Embed Size (px)
Citation preview

1656 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
Genomics and Targeted Therapies in Gastroesophageal Adenocarcinoma Ankur K. Nagaraja 1 , Osamu Kikuchi 1 , and Adam J. Bass 1 , 2 , 3
REVIEW
ABSTRACT Gastroesophageal adenocarcinomas (GEA) are devastating diseases with stark global presence. Over the past 10 years, there have been minimal improvements
in treatment approach despite numerous clinical trials. Here, we review recent progress toward understanding the molecular features of these cancers and the diagnostic and therapeutic challenges posed by their intrinsic genomic instability and heterogeneity. We highlight the potential of genomic heterogeneity to infl uence clinical trial outcomes for targeted therapies and emphasize the need for comprehensive molecular profi ling to guide treatment selection and adapt treatment to resistance and genomic evolution. Revising our clinical approach to GEA by leveraging genomic advances will be integral to the success of current and future treatments, especially as novel targets become therapeu-tically tractable.
Signifi cance: GEAs are deadly cancers with few treatment options. Characterization of the genomic landscape of these cancers has revealed considerable genetic diversity and spatial heterogeneity. Understanding these fundamental properties of GEA will be critical for overcoming barriers to the development of novel, more effective therapeutic strategies.
1 Department of Medical Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts . 2 Division of Molecular and Cel-lular Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts. 3 Broad Institute of MIT and Harvard, Cambridge, Massachusetts. Corresponding Author: Adam J. Bass, Dana-Farber Cancer Institute, 450 Brookline Avenue, Dana 810B, Boston, MA 02215. Phone: 617-632-2477; Fax: 617-582-9830; E-mail: [email protected] Cancer Discov 2019;9:1656–72 doi: 10.1158/2159-8290.CD-19-0487 ©2019 American Association for Cancer Research.
INTRODUCTION Stomach and esophageal cancers are the third and sixth
most common causes of cancer mortality worldwide, respec-tively, and together are responsible for more than 1.2 million deaths ( 1 ). These two cancers were once considered distinct diseases plainly separated into adenocarcinomas in the stom-ach and squamous cell carcinomas in the esophagus. However, recent decades have witnessed a shift in the epidemiologic and anatomic patterns of these cancers, contributing to a revised and evolving understanding of their classifi cation and pathogenesis. The worldwide incidence of gastric cancer has been declining for at least 40 years ( 2 ). Nevertheless, there are more than one million new cases annually, with the majority occurring in Eastern Asia ( 1 ). In North America and Western Europe, cancers of the distal stomach, typically associated with Helicobacter pylori ( H. pylori ) infection, have decreased dramati-cally ( 3 ). In contrast, there is a rising incidence of cancers of the
proximal stomach, directly adjacent to the esophagus ( 3 ). This rise in the stomach parallels an alarming increase in adenocar-cinomas of the lower esophagus and gastroesophageal junc-tion (GEJ). Key risk factors include gastroesophageal refl ux disease and obesity. Both gastric and esophageal adenocarci-nomas commonly emerge with intestinal metaplasia, which can result from chronic infl ammatory stimuli. The shared epidemiology, pathology, and genomic and molecular features of these adenocarcinomas suggest the common pathophysiol-ogy of esophageal and proximal gastric adenocarcinomas ( 3, 4 ). Indeed, The Cancer Genome Atlas (TCGA) has revealed defi ni-tive genomic overlap between gastric and esophageal adenocar-cinomas, and absolute molecular distinction from squamous cell carcinomas of the upper and mid-esophagus ( 5, 6 ). This review will focus on gastroesophageal adenocarcinomas (GEA); additional information on the genomics of esophageal squa-mous cell carcinomas (ESCC) can be found in ref. 6 .
In addition to the rising incidence of esophageal, GEJ, and proximal gastric adenocarcinomas, another epidemiologic trend involves an increase in cancers of the gastric corpus or body (and fundus, to a lesser extent), predominantly in non-Hispanic white women younger than 50 years old, and restricted to areas with less than 20% poverty ( 7–9 ). Whereas the current gastric cancer male:female incidence rate ratio for patients ages 60 to 74 years is 2.5, the ratio is 1.0 for patients ages 25 to 29 years ( 7 ). It has been estimated that if the upward trend in early-onset disease continues, by 2030 overall gastric cancer incidence will be increasing, and female incidence will surpass male incidence ( 7 ). The histologic and molecular subtypes of these “CYF” (corpus-dominant, young
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1657
age-dominant, female-dominant) gastric cancers have not been reported, and their risk factors are unknown, though they may be rooted in the evolving gastric microbiome in the wake of H. pylori decline, and/or linked to autoimmunity and reproductive factors (7, 8).
GEAs have dismal outcomes, with cumulative five-year relative survival of 21% to 31% in the United States (10, 11). Five-year relative survival for those with locoregional gastric cancer (31%–67%) is far inferior to that for colorectal cancer (70%–91%; ref. 10), indicating that later diagnosis alone does not account for these poor outcomes. GEAs also have substantial propensity for early spread of disease, and systemic therapy for disseminated disease remains woefully inadequate, with 5-year relative survival of 5% (10). The convergence of a new molecularly based classification, recent genomic insight into drivers of GEA pathogenesis, and an imperative clinical need make this an opportune time to address how our emerging understanding of GEA can ulti-mately be translated into new therapeutic strategies.
DISEASE CLASSIFICATION IN THE PREGENOMIC ERA
Fifty years ago, the Lauren classification subtyped gas-tric cancers into intestinal, diffuse, and indeterminate/mixed histologies (12). Intestinal-type tumors are most common, consisting of cohesive cells in glandular formations, often associated with intestinal metaplasia and H. pylori infection. Diffuse-type tumors have noncohesive scattered cells, some-times with signet-ring features, that tend toward peritoneal dissemination due to locally invasive properties. The World Health Organization (WHO) further refines the histologic classification of gastric cancer into tubular, papillary, muci-nous, poorly cohesive (including Lauren diffuse type), and mixed variants. Most esophageal adenocarcinomas (EAC) resemble intestinal-type gastric cancer, especially given their evolution from intestinal metaplasia. To date, these histo-logic classifications have not appreciably affected clinical care, including the selection of systemic agents. Another classification, the Siewert classification, is focused on refined anatomic staging of GEJ adenocarcinomas to guide surgical approaches (13). Beyond histologic and anatomic types, it is also worth noting that there have been long-standing debates regarding the comparative features of GEA in the Asian and Western populations. Asian patients, beyond having higher rates of gastric cancer, tend to have more distal gastric tumors associated with H. pylori, and less predilection toward GEJ dis-ease and adenocarcinomas of the tubular esophagus, or its antecedent, Barrett’s esophagus (14–16). Although extensive discussion of the comparisons of Eastern/Western tumors is beyond the scope of this review, early data have pointed to the genomic similarity of these tumors (17), but potential distinctions in their tumor–immune microenvironment (18).
MOLECULAR CLASSIFICATION IN THE GENOMICS ERA
The Lauren and WHO classifications are basic descriptors for the microscopic organization of gastric tumors. However, they offer no immediate scientific insight into the inner
workings of a cancer cell, nor clinical insight into rational systemic therapeutic strategies. In recent years, new genomic technologies have enabled groundbreaking studies that have revolutionized our understanding of the genomic composi-tion of GEA, ultimately providing a framework for molecular classification and new leads for therapeutic development. Pivotal studies have been led by TCGA, the Asian Cancer Research Group (ACRG), and the Oesophageal Cancer Clini-cal and Molecular Stratification (OCCAMS) Consortium (5, 6, 19, 20). Among these, ACRG focused on gastric adenocar-cinoma at a South Korean medical center, OCCAMS focused on EAC in a Western European population, and the TCGA studied both adenocarcinoma and squamous cell carcinoma spanning the stomach and esophagus using a diverse interna-tionally derived sample collection.
Within TCGA, the first published analysis included 295 gastric adenocarcinomas, inclusive of GEJ tumors, using the tools standard to TCGA-led studies: array-based somatic copy-number analysis, whole-exome sequencing, array-based DNA methylation profiling, mRNA sequencing, miRNA sequencing, and reverse-phase protein array (5). Four dis-tinct molecular subtypes of gastric cancer emerged from integration of these data: Epstein–Barr virus (EBV)–positive (8.8%), microsatellite-unstable (MSI; 21.7%), genomically stable (GS; 19.7%, enriched for Lauren diffuse type), and tumors with chromosomal instability (CIN; 49.8%; Fig. 1). In comparison with the TCGA classification, where underly-ing somatic genomic processes were central to development of the classifier, ACRG developed a classification into four groups based on array-based gene-expression profiling of 300 gastric adenocarcinomas: MSI (22.7%), microsatellite sta-ble with epithelial-to-mesenchymal transition (MSS/EMT; 15.3%), MSS/TP53+ (26.3%), and MSS/TP53− (35.7%; ref. 19). Applying the TCGA classifiers to the ACRG tumors showed the expected concordance in MSI tumors. The MSS/EMT class was enriched in diffuse-type tumors classified as GS by TCGA, and MSS/TP53+ was enriched for EBV+ tumors. A key difference was that all four ACRG subtypes had CIN tumors, with the highest proportion of CIN tumors in MSS/TP53−. The ACRG analysis demonstrated inferior survival among the MSS/EMT+ group. Although no survival associations were seen in the TCGA study, potentially owing to the thera-peutic heterogeneity of the internationally diverse sample set, subsequent studies applying the TCGA classes to two large independent cohorts demonstrated that EBV+ tumors have superior survival and GS tumors have inferior survival (21). Major genomic features of these molecular subtypes are discussed below.
Although the second TCGA study was nominally an analy-sis of esophageal cancer, this study evaluated both ESCC and EAC with the entire gastric cancer dataset in an effort to address debates regarding the comparative features of EAC, GEJ, and gastric tumors (6). As would be predicted by studies in other cancer types, the TCGA analysis identi-fied systematic differences between squamous cell carcinoma and adenocarcinoma across all molecular platforms. Indeed, these data robustly argued that high-level histologic clas-sifications transcended the organ of origin. Whereas ESCCs clustered more strongly with head and neck SCCs than with EACs, EACs were more similar to gastric tumors than
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1658 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
to ESCCs. More subtle analysis refined the comparison of EAC with gastric cancer, noting that EAC showed the most similarity to the CIN class of gastric cancer. Furthermore, a joint analysis of GEA showed an anatomic gradient, with the proportion of CIN tumors increasing proximally such that 71 of 72 tumors categorized as definitively esophageal based on anatomic location and presence of Barrett’s esophagus were CIN tumors. Although specific methylation patterns were enriched in EACs relative to distal gastric cancers, multiple analyses attempting to differentiate the molecular features of CIN tumors of the stomach and esophagus failed to dichoto-mize these cancers. Still, several somatic features were differ-entially distributed between EACs and gastric cancers. EACs have fewer APC mutations, suggesting less WNT depend-ence or alternate means of activating WNT signaling, and higher frequency of RUNX1 deletion and VEGFA and MYC amplifications. Intriguingly, new studies from the OCCAMS
Consortium found that patients with EAC with synchro-nous Barrett’s esophagus had better survival compared with patients without evident Barrett’s esophagus (22), suggesting that the most aggressive tumors might outstrip the potential for Barrett’s esophagus to take hold in the lower esophagus. Although the TCGA study did not define subgroups within EAC, whole-genome sequencing by OCCAMS suggests that mutational signatures may inform targeted therapy (23).
Together, these studies directly inform our broader view of gastroesophageal cancer. The dramatic and consistent separation of adenocarcinoma and squamous cell carcinoma clearly challenge prior notions of treating esophageal cancer as a single entity. Although still debated, these data also sug-gest the field should transition to viewing GEA more holisti-cally, especially for the CIN class of tumors. These data also indicate that any previous effort to compare gastric adenocar-cinoma and EAC, or to compare Eastern and Western gastric
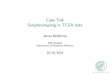
Figure 1. Molecular classification of GEA. Key features of the four TCGA subtypes of GEA spanning the lower esophagus to the distal stomach. Frequencies at each anatomic location are from ref. 6.
• Most common subtype • Increasing incidence • Increasing gradient from distal to proximal stomach • TP53 mutations • Whole-genome doubling • RTK/RAS/cell-cycle gene amplifications (e.g., ERBB2, EGFR, KRAS, CCNE1, CCND1/2/3, CDK6) • VEGFA amplification common in EAC
• Hypermethylation • CDKN2A silencing • PIK3CA, ARID1A, BCOR mutations • PD-L1/2 overexpression • Prominent immune signatures • Sensitive to immune checkpoint blockade
CIN: Chromosomal instability
EBV : Epstein–Barr virus
• Most are Lauren diffuse type • Non-cohesion, invasion, dissemination • CDH1 and RHOA mutations • CLDN18–ARHGAP26/6 fusions
GS: Genomically stable
• Hypermutation • Hypermethylation • MLH1 silencing • ARID1A, RNF43, PIK3CA, KRAS mutations • Elevated immune signatures • Sensitive to immune checkpoint blockade
MSI: Microsatellite instability
PYLORUS
ANTRUM
BODY
FUNDUSGEJ/CARDIA
LOWERESOPHAGUS/
GEJ
A
B
C
D
47.6%
27.3%
3.5%
21.7%
47.9%
13.6%
19.3%
19.3%
100%
74.6%
9.5%
6.3%
9.5%
A B C D
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1659
cancers, had an unrecognized confounding by subtype, as CIN tumors are dominant in the esophagus and GEJ (and more prevalent in the West) compared with distal stomach tumors (more prevalent in the East) where GS/diffuse, MSI, and EBV+ are more common. Although the anatomic gradi-ents of molecular subtypes and molecular features could be used to argue firmer separation of cancers in the anatomic esophagus or stomach, it is notable that such gradients are present within analogous diseases such as colorectal cancer, where methylation and MSI are more prevalent in the ascend-ing colon and CIN more common in the distal colon and rectum. For the purpose of this review and the discussion of biologically driven therapies, we will treat CIN GEA as a sin-gle category given the consistent overlap in oncogenic drivers and other molecular features.
CINCIN tumors are the predominant form of GEA. Half of
gastric antrum/pylorus tumors classify as CIN, and this pro-portion increases proximally according to the aforementioned gradient such that nearly all EACs are CIN (6). Although a firm definition of CIN has yet to be established, CIN tumors are characterized by extensive aneuploidy and lack the somatic hypermutation seen in MSI tumors. Although the term CIN has been applied to many cancers to describe the state of harboring frequent gross structural chromosomal aberrations and aneuploidy, the CIN present within GEAs is overwhelm-ingly associated with widespread focal events (i.e., less than half the chromosome arm length), especially recurrent focal amplifications at numerous oncogenic loci (24, 25).
A meta-analysis of TCGA data spanning GEA and colo-rectal cancer detailed the differential features of CIN in these diseases (25). In this report, a score was developed to subclassify CIN tumors based on high-amplitude focal amplifications (CIN-F) or low-amplitude broad amplifica-tions (CIN-B). This analysis revealed a dramatic distinction between GEA and colorectal cancer, as 75% of CIN GEA tumors are CIN-F, in contrast to only 25% of CIN colorectal cancer. These data correspond to the discrepant patterns of oncogene activation in these tumors, with amplifications predominant in GEA, and mutations, chiefly RAS, prevalent in colorectal cancer.
Within GEA, CIN-B tumors sustain more frequent somatic activating mutations of receptor tyrosine kinases (RTK) and RAS oncogenes, and inactivation of tumor suppressors in cell-cycle, WNT, and TGFβ pathways. CIN-F GEAs frequently harbor amplifications of RTKs, RAS, and cell-cycle genes. TP53 mutations are more common in CIN-F tumors (76% as compared with 54% of CIN-B tumors), as is whole-genome doubling (68% vs. 42%). These somatic features of the more prevalent CIN-F GEAs suggest distinct pathogenesis whereby a TP53-null cell may undergo genome doubling to an unstable tetraploid intermediate, which is then prone to catastrophic genomic events leading to transformation, as has been pos-ited from studies of the evolution of Barrett’s esophagus (26, 27). Indeed, this pattern is consistent with what has been observed via whole-genome sequencing of these cancers (28).
The etiologies for the distinct genomic pathways of can-cer development and the marked differences of the CIN
phenotype between GEA and colorectal cancer have not been established. A specific mutational signature of A>C transver-sions at AA dinucleotides has been observed in GEAs (20, 29) and is associated with the CIN-F phenotype (25). Although the etiology of this signature remains unresolved, it has been posited to be caused by oxidative damage (30) and associated with greater inflammatory infiltrates in EAC (23). Intrigu-ingly, this signature has been reported in colorectal cancer associated with inflammatory bowel disease (IBD; ref. 31). As IBD-associated colorectal cancers also resemble CIN GEA in their relative paucity of APC mutations and greater preva-lence of oncogene activation via amplification, these data raise the hypothesis that inflammation may contribute to the patterns of genomic evolution in GEA.
As explored in greater depth below, the pattern and puta-tive mechanisms of the predominantly focal CIN seen in GEA have definite implications for optimal therapy. Beyond the need to evaluate and target amplified rather than mutant oncoproteins, numerous studies have documented the genomic complexity and heterogeneity of oncogene profiles in GEA (23, 32–35). These features include both transforma-tion leading to cancer cells with multiple driving mitogenic oncogenes (e.g., cancer cells with coamplification of ERBB2 and MET) as well as heterogeneous tumors where distinct driving amplified oncogenes are present in distinct subclones of tumors. Either case poses a clear challenge to simple tar-geted therapy approaches, likely contributing to the failure of many such therapies in GEA.
GSGS tumors are most prevalent in the antrum/pylorus and
fundus/body (5). The origin of the GS nomenclature in TCGA followed their lack of CIN, MSI/hypermutation, and the hypermethylation found in EBV+ tumors (5). Seventy percent are Lauren diffuse type, a histology that is enriched in the estimated 10% to 15% of patients who develop gastric cancer prior to 45 years of age (36, 37). Diffuse gastric cancers are also enriched in Alaska Natives and Hispanics compared with non-Hispanic whites (38, 39). The most characteristic somatic features of GS tumors are CDH1 (E-cadherin) loss-of-function mutations in 30% (25); notably, this gene is also responsible for hereditary diffuse gastric cancer when altered in the germline (40). In families without altered CDH1, muta-tions have been described in CTNNA1, which functions in the same complex as E-cadherin; in DNA-repair genes such as PALB2, BRCA1, BRCA2, RAD51C, and ATM; and in MSR1 and STK11 (40–42). A proteomic analysis of 84 pairs of dif-fuse gastric cancer and adjacent normal tissue identified three subtypes, in order of worsening overall survival (OS): PX1, characterized by cell-cycle dysregulation; PX2, enriched in EMT pathways; and PX3, comprised of immune response proteins (43). It remains to be seen whether this classification translates clinically beyond prognostic stratification.
Beyond CDH1, the most notable constellation of genomic findings in these cancers relates to the RHO pathway. Highly recurrent missense mutations in the RHOA GTPase were identified contemporaneously by three groups in 2014 (5, 44, 45). Although missense mutations cluster in the amino-terminal GTPase domain, studies on the activity of these
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1660 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
mutations are mixed, with data supporting a mechanistic gain-of-function but also attenuation of the GTP loading of RHOA, a proxy for its activation. Intriguingly, the most recur-rent RHOA mutation is in the highly conserved core effector region at codon Y42. This residue is analogous to HRAS Y40, where mutations selectively modulate specific down-stream effects of HRAS (46). Aside from RHOA, recurrent fusion genes have been identified which include nearly the entire coding sequence of the transmembrane tight junction protein CLDN18 fused by its cytoplasmic tail to the RHO GTPase–activating proteins ARHGAP26 or ARHGAP6 (5, 47). Intriguingly, the CLDN18–RHOGAP fusions are mutually exclusive with both CDH1 and RHOA alterations, suggesting this fusion may modulate both cellular adhesion and the RHO pathway in gastric cancer pathogenesis. Moreover, given the roles of these genes in cell adhesion and motility, their unique recurrence in this disease suggests clear connection with a tumor phenotype characterized by noncohesion, inva-sion, and dissemination.
From a therapeutic perspective, the GS/diffuse gastric cancer population remains a vexing problem. As suggested by the more mesenchymal nature of these tumors, standard cytotoxic chemotherapeutic agents may be less active in these patients (21, 48). Coupled to the paucity of classic targetable oncogenes and the propensity for invasion and metastasis, this disease carries a dismal prognosis, as documented by the ACRG study (19). Deeper mechanistic inquiry aiming to define vulnerabilities of these cancers is a substantial priority within the GEA field.
MSIMSI tumors arise in the distal stomach in the antrum/
pylorus and fundus/body. Within the TCGA project, MSI tumors were not observed in the esophageal lineage despite the enrichment of hypermethylation in EAC (6). Clinically, MSI is a favorable prognostic factor in resectable primary gas-tric cancer (49). Post hoc exploratory analyses of the MAGIC and CLASSIC trials suggest that in contrast to MSS patients, who benefit from the addition of adjuvant or perioperative chemotherapy, MSI patients demonstrate better outcomes with surgery alone, and the addition of chemotherapy may have a detrimental effect in MSI patients (50–52). These data suggest that MSI tumors may be intrinsically chemoresistant, or that chemotherapy blunts the robust immune response stimulated by these hypermutated tumors. However, these observations have yet to be validated through prospective clinical trials.
As in colorectal cancer, MSI gastric adenocarcinomas typi-cally occur following MLH1 silencing in the presence of a DNA hypermethylation phenotype, or less commonly MLH1 or MSH2 mutations, leading to defective DNA mismatch repair resulting in insertion/deletion events and single- nucleotide variants (SNV). Numerous other genomic fea-tures of MSI gastric cancers resemble MSI colorectal cancer, including ARID1A, RNF43, PIK3CA, and KRAS mutations (25). Strikingly, however, the classic BRAFV600E mutations that frequently occur in sporadic MSI colorectal cancer with DNA hypermethylation are notably absent in MSI gastric cancer despite otherwise highly similar DNA methylation patterns
(5, 25). Perhaps most importantly, MSI tumors exhibit high gene-expression scores for IFNγ signaling, CD8+ T cells, and M1 macrophages, second only to EBV+ tumors, highlighting their immunogenicity (25, 53). As in other tumors with MSI, immune checkpoint blockade has demonstrated efficacy in this population (54, 55). Beyond MSI, there are also rare tumors with hypermutation not due to mismatch repair but secondary to POLE mutations. These tumors demonstrate a high frequency of SNVs, yet without the insertion/deletion events observed in MSI cancers (25). Unlike MSI tumors, these hypermutated SNV tumors do not display elevated immune signatures (25).
EBV+
EBV+ tumors localize to the fundus/body and proximal stomach and are notable for their marked DNA hypermethyl-ation. Indeed, these tumors harbor more DNA hypermethyla-tion than any other class of cancer in the TCGA collection (5). EBV+ gastric tumors epigenetically silence CDKN2A, similar to many CIN GEAs, but infrequently harbor TP53 mutation or CIN (5, 25). EBV+ gastric cancers have long been recognized to have strong lymphoid infiltration, leading to the term “lymphoepithelioma-like carcinoma” on histologic analy-sis. Accordingly, focused molecular analysis of these tumors noted prominent immune signatures (5, 53). Genomic analy-sis also identified recurrent 9p24.1 amplification at the loci of genes encoding PD-L1, PD-L2, and JAK2, consistent with elevated expression of these genes (5), an event that parallels the presence of this amplification recurrently in EBV-associ-ated lymphoid cancers (56). JAK2 transcriptionally activates both PD-1 ligands in lymphoma models (56). Moreover, EBV infection alone can induce PD-L1 expression independent of 9p24.1 amplification (57). This confluence of immune features imparts sensitivity to immune checkpoint blockade, as observed by the impressive response rates in lymphomas with 9p24.1 amplification and in EBV+ lymphomas (58), and more recently, in EBV+ gastric cancers (55). Beyond immuno-therapy, somatic analysis has also revealed highly recurrent PIK3CA-activating mutations and mutations in ARID1A and BCOR (5, 25). Thus, EBV status provides key guidance for prioritizing an immunotherapeutic approach, and raises intriguing possibilities about the utility of PI3K pathway inhibitors and DNA-demethylating agents in these cancers.
TARGETED THERAPY IN THE PRECISION MEDICINE ERA: ERBB2 AS A CAUTIONARY TALE
Given the paucity of targets in GS/diffuse gastric cancer and the exciting results with immunotherapy in MSI/EBV+ disease, the bulk of this review will discuss issues revolving around tar-geted molecular therapy for the most common subtype, CIN GEA, especially in the Western-predominant proximal gastric/ GEJ/EAC cancers. The genomic characterization of CIN GEA has unveiled a multitude of candidate oncogenic drivers that may be potential biomarkers for targeted therapies, most prominently RTKs. The poster child for this paradigm shift to precision medicine in GEA was amplification of ERBB2, which occurs in 15% to 20% of GEA (5, 6, 25). The ToGA trial
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1661
demonstrated an OS benefit with the addition of the ERBB2 mAb trastuzumab to chemotherapy for patients with advanced or metastatic gastric and GEJ cancers (13.8 vs. 11.1 months, P = 0.0046; ref. 59). The survival benefit climbed to 4.2 months in the subset of patients with higher ERBB2 levels (59, 60), com-parable to the effect of trastuzumab in patients with ERBB2+ metastatic breast cancer (61). These data led to its widespread regulatory approval and adoption in clinical practice. Although it is not FDA-approved in EAC with ERBB2 amplification, these patients are also routinely treated per the ToGA results.
Unfortunately, in stark contrast to breast cancer, the thera-peutic efficacy of ERBB2-directed agents in GEA has not extended beyond first-line trastuzumab plus chemotherapy. Several successful FDA-approved agents for ERBB2+ breast cancer have failed in large phase III trials in GEA (Table 1). The addition of pertuzumab, a mAb that blocks ERBB2 heterodi-merization with other ERBB family receptors, to trastuzumab plus chemotherapy in the first-line setting did not signifi-cantly improve OS for ERBB2+ metastatic gastric or GEJ can-cer in the JACOB trial, although it trended toward a positive result (62). Importantly, major pharmacokinetic differences in pertuzumab between ERBB2+ gastric and breast cancers were identified and adequately addressed through a phase IIa dose-finding study ( JOSHUA) prior to JACOB and confirmed by pharmacokinetic assessments of JACOB participants (63, 64). T-DM1, an antibody–drug conjugate of trastuzumab and a microtubule inhibitor, was not superior to taxane in the sec-ond-line setting in the GATSBY trial (65). Both the TRIO-013/LOGiC and TyTAN trials also failed to meet their primary endpoint of OS for the dual ERBB2/EGFR kinase inhibitor lapatinib combined with chemotherapy as first- or second-line treatment, respectively (66, 67). A preplanned subgroup analysis in the LOGiC study did show a significant OS benefit in Asian patients and in younger patients, and in the TyTAN study, patients with ERBB2 immunohistochemistry (IHC) 3+ had significantly improved OS, highlighting the importance of refining patient selection, fine-tuning the definition of biomarker positivity, and designing more effective targeted approaches for GEA with ERBB2 amplification.
Several emerging ERBB2 agents have shown encouraging efficacy in early-phase clinical trials. These new drugs include antibodies that direct a payload to ERBB2+ cells and those that are optimized to enhance immunologic attack against the cancer cell following binding of the antibody to ERBB2. A phase I study of trastuzumab deruxtecan (DS-8201), a humanized anti-ERBB2 antibody conjugated to a topoisomer-ase I inhibitor payload, demonstrated objective responses in 19 of 44 patients with advanced unresectable or metastatic ERBB2+ gastric/GEJ tumors, all of whom were previously treated with trastuzumab (68). Margetuximab (MGAH22) is a monoclonal antibody that binds the same epitope of ERBB2 as trastuzumab, but with an altered Fc domain that enhances binding to the CD16A receptor on natural killer cells and macrophages to boost antibody-dependent cell-mediated cytotoxicity. A phase I study showed good toler-ability and cytotoxic activity against ERBB2+ advanced solid tumors, including partial responses in 2 of 20 patients with GEA (69). A phase I/II study of margetuximab plus pembroli-zumab for the second-line treatment of patients with ERBB2+ GEA (post-trastuzumab) is ongoing (NCT02689284; ref. 70).
Although these newer agents offer some optimism, it is critical to assess the potential reasons why patients progress on first-line trastuzumab-based therapy and to understand why many agents that have been successful in breast cancer fail in GEA. Potential differential features of GEA and breast cancer may include fundamental lineage-related cancer cell pathophysiology, as well as more clearly delineated distinc-tions in somatic genomic patterns such as the extent of spatial heterogeneity (Fig. 2). In intralesion heterogeneity, individual oncogenes may be uniquely amplified in distinct subclones of the same tumor, or different oncogenes may be co-amplified within the same cancer cell. Compared with breast cancers, gastroesophageal cancers have more intrale-sion heterogeneity of ERBB2 expression and amplification as observed by IHC and multiregion next-generation sequencing (NGS) of primary tumors (35, 71). This intralesion heteroge-neity has direct therapeutic implications. First, the degree of ERBB2 amplification by NGS correlates with the benefit from trastuzumab (34), possibly serving as a measure of ERBB2 dependence in the tumor. Second, trastuzumab resistance has been observed to be commonly mediated by the rise of a non–ERBB2-amplified clone (34, 72). Although it is often referred to as “loss” of ERBB2, this situation more likely reflects preex-isting heterogeneity and the selection of ERBB2-negative sub-clones during trastuzumab therapy. This phenomenon might have contributed to the failure of second-line T-DM1 in the GATSBY trial, where more than 75% of patients had already progressed on trastuzumab and patients were not rebiopsied to evaluate ERBB2 status prior to randomization (65, 73).
Genomic analysis has demonstrated that more than half of ERBB2-amplified GEA tumors have concomitant baseline genomic alterations that may contribute to intrinsic tras-tuzumab resistance, including activating mutations in the PI3K pathway and amplifications of CCNE1, CDK6, EGFR, and MET, in line with the focal CIN pattern characteristic of these tumors (32, 34, 74, 75). As observed by the OCCAMS Consortium, this phenomenon of genomic co-amplification in GEA holds not only for ERBB2 but for other RTKs too (23). Moreover, genomic analysis demonstrated that patients with GEA with ERBB2 amplification and co-occurring lesions had inferior survival, especially when compared with those with the highest level of ERBB2 amplification by NGS (34). Preclinical studies suggest that dual blockade of multiple kinases present in GEA can overcome resistance to single-drug therapy, results confirmed clinically (23, 32, 33, 76). For example, a phase II study of afatinib in trastuzumab-resistant ERBB2+ GEA demonstrated an association between afatinib response and tumors harboring dual amplification of ERBB2 and EGFR (76), suggesting that combined targeting of ERBB2 and specific co-occurring genomic alterations may be essen-tial for therapeutic efficacy.
Perhaps even more striking than evolution of the tumor to an ERBB2-negative state upon trastuzumab therapy, gas-troesophageal cancers also demonstrate extensive baseline discordance in ERBB2 status between synchronous primary tumors and metastases prior to systemic therapy, in contrast to breast cancers that are ERBB2 concordant in more than 90% of cases (35). This interlesion heterogeneity suggests that the field should revisit the guidelines for assessment of ERBB2 status in GEA, which recommend testing of only a
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1662 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
Table 1. Key clinical trials for GEA
TargetTrial (reference) Phase Line of therapy Treatment ORR (%)
Median OS (months)
Median PFS (months)
HER2 ToGA ( 59 ) III 1L, HER2+ Cisplatin/fl uoropyrimidine + trastuzumab
47 13.8 6.7
Cisplatin/fl uoropyrimidine 35 11.1 5.5 P = 0.0046
HER2 JACOB ( 62 ) III 1L, HER2+ Chemotherapy + trastu-zumab + pertuzumab
57 17.5 8.5
Chemotherapy + trastuzumab
48 14.2 P = 0.057 NS
7
HER2 TRIO-013/LOGiC ( 66 )
III 1L, HER2+ CapeOx + lapatinibCapeOx
5339
12.210.5
65.4
P = 0.3492 NS
HER2 TyTAN ( 67 ) III 2L, HER2+ Paclitaxel + lapatinib 27 11.0 5.4Paclitaxel 9 8.9 4.4
P = 0.1044 NS
HER2 GATSBY ( 65 ) II/III 2L, HER2+ T-DM1 21 7.9 2.7Paclitaxel or docetaxel 20 8.6 2.9
P = 0.86 NS
EGFR EXPAND ( 85 ) III 1L Cisplatin/capecitabine + cetuximab
30 9.4 4.4
Cisplatin/capecitabine 29 10.7 5.6 P = 0.32 NSprimary endpoint
EGFR REAL3 ( 86 ) III 1L EOC + panitumumab 46 8.8 6EOC 42 11.3 7.4
P = 0.013 NSEGFR COG ( 87 ) III 2L Gefi tinib 2.7 3.7 1.6
Placebo 0.4 3.7 1.2 P = 0.29 NS
MET METGastric ( 94 )
(early termi-nation)
III 1L, MET+, HER2- mFOLFOX6 + onartuzumabmFOLFOX6
4641
11.011.3 P = 0.24 NS
6.76.8
HGF RILOMET-1 ( 96 )
(early termi-nation)
III 1L, MET+ ECX + rilotumumabECX
3045
8.810.7 P = 0.032 NS
5.66
MET AMG 337 ( 97 )(early termi-
nation)
II ≥2L for 98% of patients, MET+
AMG 337 18primary
endpoint
7.9 3.4
mTOR GRANITE-1 ( 99 )
III ≥2L EverolimusPlacebo
4.52.1
5.44.3 P = 0.124 NS
1.71.4
FGFR1/2/3 SHINE ( 103 ) II 2L, FGFR2+ AZD4547Paclitaxel
2.623
5.56.6
1.83.5 P = 0.9581 NSprimary endpoint
VEGFA AVAGAST ( 107 )
III 1L Cisplatin/fl uoropyrimidine + bevacizumab
46 12.1 6.7
Cisplatin/fl uoropyrimidine 37 10.1 5.3 P = 0.1002 NS
(continued)
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1663
TargetTrial (reference) Phase Line of therapy Treatment ORR (%)
Median OS (months)
Median PFS (months)
VEGFR2 RAINFALL ( 106 )
III 1L Cisplatin/fl uoropyrimidine + ramucirumab
41 11.2 5.7
Cisplatin/fl uoropyrimidine 36 10.7 5.4 P = 0.0106 (inves-
tigator review) P = 0.74 NS
(central independent review)
primary endpoint
VEGFR2 REGARD ( 104 ) III 2L Ramucirumab 3 5.2 2.1Placebo 3 3.8 1.3
P = 0.047
VEGFR2 RAINBOW ( 105 )
III 2L Paclitaxel + ramucirumabPaclitaxel
2816
9.67.4 P = 0.017
4.42.9
PD-1 KEYNOTE-061 ( 114 )
III 2L PembrolizumabPaclitaxel
CPS≥1: 16 14
CPS≥1: 9.1 8.3 P = 0.0421 NSOS and PFS in
CPS ≥ 1 are both primary endpoints
CPS≥1: 1.5 4.1 P = Not reportedOS and PFS in
CPS≥1 are both primary endpoints
PD-1 KEYNOTE- 059 ( 112 )
II ≥3L, gastric/GEJ Pembrolizumab (Cohort 1) CPS≥1: 15.5
CPS≥1: 5.8 CPS≥1: 2.1
CPS<1: 6.4 CPS<1: 4.9 CPS<1: 2.0Primary
endpoint
PD-1 KEYNOTE- 180 ( 115 )
II ≥3L, ESCC/EAC/GEJ
Pembrolizumab ESCC: 14.3
ESCC: 6.8 ESCC: 2.1
EAC/GEJ: 5.2
EAC/GEJ: 3.9 EAC/GEJ: 1.9
primary endpoint
PD-1 ATTRACTION-2 ( 113 )
III ≥3L NivolumabPlacebo
110
5.34.1 P < 0.0001
1.61.5
PARP GOLD ( 129 ) III 2L Paclitaxel + olaparib 24 8.8 3.7Paclitaxel 16 6.9 3.2
P = 0.026 NS
NOTE: Primary endpoint is median OS unless otherwise specifi ed. Abbreviations: CapeOx, capecitabine/oxaliplatin; CPS, PD-L1 combined positive score; ECX, epirubicin/cisplatin/capecitabine; EOC, epirubicin/oxaliplatin/capecitabine; mFOLFOX6, leucovorin/fl uorouracil/oxaliplatin; NS, not signifi cant; ORR, objective response rate.
Table 1. Key clinical trials for GEA (Continued)
single tumor site (ref. 77 ; Fig. 3 ). Although it is diffi cult to argue at this time that the presence of heterogeneous ERBB2 is suffi cient rationale to deprive a patient of trastuzumab therapy, research may ultimately show that therapy against a target clearly present in metastatic disease could be superior to targeting ERBB2 that is detectable only in the primary
lesion. Later, we discuss the potential of using cutting-edge liquid biopsy technology to confront this heterogeneity.
Aside from differences encoded in the somatic genome, optimal targeting also requires consideration of the under-lying biology of a lineage. A telling example stems from a basket trial evaluating the ERBB2 kinase inhibitor neratinib
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1664 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
Figure 2. Types of genomic heterogeneity in GEA.
Interlesion heterogeneity
Intralesionheterogeneity
Genomiccoalteration
Metastases withGene B alteration
Primary site withGene A alteration
Metastasis withGene A alteration
Gene A alteration
Gene B alteration Gene A and Bcoamplification
Gene A amplification
Figure 3. Genomic heterogeneity affects the molecular diagnosis and treatment response of GEA. Potential outcomes with testing of a single tumor site, in this case, endoscopic biopsy of the primary lesion. The inset represents a scenario in which the biopsy captures both cells with Gene A amplifica-tion and cells with Gene B amplification.
Metastasis Gene A FISH Next-generationsequencing
Circulatingtumor DNA
Response to Gene A–directed therapy
Primary
Primary
Endoscopicbiopsy
Metastasis
Gene A amplification
Gene B amplification
Gene A and B coamplification
+ Gene Aamplification
Gene Aamplification
Sensitive
+ Gene Aamplification
Gene A ± Bamplification
Initial sensitivity but withshorter time to progression
+ Gene Aamplification
Gene B ± Aamplification
Resistant
+ Gene A and Bamplification
Gene A and Bamplification
Resistant
+ in asubset of cells
Gene A and Bamplification
Gene B ± Aamplification
Resistant
− Gene Bamplification
Gene A ± Bamplification
Initial sensitivity but withshorter time to progression
in patients with ERBB2 somatic mutations (78). Although caveats should be drawn to the differences between mutation versus amplification, and small-molecule kinase inhibitor ver-sus antibody, the results were notable for robust responses in ERBB2-mutant breast cancer but remarkable lack of efficacy in GEA or colorectal cancer (78). These results evoke memo-ries of the failure to reproduce the stunning albeit transient effects of BRAF inhibition from V600E-mutant melanoma in colorectal cancers also harboring the identical mutation
(79, 80). Key lineage-dependent differences in the response to a targeted agent can have far-reaching consequences on therapeutic efficacy. As many approaches being evaluated in ERBB2+ GEA originated with clinical success in breast cancer, these results are a reminder of the importance of focused biological study of GEA.
BEYOND ERBB2: PARALLEL LESSONS FROM OTHER TARGETED THERAPIESEGFR
Phase III trials of other targeted therapies in gastro-esophageal cancer have fallen short of the mark left by trastuzumab (Table 1). EGFR is amplified in 5% of GEA and the protein is overexpressed in 30% to 50% of GEA (81–84). Neither the addition of cetuximab (EXPAND trial) nor pani-tumumab (REAL3 trial), both anti-EGFR mAbs, to chem-otherapy improved progression-free survival (PFS) or OS (85, 86). In REAL3, patients in the panitumumab plus chemo-therapy arm actually had worse OS, with the important caveat that this combination arm also received less chemotherapy because of overlapping toxicity with panitumumab (86). In the second-line or higher setting, the EGFR tyrosine kinase inhibitor (TKI) gefitinib had no benefit compared with pla-cebo (COG trial; ref. 87). However, it is critical to note that these negative EGFR trials were all conducted in unselected patient populations, irrespective of EGFR status. Indeed, subset analysis of the COG data showed a statistically signifi-cant OS benefit in EGFR-amplified patients (88), and a similar trend was observed in the EXPAND trial for tumors with high EGFR IHC expression (89), again emphasizing the simple yet crucial lesson of testing targeted therapies in biomarker-positive patient populations. More recent data highlight the
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1665
potential efficacy of EGFR-directed therapy both with and without chemotherapy in patients with bona fide EGFR-amplified GEA (81).
METClinical trials using MET-directed agents in GEA have also
been disappointing. Support for targeting MET followed marked MET inhibitor sensitivity against kinase inhibitors in MET-amplified GEA cell lines (90). Whereas MET ampli-fications occur in 6% of GEA, MET overexpression has been reported in 25% to 60% of GEA (5, 91–93). The METGastric study examined chemotherapy with onartuzumab, a mAb against the MET extracellular domain that blocks interac-tion with the MET ligand HGF (94). This trial was stopped early because no predictive cutoff for MET IHC could be identified in a parallel phase II study (95). Even MET IHC 2/3+ patients in the phase III trial had no OS benefit (11 vs. 9.7 months, P = 0.06), although statistical significance may have been thwarted by decreased power from premature termination (94). The RILOMET-1 study was also discontinued early, in this case because of decreased survival in the experimental arm of chemotherapy plus rilotumumab, a mAb against HGF (96). As compared with METGastric, which required MET IHC ≥1+ in at least 50% of cells, RILOMET-1 had looser inclusion criteria (≥1+, ≥25% cells), included fewer IHC 2/3+ patients, and had no trend toward an interaction between MET expression and outcomes. Also, there were very few MET-amplified patients in RILOMET-1, and FISH ratios were not reported in METGastric.
In contrast to these studies, MET amplification was used as the inclusion criteria for a single-arm phase II study of the MET TKI AMG 337 in heavily pretreated patients with advanced-stage tumors (97). Disappointingly, this trial was also stopped early because the primary endpoint of objective response rate (ORR; 18%) was lower than expected compared with phase I data (30%; ref. 98). A key limitation of the AMG 337 studies was that MET status was derived from archi-val tumor specimens, generally obtained prior to first-line cytotoxic therapy. In light of the above discussion regarding ERBB2 heterogeneity, this raises the hypothesis that some patients may not have been truly MET-amplified at enroll-ment. Indeed, similar to ERBB2, MET amplification is hetero-geneous between primary tumors and metastases, and MET inhibition permits outgrowth of non–MET-amplified clones (33). Moreover, in one study, 10 of 21 MET-amplified GEAs harbored coamplification of ERBB2 and/or EGFR with MET in the same tumor cells, conferring de novo resistance to MET inhibition (33). These results again emphasize the inadequacy of simple biomarker assessment in CIN GEA, and suggest we have rejected targeted therapies that might be effective if used in optimal patients or in optimal combinations.
mTORThe PI3K–AKT–mTOR pathway is frequently activated
in GEA, particularly in the EBV+ subtype, through PIK3CA-activating mutations and amplifications, and PTEN truncat-ing mutations and deletions (5, 6). The GRANITE-1 study enrolled unselected patients with gastric cancer to evaluate second- and third-line treatment with everolimus compared with placebo, unfortunately without improvement in OS (99). Biomarker analysis for this trial has not been published;
however, an earlier phase II study identified phosphorylated S6, a downstream effector of mTOR, as a potential predictive factor that remains to be validated (100).
FGFR2FGFR2 amplifications occur in 5% of GEA, with enrich-
ment in the CIN and GS subtypes (5, 25). As with MET, cell line studies in GEAs with FGFR2 amplification show robust responses to kinase inhibition (101, 102). Mechanistic stud-ies suggest that excess FGFR2 activates PI3K signaling indi-rectly through transactivation of alternative RTKs such as ERBB3 and IGF1R (102). However, no differences in PFS were observed in the randomized phase II SHINE study comparing the FGFR1/2/3 TKI AZD4547 to paclitaxel for the second- line treatment of gastric cancers with FGFR2 polysomy or amplification as determined by FISH on archival tumor speci-mens (103). A limitation of this study was the consider-able intratumor heterogeneity of FGFR2 status and lack of correlation of FGFR2 genomic status with FGFR2 mRNA expression, possibly explaining the negative results (103). Indeed, another translational clinical trial demonstrated that response to AZD4547 can be predicted by high-level homo-geneous FGFR2 amplification as opposed to subclonal ampli-fication (102), again highlighting the critical importance of identifying an effective biomarker threshold and considering heterogeneity.
Antiangiogenic TherapiesAlthough antiangiogenic therapies are currently stand-
ard of care and are distinct from the targeted oncogene approaches described above, clinical trials of these agents in unselected patients with GEA have had mixed efficacy, suggesting there may be room for improvement through investigation of biomarkers and effective combination strate-gies. The anti-VEGFR2 antibody ramucirumab demonstrated significant albeit modest OS benefit in the second-line setting both as monotherapy (vs. placebo in the REGARD trial) and combined with chemotherapy (vs. chemotherapy alone in the RAINBOW trial; refs. 104, 105). On the other hand, in the first-line setting, there was no improved OS or PFS (by central independent review) with the addition of ramucirumab to chemotherapy (RAINFALL trial; ref. 106). Similarly, the anti-VEGFA antibody bevacizumab improved overall response rate and PFS, but not OS, when added to chemotherapy for the first-line treatment of advanced gastric cancer (AVAGAST trial; ref. 107). Interestingly, biomarker analysis pinpointed high baseline plasma VEGFA levels (but not tumor VEGFA) and low tumor protein expression of neuropilin 1 (a VEGF family coreceptor) as candidate predictive biomarkers in patients from non-Asian regions (108). Future correlative studies will be integral to maximizing the efficacy of antian-giogenic therapy, especially given that VEGFA amplifications occur in 28% of EACs and 7% of gastric adenocarcinomas (5, 6). Furthermore, the clinical success of pairing anti-VEGF agents with immunotherapy in renal cell carcinoma (109) warrants evaluation of these combinations in GEA.
Immune Checkpoint BlockadeThe role of immune checkpoint blockade for GEA is reviewed
elsewhere (110) and will be addressed only briefly. Recent work
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1666 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
has demonstrated clear enrichment of responses in patients with MSI and EBV+ gastric cancer (55), again emphasizing the importance of molecular stratification in the application of immunotherapy for GEA. Pembrolizumab is approved for the second-line treatment of MSI-high/mismatch repair–deficient gastric cancer. Notably, unlike in colorectal cancer, there are also responses to immune checkpoint inhibition in non-MSI and non-EBV+ GEA. The phase III KEYNOTE-062 trial dem-onstrated noninferior OS and a more favorable safety profile for pembrolizumab compared with chemotherapy as first-line treatment for patients with PD-L1+/ERBB2− advanced gastric/GEJ adenocarcinoma (NCT02494583; ref. 111). In addition, pembrolizumab prolonged OS in the subset of patients with tumors expressing high levels of PD-L1 (17.4 vs. 10.8 months). Although the combination of pembrolizumab plus chemo-therapy improved ORR, it did not improve OS or PFS com-pared with chemotherapy alone. The phase II KEYNOTE-059 trial led to FDA approval of pembrolizumab for patients with PD-L1+ advanced gastric/GEJ adenocarcinoma who have received two or more lines of therapy (112). In an Asian popu-lation of relapsed/refractory gastric/GEJ cancers, the phase III ATTRACTION-2 study showed a modest median OS benefit for nivolumab compared with placebo (5.3 vs. 4.1 months, P < 0.0001), and a substantial benefit in 12-month OS rate (26.2% vs. 10.9%; ref. 113).
However, other studies have tempered expectations from these agents and emphasize the need for additional bio-markers beyond PD-L1. KEYNOTE-061, a phase III trial of pembrolizumab compared with paclitaxel for the second-line treatment of PD-L1+ gastric/GEJ tumors, failed to show a survival benefit for immune checkpoint blockade (114). The phase II single-arm KEYNOTE-180 trial of pembrolizumab for advanced, metastatic esophageal cancer progressing after two or more lines of therapy demonstrated an ORR of only 5.2% in patients with EAC/GEJ, in contrast to 14.3% in patients with ESCC (115). The phase III KEYNOTE-181 study compared pembrolizumab to chemotherapy in patients with advanced or metastatic ESCC or EAC/GEJ after first-line standard therapy (NCT02564263; ref. 116). Despite favora-ble trends and a better safety profile, pembrolizumab did not significantly improve OS in the intention-to-treat popu-lation. Pembrolizumab did improve OS in a prespecified subgroup analysis of patients with tumors expressing high levels of PD-L1 (9.3 vs. 6.7 months); however, this benefit was restricted to patients with ESCC (10.3 vs. 6.7 months) and not observed in patients with EAC/GEJ (6.3 vs. 6.9 months). Whereas these trials led to FDA approval of pembrolizumab in the ESCC population, numerous ongoing studies will address pivotal questions about how to enhance the efficacy of immunotherapy in GEA and identify combinations with other targeted and conventional therapies.
MOVING FORWARD: MAXIMIZING OPPORTUNITIES FOR THERAPEUTIC EFFICACY
As a field, we are now poised to leverage the failures of targeted therapy to revise our clinical approach to GEA. The prevalence of concomitant genomic alterations, especially RTK coamplifications that confer resistance to single-agent
therapy, underscores the need for comprehensive molecu-lar profiling to guide treatment selection, including combi-nation strategies. Furthermore, the breadth of interlesion tumor heterogeneity within an individual patient means that biopsy of a single lesion incompletely represents the clinically relevant genomic composition of a patient’s cancer burden.
To bypass the impracticality of taking multiple tissue biop-sies, including synchronous primary and metastatic biop-sies, emerging data suggest the clear potential of minimally invasive liquid biopsies for the isolation and sequencing of cell-free circulating tumor DNA (ctDNA) in peripheral blood (reviewed in ref. 117). Although systematic validation of the accuracy, reliability, and reproducibility of ctDNA assays is a work in progress, clinical utility has been demonstrated in several studies of GEA with amplifications of ERBB2, EGFR, MET, and FGFR2 (33, 35, 72, 76, 81, 102). In an umbrella trial of targeted therapy in GEA, approximately one third of patients had discordant oncogene amplification between synchronous primary tumor and metastatic biopsies, leading to treatment reassignment (35, 118). Biomarker concord-ance between metastases and ctDNA surpasses correlation between metastases and primary tumor, raising the hypoth-esis that ctDNA may complement traditional tissue-based genomic profiling to guide treatment in the metastatic set-ting. Beyond initial treatment selection, ctDNA may be sam-pled longitudinally during the course of treatment to trace the evolution of clonal heterogeneity, including identifying drivers of intrinsic and acquired resistance. Biomarker detec-tion and validation might also improve with ctDNA analysis; for example, higher EGFR copy number in ctDNA correlated with response to anti-EGFR therapy (81), and a similar find-ing was reported for FGFR2 amplification and response to an FGFR TKI (102). In addition, ctDNA mutational load predicted response to pembrolizumab in MSI-high meta-static gastric cancer, and lower ctDNA levels at 6 weeks post-treatment predicted improved outcomes (55).
Integrating NGS and ctDNA technologies into clinical trials will enhance patient and treatment selection, espe-cially for innovative trial designs like basket and umbrella studies. PANGEA (NCT02213289; ref. 118) and VIKTORY (NCT02299648; ref. 119) are both biomarker-based umbrella trials for metastatic GEA or gastric cancer, respectively, that prospectively use tumor genomic profiling to assign patients to targeted therapy treatment arms spanning key RTK pathway amplifications and mutations. Whereas VIKTORY focuses on primary tumor specimens, PANGEA analyzes both primary and metastatic lesions at baseline and at progres-sive disease, and both trials perform ctDNA sequencing for correlative studies. Outcomes from PANGEA are pending; however, the biomarker-driven treatment group in VIKTORY demonstrated better OS (9.8 vs. 6.9 months, P < 0.001) and PFS (5.7 vs. 3.8 months, P < 0.0001) compared with patients who received conventional second-line treatment (119). More adaptive trials such as these are needed to address the intri-cate, heterogeneous genomes of patients with GEA. Although these trials will certainly be more complex, recent experience has demonstrated that unless we change our approach, we will continue to conduct negative studies that fail to identify the efficacy of drugs that may be beneficial in a more tailored patient population. These refined clinical trial approaches
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1667
will pave the way for exploring and ultimately translating new candidate genetic dependencies and therapeutic vulner-abilities of GEA, as described below.
UNCHARTED TERRITORY: NOVEL TARGETS AND TREATMENTS ON THE HORIZON
The diversity of oncogenic amplifications in the CIN sub-type of GEA have made it challenging to identify a unifying vulnerability of these tumors. The common thread is their underlying genomic instability and aneuploidy. Long-term therapeutic advancements may require a deeper understand-ing of the causes and consequences of CIN, and the vulnera-bilities stemming from CIN. This not only includes targeting oncogenes that are activated in the presence of genomic insta-bility, but also defining vulnerabilities inherent to the under-lying state of a cell with such marked genomic disruption.
Meanwhile, the focus of targeted therapy efforts for CIN GEA has been RTK amplifications. However, there are a host of other targets worthy of evaluation. One example followed the recognition that CIN GEAs frequently activate the KRAS onco-gene not via canonical mutations seen in many other cancers but through focal high-level genomic amplification compris-ing 14% of CIN GEA and causing as much as several hundred- fold overexpression of wild-type KRAS protein (25, 120). Labo-ratory-based evaluation of the intrinsic wiring of these tumors demonstrated that MEK inhibitors, which form the backbone of many current approaches for developing combination ther-apy for RAS-driven cancers, led to marked adaptive KRAS acti-vation owing to the massive KRAS expression. This adaptive response could be overcome by dual inhibition of MEK and the protein tyrosine phosphatase SHP2, also known as PTPN11, leading to tumor regression in xenograft models (120). Phase I trials are under way to evaluate the safety and tolerability of the SHP2 inhibitors TNO155 (NCT03114319) and RMC-4630 (NCT03634982) in advanced solid tumors.
Beyond RTK/MAPK pathways, molecular dissection of CIN GEA also revealed frequent alterations in cell-cycle regulators (5, 6, 25, 121). Epigenetic silencing or deletion of CDKN2A is common, particularly in EAC and EBV+ gastric cancer, as are amplifications of cyclin–CDK proteins that coordinate the G1–S transition, specifically CCNE1, CCND1, and CDK6. On the surface, these alterations seemingly converge on a final common pathway to phosphorylate and disable the RB1 tumor suppressor. Interestingly, however, primary RB1 dele-tion rarely occurs in CIN GEA (6, 25), raising the possibility that cyclin–CDK amplifications may also promote distinct oncogenic functions and confer specific genetic dependen-cies independent of RB1 inhibition. In parallel to investi-gating these fundamental questions at the bench, there are already tangible opportunities for translation at the bedside. CDK4/6 inhibition is a candidate therapeutic strategy for GEA with amplifications of CCND1 or CDK6, or silencing/deletion of CDKN2A. Although the response to palbociclib was not encouraging in a small phase II trial of patients with gastroesophageal cancer, inclusion was based on IHC for RB nuclear expression, which may not have been an optimal bio-marker (NCT01037790; ref. 122). Furthermore, efficacy may require combinations, as seen by effects of CDK4/6 inhibitors in concert with hormonal therapy in breast cancer.
For CCNE1-amplified GEA, preclinical data from gastric cancer patient-derived xenografts and from high-grade serous ovarian cancer (HGSOC) demonstrate that targeting CDK2, the partner kinase of CCNE1, may be effective (123, 124). Notably, CCNE1 amplifications are mutually exclusive and synthetic lethal with BRCA1 loss in HGSOC (125), suggesting the necessity of homologous recombination (HR) DNA repair in these cancers secondary to CCNE1-induced replication stress. Thus, targeting the DNA-damage response may be a key therapeutic approach that is further supported by enrich-ment of an HR deficiency (HRD) mutational signature (also known as COSMIC signature 3, or the BRCA signature) in the CIN subtype, specifically associated with focal somatic copy-number alteration events (25, 126). The HRD signature cor-relates with response to platinum- and PARP inhibitor–based therapies in breast and ovarian cancers (127), suggesting there may be a subset of CIN GEA harboring similar suscep-tibility. Indeed, a retrospective analysis of patients with South Korean gastric cancer showed that those with CIN tumors yielded the greatest benefit from adjuvant chemotherapy (21), perhaps hinting at a connection between CIN, HRD, and platinum sensitivity in gastric cancer.
PARP inhibitors have been clinically evaluated in GEA. Despite promising phase II data (128), the phase III GOLD trial failed to show benefit from adding the PARP inhibitor olaparib to paclitaxel in the second-line setting (129). These negative results in the overall patient population might be understandable because sensitivity to PARP inhibition typi-cally depends on HRD. Unexpectedly, however, the subgroup of patients with loss of ATM expression by IHC also did not benefit from olaparib. Potential explanations include imma-ture follow-up of the ATM-negative subgroup, and confound-ing of treatment by favorable prognostic factors enriched in ATM-low tumors, such as PD-L1 expression (129, 130). The data also suggest that additional genomic and functional measures of HRD and replication stress should be explored as predictive biomarkers of response to PARP inhibition. Platinum sensitivity may itself be a predictive biomarker, a concept that has led to a phase III trial of PARP inhibition versus placebo as maintenance therapy in inoperable, locally advanced, or metastatic gastric cancer that responded to platinum-based first-line chemotherapy (NCT03427814; ref. 131). More broadly, there is a widening spectrum of therapeu-tic agents in the DNA-damage sphere, for example, inhibitors of CHEK1, ATR, and WEE1, which may be combined with PARP inhibition to attack cancer cells with high basal replica-tion stress, even when HR remains intact (132). Evaluation of these agents in GEA, both preclinically and clinically, may be a critical path for the future.
The development of targeted therapies for diffuse gastric cancer is a pressing unmet need. Although these tumors are generally characterized by altered cell adhesion and motil-ity, up to 75% retain strong protein expression of the tight junction molecule claudin 18 isoform 2 (CLDN18.2), a lin-eage marker highly specific to differentiated gastric mucosal epithelial cells (133). CLDN18.2 is also expressed at lower frequency in intestinal-type gastric cancers and ectopically activated in EAC (133). The phase II FAST trial randomized patients with advanced/recurrent gastric and GEJ cancers, including 45% with diffuse type histology, to first-line
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1668 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
chemotherapy with or without IMAB362 (also known as clau-diximab or zolbetuximab), a chimeric mAb against CLDN18.2 that functions not via inhibition of CLDN18.2 but instead by using CLDN18.2 as a specific marker for antibody binding to elicit immune activation (NCT01630083; refs. 134–136). Inclusion criteria required CLDN18.2 IHC ≥2+ in at least 40% of tumor cells. The addition of IMAB362 improved ORR (39% vs. 25%, P = 0.022), the primary endpoint of PFS (7.5 vs. 5.3 months, P < 0.0005), and OS (13.0 vs. 8.4 months, P = 0.0008), with even greater benefit in the subgroup with CLDN18.2 IHC ≥2+ in at least 70% of cells (135). These encouraging results have spurred two phase III trials for fur-ther evaluation of IMAB362 (NCT03504397; NCT03653507). Other approaches to target CLDN18.2+ cells using antibody–drug conjugates for delivery of a cytotoxic payload, CD3 bispecific antibodies to induce T cell–mediated killing of tumor cells, and CLDN18.2-specific chimeric antigen recep-tor T cells are under preclinical investigation (137, 138).
CONCLUSIONOur understanding of gastroesophageal cancer has rapidly
evolved over the past five years. Delving into the genomic landscape has revealed strong similarities between adenocar-cinomas of the stomach and esophagus, and their definitive distinction from squamous cell carcinomas of the esopha-gus. Moreover, these genomic blueprints have enabled clas-sification into molecular subtypes that elucidate the diverse, complex oncogenic pathways underlying GEA pathogenesis. These achievements are essential stepping stones on the path toward developing more effective therapeutic strategies. Unfortunately, however, the Occam’s razor “single target, sin-gle drug” rationale has proved too simplistic for GEA because of the intrinsic genomic instability and heterogeneity of this disease. To address these formidable obstacles, comprehensive and repeated molecular profiling will be integral to patient and treatment selection, and to the success of future trans-lational clinical trials in GEA. These changes in our clinical approach to GEA will be complemented and fueled by ongo-ing laboratory investigation into novel genetic dependencies and vulnerabilities of GEA. Ultimately, although consider-able challenges remain, the coming years hold the promise of a turning point in the battle against these deadly cancers.
Disclosure of Potential Conflicts of InterestA.J. Bass is a consultant at Lilly and Glenmark, reports receiving
commercial research grants from Novartis, Merck, Sanofi, and Bayer, and has ownership interest (including patents) in Earli, Helix Nano, and Signet Therapeutics. No potential conflicts of interest were dis-closed by the other authors.
AcknowledgmentsWe are grateful to Michael Cooper, Medical Illustrator, for col-
laborative work on figures. A.K. Nagaraja is supported by the Depart-ment of Defense Peer Reviewed Cancer Research Program Horizon Award (W81XWH-17-1-0222), the Conquer Cancer Foundation of ASCO/Boehringer Ingelheim Endowed Young Investigator Award in Gastrointestinal Cancers, and the Debbie’s Dream Foundation- Stupid Strong-AACR Gastric Cancer Research Fellowship, in memory of Candace Netzer (19-40-41-NAGA). A.J. Bass is supported by the NCI (P50CA127003, P01CA224428, and R01CA098101). Any opin-
ions, interpretations, conclusions, and recommendations expressed in this material are those of the authors.
Received April 26, 2019; revised August 9, 2019; accepted September 6, 2019; published first November 14, 2019.
REFERENCES 1. International Agency for Research on Cancer. 2018 GLOBOCAN:
Stomach. Available from: http://gco.iarc.fr/today/data/factsheets/cancers/7-Stomach-fact-sheet.pdf.
2. Luo G, Zhang Y, Guo P, Wang L, Huang Y, Li K. Global patterns and trends in stomach cancer incidence: age, period and birth cohort analysis. Int J Cancer 2017;141:1333–44.
3. Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet 2016;388:2654–64.
4. Rustgi AK, El-Serag HB. Esophageal carcinoma. N Engl J Med 2014;371:2499–509.
5. The Cancer Genome Atlas Research Network. Comprehensive molec-ular characterization of gastric adenocarcinoma. Nature 2014;513: 202–9.
6. The Cancer Genome Atlas Research Network. Integrated genomic characterization of oesophageal carcinoma. Nature 2017;541:169–75.
7. Anderson WF, Rabkin CS, Turner N, Fraumeni JF Jr, Rosenberg PS, Camargo MC. The changing face of noncardia gastric can-cer incidence among US non-Hispanic whites. J Natl Cancer Inst 2018;110:608–15.
8. Blaser MJ, Chen Y. A new gastric cancer among us. J Natl Cancer Inst 2018;110:549–50.
9. Anderson WF, Camargo MC, Fraumeni JF Jr, Correa P, Rosenberg PS, Rabkin CS. Age-specific trends in incidence of noncardia gastric cancer in US adults. JAMA 2010;303:1723–8.
10. American Cancer Society. Cancer Facts & Figures 2018. Atlanta, GA: American Cancer Society; 2018.
11. Noone AM, Cronin KA, Altekruse SF, Howlader N, Lewis DR, Petkov VI, et al. Cancer incidence and survival trends by subtype using data from the Surveillance Epidemiology and End Results Program, 1992–2013. Cancer Epidemiol Biomarkers Prev 2017;26:632–41.
12. Lauren P. The two histological main types of gastric carcinoma: dif-fuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 1965;64:31–49.
13. Siewert JR, Stein HJ. Carcinoma of the gastroesophageal junction - classification, pathology and extent of resection. Dis Esophagus 1996;9:173–82.
14. Russo A, Li P, Strong VE. Differences in the multimodal treatment of gastric cancer: East versus west. J Surg Oncol 2017;115:603–14.
15. Tachimori Y, Ozawa S, Numasaki H, Ishihara R, Matsubara H, Muro K, et al. Comprehensive registry of esophageal cancer in Japan, 2011. Esophagus 2018;15:127–52.
16. Nishi T, Makuuchi H, Ozawa S, Shimada H, Chino O. The present status and future of Barrett’s esophageal adenocarcinoma in Japan. Digestion 2018:1–6.
17. Schumacher SE, Shim BY, Corso G, Ryu MH, Kang YK, Roviello F, et al. Somatic copy number alterations in gastric adenocarcinomas among Asian and Western patients. PLoS One 2017;12:e0176045.
18. Lin SJ, Gagnon-Bartsch JA, Tan IB, Earle S, Ruff L, Pettinger K, et al. Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas. Gut 2015;64:1721–31.
19. Cristescu R, Lee J, Nebozhyn M, Kim KM, Ting JC, Wong SS, et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat Med 2015;21:449–56.
20. Weaver JMJ, Ross-Innes CS, Shannon N, Lynch AG, Forshew T, Barbera M, et al. Ordering of mutations in preinvasive disease stages of esophageal carcinogenesis. Nat Genet 2014;46:837–43.
21. Sohn BH, Hwang J-E, Jang H-J, Lee H-S, Oh SC, Shim J-J, et al. Clinical significance of four molecular subtypes of gastric cancer identified by The Cancer Genome Atlas Project. Clin Cancer Res 2017;23:4441–9.
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1669
22. Sawas T, Killcoyne S, Iyer PG, Wang KK, Smyrk TC, Kisiel JB, et al. Identification of Prognostic Phenotypes of Esophageal Adenocar-cinoma in 2 Independent Cohorts. Gastroenterology 2018;155: 1720–8.
23. Secrier M, Li X, de Silva N, Eldridge MD, Contino G, Bornschein J, et al. Mutational signatures in esophageal adenocarcinoma define etiologically distinct subgroups with therapeutic relevance. Nat Genet 2016;48:1131–41.
24. Dulak AM, Schumacher SE, van Lieshout J, Imamura Y, Fox C, Shim B, et al. Gastrointestinal adenocarcinomas of the esophagus, stomach, and colon exhibit distinct patterns of genome instability and oncogenesis. Cancer Res 2012;72:4383–93.
25. Liu Y, Sethi NS, Hinoue T, Schneider BG, Cherniack AD, Sanchez-Vega F, et al. Comparative molecular analysis of gastrointestinal adenocarcinomas. Cancer Cell 2018;33:721–35.
26. Li X, Galipeau PC, Paulson TG, Sanchez CA, Arnaudo J, Liu K, et al. Temporal and spatial evolution of somatic chromosomal altera-tions: a case-cohort study of Barrett’s esophagus. Cancer Prev Res 2014;7:114–27.
27. Stachler MD, Taylor-Weiner A, Peng S, McKenna A, Agoston AT, Odze RD, et al. Paired exome analysis of Barrett’s esophagus and adenocarcinoma. Nat Genet 2015;47:1047–55.
28. Nones K, Waddell N, Wayte N, Patch AM, Bailey P, Newell F, et al. Genomic catastrophes frequently arise in esophageal adenocarci-noma and drive tumorigenesis. Nat Commun 2014;5:5224.
29. Dulak AM, Stojanov P, Peng S, Lawrence MS, Fox C, Stewart C, et al. Exome and whole-genome sequencing of esophageal adenocarci-noma identifies recurrent driver events and mutational complexity. Nat Genet 2013;45:478–86.
30. Supek F, Lehner B. Clustered mutation signatures reveal that error-prone DNA repair targets mutations to active genes. Cell 2017; 170:534–47.
31. Robles AI, Traverso G, Zhang M, Roberts NJ, Khan MA, Joseph C, et al. Whole-exome sequencing analyses of inflammatory bowel disease-associated colorectal cancers. Gastroenterology 2016;150:931–43.
32. Kim J, Fox C, Peng S, Pusung M, Pectasides E, Matthee E, et al. Preexisting oncogenic events impact trastuzumab sensitivity in ERBB2-amplified gastroesophageal adenocarcinoma. J Clin Invest 2014;124:5145–58.
33. Kwak EL, Ahronian LG, Siravegna G, Mussolin B, Borger DR, God-frey JT, et al. Molecular heterogeneity and receptor coamplification drive resistance to targeted therapy in MET-amplified esophago-gastric cancer. Cancer Discov 2015;5:1271–81.
34. Janjigian YY, Sanchez-Vega F, Jonsson P, Chatila WK, Hechtman JF, Ku GY, et al. Genetic predictors of response to systemic therapy in esophagogastric cancer. Cancer Discov 2018;8:49–58.
35. Pectasides E, Stachler MD, Derks S, Liu Y, Maron S, Islam M, et al. Genomic heterogeneity as a barrier to precision medicine in gastroe-sophageal adenocarcinoma. Cancer Discov 2018;8:37–48.
36. Bautista MC, Jiang SF, Armstrong MA, Postlethwaite D, Li D. Impact of age on clinicopathological features and survival of patients with noncardia gastric adenocarcinoma. J Gastric Cancer 2014;14:238–45.
37. Chung HW, Noh SH, Lim JB. Analysis of demographic character-istics in 3242 young age gastric cancer patients in Korea. World J Gastroenterol 2010;16:256–63.
38. Martinson HA, Shelby NJ, Alberts SR, Olnes MJ. Gastric cancer in Alaska Native people: a cancer health disparity. World J Gastroen-terol 2018;24:2722–32.
39. Sanjeevaiah A, Cheedella N, Hester C, Porembka MR. Gastric can-cer: recent molecular classification advances, racial disparity, and management implications. J Oncol Pract 2018;14:217–24.
40. Fewings E, Larionov A, Redman J, Goldgraben MA, Scarth J, Richardson S, et al. Germline pathogenic variants in PALB2 and other cancer-predisposing genes in families with hereditary diffuse gastric cancer without CDH1 mutation: a whole-exome sequencing study. Lancet Gastroenterol Hepatol 2018;3:489–98.
41. Sahasrabudhe R, Lott P, Bohorquez M, Toal T, Estrada AP, Suarez JJ, et al. Germline mutations in PALB2, BRCA1, and RAD51C, which
regulate DNA recombination repair, in patients with gastric cancer. Gastroenterology 2017;152:983–6.
42. Hansford S, Kaurah P, Li-Chang H, Woo M, Senz J, Pinheiro H, et al. Hereditary diffuse gastric cancer syndrome: CDH1 mutations and beyond. JAMA Oncol 2015;1:23–32.
43. Ge S, Xia X, Ding C, Zhen B, Zhou Q, Feng J, et al. A proteomic landscape of diffuse-type gastric cancer. Nat Commun 2018;9:1012.
44. Wang K, Yuen ST, Xu J, Lee SP, Yan HH, Shi ST, et al. Whole-genome sequencing and comprehensive molecular profiling identify new driver mutations in gastric cancer. Nat Genet 2014;46:573–82.
45. Kakiuchi M, Nishizawa T, Ueda H, Gotoh K, Tanaka A, Hayashi A, et al. Recurrent gain-of-function mutations of RHOA in diffuse-type gastric carcinoma. Nat Genet 2014;46:583–7.
46. Joneson T, White MA, Wigler MH, Bar-Sagi D. Stimulation of mem-brane ruffling and MAP kinase activation by distinct effectors of RAS. Science 1996;271:810–2.
47. Yao F, Kausalya JP, Sia YY, Teo AS, Lee WH, Ong AG, et al. Recurrent fusion genes in gastric cancer: CLDN18-ARHGAP26 induces loss of epithelial integrity. Cell Rep 2015;12:272–85.
48. Pattison S, Mitchell C, Lade S, Leong T, Busuttil RA, Boussioutas A. Early relapses after adjuvant chemotherapy suggests primary chem-oresistance in diffuse gastric cancer. PLoS One 2017;12:e0183891.
49. Choi YY, Bae JM, An JY, Kwon IG, Cho I, Shin HB, et al. Is microsat-ellite instability a prognostic marker in gastric cancer? A systematic review with meta-analysis. J Surg Oncol 2014;110:129–35.
50. Pietrantonio F, Raimondi A, Choi YY, Kang W, Langley RE, Kim YW, et al. MSI-GC-01: Individual patient data (IPD) meta-analysis of micro-satellite instability (MSI) and gastric cancer (GC) from four rand-omized clinical trials (RCTs). J Clin Oncol 37:4s, 2019 (suppl; abstr 66).
51. Smyth EC, Wotherspoon A, Peckitt C, Gonzalez D, Hulkki-Wilson S, Eltahir Z, et al. Mismatch repair deficiency, microsatellite insta-bility, and survival: an exploratory analysis of the medical research council adjuvant gastric infusional chemotherapy (MAGIC) trial. JAMA Oncol 2017;3:1197–203.
52. Choi YY, Kim H, Yang H-K, Kim WH, Kim YW, Kook M-C, et al. Clinical impact of microsatellite instability in patients with stage II and III gastric cancer: results from the CLASSIC trial. J Clin Oncol 35:15s, 2017 (suppl; abstr 4022).
53. Derks S, Liao X, Chiaravalli AM, Xu X, Camargo MC, Solcia E, et al. Abundant PD-L1 expression in Epstein-Barr Virus-infected gastric cancers. Oncotarget 2016;7:32925–32.
54. Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017;357:409–13.
55. Kim ST, Cristescu R, Bass AJ, Kim KM, Odegaard JI, Kim K, et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat Med 2018;24: 1449–58.
56. Green MR, Monti S, Rodig SJ, Juszczynski P, Currie T, O’Donnell E, et al. Integrative analysis reveals selective 9p24.1 amplification, increased PD-1 ligand expression, and further induction via JAK2 in nodular sclerosing Hodgkin lymphoma and primary mediastinal large B-cell lymphoma. Blood 2010;116:3268–77.
57. Green MR, Rodig S, Juszczynski P, Ouyang J, Sinha P, O’Donnell E, et al. Constitutive AP-1 activity and EBV infection induce PD-L1 in Hodgkin lymphomas and posttransplant lymphoprolif-erative disorders: implications for targeted therapy. Clin Cancer Res 2012;18:1611–8.
58. Merryman RW, Armand P, Wright KT, Rodig SJ. Checkpoint blockade in Hodgkin and non-Hodgkin lymphoma. Blood Adv 2017;1:2643–54.
59. Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gas-tric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 2010;376:687–97.
60. Van Cutsem E, Bang YJ, Feng-Yi F, Xu JM, Lee KW, Jiao SC, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer 2015;18:476–84.
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1670 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
61. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001;344:783–92.
62. Tabernero J, Hoff PM, Shen L, Ohtsu A, Shah MA, Cheng K, et al. Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol 2018;19:1372–84.
63. Kang YK, Rha SY, Tassone P, Barriuso J, Yu R, Szado T, et al. A phase IIa dose-finding and safety study of first-line pertuzumab in combination with trastuzumab, capecitabine and cisplatin in patients with HER2-positive advanced gastric cancer. Br J Cancer 2014;111:660–6.
64. Kirschbrown WP, Wang B, Nijem I, Ohtsu A, Hoff PM, Shah MA, et al. Pharmacokinetic and exposure–response analysis of pertuzumab in patients with HER2-positive metastatic gastric or gastroesophageal junction cancer. Cancer Chemother Pharmacol 2019;84:539–50.
65. Thuss-Patience PC, Shah MA, Ohtsu A, Van Cutsem E, Ajani JA, Castro H, et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): an international randomised, open-label, adaptive, phase 2/3 study. Lancet Oncol 2017;18:640–53.
66. Hecht JR, Bang YJ, Qin SK, Chung HC, Xu JM, Park JO, et al. Lapa-tinib in combination with capecitabine plus oxaliplatin in human epidermal growth factor receptor 2-positive advanced or metastatic gastric, esophageal, or gastroesophageal adenocarcinoma: TRIO-013/LOGiC–a randomized phase III trial. J Clin Oncol 2016;34:443–51.
67. Satoh T, Xu RH, Chung HC, Sun GP, Doi T, Xu JM, et al. Lapa-tinib plus paclitaxel versus paclitaxel alone in the second-line treatment of HER2-amplified advanced gastric cancer in Asian populations: TyTAN–a randomized, phase III study. J Clin Oncol 2014;32:2039–49.
68. Shitara K, Iwata H, Takahashi S, Tamura K, Park H, Modi S, et al. Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-positive gastric cancer: a dose-expansion, phase 1 study. Lan-cet Oncol 2019;20:827–36.
69. Bang YJ, Giaccone G, Im SA, Oh DY, Bauer TM, Nordstrom JL, et al. First-in-human phase 1 study of margetuximab (MGAH22), an Fc-modified chimeric monoclonal antibody, in patients with HER2-positive advanced solid tumors. Ann Oncol 2017;28:855–61.
70. Catenacci DVT, Park H, Uronis HE, Kang YK, Ng M, Gold P, et al. Biomarker-guided enrichment of the antitumor activity of margetuximab (M) plus pembrolizumab (P) in patients with advanced HER2+ gastric adenocarcinoma (GEA). Ann Oncol 2018; 29(suppl_8):mdy282.046.
71. Hofmann M, Stoss O, Shi D, Buttner R, van de Vijver M, Kim W, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology 2008;52:797–805.
72. Wang DS, Liu ZX, Lu YX, Bao H, Wu X, Zeng ZL, et al. Liquid biop-sies to track trastuzumab resistance in metastatic HER2-positive gastric cancer. Gut 2019;68:1152–61.
73. Shah MA, Kang YK, Thuss-Patience PC, Ohtsu A, Ajani JA, Van Cutsem E, et al. Biomarker analysis of the GATSBY study of tras-tuzumab emtansine versus a taxane in previously treated HER2-positive advanced gastric/gastroesophageal junction cancer. Gastric Cancer 2019;22:803–16.
74. Kim ST, Banks KC, Pectasides E, Kim SY, Kim K, Lanman RB, et al. Impact of genomic alterations on lapatinib treatment outcome and cell-free genomic landscape during HER2 therapy in HER2+ gastric cancer patients. Ann Oncol 2018;29:1037–48.
75. Lee JY, Hong M, Kim ST, Park SH, Kang WK, Kim KM, et al. The impact of concomitant genomic alterations on treatment outcome for trastuzumab therapy in HER2-positive gastric cancer. Sci Rep 2015;5:9289.
76. Sanchez-Vega F, Hechtman JF, Castel P, Ku GY, Tuvy Y, Won H, et al. EGFR and MET amplifications determine response to HER2 inhibi-
tion in ERBB2-amplified esophagogastric cancer. Cancer Discov 2019;9:199–209.
77. Bartley AN, Washington MK, Colasacco C, Ventura CB, Ismaila N, Benson AB III, et al. HER2 Testing and clinical decision making in gastroesophageal adenocarcinoma: guideline from the College of American Pathologists, American Society for Clinical Pathol-ogy, and the American Society of Clinical Oncology. J Clin Oncol 2017;35:446–64.
78. Hyman DM, Piha-Paul SA, Won H, Rodon J, Saura C, Shapiro GI, et al. HER kinase inhibition in patients with HER2- and HER3-mutant cancers. Nature 2018;554:189–94.
79. Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur GA, Sosman JA, et al. Inhibition of mutated, activated BRAF in metastatic mela-noma. N Engl J Med 2010;363:809–19.
80. Kopetz S, Desai J, Chan E, Hecht JR, O’Dwyer PJ, Maru D, et al. Phase II pilot study of vemurafenib in patients with metastatic BRAF-mutated colorectal cancer. J Clin Oncol 2015;33:4032–8.
81. Maron SB, Alpert L, Kwak HA, Lomnicki S, Chase L, Xu D, et al. Tar-geted therapies for targeted populations: anti-EGFR treatment for EGFR-amplified gastroesophageal adenocarcinoma. Cancer Discov 2018;8:696–713.
82. Kim MA, Lee HS, Lee HE, Jeon YK, Yang HK, Kim WH. EGFR in gastric carcinomas: prognostic significance of protein overexpres-sion and high gene copy number. Histopathology 2008;52:738–46.
83. Wang KL, Wu TT, Choi IS, Wang H, Resetkova E, Correa AM, et al. Expression of epidermal growth factor receptor in esophageal and esophagogastric junction adenocarcinomas: association with poor outcome. Cancer 2007;109:658–67.
84. Langer R, Von Rahden BH, Nahrig J, Von Weyhern C, Reiter R, Feith M, et al. Prognostic significance of expression patterns of c-erbB-2, p53, p16INK4A, p27KIP1, cyclin D1 and epidermal growth factor receptor in oesophageal adenocarcinoma: a tissue microarray study. J Clin Pathol 2006;59:631–4.
85. Lordick F, Kang YK, Chung HC, Salman P, Oh SC, Bodoky G, et al. Capecitabine and cisplatin with or without cetuximab for patients with previously untreated advanced gastric cancer (EXPAND): a randomised, open-label phase 3 trial. Lancet Oncol 2013;14:490–9.
86. Waddell T, Chau I, Cunningham D, Gonzalez D, Okines AF, Okines C, et al. Epirubicin, oxaliplatin, and capecitabine with or without panitumumab for patients with previously untreated advanced oesophagogastric cancer (REAL3): a randomised, open-label phase 3 trial. Lancet Oncol 2013;14:481–9.
87. Dutton SJ, Ferry DR, Blazeby JM, Abbas H, Dahle-Smith A, Man-soor W, et al. Gefitinib for oesophageal cancer progressing after chemotherapy (COG): a phase 3, multicentre, double-blind, placebo- controlled randomised trial. Lancet Oncol 2014;15:894–904.
88. Petty RD, Dahle-Smith A, Stevenson DAJ, Osborne A, Massie D, Clark C, et al. Gefitinib and EGFR gene copy number aberrations in esophageal cancer. J Clin Oncol 2017;35:2279–87.
89. Lordick F, Kang Y-K, Salman P, Oh SC, Bodoky G, Kurteva GP, et al. Clinical outcome according to tumor HER2 status and EGFR expression in advanced gastric cancer patients from the EXPAND study. J Clin Oncol 31:15s, 2013 (suppl; abstr 4021).
90. Smolen GA, Sordella R, Muir B, Mohapatra G, Barmettler A, Archibald H, et al. Amplification of MET may identify a subset of cancers with extreme sensitivity to the selective tyrosine kinase inhibitor PHA-665752. Proc Natl Acad Sci U S A 2006;103:2316–21.
91. Lee HE, Kim MA, Lee HS, Jung EJ, Yang HK, Lee BL, et al. MET in gastric carcinomas: comparison between protein expression and gene copy number and impact on clinical outcome. Br J Cancer 2012;107:325–33.
92. Janjigian YY, Tang LH, Coit DG, Kelsen DP, Francone TD, Weiser MR, et al. MET expression and amplification in patients with localized gastric cancer. Cancer Epidemiol Biomarkers Prev 2011;20:1021–7.
93. Nakajima M, Sawada H, Yamada Y, Watanabe A, Tatsumi M, Yamashita J, et al. The prognostic significance of amplification and overexpression of c-met and c-erb B-2 in human gastric carcinomas. Cancer 1999;85:1894–902.
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Genomics and Targeted Therapies in GEA REVIEW
DECEMBER 2019 CANCER DISCOVERY | 1671
94. Shah MA, Bang YJ, Lordick F, Alsina M, Chen M, Hack SP, et al. Effect of fluorouracil, leucovorin, and oxaliplatin with or without onartuzumab in HER2-negative, MET-positive gastroesophageal adenocarcinoma: the METGastric Randomized Clinical Trial. JAMA Oncol 2017;3:620–7.
95. Shah MA, Cho JY, Tan IB, Tebbutt NC, Yen CJ, Kang A, et al. A rand-omized phase II study of FOLFOX with or without the MET inhibi-tor onartuzumab in advanced adenocarcinoma of the stomach and gastroesophageal junction. Oncologist 2016;21:1085–90.
96. Catenacci DVT, Tebbutt NC, Davidenko I, Murad AM, Al-Batran SE, Ilson DH, et al. Rilotumumab plus epirubicin, cisplatin, and capecitabine as first-line therapy in advanced MET-positive gas-tric or gastro-oesophageal junction cancer (RILOMET-1): a ran-domised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2017;18:1467–82.
97. Van Cutsem E, Karaszewska B, Kang YK, Chung HC, Shankaran V, Siena S, et al. A multicenter phase II study of AMG 337 in patients with MET-amplified gastric/gastroesophageal junction/esophageal adenocarcinoma and other MET-amplified solid tumors. Clin Can-cer Res 2019;25:2414–23.
98. Hong DS, LoRusso P, Hamid O, Janku F, Kittaneh M, Catenacci DVT, et al. Phase I study of AMG 337, a highly selective small-molecule MET inhibitor, in patients with advanced solid tumors. Clin Cancer Res 2019;25:2403–13.
99. Ohtsu A, Ajani JA, Bai YX, Bang YJ, Chung HC, Pan HM, et al. Everolimus for previously treated advanced gastric cancer: results of the randomized, double-blind, phase III GRANITE-1 study. J Clin Oncol 2013;31:3935–43.
100. Yoon DH, Ryu MH, Park YS, Lee HJ, Lee C, Ryoo BY, et al. Phase II study of everolimus with biomarker exploration in patients with advanced gastric cancer refractory to chemotherapy including fluo-ropyrimidine and platinum. Br J Cancer 2012;106:1039–44.
101. Xie L, Su X, Zhang L, Yin X, Tang L, Zhang X, et al. FGFR2 gene amplification in gastric cancer predicts sensitivity to the selective FGFR inhibitor AZD4547. Clin Cancer Res 2013;19:2572–83.
102. Pearson A, Smyth E, Babina IS, Herrera-Abreu MT, Tarazona N, Peckitt C, et al. High-level clonal FGFR amplification and response to FGFR inhibition in a translational clinical trial. Cancer Discov 2016;6:838–51.
103. Van Cutsem E, Bang YJ, Mansoor W, Petty RD, Chao Y, Cunning-ham D, et al. A randomized, open-label study of the efficacy and safety of AZD4547 monotherapy versus paclitaxel for the treatment of advanced gastric adenocarcinoma with FGFR2 polysomy or gene amplification. Ann Oncol 2017;28:1316–24.
104. Fuchs CS, Tomasek J, Yong CJ, Dumitru F, Passalacqua R, Goswami C, et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adeno-carcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2014;383:31–9.
105. Wilke H, Muro K, Van Cutsem E, Oh SC, Bodoky G, Shimada Y, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro- oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol 2014;15:1224–35.
106. Fuchs CS, Shitara K, Di Bartolomeo M, Lonardi S, Al-Batran SE, Van Cutsem E, et al. Ramucirumab with cisplatin and fluoropyrimi-dine as first-line therapy in patients with metastatic gastric or junc-tional adenocarcinoma (RAINFALL): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol 2019;20:420–35.
107. Ohtsu A, Shah MA, Van Cutsem E, Rha SY, Sawaki A, Park SR, et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a randomized, double-blind, placebo-controlled phase III study. J Clin Oncol 2011;29:3968–76.
108. Van Cutsem E, de Haas S, Kang YK, Ohtsu A, Tebbutt NC, Ming Xu J, et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: a biomarker evaluation from the AVAGAST randomized phase III trial. J Clin Oncol 2012;30:2119–27.
109. Labriola MK, Batich KA, Zhu J, McNamara MA, Harrison MR, Armstrong AJ, et al. Immunotherapy is changing first-line treat-
ment of metastatic renal-cell carcinoma. Clin Genitourin Cancer 2019;17:e513–e21.
110. Cohen NA, Strong VE, Janjigian YY. Checkpoint blockade in esoph-agogastric cancer. J Surg Oncol 2018;118:77–85.
111. Tabernero J, Cutsem EV, Bang Y-J, Fuchs CS, Wyrwicz L, Lee KW, et al. Pembrolizumab with or without chemotherapy versus chemo-therapy for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: The phase III KEYNOTE-062 study. J Clin Oncol 37:18s, 2019 (suppl; abstr LBA4007).
112. Fuchs CS, Doi T, Jang RW, Muro K, Satoh T, Machado M, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junc-tion cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol 2018;4:e180013.
113. Kang YK, Boku N, Satoh T, Ryu MH, Chao Y, Kato K, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previ-ous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017;390:2461–71.
114. Shitara K, Ozguroglu M, Bang YJ, Di Bartolomeo M, Mandala M, Ryu MH, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet 2018;392:123–33.
115. Shah MA, Kojima T, Hochhauser D, Enzinger P, Raimbourg J, Hollebecque A, et al. Efficacy and safety of pembrolizumab for heav-ily pretreated patients with advanced, metastatic adenocarcinoma or squamous cell carcinoma of the esophagus: the phase 2 KEYNOTE- 180 study. JAMA Oncol 2019;5:546–50.
116. Shah MA, Adenis A, Enzinger PC, Kojima T, Muro K, Bennouna J, et al. Pembrolizumab versus chemotherapy as second-line therapy for advanced esophageal cancer: Phase 3 KEYNOTE-181 study. J Clin Oncol 37:15s, 2019 (suppl; abstr 4010).
117. Heitzer E, Haque IS, Roberts CES, Speicher MR. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat Rev Genet 2019;20:71–88.
118. Joshi SS, Maron SB, Lomnicki S, Polite BN, Sharma M, Ibe J, et al. Personalized antibodies for gastroesophageal adenocarcinoma (PANGEA): a phase II precision medicine trial (NCT02213289). J Clin Oncol 36:4s, 2018 (suppl; abstr TPS198).
119. Lee J, Kim ST, Kim K, Lee H, Kozarewa I, Mortimer PGS, et al. Tumor genomic profiling guides patients with metastatic gastric cancer to targeted treatment: The VIKTORY Umbrella Trial. Cancer Discov 2019;9:1388–405.
120. Wong GS, Zhou J, Liu JB, Wu Z, Xu X, Li T, et al. Targeting wild-type KRAS-amplified gastroesophageal cancer through combined MEK and SHP2 inhibition. Nat Med 2018;24:968–77.
121. Frankell AM, Jammula S, Li X, Contino G, Killcoyne S, Abbas S, et al. The landscape of selection in 551 esophageal adenocarcinomas defines genomic biomarkers for the clinic. Nat Genet 2019;51:506–16.
122. Karasic TB, O’Hara MH, Teitelbaum UR, Damjanov N, Giantonio BJ, d’Entremont TS, et al. Phase II trial of palbociclib in patients with advanced esophageal or gastric cancer. J Clin Oncol;36:4s, 2018 (suppl; abstr 68).
123. Chen Z, Huang W, Tian T, Zang W, Wang J, Liu Z, et al. Characteri-zation and validation of potential therapeutic targets based on the molecular signature of patient-derived xenografts in gastric cancer. J Hematol Oncol 2018;11:20.
124. Au-Yeung G, Lang F, Azar WJ, Mitchell C, Jarman KE, Lackovic K, et al. Selective targeting of cyclin E1-amplified high-grade serous ovarian cancer by cyclin-dependent kinase 2 and AKT inhibition. Clin Cancer Res 2017;23:1862–74.
125. Etemadmoghadam D, Weir BA, Au-Yeung G, Alsop K, Mitchell G, George J, et al. Synthetic lethality between CCNE1 amplification and loss of BRCA1. Proc Natl Acad Sci U S A 2013;110:19489–94.
126. Alexandrov LB, Nik-Zainal S, Siu HC, Leung SY, Stratton MR. A mutational signature in gastric cancer suggests therapeutic strate-gies. Nat Commun 2015;6:8683.
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

Nagaraja et al.REVIEW
1672 | CANCER DISCOVERY DECEMBER 2019 www.aacrjournals.org
127. Gulhan DC, Lee JJ, Melloni GEM, Cortes-Ciriano I, Park PJ. Detect-ing the mutational signature of homologous recombination defi-ciency in clinical samples. Nat Genet 2019;51:912–9.
128. Bang YJ, Im SA, Lee KW, Cho JY, Song EK, Lee KH, et al. Rand-omized, double-blind phase II trial with prospective classification by ATM protein level to evaluate the efficacy and tolerability of olaparib plus paclitaxel in patients with recurrent or metastatic gastric cancer. J Clin Oncol 2015;33:3858–65.
129. Bang YJ, Xu RH, Chin K, Lee KW, Park SH, Rha SY, et al. Olaparib in combination with paclitaxel in patients with advanced gastric cancer who have progressed following first-line therapy (GOLD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol 2017;18:1637–51.
130. Smyth E. Missing a GOLDen opportunity in gastric cancer. Lancet Oncol 2017;18:1561–3.
131. Ciardiello F, Bang Y-J, Bendell JC, Cervantes A, Brachmann RK, Zhang Y, et al. A phase III, double-blind, randomized study of pamiparib versus placebo as maintenance therapy in patients with inoperable, locally advanced, or metastatic gastric cancer (GC) that responded to platinum-based first-line chemotherapy. J Clin Oncol 37:4s, 2019 (suppl; abstr TPS173).
132. Fang Y, McGrail DJ, Sun C, Labrie M, Chen X, Zhang D, et al. Sequential therapy with PARP and WEE1 inhibitors mini-mizes toxicity while maintaining efficacy. Cancer Cell 2019;35: 851–67.
133. Sahin U, Koslowski M, Dhaene K, Usener D, Brandenburg G, Seitz G, et al. Claudin-18 splice variant 2 is a pan-cancer target suitable
for therapeutic antibody development. Clin Cancer Res 2008;14: 7624–34.
134. Schuler M, Al-Batran SE, Zvirbule Z, Manikhas G, Lordick F, Rusyn A, et al. Final results of the FAST study, an international, multicenter, randomized, phase II trial of epirubicin, oxaliplatin, and capecitabine (EOX) with or without the anti-CLDN18.2 anti-body IMAB362 as first-line therapy in patients with advanced CLDN18.2+ gastric and gastroesophageal junction (GEJ) adenocar-cinoma. Ann Oncol 2016;27:614O.
135. Sahin U, Tureci Ö, Manikhas GM, Lordick F, Rusyn A, Vynnych-enko I, et al. Zolbetuximab combined with EOX as first-line therapy in advanced CLDN18.2+ gastric (G) and gastroesophageal junction (GEJ) adenocarcinoma: updated results from the FAST trial. J Clin Oncol 37:4s, 2019 (suppl; abstr 16).
136. Al-Batran S-E, Schuler MH, Zvirbule Z, Manikhas G, Lordick F, Rusyn A, et al. FAST: an international, multicenter, randomized, phase II trial of epirubicin, oxaliplatin, and capecitabine (EOX) with or without IMAB362, a first-in-class anti-CLDN18.2 antibody, as first-line therapy in patients with advanced CLDN18.2+ gastric and gastroesophageal junction (GEJ) adenocarcinoma. J Clin Oncol 34:18s, 2016; (suppl; abstr LBA4001).
137. Zhu G, Foletti D, Liu X, Ding S, Melton Witt J, Hasa-Moreno A, et al. Targeting CLDN18.2 by CD3 bispecific and ADC modalities for the treatments of gastric and pancreatic cancer. Sci Rep 2019;9:8420.
138. Jiang H, Shi Z, Wang P, Wang C, Yang L, Du G, et al. Claudin18.2-specific chimeric antigen receptor engineered T cells for the treat-ment of gastric cancer. J Natl Cancer Inst 2019;111:409–18.
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487

2019;9:1656-1672. Published OnlineFirst November 14, 2019.Cancer Discov Ankur K. Nagaraja, Osamu Kikuchi and Adam J. Bass AdenocarcinomaGenomics and Targeted Therapies in Gastroesophageal
Updated version
10.1158/2159-8290.CD-19-0487doi:
Access the most recent version of this article at:
Cited articles
http://cancerdiscovery.aacrjournals.org/content/9/12/1656.full#ref-list-1
This article cites 126 articles, 34 of which you can access for free at:
Citing articles
http://cancerdiscovery.aacrjournals.org/content/9/12/1656.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerdiscovery.aacrjournals.org/content/9/12/1656To request permission to re-use all or part of this article, use this link
Cancer Research. on August 29, 2021. © 2019 American Association forcancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst November 14, 2019; DOI: 10.1158/2159-8290.CD-19-0487