Embed Size (px)
Citation preview
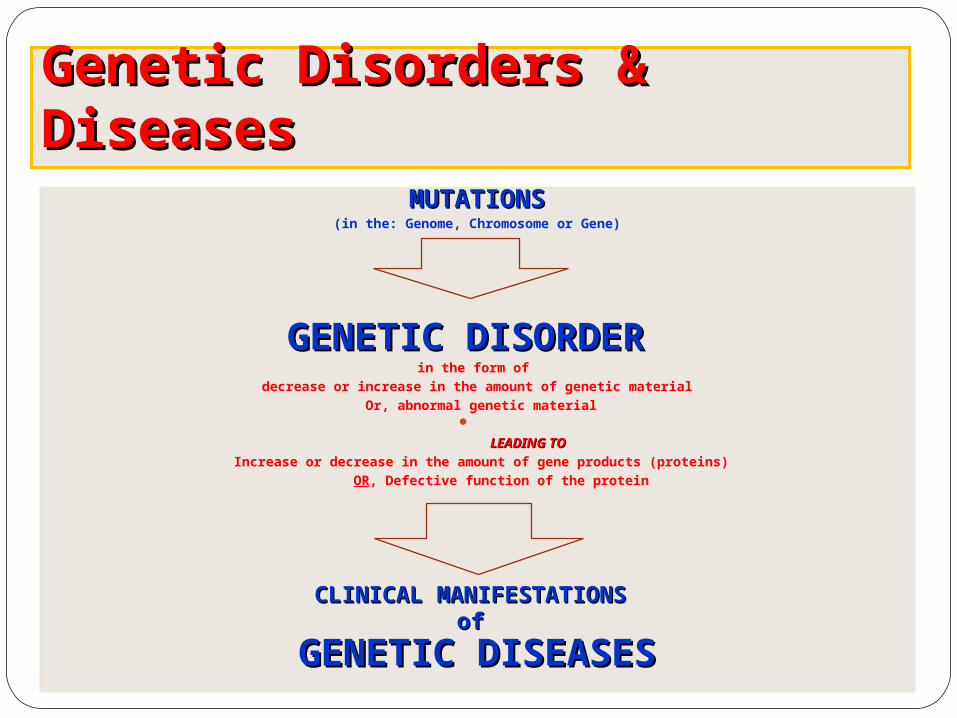
Genetic Disorders & DiseasesGenetic Disorders & DiseasesMUTATIONSMUTATIONS
(in the: Genome, Chromosome or Gene)
GENETIC DISORDERGENETIC DISORDER in the form of
decrease or increase in the amount of genetic material Or, abnormal genetic material
LEADING TOLEADING TO
Increase or decrease in the amount of gene products (proteins) OR, Defective function of the protein
CLINICAL MANIFESTATIONS CLINICAL MANIFESTATIONS of of
GENETIC DISEASESGENETIC DISEASES
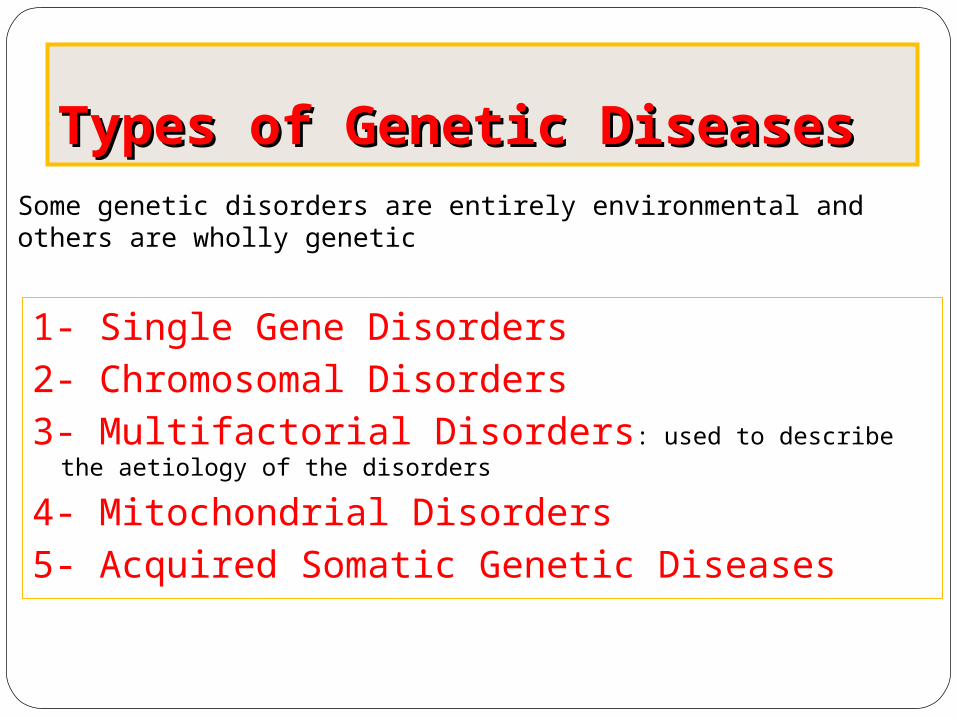
Types of Genetic DiseasesTypes of Genetic Diseases
1- Single Gene Disorders2- Chromosomal Disorders3- Multifactorial Disorders: used to describe the aetiology of the
disorders
4- Mitochondrial Disorders 5- Acquired Somatic Genetic Diseases
Some genetic disorders are entirely environmental and others are wholly genetic

Chromosomal DisordersChromosomal Disorders•Result from defect in: numbernumber (i.e. Numerical Disorders) of chromosomeschromosomes OR structurestructure (i.e. Structural Disorders) of chromosomeschromosomes • Example: Trisomy 21 (Downs syndrome) • These disorders are quite commonquite common and affect about 1/800 live born infants • Account for almost half of all spontaneous first-trimester abortions
• Do notnot follow Mendelian pattern of inheritance

Chromosomal DisordersChromosomal DisordersChromosomal DisordersChromosomal Disorders
Increase or Decrease in number of chromosomes
Change in the structure of chromosomes
Numerical Structural
Euploidy Aneuploidy
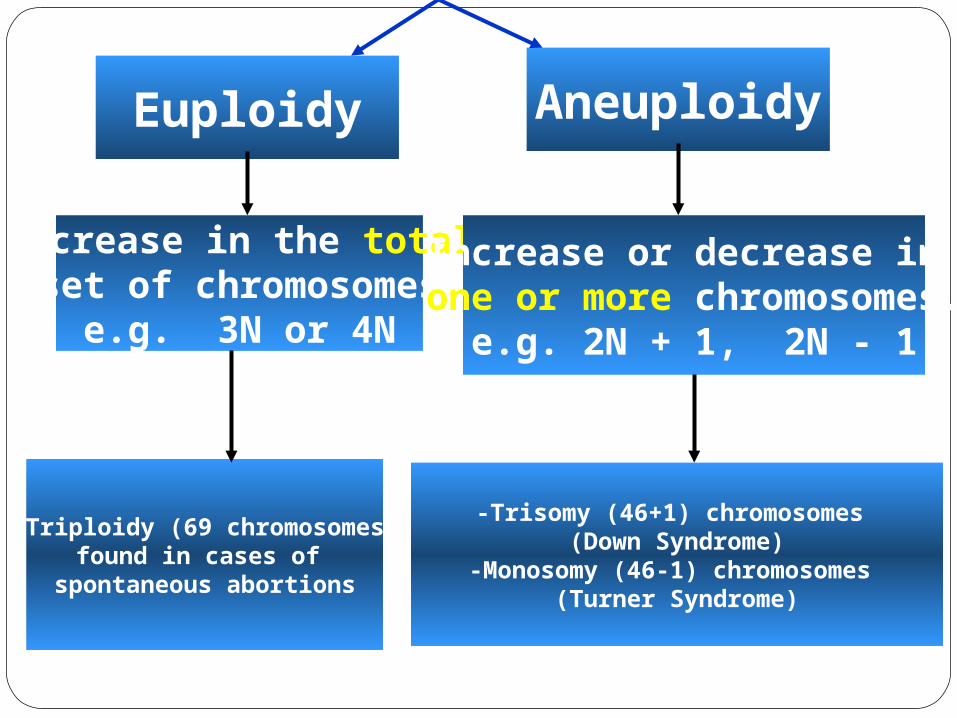
Euploidy
Increase in the totalset of chromosomes
e.g. 3N or 4N
Increase or decrease in one or more chromosomes.
e.g. 2N + 1, 2N - 1
Aneuploidy
-Triploidy (69 chromosomes)found in cases of
spontaneous abortions
-Trisomy (46+1) chromosomes (Down Syndrome)
-Monosomy (46-1) chromosomes (Turner Syndrome)

Non-Disjunction
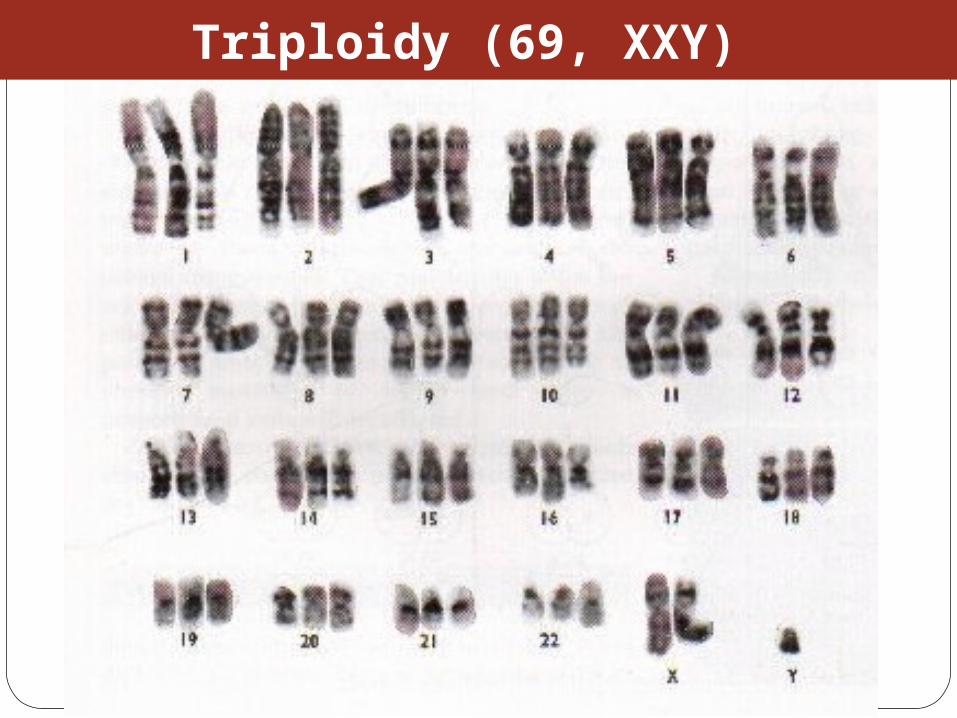
Triploidy (69, XXY)
Effect generally energy metabolism.
Effect more those tissues which require constant supply of energy e.g. muscles.
Show maternal inheritanceShow maternal inheritance:Affected females Affected females transmit the disease to all their children (boys & girls) Affected males Affected males have normal children (boys & girls) Males cannot transmit the disease as the cytoplasm is inherited only from the mother & mitochondria are present in the cytoplasm
•
Mitochondrial DisordersMitochondrial Disorders

• InteractionInteraction between environmental & genetic factors.
• Polygenic in naturePolygenic in nature, no single error in the genetic information.
• Environmental factors Environmental factors play a significant role in precipitating the disorder in genetically susceptible individuals.
• Tend to cluster in familiesfamilies
• Do notnot show characteristic pedigree pattern of inheritance.
• ExamplesExamples: Obesity, DM, Hypercholesterolemia, Hypertension
• Account for the majority of morbidity and mortality in developedcountries
Multifactorial DisordersMultifactorial Disorders

Multifactorial Disorders
Congenital malformations
Common disorders of adult life.
Single Gene DisordersSingle Gene Disorders• CausedCaused by mutation in only one gene
• Can leadlead to critical errors in the genetic information (lead to inborn errors of metabolisminborn errors of metabolism) • FollowFollow Mendelian Inheritance
• OccurOccur at a variable frequency in different population • Over 7,000 single gene disorders have been identified. • May be - Autosomal- Autosomal - Sex-linked- Sex-linked
Inborn Errors of MetabolismInborn Errors of Metabolism
Also called, Inherited metabolic
diseases or congenital metabolic diseases.
They are a large group of genetic disorders, resulting in metabolic defects
due to a single gene mutation which leads to
Reduced or absent gene product or
Production of a different protein with abnormal function.
⇒ ⇒ Single Gene DisordersSingle Gene Disorders

ENZYME A
B
C
⇒ ⇒ Single Gene DisordersSingle Gene Disorders

General Effects of Inborn Errors of Metabolism
Accumulation of a substrate or its metabolic derivatives that are harmful or may interfere with normal function of cells.
Accumulation of intermediates from alternative metabolic pathways
Decreased ability to synthesize essential compounds
Defects in energy production
⇒ ⇒ Single Gene DisordersSingle Gene Disorders
Inheritance of inborn errors of metabolism
Most of the inborn errors of metabolism are inherited as Autosomal recessive or X-linked disorders in nuclear DNA Few are inherited as autosomal dominant.
Some may involve mitochondrial functions as they are linked to mt-DNA.
The incidence of these diseases within different racial and ethnic groups varies with predominance of certain inborn errors of metabolism within particular groups.
Some of these diseases occur in large numbers in communities in which consanguinity is common.
⇒ ⇒ Single Gene DisordersSingle Gene Disorders
Inborn errors of metabolism are important causes of illness in children
They may present as acute life-threatening illness in the neonatal period or become apparent later in childhood
Rarely, clinical presentation is delayed until adult life.
⇒ ⇒ Single Gene DisordersSingle Gene Disorders
⇒ Inheritance of inborn errors of metabolism

Heterozygote carriers of a disease: It may be found during screening (as such performed on family
members of a patient with muscular dystrophy).
Before birth (intrauterine) Some inherited disorders can be detected before birth (as cystic
fibrosis). Neonatal (newborn) screening (in first days of life) As for phenylketonuria
In neonates (in first weeks of life) Many disorders involving single gene defects become apparent
clinically (give symptoms & signs).
Some disorders such as familial hypercholesterolemia may not be recognized until adult life.
Inherited disorders may be detected in different stages Inherited disorders may be detected in different stages during lifeduring life

Before birth diagnosis of inherited metabolic diseases
Prenatal diagnosis is important in detecting and preventing genetic diseases
Prenatal screening of inherited metabolic disorders is done by demonstrating the metabolic defects by chorionic villus biopsy (in
first trimester) & cultured fetal fibroblasts obtained by amniocentesis (in second trimester)
Screening is indicated in: - Women with previously affected infant - Ethnic groups thought to have a high incidence of the carrier state --------------------------------------------------------------------------N.B. prenatal screening for chromosomal abnormalities is also performed
(e.g. serum α- fetoprotein concentration for diagnosis of fetal neural tube defects & in Down’s syndrome)
Techniques For Prenatal DiagnosisTechniques For Prenatal Diagnosis1. Ultrasonography:It is safe and performed in the second trimester
2. Amniocentesis: Procedure risk : It has 0.5-1% of risk during procedure Performed in second trimester Widely available
3. Chorionic villus sampling Procedure risk : 1-2 % Performed in first trimester Specialized technique
4. Cordocentesis Procedure risk: 1% Performed in second trimester Specialized technique

5. Fetal tissue biobsy Procedure risk > 3% Performed in second trimester Very specialized technique Limited application
⇒⇒Techniques For Prenatal Diagnosis continuedTechniques For Prenatal Diagnosis continued
General Criteria For Prenatal DiagnosisGeneral Criteria For Prenatal Diagnosis
Criteria of the disorder to be diagnosed prenatally:1. High risk2. Severe disorder3. Treatment not available4. Reliable prenatal test available5. Accepted to parents
Before birth diagnosis of inherited metabolic diseases
(cont.)
1- Prenatal Diagnosis (chrorinic villus biopsy)
At earlier stage of pregnancy than amniocentesis: (from 10th week of
pregnancy, first trimester)
Biopsy can be used for karytyping and gene probe diagnosis.
It takes ~ 10 days
It has been applied particularly for Hemoglobinpathies (e.g. sickle cell disease, etc) cystic fibrosis Duchene's muscular dystrophy.
2- Prenatal Diagnosis (amniocentesis)
Carried out at about 15th week of pregnancy (second trimester) from amniotic fluid for cytogenic reasons
(e.g. detect chromosomal disorders as Down’s syndrome)
Diagnosis is usually made on the basis of enzyme studies carried out on fibroblasts cultured from the amniotic fluid.
Before birth diagnosis of inherited metabolic diseases (cont.)
Screening of Newborns
Programmes for screening all newborns for certain metabolic disorders are
performed with the following criteria:
1- The disease should not be clinically apparent at the time of screening
2- The disease should have a relatively high incidence in the population
screened.
3- The disease should be treatable & so results of screening test must be
obtained before irreversible damage is likely to have occurred.
4- Screening test should be simple (qualitative) & reliable.
Examples of screening programmes:
Phenylketonuria
Congenital hypothyroidism
Galactossemia
⇒Screening of Newborns
A positive screening qualitative test result should be confirmed by
quantitative analysis
In a second positive test, the individual might be required to be reassessed
after a period of time in some cases.

Clinical features are often nonspecific and include failure to thrive, feeding difficulties, vomiting, hypotonia and fits, etc…
There may be symptom-free period after birth
It is very important to establish whether there is a relationship between onset
of disease and changes in feeding patterns (e.g. galactosemia after introduction of milk).
So what about role lab investigations in diagnosis??
In Neonates & InfantsIn Neonates & Infants
1- Basic investigations: Carried as a part of normal care of a risk infant Nonspecific as determination of plasma glucose & blood gases May show results consistent with inherited metabolic disease.
2- Metabolic tests: Provide an additional evidence The measurement of specific metabolites Determination of enzyme activity (of the enzyme responsible for the
inherited metabolic disorder). May be a part neonatal screening i.e. for phenylketonuria in first days of
life
3- Sequencing of the specific gene (molecular genetic techniques): Using PCR and gene sequencer, etc….(Molecular Genetics) Karytyping may help in some cases: (chromosomal study,
cytogenetics)
Laboratory investigations for neonates & infants

Examples of Genetic Diseases

A.Single-gene Disorders- Adenosine deaminase deficiency
- Alpha-1-antitypsin deficiency - Cystic fibrosis - Duchenne muscular dystrophy - Familial hypercholesterolemia - Hemophilia A and B - G-6-PD deficiency - Phenylketonuria - Sickle cell anaemia - Thalassaemia
C. Multifactorial Disorders (i) Congenital malformation - Cleft lip and cleft palate - Congenital heart disease - Neural tube defects(ii) Adult onset disease - Cancer (some) - Coronary artery disease - Diabetes mellitus

Disorder Incidence
Cleft lip/ Cleft palate 1/250 – 1/600
Congenital heart disease 1/125 – 1/250
Neural tube defects 1/100 – 1/500
Coronary heart disease 1/15 – Variable
Diabetes mellitus 1/10 – 1/20
Cancer variable
Examples of Multifactorial disorder
D.Mitochondrial Disorders
Lebers hereditary optic neuropathy
E. Acquired somatic genetic disorders
Some forms of cancer





























