Embed Size (px)
Citation preview

Workshop GISCi L'Aquila giugno 2012
Gli indicatori di progressione:Ricaduta sul trattamento delle lesioni
Il punto di vista del Patologo
Paolo Dalla Palma
HPV test positivo e poi?Il 2°livello nei programmi di screening con il test HPV

Workshop GISCi L'Aquila giugno 2012
Ostor AG . Natural history of cervical intraepithelialneoplasia: a critical review .
Int J Gynecol Pathol 1993;12:186–92.

Workshop GISCi L'Aquila giugno 2012
Fattori di rischio “generico ” di progressione
• Età• Fumo di sigaretta.• Uso di lunga data di contraccettivi orali.• Parti multipli.• Nuovi partner sessuali. • Immunodepressione.
• Persistenza dell’infezione virale.

Workshop GISCi L'Aquila giugno 2012
Fattori di rischio “più specifici ” di progressione
• Persistenza di HPV di genotipo “16”• Positività dei margini chirurgici dopo
conizzazzione per lesione di alto grado ->recidiva ->progressione.
Workshop GISCi L'Aquila giugno 2012
Fattori di rischio “individuali” di progressione
Si stima che circa il 30-50% dei grandi CIN3 progre dirà a carcinoma in un periodo di 30 anni, ma i fattori individuali per la singola donna determinanti l’invasione non sono ancora noti.

Workshop GISCi L'Aquila giugno 2012
Partendo dalla sola citologia cosa si può dire di nuovo?

Workshop GISCi L'Aquila giugno 2012
Screening for Cervical Cancer: A Decision Analysis for t he U.S. Preventive Services Task Force
Agency for Healthcare Research and Quality ; May 2011
P di Ca
>PPV

Workshop GISCi L'Aquila giugno 2012
Methods for triaging HPV positive women are warranted
Identify women with
Cin3+
HPV testing is more sensitive but less specific tha n cytology .
At recruitment
Identify persistent HPV infection at major risk of
Progression
In the follow-up
IDEAL TRIAGE STRATEGY

Workshop GISCi L'Aquila giugno 2012
Screening for Cervical Cancer: A Decision Analysis for t he U.S. Preventive Services Task ForceAgency for Healthcare Research and Quality ; May 2011
MINORE
MAGGIOREEta
’

Workshop GISCi L'Aquila giugno 2012
L’ HPV test
Quale tipo di test
38.293.327.3AbbottAbbot RealTi me
50.788.958.1Alla Colposcopia
Citologia (LSIL+)
37.895.024.2BectonDickinson
BD HPV
49.185.754.7Roche-MTMCinTec p16
39.395.328.8Gen-ProbeAptima
55.474.170.8NorChipPreTect Proofer
37.695.224.0RocheCobas 4800
37.496.319.5QiagenHC2
CIN 2+PPV
CIN 2+Sens
CIN 2+Spec
A. Szarewski , J. Clin. Microbiol. June 2012 vol. 50 no. 6 1867-1873

Workshop GISCi L'Aquila giugno 2012
Sensibitità e VPN per CIN2+

Workshop GISCi L'Aquila giugno 2012
Specificità e VPP per CIN2+
Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012CIN1 CIN2 CIN3
HSIL HSILLSIL

Workshop GISCi L'Aquila giugno 2012
Combined p16/Ki67 Biomarker Test- CINtec® PLUS -
The p16/Ki67 double staining takes cytodiagnosticsof cervical dysplasia one step further:
From detecting genes of an infectious agent ….
To visualizing proteins of HPV-inducedoncogenic cell transformation
Workshop GISCi L'Aquila giugno 2012
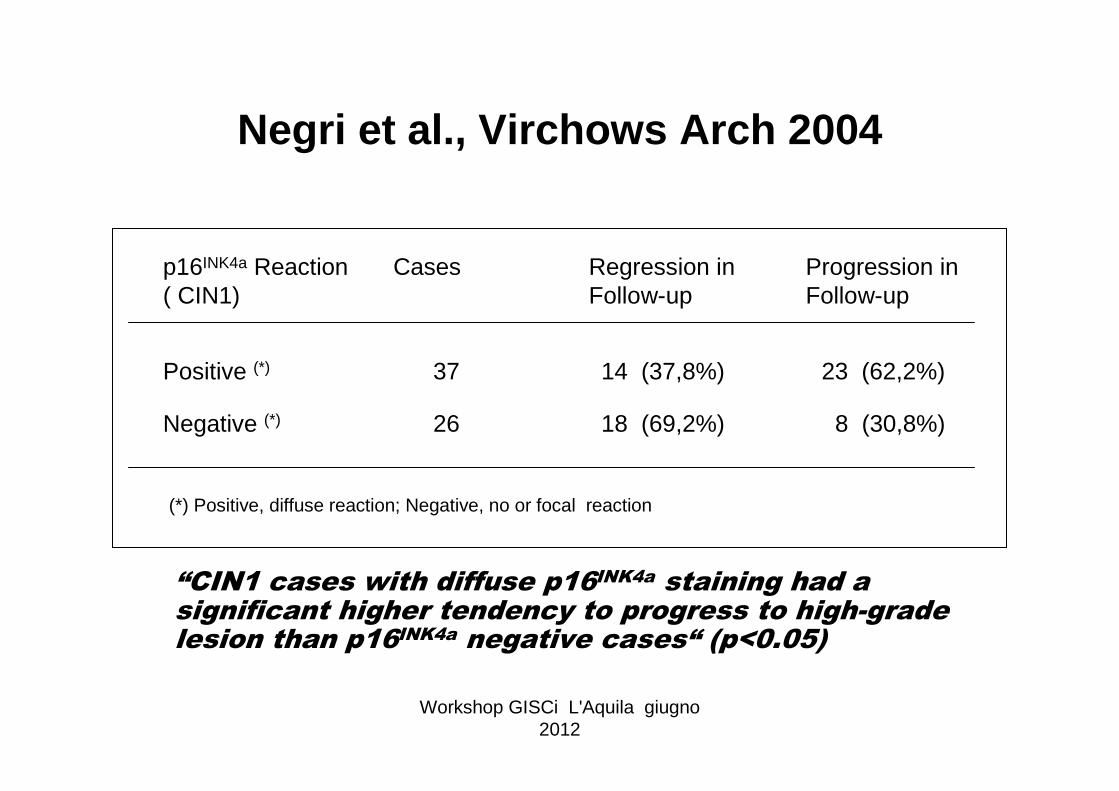
“CIN1 cases with diffuse p16INK4a staining had a significant higher tendency to progress to high-gradelesion than p16INK4a negative cases“ (p<0.05)
p16INK4a Reaction( CIN1)
Cases Regression inFollow-up
Progression in Follow-up
Positive (*) 37 14 (37,8%) 23 (62,2%)
Negative (*) 26 18 (69,2%) 8 (30,8%)
(*) Positive, diffuse reaction; Negative, no or focal reaction
Negri et al., Virchows Arch 2004

Workshop GISCi L'Aquila giugno 2012
In conclusion, p16, Ki-67, and ProEX C have been shown to be usefulmarkers for the diagnosis of neoplastic lesions of the gl andular epitheliaof the cervix uteri. However, both p16 and the prolife ration markers havestrengths and limitations. The combination of them can be helpful in some cases, particularly in the rare case of p16-negative neoplasms, yet lessuseful in others, in which both p16 and proliferation m arkers may beexpressed in nonneoplastic epithelia. Moreover, these biomarkers, particularly p16, may improve the accuracy of the diagnosis ofGlandular Dysplasia, also providing the biological background of thisstill poorly understood entity.

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012
RealTime High Risk HPV ABBOTT Molecular
The Abbott RealTie High Risk (HR) HPV assay is a qualit ative in vitro polymerase chain reaction (PCR) assay that utilizes homog eneous target amplification and detection technology for the detecti on of high risk humanpapillomavirus (HPV) DNA in cervical cells collected in liquid cytologymedia. The Abbott RealTie HR HPV assay is intended to det ect 14 high riskHPV genotypes: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68 and topartially genotype 16, 18 from other 12 high risk genoty pes.One Assay - Three Results:Women infected with HPV 16 and / or HPV 18 have an incr eased risk ofprogression to dysplasia and cervical cancer compared to w omen infectedwith other high risk HPV genotypes. Detection of the 14 high risk HPV genotypes and genotyping of HPV 16 and HPV 18 allows fo r improved riskassessment and patient management. The Abbott RealTie High Risk HPV assay enables the laboratory to be ONE STEP AHEAD by dete cting the 14 High Risk HPV genotypes and identifying HPV genotypes 1 6 and 18 with onesingle assay consolidating the two diagnostic tools of sc reening and genotyping. The assay provides the necessary informati on for patientstratification and is designed for more timely and cost e ffective HPV testing .

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012PPV (CIN2+)-86% (n=146); SPECIFICITY-96% (n=322 wnl)
mRNA FLOW FISH
sample
fixation
fixed cells,permeabilised
washing
hybridised cells
fluorescent dye
target (mRNA)
probe
mRNAhybridisation
fluorescently labelledoligonucleotide probe
Flow Cytometer

Workshop GISCi L'Aquila giugno 2012
p16+ or HPV16,18,33,35,52
p16+ or HPV16,18
p16 positiveASCUS+ or
HPV16,18,33,35,52
ASCUS+ or HPV 16,18
HPV16,18,33,35,52,31
HPV 16,18,33,35,52
HPV 16,18
0,80
0,90
1,00
1,10
1,20
1,30
1,40
1,50
1,60
1,70
0,80 0,90 1,00 1,10 1,20 1,30 1,40 1,50 1,60 1,70
relative immediate referral rate to colposcopy
rela
tive
sens
ityvi
ty fo
r CIN
2+
NTCC STUDY – women age 35-60Relative (vs. conventional cytology) sensitivity for the presence of CIN2 or more severe histology and immediate referral rate to colposcopy of HPV
testing followed by different triage strategies

Workshop GISCi L'Aquila giugno 2012
Regressione vs Progressione

Workshop GISCi L'Aquila giugno 2012
L’ HPV testNel Follow up
Il rischio di CIN2+ postIl rischio di CIN2+ post --trattamento per donne con trattamento per donne con 3 citologie negative o con un test negativo per 3 citologie negative o con un test negativo per citologia e HPV test concomitante citologia e HPV test concomitante èè uguale a uguale a quello delle donne in screening con normale quello delle donne in screening con normale citologia e quindi possono tornare alla medesima citologia e quindi possono tornare alla medesima tempistica di screening.tempistica di screening.

Workshop GISCi L'Aquila giugno 2012
Obstet Gynecol 2009;113:18–25
OBJECTIVE: To estimate the fraction of cervical intraep ithelial neoplasia 2 (CIN 2) that might regress if untreated using data from th e AtypicalSquamous Cells of Undetermined Significance/Low-Grade Sq uamousIntraepithelial Lesions Triage Study (ALTS).
A significant portion (about 40%) of CIN 2 diagnosed by c entralpanel review, even caused by high-risk–HPV genotypes, mayrepresent only regressive lesions whereas some CIN 2 may have“progressed” to CIN 3.
CONCLUSION: CONCLUSION: ThereThere waswas evidenceevidence thatthat approximatelyapproximately40% 40% ofof undiagnosedundiagnosed CIN 2 CIN 2 willwill regressregress overover 2 2 yearsyears , , butbutCIN 2 CIN 2 causedcaused by HPVby HPV --16 16 maymay bebe lessless likelylikely toto regressregressthanthan CIN 2 CIN 2 causedcaused by by otherother highhigh --riskrisk ––HPVHPV genotypesgenotypes .

Workshop GISCi L'Aquila giugno 2012
there is an increased risk of developing CIN2 or worse associated with specific high-risk HPV types (hpv 16,18,31,33), most CIN2 , if left untreated, will never progress toinvasive cancer, and, in some women, notably younger women, these lesions can regress. By contrast, the risk of CIN3 progressing to cancer is substantial if le ftuntreated (22).
J Natl Cancer Inst 2010;102:1478–1488
DNA testing for high-risk HPV genotypes (types for short) fulfills all essential criteria for a candidate cervical cancer screening tool . It is substantially more sensitive compared with Pap cytology for detecting high-grade CIN, which provides a better margin of safety in extending screening intervals . Most importantly, a recent cluster randomized trial ha s shown that HPV testing reduces cervicalcancer mortality to a greater extent than Pap cytology, a test for any candidate screening technology.
J Natl Cancer Inst 2010;102:1451–1453

Workshop GISCi L'Aquila giugno 2012

Workshop GISCi L'Aquila giugno 2012
Pertanto morfologia più test HPV con genotipizzazione
Ma se cambiassimo strategia fin dall’inizio?

Workshop GISCi L'Aquila giugno 2012
HPV group
Cytology group
p value
Screening round one
7 9 0.62
Screening round two
0 9 0.004
Total over first two rounds
7 18 0.028
NTCC - INVASIVE CERVICAL CANCER
Ronco et al. Lancet Oncol 2009





























