Embed Size (px)
Citation preview

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 681
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMESGENETICS IN CLINICAL PRACTICE
From the Department of Internal Medicine and Division of Hematology, MayoClinic College of Medicine, Rochester, Minn (D.P.S.); and H. Lee MoffittCancer Center & Research Institute at the University of South Florida, Tampa,Fla (A.F.L.).
Individual reprints of this article are not available. The entire series onGenetics in Clinical Practice will be available for purchase from the Proceed-ings Editorial Office at a later date.
© 2005 Mayo Foundation for Medical Education and Research
Genetic Testing in the Myelodysplastic Syndromes:Molecular Insights Into Hematologic Diversity
DAVID P. STEENSMA, MD, AND ALAN F. LIST, MD
The myelodysplastic syndromes (MDS) are associated with adiverse set of acquired somatic genetic abnormalities. Bone mar-row karyotyping provides important diagnostic and prognosticinformation and should be attempted in all patients who aresuspected of having MDS. Fluorescent in situ hybridization (FISH)studies on blood or marrow may also be valuable in selectedcases, such as patients who may have 5q– syndrome or those whohave undergone hematopoietic stem cell transplantation. TheMDS-associated cytogenetic abnormalities that have been de-fined by karyotyping and FISH studies have already contributedsubstantially to our current understanding of the biology of malig-nant myeloid disorders, but the pathobiological meaning of com-mon, recurrent chromosomal lesions such as del(5q), del(20q),and monosomy 7 is still unknown. The great diversity of thecytogenetic findings described in MDS highlights the molecularheterogeneity of this cluster of diseases. We review the commonand pathophysiologically interesting genetic abnormalities associ-ated with MDS, focusing on the clinical utility of conventionalcytogenetic assays and selected FISH studies. In addition, wediscuss a series of well-defined MDS-associated point mutationsand outline the potential for further insights from newer tech-niques such as global gene expression profiling and array-basedcomparative genomic hybridization.
Mayo Clin Proc. 2005;80(5):681-698
AA = all normal; AML = acute myeloid leukemia; AN = abnormal-normal;APL = acute promyelocytic leukemia; CDR = commonly deleted region;CGH = comparative genomic hybridization; CML = chronic myeloidleukemia; CMML = chronic myelomonocytic leukemia; CMML-Eos =CMML with eosinophilia; FAB = French-American-British; FISH = fluores-cent in situ hybridization; gDNA = genomic DNA; GTPase = guanosinetriphosphate hydrolases; IPSS = International Prognostic Scoring Sys-tem; MDS = myelodysplastic syndromes; M-FISH = multicolor FISH;PDGFR-βββββ = βββββ subunit of the platelet-derived growth factor receptor;SKY = spectral karyotyping; WHO = World Health Organization
DISEASE SYNOPSIS
The term myelodysplastic syndromes (MDS) describes adiverse group of acquired hematopoietic stem cell malig-nancies unified by a common functional consequence—ineffective production of mature blood cells.1,2 In MDS,cytologic dysplasia of blood and marrow cells is associated
with functional defects in neutrophils and platelets, whichcontribute to infection and bleeding complications, respec-tively, even in the absence of substantial deficits in bloodcell production. The variable risk of progression to acutemyeloid leukemia (AML) that is characteristic of MDSappears to be driven by somatic genomic instability andepigenetic genomic modification. Evidence for this in-cludes allelic imbalance arising from structural or nu-merical chromosome aberrations, defects in DNA repair,3,4
and linkage to genotoxic exposures including alkylatingagents, topoisomerase II inhibitors, environmental poisons,or radiation.1,2
This overview highlights the genetic and molecular ab-normalities in adults with MDS, methods to detect theseabnormalities, and their potential importance for diagnosis,prognosis, and therapy (Table 1). The inherited and ac-quired MDS in pediatric patients display genetic and clini-cal features distinct from those in adults5 and will not beaddressed in this review.
Most adult patients with MDS present to their physi-cians with signs and symptoms related to anemia orpancytopenia, or their ill ness is discovered incidentallywhen a blood cell count is performed for another purpose.The diagnosis of MDS is established from the character-istic appearance of a bone marrow aspirate, but in somecases cytologic features may be subtle, creating chal-lenges with respect to excluding nonneoplastic causesof cellular dysplasia. In such cases, genetic testing pro-vides an alternative means of diagnosis confirmation andoffers further insight into prognosis and managementconsiderations.
The 1976 French-American-British (FAB) Co-opera-tive Group classification scheme for MDS, revised andexpanded in 1982, provided the first widely used tool fordisease classification and prognostication.6 The FAB clas-sification is based on the proportion of immature blast cellsin the blood and marrow and on the presence or absence ofringed sideroblasts or peripheral blood monocytosis. In1999, a group of hematopathologists and clinicians operat-ing under the auspices of the World Health Organization(WHO) created a new classification system for MDS basedon the FAB framework but incorporated newer morpho-logic insights and, to a more limited extent, cytogeneticfindings (Table 2).7,8
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com682
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
TABLE 1. Genetic Abnormalities Characteristic of MDS and Their Consequences*
Genetic ormolecular abnormality Functional consequence Importance in MDS
Karyotypic findings
Del(20q), isolated del(5q), Unknown IPSS good-risk markers; del(5q31.1) is associated with–Y, normal karyotype specific 5q– syndrome (female predominance,
dysplastic micromegakaryocytes, thrombocytosis)Complex karyotype, Unknown IPSS poor-risk markers
abnormalities ofchromosome 7
Other karyotypes not listed Unknown IPSS intermediate-risk markers, likely to be subdividedabove in the future as IPSS is revised
Trisomy 8 Unknown Increased risk of leukemic transformation (single-institution studies); male predominance; oralulceration (rare)
Abnormalities of 3q21 translocations are associated with overexpression Decreased survival (single-institution studies)chromosome 1q, of MDS1/EVI1 gene; 11q23 translocations rearrange3q21, and 11q23 MLL gene
Del(12p) Unknown; ETV6 gene at 12p13 is frequently involved Relatively benign prognosis (single-institution studies)in translocations in this region, which may be crypticor associated with deletions
t(8;21)(q22;q22), Leukemogenic rearrangements of core-binding factors WHO classifies cases with these translocations asinv(16)(p13q22) or involved in transcriptional regulation AML by definition, even if they would otherwiset(16;16)(p13;q22), and be consistent with MDSt(15;17)(q22;q12)
Isodicentric X Unknown; ABCB7 at Xq12-13 plays a critical role in Iron accumulation in elderly womeniron homeostasis
t(3;3)(q21;q26) or Rearranges MDS1/EVI1 gene at 3q26 in many cases; Thrombocytosis with megakaryocyte dysplasiainv(3)(q21q26.2) GATA2 at 3q21 is overexpressed in some cases
Isolated isochromosome (17q) Unknown Occasional myeloproliferative features; rapid trans-formation to leukemia and poor response to therapy
Rearrangements of 5q33 PDGFR-β subunit constitutive activation; TEL at CMML with eosinophilia; frequent clinical responsessuch as t(5;12)(q33;p13) 12p13 is a common fusion partner, but many other to imatinib or other PDGF inhibitors; other molecularly
partners have been described defined myelodysplastic-myeloproliferative overlapsyndromes exist, including rearrangements ofPDGFR-α subunit
All metaphases abnormal Marker of clonality Poorer prognosis than patients with mixture of abnormaland normal metaphases
Point mutations
TP53 Mutations result in loss of function of tumor Mutated in 5%-10% of patients with MDS, moresuppressor p53, “the guardian of the genome”— commonly mutated in secondary MDS, may bean essential regulator of cell cycle, specifically associated with progression to AMLtransition from G0 to G1
NRAS Constitutively activates oncogene by preventing Codon 12 mutation is most common in MDS andnormal GTP recycling, resulting in uncontrolled found in 10%-15% of cases; acquisition of mutationgrowth signalling commonly associated with progression to AML
FLT3 Internal tandem duplications of juxtamembrane domain Found in up to 10% of MDS cases; acquisition ofor point mutations result in constitutive activation mutation commonly associated with progression toand uncontrolled growth signalling AML
RUNX1/AML1 Point mutations result in loss of normal trans-activating Most common point mutation described to date inpotential of the key RUNX1 core-binding factor MDS—in up to 25% of cases; associated with highsubunit and consequent changes in gene expression risk of progression to AML, previous radiation
exposure, and chromosome 7 abnormalitiesc-FMS Mutations constitutively activate the receptor for Occasionally associated with CMML
colony-stimulating factor 1, a cytokine that controlsthe production, differentiation, and function ofmonocyte-macrophages
PTPN11 Mutations alter function of the SHP2 that has diverse Rarely associated with CMML or other MDS,roles in cell signalling, including modulation of commonly associated with JMMLPDGFR phosphorylation and STAT activity
ATRX Point mutations result in loss of function of ATRX Acquired α-thalassemia; no apparent effect onmultiprotein complex with consequent changes in proliferative potential of thalassemic clonegene expression, including down-regulation of αglobin cluster, probably by epigenetic mechanisms
*Gene expression changes that have been documented via microarray analyses are not included because their relevance has not yet been established. AML =acute myeloid leukemia; ATRX = α-thalassemia mental retardation X-linked; c-FMS = McDonough feline sarcoma virus oncogene homolog; CMML =chronic myelomonocytic leukemia; FLT3 = fms-related tyrosine kinase 3; GTP = guanosine triphosphate; IPSS = International Prognostic Scoring System;JMML = juvenile myelomonocytic leukemia; MDS = myelodysplastic syndromes; NRAS = neuroblastoma viral rat sarcoma oncogene homolog; PDGFR =platelet-derived growth factor receptor; PTPN11 = protein tyrosine phosphatase, nonreceptor type 11; RUNX1 = runt-related transcription factor 1; SHP2 =SH2 domain-containing protein tyrosine phosphatase 2; STAT = signal transducer and activator of transcription; TP53 = tumor protein p53; WHO = WorldHealth Organization.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 683
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
TABLE 2. World Health Organization Classification of the Myelodysplastic Syndromes*
Disease subtype Blood findings Bone marrow findings
Refractory anemia Anemia Erythroid dysplasia only–ie, notNo blasts or rare (<1%) blasts myeloid or megakaryocytic dysplasiaNo Auer rods <5% blasts<1 × 109/L monocytes <15% ringed sideroblasts
Refractory anemia with Anemia Erythroid dysplasia onlyringed sideroblasts No blasts ≥15% ringed sideroblasts
No Auer rods <5% blasts<1 × 109/L monocytes
Refractory cytopenia with Cytopenias (bicytopenia or Dysplasia in ≥10% of cells in 2 ormultilineage dysplasia pancytopenia) more myeloid cell lines
No or rare (<1%) blasts <5% blasts in marrowNo Auer rods <15% ringed sideroblasts<1 × 109/L monocytes
Refractory cytopenia with Cytopenias (bicytopenia or Dysplasia in ≥10% of cells in 2 ormultilineage dysplasia pancytopenia) more myeloid cell linesand ringed sideroblasts No or rare (<1%) blasts ≥15% ringed sideroblasts
No Auer rods <5% blasts<1 × 109/L monocytes
Refractory anemia with Cytopenias Unilineage or multilineage dysplasiaexcess blasts 1 <5% blasts 5% to 9% blasts
No Auer rods No Auer rods<1 × 109/L monocytes
Refractory anemia with Cytopenias Unilineage or multilineage dysplasiaexcess blasts 2 5%-19% blasts 10%-19% blasts
Auer rods may be present Auer rods may be present<1 × 109/L monocytes
Myelodysplastic syndrome, Cytopenias Unilineage dysplasia in granulocytesunclassified No or rare blasts or megakaryocytes but no erythroid
No Auer rods dysplasia<5% blastsNo Auer rods
Myelodysplastic syndrome Anemia; other cytopenias Normal to increased megakaryocytesassociated with isolated possible with hypolobated nucleidel(5q) <5% blasts <5% blasts
Platelets normal or increased No Auer rodsIsolated del(5q)
*Chronic myelomonocytic leukemia and juvenile myelomonocytic leukemia are classified as myelodysplastic-myeloproliferative overlap syndromes by the World Health Organization.
Modified from Blood.7
TREATMENT OVERVIEW
The current spectrum of treatments for MDS is limited;however, encouraging results with novel agents in develop-ment offer promise.9 For most patients, management isprimarily supportive, relying on transfusions and antimi-crobials as dictated by symptoms and infectious complica-tions. Select patients will experience hematologic improve-ment with the use of recombinant hematopoietic growthfactors, including erythropoietin and granulocyte colony-stimulating factor.10,11
With the advent of new therapeutic alternatives, themanagement strategy for many patients has shifted fromsole reliance on supportive measures to more active inter-vention. The Food and Drug Administration recently ap-proved the first agent with an indication for MDS, 5-
azacitidine (Vidaza, Pharmion Corporation, Boulder,Colo), an injectable nucleoside analogue that covalentlyincorporates into DNA and depletes DNA methyltrans-ferases to promote genome hypomethylation. This maycontribute to reactivation of methylation-silenced tumorsuppressor genes. In a national cooperative group open-label randomized trial of MDS, 5-azacitidine treatmentdelayed leukemic transformation and reduced the risk ofAML progression or death.12 Most other noninvestigationalagents offer limited benefit for the general population withMDS but are reasonable considerations for select individu-als. For example, thalidomide, when administered at lowdoses for an extended schedule, may restore erythropoiesisin some patients; however, neurotoxicity and other adverseeffects limit dose escalation and prolonged drug adminis-tration, particularly in elderly individuals.13 Antithymocyte
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com684
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
globulin and other immunosuppressants may be effectivein patients with hematopoietic inhibitory immune effec-tors; such patients may be identified through predictivemodelling.14-16 Older agents such as androgens and pyri-doxine are usually ineffective.17,18 Aggressive chemother-apy similar to that used for acute leukemia should be re-served for clinical trials; it is rarely curative.19
Younger patients are often candidates for curative strat-egies such as allogeneic hematopoietic stem cell transplan-tation; however, mortality and morbidity remain high, evenin experienced and specialized centers.20 Autologous trans-plantation may benefit selected patients without an alloge-neic donor, but the potential benefit of this approachappears limited to younger patients.21 Unfortunately, thevast majority of patients with MDS are not candidates forstem cell transplantation with conventional ablative con-ditioning regimens because the median age at the time ofdiagnosis is in the seventh decade of life, and comor-bidities are common. Reduced-intensity conditioning ornonmyeloablative approaches promise to expand the up-per age limit of candidates for stem cell therapy.20,22 Theoptimal timing of transplantation is a subject of activeinvestigation.23
Iron overload remains a clinical challenge, especially inpatients who require frequent red blood cell transfusions,emphasizing the need for iron chelation therapy for patientswith otherwise favorable prognostic features in whom ex-tended survival is expected. Given the paucity of disease-altering therapies for MDS, clinical trial enrollment is para-mount to advance the field. At least 2 agents in clinicaldevelopment, the immunomodulatory drug lenalidomide(CC-5013, Revlimid; Celgene Corporation, Warren, NJ)and the demethylating agent decitabine (Dacogen, Super-gen, Inc, Dublin, Calif), have shown promising preliminaryresults, and Food and Drug Administration review shouldoccur in the months ahead.24,25
STANDARD CYTOGENETIC STUDIES ANDTEST RATIONALE
At present, the most widely available genetic test applied inthe evaluation of patients with MDS is cytogenetic analysisby conventional metaphase karyotyping. Karyotyping hasbeen applied widely since the 1970s, and the method forperforming these assays and their limitations have beenreviewed recently.26,27 Briefly, standard cytogenetic assaysinvolve light-microscopic visualization of metaphase chro-mosomes prepared by (1) inducing the cells of interest todivide, (2) arresting their division at the appropriate mitoticstage with colchicine, (3) lysing the cells, and (4) Giemsastaining of the chromosome spread to resolve the chromo-some size and banding pattern (Figure 1).
In diagnostically ambiguous cases, an abnormal kar-yotype can provide important evidence to support thepresence of a clonal, neoplastic process.28 Additionally, cy-togenetic studies provide important prognostication dis-crimination. The 1997 International Prognostic ScoringSystem (IPSS) for MDS, based on a review of 816 patientswith “primary” MDS (ie, no history of treatment with che-motherapy or radiotherapy), incorporates 3 elements withindependent prognostic power into the staging algorithm:(1) the proportion of myeloblasts in the patient’s marrow,(2) the number of blood cell lineage deficits, and (3) thetype of chromosomal abnormality present.29 Using these 3elements, a score generated by the IPSS algorithm repro-ducibly classifies patients with MDS into a highest-riskgroup with a median survival of only 0.4 years, a pair ofintermediate-risk groups, and a lowest-risk group with amedian survival of 5.7 years overall, 11.8 years for patients60 years of age or younger. The IPSS algorithm has beenvalidated independently.30,31
The IPSS clusters the varied chromosomal abnormali-ties observed in MDS into 3 risk groups: poor risk (includ-ing abnormalities of chromosome 7 or complex karyotype[≥3 clonal abnormalities]), good risk (including a normalkaryotype, isolated interstitial deletion of the long arm ofchromosome 5 [del(5q)], chromosome 20q interstitial dele-tions [del(20q)], or clonal loss of the Y chromosome, seenin 7.7% of otherwise healthy elderly men32), and intermedi-ate risk (including all other abnormalities not defined asgood or poor).29 The corresponding median survival bycytogenetic risk group was 0.8 years (poor risk), 2.4 years(intermediate risk), and 3.8 years (good risk) (Figure 2).29
The IPSS is an important clinical tool and maintainsprognostic validity for both standard therapy and alloge-neic stem cell transplantation. In one analysis, patients witha poor-risk cytogenetic pattern had a 3.5-fold greater risk ofrelapse after stem cell transplantation than did patients witha good-risk karyotype.33 Similar findings have been re-ported for patients treated with intensive antileukemic che-motherapy, with or without subsequent transplantation.19,34
Not surprisingly, acquisition of higher-risk IPSS cytoge-netic abnormalities during the course of disease adverselyimpacts survival because of leukemic evolution or cyto-penic complications.35
COMMON CYTOGENETIC ABNORMALITIES IN PRIMARY MDSAlthough not specific for MDS, the recurrent chromosomalabnormalities defined by the IPSS (ie, –7/del(7q), del(5q),del(20q), and –Y) are among the most common detected inMDS. Overall, 40% to 50% of patients with primary MDSpresent with 1 or more clonal karyotypic abnormalities,whereas in those with secondary MDS (ie, after therapeuticchemotherapy or radiotherapy for an unrelated condition),
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 685
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
FIGURE 1. Conventional cytogenetic study of bone marrow cells in a patient with amyelodysplastic syndrome (MDS). This abnormal karyotype includes several abnormalitiesassociated with MDS, including numerical abnormalities (trisomy 8 and monosomy 17[arrowheads]), and 2 common deletions (deletions of the long arm of chromosome 20 andof the long arm of chromosome 5 between bands q13 and q33 [arrows]). Because morethan 3 abnormalities are present, this karyotype is considered complex. Photographcourtesy of Jack L. Spurbeck, Cytogenetics Laboratory, Mayo Clinic, Rochester, Minn.
the proportion of patients with an abnormal karyotype ex-ceeds 80%.2,28,31,36-38 The relative frequency of specific cyto-genetic abnormalities in primary MDS ranges from as highas 30% for del(5q)—either as an isolated anomaly (10%) oras part of a more complex karyotype (20%)—to 20% fortrisomy 8 and 15% for monosomy 7.39 Numerous otherrecurrent abnormalities have been observed, but each ac-counts for less than 10% of cases of primary MDS.
CYTOGENETIC ABNORMALITIES IN SECONDARY MDSThe distribution of chromosome abnormalities is skewed intreatment-related MDS, in which structural or numericaldeletions of chromosome 7 (40%) and chromosome 5(40%) predominate.36,39 Together, abnormalities of chro-mosome 5 and 7 account for approximately 75% of karyo-typic abnormalities in secondary MDS,36 whereas all otherkaryotypic abnormalities occur with a frequency of 10% orless.39 In addition to the higher frequency of abnormalkaryotypes, secondary MDS displays a disproportionatepercentage of IPSS poor-risk abnormalities, and as withprimary MDS these are associated with an unfavorableprognosis. This cytogenetic pattern is frequently linked toand believed to be induced by prior treatment with alkylat-ing antineoplastics.36
The IPSS good-risk abnormalities occur with sufficientrarity in secondary MDS to raise suspicion that such cases
instead represent de novo and treatment-unrelated MDS.Nevertheless, single-institution studies indicate that patientswith such karyotypes fare better than their counterparts withsecondary disease who have poor-risk karyotype abnormali-ties.36 When the spectrum of abnormalities associated withprimary and secondary MDS is compared, secondary formsmore commonly exhibit monosomy 5, monosomy 7, andder(17p) aberrations, whereas in primary MDS, isolateddel(5q) and normal karyotype predominate.39 Treatmentwith topoisomerase II inhibitors has been linked to chromo-some 3q inversions or translocations and to balanced translo-cations involving 11q23 deregulating the MLL gene.40,41
OTHER RECURRENT CYTOGENETIC ABNORMALITIES IN MDSNumerous chromosomal abnormalities occur with moder-ate frequency (ie, 1%-10%) in MDS; however, because ofoverall low prevalence, their prognostic relevance remainsundefined. Limited case series have linked trisomy 8 withan increased risk of AML transformation, and abnormali-ties of chromosome 1q, 3q21, and 11q23 with an overallinferior survival.30,31,40,42 In contrast, del(12p) as a sole ab-normality has been associated with an indolent diseasecourse.31 The prognostic relevance of less common (ie,<1% of cases) yet recurrent chromosomal abnormalitiesremains uncertain.43-47 Although multiple independent andkaryotypically discordant clones may be identified in se-
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com686
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
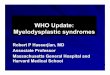
FIGURE 2. The International Prognostic Scoring System for myelodysplastic syndromes (MDS)predicts survival time (top) and time to leukemic transformation (bottom) based on the patient’sbone marrow karyotype. These Kaplan-Meier curves show that the highest risk of death andleukemia is in patients with MDS with chromosome 7 abnormalities (Chrom 7 abn) or a complexkaryotype; the lowest risk is associated with loss of the Y chromosome, isolated interstitialdeletion of the long arm of chromosome 5, a normal karyotype, or chromosome 20q interstitialdeletions [del(20q)]. Data were derived from a review of 816 patients with primary MDS. AML =acute myeloid leukemia; Misc = miscellaneous. From Blood,29 with permission.
lected cases,48,49 their prognostic importance is believed tobe influenced by the highest-risk karyotype. The MitelmanDatabase of Chromosome Aberrations in Cancer, part of theCancer Genome Anatomy Project of the National Cancer
Institute, includes a comprehensive catalogue of chromo-some abnormalities in patients with MDS that can be ac-cessed at: http://cgap.nci.nih.gov/Chromosomes/Mitelman(accessibility verified March 29, 2005).
100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
1 2 3 400
6 7 8 9 10 131211 14 15 16 17 185
1 2 3 40 6 7 8 9 10 131211 14 15 16 17 185
del(5q)Normaldel(20q)Misc. single+8DoubleMisc. doubleChrom 7 abnMisc. complexComplex
–Y 17 (2)48 (6)
489 (60)16 (2)74 (9)38 (5)
14 (2)10 (1)15 (2)66 (8)
29 (3)
No. (%)of patients
Year
Year
Perc
enta
ge
Survival
AML evolution
Perc
enta
ge
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 687
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
The karyotypic diversity included in the Mitelman data-base illustrates that the diagnostic category of MDS con-tains disorders that phenotypically overlap yet have a mo-lecularly distinct pathobiology. Although the IPSS hasproved its clinical usefulness, the IPSS intermediate-riskcategory includes potentially hundreds of chromosomalabnormalities, suggesting that further refinement of thealgorithm will be possible. As therapy for MDS improves,the prognosis associated with particular karyotypes maychange. By analogy, before the introduction of retinoic acidtherapy for acute promyelocytic leukemia (APL) in the1980s, the classic t(15;17) APL-associated chromosomaltranslocation was regarded as an intermediate-risk leuke-mia karyotype, but with modern drug therapy APL isamong the most curable AML subtypes.50
Although balanced favorable translocations such ast(15;17) and t(8;21) are relatively common in AML, they arerare in MDS in which deletions and numerical chromosomalabnormalities predominate.2,29,51 Given the responsiveness toconventional leukemia chemotherapy, the WHO categorizes4 specific rearrangements involving core-binding factor tran-scriptional repressors [ie, t(8;21)(q22;q22), inv(16)(p13q22)or t(16;16)(p13;q22), and t(15;17)(q22;q12)] as AML, re-gardless of the bone marrow myeloblast percentage.7,8 Forthose exceptional cases that harbor such karyotypic abnor-malities with a low myeloblast burden, it remains unclearwhether AML therapy impacts survival as it does in moretypical AML. 52,53
CLONAL CYTOGENETIC ABNORMALITIES IN THE ABSENCE OF
MORPHOLOGIC EVIDENCE OF MYELODYSPLASIA
In selected cases in which marrow aspiration is performedfor evaluation of cytopenias, routine staging, or follow-upof another malignancy, clonal karyotypic abnormalities maybe identified in the absence of cytologic dysplasia that wouldsupport a diagnosis of MDS.54 The constitutional karyotypein nonhematopoietic tissue in such cases has been normal,confirming an acquired somatic cytogenetic abnormality.This constellation of findings may represent a forme frusteof MDS,54 evidenced by an increased risk of leukemic trans-formation and subsequent cytopenic mortality.54 These un-common cases emphasize the importance of cytogeneticevaluation in the investigation of unexplained cytopenias,even in the absence of overt morphologic evidence of MDS.
RELEVANCE OF ALL ABNORMAL VS ABNORMAL-NORMAL
CYTOGENETIC PATTERN
When a chromosomal abnormality is detected by conven-tional cytogenetics, the abnormality may be present in allexamined metaphases (all abnormal [AA]) or in only afraction of the metaphases (sometimes termed abnormal-normal [AN]).28,35 The AA pattern correlates with higher-
risk MDS subtypes identified by the FAB MDS pathologicclassification,6 and patients with AA have a poorer overallsurvival than those with AN.28
The favorable modifying effect of increasing propor-tions of normal metaphases has precedent in other hemato-logic malignancies. The clinical usefulness of the reduc-tion in the number of abnormal metaphases with therapy isperhaps best illustrated by chronic myeloid leukemia(CML). In CML, a “major cytogenetic response” repre-sents an important therapeutic goal because patients whoachieve a complete cytogenetic remission experience asuperior progression-free survival compared with thosepatients with persistence of any proportion of metaphasesbearing the Philadelphia chromosome.55-57 By analogy, aninternational working group that created standardized re-sponse criteria for clinical trials of MDS included reduc-tions in the number of abnormal metaphases as one of theseresponse criteria, although the clinical importance of thismeasurement had not yet been formally established inMDS.58 Evidence from recent clinical trials testing newpotentially disease-modifying agents supports this notion.In a large phase 2 study of intravenous decitabine inhigher-risk MDS, 31% of patients achieved a completecytogenetic remission, with a corresponding reduction inthe relative risk of death (0.38 compared with those inwhom the abnormal clone persisted).59 These preliminarydata suggest that a cytogenetic response may also be animportant disease-modifying marker in MDS.
BONE MARROW VS PERIPHERAL BLOOD CYTOGENETIC STUDIES
IN MDSMost chromosomal studies in patients with MDS are per-formed on bone marrow cells. Peripheral blood karyotyp-ing has a higher failure rate than marrow studies and rarelyadds useful information beyond that available from themarrow study.37 Unlike CML, in which tracking the pro-portion of cells containing the Philadelphia chromosomeor its molecular equivalent is critical for monitoring ther-apy and the results may prompt management changes inthe absence of the need for an additional marrow aspira-tion, there is currently little compelling clinical indicationfor frequent assessment of chromosomal status in MDS. Inspecial situations in which chromosomal information isdesirable but a marrow examination is not required, such asmeasuring donor/host chimerism after stem cell transplan-tation, fluorescent in situ hybridization (FISH) assays (dis-cussed subsequently) may be preferable.
INDICATIONS FOR CYTOGENETIC TESTING IN MDS
When should a karyotype be obtained for patients withMDS? Given the importance of the IPSS risk assessment, a
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com688
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
chromosomal study is an essential part of the initial evalua-tion (Table 3). Acquisition of new chromosome abnormali-ties (ie, cytogenetic evolution) portends disease progres-sion and therefore justifies cytogenetic evaluation in theroutine management of MDS. Some clinicians obtain acytogenetic study every time a marrow aspiration is per-formed during the care of patients with MDS, whereasothers obtain such studies only in relationship to plannedtherapeutic trials or when there are signs of a change in thepatient’s condition. No evidence base exists to help guidethis practice, and therefore such decisions are best left tothe discretion of the individual treating clinician. Aftertransplantation, karyotypic analysis may not only help inearly determination of relapse (ie, before morphologic evi-dence of recurrent disease is present) but also is useful inassessment of donor-host chimerism in the case of sexmismatches between marrow donor and host.
MOLECULAR CYTOGENETICS IN MDS
Delineating the pathogenetically relevant alterations inMDS at the gene level, even for recurrent cytogeneticabnormalities, has proved challenging. The so-called 5q–syndrome is perhaps the best example of the difficultiesfaced. First delineated in the early 1970s, 5q– syndrome isa form of refractory anemia characterized by female pre-dominance, atypical megakaryocytes, erythroid hypoplasiawith red blood cell transfusion dependence, and a low risk ofleukemic transformation with prolonged survival. Theseclinical and pathological features are consistently associatedwith an isolated interstitial deletion of the long arm of chro-mosome 5 that involves 5q31.1.60,61 Although earlier reportsvaried in the definition of the 5q– syndrome, general consen-sus is that this description should be limited to patients with
an isolated 5q31.1 interstitial deletion in the absence of othercytogenetic abnormalities, a low bone marrow blast percent-age, and no history of genotoxic therapy.62
The WHO’s most recent classification schema for ma-lignant hematopoietic diseases formally recognizes 5q–syndrome as a discrete entity within the general category ofMDS.7 Although no other specific MDS-associated chro-mosome aberration has been recognized by the WHO as adistinct pathologic and clinical syndrome, other recurrentchromosome abnormalities have been linked with specificdisease features. For example, isolated isochromosome 17qmay be associated with myeloproliferative features andpoor response to therapy,63 isodicentric X has been linkedto iron overload in older women,64 trisomy 8 displays amale predominance,65-67 and inv(3)(q21q26.2) is associatedwith thrombocytosis with megakaryocytic dysplasia andpoor therapeutic response.42,68
Boultwood and colleagues at Oxford have carefully de-fined the commonly deleted region (CDR) in patients with5q– syndrome using FISH and other molecular mappingtechniques, and they have cloned several novel genes in theprocess.69-72 The defined CDR spans 1.5 megabase pairs at5q31.1.71 This CDR is relatively gene rich, containing noless than 40 discrete genes, 33 of which are expressed inearly hematopoietic cells.71 Several of these genes aremembers of the interleukin family or have other potentialpromoting roles in hematopoiesis. A number of geneswithin the CDR are not well characterized, and their func-tion is as yet unknown. To date, systematic sequencing ofthese genes in patients with 5q– syndrome has not re-vealed pathogenetic mutations, and thus it is now be-lieved that the pathophysiology of 5q– syndrome mayrelate to gene dosage rather than mutational gene deregu-lation in the CDR.
TABLE 3. Summary of Genetic Test Indications in Myelodysplastic Syndromes*
Conventional cytogenetics FISH
Screening No NoAt diagnosis
Bone marrow Yes Testing for 5q deletions may predict response to lenalidomide,24
Blood Not necessary unless patient refuses and panel FISH testing is reasonable if cytogenetic study isbone marrow examination inadequate
During therapyBone marrow If the patient is enrolled in a clinical study, If FISH was performed at diagnosis and the patient is enrolled
otherwise no compelling indication in a clinical study, otherwise no compelling indicationAfter hematopoietic
stem cell transplantationBone marrow At 3-6 mo and thereafter as indicated May be useful to assess chimerism in donor-recipient sex
mismatch or to assess for early relapse if FISH abnormalityis present before transplantation
Blood No May be useful for minimally invasive assessment ofchimerism and early relapse
Leukemic transformationBone marrow Yes No clear role
*See text for test interpretation. FISH = fluorescent in situ hybridization.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 689
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
Other groups are investigating additional recurrentMDS-associated chromosome abnormalities in an attemptto identify critical gene targets, including del(20q), trisomy8, del(7q), and del(9q). In selected cases, study of patientswith parallel inherited disorders may provide insight. Forexample, patients with constitutional trisomy 8 mosaicismappear to have a high risk of developing myeloid malignan-cies including MDS and leukemia.73 Chromosome 7 may beparticularly challenging because there are multiple CDRs,including 7q22 and several in the region 7q31-7q35.74-76
Perhaps the most important molecular cytogenetic dis-covery in recent years with immediate therapeutic implica-tion is the reciprocal chromosome translocation involvingchromosome 5q33, where the gene encoding the β subunitof the platelet-derived growth factor receptor (PDGFR-β)is located. Although a number of chromosomes and genesmay partner with 5q33, the clinical phenotype is distinctand is now recognized by the WHO classification aschronic myelomonocytic leukemia (CMML) with eosino-philia (CMML-Eos). (The WHO classification removed allCMML subtypes from the MDS group, where they hadbeen placed in the widely used 1982 FAB MDS classi-fication, and placed them in a separate myelodysplastic/myeloproliferative overlap category. This was done be-cause patients with CMML frequently exhibit prominentmyeloproliferative features, unlike patients with other sub-types of MDS.6,7,77) The CMML-Eos phenotype arises fromthe generation of novel fusion transcripts with constitutiveactivation of the PDGF-β receptor tyrosine kinase.78-82
Transgenic mouse models have shown that these novel re-ceptor tyrosine kinase fusion genes are singularly respon-sible for the generation of these myelodysplastic/myelopro-liferative disorders and are selectively responsive to PDGFRkinase inhibitors such as imatinib (Gleevec, Novartis, Basel,Switzerland).79,83,84 Several patients with CMML-Eos havebeen reported to achieve rapid hematologic control and sus-tained cytogenetic remission with imatinib monotherapy85 ortreatment with SU11657, an experimental agent that alsoinhibits PDGF signalling.86
FLUORESCENT IN SITU HYBRIDIZATION
Although conventional cytogenetic analysis remains thestandard for purposes of diagnosis and prognosis in MDS,interest is increasing in the application of more sensitivetechniques such as FISH. Reviews of FISH applicationsin hematologic malignancies have been published re-cently.27,87 Briefly, FISH involves hybridization of patientgenetic material with a fluorescently labelled DNA probedesigned to anneal either to specific DNA sequences or tochromosomal features such as centromeres. The advan-tages of FISH include its applicability to either peripheralblood or bone marrow, the opportunity to analyze inter-
phase cells instead of only dividing cells, and the capacityto analyze substantially more cells than is possible byconventional cytogenetic analysis. When chromosomal rear-rangements are present in only a small subset of neoplasticcells, a common situation in MDS, FISH can offer increasedsensitivity over conventional cytogenetics. For purposes ofinvestigation of specific MDS-associated chromosomal de-letions, FISH probes are extremely useful for narrowing thecommon CDRs,71,74,76,88-91 and they can also identify the pre-cise types of cells involved in the neoplastic process.90,92-98
Several groups have developed FISH “panels” that aredesigned to detect the chromosome abnormalities mostcommonly identified in patients with MDS, such as thoseinvolving chromosomes 5, 7, 8, 11, 13, and 20.99,100 SuchFISH analyses in MDS occasionally reveal cryptic cytoge-netic abnormalities that are not recognized on metaphaseanalysis.101-103 However, conventional cytogenetics andFISH should be viewed as complementary because thereare also abnormalities better detected by conventional cy-togenetics than FISH.100,103-105
Many of the abnormalities detected by FISH that are notalways recognized by conventional cytogenetics are amongthose included in the IPSS (eg, monosomy 7106) or thosefound by other groups to have prognostic importance inMDS (eg, trisomy 8102,106 and 12p rearrangements101). Chro-mosome aberrations detected only by FISH have not yetbeen shown to have the same prognostic importance asthose revealed by conventional cytogenetics, and thus atpresent there is no compelling clinical reason to performFISH at the time of diagnosis of MDS if the karyotype issuccessful. However, because the critical molecular defectis likely to be the same regardless of how the chromosomalbreakpoint is detected, specific high-yield FISH assays willprobably be incorporated eventually into prognostic andtreatment-response algorithms,107 as in CML.26,108 For ex-ample, in the European clinical trial of decitabine for MDS,2 patients had chromosomal responses detected by FISHthat correlated with clinical and cytogenetic response.59
If standard karyotyping is unsuccessful because of afibrotic marrow, failure of aspirated cells to grow in cul-ture, or other technical problems, it is reasonable to resortto FISH using a panel designed to detect abnormalitieswith recognized prognostic relevance. Additionally, inview of the promising recent findings by List et al24 of ahigh rate of complete hematologic and cytogenetic re-sponse to lenalidomide therapy in patients with MDS with5q31.1 deletions, it may be especially valuable to performFISH directed at detection of loss of the CDR on chromo-some 5, particularly when the marrow morphologic fea-tures suggest 5q– syndrome. Patients with cryptic 5q dele-tions might then be referred for appropriate clinical trials.Over time, as the presence of other cytogenetic abnormali-
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com690
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
ties is correlated with response to novel therapies, the roleof specific FISH tests in MDS is likely to expand.
MULTICOLOR FISH AND SPECTRAL KARYOTYPING
“Chromosome painting” methods such as multicolor FISH(M-FISH) or spectral karyotyping (SKY) offer the ability toanalyze all human autosomes and sex chromosomes at thesame time by labelling metaphase cells with band-selectivecolor probes (Figure 3).109,110 These methods offer greatersensitivity than conventional karyotyping and are useful forcharacterizing cryptic chromosomal rearrangements and theorigin of structurally ill-defined chromosomal material suchas “marker” chromosomes, in which the normal counterpartis not readily identified because of an ambiguous bandingpattern.
Despite the heightened power of discrimination that M-FISH and SKY technologies may offer,111 their clinicalusefulness in MDS has yet to be proved. For example, inpatients with MDS with a normal karyotype by conventionalcytogenetics, unrecognized cryptic abnormalities are rarelyidentified by M-FISH or SKY.99,100,112 In contrast, additionalrearrangements are often detected when chromosome paint-ing methods are performed in patients with MDS with abnor-mal karyotypes109,111,113-116; however, the clinical relevance ofthese abnormalities is as yet undefined.
COMPARATIVE GENOMIC HYBRIDIZATION
Comparative genomic hybridization (CGH) is a new tech-nique that applies fluorescent hybridization to detect differ-ences in DNA copy number between a patient sample and anormal control, giving insight into loss or gain of chromo-somal segments.117 The ratio of the signal strength from thepatient DNA to the reference DNA is measured in eachchromosomal region. Until recently, the resolution of CGHwas limited and only allowed detection of chromosomalgains or losses of 20 megabase pairs or greater. Despitethis, even first-generation CGH probes provided sufficientsensitivity to discover cryptic rearrangements in patientswith myeloid diseases including MDS, and soon the resolu-tion had improved to almost 1 megabase pair.118,119 Newerarray-based CGH methods, including a recently describedtiling array that maps the entire human genome with morethan 30,000 clones, promise to improve sensitivity suffi-cient to resolve even minute DNA alterations.117,120
POINT MUTATIONS IN MDS
Conventional cytogenetic studies and FISH probes detectlarge chromosomal rearrangements. However, isolatedbase pair changes or so-called point mutations may alsoinactivate or result in constitutive gain of function of theaffected gene, with important biological consequences.
Discovery of these mutations is one of the major openfrontiers in MDS molecular pathology, with initial investi-gations focusing on recognized tumor suppressor genes.
TP53The tumor suppressor gene TP53, a critical cell-cyclecheckpoint regulator, was the first gene evaluated in MDSbecause of its high frequency of inactivation in solid tu-mors. In myeloid malignancies such as MDS and AML,TP53 mutations are uncommon, detected in no more than15% of patients with primary MDS, with a higher fre-quency in atomic bomb survivors and patients treated pre-viously with chemotherapy or radiotherapy.121-130 Such mu-tations are generally demonstrable at the time of diagnosisand may have independent prognostic value.128,131
Even in tumor types in which TP53 mutations are com-mon, TP53 mutation testing is rarely performed in clinicalpractice, unless a germline mutation leading to a generalcancer susceptibility syndrome (the Li-Fraumeni syn-drome) is suspected. This is primarily because patientswith TP53-mutant neoplasias have not yet been shown tobenefit from differential clinical management. For both in-herited and acquired mutations, direct genetic analysis ofTP53 by sequencing is required because immunohis-tochemical results do not correlate well with mutation sta-tus.132,133 Newer high-throughput technology may change thecost-benefit analysis of TP53 mutation screening and makethis assay more accessible to clinicians (although its useful-ness remains to be determined). For instance, denaturinghigh-performance liquid chromatography, which separateswild-type and mutant DNA on the basis of the differentialaffinity of DNA heteroduplexes and homoduplexes onpolystyrene beads coated with a gradient of organic sol-vents, has shown promise as a more rapid TP53 screeningmethod in MDS and other tumors134 (D.P.S., unpublisheddata, 2004).
NRAS AND FLT3The RAS proto-oncogene superfamily encodes guanosinetriphosphate hydrolases (GTPase) that are critical regula-tors of cellular growth-related signals. Three RAS proto-oncogenes (H, N, and K) encode four 21-kd G proteins,including 2 alternatively spliced K-Ras products that areposttranslationally modified before incorporation into theinner leaflet of the plasma membrane. RAS mutations occurat critical regulatory sites (eg, codons 12, 13, and 61) thatinactivate the GTPase response normally stimulated by thebinding of GTPase-activating proteins, thereby extendingthe half-life and signalling activity of the Ras-GTP boundmutant. In myeloid malignancies, NRAS mutations pre-dominate, especially a common mutation in codon 12;nonetheless, the frequency of activating RAS mutations in
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 691
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
unselected cases of MDS is relatively low, ranging from10% to 15% of MDS. In contrast, in CMML, RAS muta-tions are found in 40% to 60% of patients and are believedto contribute to growth factor hypersensitivity of myelo-monocytic progenitors.130,135-139
Internal tandem duplications and other constitutively ac-tivating mutations of the receptor tyrosine kinase FLT3 arecommon in AML but are relatively rare in MDS.130,138,140-143
Acquisition of NRAS and/or FLT3 mutations has been asso-ciated with progression of MDS to AML.137,138,140
RUNX1/AML1The most common point mutations detected in MDS todate are those involving the core-binding–factor subunitRUNX1/AML1.144-151 In leukemia, this transcription factorand oncogene is involved in common balanced transloca-tions such as t(8;21), which leads to formation of aberrantlyactive chimeric fusion proteins and uncontrolled cellgrowth. Although early reports estimated that RUNX1/AML1 mutations were rare in MDS,148 more recent studieshave described these mutations in as many as 25% ofpatients,150 and single-institution studies have associatedRUNX1/AML1 mutation status with chromosome 7q abnor-malities,149 more advanced forms of MDS,150,151 and a highrisk of progression to overt leukemia.150,151
ATRXSpecific gene mutations may be associated with uniqueMDS phenotypes. For instance, the rare complication of
acquired α-thalassemia (hemoglobin H disease) arising inthe context of MDS was recently linked to mutations in theATRX gene at Xq13.1.152,153 Inherited mutations in ATRXcause a mild form of α-thalassemia and severe syndromicX-linked mental retardation,154 whereas acquired somaticATRX mutations create a severe imbalance in globin syn-thesis, a large proportion of hemoglobin H-containingcells, and the unusual finding of microcytic, hypochromicred cell indices.152,153,155 The distinct behavior of mutationslike ATRX when they are acquired in the context of MDS,rather than inherited in the germline, may offer importantinsights into MDS pathobiology.155
MUTATIONS FOUND PREDOMINANTLY IN CMMLIn addition to having unique clinical features and uniquechromosomal translocations [such as the t(5;12) PDGFRβ-TEL fusion], CMML has several point mutations thatappear with great frequency but are uncommon in otherMDS subtypes. Patients with CMML have a high fre-quency of activating RAS mutations and a disproportion-ately higher frequency of c-FMS point mutations, althoughthe latter are rare overall in myeloid disorders.156,157 Like-wise, mutations in the protein tyrosine phosphatase genePTPN11 (which cause a form of Noonan syndrome wheninherited) are extremely uncommon in MDS in general,more common in CMML, and especially common (ie,34% frequency) in the pediatric syndrome juvenile myelo-monocytic leukemia, which shares some features withCMML.158,159
FIGURE 3. Multiplex fluorescent in situ hybridization (M-FISH) study of a patient with a malignant myeloid disorder. Conventional G-bandedcytogenetic analysis (left) was karyotyped as 46,X,t(X;1)(q24;q25),t(6;8)(q25;q24.1),11,13,add(15)(q26),12mar[19]/46,XX[1].32 M-FISH analysisconfirmed the t(X;1) and t(6;8), identified the 2 markers as der(13)t(11;13), and identified the add(15) as a der(15)t(13;15). In addition,t(9;11)(p21;q23) was detected, involving chromosome 9 and one of the marker chromosomes, and was confirmed as an MLL gene rearrange-ment. Arrows designate the abnormal chromosomes. Photograph courtesy of Rhett P. Ketterling, MD, Division of Laboratory Medicine and Pathol-ogy, Mayo Clinic, Rochester, Minn. From Br J Haematol,109 with permission.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com692
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
PROSPECTS FOR A MOLECULAR CLASSIFICATION OF MDSAlthough the association of unique disease subtypes withspecific point mutations promises molecular clarity for theperplexing heterogeneity of MDS, the prospect of a mo-lecular classification to replace the current morphologic-and cytogenetics-based WHO scheme threatens to be un-wieldy. For example, one of us (D.P.S.) recently detectedacquired, clonally restricted point mutations in the GATA1gene (chromosome Xp11.23) and RUNX1/AML1 gene(chromosome 21q22.3) as well as a cancer-associatedgermline polymorphism in TP53 (chromosome 17p13.1) ina single patient with MDS with acquired thalassemia butwithout a demonstrable ATRX mutation—a phenotypeseemingly unrelated to the patient’s karyotype of trisomy 8and del(20q) (Figure 4).
The frequencies of specific point mutations describedpreviously are likely to be underestimates. Unlike AML, inwhich the marrow is almost completely replaced by neo-plastic cells, blood and marrow in MDS include a heteroge-neous mix of neoplastic and residual normal cells, anddirect sequencing may be sensitive only to mutant DNAencompassing at least 20% to 30% of the tested sample.Techniques such as denaturing high-performance liquidchromatography, denaturing gradient gel electrophoresis,and polymerase chain reaction–single-strand conforma-tional polymorphism are more sensitive to mosaicism thandirect sequencing.153,160-162 In addition, for a more accurateestimate of mutation frequency, it is important not only toassay genes of interest at the genomic DNA (gDNA) levelbut also the gene message since messenger RNA splicingvariants are common causes of human disease.163
Mutations that affect splicing can be missed if sequenc-ing of gDNA is limited only to the coding region (exons)because splicing abnormalities frequently arise from muta-tions residing in introns, both within the consensus splicedonor and acceptor sites and outside of these areas (ie, inintronic splice enhancer or inhibitor sites). In the case ofATRX, patients with MDS with clonally restricted splicingabnormalities predicted to result in loss of critical ATRXprotein domains have been described, but in all of thesecases the causative mutation has not yet been identified atthe gDNA level.155,164 A mutation in a cryptic splice en-hancer or inhibitor element at some distance from the siteof the splicing abnormality is likely responsible. The ex-pensive and time-consuming search for splicing mutationsand missense mutations as well as the need to use a tech-nique sensitive to mosaicism illustrates why point mutationdetection in MDS has not yet become mainstream.
MITOCHONDRIAL GENE MUTATIONS IN MDSA recent report of mutations in the mitochondrial genomein patients with MDS, including frequent mutations in the
cytochrome-c oxidase genes, generated some excitementbecause it offered an alternative genomic source poten-tially contributing to the MDS phenotype.165 Mitochondriaare a logical target for MDS mutation analysis, given thepresence of ringed sideroblasts—pathological iron-ladenmitochondria—in many patients, which suggests a possiblecommon metabolic disturbance in mitochondrial enzymessuch as cytochrome.166 Mitochondrial enzymes are en-coded by both the 16.6 kilobase pair mitochondrial ge-nome and the nuclear genome. However, another group ofinvestigators sequenced the entire mitochondrial genomein 10 patients with MDS and were unable to reproduce thefindings.167 Several amino acid changes were found inpatients but not controls, but the investigators suggestedthat this might be a reflection of limited clonality amonghematopoietic stem cells rather than an indication of mi-tochondrial genome instability.167 Subsequently, a novelsomatic mutation of mitochondrial transfer RNA was de-tected in a patient with MDS,168 and work continues in thisarea.
FUNCTIONAL IMPORTANCE OF POINT MUTATIONS IN MDSIn each of the genetic mutations described previously,functional consequences arise from modification of theprotein encoded. For instance, RUNX1/AML1 point muta-tions alter DNA binding and transactivating potential of themutant RUNX1/AML1.147 In light of the inherent genomicinstability in MDS, “innocent bystander” mutations, ie,those with no known functional consequence, may occurwith equal or greater frequency. Patients with MDS some-times have clonally restricted gene mutations that do notresult in amino acid substitutions and have no obviouseffect on transcript splicing (Figure 4). If there is no detri-mental effect on cell survival, darwinian pressure in themarrow will not select against hematopoietic clones bear-ing this class of mutation. ATRX mutations may be anexample of a neutral mutation with a readily discerniblephenotype (ie, defective α globin production in redcells).153,155 A vast number of point mutations likely awaitdiscovery in MDS. The task of determining which of theseare important in the pathobiology of the disease will bechallenging.
GENE EXPRESSION PROFILING
A gene need not be altered structurally to modify its ex-pression and affect normal cellular homeostasis. One of theprincipal ways in which gene expression can be altered isthrough epigenetic modification, including changes in theway DNA and its associated histones are packaged intochromatin, and, as a consequence, the accessibility of thatDNA for transcription. The term epigenetic refers to heri-
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 693
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
Patient’sblood
Patient-derivedlymphoblastoid
cell line
Wild-typeblood
FIGURE 4. Analysis of exon 6 of GATA1 in archival blood and marrow samples from a groupof patients with myelodysplastic syndromes. Top, Chromatogram from denaturing high-performance liquid chromatography Transgenomic WAVE mutation detection system. Mostpatient samples exhibit only a single peak from homoduplexed wild-type DNA (right peak),but DNA derived from a peripheral blood buffy coat from one patient exhibits a second peak(left peak, arrow), indicating the presence of a DNA heteroduplex formed from a mix of wild-type and mutant DNA. Bottom, Sequencing of the patient’s GATA1 gene revealed anacquired c.1066C>T mutation (described in terms of Genbank Accession NM_002049.2)(arrow), which was not present in DNA derived from an Epstein-Barr virus–transformedlymphoblastoid cell line from the patient or from DNA derived from a wild-type (normal)individual. Surprisingly, this clonally restricted mutation did not obviously result in anamino acid change. RNA was unavailable to determine whether the mutation might affectsplicing.
table alterations in the pattern of gene expression that arenot a consequence of changes in the nucleotide sequence ofa gene.169 Such changes are of interest in cancer, in partbecause abnormal epigenetic silencing of genes has beenshown to be associated with neoplasia development andprogression.170 For instance, 5′ methylation of cytosinenucleotides in the promoter region of tumor suppressorgenes can lead to silencing of those genes.171 In MDS, thefirst gene found to be commonly hypermethylated andsilenced was the P15INK4B gene that encodes a cyclin-dependent kinase inhibitor.172-177 Methylation silencing ofp15 is rare in patients with low leukemic cell burden;
however, it is detected in more than 75% of cases withexcess blasts and occurs uniformly with AML transforma-tion, suggesting a pathogenetic role in disease progression.Epigenetic gene silencing in human neoplasia has swiftlygained importance as a therapeutic target because of itspotential reversibility with pharmacological agents.169,178
The clinically beneficial nucleoside analogue 5-azacitidinehas dual therapeutic effects resulting from direct cytotoxic-ity as a nucleoside analogue and from inhibition of ge-nomic methylation.12,179 Treatment with decitabine, the ac-tive metabolite of 5-azacitidine, has been associated withdemethylation of hypermethylated P15INK4B in MDS, al-
Abs
orba
nce
Column retention time
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com694
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
though not consistently.179 The addition of histone de-acetylase inhibitors and other epigenetic modifiers todemethylating agents holds considerable promise for pow-erful chromatin remodelling strategies.180
Until recently, molecular investigations focused on ex-pression of 1 or more genes of interest at a time. Forexample, in a few patients with MDS with intact TP53genes (ie, no coding mutation), expression of the gene hasbeen found to be decreased.181 This down-regulation mayresult in loss of p53 function with biological consequencesequivalent to those resulting from mutational inactivation.The advent of complementary DNA microarray technologyoffers the ability to survey the expression pattern of thou-sands of genes concurrently.182 The results of MDSmicroarray studies have not yet yielded many pathophysi-ological insights, although some leads have been gener-ated.183-186 For instance, the first ATRX mutation was identi-fied after a microarray study of purified neutrophilsshowed dramatic down-regulation of the gene comparedwith normal controls (ultimately found to be the conse-quence of a point mutation in a consensus splice site).152
Another group has detected overexpression of DLK1(Delta-like homolog), a gene of unknown function withhomology to epidermal growth factor that was first identi-fied as a regulator of adipocyte differentiation, in patientswith MDS but not in patients with AML.183 If microarraystudies finally fulfil their promise, it is hoped that they willlead to more accurate MDS diagnosis, classification, andprognostic discrimination and provide more insight into thedisease pathobiology. Recent microarray-generated ad-vancements in the understanding of diffuse large B-celllymphoma187 and breast cancer188 illustrate the tremendouspower of this technology.
CONCLUSION
Genetic testing in MDS is currently an essential compo-nent of clinical care of patients, and testing optionsare likely to evolve in the near future. At present, con-ventional cytogenetic studies remain a critical part ofthe diagnostic evaluation of MDS, and the results offervaluable prognostic information. Detection of specificMDS-associated point mutations and measurement ofgene expression patterns are not yet part of routine clini-cal care, but they promise to expand clinicians’ ability todiagnose, prognosticate, and ultimately treat patients withMDS.
We thank Drs. Richard J. Gibbons (University of Oxford, Ox-ford, England) and Ayalew Tefferi (Mayo Clinic College ofMedicine, Rochester, Minn) for helpful comments on the submit-ted manuscript.
REFERENCES1. Steensma DP, Tefferi A. The myelodysplastic syndrome(s): a perspec-
tive and review highlighting current controversies [published correction ap-pears in Leuk Res. 2005;29:117]. Leuk Res. 2003;27:95-120.
2. Heaney ML, Golde DW. Myelodysplasia. N Engl J Med. 1999;340:1649-1660.
3. Ohyashiki JH, Ohyashiki K, Aizawa S, et al. Replication errors in he-matological neoplasias: genomic instability in progression of disease is differ-ent among different types of leukemia. Clin Cancer Res. 1996;2:1583-1589.
4. Sieber OM, Heinimann K, Tomlinson IP. Genomic instability—theengine of tumorigenesis? Nat Rev Cancer. 2003;3:701-708.
5. Hasle H, Niemeyer CM, Chessells JM, et al. A pediatric approach tothe WHO classification of myelodysplastic and myeloproliferative diseases.Leukemia. 2003;17:277-282.
6. Bennett JM, Catovsky D, Daniel MT, et al. Proposals for the classifica-tion of the myelodysplastic syndromes. Br J Haematol. 1982;51:189-199.
7. Vardiman JW, Harris NL, Brunning RD. The World Health Organiza-tion (WHO) classification of the myeloid neoplasms. Blood. 2002;100:2292-2302.
8. Harris NL, Jaffe ES, Diebold J, et al. World Health Organizationclassification of neoplastic diseases of the hematopoietic and lymphoid tissues:report of the Clinical Advisory Committee meeting-Airlie House, Virginia,November 1997. J Clin Oncol. 1999;17:3835-3849.
9. List AF, Molldrem J, Sanders JE. Prognosis and treatment ofmyelodysplastic syndromes. Presented at: American Society of Clinical Oncol-ogy Annual Meeting; New Orleans, La; June 7 and 8, 2004.
10. Hellstrom-Lindberg E. Efficacy of erythropoietin in the myelodysplas-tic syndromes: a meta-analysis of 205 patients from 17 studies. Br J Haematol.1995;89:67-71.
11. Hellström-Lindberg E, Gulbrandsen N, Lindberg G, et al, ScandinavianMDS Group. A validated decision model for treating the anaemia ofmyelodysplastic syndromes with erythropoietin + granulocyte colony-stimu-lating factor: significant effects on quality of life. Br J Haematol. 2003;120:1037-1046.
12. Silverman LR, Demakos EP, Peterson BL, et al. Randomized controlledtrial of azacitidine in patients with the myelodysplastic syndrome: a study ofthe cancer and leukemia group B. J Clin Oncol. 2002;20:2429-2440.
13. Raza A, Meyer P, Dutt D, et al. Thalidomide produces transfusionindependence in long-standing refractory anemias of patients with myelodys-plastic syndromes. Blood. 2001;98:958-965.
14. Molldrem JJ, Leifer E, Bahceci E, et al. Antithymocyte globulin fortreatment of the bone marrow failure associated with myelodysplastic syn-dromes. Ann Intern Med. 2002;137:156-163.
15. Steensma DP, Dispenzieri A, Moore SB, Schroeder G, Tefferi A.Antithymocyte globulin has limited efficacy and substantial toxicity inunselected anemic patients with myelodysplastic syndrome. Blood. 2003;101:2156-2158.
16. Saunthararajah Y, Nakamura R, Wesley R, Wang QJ, Barrett AJ. Asimple method to predict response to immunosuppressive therapy in patientswith myelodysplastic syndrome. Blood. 2003;102:3025-3027.
17. Chan G, DiVenuti G, Miller K. Danazol for the treatment of thrombocy-topenia in patients with myelodysplastic syndrome. Am J Hematol. 2002;71:166-171.
18. Takeda Y, Sawada H, Sawai H, et al. Acquired hypochromic andmicrocytic sideroblastic anaemia responsive to pyridoxine with low value offree erythrocyte protoporphyrin: a possible subgroup of idiopathic acquiredsideroblastic anaemia (IASA). Br J Haematol. 1995;90:207-209.
19. Oosterveld M, Wittebol SH, Lemmens WA, et al. The impact of inten-sive antileukaemic treatment strategies on prognosis of myelodysplastic syn-drome patients aged less than 61 years according to International PrognosticScoring System risk groups. Br J Haematol. 2003;123:81-89.
20. Anderson JE. Bone marrow transplantation for myelodysplasia. BloodRev. 2000;14:63-77.
21. De Witte T, Van Biezen A, Hermans J, et al, Chronic and AcuteLeukemia Working Parties of the European Group for Blood and MarrowTransplantation. Autologous bone marrow transplantation for patients withmyelodysplastic syndrome (MDS) or acute myeloid leukemia following MDS.Blood. 1997;90:3853-3857.
22. Ho AY, Pagliuca A, Kenyon M, et al. Reduced-intensity allogeneichematopoietic stem cell transplantation for myelodysplastic syndrome andacute myeloid leukemia with multilineage dysplasia using fludarabine,busulphan, and alemtuzumab (FBC) conditioning. Blood. 2004;104:1616-1623.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 695
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
23. Cutler CS, Lee SJ, Greenberg P, et al. A decision analysis of allogeneicbone marrow transplantation for the myelodysplastic syndromes: delayedtransplantation for low-risk myelodysplasia is associated with improved out-come. Blood. 2004;104:579-585.
24. List AF, Kurtin S, Glinsmann-Gibson B, et al. Efficacy and safety ofCC5013 for treatment of anemia in patients with myelodysplastic syndromes(MDS) [abstract]. In: Program and abstracts of the American Society of Hema-tology 45th Annual Meeting; San Diego, Calif; December 6-9, 2003. Abstract641.
25. Wijermans P, Lubbert M, Verhoef G, et al. Low-dose 5-aza-2′-deoxy-cytidine, a DNA hypomethylating agent, for the treatment of high-riskmyelodysplastic syndrome: a multicenter phase II study in elderly patients. JClin Oncol. 2000;18:956-962.
26. Tefferi A, Dewald GW, Litzow ML, et al. Chronic myeloid leukemia:current application of cytogenetics and molecular testing for diagnosis andtreatment. Mayo Clin Proc. 2005;80:390-402.
27. Spurbeck JL, Adams SA, Stupca PJ, Dewald GW. Primer on medicalgenomics, part XI: visualizing human chromosomes. Mayo Clin Proc. 2004;79:58-75.
28. Pierre RV, Catovsky D, Mufti GJ, et al. Clinical-cytogenetic correlationsin myelodysplasia (preleukemia). Cancer Genet Cytogenet. 1989;40:149-161.
29. Greenberg P, Cox C, LeBeau MM, et al. International scoring systemfor evaluating prognosis in myelodysplastic syndromes [published correctionappears in Blood. 1998;91:1100]. Blood. 1997;89:2079-2088.
30. Pfeilstocker M, Reisner R, Nosslinger T, et al. Cross-validation ofprognostic scores in myelodysplastic syndromes on 386 patients from a singleinstitution confirms importance of cytogenetics. Br J Haematol. 1999;106:455-463.
31. Sole F, Espinet B, Sanz GF, et al, Grupo Cooperativo Espanol deCitogenetica Hematologica. Incidence, characterization and prognostic signifi-cance of chromosomal abnormalities in 640 patients with primary myelo-dysplastic syndromes. Br J Haematol. 2000;108:346-356.
32. United Kingdom Cancer Cytogenetics Group (UKCCG). Loss of the Ychromosome from normal and neoplastic bone marrows [published correctionappears in Genes Chromosomes Cancer. 1992;5:411]. Genes ChromosomesCancer. 1992;5:83-88.
33. Nevill TJ, Fung HC, Shepherd JD, et al. Cytogenetic abnormalities inprimary myelodysplastic syndrome are highly predictive of outcome afterallogeneic bone marrow transplantation. Blood. 1998;92:1910-1917.
34. de Souza Fernandez T, Ornellas MH, Otero de Carvalho L, Tabak D,Abdelhay E. Chromosomal alterations associated with evolution frommyelodysplastic syndrome to acute myeloid leukemia. Leuk Res. 2000;24:839-848.
35. Jotterand M, Parlier V. Diagnostic and prognostic significance of cyto-genetics in adult primary myelodysplastic syndromes. Leuk Lymphoma. 1996;23:253-266.
36. Smith SM, Le Beau MM, Huo D, et al. Clinical-cytogenetic associa-tions in 306 patients with therapy-related myelodysplasia and myeloid leuke-mia: the University of Chicago series. Blood. 2003;102:43-52.
37. Billstrom R, Nilsson PG, Mitelman F. Cytogenetic analysis in 941consecutive patients with haematologic disorders. Scand J Haematol. 1986;37:29-40.
38. Perkins D, Brennan S, Carstairs K, et al. Regional cancer cytogenetics: areport on 1,143 diagnostic cases. Cancer Genet Cytogenet. 1997;96:64-80.
39. Heim S. Cytogenetic findings in primary and secondary MDS. LeukRes. 1992;16:43-46.
40. Bloomfield CD, Archer KJ, Mrozek K, et al. 11q23 balanced chromo-some aberrations in treatment-related myelodysplastic syndromes and acuteleukemia: report from an international workshop. Genes Chromosomes Can-cer. 2002;33:362-378.
41. Rubin CM, Larson RA, Anastasi J, et al. t(3;21)(q26;q22): a recurringchromosomal abnormality in therapy-related myelodysplastic syndrome andacute myeloid leukemia. Blood. 1990;76:2594-2598.
42. Jotterand Bellomo M, Parlier V, Muhlematter D, Grob JP, Beris P.Three new cases of chromosome 3 rearrangement in bands q21 and q26 withabnormal thrombopoiesis bring further evidence to the existence of a 3q21q26syndrome. Cancer Genet Cytogenet. 1992;59:138-160.
43. Rowley JD, Olney HJ. International workshop on the relationship ofprior therapy to balanced chromosome aberrations in therapy-relatedmyelodysplastic syndromes and acute leukemia: overview report. GenesChromosomes Cancer. 2002;33:331-345.
44. Olney HJ, Mitelman F, Johansson B, Mrozek K, Berger R, Rowley JD.Unique balanced chromosome abnormalities in treatment-related myelodys-
plastic syndromes and acute myeloid leukemia: report from an internationalworkshop. Genes Chromosomes Cancer. 2002;33:413-423.
45. Block AW, Carroll AJ, Hagemeijer A, et al. Rare recurring balancedchromosome abnormalities in therapy-related myelodysplastic syndromes andacute leukemia: report from an international workshop. Genes ChromosomesCancer. 2002;33:401-412.
46. Collado R, Badia L, Garcia S, Sanchez H, Prieto F, Carbonell F.Chromosome 11 abnormalities in myelodysplastic syndromes. Cancer GenetCytogenet. 1999;114:58-61.
47. Heller A, Loncarevic IF, Glaser M, et al. Breakpoint differentiation inchromosomal aberrations of hematological malignancies: identification of 33previously unrecorded breakpoints. Int J Oncol. 2004;24:127-136.
48. Han JY, Kim KH, Kwon HC, Kim JS, Kim HJ, Lee YH. Unrelatedclonal chromosome abnormalities in myelodysplastic syndromes and acutemyeloid leukemias. Cancer Genet Cytogenet. 2002;132:156-158.
49. Furuya T, Morgan R, Sandberg AA. Cytogenetic biclonality in malig-nant hematologic disorders. Cancer Genet Cytogenet. 1992;62:25-28.
50. Degos L. The history of acute promyelocytic leukaemia. Br J Haematol.2003;122:539-553.
51. Fenaux P. Chromosome and molecular abnormalities in myelodys-plastic syndromes. Int J Hematol. 2001;73:429-437.
52. Narayanan MN, Geary CG, Harrison CJ, Cinkotai KI, Lewis MJ. Threecases of the myelodysplastic syndrome with pericentric inversion of chromo-some 16. Br J Haematol. 1993;85:217-219.
53. Xue Y, Yu F, Zhou Z, Guo Y, Xie X, Lin B. Translocation (8;21) inoligoblastic leukemia: is this a true myelodysplastic syndrome? Leuk Res.1994;18:761-765.
54. Steensma DP, Dewald GW, Hodnefield JM, Tefferi A, Hanson CA.Clonal cytogenetic abnormalities in bone marrow specimens without clearmorphologic evidence of dysplasia: a form fruste of myelodysplasia? Leuk Res.2003;27:235-242.
55. Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specificinhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N EnglJ Med. 2001;344:1031-1037.
56. O’Dwyer ME, Mauro MJ, Blasdel C, et al. Clonal evolution and lack ofcytogenetic response are adverse prognostic factors for hematologic relapse ofchronic phase CML patients treated with imatinib mesylate. Blood. 2004;103:451-455.
57. Kantarjian HM, O’Brien S, Cortes JE, et al. Complete cytogenetic andmolecular responses to interferon-alpha-based therapy for chronic myelog-enous leukemia are associated with excellent long-term prognosis. Cancer.2003;97:1033-1041.
58. Cheson BD, Bennett JM, Kantarjian H, et al. Report of an internationalworking group to standardize response criteria for myelodysplastic syndromes.Blood. 2000;96:3671-3674.
59. Lubbert M, Wijermans P, Kunzmann R, et al. Cytogenetic responses inhigh-risk myelodysplastic syndrome following low-dose treatment with theDNA methylation inhibitor 5-aza-2′-deoxycytidine. Br J Haematol. 2001;114:349-357.
60. Van den Berghe H, Michaux L. 5q–, twenty-five years later: a synopsis.Cancer Genet Cytogenet. 1997;94:1-7.
61. Van den Berghe H, Cassiman JJ, David G, Fryns JP, Michaux JL, SokalG. Distinct haematological disorder with deletion of long arm of no. 5 chromo-some. Nature. 1974;251:437-438.
62. Boultwood J, Lewis S, Wainscoat JS. The 5q-syndrome. Blood. 1994;84:3253-3260.
63. Sole F, Torrabadella M, Granada I, et al. Isochromosome 17q as a soleanomaly: a distinct myelodysplastic syndrome entity? Leuk Res. 1993;17:717-720.
64. Dierlamm J, Michaux L, Criel A, et al. Isodicentric (X)(q13) in haema-tological malignancies: presentation of five new cases, application of fluores-cence in situ hybridization (FISH) and review of the literature. Br J Haematol.1995;91:885-891.
65. Pedersen B. MDS and AML with trisomy 8 as the sole chromosomeaberration show different sex ratios and prognostic profiles: a study of 115published cases. Am J Hematol. 1997;56:224-229.
66. Kimura S, Kuroda J, Akaogi T, Hayashi H, Kobayashi Y, Kondo M.Trisomy 8 involved in myelodysplastic syndromes as a risk factor for intestinalulcers and thrombosis—Behcet’s syndrome. Leuk Lymphoma. 2001;42:115-121.
67. Ogawa H, Kuroda T, Inada M, et al. Intestinal Behcet’s disease associatedwith myelodysplastic syndrome with chromosomal trisomy 8—a report of twocases and a review of the literature. Hepatogastroenterology. 2001;48:416-420.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com696
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
68. Jenkins RB, Tefferi A, Solberg LA Jr, Dewald GW. Acute leukemiawith abnormal thrombopoiesis and inversions of chromosome 3. Cancer GenetCytogenet. 1989;39:167-179.
69. Boultwood J, Fidler C, Soularue P, et al. Novel genes mapping to thecritical region of the 5q– syndrome. Genomics. 1997;45:88-96.
70. Boultwood J, Fidler C, Strickson AJ, et al. Transcription mapping of the5q– syndrome critical region: cloning of two novel genes and sequencing, ex-pression, and mapping of a further six novel cDNAs. Genomics. 2000;66:26-34.
71. Boultwood J, Fidler C, Strickson AJ, et al. Narrowing and genomicannotation of the commonly deleted region of the 5q– syndrome. Blood. 2002;99:4638-4641.
72. Fidler C, Wainscoat JS, Boultwood J. The human POP2 gene: identifi-cation, sequencing, and mapping to the critical region of the 5q– syndrome.Genomics. 1999;56:134-136.
73. Seghezzi L, Maserati E, Minelli A, et al. Constitutional trisomy 8 as firstmutation in multistep carcinogenesis: clinical, cytogenetic, and molecular dataon three cases. Genes Chromosomes Cancer. 1996;17:94-101.
74. Dohner K, Brown J, Hehmann U, et al. Molecular cytogenetic charac-terization of a critical region in bands 7q35-q36 commonly deleted in malig-nant myeloid disorders. Blood. 1998;92:4031-4035.
75. Fischer K, Frohling S, Scherer SW, et al. Molecular cytogenetic delin-eation of deletions and translocations involving chromosome band 7q22 inmyeloid leukemias. Blood. 1997;89:2036-2041.
76. Gonzalez MB, Gutierrez NC, Garcia JL, et al. Heterogeneity of struc-tural abnormalities in the 7q31.3 approximately q34 region in myeloid malig-nancies. Cancer Genet Cytogenet. 2004;150:136-143.
77. Nosslinger T, Reisner R, Koller E, et al. Myelodysplastic syndromes,from French-American-British to World Health Organization: comparison ofclassifications on 431 unselected patients from a single institution. Blood.2001;98:2935-2941.
78. Golub TR, Barker GF, Lovett M, Gilliland DG. Fusion of PDGF recep-tor beta to a novel ets-like gene, tel, in chronic myelomonocytic leukemia witht(5;12) chromosomal translocation. Cell. 1994;77:307-316.
79. Tomasson MH, Sternberg DW, Williams IR, et al. Fatal myeloprolif-eration, induced in mice by TEL/PDGFbetaR expression, depends onPDGFbetaR tyrosines 579/581. J Clin Invest. 2000;105:423-432.
80. Ross TS, Bernard OA, Berger R, Gilliland DG. Fusion of Hunting-tin interacting protein 1 to platelet-derived growth factor beta receptor(PDGFbetaR) in chronic myelomonocytic leukemia with t(5;7)(q33;q11.2).Blood. 1998;91:4419-4426.
81. Schwaller J, Anastasiadou E, Cain D, et al. H4(D10S170), a genefrequently rearranged in papillary thyroid carcinoma, is fused to the platelet-derived growth factor receptor beta gene in atypical chronic myeloid leukemiawith t(5;10)(q33;q22). Blood. 2001;97:3910-3918.
82. Magnusson MK, Meade KE, Brown KE, et al. Rabaptin-5 is a novelfusion partner to platelet-derived growth factor beta receptor in chronicmyelomonocytic leukemia. Blood. 2001;98:2518-2525.
83. Tomasson MH, Williams IR, Hasserjian R, et al. TEL/PDGFbetaRinduces hematologic malignancies in mice that respond to a specific tyrosinekinase inhibitor. Blood. 1999;93:1707-1714.
84. Ritchie KA, Aprikyan AA, Bowen-Pope DF, et al. The Tel-PDGFRbetafusion gene produces a chronic myeloproliferative syndrome in transgenicmice. Leukemia. 1999;13:1790-1803.
85. Apperley JF, Gardembas M, Melo JV, et al. Response to imatinibmesylate in patients with chronic myeloproliferative diseases with rearrange-ments of the platelet-derived growth factor receptor beta. N Engl J Med.2002;347:481-487.
86. Cain JA, Grisolano JL, Laird AD, Tomasson MH. Complete remissionof TEL-PDGFRB-induced myeloproliferative disease in mice by receptortyrosine kinase inhibitor SU11657. Blood. 2004;104:561-564.
87. Dewald GW, Ketterling RP, Wyatt WA, Stupca PJ. Cytogenetic studiesin neoplastic hematologic disorders. In: McClatchey KD, ed. Clinical Labora-tory Medicine. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins;2002:658-685.
88. Bench AJ, Nacheva EP, Hood TL, et al, UK Cancer Cytogenetics Group(UKCCG). Chromosome 20 deletions in myeloid malignancies: reduction ofthe common deleted region, generation of a PAC/BAC contig and identifica-tion of candidate genes. Oncogene. 2000;19:3902-3913.
89. La Starza R, Wlodarska I, Aventin A, et al. Molecular delineation of13q deletion boundaries in 20 patients with myeloid malignancies. Blood.1998;91:231-237.
90. Soenen V, Preudhomme C, Roumier C, Daudignon A, Lai JL, Fenaux P.17p Deletion in acute myeloid leukemia and myelodysplastic syndrome: analy-
sis of breakpoints and deleted segments by fluorescence in situ. Blood.1998;91:1008-1015.
91. Bernell P, Jacobsson B, Nordgren A, Hast R. Clonal cell lineage in-volvement in myelodysplastic syndromes studied by fluorescence in situ hy-bridization and morphology. Leukemia. 1996;10:662-668.
92. Gerritsen WR, Donohue J, Bauman J, et al. Clonal analysis ofmyelodysplastic syndrome: monosomy 7 is expressed in the myeloid lineage,but not in the lymphoid lineage as detected by fluorescent in situ hybridization.Blood. 1992;80:217-224.
93. Boultwood J, Wainscoat JS. Clonality in the myelodysplastic syn-dromes. Int J Hematol. 2001;73:411-415.
94. van Lom K, Houtsmuller AB, van Putten WL, Slater RM, LowenbergB. Cytogenetic clonality analysis of megakaryocytes in myelodysplastic syn-drome by dual-color fluorescence in situ hybridization and confocal laserscanning microscopy. Genes Chromosomes Cancer. 1999;25:332-338.
95. Anderson K, Arvidsson I, Jacobsson B, Hast R. Fluorescence in situhybridization for the study of cell lineage involvement in myelodysplasticsyndromes with chromosome 5 anomalies. Cancer Genet Cytogenet. 2002;136:101-107.
96. Bigoni R, Cuneo A, Milani R, et al. Multilineage involvement in the 5q–syndrome: a fluorescent in situ hybridization study on bone marrow smears.Haematologica. 2001;86:375-381.
97. Jaju RJ, Jones M, Boultwood J, et al. Combined immunophenotypingand FISH identifies the involvement of B-cells in 5q– syndrome. Genes Chro-mosomes Cancer. 2000;29:276-280.
98. Fagioli F, Cuneo A, Bardi A, et al. Heterogeneity of lineage involve-ment by trisomy 8 in myelodysplastic syndrome: a multiparameter analysiscombining conventional cytogenetics, DNA in situ hybridization, and bonemarrow culture studies. Cancer Genet Cytogenet. 1995;82:116-122.
99. Ketterling RP, Wyatt WA, VanWier SA, et al. Primary myelodysplasticsyndrome with normal cytogenetics: utility of ‘FISH panel testing’ and M-FISH. Leuk Res. 2002;26:235-240.100. Cherry AM, Brockman SR, Paternoster SF, et al. Comparison of inter-
phase FISH and metaphase cytogenetics to study myelodysplastic syndrome:an Eastern Cooperative Oncology Group (ECOG) study. Leuk Res. 2003;27:1085-1090.101. Andreasson P, Johansson B, Billstrom R, Garwicz S, Mitelman F, Hog-
lund M. Fluorescence in situ hybridization analyses of hematologic malignan-cies reveal frequent cytogenetically unrecognized 12p rearrangements. Leuke-mia. 1998;12:390-400.102. Beyer V, Castagne C, Muhlematter D, et al. Systematic screening at
diagnosis of -5/del(5)(q31), -7, or chromosome 8 aneuploidy by interphasefluorescence in situ hybridization in 110 acute myelocytic leukemia and high-risk myelodysplastic syndrome patients: concordances and discrepancies withconventional cytogenetics. Cancer Genet Cytogenet. 2004;152:29-41.103. Romeo M, Chauffaille MDL, Silva MRR, Bahia DMM, Kerbauy J.
Comparison of cytogenetics with FISH in 40 myelodysplastic syndrome pa-tients. Leuk Res. 2002;26:993-996.104. Bernasconi P, Cavigliano PM, Boni M, et al. Is FISH a relevant prog-
nostic tool in myelodysplastic syndromes with a normal chromosome patternon conventional cytogenetics? a study on 57 patients. Leukemia. 2003;17:2107-2112.105. Kibbelaar RE, Mulder JW, Dreef EJ, et al. Detection of monosomy 7
and trisomy 8 in myeloid neoplasia: a comparison of banding and fluorescencein situ hybridization. Blood. 1993;82:904-913.106. Brizard F, Brizard A, Guilhot F, Tanzer J, Berger R. Detection of
monosomy 7 and trisomies 8 and 11 in myelodysplastic disorders by interphasefluorescent in situ hybridization: comparison with acute non-lymphocytic leu-kemias. Leukemia. 1994;8:1005-1011.107. van Dijk JP, de Witte T. Monitoring treatment efficiency in MDS at the
molecular level: possibilities now and in the future. Leuk Res. 2004;28:101-108.108. Le Gouill S, Talmant P, Milpied N, et al. Fluorescence in situ hybridiza-
tion on peripheral-blood specimens is a reliable method to evaluate cytogeneticresponse in chronic myeloid leukemia. J Clin Oncol. 2000;18:1533-1538.109. Jalal SM, Law ME, Stamberg J, et al. Detection of diagnostically
critical, often hidden, anomalies in complex karyotypes of haematologicaldisorders using multicolour fluorescence in situ hybridization. Br J Haematol.2001;112:975-980.110. Schrock E, du Manoir S, Veldman T, et al. Multicolor spectral karyo-
typing of human chromosomes. Science. 1996;273:494-497.111. Kakazu N, Taniwaki M, Horiike S, et al. Combined spectral karyotyp-
ing and DAPI banding analysis of chromosome abnormalities in myelodys-plastic syndrome. Genes Chromosomes Cancer. 1999;26:336-345.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com 697
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
112. Trost D, Hildebrandt B, Muller N, Germing U, Royer-Pokora B. Hiddenchromosomal aberrations are rare in primary myelodysplastic syndromes withevolution to acute myeloid leukaemia and normal cytogenetics. Leuk Res.2004;28:171-177.113. Mohr B, Bornhauser M, Thiede C, et al. Comparison of spectral karyo-
typing and conventional cytogenetics in 39 patients with acute myeloid leuke-mia and myelodysplastic syndrome. Leukemia. 2000;14:1031-1038.114. Cohen N, Trakhtenbrot L, Yukla M, et al. SKY detection of chromo-
some rearrangements in two cases of tMDS with a complex karyotype. CancerGenet Cytogenet. 2002;138:128-132.115. Lindvall C, Nordenskjold M, Porwit A, Bjorkholm M, Blennow E.
Molecular cytogenetic characterization of acute myeloid leukemia andmyelodysplastic syndromes with multiple chromosome rearrangements.Haematologica. 2001;86:1158-1164.116. Van Limbergen H, Poppe B, Michaux L, et al. Identification of cytoge-
netic subclasses and recurring chromosomal aberrations in AML and MDSwith complex karyotypes using M-FISH. Genes Chromosomes Cancer. 2002;33:60-72.117. Pollack JR, Perou CM, Alizadeh AA, et al. Genome-wide analysis of
DNA copy-number changes using cDNA microarrays. Nat Genet. 1999;23:41-46.118. Wilkens L, Burkhardt D, Tchinda J, et al. Cytogenetic aberrations in
myelodysplastic syndrome detected by comparative genomic hybridizationand fluorescence in situ hybridization. Diagn Mol Pathol. 1999;8:47-53.119. Kim MH, Stewart J, Devlin C, Kim YT, Boyd E, Connor M. The
application of comparative genomic hybridization as an additional tool in thechromosome analysis of acute myeloid leukemia and myelodysplastic syn-dromes. Cancer Genet Cytogenet. 2001;126:26-33.120. Ishkanian AS, Malloff CA, Watson SK, et al. A tiling resolution DNA
microarray with complete coverage of the human genome. Nat Genet. 2004;36:299-303.121. Jonveaux P, Fenaux P, Quiquandon I, et al. Mutations in the p53 gene in
myelodysplastic syndromes. Oncogene. 1991;6:2243-2247.122. Tsushita K, Hotta T, Ichikawa A, Saito H. Mutation of p53 gene does
not play a critical role in myelodysplastic syndrome and its transformation toacute leukaemia [letter]. Br J Haematol. 1992;81:456-457.123. Sugimoto K, Hirano N, Toyoshima H, et al. Mutations of the p53 gene
in myelodysplastic syndrome (MDS) and MDS-derived leukemia. Blood.1993;81:3022-3026.124. Mori N, Hidai H, Yokota J, et al. Mutations of the p53 gene in
myelodysplastic syndrome and overt leukemia. Leuk Res. 1995;19:869-875.125. Misawa S, Horiike S. TP53 mutations in myelodysplastic syndrome.
Leuk Lymphoma. 1996;23:417-422.126. Padua RA, Guinn BA, Al-Sabah AI, et al. RAS, FMS and p53 mutations
and poor clinical outcome in myelodysplasias: a 10-year follow-up. Leukemia.1998;12:887-892.127. Tang JL, Tien HF, Lin MT, Chen PJ, Chen YC. P53 mutation in
advanced stage of primary myelodysplastic syndrome. Anticancer Res. 1998;18(5B):3757-3761.128. Kita-Sasai Y, Horiike S, Misawa S, et al. International prognostic
scoring system and TP53 mutations are independent prognostic indicators forpatients with myelodysplastic syndrome. Br J Haematol. 2001;115:309-312.129. Imamura N, Abe K, Oguma N. High incidence of point mutations of p53
suppressor oncogene in patients with myelodysplastic syndrome amongatomic-bomb survivors: a 10-year follow-up [letter]. Leukemia. 2002;16:154-156.130. Side LE, Curtiss NP, Teel K, et al. RAS, FLT3, and TP53 mutations in
therapy-related myeloid malignancies with abnormalities of chromosomes 5and 7. Genes Chromosomes Cancer. 2004;39:217-223.131. Horiike S, Kita-Sasai Y, Nakao M, Taniwaki M. Configuration of the
TP53 gene as an independent prognostic parameter of myelodysplastic syn-drome. Leuk Lymphoma. 2003;44:915-922.132. Soong R, Robbins PD, Dix BR, et al. Concordance between p53 protein
overexpression and gene mutation in a large series of common human carcino-mas. Hum Pathol. 1996;27:1050-1055.133. Baas IO, Mulder JW, Offerhaus GJ, Vogelstein B, Hamilton SR. An
evaluation of six antibodies for immunohistochemistry of mutant p53 geneproduct in archival colorectal neoplasms. J Pathol. 1994;172:5-12.134. Gross E, Kiechle M, Arnold N. Mutation analysis of p53 in ovarian
tumors by DHPLC. J Biochem Biophys Methods. 2001;47:73-81.135. Plata E, Viniou N, Abazis D, et al. Cytogenetic analysis and RAS
mutations in primary myelodysplastic syndromes. Cancer Genet Cytogenet.1999;111:124-129.
136. de Souza Fernandez T, Menezes de Souza J, Macedo Silva ML, TabakD, Abdelhay E. Correlation of N-ras point mutations with specific chromo-somal abnormalities in primary myelodysplastic syndrome. Leuk Res. 1998;22:125-134.137. Paquette RL, Landaw EM, Pierre RV, et al. N-ras mutations are associ-
ated with poor prognosis and increased risk of leukemia in myelodysplasticsyndrome. Blood. 1993;82:590-599.138. Shih LY, Huang CF, Wang PN, et al. Acquisition of FLT3 or N-ras
mutations is frequently associated with progression of myelodysplastic syn-drome to acute myeloid leukemia. Leukemia. 2004;18:466-475.139. Mitani K, Hangaishi A, Imamura N, et al. No concomitant occurrence of
the N-ras and p53 gene mutations in myelodysplastic syndromes. Leukemia.1997;11:863-865.140. Horiike S, Yokota S, Nakao M, et al. Tandem duplications of the FLT3
receptor gene are associated with leukemic transformation of myelodysplasia.Leukemia. 1997;11:1442-1446.141. Kiyoi H, Towatari M, Yokota S, et al. Internal tandem duplication of the
FLT3 gene is a novel modality of elongation mutation which causes constitu-tive activation of the product. Leukemia. 1998;12:1333-1337.142. Yokota S, Kiyoi H, Nakao M, et al. Internal tandem duplication of the
FLT3 gene is preferentially seen in acute myeloid leukemia and myelodys-plastic syndrome among various hematological malignancies: a study on alarge series of patients and cell lines. Leukemia. 1997;11:1605-1609.143. Au WY, Fung AT, Ma ES, Liang RH, Kwong YL. Low frequency of
FLT3 gene internal tandem duplication and activating loop mutation intherapy-related acute myelocytic leukemia and myelodysplastic syndrome.Cancer Genet Cytogenet. 2004;149:169-172.144. Imai Y, Kurokawa M, Izutsu K, et al. Mutations of the AML1 gene in
myelodysplastic syndrome and their functional implications in leukemogen-esis. Blood. 2000;96:3154-3160.145. Preudhomme C, Warot-Loze D, Roumier C, et al. High incidence of
biallelic point mutations in the Runt domain of the AML1/PEBP2 alpha B genein Mo acute myeloid leukemia and in myeloid malignancies with acquiredtrisomy 21. Blood. 2000;96:2862-2869.146. Imai O, Kurokawa M, Izutsu K, et al. Mutational analyses of the AML1
gene in patients with myelodysplastic syndrome. Leuk Lymphoma. 2002;43:617-621.147. Harada H, Harada Y, Tanaka H, Kimura A, Inaba T. Implications of
somatic mutations in the AML1 gene in radiation-associated and therapy-related myelodysplastic syndrome/acute myeloid leukemia. Blood. 2003;101:673-680.148. Roumier C, Fenaux P, Lafage M, Imbert M, Eclache V, Preudhomme C.
New mechanisms of AML1 gene alteration in hematological malignancies.Leukemia. 2003;17:9-16.149. Christiansen DH, Andersen MK, Pedersen-Bjergaard J. Mutations of
AML1 are common in therapy-related myelodysplasia following therapy withalkylating agents and are significantly associated with deletion or loss ofchromosome arm 7q and with subsequent leukemic transformation. Blood.2004;104:1474-1481.150. Harada H, Harada Y, Niimi H, Kyo T, Kimura A, Inaba T. High
incidence of somatic mutations in the AML1/RUNX1 gene in myelodysplasticsyndrome and low blast percentage myeloid leukemia with myelodysplasia.Blood. 2004;103:2316-2324.151. Steensma DP, Gibbons RJ, Mesa RA, Tefferi A, Higgs DR. Somatic
point mutations in RUNX1/CBFA2/AML1 are common in high-risk myelo-dysplastic syndrome, but not in myelofibrosis with myeloid metaplasia. Eur JHaematol. 2005;74:47-53.152. Gibbons RJ, Pellagatti A, Garrick D, et al. Identification of acquired
somatic mutations in the gene encoding chromatin-remodeling factor ATRX inthe alpha-thalassemia myelodysplasia syndrome (ATMDS). Nat Genet. 2003;34:446-449.153. Steensma DP, Higgs DR, Fisher CA, Gibbons RJ. Acquired somatic
ATRX mutations in myelodysplastic syndrome associated with alpha thalas-semia (ATMDS) convey a more severe hematologic phenotype than germlineATRX mutations. Blood. 2004;103:2019-2026.154. Gibbons RJ, Higgs DR. Molecular-clinical spectrum of the ATR-X
syndrome. Am J Med Genet. 2000;97:204-212.155. Steensma DP, Gibbons RJ, Higgs DR. Acquired alpha-thalassemia in
association with myelodysplastic syndrome and other hematologic malignan-cies. Blood. 2005;105:443-452.156. Stephenson J, Mufti GJ, Yoshida Y. Myelodysplastic syndromes: from
morphology to molecular biology, part II: the molecular genetics of myelodys-plasia. Int J Hematol. 1993;57:99-112.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc. • May 2005;80(5):681-698 • www.mayoclinicproceedings.com698
GENETIC TESTING IN THE MYELODYSPLASTIC SYNDROMES
157. Springall F, O’Mara S, Shounan Y, Todd A, Ford D, Iland H. c-fmspoint mutations in acute myeloid leukemia: fact or fiction? Leukemia. 1993;7:978-985.158. Watkins F, Fidler C, Boultwood J, Wainscoat JS. Mutations in PTPN11
are rare in adult myelodysplastic syndromes and acute myeloid leukemia[letter]. Am J Hematol. 2004;76:417.159. Tartaglia M, Niemeyer CM, Fragale A, et al. Somatic mutations in
PTPN11 in juvenile myelomonocytic leukemia, myelodysplastic syndromesand acute myeloid leukemia. Nat Genet. 2003;34:148-150.160. Trulzsch B, Krohn K, Wonerow P, Paschke R. DGGE is more sensitive
for the detection of somatic point mutations than direct sequencing.Biotechniques. 1999;27:266-268.161. Emmerson P, Maynard J, Jones S, Butler R, Sampson JR, Cheadle JP.
Characterizing mutations in samples with low-level mosaicism by collectionand analysis of DHPLC fractionated heteroduplexes. Hum Mutat. 2003;21:112-115.162. Ellis LA, Taylor CF, Taylor GR. A comparison of fluorescent SSCP and
denaturing HPLC for high throughput mutation scanning. Hum Mutat. 2000;15:556-564.163. Faustino NA, Cooper TA. Pre-mRNA splicing and human disease.
Genes Dev. 2003;17:419-437.164. Steensma DP, Allen SL, Gibbons RJ, Fisher CA, Higgs DR. A novel
splicing mutation in the gene encoding the chromatin-associated factor ATRXassociated with acquired hemoglobin H disease in myelodysplastic syndrome(ATMDS) [abstract]. In: Program and abstracts of the American Society ofHematology 46th Annual Meeting; San Diego, Calif; December 4-7, 2004.Abstract 3606.165. Reddy PL, Shetty VT, Dutt D, et al. Increased incidence of mitochon-
drial cytochrome c-oxidase gene mutations in patients with myelodysplasticsyndromes. Br J Haematol. 2002;116:564-575.166. Gattermann N, Aul C, Schneider W. Is acquired idiopathic sideroblastic
anemia (AISA) a disorder of mitochondrial DNA? Leukemia. 1993;7:2069-2076.167. Shin MG, Kajigaya S, Levin BC, Young NS. Mitochondrial DNA muta-
tions in patients with myelodysplastic syndromes. Blood. 2003;101:3118-3125.168. Gattermann N, Wulfert M, Junge B, Germing U, Haas R, Hofhaus
G. Ineffective hematopoiesis linked with a mitochondrial tRNA mutation(G3242A) in a patient with myelodysplastic syndrome. Blood. 2004;103:1499-1502.169. Herman JG, Baylin SB. Gene silencing in cancer in association with
promoter hypermethylation. N Engl J Med. 2003;349:2042-2054.170. Jones PA, Laird PW. Cancer epigenetics comes of age. Nat Genet.
1999;21:163-167.171. Herman JG. Hypermethylation of tumor suppressor genes in cancer.
Semin Cancer Biol. 1999;9:359-367.172. Preisler HD, Li B, Chen H, et al. P15INK4B gene methylation and
expression in normal, myelodysplastic, and acute myelogenous leukemia cellsand in the marrow cells of cured lymphoma patients. Leukemia. 2001;15:1589-1595.
173. Quesnel B, Fenaux P. P15INK4b gene methylation and myelodysplasticsyndromes. Leuk Lymphoma. 1999;35:437-443.174. Tien HF, Tang JH, Tsay W, et al. Methylation of the p15(INK4B) gene
in myelodysplastic syndrome: it can be detected early at diagnosis or duringdisease progression and is highly associated with leukaemic transformation. BrJ Haematol. 2001;112:148-154.175. Uchida T, Kinoshita T, Nagai H, et al. Hypermethylation of the
p15INK4B gene in myelodysplastic syndromes. Blood. 1997;90:1403-1409.176. Uchida T, Kinoshita T, Hotta T, Murate T. High-risk myelodysplastic
syndromes and hypermethylation of the p15Ink4B gene. Leuk Lymphoma.1998;32:9-18.177. Aoki E, Uchida T, Ohashi H, et al. Methylation status of the p15INK4B
gene in hematopoietic progenitors and peripheral blood cells in myelodys-plastic syndromes. Leukemia. 2000;14:586-593.178. Leone G, Teofili L, Voso MT, Lubbert M. DNA methylation and
demethylating drugs in myelodysplastic syndromes and secondary leukemias.Haematologica. 2002;87:1324-1341.179. Daskalakis M, Nguyen TT, Nguyen C, et al. Demethylation of a
hypermethylated P15/INK4B gene in patients with myelodysplastic syndromeby 5-Aza-2′-deoxycytidine (decitabine) treatment. Blood. 2002;100:2957-2964.180. Gore SD, Weng LJ, Figg WD, et al. Impact of prolonged infusions
of the putative differentiating agent sodium phenylbutyrate on myelodys-plastic syndromes and acute myeloid leukemia. Clin Cancer Res. 2002;8:963-970.181. Totzke G, Bruning T, Vetter H, Schulze-Osthoff K, Ko Y. P53
downregulation in myelodysplastic syndrome—a quantitative analysis bycompetitive RT-PCR [letter]. Leukemia. 2001;15:1663-1664.182. Tefferi A, Bolander ME, Ansell SM, Wieben ED, Spelsberg TC. Primer
on medical genomics, part III: microarray experiments and data analysis. MayoClin Proc. 2002;77:927-940.183. Miyazato A, Ueno S, Ohmine K, et al. Identification of myelodysplastic
syndrome-specific genes by DNA microarray analysis with purified hemato-poietic stem cell fraction. Blood. 2001;98:422-427.184. Hofmann WK, de Vos S, Komor M, Hoelzer D, Wachsman W, Koeffler
HP. Characterization of gene expression of CD34+ cells from normal andmyelodysplastic bone marrow. Blood. 2002;100:3553-3560.185. Ueda M, Ota J, Yamashita Y, et al. DNA microarray analysis of stage
progression mechanism in myelodysplastic syndrome. Br J Haematol. 2003;123:288-296.186. Pellagatti A, Esoof N, Watkins F, et al. Gene expression profiling in the
myelodysplastic syndromes using cDNA microarray technology. Br J Haema-tol. 2004;125:576-583.187. Lossos IS, Czerwinski DK, Alizadeh AA, et al. Prediction of survival in
diffuse large-B-cell lymphoma based on the expression of six genes. N Engl JMed. 2004;350:1828-1837.188. van de Vijver MJ, He YD, van’t Veer LJ, et al. A gene-expression sig-
nature as a predictor of survival in breast cancer. N Engl J Med. 2002;347:1999-2009.
The Genetics in Clinical Practice series will continue in the July issue.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.