Embed Size (px)
Citation preview

Global Mechanical Assessment
Understanding (Assessing) the Nervous System of Athletes
Dr. John Downes
[email protected] [email protected]
© GMA all rights reserved PFLM, Inc.

“The process of discovery is seeing what others have seen before and thinking something new.”
Albert Einstein
Goals for the presentation • Demonstrate global assessment
• Propose ‘What ifs’ and ‘Whys’ • Discuss possible implications: F, C, P
• Leave you interested in further investigation

Components of movement
• Neurology • Soft tissue • Joint movement
• Neuromechanics – the combining of neurology and biomechanics

Components of Neuromechanics
• Feedforward APAs ! 100 ms prior – 50+ms post
• Feedback CPAs ! 75-100 ms post
• Neural Plasticity • Task Specificity
• NM>Neural Control>APAs / CPAs> Muscle Synergies>SAID

General Adaptation Process / Homeostasis
• Specific • Adaptation
to
• Imposed • Demand

‘An intact motor system can adapt via central nervous system control and muscle system activity. The adaptations of the motor system are represented by muscle imbalances’
Craig Liebenson, DC

Presumption(s)?
• An intact nervous system free of pathology or injury performs as a neutral conduit of signals.
• The mechanical indicators of techniques are a direct indicator of change in the nervous system.
• The changes in the horizontal stay changed in the vertical

Where did this come from?
• Clinical observation that seemingly minor injuries were persistent despite quality care by ATCs, DCs, PTs, MDs.
• Noting that asymmetrical dorsiflexion was prevalent in many cases.
• Testing extremities prior to adjusting the spine indicated a tendency towards a pattern of contralateral dysfunction of UE and LE
Process of GMA
• Use the extremities as long levers to challenge the CNS to properly anchor and operate.
• Compare sides via isometric mirror image tasks.
• Observe quality of anchoring and operation. • Determine if reciprocal limb coupling
inefficiency is involved. RLS

Starting Point

Abduction LE / LLNC

Abduction LE / LLNC Oblique

Adduction LE / LLNC Oblique

Adduction UE / LLNC Oblique
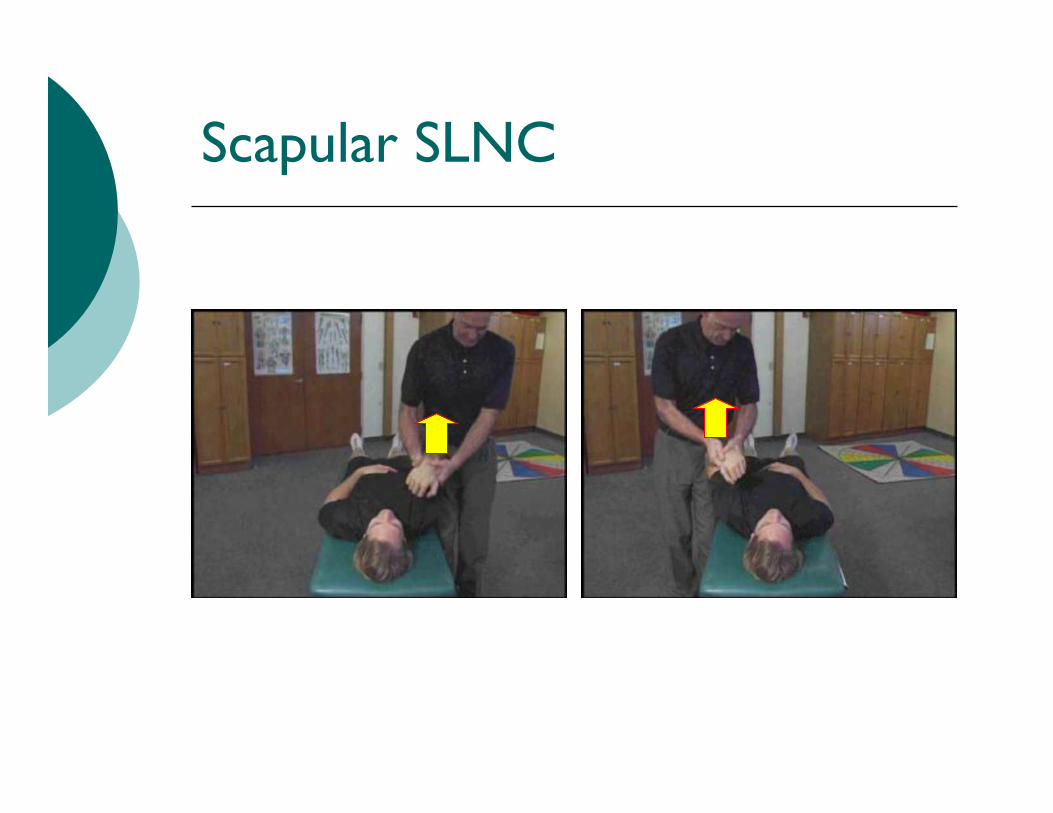
Scapular SLNC

Flexion UE / LLNC

Glossary • PFLM – Performance for Life Method • GMA – Global Mechanical Assessment • GPD – Global Proprioceptive Deficit • RLS – Reciprocal Limb Syndrome • FFA – Feed Forward Activation • FB – Feed Back • APAs – anticipatory postural adjustments • CPAs – compensatory postural adjustments • SAID-specific adaptation to imposed demand

Prevalence of GPD Group / Team Gender Total GPD Number GPD Percentage
Y N Y N
Non-athletes Male 29 23 6 79.3% 20.7% Female 25 22 3 88.0% 12.0% Total 54 45 9 83.3% 16.7%
Athletes Diving Male 7 6 1 85.7% 14.3% Female 19 17 2 89.5% 10.5% Total 26 23 3 88.5% 11.5%
Track & Field Male 14 10 4 71.4% 28.6% Female 9 8 1 88.9% 11.1% Total 23 18 5 78.3% 21.7% Total Male 21 16 5 76.2% 23.8% Female 28 25 3 89.3% 10.7% Total 49 41 8 83.7% 16.3%
Total Subjects Male 50 39 11 78.0% 22.0% Female 53 47 6 88.7% 11.3% Total 103 86 17 83.5% 16.5%

Theory of GPD
• Because it has nothing to do with pain the patient is not aware of its’ presence.
• Because it appears to change the efficiencies within the NMS instantaneously the potential for injury may increase or decrease without perception.
• If you don’t check for it pre and post you don’t really know if a change has occurred.

Reinjury
Functional Instability
Ligamentous injury
Decreased Neuromuscular Control
Proprioceptive Deficit
Structural Instability
Cycle of Injury – Lephart,Fu,Scott
1
2
3
4
Mechanical Model Neuromechanical Model

Potential for Injury/ Reinjury
Functional Instability
Ligamentous injury
Decreased Neuromuscular Control
Proprioceptive Deficit
Structural Instability
Cycle of Injury – Chiropractic / Neuromechanical Model Downes 2002
6
7
4
5
Mechanical Model Neuromechanical Model
Subluxation – Corrupted Signal
1
2
3

Panjabi’s article / implications
• A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction. Manohar M. Panjabi. Eur Spine J (2006) 15: 668–676
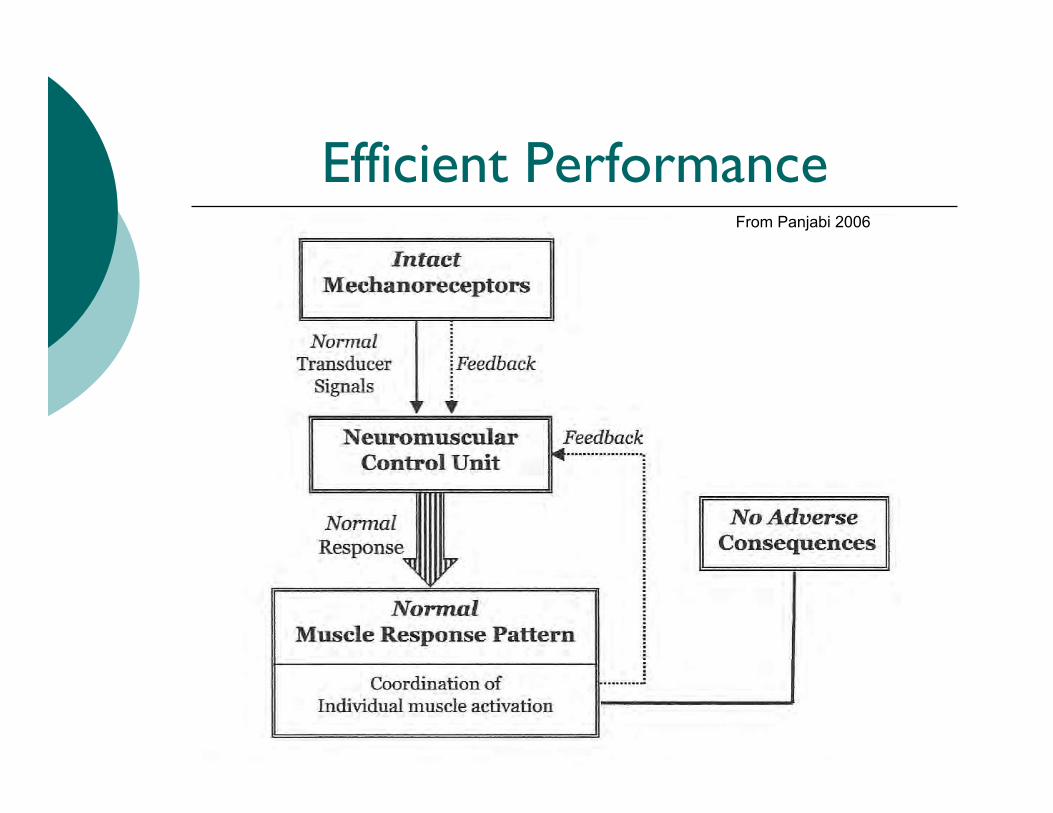
Efficient Performance From Panjabi 2006

Subfailure Injury of Ligaments in the Spine
From Panjabi 2006

Global Application
LigamentousInjury 6
Structural Instability
Potential / RepetitiveInjury
FunctionalInstability
ProprioceptiveDeficit
Decreased NeuromuscularControl
Interference
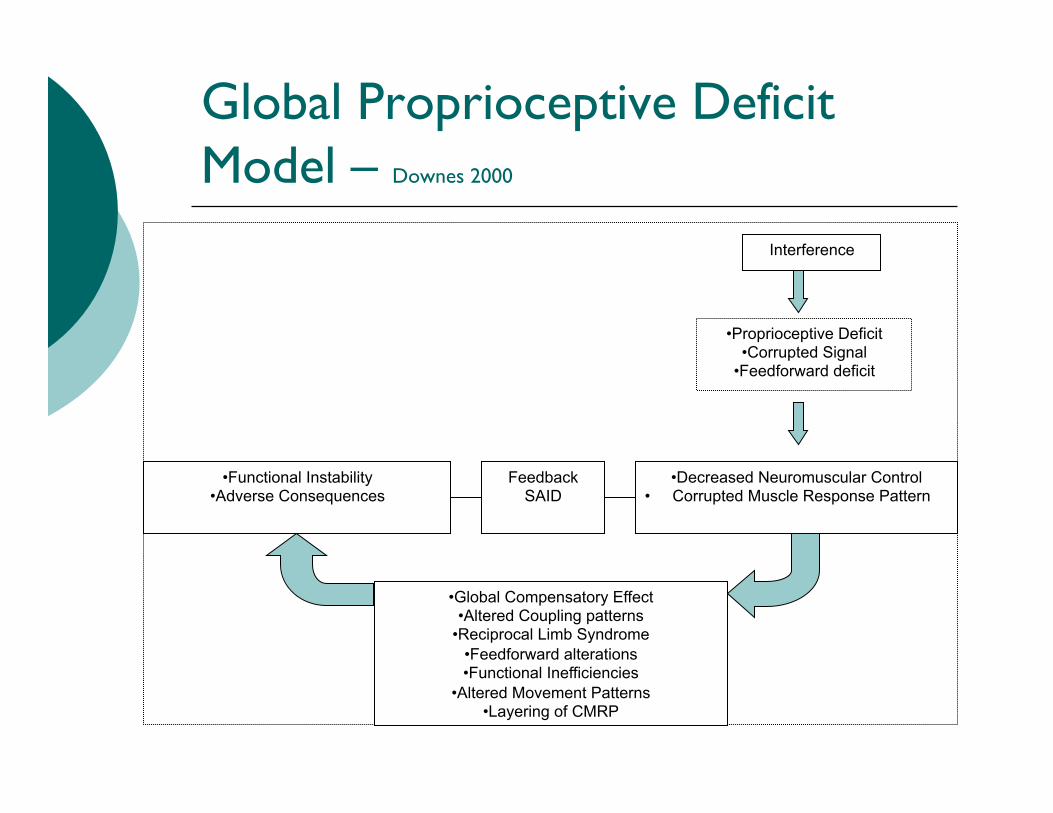
Global Proprioceptive Deficit Model – Downes 2000
Interference • Proprioceptive Deficit
• Corrupted Signal • Feedforward deficit
• Decreased Neuromuscular Control
• Corrupted Muscle Response Pattern • Functional Instability • Adverse Consequences Feedback
SAID
• Global Compensatory Effect • Altered Coupling patterns
• Reciprocal Limb Syndrome • Feedforward alterations • Functional Inefficiencies
• Altered Movement Patterns • Layering of CMRP

Patterns of GPD
• Complaint patterns, right LB / left shoulder – neck
• Lower extremity and contralateral upper extremity
• Layering – starts with all one side, then after adjusting a different pattern is seen, then after adjusting another pattern appears.
• Proper approach to management with a different sequencing of tools.

Implications
KEYWORDS:
How to join PubMed Commons
PubMed Commons home
Acta Psychol (Amst). 2015 Jan;154:10-3. doi: 10.1016/j.actpsy.2014.10.009. Epub 2014 Nov 14.
The role of head position and prior contraction in manual aiming.Sidaway B , Bonenfant D , Jandreau J , Longley A , Osborne K , Anderson D .
AbstractWe sought to determine if the asymmetrical tonic neck reflex influences the accuracy of self-selected arm positioning without vision and to ascertain if such accuracy is influenced by a pre-contraction of the prime movers. Participants reproduced an arm position using their abductors withthe head in midline, rotated towards and away from the arm. Arm movements were made with andwithout a pre-contraction of the abductors. Twenty participants performed eight trials in each of thesix different conditions. Compared to the midline position, participants undershot the referenceposition with the head turned away and overshot the position with the head rotated towards thearm. A pre-contraction caused undershooting regardless of head position. Results suggest thathead position and pre-contraction may have significant and independent effects on arm positioning.
Copyright © 2014 Elsevier B.V. All rights reserved.
Asymmetrical tonic neck reflex; Kohnstamm phenomenon; Positioning; Response bias
PMID: 25461438 DOI: 10.1016/j.actpsy.2014.10.009
[PubMed - indexed for MEDLINE]
PubMed Commons
0 comments
Format: Abstract
1 2 2 2 2 3
Author information
MeSH Terms
LinkOut - more resources
Full text links
PubMed

Head position sense

Practical application
• Elbow position under shot with head rotation towards
• Over shot with head rotation away • Undershot with core activation • What if it was due to CNS corruption? • What if you could demonstrate it and
correct it?

MOI??

Who’s safe? Who’s Injured?

HNPS – post impact injury
Sports Med. 2008;38(2):101-17.
Head and neck position sense.Armstrong B , McNair P, Taylor D.
AbstractTraumatic minor cervical strains are common place in high-impact sports (e.g. tackling) andpremature degenerative changes have been documented in sports people exposed to recurrentimpact trauma (e.g. scrummaging in rugby) or repetitive forces (e.g. Formula 1 racing drivers,jockeys). While proprioceptive exercises have been an integral part of rehabilitation of injuries in thelower limb, they have not featured as prominently in the treatment of cervical injuries. However,head and neck position sense (HNPS) testing and re-training may have relevance in themanagement of minor sports-related neck injuries, and play a role in reducing the incidence ofongoing pain and problems with function. For efficacious programmes to be developed and tested,fundamental principles associated with proprioception in the cervical spine should be considered.Hence, this article highlights the importance of anatomical structures in the cervical spineresponsible for position sense, and how their interaction with the CNS affects our ability to plan andexecute effective purposeful movements. This article includes a review of studies examiningposition sense in subjects with and without pathology and describes the effects of rehabilitationprogrammes that have sought to improve position sense. In respect to the receptors providingproprioceptive information for the CNS, the high densities and complex arrays of spindles found incervical muscles suggest that these receptors play a key role. There is some evidence suggestingthat ensemble encoding of discharge patterns from muscle spindles is relayed to the CNS and thata pattern recognition system is used to establish joint position and movement. Sensory informationfrom neck proprioceptive receptors is processed in tandem with information from the vestibularsystem. There are extensive anatomical connections between neck proprioceptive inputs andvestibular inputs. If positional information from the vestibular system is inaccurate or fails to beappropriately integrated in the CNS, errors in head position may occur, resulting in an inaccuratereference for HNPS, and conversely if neck proprioceptive information is inaccurate, then control ofhead position may be affected. The cerebellum and cortex also play a role in control of headposition, providing feed-forward and modulatory influences depending on the task requirements.Position-matching tasks have been the most popular means of testing position sense in the cervicalspine. These allow the appreciation of absolute, constant and variable errors in positioning and
Format: Abstract
1
Author information
PubMed

Neural Plasticity and Task Specificity
• High-Performance Vision Training Improves Batting Statistics for University of Cincinnati Baseball Players Joseph F. Clark, James K. Ellis, Johnny Bench, Jane Khoury, Pat Graman Published: January 19, 2012 http://dx.doi.org/10.1371/journal.pone.0029109

Head position changes coupling
• Effect of head and limb orientation on trunk muscle activation during abdominal hollowing in chronic low back pain Kevin Parfrey1, Sean GT Gibbons2, Eric J Drinkwater1,3 and David G Behm1*
• Parfrey et al. BMC Musculoskeletal Disorders 2014, 15:52 http://www.biomedcentral.com/1471-2474/15/52

Practical Demo / Application
• After history
• After questions of joint stability are resolved
• Included in pre-treatment assessment
• Utilized as a post-treatment assessment

Exploring the Neuromodulary Effects of the Vertebral Subluxation and Chiropractic Care
• Haavik, Holt, Murphy 2010
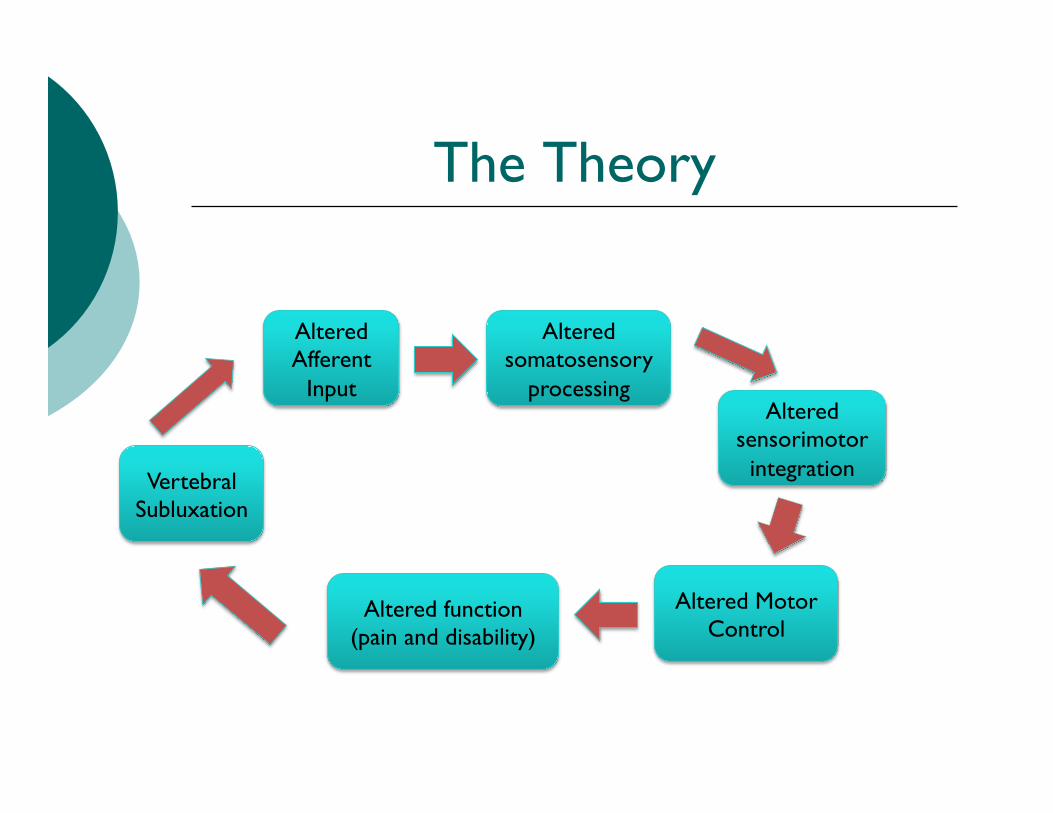
The Theory
Vertebral Subluxation
Altered Afferent
Input
Altered somatosensory
processing Altered
sensorimotor integration
Altered Motor Control
Altered function (pain and disability)

The Adjustment
Appropriate Joint
Movement
Normal Afferent
Input
Appropriate somatosensory
processing Appropriate
sensorimotor integration
Accurate Motor Control Good function
Spinal Adjustment

Cervical spine manipulation alters sensorimotor integration: A somatosensory evoked potential study Haavik Murphy 2006

Cortical responses to adjustment
• N 2O / N 30 excitation • Lasts for 20+ minutes post adjustment • Possible window of opportunity for neural
integration and increased plasticity

2012
The role of spinal manipulation in addressing disordered sensorimotorintegration and altered motor control
Heidi Haavik a,1, Bernadette Murphy b,⇑,2aNew Zealand College of Chiropractic, Auckland, New Zealandb Faculty of Health Sciences, University of Ontario Institute of Technology, 2000 Simcoe St North, Oshawa, Ontario, Canada L1H 7K4
a r t i c l e i n f o
Article history:Available online xxxx
Keywords:ProprioceptionManipulationSpinalCentral nervous systemSensorimotor integrationMotor control
a b s t r a c t
This review provides an overview of some of the growing body of research on the effects of spinal manip-ulation on sensory processing, motor output, functional performance and sensorimotor integration. Itdescribes a body of work using somatosensory evoked potentials (SEPs), transcranial magnetic nervestimulation, and electromyographic techniques to demonstrate neurophysiological changes followingspinal manipulation. This work contributes to the understanding of how an initial episode(s) of backor neck pain may lead to ongoing changes in input from the spine which over time lead to altered sen-sorimotor integration of input from the spine and limbs.
Crown Copyright ! 2012 Published by Elsevier Ltd. All rights reserved.
1. Introduction
Over the past 15 years our research group has conducted a vari-ety of human experiments that have added to our understanding ofthe central neural plastic effects of manual spinal manipulation(Haavik and Murphy, 2011; Haavik-Taylor and Murphy, 2007a,b,2008, 2010c; Haavik-Taylor et al., 2010; Marshall and Murphy,2006). Spinal manipulation is used therapeutically by a numberof health professionals, all of whom have different terminologyfor the ‘‘entity’’ that they manipulate. This ‘‘entity’’ which generallydescribes areas of muscle tightness, tenderness and restrictedmovement may be called a ‘‘vertebral (spinal) lesion’’ by physicalmedicine specialists or physiotherapists, ‘‘somatic dysfunction’’or ‘‘spinal lesion’’ by osteopaths, and ‘‘vertebral subluxation’’ or‘‘spinal fixation’’ by chiropractors (Leach, 1986). For the purposesof this article, the ‘‘manipulable lesion’’ will be referred to as anarea of spinal dysfunction or joint dysfunction. Joint dysfunctionas discussed in the literature ranges from experimentally inducedjoint effusion (Shakespeare et al., 1985), pathological joint diseasesuch as osteoarthritis (O’Connor et al., 1993) as well as the moresubtle functional alterations that are commonly treated by manip-ulative therapists (Suter et al., 1999, 2000).
Based on our research findings we have proposed that areasof spinal dysfunction, represent a state of altered afferent inputwhich may be responsible for ongoing central plastic changes
(Haavik-Taylor et al., 2010; Haavik-Taylor and Murphy, 2007c).Furthermorewe have proposed a potential mechanismwhich couldexplain how high-velocity, low-amplitude spinal manipulation,also known as spinal adjustments, improve function and reducesymptoms. We have proposed that altered afferent feedback froman area of spinal dysfunction alters the afferent ‘‘milieu’’ into whichsubsequent afferent feedback from the spine and limbs is receivedand processed, thus leading to altered sensorimotor integration(SMI) of the afferent input, which is then normalized by high-velocity, low-amplitude manipulation (Haavik-Taylor et al., 2010;Haavik-Taylor and Murphy, 2007c). For a pictorial depiction of thishypothesis, see Fig. 1.
This article will provide an overview of some of the growingbody of research on the effects of spinal manipulation on sensoryprocessing, motor output, functional performance and sensorimo-tor integration. This body of work contributes to our understandingof how an initial episode(s) of back or neck pain may lead to ongo-ing changes in input from the spine which over time lead to alteredsensorimotor integration of input from the spine and limbs.Increasing this understanding may provide a neurophysiologicalexplanation for some of the beneficial clinical effects reported bychiropractors and other manipulative therapists in day to day prac-tice. Chronic musculoskeletal pain affects the lives of millions ofindividuals and places a great burden on health care systems inthe western world. Some of the research discussed in this reviewhas the potential to identify objective neurophysiological markerswhich may be able to predict which patients will respond best tospinal manipulative treatment and/or whether a patient has hada sufficient amount of treatment to normalize neurophysiologicalmarkers of disordered sensorimotor integration. The relationship
1050-6411/$ - see front matter Crown Copyright ! 2012 Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.jelekin.2012.02.012
⇑ Corresponding author. Tel.: +1 (905) 721 8668x2778.E-mail address: [email protected] (B. Murphy).
1 Director of Research.2 Head-Kinesiology and Director of Health Sciences.
Journal of Electromyography and Kinesiology xxx (2012) xxx–xxx
Contents lists available at SciVerse ScienceDirect
Journal of Electromyography and Kinesiology
journal homepage: www.elsevier .com/locate / je lek in
Please cite this article in press as: Haavik H, Murphy B. The role of spinal manipulation in addressing disordered sensorimotor integration and alteredmotor control. J Electromyogr Kinesiol (2012), doi:10.1016/j.jelekin.2012.02.012

The Role of the Core Stability in Athletic Function Kibler & Press
• ‘Core stability’ is the ability to control the position & motion of the trunk over the pelvis to allow optimum production
• Core muscle activity is best understood as the pre-programmed integration of local, single-jt muscles and multi-jt muscles to provide stability and produce motion.
• Proximal stability for distal mobility


So what does it mean?
• If you find apparent inequality in the mirror image isometric tests … the patient has a neurological deficit
• If you find that there is a contralateral upper or lower extremity demonstrating a similar inequality … the patient has reciprocal limb syndrome RLS
• If you don’t find anything then there is no global imbalance … maybe …check head position

Pitching mechanics • Balance
counterbalance critical
• Power developed with cervical rotation
• Deceleration occurs with opposite cervical rotation
• Scapular Dyskinesis?

Shoulder Injuries
• Multifactorial • Power is generated
from the opposite lower extremity
• Scapulothoracic area has the greatest ability to adapt
• It requires a global assessment

Parting Thought
“You cannot solve the problems you now have at the same level of thinking you used to create them.”
Albert Einstein

Thank you for your attention!



























