Embed Size (px)
Citation preview
DBACKS MANUAL THERAPY APPROACH: Philosophy and Implementation in the
Professional Baseball Setting
Professional Baseball Chiropractic Society Workshop
January 29th, 2016
Ryan DiPanfilo ATC, CSCS, PRT
Assistant Athletic Trainer

Outline
I. Philosophy & PrinciplesII. Our Keys to SuccessIII. Testing & Treatment
a) Rib Cageb) Upper Extremityc) Lower Extremity
IV. Adjunct Treatmentsa) Recoveryb) Nutritional Supplementationc) Essential Oils

Dbacks Sports Medicine Healthcare Philosophy
Treatment Philosophies (where we draw from)
• PRI (Hruska)• FDM (Typaldos)• Fascial Manipulation (Stecco)• FDM• FRR/FRC (Spina)• ART (Leahy)• Self-Myofascial Release• Lymph Massage (Chikly)• Cupping• IASTM • Trigger Point Therapy (Travell &
Simons) • Dry Needling & Acupuncture• MET (Chaitow)• PRRT (Iams)
• Earthing• Nutrition/Supplementation
– Organic foods– Juicing– Alkaline Water– Nutrient IV’s
• Laser Therapy• Micro-current• Infrared Sauna Therapy• Essential Oils• Hydrotherapy• Compression Therapy (Normatec,
Recovery Pump)• Salt Tank Flotation• Visual Training

Fascial Distoration Model
• Dr. Stephen Typaldos, DO• Treatment model that
views virtually all musculoskeletal complaints as 1 or more of the 6 different types of alterations to the body’s connective tissues
• Each of the 6 alternations are identified through specific verbal and physical descriptions from the patient

Fascial Manipulation
• Luigi Stecco, Italian physiotherapist• “The mainstay of this manual method lies in
the identification of a specific, localized area of the fascia in connection with a specific limited movement. Once a limited or painful movement is identified, then a specific point on the fascia is implicated and, through the appropriate manipulation of this precise part of the fascia, movement can be restored.”
• 14 segments of body each with 6 myofascialunits
• Treatment of fascial densifications identified through palpation of specific fascialcovergence points that act on a joint during specific movements
• Centers of Coordination (CC): deep fascia usually in muscle belly
• Centers of Fusion (CF): septa, retinaculum & ligaments

ART/FRR
Active Release Technique (ART)Dr. Michael Leahy
Functional Range Release (FRR)Dr. Andreo Spina

Self-Myofascial Release
• Athlete-driven daily maintenance
• Warm-ups & cool down
• Empowers athlete for self-care (doesn’t need to rely on therapist)
• Foam rolls, trigger point balls, Tiger Tails, etc
Lymph Massage
• Gentle technique to facilitate natural drainage of lymph/waste post-activity
• Recovery & inflammation control
• Most often used post-game with pitchers

Cupping
• Mobilizes fascia/tissue & facilitates blood flow to localized area to promote healing
• Used in conjunction with movement
• By lifting tissue through suction, it offers alternative to regular downward manual pressure

Manual Therapy Keys to Success
Principles:– Look to identify location of densified, irregular
tissue AND/OR aberrant tissue tension in a specific direction that appears before end range of joint
– Be patient while waiting for release (time varies due to many different variables)
– Don’t look to force release…goal is to influence release (pressure & depth may change person-to-person, day-to-day)

Crucial Non-Manual Treatment Concepts
• Proper breathing (Diaphragm function is KEY!!!)
• Positioning (i.e. neutrality, joint centration)
• Movement quality/awareness
• Recovery
• Reference centers/fixation points
• Treating root cause/patterns (i.e. away from site of pain)
• Assessment: Test…Re-test

Testing the Injured Athlete: RIB CAGE
• Apical Expansion
• Posterior Mediastinum Expansion
• Supine IAP
• Trunk Rotation

Testing: Apical Expansion
Normal Abnormal
Ability to fill opposite chest wall
Inability to fill opposite chest wall due to either rib IR
orientation or hyperinflation

Testing: Posterior MediastinumExpansion
Normal Abnormal
Ability to fill posterior thorax upon inhalation
Inability to fill…descended pelvic floor position & flat
diaphragm positions

Testing: Supine IAP
Normal Abnormal
Proportional activation of all sections of ab wall
RA hyperactivity; inspiratorychest position; hollowing of
ab wall above groin
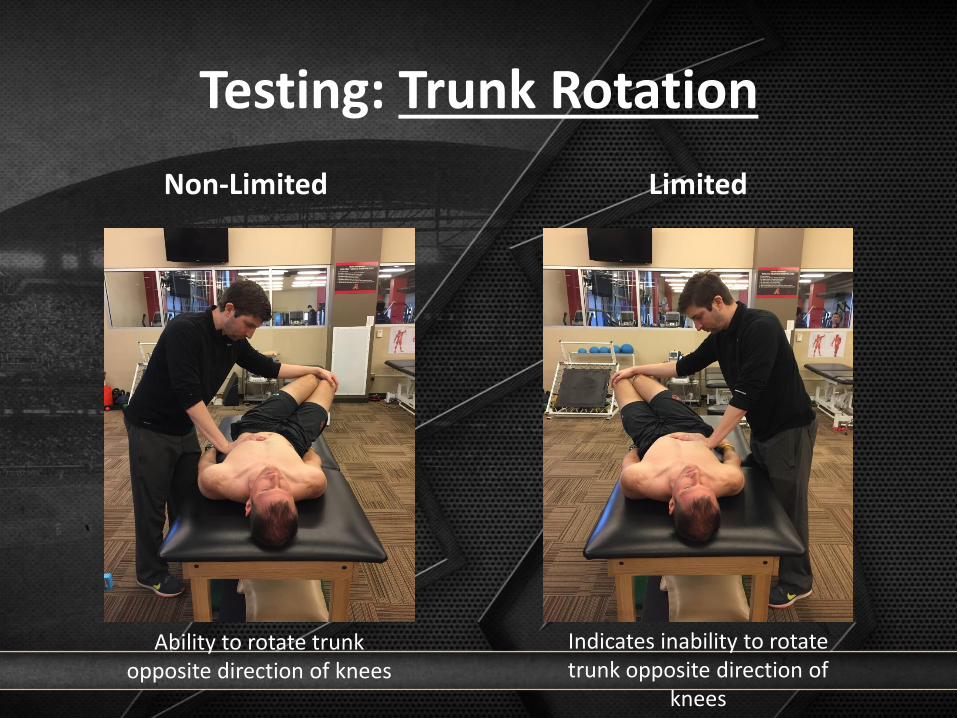
Testing: Trunk Rotation
Non-Limited Limited
Ability to rotate trunk opposite direction of knees
Indicates inability to rotate trunk opposite direction of
knees

Technique: Rib Cage
• L) AIC
– (+) R Apical Expansion, (+) R HG IR, (+) L Posterior Mediastinum
– Increase ability to fill anterior RIGHT & posterior LEFT chest wall
– Guiding ventilatory system to achieve position (diaphragm domed) to work neurologically as best as possible

Technique: Rib Cage
• Superior T4 – (+) R Apical Expansion, (+)
R HG IR, (+) L Posterior Mediastinum
– Isolate L) triangularis sternion exhalation & inhibit R) triangularis sterni on inhalation
– Isolate R) upper apical chest expansion/fill
– Inhibit neck involvement with accessory respiration
– Integrate diaphragm/abdominals at end of exhalation

Technique: Rib Cage
• Subclavius
– (+) L Apical Expansion following restoration of (-) R Apical Expansion
– R) subclavius restriction & R) neck tension
– Manually restoring rib 1-2 internal rotation ability & separation from clavicle

Technique: Rib Cage
• Infraclavicular Pump
– (+) Bilateral Apical Expansion, (+) B HG IR, (+) B TR,
– Mobilizing rib cage & teaching ribs to reciprocate/alternate with each inhale & exhale

Technique: Rib Cage
• Sibson’s Technique– Fascia from C7-T1 around
1st rib to manubrium to cupula of lung…Comprised of fascia from scalenes & longus colli muscles
– (+) R Apical Expansion, R) neck tension
– Anchoring fascia (not stretching) while allowing breathing & proper rib cage movement to reduce tension

Technique: Rib Cage
• Intercostal
– (+) R Apical Expansion, (+) R Trunk Rotation
– Facilitate rib ER & apical fill following complete exhalation to release intercostals

Testing the Injured Athlete: UPPER EXTREMITY
• HG IR/ER
• HG Horizontal ABD
• Standing and Supine Arm Lift

Testing: HG IR
Normal Abnormal
Full rotation towards table Restriction secondary to scap/rib cage positioning &
breathing

Testing: HG Horizontal ABD
Normal Abnormal
30-60°; ability to rotate trunk contralaterally
<30°; inability to rotate trunk contralaterally

Testing: Supine Arm Lift
Normal Abnormal
Lower ribs & T/L junction stabilized
Chest lifted cranially; poor lower rib fixation;
hyperextension

Testing: Standing Arm Lift
Normal Abnormal
Symmetrical cylindrical activation & expansion of ab
wall; scaps stabilized
Poor rib & T/L stabilization; upper trap hyperactivity;
elevation of scaps

Technique: Upper Extremity
• Latissimus Dorsi
– Limited Supine/Standing Arm Lift, (+) Apical Expansion, Increased lumbar lordosis, Flat T-Spine, (+) HG IR/ER
– Can often be implicated with patterned, extension-dominant overhead athlete

Technique: Upper Extremity
• Pectoralis Major– Limited Supine/Standing
Arm Lift, (+) Apical Expansion, (+) HG IR/ER, (+) HG ABD, Flat T-Spine
– Can contribute to protracted, anteriorlytipped & IR scapaccompanied by rib ER
– Leveraged with hyperinflated overhead athlete
Technique: Upper Extremity
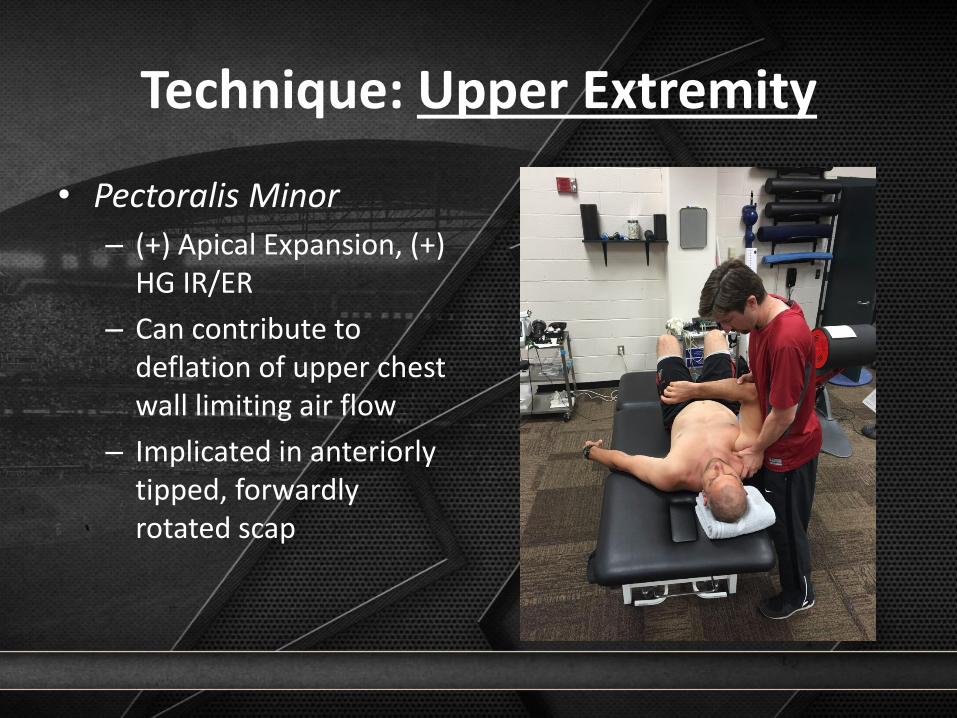
• Pectoralis Minor
– (+) Apical Expansion, (+) HG IR/ER
– Can contribute to deflation of upper chest wall limiting air flow
– Implicated in anteriorlytipped, forwardly rotated scap
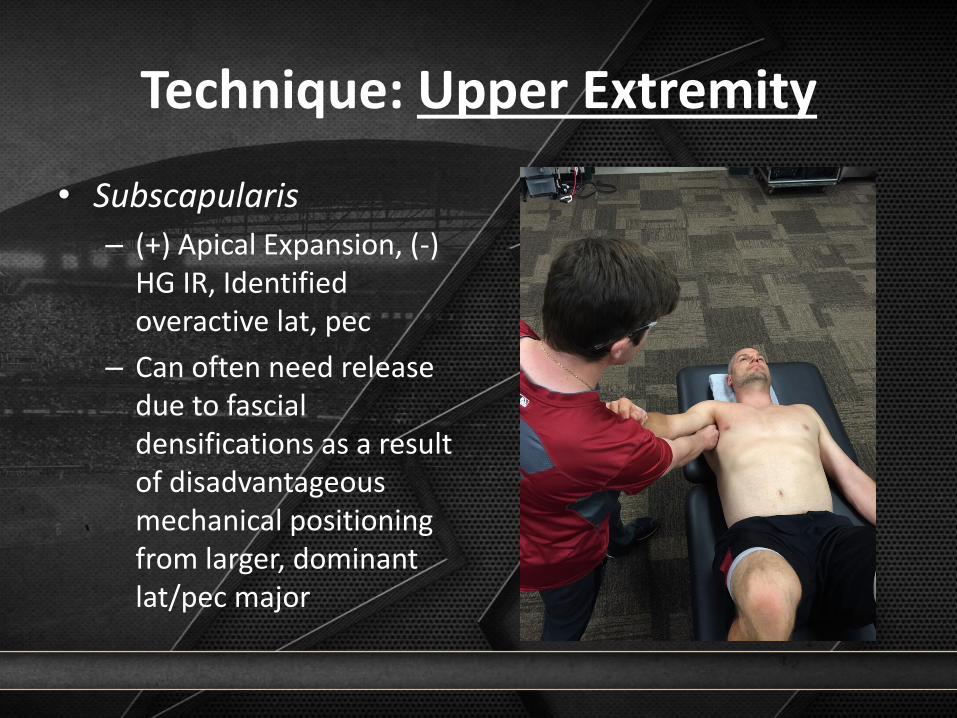
Technique: Upper Extremity
• Subscapularis
– (+) Apical Expansion, (-) HG IR, Identified overactive lat, pec
– Can often need release due to fascialdensifications as a result of disadvantageous mechanical positioning from larger, dominant lat/pec major

Testing the Injured Athlete: LOWER EXTREMITY
• Adduction Drop Test
• Extension Drop Test
• Passive Adduction Raise Test
• Seated FA IR/ER

Testing: Adduction Drop Test
Normal Abnormal
Neutral hemi-pelvis; ability to extend & adduct
Restriction secondary to anteriorly rotated & forward
hemi-pelvis

Testing: Extension Drop Test
Negative Positive
If (-) ADT = Good, non-pathoIf (+) ADT = Bad, lax anterior
capsule
If (+) ADT = Good, intact capsuleIf (-) ADT = Bad, overactive hip flexors

Testing: Passive Abduction Raise Test
Normal Abnormal
Ability for femur to ABD on pelvis due to positional
clearance
Restriction due to pelvic outlet ABD position,
overactive adductor magnus

Testing: Seated FA IR/ER
IR ER
Integrity of postero-inferior capsule/ischiofemoral
ligament if pelvis is NEUTRAL
Integrity of antero-superior capsule/iliofemoral ligament
if pelvis is NEUTRAL

Technique: Lower Extremity
• Psoas Major
– (+) ADT, (-) PART, Limited FA IR…or (-) ADT with (+) EDT
– Can be overactive as FA flexor/ER in athlete with sagittally compromised abs/hamstrings/glutes

Technique: Lower Extremity
• TFL
– (+) ADT, (-) PART, Limited FA IR
– Can be overactive as IR muscle that is dominating anterior glute medius if pelvis/rib cage in compromised position (especially on left)

Technique: Lower Extremity
• Adductor Magnus
– (-) ADT, (+) PART, Limited FA ER
– Can be overactive as frontal plane adductor (especially on right)
Technique: Lower Extremity
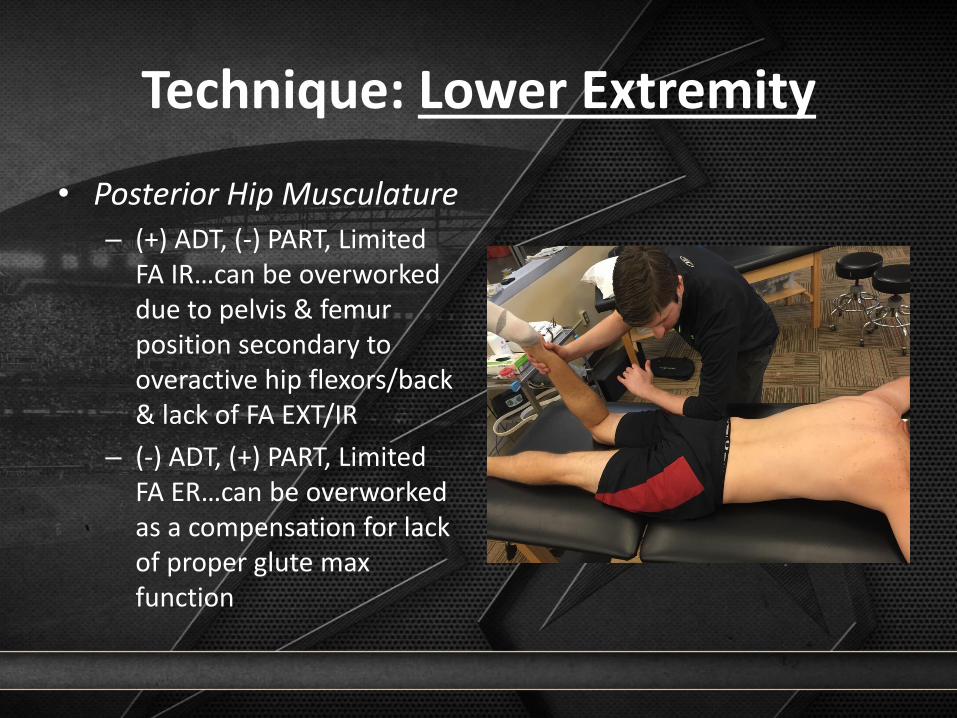
• Posterior Hip Musculature
– (+) ADT, (-) PART, Limited FA IR…can be overworked due to pelvis & femur position secondary to overactive hip flexors/back & lack of FA EXT/IR
– (-) ADT, (+) PART, Limited FA ER…can be overworked as a compensation for lack of proper glute max function

Technique: Lower Extremity
Quadriceps Hamstrings

Adjunct Treatments: Recovery
• Pool options (Hot & Cold)
• REST tank
• Infrared saunas
• Earthing mats
• Pneumatic compression

Adjunct Treatments: Nutrition
• Organic, nutrient dense food options at all times
• Alkaline water units
• Daily post-BP nutritional shakes
• Supplementation options:– Multivitamin
– Fish Oil
– Probiotic

Adjunct Treatments: Essential Oils
• Therapeutic topical applications to aid in relaxation, tissue healing, inflammation control, etc
• Healthier alternative to OTC topical ointments

Take Home Points
1. Prioritize diaphragmatic position & function2. Correct identified thorax deficiencies before
addressing extremities (i.e. rib cage mobility, ability to achieve full exhalation)
3. Athlete body awareness during treatment is a must (i.e. FEELING ribs drop into IR during full exhalation while moving into full ER during inhalation)
4. Think globally (i.e. Is pelvis-on-femur position affecting shoulder function?) & holistically
5. Test…Re-Test

References
About Fascial Manipulation. (n.d.). Retrieved January 26, 2016 from http://www.fascialmanipulation.com/en/about-fascial-manipulation.aspx?lang=enActive Release Techniques. (n.d.). Retrieved January 26, 2016 from http://www.activerelease.com/Anderson, J., & Gruver, L.A. (2014). PRI Integration for Baseball course manual. Lincoln, NE: Postural Restoration Institute.Anderson, J. (2013). PRI Impingement & Instability course manual. Lincoln, NE: Postural Restoration Institute.Anderson, J. (2013). PRI Myokinematic Restoration course manual. Lincoln, NE: Postural Restoration Institute.Functional Range Release. (n.d.). Retrieved January 26, 2016 from https://www.functionalanatomyseminars.com/Getting Started with Essential Oils. (n.d.). Retrieved January 28, 2016 from http://www.honeygheeandme.com/essential-oils/Guest Post! Foam Rolling Techniques for Runners. (2014, August 28). Retrieved January 26, 2016 from http://www.paleorunningmomma.com/guest-post-
foam-rolling-techniques-for-runners/Hruska, R. (2014). PRI Cranio-Cervical-Mandibular Restoration course manual. Lincoln, NE: Postural Restoration Institute.Hruska, R. (2013). PRI Postural Respiration course manual. Lincoln, NE. Postural Restoration Institute.Kangzhu 12 Cup Chinese Cupping Therapy Set. (n.d.). Retrieved January 26, 2016 from
http://www.chinesecupping.com/kang_zhu_12cup_cupping_set.htmlKolar, P., & Kobesova, A. (2012). Dynamic Neuromuscular Stabilization According to Kolar Standardized “Advanced Skills” course manual. Prague, Czech
Republic: Rehabilitation Prague School.Kolar, P., & Kobesova, A. (2011). Dynamic Neuromuscular Stabilization According to Kolar Standardized “C” course manual. Prague, Czech Republic:
Rehabilitation Prague School.Kolar, P., & Kobesova, A. (2010). Dynamic Neuromuscular Stabilization According to Kolar Standardized “B” course manual. Prague, Czech Republic:
Rehabilitation Prague School.Kolar, P., & Kobesova, A. (2010). Dynamic Neuromuscular Stabilization According to Kolar Standardized “A” course manual. Prague, Czech Republic:
Rehabilitation Prague School.Silent Waves: Theory and Practice of Lymph Drainage Therapy. (n.d.). Retrieved January 26, 2016 from https://chiklyinstitute.com/Products/Silent-WavesThomsen, L. (2014). PRI Pelvis Restoration – Home Study course manual. Lincoln, NE: Postural Restoration Institute.What is FDM? (n.d.). Retrieved January 26, 2016 from https://www.fascialdistortion.com/what-is-fdm/

THANK YOU!

The Functional Movement Screen as used and implemented by the
Arizona Diamondbacks
Professional Baseball Chiropractic Society Workshop
January 29th, 2016
Paul Porter MS, ATC, PES
Assistant Minor League Medical Coordinator

Functional Movement Screen
• “A ranking and grading system that documents movement patterns that are key to normal function”.
• Tool used to identify “functional limitations and asymmetries”

Limitations and Asymmetries
• What are they?
– Issues that can reduce the effects of:
• Functional Training
• Physical Conditioning
• Lead to distorted body awareness
• Why do we want to address these?
– Restore mechanically sound movement patterns to enhance training and reduce the risk of injury

Functional Movement Screen:What it is
• A functional evaluation, leading to the prescription of corrective exercises
• Test of how the “software” operates
– How the person uses their body
• Stems from a DNS background
– Developmental kinesiology
• 7 Tests
– Ranging from mobility and stability tests
Functional Movement Screen:Tests
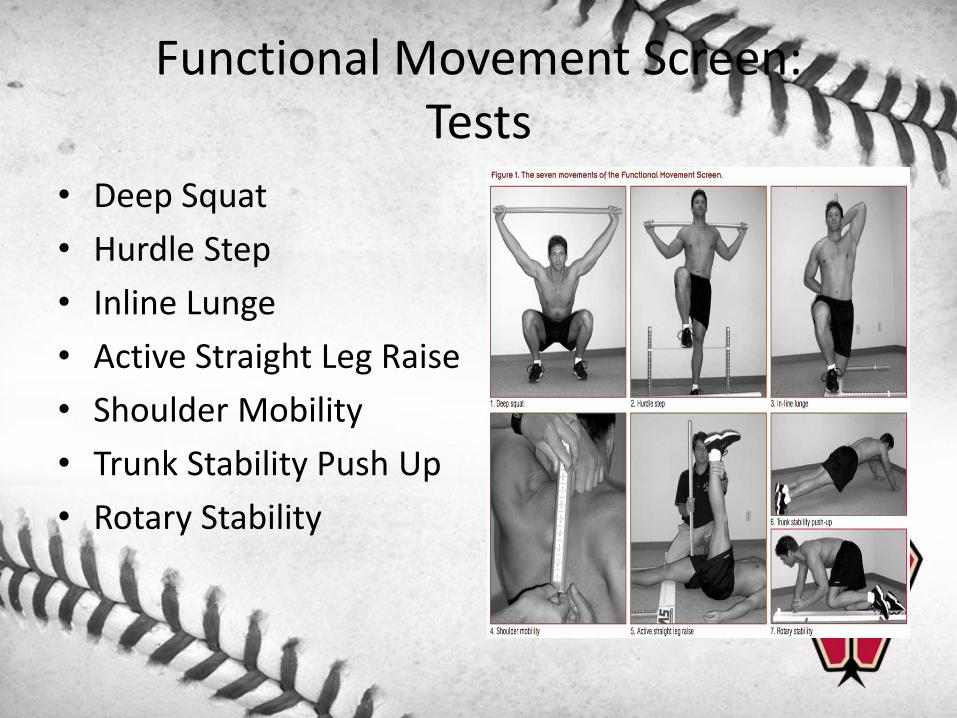
• Deep Squat
• Hurdle Step
• Inline Lunge
• Active Straight Leg Raise
• Shoulder Mobility
• Trunk Stability Push Up
• Rotary Stability

Functional Movement Screen:Scoring Sheet
• Identifying (in order of priority)– Pain with movement
(Scored as a 0)
– Inability to perform a simple movement pattern, even with compensation (Scored as a 1)
– Major asymmetry with movement (e.g. 3 on L, 1 on R)

Functional Movement Screen
• What it does:– Simplifies the concept of movement and its impact on the body
by providing:– Communication
• Simple language
– Evaluation• Quick; approx 5-8 mins
– Standardization• Functional baseline
– Safety• Identifies dangerous movement patterns• Participant readiness for exercise
– Corrective Strategies• Can be applied at any level

Functional Movement Screen:Why the Diamondbacks like it
• Insight into a player’s motor recruitment/ movement pattern
• Simplicity– Exam is easy and convenient to
implement
• Effectiveness of corrective exercise
• Common language between athletic trainers and strength and conditioning coaches
• Backed by research• Provides quantitative data to
flag at risk individuals
Functional Movement Screen:How we implement it
• Pre-participation Physical Exams– Screens performed during spring Training, mid season, end of season, and
during rehab– Spreadsheet; asymmetries, asymmetries with a 0 or a 1, scores below 14, 3 or
more asymmetries
• Test/ Retest– Short term and long term– Does what we prescribe make a change on the person’s ability to move
• Exercise selection– Why we select what we select– Is it a mobility or a motor control issue?
• Exercise prescription– Quality over quantity– Regress to most basic movement before progressing

Test Results during the Season

FMS Screen Report

Functional Movement Screen:In rehab setting
• Supplement their Postural Restoration Institute exercise prescription
• Build strength
– Body Weight
– Chops/ Lifts
– Kettle Bells
• Prevention of future injuries
– Better movement patterns; stability

Functional Movement Screen:In strength and conditioning/ prevention setting
• Supplement their Postural Restoration Institute exercise prescription
• Incorporate FMS into their warm up in the weight room prior to baseball activities
– Enhance mobility
– Correct movement dysfunctions
– Prepare body to perform baseball activities
• Create better static stability, dynamic stability

Player 1
• No asymmetry
• 3’s on four tests
• 2’s on three tests
• Focus on priority tests/ movements first
– TSPU, ASLR, SM
L
R
L
R
L
R
L
R
L
R
L
R
Total 18
2 2
Press-Up Clearing Test Negative
Rotary Stability2
2
Inline Lunge 3
Shoulder Mobility 3
Impingement Clearing Test Negative
Test Raw Score Final Score
Deep Squat 3 3
2
Posterior Rocking Clearing Test Negative
3Active Straight Leg Raise 3
Trunk Stability Push Up
3Negative
Negative
3
2
3
3
3
Hurdle Step2
2

Player 1exercise selection
• Power Push Ups
• Push Up Drive to Elbows
• Tall Kneeling Activity –TSPU
• Bear Crawl
• Bottom’s Up March
• Bottom’s Up Lunge

Player 2
• One asymmetry (Shoulder mobility)
• All final scores are 2’s.
• Address asymmetry first
• Unilateral activity before bilateral
– Half kneeling
– Rotary stability
L
R
L
R
L
R
L
R
L
R
L
R
2
Negative
Negative
2
2
2
2
Negative
2
2
2
2
2
14
2
2
2
3Negative
Negative
2
2
2
2
Hurdle Step
Shoulder Mobility
Impingement Clearing Test
Active Straight Leg Raise
Rotary Stability
Trunk Stability Push Up
Press-Up Clearing Test
Posterior Rocking Clearing Test
Total
Raw ScoreTest Final Score
Inline Lunge2
Deep Squat
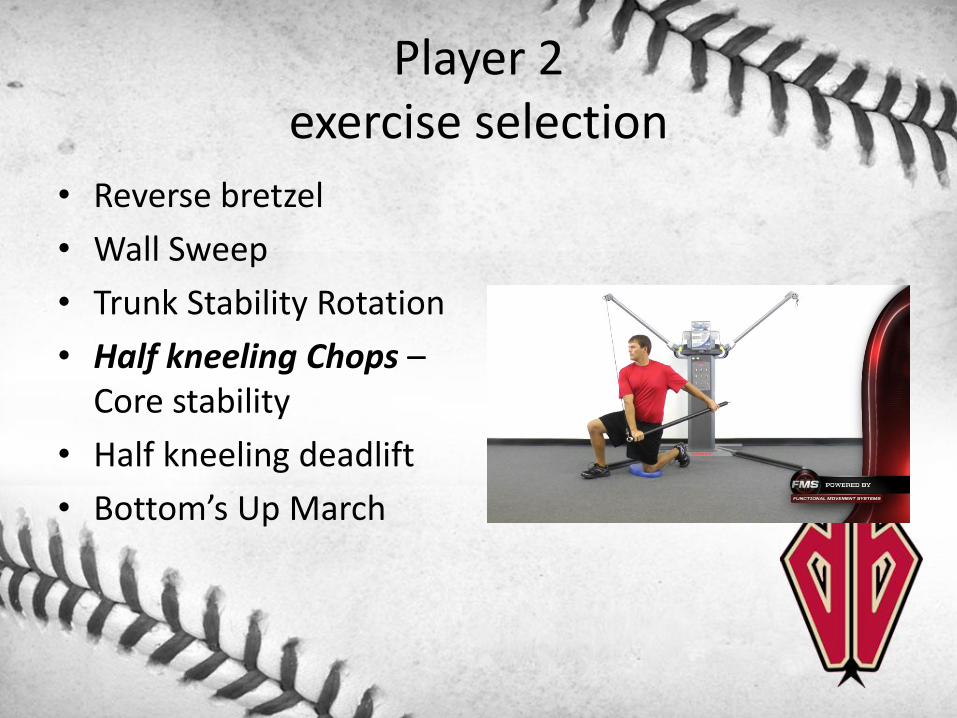
Player 2 exercise selection
• Reverse bretzel
• Wall Sweep
• Trunk Stability Rotation
• Half kneeling Chops –Core stability
• Half kneeling deadlift
• Bottom’s Up March

Player 3
• One asymmetry (Rotary Stability)
• Mixture of 3’s and 2’s
• Address asymmetry first
• Focus on pelvic control/ Active straight leg raise
L
R
L
R
L
R
L
R
L
R
L
R
Posterior Rocking Clearing Test Negative
Total 15
Press-Up Clearing Test Negative
Rotary Stability1
12
Active Straight Leg Raise2
22
Trunk Stability Push Up 2 2
Shoulder Mobility3
33
Impingement Clearing TestNegative
NegativeNegative
Hurdle Step2
22
Inline Lunge2
22
Test Raw Score Final Score
Deep Squat 3 3

Player 3exercise selection
• Leg lowering w/ kettlebell – ASLR/ pelvic stability
• Supine diagonals
• Hard roll
• Physioball Stability Rock
• Bear Crawl March

Player 4
• One asymmetry (ASLR)
• Raw score of 1 on DS and SM
• 2 on IL and HS –unilateral mover
L
R
L
R
L
R
L
R
L
R
L
R
Posterior Rocking Clearing Test Negative
Total 13
Press-Up Clearing Test Negative
Rotary Stability2
22
Active Straight Leg Raise2
23
Trunk Stability Push Up 3 3
Shoulder Mobility1
11
Impingement Clearing TestNegative
NegativeNegative
Hurdle Step2
22
Inline Lunge2
22
Test Raw Score Final Score
Deep Squat 1 1
Player 4exercise selection
• Toe Touch Progression – Hip hinge
• Leg Lowering w/ KB
• Turkish Get Up Figure 8’s
• Reverse bretzel
• Reverse bretzel w/ reach
• Physioball Stability Rock

Player 5
• 2 scores of zero due to pain in shoulder (SLAP repair Oct/15)
• One asymmetry (SM)
L
R
L
R
L
R
L
R
L
R
L
R
Posterior Rocking Clearing Test Negative
Total 11
Press-Up Clearing Test Negative
Rotary Stability0
00
Active Straight Leg Raise3
33
Trunk Stability Push Up 0 0
Shoulder Mobility1
13
Impingement Clearing TestNegative
NegativeNegative
Hurdle Step2
22
Inline Lunge3
33
Test Raw Score Final Score
Deep Squat 2 2

Player 5 exercise selection
• Reverse bretzel –Thoracic mobility
• Wall Sweep
• Trunk Stability Rotation
• Half Kneeling Dorsiflexion Stretch
• High Step w/ KB
• Bottom’s Up Lunge

References
• What is FMS? (n.d.). Retrieved December 22, 2015, from http://www.functionalmovement.com/fms
• Schwartzkopf-Phifer, K., & Kiesel, K. (2014, July). Functional movement tests and injury risk in athletes. Retrieved December 28, 2015, from http://lermagazine.com/article/functional-movement-tests-and-injury-risk-in-athletes\
• Burton, L. (2010, December 20). Tips on Using and Documenting the Scores on the Functional Movement Screen Score Sheet. Retrieved December 29, 2015, from http://functionalmovement.com/articles/Screening/2010-12-20_tips_on_using_and_documenting_the_scores_on_the_functional_movement_screen_score_sheet
• Plisky, P. (2015, December 9). The Relationship Between the FMS and Injury Risk. Retrieved December 29, 2015, from http://functionalmovement.com/articles/Research/649/the_relationship_between_the_fms_and_injury_risk


Pre-Season Assessments: What are they telling us?
Kyle Torgerson, MS, ATC, CSCS
Minor League Medical Coordinator
Arizona Diamondbacks

Overview of Material• Part I – Pre-Season Screens
– General Physician Orthopedic Evaluation– DBacks postural screen– FMS screen
• Part II – Screen Evaluations– Short Term Goals :
• Evaluating “At-Risk” individuals & Team Deficiencies
– Long Term Goals:• Collecting data throughout the season to determine:
– Low/Medium/High Risk Players
• Part III – Transforming to the Field– On Field Application– Re-Evaluating/Improving Assessment

Minor League Baseball Factors and Variables
• 200+ players during spring training
– 3 different physical dates
– Determine orthopedic “At-Risk”
– PRI Postural exam
• Sports Medicine Team = 18-24 members
– Spring Training FMS screens

What information do we expect to receive from the different screens?
ScreenWhat we are looking for?
PRIAsymmetries
(Normal, but not optimal)
FMSAsymmetries and
Total Score
OrthopedicEvaluation
Pain & Obvious abnormalities

Physician Orthopedic Evaluation
• Total Body Evaluation– Foot/Ankle
– Hand/Wrist
– Spine/Head/Neck
– Shoulder/Elbow
• Special Tests per Region
• Manual Muscles Test per Region
• Diagnostic recommendations– MRI / X-ray / CT Scan
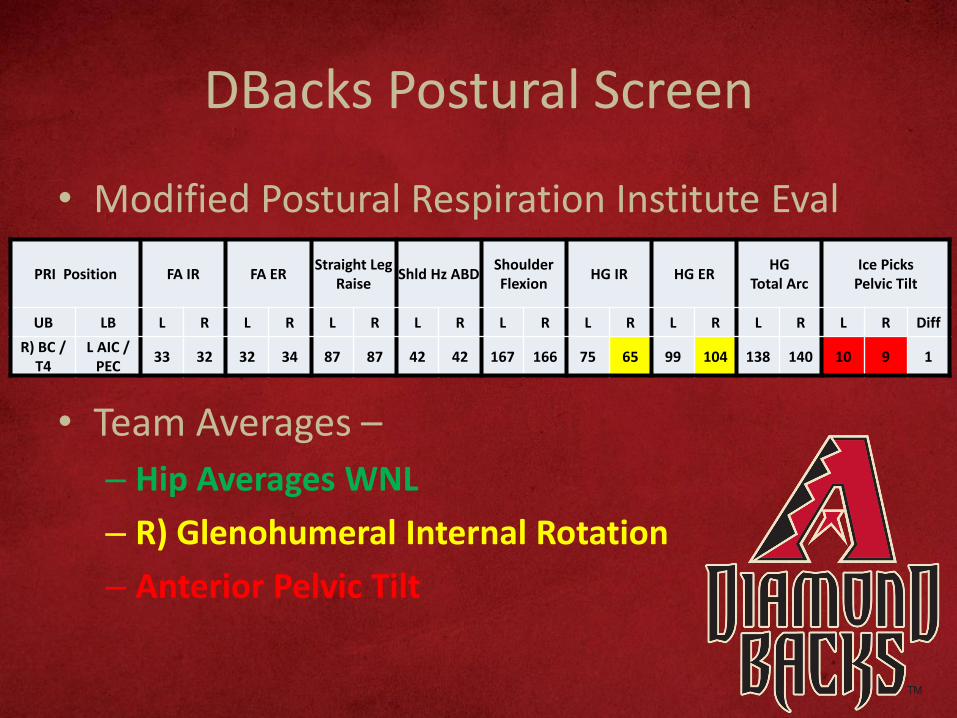
DBacks Postural Screen
• Modified Postural Respiration Institute Eval
PRI Position FA IR FA ERStraight Leg
RaiseShld Hz ABD
Shoulder Flexion
HG IR HG ERHG
Total ArcIce Picks
Pelvic Tilt
UB LB L R L R L R L R L R L R L R L R L R Diff
R) BC / T4
L AIC / PEC
33 32 32 34 87 87 42 42 167 166 75 65 99 104 138 140 10 9 1
• Team Averages –
– Hip Averages WNL
– R) Glenohumeral Internal Rotation
– Anterior Pelvic Tilt

Functional Movement Screen Evaluation
SQUAT HURDLE STEP INLINE LUNGESHOULDER MOBILITY
ACTIVE STRAIGHT LEG RAISE
TRUNK STABILITY PUSH UP ROTARY STABILITY TOTAL ASYM.
RAW FINAL L R FINAL L R FINAL L R FINAL L R FINAL RAW FINAL L R FINAL
1.83 1.83 2.00 2.07 2.00 2.76 2.76 2.76 2.83 2.79 2.69 2.14 2.10 2.03 1.97 1.97 1.93 1.90 1.90 15.17 0.48
• Team Averages –
– Split stance and shoulder mobility
– Single leg stance
– Core integration

So What does this all mean?
• ?????
• The PRI and Orthopedic evaluation gives us an idea of:– Joint capsule integrity
– Ligamentous integrity
– Joint-by-Joint integrity
• FMS evaluation gives us an idea of:– How well does the athlete move
– How well does the athlete compensate

Categories for Individual deficiencies and goals for intervention
ScreenWhat we are looking for?
Goal
PRIAsymmetries
(Normal, but not optimal)
Reciprocate & Integrate Body
AwarenessSystems
FMSAsymmetries and
Total Score
Core Control & Symmetrical
Patterns
OrthopedicEvaluation
Pain & Obvious abnormalities
Rule if player if ABLE or UNABLE
to participate

Short Terms Goals from screens:Identifying “At-Risk” Athletes
• What numbers identify athletes as at risk?
– FMS articles identifying 14 and under for an overall total are athletes who are at a higher risk for injury
– Currently, there are over 14 reliability studies on the Functional Movement Screen that indicate that it has good to excellent reliability.

Short Terms Goals from screens:Identifying “At-Risk” Team Deficiencies• Overall team numbers can point us in a
direction to assist universal warm-up
– Not perfect for each individual, but with the overall numbers in MiLB, helps overall prevention
• FA IR deficiencies (PRI Screen)
– Unable to get into the front hip
– Weak Back side (i.e. Glute Max)
Long Terms Goals from screens:
• Collecting data throughout seasons
• Comparing data– Pre-Season
– Mid-Season
– End of Season
• Attempting to make an educated guesson who are the athletes at a higher risk of injury from the data collected
Long Terms Goals from screens:
• When an athlete is injured
– Look at previous/most recent screen
• Chronic or acute injury
• What was their deficiency
• Due to injury or post-surgical
– Unable to complete a full PRI/FMS screen
– Use previous screen to address what the
player lacks

On-Field Application
• How do these evals correlate to on field performance
• Best example I can give is Femoral-Acetabular Internal Rotation
– Applies to Hitting and Pitching Mechanics
– Righties vs. Lefties

FA IR FA ER
Last First Hand L R L R
R 22 25 48 43
Right Handed Hitters

FA IR FA ER
Last First Hand L R L R
R 52 41 33 31
R 35 33 42 31
Right Handed Hitters

Left Handed Hitters
FA IR FA ER
Last First Hand L R L R
R 46 43 45 47

Left Handed Pitcher
FA IR FA ER
Last First L R L R
LHP (pre TJ) 33 40 35 33
LHP 50 51 34 34

Right Handed PitcherFA IR FA ER
Last First L R L R
RHP 33 30 34 43
• Right hander unable to get into L FA IR

Re-Evaluating Our Process
• End of season process
– Evaluate screens from beginning/middle/end
• Individual Changes?
– Assess “High Risk” guys
– Evaluate the screen
• What should we add or subtract to our screening process
• Always looking into improve

References
• Arnsberg, B. (2016, January 21). Personal Interview
• Pilsky, P. (2015, December 9). The Relationship Between the FMS and Injury Riskhttp://www.functionalmovement.com/articles/Research/649/the_relationship_between_the_fms_and_injury_risk
• Masek, J. (2015, March 15). Femoroacetabular impingement: mechanisms, diagnosis and treatment options using Postural Restoration Part 1https://co-kinetic.com/content/femoroacetabular-impingement-mechanisms-diagnosis-and-treatment-options-using-postural-restoration-part-1