn diagram in the upper right corner of the graphic shows, cases may have very similar entries in have very similar entries in the SOAP format, or they may be quite dissimilar. Templates and protocols provide us with a “pilot’s checklist” for those common problems so that we may be complete, thorough and consistent with each patient.
The Glossary allows us to use a “template” for completion of the record for common findings.

9/20/2013
3

9/20/2013
4

9/20/2013
5
9/20/2013
6
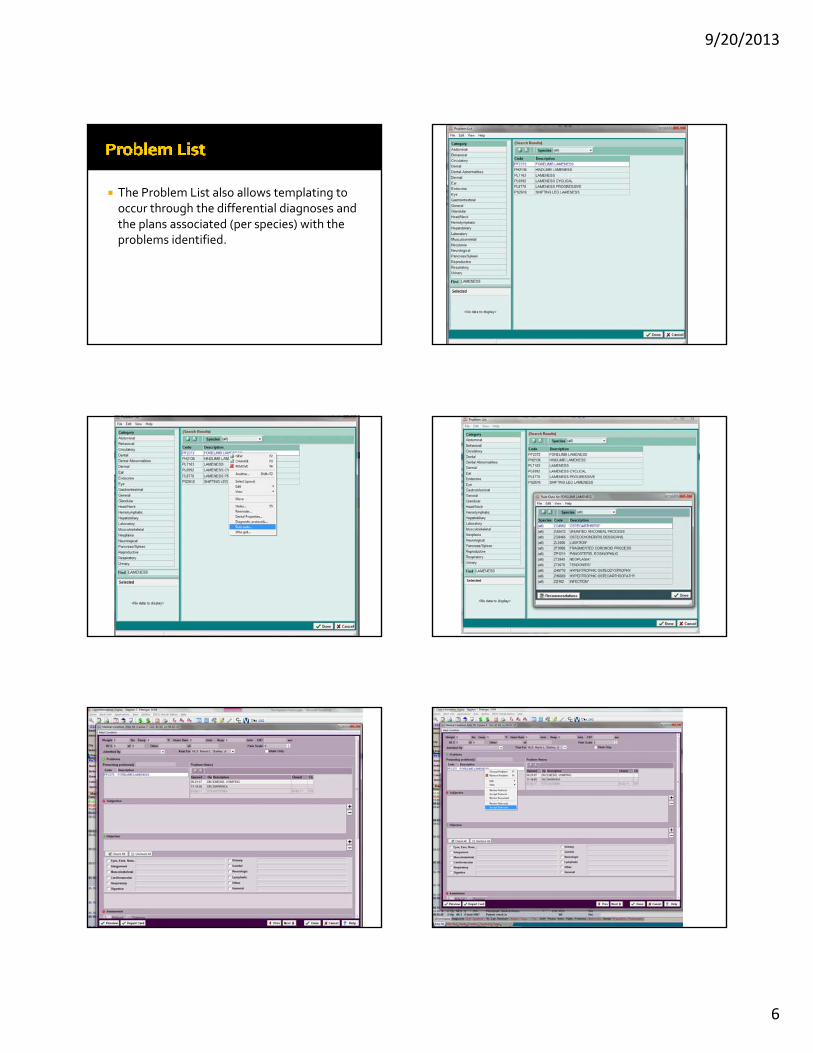
The Problem List also allows templating to occur through the differential diagnoses and the plans associated (per species) with the
fproblems identified.

9/20/2013
7
Forelimb Lameness
Polyuria with associated diagnostic plan JAVMA 2004;225:222‐229 July 15, 2004 Only 9% of the communication time in the exam room is being used to gather historical information.
Closed‐ended questioning is the norm (75%) which may result in decreased accuracy in data gatheringmay result in decreased accuracy in data gathering.
Template for history taking would help to direct more balance and allow for funneling of questions and use of “chunk and check” method of communicating.

9/20/2013
8
Reception takes appointment Client Arrives Check in and print chart Technician Doctor Discharged

9/20/2013
9
How does this differ from the Outpatient setting?
Longer admission
Less inherent structure to visits
More staff interact with the record
More items and services to order/record and invoice
Inpatient admissions occur for 4 basic reasons:
Outpatient admission to hospital
Day admission (extended outpatient)
Scheduled procedures
Emergency admission
Where does everything go? How do I make sure we charge for everything that we do?
d k h ll How do I make sure everything actually gets done?
Medical Records input needs to take care of billing. This avoids double entry (sometimes triple‐entry)
l h Realize that many systems are transaction oriented, with the medical record creation being somewhat secondary. This is okay, we can make this work just fine. Some medical record driven systems are not so good at fee capture . . .

9/20/2013
10
Inventory is inventory (with a few exceptions)
Qty delivered is placed into the record in some way.
The route and the reason for delivery is clear.
The exact medication (including strength) is obvious.
This step must take care of the billing aspect simultaneously.
Here is the way . . . .
Decide on appropriate conventions such as fwhere to record weights (preferably so that
the patient record is updated to the current weight, don’t just squirrel it away somewhere).
Decide on your nursing examination notes versus doctor’s notes.
POMR is the best way to go. Make sure your problem list is being updated along the way and the set is driving the medical record
h dSOAP each day. Diagnosis coding is appropriate when diagnoses are made (may need to adjust for granularity over the length of the visit).
When the chart is printed, it is readable by any other clinician or practice.
When the medical history is searched, you can easily find thingscan easily find things.
When trying to look for particular information, you can find it and view it easily to make future decisions based on past historical findings.
It allows you to go home earlier than before
Labels, Labels, Labels All controlled substances All medications drawn up in advance All lab work
ll d l d fl d All prescriptions drugs (including fluids)
Orders (if not advised verbally or via the Whiteboard)

9/20/2013
11
Needs a cage card Needs an ID band
P

9/20/2013
12
Stephen T. Pittenger, D.V.M.Diplomate, American Board of Veterinary Practitioners
Board Certified in Canine & Feline Practice
M i l 6 H i l f A i lMemorial‐610 Hospital for Animals910 Antoine Drive
Houston, Texas 77024713‐688‐0387





























