Embed Size (px)
Citation preview
IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 4, Apri l 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(4):37–40.www.ijcasereportsandimages.com
Giant cell tumour of the distal humerus treatedwith elbow arthroplasty: A case reportAzad Sait S, Manasseh Nithyanath, Vinoo M Cherian
ABSTRACTIntroduction: Giant cell tumour (GCT) of thedistal humerus is very rare and the treatmentdepends on the grade of the tumour. CaseReport: We present a 32yearold lady withGrade III GCT of the left distal humerustreated with en bloc excision and custom madetotal elbow replacement. Her preoperativeMayo Elbow Performance Score was 30. At 56months follow up, she is pain free with a MayoElbow Performance Score of 90 and noevidence of recurrence. Conclusion:Enneking’s staging and Campanacci’sradiographic grading helps in planning thetreatment. When the lesion has violated ajoint, en bloc excision followed byreconstruction or joint sacrifice is thetreatment of choice. The options ofreconstruction are auto or allografts, custommade endoprosthesis or allograftendoprosthetic composite. Reconstructionusing autograft is seldom feasible in elbow.
Allografts are met with high complicationrates. Custom made total elbow arthroplasty isa good option especially for primary tumoursof the elbow and can be done with goodoncologic safety. Custom made total elbowarthroplasty is a good option for CampanacciGrade III GCT of the elbow. It providesexcellent pain relief and good functionalimprovement with low complication rate.Keywords: Giant cell tumour, Elbow tumour,Elbow arthroplasty.
*********SA Sait, Nithyanath M, Cherian VM. Giant cell tumourof the distal humerus treated with elbow arthroplasty:A case report. International Journal of Case Reportsand Images 2012;3(4):37–40.
*********doi:10.5348/ijcri201204113CR10
INTRODUCTIONGiant Cell Tumour (GCT) of bone is a distinctclinicopathologic entity with distinguishing radiologicfeatures. Although approximately 6% of the GCTsaffect the humerus [1], GCT of the distal humerus israre. We present a case of distal humerus GCT whichhad breached the cortex and was successfully treatedwith custom made total elbow arthroplasty and wasprospectively followed up.
CASE REPORTThirty one year old house wife presented to us inMarch 2005 with complaints of swelling on the inner
CASE REPORT OPEN ACCESS
Azad Sait S1 , Manasseh Nithyanath2, Vinoo M. Cherian3
Affi l iations: 1Azad Sait S, Post Graduate Registrar,Department of Orthopaedics, Christian Medical College,Vellore, Tamil Nadu State, 2Manasseh Nithyanath,Associate Professor, Department of Orthopaedics,Christian Medical College, Vellore, Tamil Nadu State,3Vinoo M. Cherian, Professor, Department ofOrthopaedics, Christian Medical College, Vellore, TamilNadu State, India – 632004.Corresponding Author: Azad Sait S, Post GraduateRegistrar, Department of Orthopaedics, ChristianMedical College, Vellore, Tamil Nadu State, India –632004; Ph: 96292461 86; Fax: 41 6 228 2020;Email : azad_sait@rediffmail .com
Received: 29 July 2011Accepted: 1 4 November 2011Published: 30 Apri l 201 2
Sait et al. 37
IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 4, Apri l 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(4):37–40.www.ijcasereportsandimages.com
aspect of the left elbow for two years and pain for twomonths associated with decreased movements of theleft elbow. There was no history of trauma or systemicsymptoms. Her Activities of Daily Living were severelyaffected.Her general physical examination was withinnormal limits. Left elbow examination revealed a 5x4cm oval swelling on the medial and anteromedialaspect of distal humerus obscuring the joint line.Swelling was warm, tender, with well defined edges,smooth surface, firm consistency and immobile. Shehad a flexion deformity of 40 degrees with a furtherflexion up to 90 degrees limited by pain and spasm.Full supination and pronation were present. Her bloodinvestigations and chest radiographs were normal.Radiograph of the left elbow showed an eccentric lyticlesion of medial condyle of distal humerus which hadbreached the cortex. Mayo Elbow Performance Scorewas 30 at presentation. Bone scan showed intenseuptake in the medial condyle of the distal humeruswhile rest of the skeleton was normal. Biopsy from thelesion revealed uniform ovoid mononuclear cells withnumerous osteoclast type multinucleate giant cellswhich was consistent with GCT.She was treated with en bloc resection of the distalhumerus and custom made total elbow arthroplastyusing 316 L SS, constrained, hinged cementedprosthesis. Postoperative period was uneventful andshe was started on physiotherapy. Histopathologicexamination of the three excised specimen showed onecm tumor free margin proximally while distally thetumor had breached the cortex and involved the softtissues. She was prospectively followed up and on finalfollow up at 56 months she was pain free with flexionof 20110° and was able to carry out her personal andhouse hold works independently with a Mayo ElbowPerformance Score of 90. There was no evidence ofrecurrence or metastasis.
DISCUSSIONGCT represents 48% of primary bone tumours. Itis a locally aggressive benign bone tumour whichoccurs after the epiphyseal closure with a peak age ofincidence in the 3rd and 4th decades [2]. GCT has aslight female preponderance and this is more in thepaediatric and adolescent population [3].GCT commonly affects the long tubular bones; themost common sites being distal femur and proximaltibia, distal radius, and proximal humerus, suggestingthat in the lower extremity it tends to occur towardsthe knee; while in the upper extremity, away from theelbow [4]. Elbow per se is a rare site for primary bone
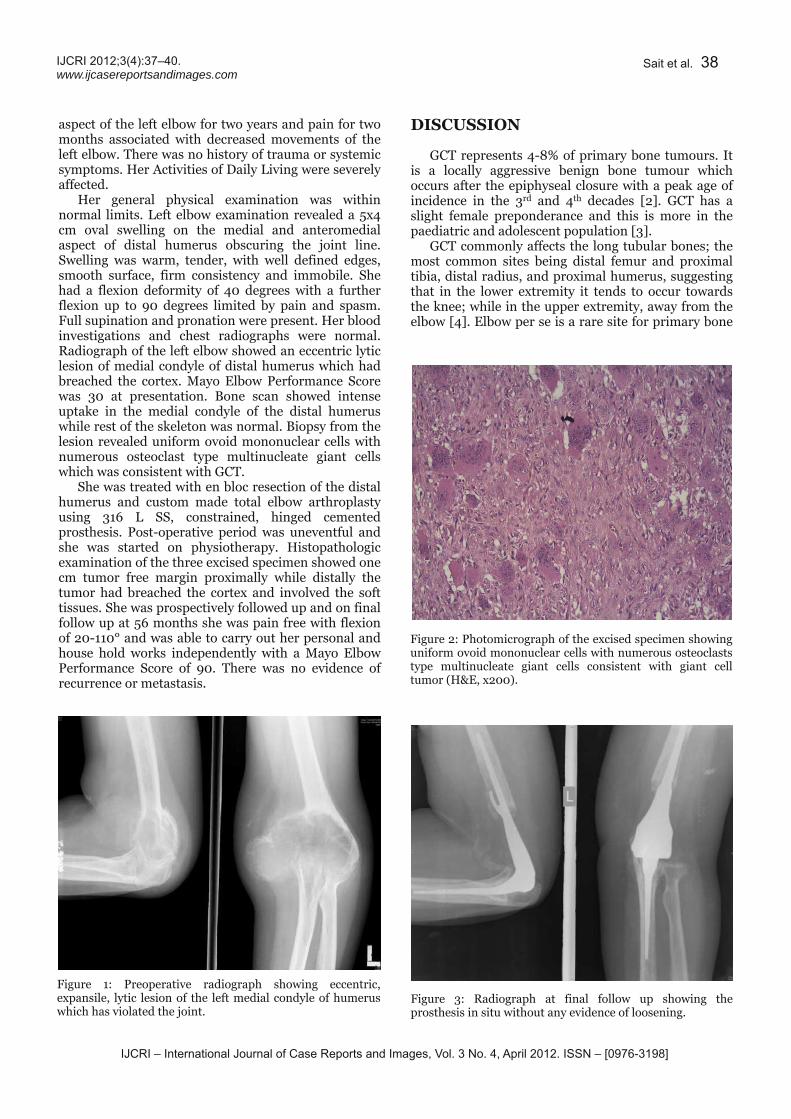
Figure 1: Preoperative radiograph showing eccentric,expansile, lytic lesion of the left medial condyle of humeruswhich has violated the joint.
Figure 2: Photomicrograph of the excised specimen showinguniform ovoid mononuclear cells with numerous osteoclaststype multinucleate giant cells consistent with giant celltumor (H&E, x200).
Figure 3: Radiograph at final follow up showing theprosthesis in situ without any evidence of loosening.
Sait et al. 38
IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 4, Apri l 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(4):37–40.www.ijcasereportsandimages.com
tumours. Only 1% of all primary bone tumours arise inthe distal humerus [5]. Thus GCT of the distalhumerus is a rarity.Enneking’s staging and Campanacci’s radiographicgrading helps in planning the treatment. It isimportant to stage the disease preoperatively with
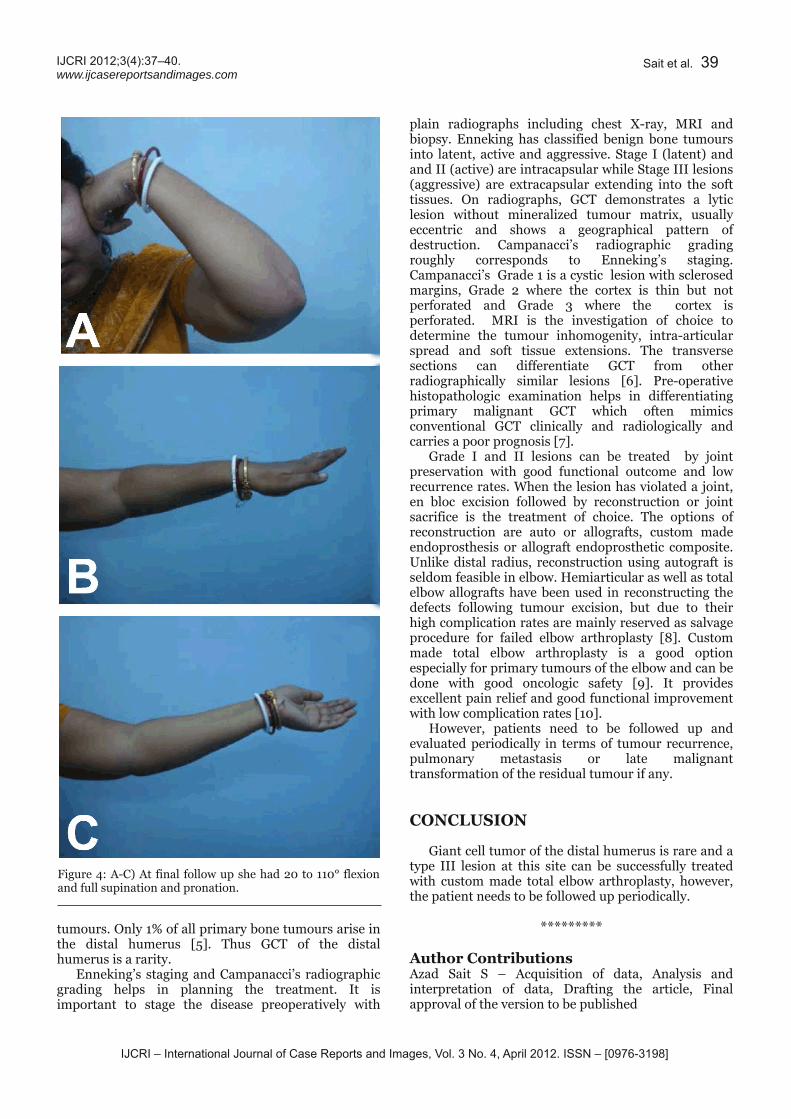
Figure 4: AC) At final follow up she had 20 to 110° flexionand full supination and pronation.
plain radiographs including chest Xray, MRI andbiopsy. Enneking has classified benign bone tumoursinto latent, active and aggressive. Stage I (latent) andand II (active) are intracapsular while Stage III lesions(aggressive) are extracapsular extending into the softtissues. On radiographs, GCT demonstrates a lyticlesion without mineralized tumour matrix, usuallyeccentric and shows a geographical pattern ofdestruction. Campanacci’s radiographic gradingroughly corresponds to Enneking’s staging.Campanacci’s Grade 1 is a cystic lesion with sclerosedmargins, Grade 2 where the cortex is thin but notperforated and Grade 3 where the cortex isperforated. MRI is the investigation of choice todetermine the tumour inhomogenity, intraarticularspread and soft tissue extensions. The transversesections can differentiate GCT from otherradiographically similar lesions [6]. Preoperativehistopathologic examination helps in differentiatingprimary malignant GCT which often mimicsconventional GCT clinically and radiologically andcarries a poor prognosis [7].Grade I and II lesions can be treated by jointpreservation with good functional outcome and lowrecurrence rates. When the lesion has violated a joint,en bloc excision followed by reconstruction or jointsacrifice is the treatment of choice. The options ofreconstruction are auto or allografts, custom madeendoprosthesis or allograft endoprosthetic composite.Unlike distal radius, reconstruction using autograft isseldom feasible in elbow. Hemiarticular as well as totalelbow allografts have been used in reconstructing thedefects following tumour excision, but due to theirhigh complication rates are mainly reserved as salvageprocedure for failed elbow arthroplasty [8]. Custommade total elbow arthroplasty is a good optionespecially for primary tumours of the elbow and can bedone with good oncologic safety [9]. It providesexcellent pain relief and good functional improvementwith low complication rates [10].However, patients need to be followed up andevaluated periodically in terms of tumour recurrence,pulmonary metastasis or late malignanttransformation of the residual tumour if any.
CONCLUSIONGiant cell tumor of the distal humerus is rare and atype III lesion at this site can be successfully treatedwith custom made total elbow arthroplasty, however,the patient needs to be followed up periodically.
*********Author ContributionsAzad Sait S – Acquisition of data, Analysis andinterpretation of data, Drafting the article, Finalapproval of the version to be published
Sait et al. 39
IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 4, Apri l 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(4):37–40.www.ijcasereportsandimages.com
Manasseh Nithyanath – Conception and design,Analysis and interpretation of data, Critical revision ofthe article, Final approval of the version to bepublishedVinoo M. Cherian – Conception and design, Analysisand interpretation of data, Critical revision of thearticle, Final approval of the version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestThe authours declare that they do not have anyfinancial interest or any conflict of interest exists.Copyright© Azad Sait S et al. 2012; This article is distributedunder the terms of Creative Commons attribution 3.0License which permits unrestricted use, distributionand reproduction in any means provided the originalauthors and original publisher are properly credited.(Please see www.ijcasereportsandimages.com/copyrightpolicy.php for more information.)
REFERENCES1. Vincent J, Vigorita, Bernard Ghelman, DouglasMintz. Orthopaedic Pathology. Second Edition.China: Lippincott Williams & Wilikins 2006:282.2. Karpik M. Giant Cell Tumor (tumorgigantocellularis, osteoclastoma) epidemiology,diagnosis, treatment. Ortop Traumatol Rehabil2010 Jun;12(3):207–5.3. Puri A, Agarwal MG, Shah M, Jambhekar NA,Anchan C, Behle S. Giant cell tumor of bone inchildren and adolescents. J Pediatr Orthop 2007Sep;27(6):635–9.4. Moser RP Jr, Kransdorf MJ, Gilkey FW, ManasterBJ. From the archives of the AFIP. Giant celltumor of the upper extremity. Radiographics 1990Jan;10(1):83–102.5. Kulkarni A, Fiorenza F, Grimer RJ, Carter SR,Tillman RM. The results of endoprostheticreplacement for tumours of the distal humerus. JBone Joint Surg Br 2003 Mar;85(2):240–3.6. Woertler K. Benign bone tumors and tumorlikelesions: value of crosssectional imaging. EurRadiol 2003 Aug;13(8):1820–35.7. Bertoni F, Bacchini P, Staals EL. Malignancy ingiant cell tumor of bone. Cancer 2003 May15;97(10):2520–9.8. Kharrazi FD, Busfield BT, Khorshad DS, HornicekFJ, Mankin HJ. Osteoarticular and total elbowallograft reconstruction with severe bone loss.Clin. Orthop. Relat. Res2008 Jan;466(1):205–9.9. Tang X, Guo W, Yang R, Tang S, Yang Y. Custommade prosthesis replacement for reconstruction ofelbow after tumor resection. J Shoulder ElbowSurg 2009 Oct;18(5):796–803.
10. Sperling JW, Pritchard DJ, Morrey BF. Total elbowarthroplasty after resection of tumors at the elbow.Clin. Orthop. Relat. Res 1999 Oct;(367):256–1.
Sait et al. 40