Embed Size (px)
Citation preview

review article
Wien Klin Wochenschr (2017) 129:81–95DOI 10.1007/s00508-016-1096-4
Gait disorders in adults and the elderly
A clinical guide
Walter Pirker · Regina Katzenschlager
Received: 7 May 2016 / Accepted: 14 September 2016 / Published online: 21 October 2016© The Author(s) 2016. This article is available at SpringerLink with Open Access.
Summary Human gait depends on a complex inter-play of major parts of the nervous, musculoskeletaland cardiorespiratory systems. The individual gaitpattern is influenced by age, personality, mood andsociocultural factors. The preferred walking speed inolder adults is a sensitive marker of general healthand survival. Safe walking requires intact cognitionand executive control. Gait disorders lead to a lossof personal freedom, falls and injuries and result ina marked reduction in the quality of life. Acute on-set of a gait disorder may indicate a cerebrovascularor other acute lesion in the nervous system but alsosystemic diseases or adverse effects of medication,in particular polypharmacy including sedatives. Theprevalence of gait disorders increases from 10% inpeople aged 60–69 years to more than 60% in com-munity dwelling subjects aged over 80 years. Sen-sory ataxia due to polyneuropathy, parkinsonism andfrontal gait disorders due to subcortical vascular en-cephalopathy or disorders associated with dementiaare among the most common neurological causes.Hip and knee osteoarthritis are common non-neu-
Both authors agree with the revised version of themanuscript. F. Kralinger and D. Maestro consented to bementioned in the acknowledgement section of themanuscript.
W. Pirker, MD (�)Department of Neurology, Medical University of Vienna,Währinger Gürtel 18–20, 1090 Vienna, [email protected]
W. Pirker, MDDepartment of Neurology, Wilhelminenspital, Vienna,Austria
R. Katzenschlager, MDDepartment of Neurology and Karl Landsteiner Institute forNeuroimmunological and Neurodegenerative Conditions,Donauspital, Vienna, Austria
rological causes of gait disorders. With advancingage the proportion of patients with multiple causesor combinations of neurological and non-neurologi-cal gait disorders increases. Thorough clinical obser-vation of gait, taking a focused patient history andphysical, neurological and orthopedic examinationsare basic steps in the categorization of gait disordersand serve as a guide for ancillary investigations andtherapeutic interventions. This clinically oriented re-view provides an overview on the phenotypic spec-trum, work-up and treatment of gait disorders.
Keywords Aging · Falls · Neurological gait disorders ·Parkinsonism · Orthopaedic gait disorders
Introduction
Walking is a common activity of daily living and at thesame time a very complex one. It involves all levelsof the nervous system and many parts of the muscu-loskeletal apparatus as well as the cardiorespiratorysystem. A person’s gait pattern is strongly influencedby age, personality and mood. Moreover, sociocul-tural factors play a role: for instance, persons living inlarge cities walk significantly faster than those livingin rural areas [1]. The prevalence of gait and balancedisorders markedly increases with age, from around10% between the ages of 60 and 69 years to morethan 60% in those over 80 years [2]. Gait impairmentsmay greatly affect the quality of life [2] and restrictthe personal independence of those affected. More-over, balance and gait problems may be precursorsof falls, which are the most common cause of severeinjuries in the elderly [3]. Walking is a sensitive in-dicator of overall health status and the self-selectedwalking speed closely correlates with individual lifeexpectancy in elderly persons [4]. Importantly, slowgait in elderly non-demented persons correlates more
K Gait disorders in adults and the elderly 81
review article
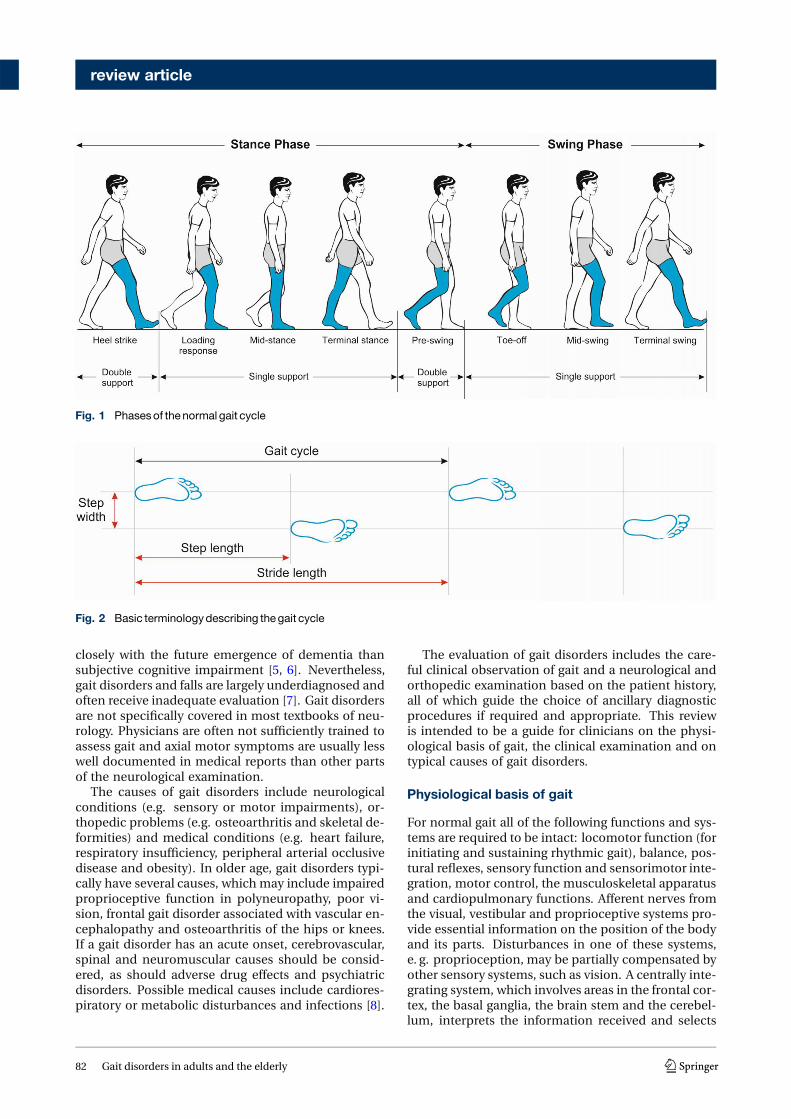
Fig. 1 Phasesof thenormal gait cycle
Fig. 2 Basic terminologydescribing thegait cycle
closely with the future emergence of dementia thansubjective cognitive impairment [5, 6]. Nevertheless,gait disorders and falls are largely underdiagnosed andoften receive inadequate evaluation [7]. Gait disordersare not specifically covered in most textbooks of neu-rology. Physicians are often not sufficiently trained toassess gait and axial motor symptoms are usually lesswell documented in medical reports than other partsof the neurological examination.
The causes of gait disorders include neurologicalconditions (e.g. sensory or motor impairments), or-thopedic problems (e.g. osteoarthritis and skeletal de-formities) and medical conditions (e.g. heart failure,respiratory insufficiency, peripheral arterial occlusivedisease and obesity). In older age, gait disorders typi-cally have several causes, which may include impairedproprioceptive function in polyneuropathy, poor vi-sion, frontal gait disorder associated with vascular en-cephalopathy and osteoarthritis of the hips or knees.If a gait disorder has an acute onset, cerebrovascular,spinal and neuromuscular causes should be consid-ered, as should adverse drug effects and psychiatricdisorders. Possible medical causes include cardiores-piratory or metabolic disturbances and infections [8].
The evaluation of gait disorders includes the care-ful clinical observation of gait and a neurological andorthopedic examination based on the patient history,all of which guide the choice of ancillary diagnosticprocedures if required and appropriate. This reviewis intended to be a guide for clinicians on the physi-ological basis of gait, the clinical examination and ontypical causes of gait disorders.
Physiological basis of gait
For normal gait all of the following functions and sys-tems are required to be intact: locomotor function (forinitiating and sustaining rhythmic gait), balance, pos-tural reflexes, sensory function and sensorimotor inte-gration, motor control, the musculoskeletal apparatusand cardiopulmonary functions. Afferent nerves fromthe visual, vestibular and proprioceptive systems pro-vide essential information on the position of the bodyand its parts. Disturbances in one of these systems,e. g. proprioception, may be partially compensated byother sensory systems, such as vision. A centrally inte-grating system, which involves areas in the frontal cor-tex, the basal ganglia, the brain stem and the cerebel-lum, interprets the information received and selects
82 Gait disorders in adults and the elderly K

review article
Table 1 Parameters for theclinical examinationof gait
Sitting unaided
Standing up from a sitting position (unaided and with/without use of upperlimbs)
Posture (trunk, neck and head, upright, bent or asymmetrical)
Stance (narrow/wide base)
Gait initiation (blockage)
Walking (smooth, stiff, insecure, symmetrical, limping)
Step length, lifting of feet, contact with ground, wide/narrow base
Speed
Arm swing
Freezing
Turning
Postural reflexes (pull or push test)
Sitting down (“motor recklessness”)
Complex tests of stance and gait
Tandem stance
Tandem gait
Romberg’s test (standing with eyes closed and narrow base)
Blind gait
Walking backwards
Walking fast
Walking slowly (in a deliberate manner)
Running
Turning quickly
Turning on the spot
Unterberger’s test (walking on the spot with eyes closed)
Standing and walking on heels
Standing and walking on toes
Hopping on one foot
Dual task maneuver (walking while talking or carrying objects)
Functional reach
Table 2 Classificationof fall syndromes (modified fromNutt [31])
Type Causes
Collapsing
– Atonic seizure, negative my-oclonus, cataplexy
– Syncope Orthostatic hypotension and others
Tonic (“falling like a log”)
– While standing PSP, thalamic astasia, tonic seizure
– On changing posture/position Parkinson’s disease (PD)
Tripping Weak foot extensors, spasticity, PD
Freezing PD, frontal gait disorder
No specific pattern Attention deficit, dementia
PSP progressive supranuclear palsy; PD Parkinson’s disease
the motor programs required for walking. The effer-ent system comprises descending pathways includingthe pyramidal tract, peripheral nerves, neuromuscu-lar end plate and muscles. To some degree, rhythmicgait can also be sustained by spinal centers, resultingin spinal gait patterns in paraplegic patients while de-vices support them against gravity. In primates, brain
stem centers have a central role in generating auto-matic walking, in particular the so-called midbrainlocomotor center, which includes the pedunculopon-tine nucleus [9].
Initiating gait requires a stable upright body posi-tion. Functioning postural reflexes are necessary toassume and sustain a stable body position. To startwalking, one leg is raised and directed forward by flex-ing the hips and knee. Activation of the supportingcontralateral leg and trunk muscles moves the body’scenter of gravity over the weight-bearing leg and for-ward. The heel of the swinging leg is then placedon the ground. The body weight is gradually shiftedto the sole and then onwards to the toes. Duringmid-stance, the opposite leg is lifted and moves for-ward until the heel strikes the ground. Meanwhile, thebody is held upright, the shoulders and pelvis remainrelatively level and each arm swings in the directionopposite to that of its ipsilateral leg. The gait cycle(Fig. 1) is divided into the stance and swing phase.The stance phase constitutes approximately 60% ofthe gait cycle and is subdivided into initial contact(heel strike), loading response, mid-stance, terminalstance and pre-swing. Both feet are on the groundat the beginning and end of the stance phase. Eachof these two double support periods lasts for approx-imately 10–12% of the gait cycle. The swing phasetakes up about 40% of the gait cycle and is subdividedinto initial swing (toe-off), mid-swing (tibia vertical)and terminal swing, terminated by the heel strikingthe ground [9, 10].
Important measures of gait (Fig. 2) include walkingspeed, cadence (number of steps per unit of time),walking base width (measured from midpoint to mid-point of both heels), step length (measured from thepoint of foot contact to the point of contralateral footcontact) and stride length (linear distance coveredby one gait cycle). The preferred walking speed inhealthy adults up to the age of 59 years is approxi-mately 1.4 m/s [11]. Average stride lengths in healthyadults range between 150 and 170 cm. The averagecadence in young adults was reported to range be-tween 115 and 120 steps/min. Ageing is associatedwith a decline in gait speed and step length whereascadence remains relatively stable. Elderly subjectsprefer a 40% wider step width than young persons(average step width in elderly women approximately8 cm and in elderly men 10 cm) [12].
Role of cognition
Investigations over the past two decades have demon-strated the strong effects of cognition on gait [13],including the role of gait speed and gait disordersin older age as an indicator for the future develop-ment of dementia and of life expectancy [4–6]. Cogni-tive control is relevant for circumnavigating obstaclesand for choosing the optimal route. Frontal execu-tive functions, visuospatial perception and attention
K Gait disorders in adults and the elderly 83

review article
Table 3 Risk factors for falls
Female gender, low body weight, age >80 years
Number of falls in previous year/month
Use of sedatives, particularly with long half-life
Limited physical activity
Difficulties rising from sitting position
Reduced muscle strength in the lower limbs
Impaired balance Standing
Walking
Turning
Impaired postural reflexes
Impaired vision
Impaired cognitive functions, depression, anxiety
Table 4 Generalmeasures toprevent falls and fall-relatedinjuries
Check entire list of medication
Avoid sedatives, particularly with long half-life
Avoid (classical) neuroleptics and tricyclic antidepressants
Check the indications for and dose of atypical neuroleptics
Increase physical activity
Healthy diet, avoid malnutrition and overweight
Muscle training
Balance training
Anxiolytic and antidepressant therapy
Behavioral therapy for anxiety, depression and dementia
Therapy of orthostatic hypotension
Treatment for osteoporosis
Adequate footwear
Protective devices such as hip protectors
Remove risks at home and adjust personal environment
Electronic warning systems
all contribute to walking safely. Psychological factorsalso influence gait. For instance, depression is asso-ciated with slower gait and anxiety may lead to anoverly cautious gait. The role of cognition for gaitis revealed in the multitask paradigm where personsare asked to perform mental tasks while walking. El-derly persons who stop walking while talking havea significantly higher risk of falling [14]. Further in-vestigations have shown that patients with dementiawalk slowly but in relation to their motor and cog-nitive deficits, they actually walk too fast leading toan increased risk of falling [15]. In situations wherethere is a risk of falling, healthy persons adopt a pos-ture first strategy, which prioritizes the maintenanceof balance over other tasks. This strategy is lost inpatients with Parkinson’s disease [16]. These multi-ple interactions demonstrate that improving cognitivefunctioning may have an essential role in the rehabil-itation of gait disorders.
Clinical examination of gait
The clinical examination of gait provides a quick butintegrative overview of the function of the structuresinvolved in walking. It is important to observe theentire patient, from the front and from all sides, whilewalking over a distance of at least several meterswithout obstacles. If possible, walking should be ob-served without the subject wearing shoes. Normalwalking appears rhythmical, flowing, effortless, withfreely swinging legs and with an upright body pos-ture. Normal walking is accompanied by movementsof the head, the trunk and the arms (in the direc-tion opposite to the movement of each leg). Table 1summarizes the parameters that should be clinicallyexamined, which include step length, stride length,step width, rhythm, speed, posture, swinging of armsand legs and the duration and type of contact withthe floor [13].
Semiquantitative methods of gait assessment maybe applied for diagnostic purposes (e. g. spinal tap testwhen normal pressure hydrocephalus is suspected)and to evaluate therapies. Examples include measur-ing the freely chosen and the maximum speed overa defined distance, such as 10 m using a stop watch.The number of steps taken over that distance can alsobe counted [17]. The timed up and go (TUG) test isa simple assessment developed to evaluate the risk offalling in geriatric patients: measured as the time thata patient requires to stand up from a chair with armrests, walk 3 m (using usual walking aids if necessary),turn around, walk back and sit back down [18].
A general neurological assessment should alwaysfollow the evaluation of gait. Nearly all componentsof the clinical neurological examination may provideadditional information, which may help in the classi-fication of a gait disorder. It is advisable to performthe examination with most of the patient’s clothes re-moved, if possible. This also helps with the evaluationof any orthopedic abnormalities. The patient shouldbe inspected from all sides while standing still. Thisallows detection of asymmetries, postural abnormali-ties, differences in leg length and axial or other defor-mities. Orthopedic disturbances are frequently asso-ciated with asymmetrical gait patterns (limping). Insome cases, ophthalmological and medical examina-tions are useful to assess cardiorespiratory functionand orthostatic blood pressure regulation or to per-form angiological tests. An otological or neuro-otolog-ical assessment may be required if a vestibular causeof a gait disorder is suspected. The subject historymust include questions on any neurological, ortho-pedic and medical symptoms or prior history, patientmedication and detailed questioning with respect toany falls. Maximum walking distance, the number ofrests needed to cover that distance, limiting factors,such as pain or shortness of breath as well as the useof walking aids should be documented.
84 Gait disorders in adults and the elderly K

review article
Table 5 Phenomenological classificationof gait disorders(modified fromRuzicka andJankovic [9])
Gait disorder Characteristics
Hemispastic gait Unilateral extension and circumduc-tion
Paraspastic gait Bilateral extension and adduction,stiff
Ataxic gait Broad base, lack of coordination
Sensory ataxic gait Cautious, worsening without visualinput
Cautious gait Broad based, cautious, slow, anx-ious
Freezing gait Blockage, e. g. on turning
Propulsive gait Centre of gravity in front of body,festination
Astasia Primary impairment of stance/balance
Dystonic gait Abnormal posture of foot/leg
Choreatic gait Irregular, dance-like, broad-based
Steppage gait Weakness of foot extensors
Waddling gait Broad-based, swaying, drop ofswinging leg
Antalgic gait Shortened stance phase on affectedside
Vertiginous gait Insecure, tendency to fall to oneside
Psychogenic gait disorder Bizarre, rarely falls
History and classification of falls
In elderly persons, pre-existing difficulties with walk-ing and balance are more commonly the cause of fallsthan acute disturbances, such as syncope, seizures orstroke [19]. Almost one third of all persons over theage of 65 years fall every year and more than half ofthose fall more than once. Approximately 10–15% ofthese falls lead to serious injuries, such as traumaticbrain injury or hip fractures. It has been estimatedthat inadvertent injuries are the fifth most commoncause of death in elderly persons [3]. Persons at riskshould be questioned about the type and frequency offalls and any symptoms prior to or following falls. Fac-tors that might precipitate falls in the home includeloose carpets on wooden floors. A precise history ofthe patient’s medication is essential, in particular withrespect to drugs with sedating or blood pressure low-ering effects, such as tricyclic antidepressants, seda-tives, anxiolytics, neuroleptics and antihypertensivedrugs [13, 20]. Polypharmacy is regarded as an im-portant risk factor for falls in the elderly; however,newer studies suggest that polypharmacy only posesa risk if it includes medications that increase the riskfor falls, such as sedatives, antidepressants and ben-zodiazepines [21, 22]. Table 2 shows a phenomeno-logical classification of falls, which may assist in theetiological classification. Table 3 summarizes relevantrisk factors for falls and Table 4 shows general mea-sures recommended for the prevention of falls andfall-related injuries. For further reading on the topic
of falls we refer to the excellent reviews by Bloem andhis group [20, 23, 24].
Protective strategies and age-related changes ofgait
Even in healthy persons, any suspected or actualthreat to balance induces changes in the strategiesfor standing and walking: the stance and gait baseis widened, bipedal floor contact is prolonged, steplength becomes shorter, the feet are lifted less highduring the swing phase, walking becomes slower andthe posture becomes stooped. A typical examplewhere this may occur in healthy persons is walkingon icy ground or on a slippery floor [9]. The fearof falling and the actual risk of falling increase withage. Older persons are therefore more likely to usethese protective gait strategies. As muscle powerdiminishes and proprioception and vision becomeimpaired with age, body sway on standing, which isconstantly present to a slight degree, increases. Inyounger persons this sway can be compensated byactivating the muscle groups around the upper anklejoints. Older persons shift this compensation to theproximal muscle groups around the hips due to lossof distal proprioception. This requires an increasedreliance on vestibular afferents, which undergo lesschange during the ageing process.
The preferred walking speed in apparently healthyelderly subjects declines by 1% per year from a meanof 1.3 m/s in the seventh decade to a mean of 0.95 m/sin those aged over 80 years [11]. The decline in walk-ing speed is caused by a decrease in step length ratherthan by a change in cadence [25]. Although these gaitchanges are to some degree a consequence of normalageing, individual walking speed in elderly subjects isa strong indicator of general health and survival [4].
Epidemiology and classification of gait disorders
The Bruneck study, in which a representative sampleof the population of a small region in northern Italy isbeing followed longitudinally, has provided valuableepidemiological data on various gait disorders in 488persons: between the ages of 60 and 97 years one thirdof this population had a gait disorder, with a markedincrease in prevalence with age, between the ages of60 and 69 years, the prevalence was 10% and in thoseover 80 years it was >60% [2]. In two thirds of thoseaffected by any gait disorder, the cause was neurologi-cal and in approximately one half, the cause was non-neurological, indicating that there was a considerableoverlap of patients affected by neurological as well asby non-neurological gait disorders. Among the neuro-logical causes, sensory ataxia (18%) and parkinsonian(16%) gait disorders were the most common, followedby frontal (8%), cerebellar ataxic gait disorders, cau-tious gait and hypotonic paretic, spastic, vestibularand dyskinetic gait disorders. In approximately one
K Gait disorders in adults and the elderly 85

review article
Fig. 3 Graphic represen-tationof the step sequenceinclassical gait disorders.anormal gait,b spasticparapareticgait,ccerebellarataxic gait,dparkinso-niangait ande frontal gait.Notenarrowstepwidthandinwards rotation inpara-spastic gait, broadenedbaseandmarked irregularityin cerebellar gait, shortenedandmildly irregular steplength inparkinsoniangaitandbroad-based, short-stepped, irregularwalking infrontal gait disorder
third of the patients the gait disorder was due to morethan one neurological cause, making a precise classifi-cation difficult [2]. It has to be pointed out that theseprevalence rates refer to elderly people living in thecommunity. Substantially higher rates of gait disor-ders are to be expected among geriatric hospital andnursing home residents [3].
Table 5 shows a phenomenological classification ofcommon gait disorders. Here we use a more hierar-chical, clinicoanatomical classification and differen-tiate gait disorders due to musculoskeletal (orthope-dic), neuromuscular (peripheral neurological), spinaland brain disorders. Fig. 3 features a graphic repre-sentation of the step sequence in normal gait and insome important gait disorders.
Musculoskeletal gait disorders
Osteoarthritis and skeletal deformities of the lower ex-tremities are the most common reasons for non-neu-rological gait disorders in adults [2]. The resulting or-thopedic gait disturbances may be characterized bya limited range of motion, avoidance of weight-bear-ing and asymmetry or limping.
Antalgic gait
To avoid pain weight is put on the affected leg foras short a time as possible, resulting in a limp. Thepatients appear to be walking as if there were a thornin the sole of the foot. To reduce the load on theaffected leg the patients lift and lower their foot ina fixed ankle position. Walking aids, such as crutchesare carried on the unaffected side in order to shiftweight away from the affected side and to the upperextremity. Typical causes are painful conditions in thelower extremities, such as knee osteoarthritis, anklesprains and stress fractures of the foot [10].
Coxalgic gait
In patients with hip pain the upper trunk is typicallyshifted towards the affected side during the stancephase on the affected leg. This is an unconsciousadaptive maneuver which reduces the forces exertedon the affected hip during the stance phase. In con-trast to the Duchenne sign as a consequence of glu-teus medius muscle weakness (see waddling gait), thecontralateral hemipelvis does not drop but remainslevel during the stance phase of the affected side [10].
86 Gait disorders in adults and the elderly K
review article
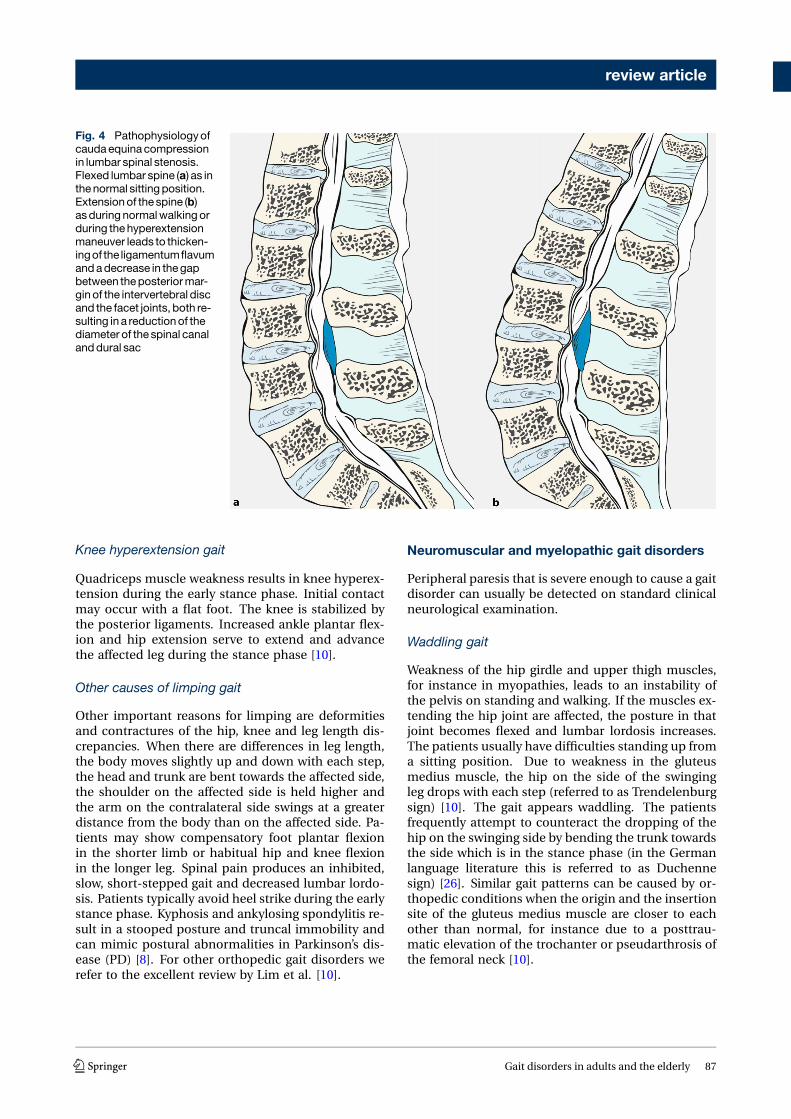
Fig. 4 Pathophysiologyofcaudaequinacompressionin lumbar spinal stenosis.Flexed lumbar spine (a) as inthenormal sittingposition.Extensionof the spine (b)asduring normalwalkingorduring thehyperextensionmaneuver leads to thicken-ingof the ligamentumflavumandadecrease in thegapbetween theposteriormar-ginof the intervertebral discand the facet joints, both re-sulting in a reductionof thediameter of the spinal canalanddural sac
Knee hyperextension gait
Quadriceps muscle weakness results in knee hyperex-tension during the early stance phase. Initial contactmay occur with a flat foot. The knee is stabilized bythe posterior ligaments. Increased ankle plantar flex-ion and hip extension serve to extend and advancethe affected leg during the stance phase [10].
Other causes of limping gait
Other important reasons for limping are deformitiesand contractures of the hip, knee and leg length dis-crepancies. When there are differences in leg length,the body moves slightly up and down with each step,the head and trunk are bent towards the affected side,the shoulder on the affected side is held higher andthe arm on the contralateral side swings at a greaterdistance from the body than on the affected side. Pa-tients may show compensatory foot plantar flexionin the shorter limb or habitual hip and knee flexionin the longer leg. Spinal pain produces an inhibited,slow, short-stepped gait and decreased lumbar lordo-sis. Patients typically avoid heel strike during the earlystance phase. Kyphosis and ankylosing spondylitis re-sult in a stooped posture and truncal immobility andcan mimic postural abnormalities in Parkinson’s dis-ease (PD) [8]. For other orthopedic gait disorders werefer to the excellent review by Lim et al. [10].
Neuromuscular and myelopathic gait disorders
Peripheral paresis that is severe enough to cause a gaitdisorder can usually be detected on standard clinicalneurological examination.
Waddling gait
Weakness of the hip girdle and upper thigh muscles,for instance in myopathies, leads to an instability ofthe pelvis on standing and walking. If the muscles ex-tending the hip joint are affected, the posture in thatjoint becomes flexed and lumbar lordosis increases.The patients usually have difficulties standing up froma sitting position. Due to weakness in the gluteusmedius muscle, the hip on the side of the swingingleg drops with each step (referred to as Trendelenburgsign) [10]. The gait appears waddling. The patientsfrequently attempt to counteract the dropping of thehip on the swinging side by bending the trunk towardsthe side which is in the stance phase (in the Germanlanguage literature this is referred to as Duchennesign) [26]. Similar gait patterns can be caused by or-thopedic conditions when the origin and the insertionsite of the gluteus medius muscle are closer to eachother than normal, for instance due to a posttrau-matic elevation of the trochanter or pseudarthrosis ofthe femoral neck [10].
K Gait disorders in adults and the elderly 87

review article
Steppage gait
When the muscles that lift the foot are paretic thepatient must lift the leg higher than usual during theswing phase. The resulting gait pattern is referred to assteppage gait. Patients are unable to stand or walk ontheir heels. Peroneal splints and orthopedic footwearare usually helpful. Patients with pareses of the plan-tar flexors muscles cannot flex the foot at the end ofthe stance phase. They cannot perform toe walking[9].
Neurogenic and intermittent claudication
Intermittent claudication is a symptom of peripheralarterial occlusive disease. After having walked overa distance which is individually characteristic, the pa-tients experience pain or cramps in the calves, feet orthighs which typically subsides on standing still.
Lumbar spinal stenosis and neurogenic claudicationLumbar spinal stenoses may induce symptoms fol-lowing an individually typical latency on standing orwhen walking due to swelling of the cauda equina,which leads to compression. This is referred to as neu-rogenic claudication. The symptoms of lumbar spinalstenosis can be explained by an increase in lumbarlordosis and spinal canal stenosis in an upright posi-tion compared to the sitting position (Fig. 4, [27]) or ifspondylolisthesis is present by a shift of the vertebraewhile standing and walking. Following an individu-ally characteristic distance, walking becomes associ-ated with deep muscular pain and with neurologicaldeficits, such as sensory deficits and paresis in thelower limbs, which resolve within minutes when theaffected person sits or lies down. Activities performedin a flexed posture, such as cycling often cause lessproblems than walking. For the same reason, walkinguphill may be tolerated better than walking downhill.Clinical neurological examination at rest may be en-tirely normal but there is usually pain on hyperexten-sion of the lumbar spine [10].
Non-surgical treatment includes training how to liftthe pelvis while standing and walking or corsets tocounteract lordosis. Frequently these measures are oflimited value and often surgical decompression is theonly effective treatment [28].
Myelopathic gait
Cervical spondylotic myelopathy is a relatively com-mon cause of gait disturbance in the elderly [3]. De-generative osteophytes and ligamentous hypertrophylead to narrowing of the spinal canal and mechanicalcompression of the cervical spinal cord. Gait and bal-ance problems are the main clinical manifestations.The gait is stiff and paraparetic spastic but may alsobe spastic ataxic due to dorsal column dysfunction.Cervical pain, upper limb sensory symptoms and loss
of dexterity are common but may be absent in a mi-nority of affected patients. In severe cases, urinaryurgency may occur. Compressive cervical myelopathytends to be progressive and surgical decompressionshould be considered in symptomatic cases [29].
Gait disorders associated with brain dysfunction
This category encompasses all gait disorders related tobrain disease or dysfunction, i. e. the neurological gaitdisorders in a narrower sense. It largely overlaps withthe categories ofmiddle and higher level gait disordersin the classification proposed by Nutt et al. [30–32];however, some middle level gait disorders, such asspastic gait may also be caused by spinal lesions.
Cautious gait
Cautious gait (sometimes termed senile gait) refers toan excessive degree of age-related changes in walk-ing and fear of falling. The walking difficulties seemout of proportion when considering the patient’s ac-tual sensory or motor deficits. The gait appears slow,with a wider base than normal, reduced arm swingbilaterally and a slightly stooped posture. This type ofgait change often occurs after the first time a patienthas fallen. Without treatment, excessively cautiousgait may lead to considerable handicap. Phobic gaitdisorder can be considered the maximum variant ofcautious gait: these patients suffer from excessive fearof falling of which they are aware and which may re-sult in a complete inability to walk. Gait may improveeven with very slight support, such as another persontouching the patient’s hand. Some patients respondto gait and balance training and anxiolytics [9].
Spastic gait disorders
Spastic hemiparetic gaitSpastic hemiparesis is characterized by a dominanceof the tonus in the upper limb flexor muscles: thearm is held in an adducted posture and is bent androtated inwards, the forearm is pronated and the handand the fingers are flexed. The leg is slightly bent atthe hip, the knee cannot be extended fully at the endof the stance phase and the foot is inverted and ina plantar flexed position. Gait is slow, with a wide baseand asymmetrical with a shortened weight-bearingphase on the paretic side. During the swing phase, theparetic leg performs a lateral movement (circumduc-tion) which is characteristic of this gait disorder, alsotermed Wernicke-Mann gait. Spastic gait problemstypically worsen on attempts to walk faster. Treat-ment mainly consists of physiotherapy although insome cases local botulinum toxin injections may behelpful.
88 Gait disorders in adults and the elderly K

review article
Spastic paraparetic gaitIn paraspastic gait, the legs are usually slightly bent atthe hip and in an adducted position. The knees areextended or slightly bent and the feet are in a plantarflexion position. This posture requires circumductionof the legs during walking. The gait may appear stiff(spastic gait disorder) or stiff as well as insecure (spas-tic ataxic gait disorder). In spastic paraparetic gait,each leg appears to be dragged forward. If the muscletone in the adductors is marked, the resulting gait dis-order is referred to as scissor gait. Treatment optionsinclude physiotherapy and medication with a musclerelaxing effect, such as baclofen and tizanidine. Inselected cases, botulinum toxin injections may helpalleviate spasticity and improve motor function [9].
Ataxic gait disorders
Cerebellar ataxic gaitCerebellar ataxia and sensory ataxia can be distin-guished based on clinical characteristics. In sensoryataxia, the loss of proprioception may partially becompensated by visual input. In contrast, this is notthe case in cerebellar ataxia; therefore, standing stillwith a narrow stance base (Romberg’s test) and walk-ing with closed eyes lead to a worsening of imbalancein sensory ataxia, whereas these tests reveal less differ-ence in cerebellar ataxia. In cerebellar ataxia, stanceand gait appear broad based, insecure and wobbly.Leg movements and step length are irregular andvariable. The ataxia increases on turning and duringcomplex gait tests, such as tandem walk and walkingon uneven surfaces. Gait initiation is usually normal.The patients attempt to compensate lateral body swayby walking cautiously, stooping slightly and steadyingthe stance foot by bending at the hip. The causes ofcerebellar disease may be vascular, toxic (e. g. alco-hol), degenerative (e. g. hereditary cerebellar ataxias),inflammatory (e. g. multiple sclerosis) or neoplas-tic. The pathomechanism includes disturbances ofbalance and motor coordination. Studies in humanswith cerebellar lesions have convincingly demon-strated that cerebellar gait ataxia is more closelyrelated to balance than to leg placement deficits [33].Control of balance is predominantly localized in thevermis region of the cerebellum. The intermediaryzone or paravermal structures are important for thecontrol of the timing and amplitude of targeted limbmovements; however, the cerebellar hemispheres arealso involved in the control of bipedal human gait[34]. Unilateral lesions of the cerebellar hemispheresinduce ipsilateral limb ataxia. Isolated lesions of thevermis or the paravermal structures may cause gaitataxia without affecting the limbs. In some patientswith cerebellar disease, postural innervation is asso-ciated with slow oscillations of the entire body or thehead (titubation).
Sensory ataxic gaitDisturbances of proprioceptive function may occur insensory polyneuropathy or dorsal column lesions. Insensory ataxia, stance and gait appear broad basedand insecure. The step length is shortened. Gaitis slower and more cautious compared to cerebellarataxia. The feet are sometimes lifted high and gaitmay have a stomping quality. The patients use visualcontrol to compensate for the loss of proprioception.Consequently, loss of visual function causes markedworsening of ataxia. This may become evident duringclinical testing (Romberg’s test, walking with closedeyes), walking in darkness or a sudden disturbance ofvision (e. g. due to acute ischemic optic neuropathyif the contralateral eye has pre-existing impaired vi-sion). Ataxic gait and the associated risk of falling arealso worsened if circumstances require a slower gait,e. g. unknown territory or obstacles [35]. As in cere-bellar ataxia, complex clinical tests including tandemwalk and walking on uneven surfaces increase inse-curity in sensory ataxic gait. Some hereditary ataxiasmay cause both cerebellar and sensory type ataxia dueto a combination of cerebellar disease and sensoryneuropathy or a dorsal column lesion. Examples in-clude spinocerebellar ataxias that are associated withpolyneuropathy. Treatment should target the under-lying cause if possible. Physiotherapy including gaitand balance training should be offered although theeffect of this approach is often limited. Walking aidsappropriate for each disease stage need to be consid-ered.
Frontal gait disorder/higher level gait disorders
Frontal gait disorders are common in older age. Theymay lead to a misdiagnosis of Parkinson’s disease(PD), particularly if tremor (of any cause) is alsopresent. These gait problems may however also occurin younger patients who have frontal lesions. Variousterms for this type of gait disorder have been usedin the literature, including frontal gait ataxia, gaitapraxia, magnetic apraxia, lower body parkinsonismand marche à petits pas, all of which describe thesame clinical syndrome [9].
Nutt, Marsden and Thompson coined the terms“highest” or “higher level gait disorder” in 1993 [30].This comprises all gait or balance problems whichare not explained by peripheral (motor and sensory),pyramidal, cerebellar of basal ganglia lesions. Thisgroup of gait disorders includes frontal as well assenile gait disorder (cautious gait), subcortical andfrontal balance impairment (subcortical/frontal dis-equilibrium) and isolated gait ignition failure. Mag-netic resonance imaging (MRI) studies have shownthat this group of gait disorders may be caused byfrontal as well as parietal lesions [36]. Further causesinclude lesions in the corpus callosum, which mayinduce gait problems by disrupting interhemisphericcommunication [37]. A recent imaging study sug-
K Gait disorders in adults and the elderly 89

review article
gested that balance and gait problems in patientswith higher level gait disorders are associated withgrey matter atrophy in the midbrain and caused bydysfunction in a network linking the primary mo-tor cortex with the midbrain locomotor region [38].These novel clinico-anatomical findings seem to jus-tify the use of the term “higher level gait disorders”,although this concept has been criticized by someauthors for its complexity [25, 39]. In clinical practicethe term “frontal gait disorder” remains in commonuse. Common causes of frontal gait disorders includevascular lesions (e.g. white matter and basal ganglialacunar infarction and territorial infarction in the an-terior cerebral artery territory). In normal pressurehydrocephalus, clinical problems which may emergein association with the typical gait disorder are blad-der problems and cognitive deficits. Further causesinclude advanced Alzheimer’s disease, frontotempo-ral lobar degeneration and space occupying lesionsof the frontal lobe. Patients with frontal gait disordersfrequently appear to have forgotten how to performthe act of walking. They have difficulties standing up,inadequately adapt the posture when changing posi-tion (for instance, they may extend rather than bendthe trunk and legs on attempting to stand up) andhave difficulties achieving a stable position. The gaithas a broad base, step length is short and they appearanxious. The arms may be extended laterally andarm swing may be reduced. Trunk posture may bestooped, upright or even hyperextended. Inhibitionof gait initiation is common and is the only symp-tom in isolated gait ignition failure. Some patientsattempt to initiate gait by swaying the trunk laterallyor performing exaggerated arm movements. Walkingappears to present great difficulty and is shuffling,the feet may appear glued to the ground (“magneticfeet”). In other cases, patients seem to be scufflingtheir feet. After having walked a few meters, gait of-ten improves. Blocked gait or freezing episodes mayoccur, particularly on turning and when faced withobstacles such as thresholds. Balance and posturalstability are impaired. In some patients, retropulsionoccurs which may lead to backward falls.
There is a marked discrepancy between the severityof a patient’s gait difficulties and the moderate impair-ment in a sitting or supine position. Many patients arecapable of performing regular, rapid stepping move-ments while in a sitting position. Conversely, mildrigidity, gegenhalten and bradykinesia are commonlyfound, predominantly in the lower limbs, hence theterm lower body parkinsonism [40]. Depending onthe etiology, patients may have increased deep ten-don reflexes or positive pyramidal tract signs, signsof pseudobulbar palsy (e.g. dysarthria, dysphagia),frontal release signs (e.g. snout or grasp reflex) orcognitive changes including dementia. In some cases,causal treatment is available, such as shunting in nor-mal pressure hydrocephalus and treatment of vascularrisk factors; however, in most cases physiotherapy in-
cluding gait training is the only option, often with lim-ited permanent effects. Rhythmic acoustic or visualsignals, which may be employed in PD are rarely ef-fective. There is no evidence of efficacy of antiparkin-sonian drugs, including levodopa, although they maybe worth trying in cases with clinical parkinsonism.
Parkinsonian gait (rigid akinetic gait disorder)
The cardinal motor signs of PD are bradykinesia, rigid-ity, rest tremor and impaired postural stability. In themajority of patients, the symptoms initially affect onlyone side of the body and spread to the other side. Evenat very early stages of the illness, walking frequentlyappears somewhat slow. In hemiparkinsonism, phys-iological arm swing is reduced and the leg may beslightly dragged on the affected side. As the diseaseprogresses, the typical rigid akinetic gait impairmentdevelops, which includes slow gait with a short steplength, a narrow base and a stooped posture involv-ing neck, shoulders and trunk. Arm swing is reducedand in more advanced stages the arms are held in anadducted and bent position. The feet are lifted lesshigh than normally, which may lead to shuffling gait.The step to step variability of the gait cycle increases.When asked to walk faster, patients increase the stepfrequency rather than step length. Performing othertasks simultaneously, such as walking while talking,worsens the gait. Commonly, patients with PD find iteasier to climb up stairs than to walk on a level sur-face. Standing up from a sitting position is impaired,which becomes apparent when patients are asked torise without using the arms. Many patients developa propensity to lean forward while walking, associatedwith increased step frequency, reduced stride lengthand bent truncal posture. This particular gait patternin PD is referred to as festination and carries a risk offorward falls. Impaired postural reflexes are a domi-nant cause of falls in PD and are apparent on perform-ing the pull or push test. Changing position becomesdifficult as axial bradykinesia increases. Patients turnen bloc using many small steps.
FreezingDifficulties with gait initiation and freezing typicallyoccur on turning or when approaching obstacles ornarrow passages such as doors. In some PD patientsfreezing develops at a very early stage and resolvesafter starting antiparkinsonian medication. In PDpatients with motor fluctuations freezing is usuallylinked to periods with loss of levodopa response (OFFphases). As the disease progresses, however, freezingmay become resistant to levodopa and may occurduring periods of otherwise good levodopa response(ON phases). Rarely, freezing may improve overnightas the effect of dopaminergic medication wears off,suggesting a causal role of dopaminergic drugs [41].There are three phenomenologically distinct typesof freezing: the purely akinetic form is rare and is
90 Gait disorders in adults and the elderly K

review article
characterized by start failure or a complete stop whilewalking, the second type involves shuffling on thespot and the third an insufficient shuffling with verysmall steps [42].
Management of parkinsonian gait difficultiesThe gait disorder and to a lesser degree the postu-ral instability of PD often respond to antiparkinso-nian medication; however, levodopa and particularlydopamine agonists may contribute to an existing or-thostatic hypotension and thereby may make walkingmore insecure. Management includes modificationof the antiparkinsonian medication, medical andnon-medical treatment of orthostatic hypotension,cholinesterase inhibitors in patients with cognitiveimpairment and physiotherapy. Walking aids, such as4-wheel walkers with brakes, may be helpful. In freez-ing, improvements in overcoming the blockages cansometimes be achieved by using rhythmical acousticsignals (e.g. counting and clapping) or visual impulses(e.g. horizontal stripes attached to or painted on thefloor in spots where freezing typically occurs at homeor holding a walking stick upside down in front of thefoot). A new technique is the use of a stick projectinga laser line on the floor to step over [43]. These trickstend to be more effective while they represent novelstimuli. Cognitive strategies may also be helpful, suchas directing one’s attention to each individual steprather than the act of walking as such, consciouslyattempting to make individual large steps or mentallycounting [41]. Surgery for PD (mainly deep brainstimulation) usually improves only those aspects ofgait and posture that are associated with motor fluc-tuations and dyskinesia and which are responsive tolevodopa.
Other conditions associated with rigid akinetic gaitdisorderIn PD a marked rigid akinetic gait disorder with clin-ically relevant postural instability usually occurs inadvanced disease stages. If these problems presentearly into the disease course or on presentation, thediagnosis should be carefully re-evaluated. In thesecases, possible causes include old age or a longerdisease duration than realized by the patients, e. g. ifthey attributed the general slowing to the ageing pro-cess. Comorbidities may be present, such as vascularencephalopathy, sensory ataxic gait disorder due topolyneuropathy or spasticity due to cervical myelopa-thy. Other differential diagnoses include frontal gaitand secondary parkinsonian syndromes, in particularvascular parkinsonism. The atypical parkinsoniansyndromes, such as multiple system atrophy (MSA)and progressive supranuclear palsy (PSP) typicallylead to early problems with balance and gait. Theseneurodegenerative conditions respond less well todopaminergic therapy than PD and have a morerapid disease course.
Multiple system atrophy (MSA). Patients with MSAoften have combined parkinsonism and cerebellarsigns, resulting in a gait disorder that is rigid akineticas well as ataxic. Orthostatic dysregulation may con-tribute to the difficulties in walking, even in earlydisease stages. Postural abnormalities in MSA maybe severe and may further impair gait. These includea marked forward flexion of the neck (disproportion-ate antecollis), and a forward or pronounced lateralflexion of the trunk termed Pisa syndrome. Camp-tocormia is a massive forward flexion of the trunkon standing or sitting which completely resolves ina supine position. Camptocormia may also occur inPD.
Progressive supranuclear palsy (PSP). Patients withPSP typically fall during the first year of the illnessand this frequently happens backwards. Posture tendsto be upright rather than bent forward and the neckmay be hyperextended (retrocollis). Gait may be rigidakinetic as in PD but is more typically broad based.Many patients with PSP tend to fling the legs forwardin an uncontrolled manner while walking and to turnaround abruptly. Similarly, sitting down is typically anabrupt movement and appears as if the patients wouldlet themselves fall onto the chair. These changes inmotor control have been termed motor recklessness.The cardinal symptoms of the classical clinical type ofPSP (also termed Richardson syndrome) are predom-inantly axial parkinsonism and restrictions in verticalgaze range. Another relevant clinical manifestation ispure akinesia with freezing gait, predominantly withgait impairment and freezing [44].
Patients with atypical parkinsonian syndromesshould primarily receive levodopa and if well-toler-ated, high doses should be tried. Response is usuallymodest in MSA and poor in PSP. Physiotherapy shouldinclude gait training and the adaptation of appropri-ate walking aids and protection from falls.
Dystonic gait disorder
Primary generalized dystonias have a usual onset inchildhood and in early adulthood. Secondary dysto-nias affecting gait may also occur in adulthood andinclude toxic or hypoxic basal ganglia damage andtardive dystonia following long-term treatment withdopamine receptor blocking drugs. Moreover, PDmaybe associated with dystonic OFF symptoms as well asdystonia as part of levodopa-induced dyskinesia.
Dystonic gait disorders frequently appear bizarre,particularly because activity increases dystonic tonusand posture. The abnormal posture of the foot indystonic gait typically involves inversion, plantar flex-ion and tonic extension of the big toe. In many pa-tients complex types of walking, such as walking back-wards and running are paradoxically less impairedthan walking forward and may seem completely unaf-fected. Sensory tricks, e. g. resting one’s hand on one’sneck, may improve or even normalize dystonic gait
K Gait disorders in adults and the elderly 91

review article
in some patients, all of which may lead to confusionwith a psychogenic gait disorder.
Choreatic gait disorder
Huntington’s disease has an autosomal dominant in-heritance pattern and may become manifest at anyage. It is characterized by cognitive decline and psy-chiatric disturbance and the choreatic movement dis-order also affects the patients’ gait. Choreatic gait dis-orders may also occur in levodopa-induced dyskinesiain PD, in tardive dyskinesia and, less frequently, withhypoxic lesions in the basal ganglia, e. g. following car-diopulmonary bypass surgery (“post pump” chorea).Typical choreatic gait is impaired by sudden involun-tary movements affecting knee and hip flexion and itappears irregular, dance-like and swaying. There ismarked variability in step length and direction. Tocompensate for these intrusive movements, patientswiden the stance base and walk more slowly. Fallstypically occur only in severe cases. Tardive dyski-nesia and levodopa-induced dyskinesia may appearstereotypical or bizarre.
Myoclonic gait disorder
Myoclonus consist of short-lasting, involuntary jerkswhich result in the movement of a joint (positive my-oclonus) or with sudden loss of muscle tone (negativemyoclonus). Myoclonus of the trunk and the lowerlimbs may cause gait difficulties and insecurity onstanding up, sudden giving way of the hips and kneesand falls. A typical cause of this clinical syndrome inolder age groups is generalized cerebral ischemia orhypoxia.
Orthostatic tremor
Orthostatic tremor is a rare neurological disorderwhich may greatly affect the patients’ quality of lifeand may result in marked impairment. Its causeremains unidentified. While sitting or lying down,patients have entirely normal neurological findings.Once patients stand up, however, a tremor of veryhigh frequency (13–20 Hz) sets in, which is perceivedas an inability to stand and as fear of falling, ratherthan actual tremor and which is barely recognizableon inspection due to the high frequency. It mainlyaffects the muscles of the lower extremities and thetrunk and affects standing much more than walking.Falls occur but are relatively rare in relation to the pa-tients’ fear of falling. These characteristics frequentlylead to confusion with a functional disorder, witha long average latency period between disease onsetand the correct diagnosis, which further heightenspatient distress. Clonazepam shows at least mildbenefits in the majority of patients. Patients withorthostatic tremor may also benefit from propranololor gabapentin [45].
Subcortical disequilibrium (thalamic astasia)
Thalamic astasia typically occurs following unilaterallesions in the thalamus (ventrolateral or posterior nu-cleus) or in the lenticular nucleus. Infarctions andhemorrhages in these areas lead to a tendency to fallbackwards or to the contralateral side while sittingor standing, including in patients who have no rele-vant motor deficits. Although the affected patients areaware of this disturbance, they appear to ignore it andare unable to influence it. Possible associated prob-lems include motor neglect of the contralateral sideof the body or a contralateral sensory deficit. Follow-ing an acute onset, thalamic astasia usually improvesover days to months [46]. The pathomechanism of thedisturbance is probably related to the so-called pushersyndrome, which may occur in larger strokes: patientswith marked hemiparesis or hemiplegia push awayfrom the unaffected side due to an impaired subjectiveperception of the vertical in the frontal plane [47]. Le-sions of the pontomesencephalic area which involvethe pedunculopontine nucleus may cause marked im-pairment of balance and gait, with problems of gaitinitiation and irregular gait patterns.
Vestibulopathic gait
Acute vestibular disturbances lead to massive insecu-rity when standing and walking, with a propensity tofall. Acute peripheral vestibular dysfunction on oneside leads to the feeling of being pulled to the ipsilat-eral side and to falls to that side. Unilateral chronicvestibular dysfunction may cause consistent devia-tions from a straight line while walking (veering gait),which can be observed particularly well during blindgait. In patients with bilateral vestibulopathy, walk-ing may become very insecure due to lateral pulsion,vertigo and oscillopsia while walking. These prob-lems may be enhanced by reduced visual input, forinstance in dim light or by uneven surfaces. Patientswith vestibular gait disorders typically experience lessdifficulty while walking fast or running than duringslow gait [48].
Psychogenic gait disorders
In the past, the diagnosis of a psychogenic or func-tional gait disorder used to be made only once allpotential organic causes had been ruled out. Nowa-days, inconsistencies in the clinical neurological find-ings are considered the most important indicator ofa functional neurological disorder. Clinical findingsthat support the diagnosis include a lack of persis-tence of a symptom or sign and temporary completeresolution while the patient feels unobserved or is be-ing distracted by other tasks [49]. Almost any type ofgait problemmay occur. Patients may walk excessivelyslowly or show truncal trembling or jerks. Frequently,the gait appears bizarre and massively insecure. In re-
92 Gait disorders in adults and the elderly K

review article
lation to the insecurity demonstrated on examination,the patients are typically much less incapacitated inthe daily lives than expected and falls are much lesscommon. If these patients do fall, they typically donot incur injuries. Recently, effort-associated behav-ior disproportionate to the severity of gait impairment(the huffing and puffing sign) have been identified ashighly specific for functional gait disorders [50]. Otherclinical signs potentially pointing towards a functionalnature of a gait disorder are manipulation-resistantdorsiflexion of the first toe, fixed plantar flexion andinversion of one foot or both feet and the “swivel chairsign”. The latter denotes a marked discrepancy be-tween disturbed upright walking and normal forwardmotion when using a swivel chair [50].
Some organic neurological conditions, such as theneuroacanthocytosis syndromes or generalised dys-tonia, may be characterized by a bizarre walking pat-tern, which may lead to an erroneous diagnosis ofa psychogenic gait disorder. The differential diagnosesalso include cautious gait (senile gait disorder), peri-odic paralysis, episodic ataxias, paroxysmal dyskine-sia and cataplexy. Patients with functional gait disor-ders should be offered physiotherapy and psychother-apy, potentially involving suggestion, although no ap-proach has as yet been proven to be efficacious.
Conclusion
Bipedal gait is a fundamental function that deter-mines human life beyond early infancy almost asmuch as speech, higher cognitive abilities and useof complex tools. As the prevalence of gait disordersincreases with age, the number of people affected willsubstantially increase in the coming decades due tothe expected demographic changes. Gait disorderslead to a loss of personal freedom and to reducedquality of life. Gait impairments are also precursorsof falls and therefore of potentially severe injuries inelderly persons.
The causes of gait disorders include neurological,orthopedic, medical and psychiatric conditions andmultifactorial etiology becomes more common withadvancing age, making classification and manage-ment more complex. Any gait disorder should bethoroughly investigated in order to improve patientmobility and independence, to prevent falls and todetect the underlying causes as early as possible.Thorough clinical observation of gait, careful historytaking focussed on gait and falls and physical, neuro-logical and orthopedic examinations are basic stepsin the categorization of gait disorders and serve asa guide for ancillary investigations and therapeuticinterventions.
Prevention and treatment of iatrogenic, especiallymedication-induced, gait disorders are importantmeasures to reduce the burden of falls in the geriatricpopulation. Several gait disorders are amenable tospecific treatment. Levodopa is the drug of choice
for the treatment of the gait disorder of PD and insome other parkinsonian syndromes. Rare condi-tions, such as myoclonus and orthostatic tremor alsomay respond well to medication. In normal pres-sure hydrocephalus, cervical spondylotic myelopathy,lumbar spinal stenosis and hip or knee osteoarthritis,surgical treatment should be considered. Patientswith gait disorders not amenable to specific treat-ment (e. g. many neuromuscular conditions, frontalgait disorders) may benefit from multimodal reha-bilitation, gait training, use of assistive devices andfall prevention measures. Commonly used exerciseinterventions such as muscle strength, power and re-sistance training as well as coordination training canimprove habitual and maximum gait speed in elderlysubjects [51]. These exercise programs can be indi-vidualized according to the type of gait impairment,the therapist’s experience and patient’s preferences.
Acknowledgements The authors thankDoz. Franz Kralinger,Department of Trauma Surgery,Wilhelminenpital, Vienna fora critical review of the manuscript section on musculoskele-tal/orthopedic gait disorders and Mr. Daniel Maestro, Med-ical Media Service of the Medical University of Vienna, forpreparing the figures.
Conflict of interest W. Pirker and R. Katzenschlager declarethat they have no competing interests.
Open access funding provided by Medical University of Vi-enna.
Open Access This article is distributed under the terms ofthe Creative Commons Attribution 4.0 International License(http://creativecommons.org/licenses/by/4.0/), which per-mits unrestricted use, distribution, and reproduction in anymedium, provided you give appropriate credit to the origi-nal author(s) and the source, provide a link to the CreativeCommons license, and indicate if changes were made.
References
1. Ebersbach G, Sojer M, Muller J, Heijmenberg M, PoeweW. Sociocultural differences in gait. Mov Disord.2000;15(6):1145–7.
2. Mahlknecht P, Kiechl S, Bloem BR, Willeit J, Scherfler C,Gasperi A, et al. Prevalence andburdenof gait disorders inelderly men and women aged 60–97 years: a population-basedstudy. PLOSONE.2013;8(7):e69627.
3. Sudarsky L. Gait disorders: prevalence, morbidity, andetiology. AdvNeurol. 2001;87:111–7.
4. Studenski S,PereraS,PatelK,RosanoC,FaulknerK, InzitariM, et al. Gait speed and survival in older adults. JAMA.2011;305(1):50–8.
5. Mielke MM, Roberts RO, Savica R, Cha R, Drubach DI,Christianson T, et al. Assessing the temporal relationshipbetween cognition and gait: slow gait predicts cognitivedecline in theMayoClinic StudyofAging. JGerontol ABiolSciMedSci. 2013;68(8):929–37.
6. Verghese J, Annweiler C, Ayers E, Barzilai N, BeauchetO, Bennett DA, et al. Motoric cognitive risk syndrome:multicountry prevalence and dementia risk. Neurology.2014;83(8):718–26.
7. Rubenstein LZ, Solomon DH, Roth CP, Young RT, ShekellePG,Chang JT, etal. Detectionandmanagementof falls and
K Gait disorders in adults and the elderly 93

review article
instability in vulnerable elders by community physicians.JAmGeriatrSoc. 2004;52(9):1527–31.
8. Alexander NB, Goldberg A. Gait disorders: search formultiplecauses. CleveClinJMed. 2005;72(7):586.
9. Ružicka E, Jankovic JJ. Disorders of gait. In: JankovicJJ, Tolosa E, editors. Parkinson’s disease and movementdisorders, 4th edn. Philadelphia: Lippincott,WilliamsandWilkins;2002. pp.409–29.
10. Lim MR, Huang RC, Wu A, Girardi FP, Cammisa FP Jr..Evaluationoftheelderlypatientwithanabnormalgait. JAmAcadOrthopSurg. 2007;15(2):107–17.
11. Bohannon RW, Williams Andrews A. Normal walkingspeed: a descriptive meta-analysis. Physiotherapy.2011;97(3):182–9.
12. AboutorabiA,ArazpourM,BahramizadehM,HutchinsSW,Fadayevatan R. The effect of aging on gait parameters inable-bodied older subjects: a literature review. Aging ClinExpRes. 2015;doi:s40520-015-0420-6.
13. Snijders AH, van de Warrenburg BP, Giladi N, Bloem BR.Neurological gait disorders in elderly people: clinical ap-proachandclassification. LancetNeurol. 2007;6(1):63–74.
14. Lundin-Olsson L, Nyberg L, Gustafson Y. “Stops walkingwhen talking” as a predictor of falls in elderly people.Lancet. 1997;349(9052):617.
15. vanIerselMB,VerbeekAL,BloemBR,MunnekeM,EsselinkRA,RikkertMG.Frail elderly patientswithdementia go toofast. JNeurolNeurosurgPsychiatr. 2006;77(7):874–6.
16. Bloem BR, Grimbergen YA, van Dijk JG, Munneke M. The“posture second” strategy: a review of wrong priorities inParkinson’sdisease. JNeurolSci. 2006;248(1–2):196–204.
17. Ravdin LD, Katzen HL, Jackson AE, Tsakanikas D, AssurasS, RelkinNR. Features of gaitmost responsive to tap test innormal pressure hydrocephalus. Clin Neurol Neurosurg.2008;110(5):455–61.
18. NordinE,LindelofN,RosendahlE, JensenJ,Lundin-OlssonL. Prognostic validity of the Timed Up-and-Go test, amodifiedGet-Up-and-Gotest, staff’sglobal judgementandfallhistory inevaluating fall riskinresidential care facilities.AgeAgeing. 2008;37(4):442–8.
19. Stolze H, Klebe S, Zechlin C, Baecker C, Friege L, DeuschlG. Falls in frequentneurological diseases –prevalence, riskfactorsandaetiology. JNeurol. 2004;251(1):79–84.
20. Voermans NC, Snijders AH, Schoon Y, Bloem BR. Whyold people fall (and how to stop them). Pract Neurol.2007;7(3):158–71.
21. RichardsonK,BennettK,KennyRA.Polypharmacy includ-ing falls risk-increasingmedications and subsequent fallsincommunity-dwellingmiddle-agedandolder adults. AgeAgeing. 2015;44(1):90–6.
22. Park H, Satoh H, Miki A, Urushihara H, Sawada Y. Medi-cations associated with falls in older people: systematicreview of publications from a recent 5-year period. Eur JClinPharmacol. 2015;71(12):1429–40.
23. BoersI,GerschlagerW,StalenhoefPA,BloemBR.Falls intheelderly. II.Strategiesforprevention.WienKlinWochenschr.2001;113(11–12):398–407.
24. BloemBR,Boers I,CramerM,WestendorpRG,GerschlagerW. Falls in the elderly. I. Identification of risk factors. WienKlinWochenschr. 2001;113(10):352–62.
25. Alexander NB. Gait disorders in older adults. J AmGeriatrSoc. 1996;44(4):434–51.
26. Wirth CJ, Zichner L, Tschauner C. Orthopädie und or-thopädische Chirurgie: Becken, Hüfte. Stuttgart: GeorgThieme;2004.
27. Chung SS, Lee CS, Kim SH, Chung MW, Ahn JM. Effect oflow back posture on the morphology of the spinal canal.SkeletalRadiol. 2000;29(4):217–23.
28. Lurie J, Tomkins-Lane C. Management of lumbar spinalstenosis. BMJ.2016;352:h6234.
29. Kuhtz-Buschbeck JP, JohnkK,Mader S, StolzeH,MehdornM. Analysis of gait in cervical myelopathy. Gait Posture.1999;9(3):184–9.
30. Nutt JG, Marsden CD, Thompson PD. Human walkingand higher-level gait disorders, particularly in the elderly.Neurology. 1993;43(2):268–79.
31. Nutt JG. Classification of gait and balance disorders. AdvNeurol. 2001;87:135–41.
32. Nutt JG.Higher-level gait disorders: an open frontier. MovDisord. 2013;28(11):1560–5.
33. Morton SM, Bastian AJ. Relative contributions of balanceand voluntary leg-coordination deficits to cerebellar gaitataxia. JNeurophysiol. 2003;89(4):1844–56.
34. Ilg W, Timmann D. Gait ataxia – specific cerebel-lar influences and their rehabilitation. Mov Disord.2013;28(11):1566–75.
35. Wuehr M, Schniepp R, Schlick C, Huth S, Pradhan C,DieterichM, et al. Sensory loss andwalking speed relatedfactors for gait alterations in patients with peripheralneuropathy. GaitPosture. 2014;39(3):852–8.
36. Benson RR, Guttmann CR, Wei X, Warfield SK, Hall C,Schmidt JA, et al. Older people with impaired mobilityhave specific loci of periventricular abnormality on MRI.Neurology. 2002;58(1):48–55.
37. deLaatKF,TuladharAM,vanNordenAG,NorrisDG,ZwiersMP,deLeeuwFE.Lossofwhitematter integrity isassociatedwith gait disorders in cerebral small vessel disease. Brain.2011;134(Pt1):73–83.
38. Demain A, Westby GW, Fernandez-Vidal S, Karachi C,Bonneville F, Do MC, et al. High-level gait and balancedisorders in the elderly: a midbrain disease? J Neurol.2014;261(1):196–206.
39. Stolze H, Vieregge P, Deuschl G. Gait disturbances inneurology.Nervenarzt. 2008;79(4):485–99.
40. FitzGerald PM, Jankovic J. Lower body parkinsonism: evi-denceforvascularetiology.MovDisord. 1989;4(3):249–60.
41. Nonnekes J, Snijders AH, Nutt JG, Deuschl G, GiladiN, Bloem BR. Freezing of gait: a practical approach tomanagement. LancetNeurol. 2015;14(7):768–78.
42. Bloem BR, Hausdorff JM, Visser JE, Giladi N. Falls andfreezing of gait in Parkinson’s disease: a review of twointerconnected, episodic phenomena. Mov Disord.2004;19(8):871–84.
43. Donovan S, Lim C, Diaz N, Browner N, Rose P, SudarskyLR, et al. Laserlight cues for gait freezing in Parkinson’sdisease: an open-label study. ParkinsonismRelat Disord.2011;17(4):240–5.
44. Ling H. Clinical approach to progressive supranuclearpalsy. JMovDisord. 2016;9(1):3–13.
45. HassanA, Ahlskog JE,Matsumoto JY,Milber JM,Bower JH,Wilkinson JR. Orthostatic tremor: Clinical, electrophysio-logic, and treatment findings in 184 patients. Neurology.2016;86(5):458–64.
46. Masdeu JC, Gorelick PB. Thalamic astasia: inability tostand after unilateral thalamic lesions. Ann Neurol.1988;23(6):596–603.
47. KarnathHO.Pushersyndrome–afrequentbutlittle-knowndisturbance of body orientation perception. J Neurol.2007;254(4):415–24.
48. BrandtT, StruppM,Benson J,DieterichM.Vestibulopathicgait.Walkingandrunning. AdvNeurol. 2001;87:165–72.
49. StoneJ.Functionalneurologicaldisorders: theneurologicalassessmentastreatment. PractNeurol. 2016;16(1):7–17.
94 Gait disorders in adults and the elderly K

review article
50. Sokol LL, Espay AJ. Clinical signs in functional (psy-chogenic) gait disorders: a brief survey. J ClinMovDisord.2016;3:3.
51. Hortobagyi T, Lesinski M, Gabler M, VanSwearingenJM, Malatesta D, Granacher U. Effects of three types of
exercise interventions on healthy old adults’ gait speed:A systematic review and meta-analysis. Sports Med.2015;45(12):1627–43.
K Gait disorders in adults and the elderly 95