Embed Size (px)
Citation preview

REVIEW
Gastrointestinal hormones and polycystic ovary syndrome
Jing Ma • Tzu Chun Lin • Wei Liu
Received: 19 February 2014 / Accepted: 16 April 2014
� Springer Science+Business Media New York 2014
Abstract Polycystic ovary syndrome (PCOS) is an endo-
crine disease of women in reproductive age. It is character-
ized by anovulation and hyperandrogenism. Most often
patients with PCOS have metabolic abnormalities such as
dyslipidemia, insulin resistance, and glucose intolerance. It
is not surprising that obesity is high prevalent in PCOS. Over
60 % of PCOS women are obese or overweight. Modulation
of appetite and energy intake is essential to maintain energy
balance and body weight. The gastrointestinal tract, where
nutrients are digested and absorbed, plays a central role in
energy homeostasis. The signals from the gastrointestinal
tract arise from the stomach (ghrelin release), proximal small
intestine (CCK release), and distal small intestine (GLP-1
and PYY) in response to food. These hormones are recog-
nized as ‘‘appetite regulatory hormones.’’ Weight loss is the
key in the treatments of obese/overweight patients with
PCOS. However, current non-pharmacologic management
of body weight is hard to achieve. This review highlighted
the gastrointestinal hormones, and discussed the potential
strategies aimed at modifying hormones for treatment in
PCOS.
Keywords Gastrointestinal hormones � Obesity � PCOS
Introduction
Polycystic ovary syndrome (PCOS) is a common reason for
female infertility, affecting up to 4–7 % of women at
reproductive age according to the National Institutes of
Health (NIH) criteria [1, 2] or 15–18 % according to the
criteria of the European Society of Human Reproductive and
Embryology/American Society for Reproductive Medicine
(ESHRE/ASRM) [3]. The etiology of PCOS remains
unclear. Recent study reported that adiponectin gene poly-
morphisms are related to the development of PCOS [4]. The
clinical features of PCOS include hyperandrogenism and
ovarian dysfunction. Women with PCOS have increased
chance of metabolism dysfunctions [5], such as hyperinsu-
linaemia and dyslipidemia, eventually develop into obesity,
type 2 diabetes mellitus (T2DM), and cardiovascular dis-
eases (CVD) [3]. Chronic low-grade inflammation is likely
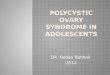
the important factor of insulin resistance in PCOS [6]. High
prevalence of obesity exacerbates insulin resistance, the
abdominal fat deposition, and androgen secretion in women
with PCOS [7] (Fig. 1). Animal models of PCOS exposure to
chronic hyperandrogenism present increased food intake [8].
It suggests that impaired appetite regulation might contribute
to the pathophysiology of PCOS [9]. Therefore, dietary,
exercise, medication and surgery are always major therapies
of weight loss in patients with PCOS [10, 11]. The paper
focused on the body weight management related to gastro-
intestinal hormones modification in PCOS.
Energy intake and gastrointestinal hormones in PCOS
Modulation of appetite and energy intake is essential to
maintain energy balance and body weight. Short-term
appetite and food intake can be regulated by the hypothala-
mus, which constitutes a central control mechanism, and by a
peripheral mechanism, constituted by signals arising from
the gastrointestinal tract [12]. The crucial roles of gastric
emptying/distention and the release of peptide hormones
such as cholecystokinin (CCK), glucagon-like peptide
J. Ma � T. C. Lin � W. Liu (&)
Division of Endocrinology and Metabolism, Department
of Internal Medicine, Renji Hospital Affiliated to Shanghai
Jiaotong University School of Medicine, Shanghai, China
e-mail: [email protected]
123
Endocrine
DOI 10.1007/s12020-014-0275-1

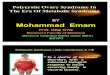
(GLP-1), and peptide tyrosine–tyrosine (PYY) in response to
nutrient intake are increasingly being recognized as impor-
tant physiological regulators of appetite (Fig. 2). A better
understanding of the appetite regulation in PCOS is required
to enable the development of effective therapies [13, 14].
Ghrelin
Ghrelin, a 28-amino acid peptide, is an orexigenic hor-
mone, which is secreted mostly from the gastric mucosa;
small quantities can be found in the duodenum and hypo-
thalamus [15]. Plasma ghrelin concentrations are high in
the fasting state and decrease with nutrient ingestion [16].
Ghrelin declines equally after gastric, intraduodenal, and
intrajejunal nutrient infusions in rodents and humans,
suggesting that gastric distension does not regulate its
suppression [17, 18]. Rather, exposure of the small intes-
tine to nutrients is required to suppress ghrelin [18]. Fasting
and postprandial fluctuations of ghrelin are also related to
insulin concentrations and sensitivity [19]. For example,
obese individuals with insulin resistance have a blunted
suppression of ghrelin in response to nutrients [20].
In both rodents [15] and humans [21], exogenous ghrelin
administration increases energy intake, while patients with
Prader-Willi syndrome, characterized by excessive feeding
behavior, have high levels of circulating ghrelin [22].
Proximal Roux-en-Y gastric bypass decreases ghrelin
secretion, which may contribute to weight loss after this
procedure [23]. Ghrelin modulates appetite via the arcuate
nucleus (ARC) of the hypothalamus [24]; it enhances
neuropeptide Y (NPY) and agouti-related peptide (AgRY)
gene expression and release in the lateral hypothalamic
nucleus (LHA), and inhibits the anorexigenic proopio-
melanocortin (POMC) neurons in the ARC [25]. In contrast
to ghrelin, leptin, an anorexigenic hormone, inhibits orex-
igenic neurons containing NPY and AgRY, while stimu-
lating POMC neurons in the ARC [26]. Leptin attenuates
the activity of ghrelin in the ARC and suppresses food
intake. Thus, ghrelin and leptin interact with each other in
the appetite center, in the so-called ‘‘ghrelin-leptin tango’’
[27]. Ghrelin receptor antagonist, JMV 2959, which is
under research, might have the benefit in the treatment of
obesity [28].
Ghrelin levels in PCOS patients are reported to be
decreased [29] or not different [30] compared to control
subjects. Postprandial fluctuations of ghrelin are related to
insulin concentrations and insulin sensitivity [31]. Ghrelin
levels are lower in obese women suffering from PCOS than
lean women with PCOS and health controls [32]. The
impaired postprandial ghrelin levels may be involved in the
development of obesity in PCOS [32]. Some studies sug-
gested that low ghrelin levels in PCOS might be a conse-
quence of the high androgen levels [33]. Moreover,
luteinizing hormone/follicle-stimulating hormone ratio is
also related to ghrelin levels [34].
GLP-1
GLP-1 is released from L-cells, most densely located in the
ileum and colon, although they have also been found more
proximally in the duodenum and jejunum [35]. Fasting
plasma concentrations of total and intact GLP-1 are lowFig. 1 The reproductive and metabolic disorder of PCOS and the
relationship with obesity
Fig. 2 Schematic
representation of
gastrointestinal regulation of
appetite
Endocrine
123

(5–10 pmol/L); in response to a meal rich in fat or carbo-
hydrate, circulating levels of GLP-1 increase up to five fold
within minutes [36]. The half-life of GLP-1 is short
(*2 min), due largely to rapid degradation by the enzyme,
dipeptidyl peptidase-IV (DPP-IV) [37]. DPP-IV, also
known as CD26, cleaves dipeptides from the N-terminal to
inactivate GLP-1 [38]. A large proportion of GLP-1 is
degraded before entering the systemic circulation, by DPP
IV expressed on blood vessels draining the intestinal
mucosa [39].
GLP-1 is one of two known incretin hormones, together
with glucose-dependent insulinotropic polypeptide (GIP).
The insulinotropic effect of GLP-1 is glucose-dependent,
via interaction with a specific receptor expressed on the cell
membrane of b-cells [40]. GLP-1 receptors are found on
b- and D-cells of the pancreas, parietal cells of the stom-
ach, pylorus, adipose tissue, lungs, and the brain. It has
been shown that GLP-1 stimulates b-cell proliferation and
induces islet neogenesis, inhibits apoptosis, and enhances
the differentiation of new b-cells from progenitors in the
pancreatic duct epithelium [41]. In healthy subjects,
endogenous GLP-1 reduces glucagon release from the
a-cells of the pancreas [42], and intravenous administration
of GLP-1 lowers glucagon secretion in patients with T2DM
[43]. Among the multiple physiological effects of GLP-1,
its effect on gastric emptying may outweigh its insulino-
tropic effect in the regulation of postprandial glycaemia
[44]. The mechanism underlying the action of GLP-1 on
motility is complex and not well understood.
Intracerebroventricular injection of GLP-1 inhibits
feeding in rats [45], as does peripheral infusion of GLP-1
and its agonist, exendin-4 [46]. Peripheral administration
of GLP-1 is associated with enhanced satiety and reduction
of food intake in healthy humans [47], the obese [48], and
patients with T2DM [49]. GLP-1 analogs, such as exena-
tide and liraglutide, and DPPIV inhibitors, such as sitag-
liptin are used for the management of glycaemia control in
type 2 diabetic patients.
The incretin effect is reported to be substantially atten-
uated, which potentially leads to insufficient insulin
secretion and potentiates postprandial hyperglycaemia in
type 2 patients [50]. A direct comparison of the incretin
response to intraduodenal glucose deliver between type 2
patients and healthy subjects has been undertaken [51]. It
has shown there were no differences in overall GLP-1
responses to each glucose load between type 2 patients and
healthy subjects. However, an early, albeit transient, peak
in GLP-1 secretion, in response to glucose in healthy vol-
unteers is missing in patients with T2DM.
Some studies reported that the incretin effect is impaired
in obesity with normal glucose tolerance compared to the
lean subjects. It seems that plasma GLP-1 level is inversely
related to BMI. In response to glucose, obese subjects have
lower plasma GLP-1 concentrations [52]. The decreased
levels of incretin hormones may explain the impaired in-
cretin effect in obese subjects [53]. Although some other
studies reported that there were no differences in plasma
GLP-1 between obese and lean people [54, 55], restored
postprandial GLP-1 secretion following weight loss sug-
gests that GLP-1 plays a role in regulation of satiation [56].
The mechanism is likely to be related to exposure of more
distal small intestinal regions (with a larger density of
L-cells) to ingested nutrients. There is evidence of inter-
action between GLP-1 and leptin at peripheral and central
level. Study showed that leptin stimulated GLP-1 secretion
in human L-cells in vitro and in obese mouse [57]. This
interaction is important for understanding the potential to
achieve and maintain weight loss in obesity [58].
Studies on the levels of GLP-1 in PCOS patients have
not been consistent. It has been reported that there was no
difference in incretin hormones between lean patients with
PCOS and controls [59, 60]. It seems that GIP and GLP-1
secretions are not related to hyperinsulinaemia in PCOS.
However, in some larger studies, during OGTT, it exhib-
ited a lower level of GIP [60] or GLP-1 [61] in obese
women with PCOS compared with lean healthy volunteers.
The enteroinsular axis might be impaired in women with
PCOS. It still needs more research studies about the GLP-1
secretion in PCOS.
CCK
CCK is secreted from the I-cells in the duodenum and
upper jejunum, and is also found in the brain. There are a
number of bioactive forms, such as CCK-8, CCK-22, CCK-
33, and CCK-58, of which CCK-33 is the major form in
human plasma and intestine [62]. The half-life of CCK is
*1-2 min. In healthy volunteers, the fasting CCK con-
centration of 1 pmol/L increases to 5–10 pmol/L in
response to a mixed meal [63], peaks at about 30 min, and
returns to the fasting value after *3–5 h [64]. Protein, and
particularly fat, are strong stimuli for CCK secretion,
whereas carbohydrate results in much less stimulation [65].
Small intestinal fat exerts a potent action on slowing
gastric emptying which, in humans, is regulated predomi-
nantly by CCK, via CCK-1 receptors, and abolished by the
CCK-1 antagonist, loxiglumide [66, 67]. CCK slows gas-
tric emptying by relaxing the proximal stomach, increasing
basal and phasic pyloric pressures and suppressing antral
motility [67, 68], mediated by a vago-vagal reflex pathway
[69]. In contrast to its actions on the stomach, exogenous
CCK increases small intestinal motor activity and shortens
the intestinal transit time [70].
CCK was the first gastrointestinal hormone found to be
related to appetite [71]. CCK exerts its effects via two
receptors, CCK-1 and CCK-2. The suppressive effect of
Endocrine
123

CCK on energy intake in rats and humans is predominantly
mediated by CCK-1 receptors [72]. CCK-1 receptor antag-
onists increase meal size, while CCK-1 receptor deficient
rats develop hyperphagia and obesity [73]. In rats, it has been
demonstrated that chronic administration of a CCK antago-
nist results in weight gain out of proportion to increased
feeding [74], but this probably reflects a synergistic effect
between CCK and leptin on energy intake and long-term
balance of body weight [75]. In humans, exogenous CCK
dose-dependently reduces energy intake at a buffet style
meal [76] and the CCK-1 antagonist, loxiglumide, increases
energy intake modestly in healthy adults [77].
Just as GLP-1, potential medications based on CCK to
treat obesity were unsuccessful due to the rapid enzymatic
degradation within minutes [78]. Following studies
develop CCK-1 receptors agonist, (pGlu-Gln)-CCK-8,
which is modified N-terminally. (pGlu-Gln)-CCK-8 is
enzymatically stable with improved therapeutic action
profile. In animals studies, (pGlu-Gln)-CCK-8 markedly
reduces energy intake and body weight [79]. Meantime,
(pGlu-Gln)-CCK-8 injection is associated with modulation
of blood glucose and IR [80]. Further development of
(pGlu-Gln)-CCK-8 is hindered by renal filtration [81].
Recently, potential therapy of (pGlu-Gln)-CCK-8 is the
PEGylated form of (pGlu-Gln)-CCK-8. (pGlu-Gln)-CCK-
8[mPEG] provides antiobesity and antidiabetes effects with
prolonged half-life of CCK-8 [82]. Further studies of
(pGlu-Gln)-CCK-8[mPEG] in human are needed for the
future treatment for obesity and diabetes.
CCK levels are lower in women with PCOS [9, 83].
Obese PCOS patients with hyperandrogenism had lower
levels of CCK compared to obese PCOS women without
hyperandrogenism [83]. It suggests the postprandial CCK
is negatively correlated with the levels of free testosterone
[9]. So far, there are just a few studies about CCK levels in
PCOS. It needs further studies to clarify the mechanism
under the correlation between hyperandrogenism and
plasma CCK in PCOS patients.
PYY
PYY is co-located with GLP-1 in the L-cells of the distal
gut and is involved in the so-called ‘‘ileal brake’’ [84].
Plasma concentrations of PYY are low in the fasting state,
and increase about 30 min after exposure of the small
intestine to nutrients [85]. PYY is secreted in a load-
dependent fashion, with fat being the most potent stimulus,
followed by carbohydrate and then protein [86, 87]. The
secretion of PYY in response to small intestinal fat is
mediated partly by CCK [88]. Because of its capacity to
slow gastric emptying, PYY is also likely to improve
postprandial glycaemia, although there is no evidence for
an insulinotropic effect.
PYY circulates as two main forms, PYY3-36 and
PYY1-36, with the former being active in suppressing
appetite [89]. In addition to delaying gastric and gall-
bladder emptying, inhibiting gastric and pancreatic secre-
tion, and slowing colonic transit [90], peripheral adminis-
tration of PYY3-36 reduces food intake in rats, monkeys,
and humans [91–93]. In humans, both pharmacological and
‘‘physiological’’ intravenous PYY3-36 infusions elicit
fullness and suppression of food intake, the latter lasting
over 12 h, despite the plasma PYY concentration falling to
baseline [94]. In addition, there is a synergistic effect of
exogenous PYY3-36 with GLP-17-36 on reduction of
energy intake [93], whereas exogenous PYY reduces cir-
culating ghrelin concentrations [95]. It remains contentious
whether the suppressive effect of PYY3-36 on energy
intake in humans represents an aversive effect; there are no
specific antagonists of PYY which are available for use in
humans.
Injection of PYY3-36 into the ARC in rats decreases
NPY expression while stimulating expression of POMC,
which would account for reduced food intake [94]. The
putative pre-synaptic NPY Y2 receptor (Y2R) in the ARC
of the hypothalamus appears to mediate these effects [96].
Like GLP-1, plasma concentrations of PYY are slightly
lower in the fasting and postprandial states and hunger is
greater, in obese compared to lean individuals [97]. Low
PYY levels predict a trend to overweight, but in obese
children, PYY is normalized following weight loss [98].
However, the obese are as sensitive as lean subjects to
suppression of food intake by exogenous PYY3-36 [95].
Again, like GLP-1, obese patients have elevated PYY
levels after jejunoileal bypass surgery, which may con-
tribute to loss of appetite [99]. Thus, the analogs and
degradation inhibitor of PYY3–36 have the potential for
the treatment of obesity [100, 101].
There is no difference in fasting PYY between lean
patients with PCOS and controls [102]. However, fasting
and postprandial PYY levels are lower in obese patients
with PCOS [103]. It has been observed that there is an
inverse correlation between fasting levels of PYY and
HOMA-IR in women with PCOS. The impaired post-
prandial PYY levels may contribute to insulin resistance
[103]. Metformin treatment in PCOS increased PYY levels
which are parallel with improvement of insulin sensitivity
[102].
Weight management in the treatment of PCOS
Weight loss is primary therapy for overweight or obese
patients with PCOS. Even slight weight loss as 5 %
reduction significantly improves IR and ovulation
resumption [104]. Body weight loss increases the effi-
ciency of several infertility treatments in PCOS. Current
Endocrine
123

therapies for weight loss are all related to changes of gut
hormones.
Diet
Lifestyle adjustment (diet, exercise, and behavioral modi-
fication) is always the first-line treatment for overweight/
obese females with PCOS [105]. Both Low Glucose Index
(GI) diet and hypocarloric diet interventions have benefi-
cial effects for obese PCOS patients [106]. Low GI diet
improves irregular menstrual patterns compared with con-
ventional diet [107]. The effect of a hypocaloric diet on
insulin resistance was even better than metformin [108].
Compared to glucose ingestion, protein causes less glu-
cose/insulin fluctuation [109]. Whey protein supplement
profoundly slows gastric emptying of the carbohydrate and
stimulates the release of GLP-1 [110]. Fat restriction is
equally effective in weight loss and menstrual cycle
improvement as low carbohydrate diet. Fatty acids also
play a role in the treatment of metabolic disorder in PCOS.
It has been reported that diet supplied with LC n - 3
PUFA suppressed plasma bioavailable testosterone con-
centrations [111]. However, the dietary strategies alone
normally are not sufficient.
Acupuncture
Acupuncture is an important part of the traditional Chinese
treatment. Manual and electrical acupuncture activates the
afferent nerve fibers [112] to reduce abdominal visceral
adipose tissue and BMI in patients with PCOS [113]. After
a few weeks of treatment of acupuncture, the reduction of
body weight is related to decreased serum insulin and
leptin levels, and increased plasma PYY and CCK levels in
obese women [114, 115]. When the acupuncture is com-
bined with low-calorie diet, lipid profile is improved [116].
Acupuncture is an effective treatment for obesity with less
adverse effect [117].
Metformin
Metformin is widely used in treatment of T2DM, in par-
ticular, in overweight or obesity. The primary effect of
metformin is believed to suppress hepatic gluconeogenesis,
reduce glucose absorption, improve insulin sensitivity, and
increase peripheral glucose uptake. Since hyperinsulina-
emia plays an important role in the pathogenesis of PCOS,
metformin intervention is used to restore endocrine func-
tion in PCOS. It has been observed that combination of
metformin and lifestyle modification resulted in a signifi-
cantly weight loss compared to lifestyle modification alone
[118]. Clinical trials confirmed that metformin is effective
in the improvement of ovarian function and menstrual
cycle, and reduction of serum androgen levels in obese
patients with PCOS [119]. The weight reduction is related
to the increase in plasma PYY, ghrelin, and GLP-1 levels
[102, 120, 121]. Unfortunately, many of the above-dis-
cussed effects of metformin were not observed
consistently.
Berberine
Berberine (BBR), a type of isoquinoline derivative alka-
loid, is extracted from Chinese medical herbs. Normally, it
is used as an oral drug for the treatment of gastrointestinal
infections. Recent studies showed that 3 months of treat-
ment of BBR decreased WC, waist-hip ratio, TC, TG, and
LDL-C, increased HDL-C and SHBG, and improved
insulin resistance in women with PCOS [122]. Compared
to metformin, BBR brings more potential benefits to
patients with PCOS both in metabolic and endocrine
parameters [123]. The possible mechanisms of BBR
include upregulating hepatic low-density lipoprotein
receptor mRNA expression, activating AMP-activated
protein kinase in both adipose and muscle tissues, stimu-
lating glycolysis in peripheral tissue cells, promoting
secretion of insulin, inhibiting liver gluconeogenesis, and
promoting secretion of intestinal GLP-1 [124]. The effect
of BBR on antimicrobial activity may be involved in the
development of anti-obesity treatment [125]. The major
side effects of BBR include diarrhea, constipation, flatu-
lence, and abdominal pain.
GLP-1 agonists
GLP-1receptor agonists were used as a medication in the
treatment of diabetes. Recent studies provided data about
the safety and efficacy of GLP-1 receptor agonist on weight
loss in overweight and obese adults and adolescents [126–
128]. Peripheral GLP-1 administration is associated with
enhanced postmeal satiety and reduced food intake at the
subsequent meal [129]. A meta-analysis showed that
energy intake was reduced by 174 kcal or 11.7 % in
ad libitum following intravenous GLP-1 infusion [130].
Exenatide treatment for 3 months reduced BMI and
improved insulin resistance of adolescents with severe
obesity [131]. During the treatment, subjects experienced
more gastrointestinal adverse events such as nausea,
vomiting, and diarrhea after exenatide compared with
placebo. However, the symptoms decreased over time. It
appeared that gastrointestinal symptoms were not corre-
lated with weight loss reduction [132]. The overall patient
satisfaction with GLP-1R agonist treatment is fairly high
[133]. A further reduction in BMI was observed in longer-
term use of exenatide [134]. In patients with PCOS, exe-
natide was more effective than metformin in promoting
Endocrine
123

weight loss [135]. The combination of exenatide/liraglutide
and metformin was superior to exenatide/liraglutide or
metformin monotherapy in improving menstrual cyclicity,
ovulation rate, free androgen index, and insulin sensitivity
[135, 136].
Surgical therapy
Patients with PCOS require a combination therapy of life
modification and drug treatment. However, weight loss
with these approaches is often difficult to achieve for
patients. Bariatric surgery could be an alternative treatment
in metabolic dysfunction restoration and pregnancy out-
comes improvement [137]. For example, the mean weight
loss in 12 women with PCOS was 41 kg after bariatric
surgery (either biliopancreatic diversion or Laparoscopic
adjustable gastric banding) [138]. Following the weight
loss, various clinical problems such as dyslipidemia, fer-
tility, and/or hirsutism related to PCOS were significantly
improved [139]. The mechanism of weight loss induced by
bariatric surgery is not certain. One possible mechanism is
that the gastric volume is reduced [140, 141]. The other
mechanism is the changes of gastrointestinal hormones
[140]. In postoperative state, a quick delivery of nutrients
to the small intestine leads to an overstimulation or pro-
liferation of the endocrine cells, or reduced degradation of
the secreted hormones [142]. Therefore, the increased
postprandial PYY and GLP-1 response [141, 143, 144]
were observed. Plasma PYY and GLP-1 start increasing as
early as 2 days after surgery and before important weight
loss [144]. Recent study reported that weight loss after
Roux-en-Y gastric bypass (RYGB) surgery is also related
to reductions of brain activation in response to high caloric
foods [145].
Conclusion
PCOS is one of most common endocrine diseases in
women of reproductive age with clinical feature of poly-
cystic ovaries, hyperandrogen, and insulin resistance.
Woman with PCOS has a high prevalence of T2DM and
CVD. Most patients are overweight or obese. Therefore,
weight loss is important in the treatment of PCOS. Current
therapy for weight loss is less than ideal, and bariatric
surgery is invasive. Gastrointestinal hormones are crucial
in regulation of food intake and body weight. Dietary or
pharmacological strategies based on regulation of gastro-
intestinal hormones are likely to be of fundamental
importance in the management of obesity. Therapy aimed
at the gastrointestinal hormones will be the new direction
of treatment for PCOS.
Acknowledgments This work was supported by grant from the
Shanghai Jiaotong University, School of Medicine, Science and
Technology Fund (Grant No. 12XJ10015).
Disclosure There are no conflicts of interest to disclose.
References
1. E.S. Knochenhauer, T.J. Key, M. Kahsar-Miller, W. Waggoner,
L.R. Boots, R. Azziz, Prevalence of the polycystic ovary syn-
drome in unselected black and white women of the southeastern
United States: a prospective study. J. Clin. Endocrinol. Metab.
83, 3078–3082 (1998)
2. E. Diamanti-Kandarakis, C.R. Kouli, A.T. Bergiele, F.A. Fil-
andra, T.C. Tsianateli, G.G. Spina, E.D. Zapanti, M.I. Bartzis, A
survey of the polycystic ovary syndrome in the Greek island of
Lesbos: hormonal and metabolic profile. J. Clin. Endocrinol.
Metab. 84, 4006–4011 (1999)
3. W.A. March, V.M. Moore, K.J. Willson, D.I. Phillips, R.J.
Norman, M.J. Davies, The prevalence of polycystic ovary syn-
drome in a community sample assessed under contrasting
diagnostic criteria. Hum. Reprod. 25, 544–551 (2010)
4. H. Jia, L. Yu, X. Guo, W. Gao, Z. Jiang, Associations of
adiponectin gene polymorphisms with polycystic ovary syn-
drome: a meta-analysis. Endocrine 42, 299–306 (2012)
5. M. Brower, K. Brennan, M. Pall, R. Azziz, The severity of
menstrual dysfunction as a predictor of insulin resistance in
PCOS. J. Clin. Endocrinol. Metab. 98, E1967–E1971 (2013)
6. S.F. Witchel, S.E. Recabarren, F. Gonzalez, E. Diamanti-
Kandarakis, K.I. Cheang, A.J. Duleba, R.S. Legro, R. Homburg,
R. Pasquali, R.A. Lobo, C.C. Zouboulis, F. Kelestimur, F.
Fruzzetti, W. Futterweit, R.J. Norman, D.H. Abbott, Emerging
concepts about prenatal genesis, aberrant metabolism and
treatment paradigms in polycystic ovary syndrome. Endocrine
42, 526–534 (2012)
7. S.S. Lim, R.J. Norman, M.J. Davies, L.J. Moran, The effect of
obesity on polycystic ovary syndrome: a systematic review and
meta-analysis. Obes. Rev. 14, 95–109 (2013)
8. N. Kanaya, S. Vonderfecht, S. Chen, Androgen (dihydrotestos-
terone)-mediated regulation of food intake and obesity in female
mice. J.Steroid Biochem. Mol. Biol. 138, 100–106 (2013)
9. A.L. Hirschberg, S. Naessen, M. Stridsberg, B. Bystrom, J.
Holtet, Impaired cholecystokinin secretion and disturbed appe-
tite regulation in women with polycystic ovary syndrome.
Gynecol. Endocrinol. 19, 79–87 (2004)
10. D. Mahoney, Lifestyle modification intervention among infertile
overweight and obese women with polycystic ovary syndrome.
J. Am. Assoc. Nurse Pract. (2013). doi:10.1002/2327-6924.
12073
11. B.A. Gower, P.C. Chandler-Laney, F. Ovalle, L.L. Goree, R.
Azziz, R.A. Desmond, W.M. Granger, A.M. Goss, G.W. Bates,
Favourable metabolic effects of a eucaloric lower-carbohydrate
diet in women with PCOS. Clin. Endocrinol. 79, 550–557
(2013)
12. P.J. Havel, Peripheral signals conveying metabolic information
to the brain: short-term and long-term regulation of food intake
and energy homeostasis. Exp. Biol. Med. (Maywood) 226,
963–977 (2001)
13. R. Deniz, B. Gurates, S. Aydin, H. Celik, I. Sahin, Y. Baykus, Z.
Catak, A. Aksoy, C. Citil, S. Gungor, Nesfatin-1 and other
hormone alterations in polycystic ovary syndrome. Endocrine
42, 694–699 (2012)
14. S. Aydin, Multi-functional peptide hormone NUCB2/nesfatin-1.
Endocrine 44, 312–325 (2013)
Endocrine
123

15. M. Tschop, D.L. Smiley, M.L. Heiman, Ghrelin induces adi-
posity in rodents. Nature 407, 908–913 (2000)
16. G. Gomez, E.W. Englander, G.H. Greeley Jr, Nutrient inhibition
of ghrelin secretion in the fasted rat. Regul. Pept. 117, 33–36
(2004)
17. J. Overduin, R.S. Frayo, H.J. Grill, J.M. Kaplan, D.E. Cum-
mings, Role of the duodenum and macronutrient type in ghrelin
regulation. Endocrinology 146, 845–850 (2005)
18. B.A. Parker, S. Doran, J. Wishart, M. Horowitz, I.M. Chapman,
Effects of small intestinal and gastric glucose administration on
the suppression of plasma ghrelin concentrations in healthy
older men and women. Clin. Endocrinol. 62, 539–546 (2005)
19. W.A. Blom, A. Stafleu, C. de Graaf, F.J. Kok, G. Schaafsma,
H.F. Hendriks, Ghrelin response to carbohydrate-enriched
breakfast is related to insulin. Am. J. Clin. Nutr. 81, 367–375
(2005)
20. Y. Greenman, N. Golani, S. Gilad, M. Yaron, R. Limor, N.
Stern, Ghrelin secretion is modulated in a nutrient- and gender-
specific manner. Clin. Endocrinol. 60, 382–388 (2004)
21. A.M. Wren, L.J. Seal, M.A. Cohen, A.E. Brynes, G.S. Frost,
K.G. Murphy, W.S. Dhillo, M.A. Ghatei, S.R. Bloom, Ghrelin
enhances appetite and increases food intake in humans. J. Clin.
Endocrinol. Metab. 86, 5992 (2001)
22. D.E. Cummings, K. Clement, J.Q. Purnell, C. Vaisse, K.E.
Foster, R.S. Frayo, M.W. Schwartz, A. Basdevant, D.S. Weigle,
Elevated plasma ghrelin levels in Prader Willi syndrome. Nat.
Med. 8, 643–644 (2002)
23. D.E. Cummings, D.S. Weigle, R.S. Frayo, P.A. Breen, M.K. Ma,
E.P. Dellinger, J.Q. Purnell, Plasma ghrelin levels after diet-
induced weight loss or gastric bypass surgery. N. Engl. J. Med.
346, 1623–1630 (2002)
24. P.J. Currie, A. Mirza, R. Fuld, D. Park, J.R. Vasselli, Ghrelin is
an orexigenic and metabolic signaling peptide in the arcuate and
paraventricular nuclei. Am. J. Physiol. Regul. Integr. Comp.
Physiol. 289, R353–R358 (2005)
25. M. Nakazato, N. Murakami, Y. Date, M. Kojima, H. Matsuo, K.
Kangawa, S. Matsukura, A role for ghrelin in the central regu-
lation of feeding. Nature 409, 194–198 (2001)
26. M.A. Cowley, J.L. Smart, M. Rubinstein, M.G. Cerdan, S. Di-
ano, T.L. Horvath, R.D. Cone, M.J. Low, Leptin activates
anorexigenic POMC neurons through a neural network in the
arcuate nucleus. Nature 411, 480–484 (2001)
27. D.E. Cummings, K.E. Foster, Ghrelin-leptin tango in body-
weight regulation. Gastroenterology 124, 1532–1535 (2003)
28. A. Moulin, L. Brunel, D. Boeglin, L. Demange, J. Ryan, C.
M’Kadmi, S. Denoyelle, J. Martinez, J.A. Fehrentz, The 1,2,4-
triazole as a scaffold for the design of ghrelin receptor ligands:
development of JMV 2959, a potent antagonist. Amino Acids
44, 301–314 (2013)
29. G. Arusoglu, G. Koksal, N. Cinar, S. Tapan, D.Y. Aksoy, B.O.
Yildiz, Basal and meal-stimulated ghrelin, PYY, CCK levels
and satiety in lean women with polycystic ovary syndrome:
effect of low-dose oral contraceptive. J. Clin. Endocrinol.
Metab. 98, 4475–4482 (2013)
30. Japur, CC, Diez-Garcia, RW, de Oliveira Penaforte, FR, de Sa,
MF, Imbalance between postprandial ghrelin and insulin
responses to an ad libitum meal in obese women with polycystic
ovary syndrome. Reprod. Sci. (2014) [Epub ahead of print]
31. I.T. Ozgen, M. Aydin, A. Guven, Y. Aliyazicioglu, Character-
istics of polycystic ovarian syndrome and relationship with
ghrelin in adolescents. J. Pediatr. Adolesc. Gynecol. 23,
285–289 (2010)
32. T.M. Barber, F.F. Casanueva, F. Karpe, M. Lage, S. Franks, M.I.
McCarthy, J.A. Wass, Ghrelin levels are suppressed and show a
blunted response to oral glucose in women with polycystic ovary
syndrome. Eur. J. Endocrinol 158, 511–516 (2008)
33. M. Mitkov, B. Pehlivanov, Orbetzova, M:Serum ghrelin level in
women with polycystic ovary syndrome and its relationship with
endocrine and metabolic parameters. Gynecol. Endocrinol. 24,
625–630 (2008)
34. A. Bideci, M.O. Camurdan, E. Yesilkaya, F. Demirel, P. Cinaz,
Serum ghrelin, leptin and resistin levels in adolescent girls with
polycystic ovary syndrome. J. Obstet. Gynaecol. Res. 34,
578–584 (2008)
35. M.J. Theodorakis, O. Carlson, S. Michopoulos, M.E. Doyle, M.
Juhaszova, K. Petraki, J.M. Egan, Human duodenal enteroen-
docrine cells: source of both incretin peptides, GLP-1 and GIP.
Am. J. Physiol. Endocrinol. Metab. 290, E550–E559 (2006)
36. C.F. Deacon, What do we know about the secretion and degra-
dation of incretin hormones? Regul. Pept. 128, 117–124 (2005)
37. R. Mentlein, B. Gallwitz, W.E. Schmidt, Dipeptidyl-peptidase
IV hydrolyses gastric inhibitory polypeptide, glucagon-likepeptide-1(7–36)amide, peptide histidine methionine and is
responsible for their degradation in human serum. Eur. J. Bio-
chem. 214, 829–835 (1993)
38. R. Mentlein, Dipeptidyl-peptidase IV (CD26)–role in the inac-
tivation of regulatory peptides. Regul. Pept. 85, 9–24 (1999)
39. L. Hansen, C.F. Deacon, C. Orskov, J.J. Holst, Glucagon-like
peptide-1-(7–36)amide is transformed to glucagon-like peptide-
1-(9–36)amide by dipeptidyl peptidase IV in the capillaries
supplying the L cells of the porcine intestine. Endocrinology
140, 5356–5363 (1999)
40. L.A. Scrocchi, T.J. Brown, N. MaClusky, P.L. Brubaker, A.B.
Auerbach, A.L. Joyner, D.J. Drucker, Glucose intolerance but
normal satiety in mice with a null mutation in the glucagon-like
peptide 1 receptor gene. Nat. Med. 2, 1254–1258 (1996)
41. R. Perfetti, J. Zhou, M.E. Doyle, J.M. Egan, Glucagon-like
peptide-1 induces cell proliferation and pancreatic-duodenum
homeobox-1 expression and increases endocrine cell mass in the
pancreas of old, glucose-intolerant rats. Endocrinology 141,
4600–4605 (2000)
42. J. Schirra, M. Nicolaus, R. Roggel, M. Katschinski, M. Storr,
H.J. Woerle, B. Goke, Endogenous glucagon-like peptide 1
controls endocrine pancreatic secretion and antro-pyloro-duo-
denal motility in humans. Gut 55, 243–251 (2006)
43. J.J. Meier, B. Gallwitz, S. Salmen, O. Goetze, J.J. Holst, W.E.
Schmidt, M.A. Nauck, Normalization of glucose concentrations
and deceleration of gastric emptying after solid meals during
intravenous glucagon-like peptide 1 in patients with type 2
diabetes. J. Clin. Endocrinol. Metab. 88, 2719–2725 (2003)
44. M.A. Nauck, U. Niedereichholz, R. Ettler, J.J. Holst, C. Orskov,
R. Ritzel, W.H. Schmiegel, Glucagon-like peptide 1 inhibition
of gastric emptying outweighs its insulinotropic effects in
healthy humans. Am. J. Physiol. 273, E981–E988 (1997)
45. J.J. Hwa, L. Ghibaudi, P. Williams, M.B. Witten, R. Tedesco,
C.D. Strader, Differential effects of intracerebroventricular
glucagon-like peptide-1 on feeding and energy expenditure
regulation. Peptides 19, 869–875 (1998)
46. F. Rodriquez de Fonseca, M. Navarro, E. Alvarez, I. Roncero,
J.A. Chowen, O. Maestre, R. Gomez, R.M. Munoz, J. Eng, E.
Blazquez, Peripheral versus central effects of glucagon-like
peptide-1 receptor agonists on satiety and body weight loss in
Zucker obese rats. Metabolism 49, 709–717 (2000)
47. J.J. Meier, M.A. Nauck, Glucagon-like peptide 1(GLP-1) in biol-
ogy and pathology. Diabetes Metab. Res. Rev. 21, 91–117 (2005)
48. E. Naslund, M. Gutniak, S. Skogar, S. Rossner, P.M. Hellstrom,
Glucagon-like peptide 1 increases the period of postprandial
satiety and slows gastric emptying in obese men. Am. J. Clin.
Nutr. 68, 525–530 (1998)
49. M.A. Nauck, J.J. Meier, Glucagon-like peptide 1 and its deriv-
atives in the treatment of diabetes. Regul. Pept. 128, 135–148
(2005)
Endocrine
123

50. M. Nauck, F. Stockmann, R. Ebert, W. Creutzfeldt, Reduced
incretin effect in type 2 (non-insulin-dependent) diabetes. Dia-
betologia 29, 46–52 (1986)
51. J. Ma, A.N. Pilichiewicz, C. Feinle-Bisset, J.M. Wishart, K.L.
Jones, M. Horowitz, C.K. Rayner, Effects of variations in duo-
denal glucose load on glycaemic, insulin, and incretin responses
in type 2 diabetes. Diabet. Med. 29, 604–608 (2012)
52. L.R. Ranganath, J.M. Beety, L.M. Morgan, J.W. Wright, R.
Howland, V. Marks, Attenuated GLP-1 secretion in obesity:
cause or consequence? Gut 38, 916–919 (1996)
53. S. Madsbad, The role of glucagon-like peptide-1 impairment in
obesity and potential therapeutic implications. Diabet. Obes.
Metab. 16, 9–21 (2014)
54. F.K. Knop, K. Aaboe, T. Vilsboll, A. Volund, J.J. Holst, T.
Krarup, S. Madsbad, Impaired incretin effect and fasting hy-
perglucagonaemia characterizing type 2 diabetic subjects are
early signs of dysmetabolism in obesity. Diabet. Obes. Metab.
14, 500–510 (2012)
55. T. Vilsboll, T. Krarup, J. Sonne, S. Madsbad, A. Volund, A.G.
Juul, J.J. Holst, Incretin secretion in relation to meal size and
body weight in healthy subjects and people with type 1 and type
2 diabetes mellitus. J. Clin. Endocrinol. Metab. 88, 2706–2713
(2003)
56. C. Verdich, S. Toubro, B. Buemann, L. Madsen, J. Juul, J. Holst, A.
Astrup, The role of postprandial releases of insulin and incretin
hormones in meal-induced satiety–effect of obesity and weight
reduction. Int. J. Obes. Relat. Metab. Disord. 25, 1206–1214 (2001)
57. Y. Anini, P.L. Brubaker, Role of leptin in the regulation of
glucagon-like peptide-1 secretion. Diabetes 52, 252–259 (2003)
58. J.G. Barrera, D.A. Sandoval, D.A. D’Alessio, R.J. Seeley, GLP-
1 and energy balance: an integrated model of short-term and
long-term control. Nat. Rev. Endocrinol. 7, 507–516 (2011)
59. R. Gama, F. Norris, J. Wright, L. Morgan, S. Hampton, S.
Watkins, V. Marks, The entero-insular axis in polycystic ovarian
syndrome. Ann. Clin. Biochem. 33(Pt 3), 190–195 (1996)
60. C. Pontikis, M.P. Yavropoulou, K.A. Toulis, K. Kotsa, K.
Kazakos, A. Papazisi, A. Gotzamani-Psarakou, J.G. Yovos, The
incretin effect and secretion in obese and lean women with
polycystic ovary syndrome: a pilot study. J. Women’s Health 20,
971–976 (2011)
61. J. Vrbikova, M. Hill, B. Bendlova, T. Grimmichova, K. Dvo-
rakova, K. Vondra, G. Pacini, Incretin levels in polycystic ovary
syndrome. Eur. J. Endocrinol. 159, 121–127 (2008)
62. J.F. Rehfeld, G. Sun, T. Christensen, J.G. Hillingso, The pre-
dominant cholecystokinin in human plasma and intestine is
cholecystokinin-33. J. Clin. Endocrinol. Metab. 86, 251–258
(2001)
63. R.A. Liddle, I.D. Goldfine, M.S. Rosen, R.A. Taplitz, J.A.
Williams, Cholecystokinin bioactivity in human plasma.
Molecular forms, responses to feeding, and relationship to
gallbladder contraction. J. Clin. Invest. 75, 1144–1152 (1985)
64. T.H. Moran, K.P. Kinzig, Gastrointestinal satiety signals II.
Cholecystokinin. Am. J. Physiol. Gastrointest. Liver Physiol.
286, G183–G188 (2004)
65. R.A. Liddle, Regulation of cholecystokinin secretion in humans.
J. Gastroenterol. 35, 181–187 (2000)
66. C. Feinle, M. D’Amato, N.W. Read, Cholecystokinin-A recep-
tors modulate gastric sensory and motor responses to gastric
distension and duodenal lipid. Gastroenterology 110, 1379–1385
(1996)
67. W. Schwizer, J. Borovicka, P. Kunz, R. Fraser, C. Kreiss, M.
D’Amato, G. Crelier, P. Boesiger, M. Fried, Role of cholecys-
tokinin in the regulation of liquid gastric emptying and gastric
motility in humans: studies with the CCK antagonist loxiglu-
mide. Gut 41, 500–504 (1997)
68. C.K. Rayner, H.S. Park, S.M. Doran, I.M. Chapman, M. Horo-
witz, Effects of cholecystokinin on appetite and pyloric motility
during physiological hyperglycemia. Am. J. Physiol. Gastroin-
test. Liver Physiol. 278, G98–G104 (2000)
69. J. Glatzle, Y. Wang, D.W. Adelson, T.J. Kalogeris, T.T. Zittel,
P. Tso, J.Y. Wei, H.E. Raybould, Chylomicron components
activate duodenal vagal afferents via a cholecystokinin A
receptor-mediated pathway to inhibit gastric motor function in
the rat. J. Physiol. 550, 657–664 (2003)
70. J.G. Gutierrez, W.Y. Chey, V.P. Dinoso, Actions of cholecys-
tokinin and secretin on the motor activity of the small intestine
in man. Gastroenterology 67, 35–41 (1974)
71. J. Gibbs, R.C. Young, G.P. Smith, Cholecystokinin elicits sati-
ety in rats with open gastric fistulas. Nature 245, 323–325 (1973)
72. T.H. Moran, P.J. Ameglio, G.J. Schwartz, P.R. McHugh,
Blockade of type A, not type B, CCK receptors attenuates
satiety actions of exogenous and endogenous CCK. Am.
J. Physiol. 262, R46–R50 (1992)
73. T.H. Moran, S. Bi, Hyperphagia and obesity in OLETF rats
lacking CCK-1 receptors. Philos. Trans. R. Soc. Lond. B Biol.
Sci. 361, 1211–1218 (2006)
74. K. Meereis-Schwanke, H. Klonowski-Stumpe, L. Herberg, C.
Niederau, Long-term effects of CCK-agonist and -antagonist on
food intake and body weight in Zucker lean and obese rats.
Peptides 19, 291–299 (1998)
75. L. Wang, M.D. Barachina, V. Martinez, J.Y. Wei, Y. Tache,
Synergistic interaction between CCK and leptin to regulate food
intake. Regul. Pept. 92, 79–85 (2000)
76. I.M. Brennan, T.J. Little, K.L. Feltrin, A.J. Smout, J.M. Wishart,
M. Horowitz, C. Feinle-Bisset, Dose-dependent effects of cho-
lecystokinin-8 on antropyloroduodenal motility, gastrointestinal
hormones, appetite, and energy intake in healthy men. Am.
J. Physiol. Endocrinol. Metab. 295, E1487–E1494 (2008)
77. C. Beglinger, L. Degen, D. Matzinger, M. D’Amato, J. Drewe,
Loxiglumide, a CCK-A receptor antagonist, stimulates calorie
intake and hunger feelings in humans. Am. J. Physiol. Regul.
Integr. Comp. Physiol. 280, R1149–R1154 (2001)
78. F.P. O’Harte, M.H. Mooney, C.M. Kelly, P.R. Flatt, Glycated
cholecystokinin-8 has an enhanced satiating activity and is
protected against enzymatic degradation. Diabetes 47,
1619–1624 (1998)
79. I.A. Montgomery, N. Irwin, P.R. Flatt, Beneficial effects of
(pGlu-Gln)-CCK-8 on energy intake and metabolism in high fat
fed mice are associated with alterations of hypothalamic gene
expression. Hormon. Metab. Res. 45(6), 471–473 (2013)
80. N. Irwin, I.A. Montgomery, R.C. Moffett, P.R. Flatt, Chemical
cholecystokinin receptor activation protects against obesity-
diabetes in high fat fed mice and has sustainable beneficial
effects in genetic ob/ob mice. Biochem. Pharmacol. 85, 81–91
(2013)
81. N. Irwin, P.R. Flatt, Enteroendocrine hormone mimetics for the
treatment of obesity and diabetes. Curr. Opin. Pharmacol. 13,
989–995 (2013)
82. N. Irwin, P. Frizelle, F.P. O’Harte, P.R. Flatt, (pGlu-Gln)-CCK-
8[mPEG]: a novel, long-acting, mini-PEGylated cholecystokinin
(CCK) agonist that improves metabolic status in dietary-induced
diabetes. Biochim. et Biophys. Acta 1830, 4009–4016 (2013)
83. B. Bidzinska-Speichert, A. Lenarcik, U. Tworowska-Bard-
zinska, R. Slezak, G. Bednarek-Tupikowska, A. Milewicz,
Pro12Ala PPAR gamma2 gene polymorphism in PCOS women:
the role of compounds regulating satiety. Gynecol. Endocrinol.
28, 195–198 (2012)
84. J. Wen, S.F. Phillips, M.G. Sarr, L.J. Kost, Holst, JJ:PYY and
GLP-1 contribute to feedback inhibition from the canine ileum
and colon. Am. J. Physiol. 269, G945–G952 (1995)
Endocrine
123

85. R.P. Vincent, C.W. le Roux, The satiety hormone peptide YY as
a regulator of appetite. J. Clin. Pathol. 61, 548–552 (2008)
86. M.S. Huda, J.P. Wilding, J.H. Pinkney, Gut peptides and the
regulation of appetite. Obes. Rev. 7, 163–182 (2006)
87. L. Degen, S. Oesch, M. Casanova, S. Graf, S. Ketterer, J. Drewe,
C. Beglinger, Effect of peptide YY3-36 on food intake in
humans. Gastroenterology 129, 1430–1436 (2005)
88. H.C. Lin, W.Y. Chey, X. Zhao, Release of distal gut peptide YY
(PYY) by fat in proximal gut depends on CCK. Peptides 21,
1561–1563 (2000)
89. G.A. Eberlein, V.E. Eysselein, M. Schaeffer, P. Layer, D.
Grandt, H. Goebell, W. Niebel, M. Davis, T.D. Lee, J.E. Shively
et al., A new molecular form of PYY: structural characterization
of human PYY(3–36) and PYY(1–36). Peptides 10, 797–803
(1989)
90. R.L. Conter, J.J. Roslyn, I.L. Taylor, Effects of peptide YY on
gallbladder motility. Am. J. Physiol. 252, G736–G741 (1987)
91. N. Vrang, A.N. Madsen, M. Tang-Christensen, G. Hansen, P.J.
Larsen, PYY(3–36) reduces food intake and body weight and
improves insulin sensitivity in rodent models of diet-induced
obesity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 291,
R367–R375 (2006)
92. T.H. Moran, U. Smedh, K.P. Kinzig, K.A. Scott, S. Knipp, E.E.
Ladenheim, Peptide YY(3–36) inhibits gastric emptying and
produces acute reductions in food intake in rhesus monkeys.
Am. J. Physiol. Regul. Integr. Comp. Physiol. 288, R384–R388
(2005)
93. N.M. Neary, C.J. Small, M.R. Druce, A.J. Park, S.M. Ellis, N.M.
Semjonous, C.L. Dakin, K. Filipsson, F. Wang, A.S. Kent, G.S.
Frost, M.A. Ghatei, S.R. Bloom, Peptide YY3-36 and glucagon-
like peptide-17–36 inhibit food intake additively. Endocrinology
146, 5120–5127 (2005)
94. R.L. Batterham, M.A. Cowley, C.J. Small, H. Herzog, M.A.
Cohen, C.L. Dakin, A.M. Wren, A.E. Brynes, M.J. Low, M.A.
Ghatei, R.D. Cone, S.R. Bloom, Gut hormone PYY(3-36)
physiologically inhibits food intake. Nature 418, 650–654
(2002)
95. R.L. Batterham, M.A. Cohen, S.M. Ellis, C.W. Le Roux, D.J.
Withers, G.S. Frost, M.A. Ghatei, S.R. Bloom, Inhibition of
food intake in obese subjects by peptide YY3-36. N. Engl.
J. Med. 349, 941–948 (2003)
96. C.R. Abbott, C.J. Small, A.R. Kennedy, N.M. Neary, A. Sajedi,
M.A. Ghatei, S.R. Bloom, Blockade of the neuropeptide Y Y2
receptor with the specific antagonist BIIE0246 attenuates the
effect of endogenous and exogenous peptide YY(3–36) on food
intake. Brain Res. 1043, 139–144 (2005)
97. C.W. le Roux, R.L. Batterham, S.J. Aylwin, M. Patterson, C.M.
Borg, K.J. Wynne, A. Kent, R.P. Vincent, J. Gardiner, M.A.
Ghatei, S.R. Bloom, Attenuated peptide YY release in obese
subjects is associated with reduced satiety. Endocrinology 147,
3–8 (2006)
98. C.L. Roth, P.J. Enriori, K. Harz, J. Woelfle, M.A. Cowley, T.
Reinehr, Peptide YY is a regulator of energy homeostasis in
obese children before and after weight loss. J. Clin. Endocrinol.
Metab. 90, 6386–6391 (2005)
99. E. Naslund, P. Gryback, P.M. Hellstrom, H. Jacobsson, J.J.
Holst, E. Theodorsson, L. Backman, Gastrointestinal hormones
and gastric emptying 20 years after jejunoileal bypass for
massive obesity. Int. J. Obes. Relat. Metab. Disord. 21, 387–392
(1997)
100. S.L. Pedersen, P.G. Sasikumar, S. Chelur, B. Holst, A. Artmann,
K.J. Jensen, N. Vrang, Peptide hormone isoforms: N-terminally
branched PYY3–36 isoforms give improved lipid and fat-cell
metabolism in diet-induced obese mice. J. Pept. Sci. 16,
664–673 (2010)
101. M.L. Addison, J.S. Minnion, J.C. Shillito, K. Suzuki, T.M. Tan,
B.C. Field, N. Germain-Zito, C. Becker-Pauly, M.A. Ghatei,
S.R. Bloom, K.G. Murphy, A role for metalloendopeptidases in
the breakdown of the gut hormone, PYY 3–36. Endocrinology
152, 4630–4640 (2011)
102. T. Tsilchorozidou, R.L. Batterham, G.S. Conway, Metformin
increases fasting plasma peptide tyrosine tyrosine (PYY) in
women with polycystic ovarian syndrome (PCOS). Clin.
Endocrinol. 69, 936–942 (2008)
103. K. Zwirska-Korczala, K. Sodowski, S.J. Konturek, D. Kuka, M.
Kukla, T. Brzozowski, W. Cnota, E. Wozniak-Grygiel, J. Ja-
worek, R. Buldak, B. Rybus-Kalinowska, M. Fryczowski,
Postprandial response of ghrelin and PYY and indices of low-
grade chronic inflammation in lean young women with poly-
cystic ovary syndrome. J. Physiol. Pharmacol. 59(Suppl 2),
161–178 (2008)
104. H. Lee, J.Y. Oh, Y.A. Sung, H. Chung, Is insulin resistance an
intrinsic defect in asian polycystic ovary syndrome? Yonsei
Med. J. 54, 609–614 (2013)
105. D. Panidis, K. Tziomalos, E. Papadakis, C. Vosnakis, P. Chatzis,
I. Katsikis, Lifestyle intervention and anti-obesity therapies in
the polycystic ovary syndrome: impact on metabolism and fer-
tility. Endocrine 44, 583–590 (2013)
106. R.L. Thomson, J.D. Buckley, M. Noakes, P.M. Clifton, R.J.
Norman, G.D. Brinkworth, The effect of a hypocaloric diet with
and without exercise training on body composition, cardiomet-
abolic risk profile, and reproductive function in overweight and
obese women with polycystic ovary syndrome. J. Clin. Endo-
crinol. Metab. 93, 3373–3380 (2008)
107. K.A. Marsh, K.S. Steinbeck, F.S. Atkinson, P. Petocz, J.C.
Brand-Miller, Effect of a low glycemic index compared with a
conventional healthy diet on polycystic ovary syndrome. Am.
Erican J. Clin. Nutr. 92, 83–92 (2010)
108. F. Esfahanian, M.M. Zamani, R. Heshmat, F. Moini nia, Effect
of metformin compared with hypocaloric diet on serum
C-reactive protein level and insulin resistance in obese and
overweight women with polycystic ovary syndrome. J. Obstet.
Gynaecol. Res. 39, 806–813 (2013)
109. S.E. Kasim-Karakas, W.M. Cunningham, A. Tsodikov, Relation
of nutrients and hormones in polycystic ovary syndrome. Am.
J. Clin. Nutr. 85, 688–694 (2007)
110. A. Karamanlis, R. Chaikomin, S. Doran, M. Bellon, F.D. Bar-
tholomeusz, J.M. Wishart, K.L. Jones, M. Horowitz, C.K.
Rayner, Effects of protein on glycemic and incretin responses
and gastric emptying after oral glucose in healthy subjects. Am.
J. Clin. Nutr. 86, 1364–1368 (2007)
111. N. Phelan, A. O’Connor, T. Kyaw Tun, N. Correia, G. Boran,
H.M. Roche, J. Gibney, Hormonal and metabolic effects of
polyunsaturated fatty acids in young women with polycystic
ovary syndrome: results from a cross-sectional analysis and a
randomized, placebo-controlled, crossover trial. Am. J. Clin.
Nutr. 93, 652–662 (2011)
112. Y.H. Zheng, X.H. Wang, M.H. Lai, H. Yao, H. Liu, H.X. Ma,
Effectiveness of abdominal acupuncture for patients with
obesity-type polycystic ovary syndrome: a randomized con-
trolled trial. J. Altern. Complement. Med. 19, 740–745 (2013)
113. H. Zhang, Y. Peng, Z. Liu, S. Li, Z. Lv, L. Tian, J. Zhu, X. Zhao,
M. Chen, Effects of acupuncture therapy on abdominal fat and
hepatic fat content in obese children: a magnetic resonance
imaging and proton magnetic resonance spectroscopy study.
J. Altern. Complement. Med. 17, 413–420 (2011)
114. B. Xu, J.H. Yuan, Z.C. Liu, M. Chen, X.J. Wang, Effect of
acupuncture on plasma peptide YY in the patient of simple
obesity. Zhongguo zhen jiu (Chin. Acupunct. Moxib.) 25,
837–840 (2005)
Endocrine
123

115. F. Gucel, B. Bahar, C. Demirtas, S. Mit, C. Cevik, Influence of
acupuncture on leptin, ghrelin, insulin and cholecystokinin in
obese women: a randomised, sham-controlled preliminary trial.
Acupunct. Med. 30, 203–207 (2012)
116. H. Abdi, B. Zhao, M. Darbandi, M. Ghayour-Mobarhan, S.
Tavallaie, A.A. Rahsepar, S.M. Parizadeh, M. Safariyan, M.
Nemati, M. Mohammadi, P. Abbasi-Parizad, S. Darbandi, S.
Akhlaghi, G.A. Ferns, The effects of body acupuncture on
obesity: anthropometric parameters, lipid profile, and inflam-
matory and immunologic markers. Sci.World. J. 2012, 603539
(2012)
117. S.H. Cho, J.S. Lee, L. Thabane, J. Lee, Acupuncture for obesity:
a systematic review and meta-analysis. Int. J. Obes. 33, 183–196
(2009)
118. K.M. Hoeger, L. Kochman, N. Wixom, K. Craig, R.K. Miller,
D.S. Guzick, A randomized, 48-week, placebo-controlled trial
of intensive lifestyle modification and/or metformin therapy in
overweight women with polycystic ovary syndrome: a pilot
study. Fertil. Steril. 82, 421–429 (2004)
119. J. Xiao, S. Chen, C. Zhang, S. Chang, The effectiveness of
metformin ovulation induction treatment in patients with PCOS:
a systematic review and meta-analysis. Gynecol. Endocrinol. 28,
956–960 (2012)
120. M. Shaker, Z.I. Mashhadani, A.A. Mehdi, Effect of Treatment
with Metformin on Omentin-1, Ghrelin and other Biochemical,
Clinical Features in PCOS Patients. Oman Med. J. 25, 289–293
(2010)
121. P.F. Svendsen, L. Nilas, S. Madsbad, J.J. Holst, Incretin hor-
mone secretion in women with polycystic ovary syndrome: roles
of obesity, insulin sensitivity, and treatment with metformin.
Metabolism 58, 586–593 (2009)
122. W. Wei, H. Zhao, A. Wang, M. Sui, K. Liang, H. Deng, Y. Ma,
Y. Zhang, H. Zhang, Y. Guan, A clinical study on the short-term
effect of berberine in comparison to metformin on the metabolic
characteristics of women with polycystic ovary syndrome. Eur.
J. Endocrinol. 166, 99–105 (2012)
123. Y. An, Z. Sun, Y. Zhang, B. Liu, Y. Guan, M. Lu, The use of
berberine for women with polycystic ovary syndrome under-
going IVF treatment. Clin. Endocrinol. 80, 425–431 (2014)
124. X. Zhang, Y. Zhao, M. Zhang, X. Pang, J. Xu, C. Kang, M. Li,
C. Zhang, Z. Zhang, Y. Zhang, X. Li, G. Ning, L. Zhao,
Structural changes of gut microbiota during berberine-mediated
prevention of obesity and insulin resistance in high-fat diet-fed
rats. PloS One 7, e42529 (2012)
125. W. Xie, D. Gu, J. Li, K. Cui, Y. Zhang, Effects and action
mechanisms of berberine and Rhizoma coptidis on gut microbes
and obesity in high-fat diet-fed C57BL/6 J mice. PloS One 6,
e24520 (2011)
126. T. Vilsboll, M. Christensen, A.E. Junker, F.K. Knop, L.L.
Gluud, Effects of glucagon-like peptide-1 receptor agonists on
weight loss: systematic review and meta-analyses of randomised
controlled trials. Br. Med. J. 344, d7771 (2012)
127. M. Monami, I. Dicembrini, N. Marchionni, C.M. Rotella, E.
Mannucci, Effects of glucagon-like peptide-1 receptor agonists
on body weight: a meta-analysis. Exp. Diabetes Res. 2012,
672658 (2012)
128. A.S. Kelly, K.D. Rudser, B.M. Nathan, C.K. Fox, A.M. Metzig,
B.J. Coombes, A.K. Fitch, E.M. Bomberg, M.J. Abuzzahab, The
effect of glucagon-like peptide-1 receptor agonist therapy on
body mass index in adolescents with severe obesity: a ran-
domized, placebo-controlled, clinical trial. J. Am. Med. Assoc.
Pediatr. 167, 355–360 (2013)
129. Gallwitz, B, Extra-pancreatic effects of incretin-based therapies.
Endocrine. (2014) [Epub ahead of print]
130. C. Verdich, A. Flint, J.P. Gutzwiller, E. Naslund, C. Beglinger,
P.M. Hellstrom, S.J. Long, L.M. Morgan, J.J. Holst, A. Astrup,
A meta-analysis of the effect of glucagon-like peptide-1 (7–36)
amide on ad libitum energy intake in humans. J. Clin. Endo-
crinol. Metab. 86, 4382–4389 (2001)
131. A.S. Kelly, A.M. Metzig, K.D. Rudser, A.K. Fitch, C.K. Fox,
B.M. Nathan, M.M. Deering, B.L. Schwartz, M.J. Abuzzahab,
L.M. Gandrud, A. Moran, C.J. Billington, Schwarzenberg,
SJ:Exenatide as a weight-loss therapy in extreme pediatric
obesity: a randomized, controlled pilot study. Obesity 20,
364–370 (2012)
132. R.A. DeFronzo, R.E. Ratner, J. Han, D.D. Kim, M.S. Fineman,
A.D. Baron, Effects of exenatide (exendin-4) on glycemic
control and weight over 30 weeks in metformin-treated patients
with type 2 diabetes. Diabetes Care 28, 1092–1100 (2005)
133. M. Davies, R. Pratley, M. Hammer, A.B. Thomsen, R. Cuddihy,
Liraglutide improves treatment satisfaction in people with Type
2 diabetes compared with sitagliptin, each as an add on to
metformin. Diabet. Med. 28, 333–337 (2011)
134. J. Rosenstock, L.J. Klaff, S. Schwartz, J. Northrup, J.H. Hol-
combe, K. Wilhelm, M. Trautmann, Effects of exenatide and
lifestyle modification on body weight and glucose tolerance in
obese subjects with and without pre-diabetes. Diabetes Care 33,
1173–1175 (2010)
135. K. Elkind-Hirsch, O. Marrioneaux, M. Bhushan, D. Vernor, R.
Bhushan, Comparison of single and combined treatment with
exenatide and metformin on menstrual cyclicity in overweight
women with polycystic ovary syndrome. J. Clin. Endocrinol.
Metab. 93, 2670–2678 (2008)
136. S.M. Jensterle, T. Kocjan, M. Pfeifer, N.A. Kravos, A. Janez,
Short-term combined treatment with liraglutide and metformin
leads to significant weight loss in obese women with polycystic
ovary syndrome and previous poor response to metformin. Eur.
J. Endocrinol. 170, 451–459 (2014)
137. H.F. Escobar-Morreale, Surgical management of metabolic
dysfunction in PCOS. Steroids 77, 312–316 (2012)
138. H.F. Escobar-Morreale, J.I. Botella-Carretero, F. Alvarez-Blas-
co, J. Sancho, J.L. San Millan, The polycystic ovary syndrome
associated with morbid obesity may resolve after weight loss
induced by bariatric surgery. J. Clin. Endocrinol. Metab. 90,
6364–6369 (2005)
139. G.M. Eid, D.R. Cottam, L.M. Velcu, S.G. Mattar, M.T. Koryt-
kowski, G. Gosman, P. Hindi, P.R. Schauer, Effective treatment
of polycystic ovarian syndrome with Roux-en-Y gastric bypass.
Surg. Obes. Relat. Dis. 1, 77–80 (2005)
140. R. Morinigo, V. Moize, M. Musri, A.M. Lacy, S. Navarro, J.L.
Marin, S. Delgado, R. Casamitjana, J. Vidal, Glucagon-like
peptide-1, peptide YY, hunger, and satiety after gastric bypass
surgery in morbidly obese subjects. J. Clin. Endocrinol. Metab.
91, 1735–1740 (2006)
141. S. Evans, Z. Pamuklar, J. Rosko, P. Mahaney, N. Jiang, C. Park,
A. Torquati, Gastric bypass surgery restores meal stimulation of
the anorexigenic gut hormones glucagon-like peptide-1 and
peptide YY independently of caloric restriction. Surg. Endosc.
26, 1086–1094 (2012)
142. M.B. Mumphrey, L.M. Patterson, H. Zheng, H.R. Berthoud,
Roux-en-Y gastric bypass surgery increases number but not
density of CCK-, GLP-1-, 5-HT-, and neurotensin-expressing
enteroendocrine cells in rats. Neurogastroenterol. Motil. 25,
e70–e79 (2013)
143. J. Korner, M. Bessler, L.J. Cirilo, I.M. Conwell, A. Daud, N.L.
Restuccia, S.L. Wardlaw, Effects of Roux-en-Y gastric bypass
surgery on fasting and postprandial concentrations of plasma
ghrelin, peptide YY, and insulin. J. Clin. Endocrinol. Metab. 90,
359–365 (2005)
144. C.W. le Roux, R. Welbourn, M. Werling, A. Osborne, A.
Kokkinos, A. Laurenius, H. Lonroth, L. Fandriks, M.A. Ghatei,
S.R. Bloom, T. Olbers, Gut hormones as mediators of appetite
Endocrine
123

and weight loss after Roux-en-Y gastric bypass. Ann. Surg. 246,
780–785 (2007)
145. C.N. Ochner, E. Stice, E. Hutchins, L. Afifi, A. Geliebter, J.
Hirsch, J. Teixeira, Relation between changes in neural
responsivity and reductions in desire to eat high-calorie foods
following gastric bypass surgery. Neuroscience 209, 128–135
(2012)
Endocrine
123