Embed Size (px)
Citation preview

© 2000 Wiley-Liss, Inc.
Seminars in Surgical Oncology 2000; 18:281–286SSU 955
Genes Implicated in Hereditary BreastCancer Syndromes
PATRICIA N. TONIN, PhD1,2,3*1Department of Medicine, Division of Medical Genetics, McGill University, Montréal,
Québec, Canada2Department of Human Genetics, McGill University, Montréal, Québec, Canada
3Montréal General Hospital Research Institute, Montréal, Québec, Canada
The medical histories of breast cancer-prone families have been described for over a century.The pattern of breast cancer occurrences in these families is most consistent with an autoso-mal dominant mode of inheritance. The location of a gene that could explain the pattern oftransmission of the breast cancer trait in families averaging early (pre-menopausal) onset ofbreast cancer was reported in 1990. Since then, two genes have been identified: BRCA1 andBRCA2. Germ-line mutations in these two genes confer susceptibility to breast (female andmale) and ovarian cancer, and account for a significant proportion of hereditary breast cancerin two cancer syndromes: site-specific breast cancer and the breast-ovarian cancer syndrome.Other hereditary syndromes that feature breast cancer are Li-Fraumeni syndrome, Cowdendisease, and ataxia telangiectasia, whose carriers have been shown to harbor germ-line muta-tions in TP53, PTEN, and ATM, respectively. There may be other genetic factors that contrib-ute to hereditary breast cancer, since not all families with multiple cases of breast cancerharbor germ-line BRCA1 or BRCA2 mutations. Host factors (such as lifestyle choices) andother genes may modulate risk of breast cancer in mutation carriers. Semin. Surg. Oncol.18:281–286, 2000. © 2000 Wiley-Liss, Inc.
KEY WORDS: breast neoplasms; male breast neoplasms; ovarian neoplasms; BRCA1;hereditary neoplastic syndromes; tumor suppressor genes; mutation; germ-line mutation; genetic predisposition to disease; age factors; risk assessment;linkage (genetics); pedigree; Jews; polymerase chain reaction; Li-Fraumenisyndrome; TP53; ataxia telangiectasia; multiple hamartoma syndrome
Contract grant sponsor: Cancer Research Society and Medical ResearchCouncil of Canada.
*Correspondence to: Patricia Tonin, Ph.D., Medical Genetics, MontrealGeneral Hospital, 1650 Cedar Avenue, Room L10-120, Montreal, Que-bec, Canada H3A 1A1. E-mail: [email protected]
INTRODUCTION
Breast cancer is the most common malignancy amongwomen. As with all cancers, breast cancer is a genetic dis-ease, arising from an accumulation of mutations that pro-mote clonal selection of cells with increasingly aggressivebehavior. The vast majority of described mutations in breastcancer are somatic (acquired) mutations found only in tu-mor cells and not in normal tissue from the same individual.What was perhaps the first suggestion of the existence of ahereditary factor in breast cancer came from the descrip-tion of a family with four generations of breast cancer,reported more than a century ago [1]. Since then a vastnumber of breast cancer families have been reported. Thenumber of cancers in many of these families was too greatto be explained by chance or by environmental factors. Astriking feature of many of these families was the earlyage of onset of breast cancer: the patients were often pre-menopausal, with an average age at diagnosis of under 50.
The pattern of breast cancer occurrences in these familiesis most consistent with an autosomal dominant mode ofinheritance [2]. This implies a mode of genetic transmis-sion wherein a single mutant allele, a specific form of agene, is sufficient to promote breast cancer, and the alleleis carried on the non-sex chromosome. Thus, in a familywith multiple cases of breast cancer, each child has a 50%risk of inheriting the disease-related allele. One may ex-pect that certain branches of the family will contain mul-tiple cases of breast cancer while other branches do not.This mode of transmission on an autosome (not on the Xor Y chromosome) also implies that the mutant allele can

282 Tonin
be transmitted by either the female members or the malemembers of a family.
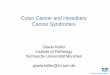
Analysis of data collected during the Cancer and Ste-roid Hormone Study (CASH) [3] provided some measureof the effect of family history on breast cancer. The CASHregistry collected family history data on 4,370 cases ofbreast cancer and 4,688 controls. Empiric risk estimatesprovide an alternate method of quantifying the magnitudeof risk associated with a family history of breast cancer.The estimates shown in Table I are derived from math-ematical models that used the population-based family his-tory of the CASH registry [4]. In this study group, womenwith both a mother and sister with breast cancer have anapproximately 14-fold greater risk of developing breastcancer. The cumulative risk by age 80 for breast cancer isthe highest for an individual with two first-degree rela-tives diagnosed with breast cancer under age 50 (Table I).It is therefore apparent that both the number of relativeswith breast cancer and the age at onset of breast cancerhave an impact on the relative risk of breast cancer. Com-plex analyses of the manner in which traits segregate inthe breast cancer families provided the first evidence that,in some families, the incidence of breast cancer could beattributed to an autosomal dominant susceptibility allelewith a lifetime penetrance (expression of a genetic trait inan individual with the mutant allele) of 92% [4,5]. Fur-thermore, the effect of a mutant allele on the risk of breastcancer was shown to be a function of a woman’s age, withthe ratio of age-specific risks greatest at young ages. Theproportion of cases with the susceptibility allele was pre-dicted to be 36% among ages 20 to 29 years, and only 1%among ages 80 and older. These studies also suggested thatone or more breast cancer susceptibility alleles contributeto 5% to 10% of all breast cancer, and that approximatelyone of every 152 women in the general population maycarry a predisposing mutation in one of these genes.
Clinical investigations of familial aggregation of breast
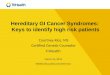
cancer have identified several genetic syndromes with anautosomal dominant pattern of inheritance that featuresbreast cancer [6]. The syndromes in which genes are knownor are suggested to cause inherited breast cancer and othercancers are shown in Table II.
BRCA1 AND BRCA2 GENES
The existence of the BRCA1 gene, which predisposesto breast cancer, was demonstrated by linkage analysis in1990 [7]. Using polymorphic markers, which would dis-tinguish the parental origins of alleles and are representa-tive of different chromosomal regions, linkage wasestablished to the long arm of chromosome 17 at regionq21. Subsequent reports provided evidence for the coin-cident transmission of breast cancer and ovarian cancersusceptibility in several previously unreported families,and confirmed results of linkage between breast and ova-rian cancers and genetic markers on chromosome 17q[8,9]. Families with early age of onset (pre-menopausal)of breast cancer were more likely to be linked to theBRCA1 locus [7,9], consistent with earlier predictionsbased on the analysis of the data in the CASH registry [4].Through an intense cloning effort, the identity of BRCA1was discovered in 1994 [10]. Around the same time, evi-dence for the existence of another breast cancer suscepti-bility gene, BRCA2, was provided by linkage analyses[11], and subsequently identified about a year later [12,13].The identification of the breast cancer susceptibility genesBRCA1 and BRCA2 allows for the direct detection ofmutation carriers.
Germ-line mutations in BRCA1 and BRCA2 have beenreported in at least two syndromes that feature breast can-cer: site-specific breast cancer and breast-ovarian cancersyndrome (Table II). The striking feature common to fami-lies of both syndromes is the young age at onset of breastcancer. Until recently, the most widely quoted estimatesof cancer risk in carriers of mutant alleles were based on
TABLE I. Estimated Effect of Family History on Lifetime BreastCancer Risk*
Cumulative breastAffected relative(s) cancer risk(on the same side Age of affected by age 80of the family) relative(s) (years) (%)
One first-degree < 50 13–21> 50 9–11
One second-degree < 50 10–14> 50 8–9
Two first-degree < 50 35–48> 50 11–24
Two-second-degree < 50 21–26> 50 9–16
*Empiric risk estimates were derived from mathematical models thatused population-based family history data [63]. Empiric risks describedare the cumulative risk for breast cancer incidence by age 80 given aparticular family history.
TABLE II. Hereditary Cancer Syndromes that FeatureBreast Cancer
Syndrome Gene Manifestations
Breast–ovarian cancer BRCA1 Breast (female) and male) andovarian cancers
BRCA2Site-specific breast cancer BRCA1 Breast cancer (female and
male)BRCA2
Li-Fraumeni syndrome TP53 Sarcoma, leukemia, breast,brain and adrenal cancers
Cowden disease PTEN Breast and thyroid cancers,multiple hamartomas ofskin and gastrointestinaltract
Ataxia telangiectasia ATM Leukemia, lymphomas, breastcancers

Hereditary Breast Cancer Syndromes 283
the selected high-risk families involved in the InternationalBreast Cancer Linkage Consortium (IBCLC). A study in-volving families with at least four cases of breast or ova-rian cancer diagnosed under age 60 [14] suggested acumulative risk of breast and ovarian cancer in BRCA1carriers by age 70, estimated at 87% and 44%, respectively.A slightly higher risk by age 70 (63%) was estimated in are-evaluation of the same data [15]. The analyses in an-other study [16] of two large BRCA2-linked families sug-gested a cumulative risk of breast cancer in BRCA2 carriersat age 80. This study also demonstrated a cumulative riskof male breast cancer that was estimated to be 6% by age70, which is higher than the cumulative lifetime risk of0.1% in the general population. Male breast cancer hasbeen reported more often in BRCA2-linked families thanin BRCA1-linked families [17,18].
Lower risks of breast and ovarian cancer in mutationcarriers have been reported in population-based studies[19]. It appears that some mutation carriers described inthese studies do not come from typical hereditary breastand ovarian cancer families. It has been suggested that otherfactors may modulate risk in mutation carriers, and mayaccount for the reduced penetrance. Recent studies haveshown that lifestyle choices such as smoking [20] and oralcontraceptive pill usage [21] may modulate risk of breastand ovarian cancer, respectively, in mutation carriers.
Prior to the identification of the breast cancer suscepti-bility genes, risk was assessed by inspection of the pedi-gree (number of cases of breast cancer) and age atdiagnosis to establish the risk of breast cancer in the de-scendants of family members with breast cancer. Whenthe location of BRCA1 on chromosome 17q21 was re-ported [7], one could then apply linkage analysis to es-tablish risk in family members. This approach requiredthe cooperation of family members in obtaining bloodsamples. These samples then underwent molecular genetictesting, on DNA extracted from the lymphocytes, to estab-lish whether individuals within the same family had in-herited the genetic marker on chromosome 17q21,which segregated with the disease. This approach wasalso limited because sporadic disease could not be dis-tinguished from breast cancer attributed to a geneticbasis; thus the absence of linkage per se could not ruleout the possibility of genetic basis for a particular fam-ily. Conversely, linkage could occur, but the breast can-cer cases could be due to a chance clustering in a family.With this approach, however, the more breast cancer caseswithin a family, the more powerful are the results of thecomputed linkage analyses, and greater is the likelihoodthat the disease had a genetic basis in the family.
The identification of BRCA1 and BRCA2 facilitatescarrier detection and genetic counseling. More than 100mutations in each gene have been described to date, andthe majority of the mutations are private and reported in
only one family (see Breast Information Core Data Base[22]). BRCA1 is comprised of 5,592 nucleotide pairs with24 exons (a segment of the gene that encodes amino acidsequence of the protein; adjacent exons are separated byintrons, which are spliced out during RNA processing),and BRCA2 is composed of 10,254 nucleotide pairs and27 exons [10,12,13]. The coding sequences of both genesare spread across large tracts of DNA, comprising morethan 1,000,000 nucleotides. The large size and complexityof each gene, and the absence of “hot spots” for muta-tions, have made sequence analysis an arduous and costlyendeavor. After informed consent is obtained, mutationanalysis begins with the acquisition of a blood sample froman affected individual in a high-risk family. The observa-tion that a large majority of germ-line mutations are thetype predicted to result in the production of truncated pro-teins has enabled molecular biologists to use the proteintruncation test (PTT) as an option for mutation analysis[23,24]. Conventional mutation analysis using polymerasechain reaction (PCR)-based technology is performed bysequencing the tracts of genomic DNA that represent thecoding exons extracted from blood lymphocytes. Often,two or more methods are employed to identify sequencevariations more rapidly. In the absence of a known func-tion for BRCA1 and BRCA2, the interpretation of sequencevariations currently rests on the effect the sequence varia-tion has on the predicted protein. Mutations such as frame-shift or nonsense mutations change a codon from an aminoacid to a stop codon, resulting in truncated proteins whichare easier to interpret from missense mutations (mutationsresulting in substitutions of amino acids in the proteinchain) of unknown significance.
Within defined ethnic groups, specific, relatively fre-quent mutations have been identified. Three founder mu-tations (185delAG and 5382insC in BRCA1, and 6174delTin BRCA2) have been identified in the Ashkenazi Jewishfamilies of eastern European ancestry [25–29]. These mu-tations are carried by about 2.5% of the Ashkenazi Jewishpopulation [30–32]. While all three mutations confer anincreased risk to breast and ovarian cancer, the penetranceof the BRCA2 mutation may be less than the BRCA1185delAG mutation. Genetic analyses reveal that thesefounder mutations are likely very old; most carriers in thecommunity are descended from a few ancestors who had ahigh frequency of the gene harboring the sequence varia-tion. Founder mutations may be maintained in populationsdue to a number of factors, such as geographic isolation orreligious affiliations. Specific mutations have also beenidentified in diverse populations, such as in Icelandic,Swedish, British, Austrian, Dutch, Belgian, Russian, Hun-garian, and French Canadian families. Genetic analysis hasprovided evidence for founder effects in these ethnic groups[33–42]. The identification of founder mutations facilitatescarrier detection for certain well-defined populations be-

284 Tonin
cause the mutation screen can be limited to specific panelsof mutations.
A negative test for BRCA1 and BRCA2 in an individualfrom a high-risk family could be due to several possiblefactors, including unidentified mutation due to the limita-tions of sequence analysis, other known or unknown genes(see below), and familial aggregation of breast cancer casesdue to chance (possibly due to shared environmental riskfactors). If the case tested in the family was a sporadicbreast cancer, and thus the occurrence of the disease in thebreast cancer family was by chance, this would also con-found the linkage analysis.
Several studies have found that up to 20% of familieswith multiple cases of breast cancer show no linkage toeither BRCA1 or BRCA2 after extensive testing [43]. Al-though this could be due to as-yet-unidentified mutationsin these genes, it is possible that novel genes (such asBRCA3?) will be identified in some of these families [44].
TUMOR SUPRESSOR GENE TP53
Breast cancer is also found in rare genetic syndromes,such as Li-Fraumeni syndrome (LFS) (Table II). The spec-trum of cancers in LFS families also includes soft tissuesarcomas, brain tumors, osteosarcomas, leukemia, andadrenocorticol carcinoma [45]. The diverse tumor types infamily members characteristically develop at unusuallyearly ages, and multiple primary tumors are frequent. Theclassic definition of this syndrome is the development of asarcoma in an individual before age 45, who has two first-degree relatives diagnosed with cancer before the age of45. Segregation analysis demonstrated that the observedcancer distribution in families best fit a rare autosomaldominant gene model [46]. This model predicted that inat-risk families the probability of developing any invasivecancer (with the exception of skin cancers) approaches 50%by age 30, and more than 90% by age 70 [47]. The tumorsuppressor gene, TP53, located on chromosome 17 at re-gion p13.1, was a likely candidate because somatic inacti-vating mutations in TP53 had been reported in the types oftumors encountered in the LFS families. TP53 was also astrong candidate because transgenic mice carrying mutantTP53 alleles have an increased incidence of cancers foundin association with individuals in LFS families. Germ-linemutations in the TP53 may account for up to 1% of breastcancer cases diagnosed under the age of 35 [47]. Althoughmutations in TP53 have been reported to occur throughoutthe gene, mutation analysis in LFS families has revealedthat the majority of mutations are located between exons 5and 8, and that approximately 50% of patients with LFShave no mutation in the coding region of TP53 [48]. Anexhaustive analysis for germ-line TP53 mutation did notreveal any mutation in a large, classical LFS kindred [49].Since germ-line mutations are identified in only 30% offamilies, it is possible that other factors (genetic or envi-
ronmental) may be contributing to the development of can-cer in LFS families.
PTEN GENE
Multiple hamartomatous lesions, especially of the skin,mucus membranes, colon, breast, and thyroid, and mul-tiple facial trichilemmomas are encountered in Cowdendisease (Table I). Hamartomatous polyps of the colon alsooccur, and there are neoplasms of the thyroid and breast.Family-based analysis suggested an autosomal dominantmode of inheritance with high penetrance in both sexes[50], and a high frequency of breast cancer (up to 30%) infemales [51]. Linkage analysis of Cowden disease fami-lies revealed a locus on chromosome 10q22-23 [52]. PTENwas the strongest candidate gene that mapped to this inter-val on chromosome 10 and was previously shown to har-bor somatic mutations in a number of tumor types,particularly breast cancer, that feature in Cowden disease.Therefore, a combination of linkage analysis and candi-date gene approaches led to the discovery that individualswith Cowden disease harbored germline mutations inPTEN [53]. Although the reported mutations are dispersedthroughout the gene, there is a tendency of mutations tocluster in exon 5 [54].
ATAXIA TELANGIECTASIS MUTATED(ATM) GENE
Ataxia telangiectasia (AT) is an autosomal recessivedisorder characterized by cerebellar ataxia, telangiectases,immune defects, and a predisposition to malignancy. Themode of inheritance in this syndrome implies the alleleexerts its phenotype effect only if present in a homozy-gous state. Thus, unlike the situation of carriers of BRCA1,BRCA2, TP53, and PTEN described above, the affectedindividual must have inherited at-risk alleles from bothparents. Cells from AT patients are abnormally sensitiveto ionizing radiation, and chromosomal breakage is a fea-ture. Mutations in the ATM located on chromosome 11q23have been described in AT patients. An early study exam-ining the risk of cancer in heterozygotes (individuals hav-ing one mutant allele) revealed that females predicted tobe heterozygous for AT (that is, having one mutant andone normal allele at the AT locus) were at increased riskfor breast cancer [56]. The estimated risk for breast cancerwas 5.1 in a prospective study of 1,599 adult relatives withAT distributed in 161 families [56]. In addition, womenwith breast cancer were more likely to have been exposedto ionizing radiation than were the controls without can-cer. The contribution of the AT gene in familial cancer islikely to be minimal, as one study found no evidence oflinkage analysis to the AT locus on chromosome 11q infamilial cancer [57]. Genotyping of relatives of AT patientsrevealed that the breast cancer risk for AT heterozygouswomen is not limited to young women who are AT het-

Hereditary Breast Cancer Syndromes 285
erozygotes [58]. In that study it was estimated that, of allbreast cancers in the U.S., 6.6% might occur in womenwho are AT heterozygotes. A germ-line mutation analysisof the ATM detected heterozygous ATM mutation in 1%of the controls, consistent with the frequency of AT carri-ers predicted from epidemiological studies [59].
OTHER GENES THAT MODIFY RISK INHEREDITARY CANCER FAMILIES
The observation that mutation carriers who do not comefrom typical hereditary breast cancer families may havesignificantly lower risks of breast and ovarian cancer sug-gests that there may be other genes that can modulate theeffects of mutation carriers. One such gene may be HRAS1.A human homologue of the Harvey rat sarcoma-1 viraloncogene, HRAS1 is located on chromosome 11 regionp15.5. The HRAS1 locus is tightly linked to a mini-satel-lite (short tracks of repeated nucleotide sequences) locatedapproximately 1,000 base pairs downstream from the gene-coding sequences. The mini-satellite DNA is composed of30 to 100 units of a 28 base-pair consensus sequence, and30 alleles of 1,000 to 3,000 base pairs have been described.Rare alleles appear in the genomes of patients with cancerabout three times as often as in controls without cancer[60,61]. Since the carrier frequency is between 5% and20%, approximately 3% to 8% of all breast cancer couldbe attributed to HRAS1 [61]. There was a significant as-sociation of the rare HRAS1 alleles in four types of can-cer, including breast cancer. Recently, a modifier effectassociated with the rare HRAS1 alleles on the penetranceof the BRCA1 gene in causing ovarian cancer was dem-onstrated [62]. Although rare HRAS1 alleles did not ap-pear to modulate risk of breast cancer in mutation carriers,the risk for ovarian cancer was 2.11-fold greater for BRCA1carriers harboring one or two rare HRAS1 alleles than forcarriers with only common alleles.
CONCLUSIONS
While the identification of cancer susceptibility geneshas improved risk assessment, questions remain concern-ing the risks and benefits of mutation testing. Until a clearerpicture emerges, risk assessment and the interpretation oftest results should occur in the context of a genetic coun-seling unit specializing in adult-onset cancers.
REFERENCES1. Broca PP: “Traite des Tumeurs”. Vols. 1 and 2. Paris: Asselin; 1866–
1869.2. Lynch HT: “Genetics and Breast Cancer.” New York: Reinhold;
1981.3. Stattin RW, Rubin GL, Webster LA, et al: Family history and the
risk of breast cancer. JAMA 1985;253:1908–1913.4. Claus EB, Risch N, Thompson WD: Genetic analysis of breast can-
cer in the cancer and steroid hormone study. Am J Hum Genet1991;48:232–242.
5. Newman B, Austin MA, Lee M, King MC: Inheritance of human
breast cancer: evidence for autosomal dominant transmission in high-risk families. Proc Natl Acad Sci USA 1988;85:3044–3048.
6. Hoskins KF, Stopfer JE, Calzone KA, et al: Assessment and coun-seling for women with a family history of breast cancer. A guide forthe clinician. JAMA 1995;273:577–585.
7. Hall JM, Lee MK, Newman B, et al: Linkage of early onset familialbreast cancer to chromosome 17q21. Science 1990;250(4988):1684–1689.
8. Narod SA, Feunteun J, Lynch HT, et al: Familial breast-ovariancancer locus on chromosome 17q12-q23. Lancet 1991;338(8759):82–83.
9. Easton DF, Bishop DT, Ford D, Crockford GP: Genetic linkageanalysis in familial breast and ovarian cancer: results from 214 fami-lies. The Breast Cancer Linkage Consortium. Am J Hum Genet1993;52:678–701.
10. Miki Y, Swensen J, Shattuck-Eidens D, et al: A strong candidate forthe breast and ovarian cancer susceptibility gene BRCA1. Science1994;266(5182):66–71.
11. Wooster R, Neuhausen SL, Mangion J, et al: Localization of a breastcancer susceptibility gene, BRCA2, to chromosome 13q12-13 bygenetic linkage analysis. Science 1994;265(5181):2088–2090.
12. Wooster R, Bignell G, Lancaster J, et al: Identification of the breastcancer susceptibility gene BRCA2 [published erratum appears inNature 1996;379(6567):749]. Nature 1995;378(6559):789–792.
13. Tavtigian SV, Simard J, Rommens J, et al: The complete BRCA2gene and mutations in chromosome 13q-linked kindreds. Nat Genet1996:12:333–337.
14. Ford D, Easton DF, Stratton M, et al; Genetic heterogeneity andpenetrance analysis of BRCA1 and BRCA2 genes in breast cancerfamilies. The Breast Cancer Linkage Consortium. Am J Hum Genet1998;62:676–689.
15. Easton DF, Ford D, Bishop DT: Breast and ovarian cancer inci-dence in BRCA1 mutation carriers. The Breast Cancer Linkage Con-sortium. Am J Hum Genet 1995;56:265–271.
16. Easton DF, Steele L, Fields P, et al: Cancer risks in two large breastcancer families linked to BRCA2 on chromosome 13q12-13. Am JHum Genet 1997;61:120–128.
17. Strattton MR, Ford D, Neuhausen S, et al: Familial male breast can-cer is not linked to the BRCA1 locus on chromosome 17q. Nat Genet1994;7:103–107.
18. Couch FJ, Farid LM, DeShano ML, et al: BRCA2 germline muta-tions in male breast cancer cases and breast cancer families. NatGenet 1996;13:123–125.
19. Struewing JP, Hartge P, Wacholder S, et al: The risk of cancer asso-ciated with specific mutations of BRCA1 and BRCA2 amongAshkenazi Jews. N Engl J Med 1997;336:1401–1408.
20. Brunet J, Ghadirian P, Rebbek TR, et al: The effect of smoking onbreast cancer in BRCA1 and BRCA2 carriers. J Natl Cancer Inst1998;90:761–766.
21. Narod SA, Risch H, Moslehi R, et al: Oral contraceptives and therisk of hereditary ovarian cancer. Hereditary Ovarian Cancer Clini-cal Group. N Engl J Med 1998; 339:424–426.
22. Breast Cancer Information Core (BIC) [web page]. Bethesda, MD;National Human Genome Research Institute [cited 00 March 13].Available from: http://www.nhgri.nih.gov/Intramural_research/Lab_transfer/Bic.
23. Hogervorst FB, Cornelis RS, Bout M, et al: Rapid detection ofBRCA1 mutations by the protein truncation test. Nat Genet 1995;10:208–212.
24. Weber BH, Brohm M, Stec I, et al: A somatic truncating mutation inBRCA2 in sporadic breast tumor [letter]. Am J Hum Genet1996;59:962–964.
25. Friedman LS, Szabo CI, Ostermeyer EA, et al: Novel inherited mu-tations and variable expressivity of BRCA1 alleles, including thefounder mutation 185delAG in Ashkenazi Jewish families. Am JHum Genet 1995;57:1284–1297.
26. Struewing JP, Brody LC, Erdos MR, et al: Detection of eight BRCA1mutations in 10 breast/ovarian cancer families, including 1 familywith male breast cancer. Am J Hum Genet 1995;57:1–7.
27. Tonin P, Weber B, Offit K, et al: Frequency of recurrent BRCA1and BRCA2 mutations in Ashkenazi Jewish breast cancer families[Review]. Nat Med 1996;2:1179–1183.

286 Tonin
28. Berman DB, Costalas J, Schultz DC, et al: A common mutation inBRCA2 that predisposes to a variety of cancers is found in bothJewish Ashkenazi and non-Jewish individuals. Cancer Res1996;56:3409–3414.
29. Neuhausen S, Gilweski T, Norton L, et al: Recurrent BRCA26174delT mutations in Ashkenazi Jewish women affected by breastcancer. Nat Genet 1996;13:126–128.
30. Struewing JP, Abeliovich D, Peretz T, et al: The carrier frequencyof the BRCA1 185delAG mutation is approximately 1 percent inAshkenazi Jewish individuals [published erratum appears in NatGenet 1996;12:110]. Nat Genet 1995;11:198–200.
31. Oddoux C, Struewing JP, Clayton CM, et al: The carrier frequencyof the BRCA2 6174delT mutation among Ashkenazi Jewish indi-viduals is approximately 1%. Nat Genet 1996;14:188–190.
32. Roa BB, Boyd AA, Volcik K, Richards CS: Ashkenazi Jewish popu-lation frequencies for common mutations in BRCA1 and BRCA2.Nat Genet 1996;14:185–187.
33. Gayther SA, Warren W, Mazoyer S, et al: Germline mutationsof the BRCA1 gene in breast and ovarian cancer families pro-vide evidence for genotype-phenotype correlation. Nat Genet1995;11:428–433.
34. Shattuck-Eidens D, McClure M, Simard J, et al: A collaborativesurvey of 80 mutations in the BRCA1 breast and ovarian cancersusceptibility gene. Implications for presymptomatic testing andscreening. JAMA 1995;273:535–541.
35. Johannsson O, Ostermeyer EA, Hakansson S, et al: FoundingBRCA1 mutations in hereditary breast and ovarian cancer in south-ern Sweden. Am J Hum Genet 1996;58: 441–450.
36. Johannesdottir G, Gudmundsson J, Bergthorsson JT, et al: Highprevalence of the 999del5 mutation in Icelandic breast and ovariancancer patients. Cancer Res 1996;56:3663–3665.
37. Wagner TM, Moslinger R, Zielinski C, et al: New Austrian muta-tion in BRCA1 gene detected in three unrelated HBOC families[letter]. Lancet 1996;347(9010):1263.
38. Gayther SA, Harrington P, Russell P, et al: Frequently occurringgerm-line mutations of the BRCA1 gene in ovarian cancer familiesfrom Russia [letter]. Am J Hum Genet 1997;60:1239–1242.
39. Peelen T, van Vliet M, Petrij-Bosch A, et al: A high proportion ofnovel mutations in BRCA1 with strong founder effects among Dutchand Belgian hereditary breast and ovarian cancer families. Am JHum Genet 1997;60:1041–1049.
40. Ramus SJ, Kote-Jarai Z, Friedman LS, et al: Analysis of BRCA1and BRCA2 mutations in Hungarian families with breast or breast-ovarian cancer [letter]. Am J Hum Genet 1997;60:1242–1246.
41. Shattuch-Eidens D, Oliphant A, McClure M, et al: BRCA1 sequenceanalysis in women at high risk for susceptibility mutations. Riskfactor analysis and implications for genetic testing. JAMA1997;278:1242–1250.
42. Tonin PN, Mes-Masson AM, Futreal PA, et al: Founder BRCA1and BRCA2 mutations in French Canadian breast and ovarian can-cer families. Am J Hum Genet 1998;63:1341–1351.
43. Serova OM, Mazoyer S, Puget N, et al: Mutations in BRCA1 andBRCA2 in breast cancer families: are there more breast cancer sus-ceptibility genes? Am J Hum Genet 1997;60:486–495.
44. Ford D, Easton DF, Bishop DT, et al: Risks of cancer in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Lancet1994;343(8899):692–695.
45. Li FP, Fraumeni JF Jr: Soft-tissue sarcoma, breast cancer, and otherneoplasms. A familial syndrome? Ann Intern Med 1969;71:747–752.
46. Strong LC, Stine M, Norsted TL: Cancer in survivors of childhoodsoft tissue sarcoma and their relatives. J Natl Cancer Inst1987;79:1213–1220.
47. Malkin D, Li FP, Strong LC, et al: Germ line p53 mutations in afamilial syndrome of breast cancer, sarcomas, and other neoplasms.Science 1990;250(4985):1233–1238.
48. Frebourg T, Barbier N, Yan YX, et al: Germline-p53 mutations in15 families with Li-Fraumeni syndrome. Am J Hum Genet1995;56:608–615.
49. Evans SC, Mims B, McMasters KM, et al: Exclusion of a p53germline mutation in a classic Li-Fraumeni syndrome family. HumGenet 1998;102:681–686.
50. Starink TM, van der Veen JP, Arwert F, et al: The Cowden syn-drome: a clinical and genetic study in 21 patients. Clin Genet1986;29:222–233.
51. Schrager CA, Schneider D, Gruener AC, et al: Clinical and patho-logical features of breast disease in Cowden’s syndrome: anunderrecognized syndrome with an increased risk of breast cancer.Hum Pathol 1998;29:47–53.
52. Nelen MR, Padberg GW, Peeters EA, et al: Localization of the genefor Cowden disease to chromosome 10q22-23. Nat Genet1996;13:114–116.
53. Liaw D, Marsh DJ, Li J, et al: Germline mutations of the PTENgene in Cowden disease, an inherited breast and thyroid cancer syn-drome. Nat Genet 1997;16:64–67.
54. Nelen MR, van Stavern WC, Peeters EA, et al: Germline mutationsin PTEN/MMAC1 gene in patients with Cowden disease. Hum MolGenet 1997;6:1383–1387.
55. Swift M, Reitnauer PJ, Morrell D, Chase CL: Breast and other can-cers in families with ataxia-telangiectasia. N Engl J Med1987;316:1289–1294.
56. Swift M, Morrell D, Massey RB, Chase CL: Incidence of cancer in161 families affected by ataxia-telangiectasia. N Engl J Med1991;325:1831–1836.
57. Wooster R, Ford D, Mangion J, et al: Absence of linkage to theataxia telangiectasia locus in familial breast cancer. Hum Genet1993;92:91–94.
58. Athma P, Rappaport R, Swift M: Molecular genotyping shows thatataxia-telangiectasia heterozygotes are predisposed to breast can-cer. Cancer Genet Cytogenet 1996;92:130–134.
59. FitzGerald MG, Bean JM, Hegde SR, et al: Heterozygous ATM mu-tations do not contribute to early onset of breast cancer. Nat Genet1997;15:307–310.
60. Krontiris TG, DiMartino NA, Colb M, Parkinson DR: Unique allelicrestriction fragments of the human Ha-ras locus in leukocyte and tu-mour DNAs of cancer patients. Nature 1985;313(6001):369–374.
61. Krontiris TG, Devlin B, Karp DD, et al: An association between therisk of cancer and mutations in the HRAS1 minisatellite locus. NEngl J Med 1993;329:517–523.
62. Phelen CM, Rebbeck TR, Weber BL, et al: Ovarian cancer risk inBRCA1 carriers is modified by the HRAS1 variable number of tan-dem repeat (VNTR) locus. Nature Genet 1996;12:309–311.
63. Claus EB, Risch N, Thompson WD: Autosomal dominant inherit-ance of early-onset breast cancer. Implications for risk prediction.Cancer 1994;73:643–651.