Embed Size (px)
Citation preview

Gut, 1976, 17, 719-728
Gastritis duodenitis, and circulating levels of gastrinin duodenal ulcer before and after vagotomyD. D. MEIKLE, K. B. TAYLOR, S. C. TRUELOVE, AND R. WHITEHEAD
From the Nuffield Department of Surgery, the Nuffield Department of Clinical Medicine, and theDepartment ofMorbid Anatomy, Radcliffe Infirmary, Oxford, and the Gastroenterology Division,Department of Medicine, Stanford University Medical Center, California, USA
SUMMARY Biopsy specimens have been taken from five standard sites in the stomach and from theduodenal bulb in order to investigate the association of gastritis and duodenitis with duodenal ulcer.Twenty patients with chronic duodenal ulcer were investigated in this manner and in addition hadgastric secretion tests and a radio-immune assay of serum gastrin under differing conditions. Thepatients were then treated either by a truncal vagotomy and pyloroplasty (TVP) or by a highly selec-tive vagotomy without a drainage procedure (HSV). All the investigations were repeated threemonths postoperatively. Duodenal ulcer was usually associated with gastritis, although this varied inextent and severity from patient to patient. In nearly all the patients, gastritis was present at thepyloric end of the stomach and along the lesser curve. In more than half of the patients, gastritis wasalso present in the body of the stomach but the fundus was usually spared. Chronic duodenitis was
found in the duodenal bulb in all these patients. After vagotomy there was a marked increase in boththe extent and severity of the proximal gastritis in both treatment groups but the distal gastritis re-
main almost unchanged. There was little change in the incidence of duodenitis after vagotomy butits severity was lessened. No correlation was found between the peak acid output (PAO) in responseto Histalogandthe severity ofthe gastritis or the duodenitis either before or after operation, with oneexception. The postoperative PAO was significantly less in those patients who developed a severeproximal gastritis after vagotomy. No relationship was found between the severity of the distalgastritis and the levels of serum gastrin. No correlation was found between either the basal or peakacid output and the corresponding serum gastrin levels before or after vagotomy.
The gastritis and duodenitis associated with a chronicpeptic ulcer have received comparatively little studyby the modem method of obtaining multiple biopsyspecimens under vision through a fibreoptic endo-scope. Our principal object in the present study wasto determine the extent and severity of any gastritisor duodenitis in a group of patients with chronicduodenal ulcer who had already been selected forsurgical treatment and to determine the effects oftwo types ofvagotomy on the mucosa of the stomachand duodenal bulb. In addition, we set out to deter-mine the levels of circulating gastrin in these patientsin response to various stimuli, both before and afteroperation, and to relate these levels to gastric acidoutput and to the histological state of the mucosa.
Received for publication 11 June 1976
Methods
PATIENTSTwenty patients attending the Radcliffe Infirmarywith chronic duodenal ulcer who had already beenselected for surgical treatment were studied shortlybefore operation and three months postoperatively.Ten of the patients were treated by bilateral truncalvagotomy combined with a Heinicke-Miculiczpyloroplasty (TVP) and the other 10 by a highlyselective vagotomy without a gastric drainage pro-cedure (HSV). These two operations were performedat random and the two treatment groups proved tobe well matched in terms of age, sex, and length ofulcer history. The majority of the operations wereperformed by one of us (D.D.M.) and the remainderbytwo consultant surgeons attheRadcliffe Infirmary.
719
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

D. D. Meikle, K. B. Taylor, S. C. Truelove, and R. Whitehead
BIOPSY OF MUCOSA OF STOMACH ANDDUODENAL BULBEndoscopy was usually performed with an OlympusGIF-D, a forward-viewing instrument through whichgood-sized biopsy specimens can be obtained. Afew examinations were made with an Olympus JFB,a sideways viewing instrument which is highly flexiblebut suffers from the disadvantage that the biopsyspecimens tend to be smaller.
Biopsy specimens were obtained from fivestandard sites within the stomach and also from theduodenal bulb at least 1 cm distant from the ulcer(Fig. 1). The specimens were floated off the biopsyforceps into physiological saline and were then im-mediately transferred to formol saline for fixation.The histological preparation of the specimens wasperformed by one technician who is solely engagedin dealing with biopsy specimens from the gastro-intestinal tract. Multiple specimens were cut fromeach biopsy specimen and were mounted on threeslides, with at least five sections on each slide. Oneslide from each biopsy specimen was stained by ironhaematoxylin and eosin, another by the periodicacid-Schiff method, and the third by a reticulinstain. The slides were examined by one of us (R.W.),who was unaware of the name of the patient, whetherthe specimen had been taken before or after opera-tion, and to which treatment group the patientbelonged.
Gastritis was graded according to the classifica-tion of Whitehead et al. (1972) and duodenitisaccording to that of Whitehead et al. (1975). Thegrades of gastritis or duodenitis are shown in oursubsequent figures according to the key given inFig. 2.
Fig. 1 Standard biopsy sites within the stomach andduodenal bulb. Each site is designated by the numbershown.
Gastric Biopsies
D Normal Mucosa
El Superficial Gastritis
Mild Atrophic Gastritis
ModerateEl Atrophic Gastritis
Duodenal Biopsies
D Normal Mucosa
El Mild Duodenitis
E Moderate Duodenitis
O Severe Duodenitis
I 1 Unsatisfactory Biopsy
Fig. 2 Key to Figs. 3, 4, and 5.
GASTRITIS INDEXTo facilitate comparison of the different histologicalpictures found in the various biopsy specimens, eachgrade of gastritis was given a number. Normalmucosa was designated 0, superficial gastritis 1,mild atrophic gastritis 2, moderately severe atrophicgastritis 3, and severe atrophic gastritis 4. As thehistological abnormalities in the different grades ofgastritis appear to be progressively more severefrom grades 1 to 4 it seems reasonable to score eachbiopsy according to its grade as an index of theseverity of gastritis. Then, for example, each biopsyspecimen showing superficial gastritis scores 1 whilea specimen with severe atrophic gastritis scores 4. Agastritis index for the whole stomach or for theantrum or the body can then be obtained by summ-ing the appropriate biopsy indices.
DUODENITIS INDEXIn a similar way grades of duodenitis found in theduodenal bulb biopsy specimens were given an index
15) of 1 for mild duodenitis, 2 for moderately severeduodenitis, and 3 for severe duodenitis. Normalmucosa was scored 0.
GASTRIC ACID OUTPUTGastric acid output was estimated both before andafter operation in all patients by gastric secretiontests which were performed in the morning after anovernight fast. A Salem size 14 French gauge naso-gastric sump tube was passed into the stomach andthe patient positioned horizontally, lying on theleft side. The position of the tube was checked bymeans of the water test (Findlay et al., 1972). Restingcontents were aspirated and discarded and 15-minute collections of gastric juice were then made byfrequent, intermittent hand aspiration using a 20 mlsyringe. After a basal hour, betazole hydrochloride(Histalog), 1-7 mg per kg, was injected subcutane-
720
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

Gastritis, duodenitis, and circulating levels ofgastrin in duodenal ulcer before and after vagotomy
ously and a further eight 15-minute collections weremade. During the test blood samples were collectedintermittently for estimations of serum gastrin as willbe described.The Histalog gastric secretion test was repeated
three months after operation. In addition, at thistime, all the patients agreed to have an insulin test.The same technique was used for collecting thegastric juice but soluble insulin, in a dose of 0-2units per kg body weight, was given intravenouslyinstead of Histalog. Blood samples were collectedduring the basal hour and at 30, 45, and 60 minutesafter the insulin injection for blood sugar measure-ments. A fall in blood glucose level below 40 mg/100 ml (2-2 mmol/l) was achieved in all cases.
AnalysisAfter noting the volume, 1 ml of each 15-minutesample of gastric aspirate was titrated with 0-1 NNa OH to a pH 7 end-point using a micro-electrodepH meter. The total acid output of each 15-minutesample was expressed in mmol.
Basal acid output (BAO) was calculated for thewhole hour by addition of the four quarter-hoursamples. The peak acid output (PAO) after Histalogor insulin was calculated by adding the two highest
E._
q
ECz
consecutive 15-minute outputs and multiplying bytwo. In addition, the insulin tests were assessed bythe criteria of Hollander (1948).
BLOOD SAMPLING FOR SERUM GASTRINSTUDIESBlood samples (10 ml) for serum gastrin estimationswere drawn from an indwelling tapped Tefloncannula which was positioned in an arm vein at thebeginning of the test and retained until the lastsample had been drawn.During the gastric secretion tests the first venous
blood sample was taken half an hour before theHistalog or insulin was administered. After Histalog,four additional venous blood samples were taken athalf-hour intervals and, after the insulin, usuallyeight further samples at quarter-hour intervals.
In addition, fasting and postprandial bloodsamples for gastrin assay were collected on a separ-ate morning both before and three months afteroperation. The patients were asked to fast frommidnight and to come to the hospital by 9 a.m. Afasting blood sample was taken and they were givena breakfast. At intervals of 30 minutes, timed fromwhen the breakfast was started, four additionalvenous blood samples were collected. In most cases
o Pre-op
* Post-op
Fig. 3 The distribution andseverity of gastritis andduodenitis in duodenal ulcer.
o .
.r1-1..
10 ",XP* SITE
BIOPSY SITES
a- a,.CL ffi
o _ ,0 @Z _= c,=c= w
721
&4-j
0la = '*c 4m 1-zL6 X 4.)
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

D. D. Meikle, K. B. Taylor, S. C. Truelove, and R. Whitehead
the breakfast consisted of cereal with milk andsugar, bacon and egg, toast, and tea or coffee.Occasionally, however, the patient was not able toeat this full breakfast and had a more limited meal.However, each patient had a similar breakfastafter operation to the one taken before operation.
After each of the different tests the blood sampleswere centrifuged and the serum separated and storedin Bijou bottles in a deep freeze at minus 20°C. Eachspecimen was given a code number and at intervalsof two to three months the samples were collectedtogether in an insulated box containing dry ice anddispatched by air freight to California for the radio-immunoassay. As other samples of serum withsimilar styled code numbers from patients withother diseases were also included, the results of theradio-immuno assay were not biased by any know-ledge of the type of specimen.
ESTIMATION OF SERUM GASTRIN ACTIVITYThis was carried out in the Department of Medicine,Stanford University Medical Center, by a modifica-tion of the radio-immunoassay method of Yalowand Berson (1970).
Antisera to crude procine gastrin conjugated withbovine-serum albumin by the method of Yip andJordan (1970) were obtained by immunization ofHartley-strain female guinea-pigs according to aschedule of multiple subcutaneous injections at onemonth intervals. These antisera have been charac-terized by Rosenquist and Holmquist (1974). Theyrecognize the C-terminal tetrapeptide of synthetichuman gastrin I (ICI) and display increasing bindingover the tetraoctapeptide range.
Synthetic human gastrin I (ICI Batch No. 630/20)labelled with 125iodine by the modified chloramine-T method of Hunter and Greenwood (1962) wasused as the trace. Antisera concentrations wereselected to give a maximal binding capacity ofapproximately 30%. All serum samples were testedin triplicate, with duplicate controls (no antibodyadded). Separation of antibody-bound to antibody-free gastrin was effected by adding an equal volumeof polyethylene glycol 6000 (PEG), 30% wt/wtsolution in distilled water to the reaction mixture.Standard inhibition curves were established for eachassay.
Radioactivity in the PEG precipitates was esti-mated in an automatic gamma counter (NuclearChicago Model 1035, Serial 130). The counts weretransmitted by teletype to a computer and thecomputer data expressed as means ± one standarddeviation, a standard curve being obtained for thesame assay. Our own observations have establisheda normal range of 0-200 pg/ml for human subjectsunder fasting conditions.
Results
EXTENT AND SEVERITY OF GASTRITIS ANDDUODENITIS ASSOCIATED WITH CHRONICDUODENAL ULCER BEFORE AND AFTERVAGOTOMYFigure 3 shows the histological findings in the biopsyspecimens taken from the six standard sites in eachpatient both before and three months after vag-otomy. It can be seen that the fundus of the stomachwas normal in 17 (85 %) of the 20 patients with duo-denal ulcer before operation. In only three (15%)were the fundal biopsy specimens abnormal andthey showed superficial gastritis only. The percent-age of normal biopsy specimens decreased as thesite of biopsy progressed down the stomach fromthe proximal fundal to the distal pre-pyloric site and,in addition, the more severe grades of gastritiswere found distally. Thus it is seen that duodenalulcer is usually associated with gastritis, althoughthis varies in extent and severity from patient topatient. In the majority there is gastritis involvingthe pre-pyloric region and mid-lesser curve. Thestomach proximal to this, corresponding to the bodygland area, is only occasionally involved. Thegastritis is not only much more frequent in the distalstomach but it is also more severe.The duodenal bulb biopsy specimens all showed
an increased chronic inflammatory cell infiltrate ofthe lamina propria and this was of moderate orsevere degree in 17 (85 %). Thus we can conclude thatduodenal ulceration is always associated with duo-denitis. Furthermore, as the biopsy specimens weretaken from an area of the bulb well clear of theulcer, the duodenitis is at least a regional mani-festation and not purely localized to the immediatevicinity of the ulcer.
After treatment by either form of vagotomy therewas a decrease in the number of normal specimensat each site except at the pre-pyloric site where therewas no change. In addition, more of the biopsyspecimens showed atrophic gastritis at the fundaland mid-greater curve biopsy sites. When the in-dices of gastritis found preoperatively at the differentbiopsy sites were compared with those found afteroperation, the postoperative deterioration at thefundus was highly significant (p < 0-01) and that atthe mid-greater curve site significant (p < 0 05). Atthe two distal sites, the mid-lesser curve and the pre-pyloric, the changes were not statistically significant.In specimens from the duodenal bulb, however,there was some improvement postoperatively in theincidence and severity of the duodenitis.
Similar postoperative changes in the picture ofgastritis and duodenitis were seen regardless of theparticular form of vagotomy (Figs. 4 and 5). In
722
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

Gastritis, duodenitis, and circulating levels ofgastrin in duodenal ulcer before and after vagotomy
108-
o
Bt1F 0 S S B
-ft I... ... ...C?t.... p
o Pre-op
* Post-op
o *....1. . ..........
810
-,_ B * .S.
BIOPSY S ITES
10
86
4
2u
2
46
810
0
Fig. 4 The distribution andseverity ofgastritis andduodenitis in duodenal ulcer
,o .. t.... before and after HSV.
-W 0 .0
... co..... C
am ED =
o Pre-op* Post-op
.
I%A:3
c:3LL.
cs
sQ
B IOPSY S ITES
-0 0.
IFig. 5 The distribution andseverity ofgastritis and
*- duodenitis in duodenal ulcerbefore and after TVP.
each group there was an improvement in the duo-denitis but an increase in both the incidence andseverity of the gastritis affecting the proximalstomach (corresponding to the body and fundus)with atrophic gastritis developing in the fundusafter operation in several patients, whereas noneshowed this before operation. After TVP, there wasgreater improvement in the duodenitis, less atrophyat the fundus, an improvement in the severity butnot in the incidence at the pyloric end of the stomach,and an increased incidence of gastritis at the middleof the lesser curve. When the two distal biopsy siteswere considered together as a measure of antralgastritis, there was very little difference between thetwo post-vagotomy groups, although there was a
slight overall worsening in the TVP group. Thesepostoperative differences between the two treatmentgroups, which were well matched preoperatively,are not statistically significant. However, each groupconsisted of only 10 patients and it would beadvisable to study a larger number before decidingthat there is no difference between the two opera-tions in this respect.
GASTRIC ACID OUTPUT BEFORE AND
AFTER VAGOTOMYIn Fig. 6 the pre- and postoperative acid outputvalues are shown. It can be seen that both opera-tions produced a highly significant reduction of thePAO in response to Histalog stimulation. In addi-
c
E._
wo
coE
v
S
E0C
Eu
:
VWaCDE
E02%Ac
S
w
Eu
:
> o2 0(U...._ , L, >, :3 a D
Ei i a. cL cj a) D
.v
-n- e...t..w.s -.- I... .... Vr
I
723
0
..... . ...... . ...... . .....
4)
n4i
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from
D. D. Meikle, K. B. Taylor, S. C. Truelove, and R. Whitehead
30
ETE 20-
I0
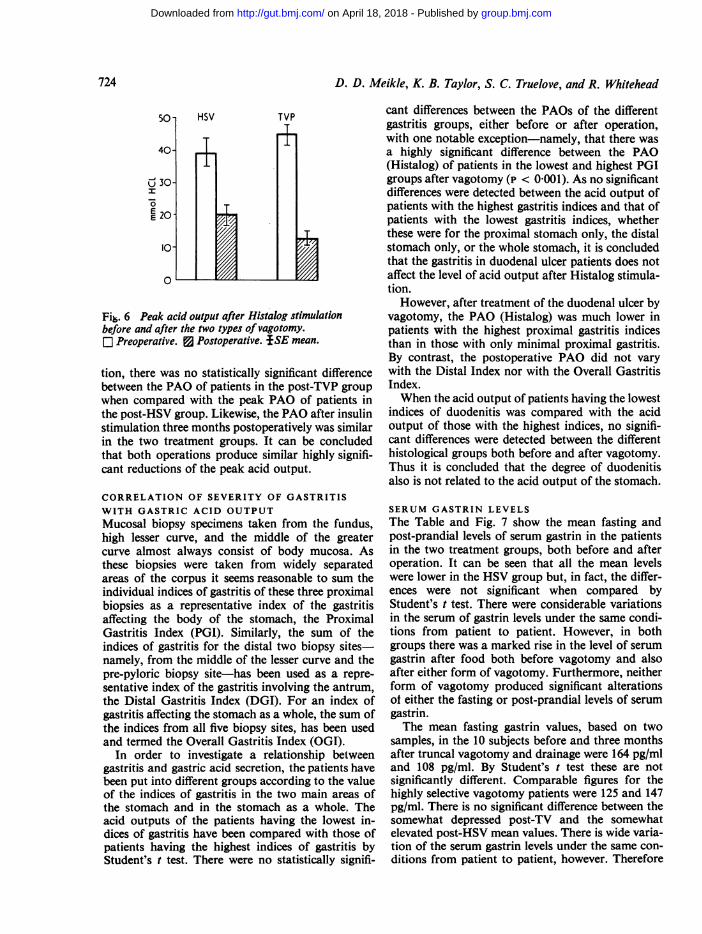
Fir. 6 Peak acid output after Histalog stimulationbefore and after the two types of vagotomy.[ Preoperative. 3 Postoperative. *SE mean.
tion, there was no statistically significant differencebetween the PAO of patients in the post-TVP groupwhen compared with the peak PAO of patients inthe post-HSV group. Likewise, the PAO after insulinstimulation three months postoperatively was similarin the two treatment groups. It can be concludedthat both operations produce similar highly signifi-cant reductions of the peak acid output.
CORRELATION OF SEVERITY OF GASTRITISWITH GASTRIC ACID OUTPUTMucosal biopsy specimens taken from the fundus,high lesser curve, and the middle of the greatercurve almost always consist of body mucosa. Asthese biopsies were taken from widely separatedareas of the corpus it seems reasonable to sum theindividual indices of gastritis of these three proximalbiopsies as a representative index of the gastritisaffecting the body of the stomach, the ProximalGastritis Index (PGI). Similarly, the sum of theindices of gastritis for the distal two biopsy sites-namely, from the middle of the lesser curve and thepre-pyloric biopsy site-has been used as a repre-sentative index of the gastritis involving the antrum,the Distal Gastritis Index (DGI). For an index ofgastritis affecting the stomach as a whole, the sum ofthe indices from all five biopsy sites, has been usedand termed the Overall Gastritis Index (OGI).
In order to investigate a relationship betweengastritis and gastric acid secretion, the patients havebeen put into different groups according to the valueof the indices of gastritis in the two main areas ofthe stomach and in the stomach as a whole. Theacid outputs of the patients having the lowest in-dices of gastritis have been compared with those ofpatients having the highest indices of gastritis byStudent's t test. There were no statistically signifi-
cant differences between the PAOs of the differentgastritis groups, either before or after operation,with one notable exception-namely, that there wasa highly significant difference between the PAO(Histalog) of patients in the lowest and highest PGIgroups after vagotomy (p < 0-001). As no significantdifferences were detected between the acid output ofpatients with the highest gastritis indices and that ofpatients with the lowest gastritis indices, whetherthese were for the proximal stomach only, the distalstomach only, or the whole stomach, it is concludedthat the gastritis in duodenal ulcer patients does notaffect the level of acid output after Histalog stimula-tion.
However, after treatment of the duodenal ulcer byvagotomy, the PAO (Histalog) was much lower inpatients with the highest proximal gastritis indicesthan in those with only minimal proximal gastritis.By contrast, the postoperative PAO did not varywith the Distal Index nor with the Overall GastritisIndex.When the acid output of patients having the lowest
indices of duodenitis was compared with the acidoutput of those with the highest indices, no signifi-cant differences were detected between the differenthistological groups both before and after vagotomy.Thus it is concluded that the degree of duodenitisalso is not related to the acid output of the stomach.
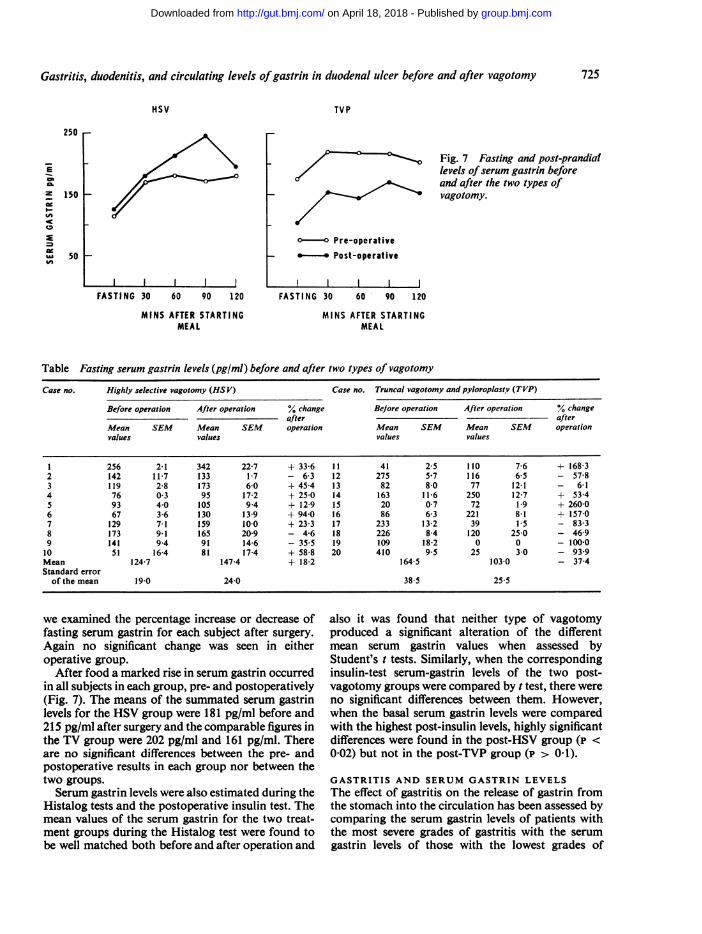
SERUM GASTRIN LEVELSThe Table and Fig. 7 show the mean fasting andpost-prandial levels of serum gastrin in the patientsin the two treatment groups, both before and afteroperation. It can be seen that all the mean levelswere lower in the HSV group but, in fact, the differ-ences were not significant when compared byStudent's t test. There were considerable variationsin the serum of gastrin levels under the same condi-tions from patient to patient. However, in bothgroups there was a marked rise in the level of serumgastrin after food both before vagotomy and alsoafter either form of vagotomy. Furthermore, neitherform of vagotomy produced significant alterationsof either the fasting or post-prandial levels of serumgastrin.The mean fasting gastrin values, based on two
samples, in the 10 subjects before and three monthsafter truncal vagotomy and drainage were 164 pg/mland 108 pg/mI. By Student's t test these are notsignificantly different. Comparable figures for thehighly selective vagotomy patients were 125 and 147pg/ml. There is no significant difference between thesomewhat depressed post-TV and the somewhatelevated post-HSV mean values. There is wide varia-tion of the serum gastrin levels under the same con-ditions from patient to patient, however. Therefore
724
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from
Gastritis, duodenitis, and circulating levels ofgastrin in duodenal ulcer before and after vagotomy
HSV
FASTING 30 60 90 120
MINS AFTER STARTINGMEAL
TVP
o-o Pre-operative- *-. Post-operative
FASTING 30 60 90 120
MINS AFTER STARTINGMEAL
Fig. 7 Fasting and post-prandiallevels ofserum gastrin beforeand after the two types ofvagotomy.
Table Fasting serum gastrin levels (pg/ml) before and after two types of vagotomy
Case no. Highly selective vagotomy (HS V) Case no. Truncal vagotomy and pyloroplasty (TVP)
Before operation After operation % change Bejore operation After operation changeafter afier
Mean SEM Mean SEM operation Mean SEM Mean SEM operationvalues values values values
1 256 2-1 342 22-7 + 33-6 11 41 25 110 7-6 + 168-32 142 11 7 133 1-7 - 6-3 12 275 5 7 116 6-5 - 57-83 119 2-8 173 6-0 + 45-4 13 82 8-0 77 12-1 - 6 14 76 03 95 17-2 + 25-0 14 163 11-6 250 127 + 5345 93 40 105 94 + 129 15 20 07 72 1.9 + 260-06 67 3-6 130 13-9 + 940 16 86 6-3 221 8 1 + 15707 129 7-1 159 100 + 23-3 17 233 13-2 39 15 - 83-38 173 9 1 165 20-9 - 4-6 18 226 8-4 120 250 - 46-99 141 94 91 14-6 - 355 19 109 18-2 0 0 - 100*010 51 16-4 81 17-4 + 588 20 410 95 25 30 - 939Mean 124-7 147-4 + 18-2 164-5 103-0 - 37-4Standard error
of the mean 19.0 24-0 38 5 25 5
we examined the percentage increase or decrease offasting serum gastrin for each subject after surgery.Again no significant change was seen in eitheroperative group.
After food a marked rise in serum gastrin occurredin all subjects in each group, pre- and postoperatively(Fig. 7). The means of the summated serum gastrinlevels for the HSV group were 181 pg/ml before and215 pg/ml after surgery and the comparable figures inthe TV group were 202 pg/ml and 161 pg/ml. Thereare no significant differences between the pre- andpostoperative results in each group nor between thetwo groups.Serum gastrin levels were also estimated during the
Histalog tests and the postoperative insulin test. Themean values of the serum gastrin for the two treat-ment groups during the Histalog test were found tobe well matched both before and after operation and
also it was found that neither type of vagotomyproduced a significant alteration of the differentmean serum gastrin values when assessed byStudent's t tests. Similarly, when the correspondinginsulin-test serum-gastrin levels of the two post-vagotomy groups were compared by t test, there wereno significant differences between them. However,when the basal serum gastrin levels were comparedwith the highest post-insulin levels, highly significantdifferences were found in the post-HSV group (p <0-02) but not in the post-TVP group (p > 0 1).
GASTRITIS AND SERUM GASTRIN LEVELSThe effect of gastritis on the release of gastrin fromthe stomach into the circulation has been assessed bycomparing the serum gastrin levels of patients withthe most severe grades of gastritis with the serumgastrin levels of those with the lowest grades of
250 r
150 1-
E
z
IS
:A
50
725
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

D. D. Meikle, K. B. Taylor, S. C. Truelove, and R. Whitehead
gastritis. As there were no significant differencesbetween the corresponding serum gastrin levels of thetwo treatment groups, the two groups have beencombined for this purpose. No statistically signifi-cant differences were found between the levels ofserum gastrin of the patients in the lowest and highestgroups of PGI or DGI or OGI, either before orafter operation.
DUODENITIS AND SERUM GASTRIN LEVELSIn a similar way, the relationship between theseverity of duodenitis and the serum gastrin hasbeen investigated by comparing the correspondinglevels of serum gastrin of each of the patients in thelowest duodenitis indices group with that of each ofthe patients in the highest duodenitis indices groupby Student's unpaired t test. Again no significantdifferences were found and it is concluded that theserum gastrin levels of patients with severe duo-denitis of the duodenal bulb associated with duo-denal ulcer are not different from those patientswith only mild duodenitis and the same is true forthese patients after vagotomy.
COMPARISON OF ACID OUTPUT WITHSERUM GASTRIN LEVELSTo determine whether there is a correlation betweenthe serum gastrin levels and the acid output the co-efficients of linear correlation were determined usingthe Bravais-Pearson formula programmed into acomputer. It was found that there were no significantcorrelations between the levels of serum gastrin inthe samples taken during the basal hour of the pre-operative Histalog test, the postoperative Histalog,or postoperative insulin tests and the respective BAOvalues of the two treatment groups, with one excep-tion. This occurred in the post-TVP group, duringthe insulin test, where the r value was 0l8. When thedifferent highest gastrin levels after Histalog orinsulin were correlated with the corresponding PAOvalues of patients in the different treatment groups,the r values were all low. This lack of correlation isprobably because the serum gastrin is only one ofseveral variables in the control of gastric acidity.Also, the serum gastrin levels fluctuate widely fromtime to time and blood samples for assay were onlycollected at half-hourly intervals. In this study, noattempt was made to correlate the serum gastrinlevel with rates of acid secretion in individualpatients.
Discussion and conclusions
The question of the association between chronicpeptic ulcer and gastritis remains controversial. Inthe past, the methods of study have been defective.
Post-mortem material is useless for studying gastricpathology unless very special steps are taken to pre-vent autolysis (Faber, 1935). The study of resectedportions of stomach suffers from the limitation thathistological changes in the mucosa occur during thecourse of the operation (Schindler et al., 1939;Sanders and Mecray, 1941). Blind biopsy was a use-ful step forward but usually the specimen came fromonly one site in the stomach, although there was theadvantage that serial studies were possible.Modern fibreoptic endoscopy has transformed the
situation. The whole of the upper gastrointestinaltract as far as the descending duodenum can bevisualized and biopsy specimens obtained undervision. The method is new and so far has not beenemployed very much for scientific investigation al-though widely used as a diagnostic tool.
In the present study, biopsy specimens have beenobtained from five sites within the stomach and alsofrom the duodenal bulb. In addition, the gastricacid secretion and circulating levels of gastrin havebeen measured in every patient. All these observa-tions were performed initially on patients with duo-denal ulcer who had been selected for surgical treat-ment. Half the patients were treated by a truncalvagotomy and pyloroplasty (TVP) and half by thenew operation of highly selective vagotomy. Threemonths after the operation, the various investiga-tions were all repeated.
Gastritis was present in nearly all these patientswith duodenal ulcer but it tended to be concentratedand to be most severe in the distal part of thestomach-namely, in the antrum and along the lessercurve. More than half of the patients showed somedegree of gastritis in the body of the stomach but thefundus was usually spared. The findings contrastwith what is found in gastric ulcer, in which wide-spread gastritis is a common finding (Gear et al.,1971).The effect of vagotomy on the histological picture
was similar whichever type of vagotomy was per-formed. After TVP and HSV alike, the gastritis inthe pyloric end of the stomach tended to lessen,whereas it became worse in the more proximal areas.It is especially noteworthy that, after vagotomy,the fundus was frequently affected by gastritis,whereas it was exceptional for it to be affectedbeforehand. Moreover, the postoperative fundalgastritis was frequently atrophic and not merelysuperficial.Two points are worthy of discussion in this con-
text. The first is that it is possible that the proximalgastritis which develops after a vagotomy may be aprogressive change which will eventually lead tosevere atrophic gastritis in a large proportion of thepatients. This would explain previous findings that
726
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

Gastritis, duodenitis, and circulating levels ofgastrin in duodenal ulcer before and after vagotomy
intrinsic factor secretion and vitamin B12 absorptionare diminished after vagotomy (Cox et al., 1964;Bitsch et al., 1966; Adams et al., 1967). There is alsothe possibility that atrophic gastritis is a pre-cancerous lesion. Both megaloblastic anaemia andcancer of the stomach are late complications ofpartial gastrectomy, after which gastritis is verycommon in the gastric stump (Stalsberg and Taksdal,1971). It is often supposed that a vagotomy is far lesslikely to be followed by widespread gastritis but thepresent results cast doubt on this view. It appears tobe highly desirable that the patients included in thepresent study should be re-examined by endoscopywith biopsy after a further interval of time to deter-mine if the gastritis has continued to progress.The second point concerns the mechanism for
the development of gastritis postoperatively in areasof the stomach previously healthy. If the function ofthe pylorus has been disrupted by a pyloroplasty, itis easy to see that reflux of duodenal contents mayreadily occur and might be responsible for causingthe gastritis. However, in the present series, patientstreated by highly selective vagotomy, in which thepylorus is left untouched and the vagal nerve supplyto the antrum and duodenum is preserved, showed aworsening of the gastritis in the proximal stomachsimilar to that found after TVP. This suggests thatthe pyloroplasty is not relevant to the proximalgastritis, and, by a process of exclusion, one is drivento conclude that the vagotomy is responsible. How-ever, we are totally ignorant of the mechanismswhereby division of the vagal nerve could inducemucosal disease. It is possible that the gastritis is theresult of trophic changes after the vagotomy but, atthe present time, this is no more than speculation.There was no correlation between the severity of
the distal gastritis, even with atrophy, and the levelsof gastrin in the serum. Whether this means that thesize and function of the antral gastrin-secreting cellpopulation is unaffected by the antral gastritisassociated with peptic ulcer disease or that changein the one is compensated for by inverse change inthe other can be resolved only by quantitativedeterminations of the antral G-cell mass.
Duodenitis appears to be an invariable accom-paniment of chronic duodenal ulcer, as judged bythe present series. Although only the duodenal bulbwas biopsied, care was taken to obtain the biopsyspecimen well away from the actual ulcer. Aftervagotomy, the duodenitis frequently improves. It ispossible that the sharp reduction in the acid andpepsin output of the stomach brought about byvagotomy is responsible for the alleviation of theduodenitis, although, if this is the explanation, itmakes the worsening of the gastritis in all theproximal areas of the stomach even more mysterious.
A further reason for doubting whether the improve-ment in the duodenitis which occurs after vagotomycan be attributed to the reduction in the acid outputof the stomach is that the degree of duodenitisbefore operation is not correlated with the acid out-put of the stomach.
After a vagotomy, whether it be highly selectiveor truncal, the fasting levels of serum gastrin showno significant change from preoperative levels.Furthermore, preoperative levels do not differ fromthose in a healthy control group of subjects, a findingin accord with those of Trudeau and McGuigan(1970) and Wesdorp and Fischer (1974) but differentfrom that of Becker et al. (1973), who found signifi-cantly higher fasting serum-gastrin levels in patientswith duodenal ulcer compared with control subjects.McGuigan and Trudeau (1972) reported four
patients who were treated by vagotomy and ant-rectomy for duodenal ulcer and in whom postopera-tive fasting serum-gastrin levels were markedly re-duced, almost certainly due to removal of a majorsource of gastrin secretion. These authors found nosignificant change in fasting gastrin levels in 24duodenal ulcer patients after truncal vagotomy andpyloroplasty, however, although the rates of gastricacid secretion were much reduced. Incompletevagotomy was not responsible for this absence ofchange. These results are in complete contrast tothose of Becker et al. (1973) who found no signifi-cant change in fasting gastrin levels after antrectomywith vagotomy and a significant increase after pylo-roplasty and vagotomy. Stern and Walsh (1973) re-ported raised fasting serum gastrin levels in eightsubjects after truncal vagotomy and pyloroplasty.However, these subjects had not been studied beforethe operation. In addition, several of them were notexamined until some years after the operation, bywhich time a severe proximal gastritis might havedeveloped, producing a more profound hypochlor-hydria with resultant lack ofG cell suppression. Ourown data confirm those of McGuigan and Trudeau(1970). We have found no significant change in thefasting serum gastrin after truncal vagotomy andpyloroplasty. Furthermore, we have shown'that nosignificant change in fasting serum gastrin occurs asa consequence of highly selective vagotomy withoutany drainage procedure.
It is clear that there is considerable variation inbasal gastrin levels between individuals and in thesame individual when sampling is conducted in whatseems to be similar conditions.The post-prandial gastrin responses we observed
seemed to be unaffected by vagotomy. Increases ordecreases of peak responses occurred in differentsubjects after both truncal and highly selectivevagotomy. These variations might be an expression
727
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

728 D. D. Meikle, K. B. Taylor, S. C. Truelove, and R. Whitehead
of variable rates of postoperative recovery of homeo-static control. Clearly no hypothesis can be con-structed with confidence, but later studies of thesame patients, together with similar gastric biopsystudies, may help to resolve some of the confusionwhich at present obtains.The absence of significant differences in fasting
and post-prandial serum gastrin levels before andafter either truncal vagotomy, which denervates theantrum, or highly selective vagotomy, which doesnot, suggests that lesser vagal activity than thatoccurring during an insulin test is not an importantfactor in the stimulation of gastrin release from theantrum. In spite of the unchanged levels of circulat-ing gastrin after vagotomy, the acid output of thestomach is much reduced by either operation,illustrating by contrast the crucial role of the vagusin parietal-cell function. One important question iswhether this inhibition of the physiological activityof the gastric parietal cell may be the first step in aprocess which leads eventually to atrophy of thegastric mucosa.
This study was supported in part by USPHS GrantAM 06971 and the U.S. Veterans Administration andalso in part by a grant from the Cancer ResearchCampaign. We wish to thank Mrs Stella Linberg,Mrs Janet Constantinou, Mrs Ysanne Smart, andMrs Elizabeth Calvert for their assistance.
References
Adams, J. F., Cox, A. G., Kennedy, E. H., and Thompson, J.(1967). Effect of medical and surgical vagotomy on in-trinsic factor secretion. British Medical Journal, 3, 473-476.
Becker, H. D., Reeder, D. D., and Thompson, J. C. (1973).Effect of truncal vagotomy with pyloroplasty or withantrectomy on food-stimulated gastrin values in patientswith duodenal ulcer. Surgery, 74, 580-586.
Bitsch, V., Christiansen, P. M., Faber, V., and R0dbro, P.(1966). Gastric secretory patterns before and after vago-tomy. Lancet, 1, 1288-1291.
Cox, A. G., Bond, M. R., Podmore, D. A., and Rose, D. P.(1964). Aspects of nutrition after vagotomy and gastro-jejunostomy. British Medical Journal, 1, 465-469.
Faber, K. (1935). Gastritis and its Consequences. OxfordUniversity Press: London.
Findlay, J. M., Prescott, R. J., and Sircus, W. (1972).Comparative evaluation of water recovery test and fluoro-scopic screening in positioning a nasogastric tube duringgastric secretory studies. British Medical Journal, 4, 458-461.
Gear, M. W. L., Truelove, S. C., and Whitehead, R. (1971).Gastric ulcer and gastritis. Gut, 12, 639-645.
Hollander, F. (1948). Laboratory procedures in the study ofvagotomy. Gastroenterology, 11, 419-425.
Hunter, W. M., and Greenwood, F. C. (1962). Preparation ofiodine-131 labelled human growth hormone of high specificactivity. Nature, 194, 495-496.
McGuigan, J. E., and Trudeau, W. L. (1972). Serum gastrinlevels before and after vagotomy and pyloroplasty orvagotomy and antrectomy. New England Journal ofMedicine, 286, 184-188.
Rosenquist, G. L., and Holmquist, A. M. (1974). The speci-ficity of antibodies directed to porcine gastrin. Immuno-chemistry, 11, 489-494.
Sanders, G. B., and Mecray, P. M. (1941). Pseudogastritisof operative origin. Annals of Surgery, 114, 986-996.
Schindler, R., Necheles, H., and Gold, R. L. (1939). Surgicalgastritis. Surgery, Gynecology, and Obstetrics, 69, 281-286.
Stalsberg, H., and Taksdal, S. (1971). Stomach cancerfollowing gastric surgery for benign conditions. Lancet, 2,1175-1177.
Stern, D. H., and Walsh, J. H. (1973). Gastrin release inpostoperative ulcer patients: evidence for release of duo-denal gastrin. Gastroenterology, 64, 363-369.
Trudeau, W. L., and McGuigan, J. E. (1970). Serum gastrinlevels in patients with peptic ulcer disease. Gastroenter-ology, 59, 6-12.
Wesdorp, R. I. C., and Fischer, J. E. (1974). Plasma-gastrinand acid secretion in patients with peptic ulceration.Lancet, 2, 857-860.
Whitehead, R., Roca, M., Meikle, D. D., Skinner, J. M.,and Truelove, S. C. (1975). The histological classificationof duodenitis in fibreoptic biopsy specimens. Digestion, 13,129-136.
Whitehead, R., Truelove, S. C., and Gear, M. W. L. (1972).The histological diagnosis of chronic gastritis in fibre-optic gastroscope biopsy specimens. Journal of ClinicalPathology, 25, 1-11.
Yalow, R. S., and Berson, S. A. (1970). Size and chargedistinctions between endogenous human plasma gastrin inperipheral blood and heptadecapeptide gastrins. Gastro-enterology, 58, 609-615.
Yip, B. S. S. C., and Jordan, P. H., Jr. (1970). Radio-immunoassay of gastrin using antiserum to porcinegastrin 1 (34796). Proceedings of the Society for Experi-mental Biology and Medicine, 134, 380-385.
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from

before and after vagotomy.levels of gastrin in duodenal ulcer Gastritis duodenitis, and circulating
D D Meikle, K B Taylor, S C Truelove and R Whitehead
doi: 10.1136/gut.17.9.7191976 17: 719-728 Gut
http://gut.bmj.com/content/17/9/719Updated information and services can be found at:
These include:
serviceEmail alerting
online article. article. Sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
CollectionsTopic
collections Articles on similar topics can be found in the following
(848)Gastrointestinal hormones (1689)Stomach and duodenum
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 18, 2018 - Published by http://gut.bmj.com/Downloaded from





























