Embed Size (px)
Citation preview
11
Robert W. Irwin, MDAndrew J. Haig, MD
Thiru M. Annaswamy, MD MASamuel M. Bierner, MD, MRM
AANEM 60th Annual MeetingSan Antonio, Texas
Copyright © October 2013American Association of Neuromuscular
& Electrodiagnostic Medicine2621 Superior Drive NW
Rochester, MN 55901
Printed by Johnson Printing Company, Inc.
Fundamentals of Spine Care for the Non-Spine Physician
22
Please be aware that some of the medical devices or pharmaceuticals discussed in this handout may not be cleared by the FDA or cleared by the FDA for the specific use described by the authors and are “off-label” (i.e. use not described on the product’s label). “Off-label” devices or pharmaceuticals may be used if, in the judgment of the treating physician, such use is medically indicated to treat a patient’s condition. Information regarding the FDA clearance status of a particular device or pharmaceutical may be obtained by reading the product’s package labeling, by contacting a sales representative or legal counsel of the manufacturer of the device or pharmaceutical, or by contacting the FDA at 1-800-638-2041.

33
Table of Contents
Program Committee & Course Objectives 4
Faculty 5
Physical Examination and History in the Diagnosis of Lumbar Pain 7Robert W. Irwin, MD
Putting It All Together: The Electrodiagnostic Examination and the Patient with a Spinal Disorder 13Andrew J. Haig, MD
Effective Use of Diagnostic Studies in Optimizing Patient Management 19Thiru M. Annaswamy, MD, MA
Treatment Options for the Lumbar Spine 23Samuel M. Bierner, MD
CME Questions 31
No one involved in the planning of this CME activity had any relevant financial relationships to disclose.
Chair: Robert W. Irwin, MD
The ideas and opinions expressed in this publication are solely those of the specific authors and do not necessarily represent those of the AANEM.
Fundamentals of Spine Care for the Non-Spine Physician

4
Objectives - Participants will acquire skills to (1) Describe the key physical exam maneuvers to accurately make a diagnosis of lumbar disc herniation, sacroiliac joint pain, and lumbar facet pain, (2) explain how diagnostic studies can affect treatment plans and influence outcomes in diseases of the lumbar spine, (3) identify what EDX tests can be helpful in patients with lumbar disease and know when it is useful to order them, and (4) discuss the different treatment modalities including medications, therapies, and injections and know how to use them to obtain the best outcome.Target Audience:
• Neurologists, physical medicine and rehabilitation and other physicians interested in neuromuscular and electrodiagnostic medicine• Health care professionals involved in the diagnosis and management of patients with neuromuscular diseases• Researchers who are actively involved in the neuromuscular and/or electrodiagnostic research
Accreditation Statement - The AANEM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education (CME) for physicians. CME Credit - The AANEM designates this live activity for a maximum of put in 3.25 AMA PRA Category 1 Credits™. If purchased, the AANEM designates this enduring material for a maximum of 5.75 AMA PRA Category 1 Credits™. This educational event is approved as an Accredited Group Learning Activity under Section 1 of the Framework of Continuing Professional Development (CPD) options for the Maintenance of Certification Program of the Royal College of Physicians and Surgeons of Canada. Physicians should claim on the credit commensurate with the extent of their participation in the activity. CME for this course is available 10/2013 – 10/2016.CEUs Credit - The AANEM has designated this live activity for a maximum of 3.25 AANEM CEU’s. If purchased, the AANEM designates this enduring material for a maximum of 5.75 CEU’s.
Objectives
David B. Shuster, MDDayton, OH
Zachary Simmons, MDHershey, PA
Jeffrey A. Strommen, MDRochester, MN
T. Darrell Thomas, MDKnoxville, TN
Vincent Tranchitella, MD, ChairYork, PA
Thomas Bohr, MD, FRCPCLoma Linda, CA
Jasvinder P. Chawla, MBBS, MD, MBAAtlanta, GA
Robert W. Irwin, MDMiami, FL
Shawn Jorgensen, MDQueensbury, NY
A. Atruro Leis, MDJackson, MS
Maxim Moradian, MDNew Orleans, LA
2012-2013 Program Committee
2012-2013 AANEM PresidentPeter A. Grant, MD
Medford, OR

55
Robert W. Irwin, MDAssistant Dean for Student Affairs, University of Miami Miller School of MedicineDirector, Musculoskeletal Ultrasound EducationUniversity of MiamiMiami, FL
Dr. Irwin earned his medical degree from the University of New Mexico School of Medicine, and completed his internship and residency in internal medicine and physical medicine and rehabilitation (PM&R) at Louisiana State University School of Medicine. He is the assistant dean for Student Affairs at the University of Miami Miller School of Medicine. He is the director of musculoskeletal ultrasound education at the University of Miami/Jackson Residency program and is the course coordinator for the undergraduate medical school courses on musculoskeletal medicine. He is an author or coauthor on 15 publications including textbook chapters and peer reviewed publications. He is board certified in physical medicine and rehabilitation, pain medicine and sports medicine, through the American Board of Physical Medicine and Rehabilitation. His main field of interest is spine and sports care and has focused on interventional skills for spine and sports injuries.
Andrew J. Haig, MDProfessor of Physical Medicine & RehabilitationMedical Director, Telemedicine SystemUniversity of MichicanAnn Arbor, MI
Dr. Haig received his medical degree from the Medical College of Wisconsin, and completed his residency at Northwestern University’s Rehabilitation Institute of Chicago. He is a tenured professor of physical medicine and rehabilitation at the University of Michigan and medical director of the university’s telemedicine system. He serves as a volunteer associate professor at the Medical College of Wisconsin in addition to his current role at Michigan. Dr. Haig is known for developing the standardized protocol for examination of the back muscles, called “paraspinal mapping.” Using that technique he performed the first masked studies in the 60-year history of diagnostic needle electromyography, with later studies demonstrating the superiority of electrodiagnosis over advanced imaging for some spinal disorders. Dr. Haig founded the University of Michigan Spine Fellowship. He is on the editorial board of five medical journals and is editor of a textbook on back. He is certified by the American Board of Physical Medicine and Rehabilitation, the American Board of Electrodiagnostic Medicine, and the American Board of Pain Medicine.
Thiru M. Annaswamy, MD MAAssociate Professor, Department of Physical Medicine & RehabilitationUniversity of Texas Southwestern Medical Center at DallasStaff Physician, VA Medical CenterDallas, TX
Dr. Annaswamy received his medical degree at Mysore Medical College, Mysore, India and master’s degree in Kinesiology, motor control and biomechanics from the University of Texas at Austin. He received his post-graduate medical training in physical medicine and rehabilitation (PM&R) at Harvard Medical School/Spaulding Rehabilitation Hospital. He is an associate professor with the Department of PM&R at the University of Texas Southwestern Medical Center (UTSWMC) at Dallas and a full-time staff physician at the VA Medical Center in PM&R. He has been on faculty at UTSWMC since 1999. His clinical interests are in the evaluation and management of spine disorders, musculoskeletal disorders and diseases of the muscles & nerves. He is board certified in PM&R and subspecialty certified in neuromuscular medicine, electrodiagnostic medicine and pain medicine. His research interests are in virtual reality based simulation of injection procedures, virtual reality applications in rehabilitation, gait and movement analysis, electrophysiological and musculoskeletal research and clinical outcomes research.
Samuel M. Bierner, MD, MRMProfessor of Physical Medicine & RehabilitationDirector, Residency ProgramUniversity of Texas Southwestern Medical CenterDallas, TX
Dr. Bierner received his medical degree from University of Texas Medical School in San Antonio. He completed residencies in pathology at Parkland Memorial Hospital (Dallas), and physical medicine and rehabilitation (PM&R) at Baylor University Medical School (Dallas) and University of Washington Hospitals (Seattle, WA). His fellowship was at National Institutes of Health in Bethesda, MD. Dr. Bierner is a professor of PM&R and residency program director at University of Texas Southwestern Medical Center. He is the PM&R advisor to medical students. He is an author or co-author on 10 publications. Dr. Bierner is vice chair of Education for the AAPM&R Medical Rehabilitation Council and was elected to the UT Southwestern Academy of Teachers. He is interested in epidemiologic aspects of chronic pain in various populations (MS, stroke, FMS), as well as educating young physicians in statistics, research design, ethics and quality improvement. He is board-certified in neuromuscular medicine and pain medicine in addition to PM&R. He is a reviewer for the PM&R Journal, as well as the American Journal of PM&R, the Journal of Applied Biobehavioral Research and the journal Pain Practice.
Faculty
Fundamentals of Spine Care for the Non-Spine Physician

66 7
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
7
Physical Examination and History in the Diagnosis of Lumbar Pain
Robert W. Irwin, M.D.Assistant Dean for Student Affairs, University of Miami Miller School of Medicine
Director, Musculoskeletal Ultrasound EducationUniversity of Miami
Miami, FL
INTRODUCTION
One of the most gratifying parts of medicine is the ability to obtain a history of an illness, perform a physical examination, and have a fair certainty of what is going on with the patient and how they can be helped. This has been the cornerstone of spine care for decades. Unfortunately, with the improvements of technology, the physical examination is being replaced by imaging studies. So much so that newer physicians may not even perform a physical examination, but just obtain a study and treat the findings. This, in turn, has led to an increase in healthcare cost and, in some cases, less than optimal care for some patients.
In the mid-1990s, this phenomenon began to be researched. The study by Jensen1 evaluating magnetic resonance imaging (MRI) of the lumbar spine in men over the age of 35 without any back pain found a surprising number of abnormalities that included frank disc herniations. With this in mind, the medical community has struggled to find the best way to evaluate a patient with back pain. Unfortunately, not all physicians are comfortable with the physical examination of the patient with lumbar complaints. The literature review that follows should help guide physicians in the performance of an appropriate physical examination and history on their patients.
DEFINITIONS OF DISEASE STATES THAT CAN CAUSE LOW BACK PAIN
There are a number of diagnoses involving the lumbar spine. When evaluating the literature, the term low back pain (LBP) has been used as the diagnosis for many of these studies. It is now understood that LBP covers a heterogeneous group of diseases, and, therefore, these studies have led to results that have not
been well translated to the general back pain population. When talking about the lumbar spine, the following diagnoses can be considered as possible sources of LBP: sacroiliac joint (SIJ) pain, herniated nucleus pulposus (HNP), facet pain, degenerative disc disease (DDD), and lumbar spinal stenosis (LSS). This is not an all-inclusive list, but it includes the major diagnoses that will be discussed here. When the symptom of radiation down the leg, or sciatica, is included diagnostic accuracy can be improved, but there is still a wide amount of variability in making the diagnosis.
The fact is that a lumbar disc herniation is not the only diagnosis which can cause LBP with symptoms of sciatica. In fact, while many physicians routinely will give the diagnosis of sciatica for their patients, it is not sufficient to use this diagnoses to set up treatment. This can lead to inappropriate treatments, the false assumtion that the problem will not get better without surgery, and then the possible decrease of the chance of improvement from a successful surgery. Even in te case of SIJ pain, a diagnosis that many physicians believe causes no radiation of pain, Slipman found up to 28% of persons with SIJ pain have pain in the lower leg while 12% complain of pain in the foot.2 As a result, the physical examination must be used, in conjunction with testing, to arrive at an accurate diagnosis. Given that the choice of imaging is based on the physical examination, it behooves physicians to be as accurate as possible with the physical examination. In this age of evidence-based medicine, the literature can help determine the sensitivity and specificity of physical examination maneuvers and the information gleaned from the history for the various diagnoses.

7
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
7
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
7
Physical Examination and History in the Diagnosis of Lumbar Pain
Robert W. Irwin, M.D.Assistant Dean for Student Affairs, University of Miami Miller School of Medicine
Director, Musculoskeletal Ultrasound EducationUniversity of Miami
Miami, FL
INTRODUCTION
One of the most gratifying parts of medicine is the ability to obtain a history of an illness, perform a physical examination, and have a fair certainty of what is going on with the patient and how they can be helped. This has been the cornerstone of spine care for decades. Unfortunately, with the improvements of technology, the physical examination is being replaced by imaging studies. So much so that newer physicians may not even perform a physical examination, but just obtain a study and treat the findings. This, in turn, has led to an increase in healthcare cost and, in some cases, less than optimal care for some patients.
In the mid-1990s, this phenomenon began to be researched. The study by Jensen1 evaluating magnetic resonance imaging (MRI) of the lumbar spine in men over the age of 35 without any back pain found a surprising number of abnormalities that included frank disc herniations. With this in mind, the medical community has struggled to find the best way to evaluate a patient with back pain. Unfortunately, not all physicians are comfortable with the physical examination of the patient with lumbar complaints. The literature review that follows should help guide physicians in the performance of an appropriate physical examination and history on their patients.
DEFINITIONS OF DISEASE STATES THAT CAN CAUSE LOW BACK PAIN
There are a number of diagnoses involving the lumbar spine. When evaluating the literature, the term low back pain (LBP) has been used as the diagnosis for many of these studies. It is now understood that LBP covers a heterogeneous group of diseases, and, therefore, these studies have led to results that have not
been well translated to the general back pain population. When talking about the lumbar spine, the following diagnoses can be considered as possible sources of LBP: sacroiliac joint (SIJ) pain, herniated nucleus pulposus (HNP), facet pain, degenerative disc disease (DDD), and lumbar spinal stenosis (LSS). This is not an all-inclusive list, but it includes the major diagnoses that will be discussed here. When the symptom of radiation down the leg, or sciatica, is included diagnostic accuracy can be improved, but there is still a wide amount of variability in making the diagnosis.
The fact is that a lumbar disc herniation is not the only diagnosis which can cause LBP with symptoms of sciatica. In fact, while many physicians routinely will give the diagnosis of sciatica for their patients, it is not sufficient to use this diagnoses to set up treatment. This can lead to inappropriate treatments, the false assumtion that the problem will not get better without surgery, and then the possible decrease of the chance of improvement from a successful surgery. Even in te case of SIJ pain, a diagnosis that many physicians believe causes no radiation of pain, Slipman found up to 28% of persons with SIJ pain have pain in the lower leg while 12% complain of pain in the foot.2 As a result, the physical examination must be used, in conjunction with testing, to arrive at an accurate diagnosis. Given that the choice of imaging is based on the physical examination, it behooves physicians to be as accurate as possible with the physical examination. In this age of evidence-based medicine, the literature can help determine the sensitivity and specificity of physical examination maneuvers and the information gleaned from the history for the various diagnoses.
assumption

888
LUMABAR DISC HERINATIONS
History
The history and physical examination usually are combined when assessing a patient. In this review of the literature, these two aspects of patient evaluation will be separated to see what information can be most helpful. There is a paucity of studies regarding the history obtained from patients with lumbar disc herniations. There are two studies that directly assess the history and its predictability in lumbar disc herniation. The markers evaluated included age, sex, duration of disease, educational level, smoking habits, comorbidities, sports activities, job type, family history of sciatica, previous history of sciatica, pain based on position, pain worsening at night, leg and back pain, dermatomal pain, valsalva maneuver, paroxysmal pain, and a complaint of weakness.3,4 In the Vroomen study, sensitivities and specificities were not reported, however odds ratios were used to evaluated these components in the presence of a disc herniation as diagnosed by MRI.3 In this study, primary care patients who were over the age of 41 and had dermatomal pain complaints, pain worsening with valsalva maneuver (e.g., coughing, sneezing, or straining), paroxysmal pain, a complaint of weakness and leg pain greater than back pain were all more likely to be those patients with disc herniation.3 The last two elements were also found to be important by another investigator. Lauder and colleagues found that leg pain greater than back pain had a sensitivity/specificity of 86%/12% in the diagnosis of lumbar HNP.4 A complaint of weakness had a sensitivity/specificity of 70%/45%, when compared to electrodiagnostic (EDX) testing.4 In this study, the most specific element of the history was a complaint of burning pain and had a sensitivity/specificity of41%/63%, and a complaint of numbness was 71%/41%.4 Thus, while the evaluation of the history needs more research, it appears that leg pain greater than back pain and a complaint of weakness are moderately sensitive in the history of patients with lumbar HNP.
Physical Examination
While the evidence-based use of elements of the history in assessing lumbar HNP is weak, there is quite a bit more for the physical examination. The most commonly used physical examination maneuvers include straight leg raise (SLR), Slump test, dermatomal sensation, manual muscle testing of strength, and muscle stretch reflexes. Even though there are a number of studies on the physical examination, the sensitivities and specificities are quite varied. In 2011, the Cochrane Collaboration reviewed the literature on physical examination maneuvers.5 One of the biggest difficulties in evaluating these findings is a lack of a gold standard for the diagnosis of lumbar HNP. Some studies used MRI as the standard, while others used surgery, and even a disability questionnaire.3-8 Physicians should be cognizant of the possibility of introducing verification bias into these studies. This occurs when one group is given one type of treatment (e.g., surgery) while another gets something else (e.g., conservative treatment) based on the index tests.
Starting with inspecting the spine for scoliosis, a varied sensitivity ranging 39-68% and a specificity ranging 62-89% was found.5 In what the Cochrane Collaboration considers the strongest study
evaluating this maneuver, the sensitivity/specificity is 63%/89%.5 Unfortunately, these results have not been able to be duplicated in other studies. The sensitivity and specificity of other physical examination maneuvers are shown in Table 1. One study’s data not included in this chart is a study by Ekdahl and colleagues that used the Roland Morris Disability Questionnaire as their gold standard. This study found good validity for both men and women for the finger-to-floor distance test in the setting of radicular pain and that the SLR was less valid.6
Table 1. Sensitivity and specificity of physical examination maneuvers in lumbar herniated nucleus pulposusFor all Cochrane Collaboration data, the RS is noted.
Physical examination maneuver Result: sensitivity/specificityContralateral SLR 1. 23-42%/85-100%4
2. 29%/90%5(RS surgery or imaging)
SLR 1. 64%/57%3
2. 72-97%/11-66%4
3. 52%/89%8
4. 92%/28%5(RS of surgery)5. 35-97%/10-100%5 (RS
imaging)Slump test 1. 84%/83%8
2. 44-94%/23-60%5 (RS imaging)
Sensation in dermatomes 1. 28%/66%3
2. 28-67%/42-69%5 (RS surgery)
Weakness 1. 27%/93%3
Wasting 1. 15-38%/50-94%5,7 (RS surgery)
Reflexes 1. 14%/93%3
2. 31-61%/60-89%5 (RS surgery)
Finger-to-floor distance/flexion 1. 45%/74%3
2. 85-90%/16-29%5 (RS surgery)
Scoliosis by inspection 1. 39-64%/62-89%5 (RS surgery)
RS=reference standard, SLR=straight leg raise
Upon reviewing the Table, there is no clear cut difference between which maneuver is the most sensitive and specific for diagnosing lumbar HNP. In fact, the Cochrane Collaboration found no significant evidence for the use of one test over another, except in a surgical population, and suggested that the selection bias from these studies does not allow for generalizability to the population overall. Some authors have evaluated whether a series of elements in the physical examination would be more helpful. In the Vroomen study, they found that age, duration of disease of 15-30 days, paroxysmal pain, pain worse in the leg than in the back, typical dermatomal distribution of pain, pain worse on coughing/sneezing/straining, finger-to-floor distance, and paresis when used together had a sensitivity of 72% with a specificity of 80%.3 In the Lauder study, there was a 100% specificity when using three or four of the following components: sensation, reflexes, weakness and SLR.4 The Cochrane Collaboration found that combining positive test results could increase the specificity,
PHYSICAL EXAMINATION AND HISTORY IN THE DIAGNOSIS OF LUMBAR PAIN
9
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
9
but few studies were available that assessed this combining effect.5 Overall, the conclusion was that if the SLR and one other test were used, then the sensitivity was low, but the specificity ranged from 66-100%.5
Summary for Lumbar Herniated Nucleus Pulposus
When evaluating the physical examination in the diagnosis of lumbar HNP, we find a few things may be helpful. First, we cannot rely on any one test. Complaints of weakness or leg pain > back pain may give us fair sensitivity. The physical examination will require that we perform a number of maneuvers. It appears that the straight leg raise, when combines with two other tests of either sensation loss, reflex loss or weakness on manual muscle testing can give us a fairly specific examination, and we should feel comfortable with that. This allows the practitioner to start treatment prior to ordering imaging studies. It is possible to make the diagnosis with a modicum of certainty, and if the patient does not respond to treatment, of if you are still not certain of the diagnosis then imaging may enhance this specificity.
SACROOILIAC JOINT PAIN
The diagnosis of SIJ pain is a controversial one. In the early 20th century, the SIJ was considered a major cause of LBP, with or without sciatica. By mid-century, eyes shifted to the lumbar HNP as a more viable diagnosis and, in turn, the diagnosis of SIJ pain fell out of favor in the medical community.9 The prevalence of SIJ pain varies from 13-30% in patients with chronic pain.10 This represents a significant number of patients. Unfortunately, there is less literature on the history and physical examination and diagnosis for SIJ pain than for lumbar HNP. In one study, Dreyfuss and colleagues looked at a number of historical relationships to SIJ pain. The reference standard was intra-articular injections. They found poor sensitivity for all historical data including: being better with standing, sitting, walking, and lying down; or being worse with bowel movements, job activities, wearing heels or boots, and coughing or sneezing. They did find a high specificity for pain being better with standing, walking, and sitting (98%, 77%, and 80%, respectively). In a later study, using dual blocks as the criterion standard, Irwin and colleagues found no correlation between a diagnosis of SIJ pain and weight, tobacco use, or gender. There may have been some selection bias as this was a retrospective study. A study by Slipman and colleagues evaluated pain patterns in SIJ pain. They did find that, while LBP was most common in SIJ pain, up to 14% of patients had radiating pain to the ankle and 12% had it to the foot.2
With the history being less than helpful, the physical examination is even more important. Intra-articular injections have been used as the criterion standard for the studies regarding SIJ pain, which leaves the door open for a discussion of whether the pathology is intra-articular or extra-articular.10-13 For the purposes of this review, these will not be differentiated. These studies have reviewed 13 separate examination maneuvers (Table 2). In the Maigne study, sensitivity and specificity were not provided, but no maneuver was found to be significant. Those with high sensitivity (above 75%) in the Dreyfus study include pain in the SIJ area, the buttock, and the posterior superior iliac spine (PSIS) area and
sacral sulcus tenderness.11 Fortin determined that pain in the PSIS area was 100% specific.12 Laslett and colleagues found the thigh thrust to be sensitive while the distraction test was more specific.13
Table 2. Sensitivity and specificity of physical examination maneuvers in sacroiliac joint pain
Physical examination maneuver Result: sensitivity/specificitySIJ pain 85%/8%11
Groin pain 19%/63%11
Buttock pain 80%/14%11
PSIS pointing (Fortin Finger test) 76%/47%11
100% specificity12
Gillet’s 43%/68%11
Thigh thrust 36%/50%88%/69%13
Patrick’s (Fabere) 69%/16%11
Not significant10
Gaenslen’s 71%/26%11
Not significant10
53%/77%13
Midsacral thrust 53%/29%11
63%/75%13
Spring (sacral pressure) 75%/35%11
Not significant10
Sacral sulcus tender 95%/9%11
Distraction Not significant10
60%/81%13
Compression Not significant10
69%/69%13
PSIS=posterior superior iliac spine, SIJ=sacroiliac joint
It is helpful to review whether multiple tests would increase either the sensitivity and/or specificity of the physical examination. Dreyfus found no combination of tests to be greater than 90% specific unless one performed more than 10 physical examination maneuvers.11 In the Laslett study, sensitivity was greater than 90% if one had between one and three of the following tests positive: distraction, right or left Gaenslen’s test, thigh thrust, and sacral thrust.13 Requiring four or more tests to be positive significantly decreased the sensitivity, however only if three or more tests were required was the specificity greater than 75%. In this study, one of those tests that needed to be positive was the Gaenslen’s test along with two others. This study then suggests an optimal examination would include Gaenslen’s test and two of the other four mentioned above being positive, resulting in good sensitivity and fair specificity.13
Summary for Sacroiliac Joint Pain
The history obtained in the evaluation of SIJ pain is neither sensitive nor specific. There is overlap with sciatica symptoms, and that should be considered in those patients who present with these symptoms. Three physical examination maneuvers, including Gaenslen’s test, thigh thrust, distraction and sacral thrust, will give good sensitivity and fair specificity, but the study that determined this has not been duplicated in the literature. It appears that pointing to the PSIS area will have just as good of a diagnostic value as the combination.
LUMBAR DISK HERNIATIONS

9
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
88
LUMABAR DISC HERINATIONS
History
The history and physical examination usually are combined when assessing a patient. In this review of the literature, these two aspects of patient evaluation will be separated to see what information can be most helpful. There is a paucity of studies regarding the history obtained from patients with lumbar disc herniations. There are two studies that directly assess the history and its predictability in lumbar disc herniation. The markers evaluated included age, sex, duration of disease, educational level, smoking habits, comorbidities, sports activities, job type, family history of sciatica, previous history of sciatica, pain based on position, pain worsening at night, leg and back pain, dermatomal pain, valsalva maneuver, paroxysmal pain, and a complaint of weakness.3,4 In the Vroomen study, sensitivities and specificities were not reported, however odds ratios were used to evaluated these components in the presence of a disc herniation as diagnosed by MRI.3 In this study, primary care patients who were over the age of 41 and had dermatomal pain complaints, pain worsening with valsalva maneuver (e.g., coughing, sneezing, or straining), paroxysmal pain, a complaint of weakness and leg pain greater than back pain were all more likely to be those patients with disc herniation.3 The last two elements were also found to be important by another investigator. Lauder and colleagues found that leg pain greater than back pain had a sensitivity/specificity of 86%/12% in the diagnosis of lumbar HNP.4 A complaint of weakness had a sensitivity/specificity of 70%/45%, when compared to electrodiagnostic (EDX) testing.4 In this study, the most specific element of the history was a complaint of burning pain and had a sensitivity/specificity of41%/63%, and a complaint of numbness was 71%/41%.4 Thus, while the evaluation of the history needs more research, it appears that leg pain greater than back pain and a complaint of weakness are moderately sensitive in the history of patients with lumbar HNP.
Physical Examination
While the evidence-based use of elements of the history in assessing lumbar HNP is weak, there is quite a bit more for the physical examination. The most commonly used physical examination maneuvers include straight leg raise (SLR), Slump test, dermatomal sensation, manual muscle testing of strength, and muscle stretch reflexes. Even though there are a number of studies on the physical examination, the sensitivities and specificities are quite varied. In 2011, the Cochrane Collaboration reviewed the literature on physical examination maneuvers.5 One of the biggest difficulties in evaluating these findings is a lack of a gold standard for the diagnosis of lumbar HNP. Some studies used MRI as the standard, while others used surgery, and even a disability questionnaire.3-8 Physicians should be cognizant of the possibility of introducing verification bias into these studies. This occurs when one group is given one type of treatment (e.g., surgery) while another gets something else (e.g., conservative treatment) based on the index tests.
Starting with inspecting the spine for scoliosis, a varied sensitivity ranging 39-68% and a specificity ranging 62-89% was found.5 In what the Cochrane Collaboration considers the strongest study
evaluating this maneuver, the sensitivity/specificity is 63%/89%.5 Unfortunately, these results have not been able to be duplicated in other studies. The sensitivity and specificity of other physical examination maneuvers are shown in Table 1. One study’s data not included in this chart is a study by Ekdahl and colleagues that used the Roland Morris Disability Questionnaire as their gold standard. This study found good validity for both men and women for the finger-to-floor distance test in the setting of radicular pain and that the SLR was less valid.6
Table 1. Sensitivity and specificity of physical examination maneuvers in lumbar herniated nucleus pulposusFor all Cochrane Collaboration data, the RS is noted.
Physical examination maneuver Result: sensitivity/specificityContralateral SLR 1. 23-42%/85-100%4
2. 29%/90%5(RS surgery or imaging)
SLR 1. 64%/57%3
2. 72-97%/11-66%4
3. 52%/89%8
4. 92%/28%5(RS of surgery)5. 35-97%/10-100%5 (RS
imaging)Slump test 1. 84%/83%8
2. 44-94%/23-60%5 (RS imaging)
Sensation in dermatomes 1. 28%/66%3
2. 28-67%/42-69%5 (RS surgery)
Weakness 1. 27%/93%3
Wasting 1. 15-38%/50-94%5,7 (RS surgery)
Reflexes 1. 14%/93%3
2. 31-61%/60-89%5 (RS surgery)
Finger-to-floor distance/flexion 1. 45%/74%3
2. 85-90%/16-29%5 (RS surgery)
Scoliosis by inspection 1. 39-64%/62-89%5 (RS surgery)
RS=reference standard, SLR=straight leg raise
Upon reviewing the Table, there is no clear cut difference between which maneuver is the most sensitive and specific for diagnosing lumbar HNP. In fact, the Cochrane Collaboration found no significant evidence for the use of one test over another, except in a surgical population, and suggested that the selection bias from these studies does not allow for generalizability to the population overall. Some authors have evaluated whether a series of elements in the physical examination would be more helpful. In the Vroomen study, they found that age, duration of disease of 15-30 days, paroxysmal pain, pain worse in the leg than in the back, typical dermatomal distribution of pain, pain worse on coughing/sneezing/straining, finger-to-floor distance, and paresis when used together had a sensitivity of 72% with a specificity of 80%.3 In the Lauder study, there was a 100% specificity when using three or four of the following components: sensation, reflexes, weakness and SLR.4 The Cochrane Collaboration found that combining positive test results could increase the specificity,
PHYSICAL EXAMINATION AND HISTORY IN THE DIAGNOSIS OF LUMBAR PAIN
9
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
9
but few studies were available that assessed this combining effect.5 Overall, the conclusion was that if the SLR and one other test were used, then the sensitivity was low, but the specificity ranged from 66-100%.5
Summary for Lumbar Herniated Nucleus Pulposus
When evaluating the physical examination in the diagnosis of lumbar HNP, we find a few things may be helpful. First, we cannot rely on any one test. Complaints of weakness or leg pain > back pain may give us fair sensitivity. The physical examination will require that we perform a number of maneuvers. It appears that the straight leg raise, when combines with two other tests of either sensation loss, reflex loss or weakness on manual muscle testing can give us a fairly specific examination, and we should feel comfortable with that. This allows the practitioner to start treatment prior to ordering imaging studies. It is possible to make the diagnosis with a modicum of certainty, and if the patient does not respond to treatment, of if you are still not certain of the diagnosis then imaging may enhance this specificity.
SACROOILIAC JOINT PAIN
The diagnosis of SIJ pain is a controversial one. In the early 20th century, the SIJ was considered a major cause of LBP, with or without sciatica. By mid-century, eyes shifted to the lumbar HNP as a more viable diagnosis and, in turn, the diagnosis of SIJ pain fell out of favor in the medical community.9 The prevalence of SIJ pain varies from 13-30% in patients with chronic pain.10 This represents a significant number of patients. Unfortunately, there is less literature on the history and physical examination and diagnosis for SIJ pain than for lumbar HNP. In one study, Dreyfuss and colleagues looked at a number of historical relationships to SIJ pain. The reference standard was intra-articular injections. They found poor sensitivity for all historical data including: being better with standing, sitting, walking, and lying down; or being worse with bowel movements, job activities, wearing heels or boots, and coughing or sneezing. They did find a high specificity for pain being better with standing, walking, and sitting (98%, 77%, and 80%, respectively). In a later study, using dual blocks as the criterion standard, Irwin and colleagues found no correlation between a diagnosis of SIJ pain and weight, tobacco use, or gender. There may have been some selection bias as this was a retrospective study. A study by Slipman and colleagues evaluated pain patterns in SIJ pain. They did find that, while LBP was most common in SIJ pain, up to 14% of patients had radiating pain to the ankle and 12% had it to the foot.2
With the history being less than helpful, the physical examination is even more important. Intra-articular injections have been used as the criterion standard for the studies regarding SIJ pain, which leaves the door open for a discussion of whether the pathology is intra-articular or extra-articular.10-13 For the purposes of this review, these will not be differentiated. These studies have reviewed 13 separate examination maneuvers (Table 2). In the Maigne study, sensitivity and specificity were not provided, but no maneuver was found to be significant. Those with high sensitivity (above 75%) in the Dreyfus study include pain in the SIJ area, the buttock, and the posterior superior iliac spine (PSIS) area and
sacral sulcus tenderness.11 Fortin determined that pain in the PSIS area was 100% specific.12 Laslett and colleagues found the thigh thrust to be sensitive while the distraction test was more specific.13
Table 2. Sensitivity and specificity of physical examination maneuvers in sacroiliac joint pain
Physical examination maneuver Result: sensitivity/specificitySIJ pain 85%/8%11
Groin pain 19%/63%11
Buttock pain 80%/14%11
PSIS pointing (Fortin Finger test) 76%/47%11
100% specificity12
Gillet’s 43%/68%11
Thigh thrust 36%/50%88%/69%13
Patrick’s (Fabere) 69%/16%11
Not significant10
Gaenslen’s 71%/26%11
Not significant10
53%/77%13
Midsacral thrust 53%/29%11
63%/75%13
Spring (sacral pressure) 75%/35%11
Not significant10
Sacral sulcus tender 95%/9%11
Distraction Not significant10
60%/81%13
Compression Not significant10
69%/69%13
PSIS=posterior superior iliac spine, SIJ=sacroiliac joint
It is helpful to review whether multiple tests would increase either the sensitivity and/or specificity of the physical examination. Dreyfus found no combination of tests to be greater than 90% specific unless one performed more than 10 physical examination maneuvers.11 In the Laslett study, sensitivity was greater than 90% if one had between one and three of the following tests positive: distraction, right or left Gaenslen’s test, thigh thrust, and sacral thrust.13 Requiring four or more tests to be positive significantly decreased the sensitivity, however only if three or more tests were required was the specificity greater than 75%. In this study, one of those tests that needed to be positive was the Gaenslen’s test along with two others. This study then suggests an optimal examination would include Gaenslen’s test and two of the other four mentioned above being positive, resulting in good sensitivity and fair specificity.13
Summary for Sacroiliac Joint Pain
The history obtained in the evaluation of SIJ pain is neither sensitive nor specific. There is overlap with sciatica symptoms, and that should be considered in those patients who present with these symptoms. Three physical examination maneuvers, including Gaenslen’s test, thigh thrust, distraction and sacral thrust, will give good sensitivity and fair specificity, but the study that determined this has not been duplicated in the literature. It appears that pointing to the PSIS area will have just as good of a diagnostic value as the combination.
11
13
13

101010
LUBMAR FACET PAIN
In evaluating the patient with LBP, the lumbar facet pain syndrome should be considered. The literature regarding the evaluation for this diagnosis is even less prevalent than the previous two diagnoses and there is even less agreement on what is helpful. In this case, LBP with symptoms of sciatica do not occur together. Back and thigh pain have been noted in this patient group, but not back and leg pain.14 The history for this disease process has been elusive. Some researchers have found no pathognomonic historical elements for this pain syndrome15 while others have been able to find certain aspects that may be helpful. Fairbanks found that those patients who were diagnosed with facet pain by intra-articular injections had back and thigh pain, had acute onset, their pain was worse with sitting and with flexion, only back pain was elicited with the SLR, and they were younger.14 He also found their pain to be better with walking and they had pain with extension, but these were not found to be statistically significant.14
In 1998, Revel and colleagues returned to the lumbar facet to see if they could be able to predict who would have facet pain diagnosed with physical examination. This article found that patients had a higher likelihood of responding to an injection if a they met these five criteria: (1) pain not worsened by coughing, (2) pain not worsened by straightening from flexion, (3) pain not worsened by extension/rotation, (4) pain not worsened by hyperextension, and (5) pain improved in the supine position.16 This was contrary to what many had been espousing as the best way to examine for facet pain, which was pain with extension/rotation. This, however, had never been proven in the literature and had been thought to be correct because it made sense to many that “loading” the facet joint should cause pain; it was accepted without validation. When Laslett revisited these criteria in 2006, he found a number of false-positives with this maneuver, but he found it to be 100% sensitive and 22% specific in predicting whether a patient would get 95% relief of their pain with an intra-articular injection.17 This lessened to a sensitivity of 86% and specificity of 22% if the criteria for the diagnosis was lowered to achieving 75% pain relief with the intra-articular injections.17 In that study, the authors found that a combination of three or more of the following gave a sensitivity of 85% and a specificity of 91%: age greater than 50 years, symptoms better with walking, symptoms better with sitting, onset of pain in the paraspinals, and pain with extension and rotation combined.17
Summary for Facet Pain
The literature is not in agreement with any history or physical examination maneuvers that can help diagnose lumbar facet pain. Given this, one should consider other causes of LBP in this diagnosis in a patient who is not improving with treatments. One will no doubt need a combination of tests to make a clinical diagnosis with any certainty, but the combination of which tests and history remains to be seen. This author suggests a higher index of suspicion in patients with no PSIS tenderness and LBP only may be a good place to start in this disease.
DEGENERATIVE DISC DISEASE
DDD has been noted to be one of the major causes of LBP in the chronic pain population. One cohort study looked at the presence of disc degeneration on MRI and found it was not related to the development or duration of LBP and suggested a clinical correlation to help with the diagnosis.18 More recent studies suggest that modic changes on MRI are well correlated with LBP and can be treated with antibiotics, suggesting that this is not just degeneration but also an infectious process.19,20 This leaves the clinician needing to rely on clinical data to help make the diagnosis. Unfortunately, the literature does not help much. In a landmark study by Schwartzer, in which provocative discography was used as the reference standard, he found no clinical assessment tool correlated with painful disc on the discogram.21 In this study, pain increased by sitting, standing, walking, with forward flexion, extension, and rotation/extension, nor pain relieved by sitting, standing, or walking were helpful in making the diagnosis. He also found no referral pain pattern to be helpful, not to the buttock, groin, thigh, calf, or foot.21
SPINAL STENOSIS
Lumbar stenosis classically is thought of as causing pseudoclaudication, but the presentation is not always clear. There are three major types of lumbar stenosis. These include central stenosis, lateral recess stenosis, and neuroforaminal stenosis, and they may have different clinical presentations. Cauda equine syndrome (CES) may be a result of central stenosis, but it is not seen in the other two types of stenosis. Neuroforaminal stenosis is the result of factors that narrow the exit foramen for the nerve roots. As such, this type of stenosis may present with more sciatica symptoms. Lateral recess stenosis can be caused by facet or ligamentum flavum hypertrophy or HNP and can affect a single nerve root as it transverses the canal to reach the neural foramen. This also may present with the classic sciatica symptoms. In the literature, the studies that address history and physical examination either do not specify which type of stenosis is included or they only deal with central stenosis.
In one study, the authors found that patients with lumbar stenosis may have leg cramps, present with unilateral or bilateral symptoms, and/or have hamstring tightness, but neither sensitivity nor specificity of these symptoms was discussed.22 In another article, the authors compared two presentations of lumbar stenosis, CES and radicular type. They developed a questionnaire tool and then applied it to a group of patients.23 They found that key predictive factors for overlapping symptoms between the two types of lumbar stenosis were age greater than 50 years, lower-extremity pain or numbness, increased pain when walking, increased pain when standing, and relief of symptoms on bending forward. This study compared the two presentations to see if they could differentiate them. The physical examination was not found to be helpful. The sensitivity of the following historical questions were greater than 90% for both types of stenosis: (1) numbness or pain down to the thighs/calves or shin, (20) numbness or pain worse with walking and better with taking a rest, (3) standing bringing on the pain in the thighs/calves or shins, and (4) bending forward reduced pain.23 This study did not address how to differentiate lumbar stenosis from other disease states.
PHYSICAL EXAMINATION AND HISTORY IN THE DIAGNOSIS OF LUMBAR PAIN
11
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
In the only study that truely addresses the issue of the accuracy of the history and examination, Suri and colleagues found a specificity of greater than 84% was associated with orthopedic comorbidities, bilateral buttock or leg pain, no pain when seated, improvement of pain when bending forward or seated, urinary disturbance, perineal numbness, and bilateral plantar numbness.24 Sensitivity of greater than 82% was found if there was neurogenic claudication, pain was exacerbated while standing up, or pain was below the buttocks, in the thigh, or gluteal area.24 In this study, a sensitivity of greater than 90% was associated with two portions of the physical examination. These were a wide based gait or an abnormal Rhomberg sign.24
SUMMARY
The physical examination for lumbar pain with sciatica symptoms can be very helpful in differentiating some, but not all, of the causes. The history and physical examination is most effective in lumbar disc herniations, where the specificity can be as high as 100% with only three or four physical examination maneuvers. This can be especially helpful when assessing these findings along with imaging and EDX studies. The SIJ pain syndrome and facet syndrome are less likely to have such specificity for the history and physical examination but all have some elements that can help in establishing a preliminary diagnosis and embarking on a treatment plan. There are a number of elements in the history and physical examination that yield good sensitivity either alone or in conjunction with other elements. The sensitivity of certain elements in LSS can be as high as 90%, thus this diagnosis can be made prior to obtaining imaging studies. Lumbar disc degeneration is the hardest to diagnose with the history and physical examination. Caution is advised when offering this diagnosis early on in treatment and with only a history and physical examination.
REFERENCES
1. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 1994;331:69-73.
2. Slipman CW, Jackson HB, Lipetz JS, Chan KT, Lenrow D, Vresilovic EJ. Sacroiliac joint pain referral zones. Arch Phys Med Rehabil 2000;81:334-338.
3. Vroomen PC, de Krom MC, Wilmink JT, Kester AD, Knottnerus JA. Diagnostic value of history and physical examination in patients suspected of lumbosacral nerve root compression. J Neurol Neurosurg Psychiatry 2002;72:630-634.
4. Lauder TD, Dillingham TR, Andary M, et al. Effect of history and exam in predicting electrodiagnostic outcome among patients with suspected lumbosacral radiculopathy. Am J Phys Med Rehabil 2000;79:60-68; quiz 75-76.
5. van der Windt DA, Simons E, Riphagen, II, et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev 2011:CD007431.
6. Ekedahl KH, Jonsson B, Frobell RB. Validity of the fingertip-to-floor test and straight leg raising test in patients with acute and subacute low back pain: a comparison by sex and radicular pain. Arch Phys Med Rehabil 2010;91:1243-1247.
7. Kerr RS, Cadoux-Hudson TA, Adams CB. The value of accurate clinical assessment in the surgical management of the lumbar disc protrusion. J Neurol Neurosurg Psychiatry 1988;51:169-173.
8. Majlesi J, Togay H, Unalan H, Toprak S. The sensitivity and specificity of the Slump and the Straight Leg Raising tests in patients with lumbar disc herniation. J Clin Rheumatol 2008;14:87-91.
9. Irwin RW, Watson T, Minick RP, Ambrosius WT. Age, body mass index, and gender differences in sacroiliac joint pathology. Am J Phys Med Rehabil 2007;86:37-44.
10. Maigne JY, Aivaliklis A, Pfefer F. Results of sacroiliac joint double block and value of sacroiliac pain provocation tests in 54 patients with low back pain. Spine 1996;21:1889-1892.
11. Dreyfuss P, Michaelsen M, Pauza K, McLarty J, Bogduk N. The value of medical history and physical examination in diagnosing sacroiliac joint pain. Spine 1996;21:2594-2602.
12. Fortin JD, Falco FJ. The Fortin Finger Test: an indicator of sacroiliac pain. Am J Orthop 1997;26:477-480.
13. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests. Man Ther 2005;10:207-218.
14. Fairbank JC, Park WM, McCall IW, O’Brien JP. Apophyseal injection of local anesthetic as a diagnostic aid in primary low-back pain syndromes. Spine 1981;6:598-605.
15. Dreyfuss PH, Dreyer SJ, Nass. Lumbar zygapophysial (facet) joint injections. Spine J 2003;3:50S-59S.
16. Revel M, Poiraudeau S, Auleley GR, et al. Capacity of the clinical picture to characterize low back pain relieved by facet joint anesthesia. Proposed criteria to identify patients with painful facet joints. Spine 1998;23:1972-1976; discussion 1977.
17. Laslett M, McDonald B, Aprill CN, Tropp H, Oberg B. Clinical predictors of screening lumbar zygapophyseal joint blocks: development of clinical prediction rules. Spine J 2006;6:370-379.
18. Borenstein DG, O’Mara JW, Jr., Boden SD, et al. The value of magnetic resonance imaging of the lumbar spine to predict low-back pain in asymptomatic subjects: a seven-year follow-up study. J Bone Joint Surg Am 2001;83-A:1306-1311.
19. Albert HB, Sorensen JS, Christensen BS, Manniche C. Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy. Eur Spine J 2013;22:697-707.
20. Albert HB, Lambert P, Rollason J, et al. Does nuclear tissue infected with bacteria following disc herniations lead to Modic changes in the adjacent vertebrae? Eur Spine J 2013;22:690-696.
21. Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine 1995;20:1878-1883.
22. Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol 2010;24:253-265.
23. Konno S, Kikuchi S, Tanaka Y, et al. A diagnostic support tool for lumbar spinal stenosis: a self-administered, self-reported history questionnaire. BMC musculoskeletal disorders 2007;8:102.
24. Suri P, Rainville J, Kalichman L, Katz JN. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA 2010;304:2628-2636.
LUMBAR

11
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
1010
LUBMAR FACET PAIN
In evaluating the patient with LBP, the lumbar facet pain syndrome should be considered. The literature regarding the evaluation for this diagnosis is even less prevalent than the previous two diagnoses and there is even less agreement on what is helpful. In this case, LBP with symptoms of sciatica do not occur together. Back and thigh pain have been noted in this patient group, but not back and leg pain.14 The history for this disease process has been elusive. Some researchers have found no pathognomonic historical elements for this pain syndrome15 while others have been able to find certain aspects that may be helpful. Fairbanks found that those patients who were diagnosed with facet pain by intra-articular injections had back and thigh pain, had acute onset, their pain was worse with sitting and with flexion, only back pain was elicited with the SLR, and they were younger.14 He also found their pain to be better with walking and they had pain with extension, but these were not found to be statistically significant.14
In 1998, Revel and colleagues returned to the lumbar facet to see if they could be able to predict who would have facet pain diagnosed with physical examination. This article found that patients had a higher likelihood of responding to an injection if a they met these five criteria: (1) pain not worsened by coughing, (2) pain not worsened by straightening from flexion, (3) pain not worsened by extension/rotation, (4) pain not worsened by hyperextension, and (5) pain improved in the supine position.16 This was contrary to what many had been espousing as the best way to examine for facet pain, which was pain with extension/rotation. This, however, had never been proven in the literature and had been thought to be correct because it made sense to many that “loading” the facet joint should cause pain; it was accepted without validation. When Laslett revisited these criteria in 2006, he found a number of false-positives with this maneuver, but he found it to be 100% sensitive and 22% specific in predicting whether a patient would get 95% relief of their pain with an intra-articular injection.17 This lessened to a sensitivity of 86% and specificity of 22% if the criteria for the diagnosis was lowered to achieving 75% pain relief with the intra-articular injections.17 In that study, the authors found that a combination of three or more of the following gave a sensitivity of 85% and a specificity of 91%: age greater than 50 years, symptoms better with walking, symptoms better with sitting, onset of pain in the paraspinals, and pain with extension and rotation combined.17
Summary for Facet Pain
The literature is not in agreement with any history or physical examination maneuvers that can help diagnose lumbar facet pain. Given this, one should consider other causes of LBP in this diagnosis in a patient who is not improving with treatments. One will no doubt need a combination of tests to make a clinical diagnosis with any certainty, but the combination of which tests and history remains to be seen. This author suggests a higher index of suspicion in patients with no PSIS tenderness and LBP only may be a good place to start in this disease.
DEGENERATIVE DISC DISEASE
DDD has been noted to be one of the major causes of LBP in the chronic pain population. One cohort study looked at the presence of disc degeneration on MRI and found it was not related to the development or duration of LBP and suggested a clinical correlation to help with the diagnosis.18 More recent studies suggest that modic changes on MRI are well correlated with LBP and can be treated with antibiotics, suggesting that this is not just degeneration but also an infectious process.19,20 This leaves the clinician needing to rely on clinical data to help make the diagnosis. Unfortunately, the literature does not help much. In a landmark study by Schwartzer, in which provocative discography was used as the reference standard, he found no clinical assessment tool correlated with painful disc on the discogram.21 In this study, pain increased by sitting, standing, walking, with forward flexion, extension, and rotation/extension, nor pain relieved by sitting, standing, or walking were helpful in making the diagnosis. He also found no referral pain pattern to be helpful, not to the buttock, groin, thigh, calf, or foot.21
SPINAL STENOSIS
Lumbar stenosis classically is thought of as causing pseudoclaudication, but the presentation is not always clear. There are three major types of lumbar stenosis. These include central stenosis, lateral recess stenosis, and neuroforaminal stenosis, and they may have different clinical presentations. Cauda equine syndrome (CES) may be a result of central stenosis, but it is not seen in the other two types of stenosis. Neuroforaminal stenosis is the result of factors that narrow the exit foramen for the nerve roots. As such, this type of stenosis may present with more sciatica symptoms. Lateral recess stenosis can be caused by facet or ligamentum flavum hypertrophy or HNP and can affect a single nerve root as it transverses the canal to reach the neural foramen. This also may present with the classic sciatica symptoms. In the literature, the studies that address history and physical examination either do not specify which type of stenosis is included or they only deal with central stenosis.
In one study, the authors found that patients with lumbar stenosis may have leg cramps, present with unilateral or bilateral symptoms, and/or have hamstring tightness, but neither sensitivity nor specificity of these symptoms was discussed.22 In another article, the authors compared two presentations of lumbar stenosis, CES and radicular type. They developed a questionnaire tool and then applied it to a group of patients.23 They found that key predictive factors for overlapping symptoms between the two types of lumbar stenosis were age greater than 50 years, lower-extremity pain or numbness, increased pain when walking, increased pain when standing, and relief of symptoms on bending forward. This study compared the two presentations to see if they could differentiate them. The physical examination was not found to be helpful. The sensitivity of the following historical questions were greater than 90% for both types of stenosis: (1) numbness or pain down to the thighs/calves or shin, (20) numbness or pain worse with walking and better with taking a rest, (3) standing bringing on the pain in the thighs/calves or shins, and (4) bending forward reduced pain.23 This study did not address how to differentiate lumbar stenosis from other disease states.
PHYSICAL EXAMINATION AND HISTORY IN THE DIAGNOSIS OF LUMBAR PAIN
11
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
In the only study that truely addresses the issue of the accuracy of the history and examination, Suri and colleagues found a specificity of greater than 84% was associated with orthopedic comorbidities, bilateral buttock or leg pain, no pain when seated, improvement of pain when bending forward or seated, urinary disturbance, perineal numbness, and bilateral plantar numbness.24 Sensitivity of greater than 82% was found if there was neurogenic claudication, pain was exacerbated while standing up, or pain was below the buttocks, in the thigh, or gluteal area.24 In this study, a sensitivity of greater than 90% was associated with two portions of the physical examination. These were a wide based gait or an abnormal Rhomberg sign.24
SUMMARY
The physical examination for lumbar pain with sciatica symptoms can be very helpful in differentiating some, but not all, of the causes. The history and physical examination is most effective in lumbar disc herniations, where the specificity can be as high as 100% with only three or four physical examination maneuvers. This can be especially helpful when assessing these findings along with imaging and EDX studies. The SIJ pain syndrome and facet syndrome are less likely to have such specificity for the history and physical examination but all have some elements that can help in establishing a preliminary diagnosis and embarking on a treatment plan. There are a number of elements in the history and physical examination that yield good sensitivity either alone or in conjunction with other elements. The sensitivity of certain elements in LSS can be as high as 90%, thus this diagnosis can be made prior to obtaining imaging studies. Lumbar disc degeneration is the hardest to diagnose with the history and physical examination. Caution is advised when offering this diagnosis early on in treatment and with only a history and physical examination.
REFERENCES
1. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 1994;331:69-73.
2. Slipman CW, Jackson HB, Lipetz JS, Chan KT, Lenrow D, Vresilovic EJ. Sacroiliac joint pain referral zones. Arch Phys Med Rehabil 2000;81:334-338.
3. Vroomen PC, de Krom MC, Wilmink JT, Kester AD, Knottnerus JA. Diagnostic value of history and physical examination in patients suspected of lumbosacral nerve root compression. J Neurol Neurosurg Psychiatry 2002;72:630-634.
4. Lauder TD, Dillingham TR, Andary M, et al. Effect of history and exam in predicting electrodiagnostic outcome among patients with suspected lumbosacral radiculopathy. Am J Phys Med Rehabil 2000;79:60-68; quiz 75-76.
5. van der Windt DA, Simons E, Riphagen, II, et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev 2011:CD007431.
6. Ekedahl KH, Jonsson B, Frobell RB. Validity of the fingertip-to-floor test and straight leg raising test in patients with acute and subacute low back pain: a comparison by sex and radicular pain. Arch Phys Med Rehabil 2010;91:1243-1247.
7. Kerr RS, Cadoux-Hudson TA, Adams CB. The value of accurate clinical assessment in the surgical management of the lumbar disc protrusion. J Neurol Neurosurg Psychiatry 1988;51:169-173.
8. Majlesi J, Togay H, Unalan H, Toprak S. The sensitivity and specificity of the Slump and the Straight Leg Raising tests in patients with lumbar disc herniation. J Clin Rheumatol 2008;14:87-91.
9. Irwin RW, Watson T, Minick RP, Ambrosius WT. Age, body mass index, and gender differences in sacroiliac joint pathology. Am J Phys Med Rehabil 2007;86:37-44.
10. Maigne JY, Aivaliklis A, Pfefer F. Results of sacroiliac joint double block and value of sacroiliac pain provocation tests in 54 patients with low back pain. Spine 1996;21:1889-1892.
11. Dreyfuss P, Michaelsen M, Pauza K, McLarty J, Bogduk N. The value of medical history and physical examination in diagnosing sacroiliac joint pain. Spine 1996;21:2594-2602.
12. Fortin JD, Falco FJ. The Fortin Finger Test: an indicator of sacroiliac pain. Am J Orthop 1997;26:477-480.
13. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests. Man Ther 2005;10:207-218.
14. Fairbank JC, Park WM, McCall IW, O’Brien JP. Apophyseal injection of local anesthetic as a diagnostic aid in primary low-back pain syndromes. Spine 1981;6:598-605.
15. Dreyfuss PH, Dreyer SJ, Nass. Lumbar zygapophysial (facet) joint injections. Spine J 2003;3:50S-59S.
16. Revel M, Poiraudeau S, Auleley GR, et al. Capacity of the clinical picture to characterize low back pain relieved by facet joint anesthesia. Proposed criteria to identify patients with painful facet joints. Spine 1998;23:1972-1976; discussion 1977.
17. Laslett M, McDonald B, Aprill CN, Tropp H, Oberg B. Clinical predictors of screening lumbar zygapophyseal joint blocks: development of clinical prediction rules. Spine J 2006;6:370-379.
18. Borenstein DG, O’Mara JW, Jr., Boden SD, et al. The value of magnetic resonance imaging of the lumbar spine to predict low-back pain in asymptomatic subjects: a seven-year follow-up study. J Bone Joint Surg Am 2001;83-A:1306-1311.
19. Albert HB, Sorensen JS, Christensen BS, Manniche C. Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy. Eur Spine J 2013;22:697-707.
20. Albert HB, Lambert P, Rollason J, et al. Does nuclear tissue infected with bacteria following disc herniations lead to Modic changes in the adjacent vertebrae? Eur Spine J 2013;22:690-696.
21. Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine 1995;20:1878-1883.
22. Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol 2010;24:253-265.
23. Konno S, Kikuchi S, Tanaka Y, et al. A diagnostic support tool for lumbar spinal stenosis: a self-administered, self-reported history questionnaire. BMC musculoskeletal disorders 2007;8:102.
24. Suri P, Rainville J, Kalichman L, Katz JN. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA 2010;304:2628-2636.

12

13
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
Readers will know quite a bit about electrodiagnostic (EDX) medicine and will have been exposed to spine care. They undoubtedly believe that the EDX examination is useful in their personal management of spinal disorders. However, the logic behind this belief needs to be rational if they are to provide the best care and if they are to justify their practice to others. That logic requires integration of EDX and spine medicine. The purpose of this discussion is to outline and examine the logic behind EDX in spinal disorders.
Logical practice is not equivalent to “evidence-based medicine.” In fact, in a very mathematical and scientific way, optimal practice requires that the practitioner deviate from evidence-based rules. The majority of back pain management is, and should be, based on the vast variability in patient, physician, environment, and time variables, rather than the reductionist evidence that current scientific methodology values. While studies—some performed by the author’s group—provide information about what is true in general, this discussion attempts to focus on the pathway in which those truths are best unfolded. There has been precious little research about the nonlinear, recursive pathways of care that are in fact the core of medical decisionmaking. Given the bias of current funding sources towards older models of research, that research is not imminently forthcoming either. Yet, clinicans must make decisions regarding their patients. To help make these decisions, four questions will be asked:
13
Putting It All Together: The Electrodiagnostic Examination and the Patient With a
Spinal DisorderAndrew J. Haig, MD
Professor of Physical Medicine & RehabilitationMedical Director, Telemedicine System
University of MichicanAnn Arbor, MI
1. Is EDX useful for spinal disorders?
2. When is EDX useful?
3. What EDX evaluations are useful?
4. What don’t we know?
IS ELECTRODIAGNOSTIC MEDICINE USEFUL FOR SPINAL DISORDERS?
Yes, there is very strong evidence that EDX can diagnose some spinal disorders and detect some non-spinal disorders that mimic spinal disorders. The EDX examination provides the only useful test for some conditions, is the best test for others, and can be useful alternative for still others. The information gleaned from the EDX examination does impact the outcome in many cases.
WHEN IS ELECTRODIAGNOSTIC MEDICINE USEFUL?
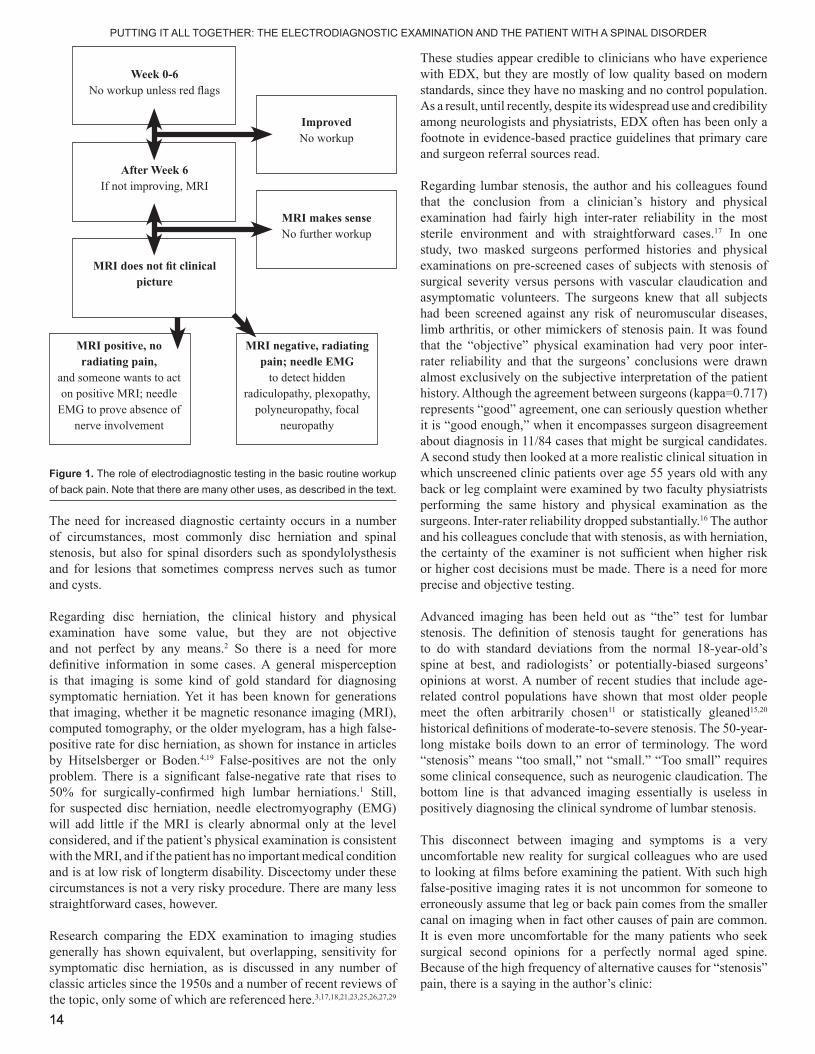
In general, EDX is useful when the diagnostic certainty is not sufficient to justify the risk of a next treatment step, and when it has a possibility of changing diagnostic certainty. EDX is useful when it can determine the severity of a lesion and that documentation of severity certainty improves the outcome. EDX is useful when it can predict the course of disease over time, whether it be natural history or the response to intervention, and where that knowledge will change the outcome. EDX is useful when it provides helpful data for research on spinal disorders. Figure 1 shows a basic framework for the routine use of EDX testing. There are many other uses, however.
1414
PUTTING IT ALL TOGETHER: THE ELECTRODIAGNOSTIC EXAMINATION AND THE PATIENT WITH A SPINAL DISORDER
The need for increased diagnostic certainty occurs in a number of circumstances, most commonly disc herniation and spinal stenosis, but also for spinal disorders such as spondylolysthesis and for lesions that sometimes compress nerves such as tumor and cysts.
Regarding disc herniation, the clinical history and physical examination have some value, but they are not objective and not perfect by any means.2 So there is a need for more definitive information in some cases. A general misperception is that imaging is some kind of gold standard for diagnosing symptomatic herniation. Yet it has been known for generations that imaging, whether it be magnetic resonance imaging (MRI), computed tomography, or the older myelogram, has a high false-positive rate for disc herniation, as shown for instance in articles by Hitselsberger or Boden.4,19 False-positives are not the only problem. There is a significant false-negative rate that rises to 50% for surgically-confirmed high lumbar herniations.1 Still, for suspected disc herniation, needle electromyography (EMG) will add little if the MRI is clearly abnormal only at the level considered, and if the patient’s physical examination is consistent with the MRI, and if the patient has no important medical condition and is at low risk of longterm disability. Discectomy under these circumstances is not a very risky procedure. There are many less straightforward cases, however.
Research comparing the EDX examination to imaging studies generally has shown equivalent, but overlapping, sensitivity for symptomatic disc herniation, as is discussed in any number of classic articles since the 1950s and a number of recent reviews of the topic, only some of which are referenced here.3,17,18,21,23,25,26,27,29
These studies appear credible to clinicians who have experience with EDX, but they are mostly of low quality based on modern standards, since they have no masking and no control population. As a result, until recently, despite its widespread use and credibility among neurologists and physiatrists, EDX often has been only a footnote in evidence-based practice guidelines that primary care and surgeon referral sources read.
Regarding lumbar stenosis, the author and his colleagues found that the conclusion from a clinician’s history and physical examination had fairly high inter-rater reliability in the most sterile environment and with straightforward cases.17 In one study, two masked surgeons performed histories and physical examinations on pre-screened cases of subjects with stenosis of surgical severity versus persons with vascular claudication and asymptomatic volunteers. The surgeons knew that all subjects had been screened against any risk of neuromuscular diseases, limb arthritis, or other mimickers of stenosis pain. It was found that the “objective” physical examination had very poor inter-rater reliability and that the surgeons’ conclusions were drawn almost exclusively on the subjective interpretation of the patient history. Although the agreement between surgeons (kappa=0.717) represents “good” agreement, one can seriously question whether it is “good enough,” when it encompasses surgeon disagreement about diagnosis in 11/84 cases that might be surgical candidates. A second study then looked at a more realistic clinical situation in which unscreened clinic patients over age 55 years old with any back or leg complaint were examined by two faculty physiatrists performing the same history and physical examination as the surgeons. Inter-rater reliability dropped substantially.16 The author and his colleagues conclude that with stenosis, as with herniation, the certainty of the examiner is not sufficient when higher risk or higher cost decisions must be made. There is a need for more precise and objective testing.
Advanced imaging has been held out as “the” test for lumbar stenosis. The definition of stenosis taught for generations has to do with standard deviations from the normal 18-year-old’s spine at best, and radiologists’ or potentially-biased surgeons’ opinions at worst. A number of recent studies that include age-related control populations have shown that most older people meet the often arbitrarily chosen11 or statistically gleaned15,20
historical definitions of moderate-to-severe stenosis. The 50-year-long mistake boils down to an error of terminology. The word “stenosis” means “too small,” not “small.” “Too small” requires some clinical consequence, such as neurogenic claudication. The bottom line is that advanced imaging essentially is useless in positively diagnosing the clinical syndrome of lumbar stenosis.
This disconnect between imaging and symptoms is a very uncomfortable new reality for surgical colleagues who are used to looking at films before examining the patient. With such high false-positive imaging rates it is not uncommon for someone to erroneously assume that leg or back pain comes from the smaller canal on imaging when in fact other causes of pain are common. It is even more uncomfortable for the many patients who seek surgical second opinions for a perfectly normal aged spine. Because of the high frequency of alternative causes for “stenosis” pain, there is a saying in the author’s clinic:
Week 0-6 No workup unless red flags
ImprovedNo workup
MRI makes senseNo further workup
After Week 6If not improving, MRI
MRI does not fit clinical picture
MRI positive, no radiating pain,
and someone wants to act on positive MRI; needle
EMG to prove absence of nerve involvement
MRI negative, radiating pain; needle EMG
to detect hidden radiculopathy, plexopathy,
polyneuropathy, focal neuropathy
Figure 1. The role of electrodiagnostic testing in the basic routine workup of back pain. Note that there are many other uses, as described in the text.

15
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
15
Nobody with stenosis goes to surgery until you:
• Poke the troch
• Whip the hip
• Upset the facet
• And smack the sacroiliac
These four pain generators (i.e., the trochanter, the hip joint, the facet joints, and the sacroiliac joints), along with polyneuropathy, are common causes of pain that mimics stenosis. Even when a person does have clinical stenosis, their disabling pain sometimes comes from one of these nonsurgical disorders.
There is compelling evidence that EDX is able to positively diagnose clinically evident lumbar spinal stenosis. The author’s group first used the prevailing gold standard of requiring an imaging abnormality combined with a clinical syndrome, and they improved on it by having the radiologist masked and requiring a masked comprehensive clinical history and physical examination conducted by a subspecialist physiatrist. They further added a review of the data by a masked senior spine surgeon to ensure that there was no question of the diagnosis. Interestingly, of 149 cases, agreement between the three physicians regarding the status of stenosis, mechanical back pain, or asymptomatic volunteer occurred in only 55 subjects. In that group, a paraspinal mapping EMG score of >4 was 100% specific (when positive, the subject had stenosis).9 Inexplicably, the study was not cited in subsequent evidence-based reviews.
In a study of the larger population (126 subjects eventually qualified), a paraspinal mapping score of greater than 4 discriminated those with stenosis from the others with a statistical significance of p<0.05.15 No MRI parameter had any statistically significant discriminant value. A paraspinal mapping EMG score of greater than 4 had an 86-90% specificity and 33% sensitivity for detecting stenosis compared to either the back pain or asymptomatic groups (each p<0.04). A composite limb and paraspinal fibrillation score had a sensitivity of 47.8% and specificity of 87.5%, p=0.008; and H-wave sensitivity was 36.4% with a specificity of 91.3%, p=0.026, for stenosis versus all control subjects. A subsequent study by Yagci’s group in Turkey used paraspinal mapping and a limited limb examination in what appeared to be a more severely involved surgical population, and they found both sensitivity and specificity to be over 90%.30
Another analysis of this group looked at the overall impression of the diagnostician.11 The radiologist’s impression again was useless (p>0.80). The impression of the masked EDX physicians was not so useful either. The problem was due almost exclusively to one error: the EDX physicians held on to the old belief that any paraspinal finding is abnormal, despite the fact that it has been established that asymptomatic volunteers can have fibrillations and that these increase with age. When the 95% confidence interval value established for paraspinal mapping scores for older persons (a paraspinal mapping score of greater than 4) was imposed on the EDX physician’s impression, the final EDX conclusion became significantly diagnostic. The critical lesson
is that arbitrary exploration or interpretation of paraspinal EMG invalidates the results.
EDX evaluation is not only useful for positively diagnosing radiculopathy. It can detect alternative diagnoses or diagnoses that impact treatment. The previously mentioned study of persons with clinical stenosis, asymptomatic volunteers, and persons with mechanical back pain included screening questions to eliminate the risk of polyneuropathy and a comprehensive study history and physical examination. Yet 8 of 149 subjects were found on needle EMG alone to have a neuromuscular disease that could mimic spinal stenosis.15 In other cases clinical stenosis may still be present, but the presence of a polyneuropathy can impact surgical outcomes.5
Good clinicians worry about missing cancer and infections of the spine. So they order MRI scans at some point. While, in general, MRI is quite good at detecting spinal tumors, needle EMG is pretty good, too, as noted during the days prior to noninvasive spinal imaging.22 In addition, spinal imaging can never detect radicular pain from pelvic tumors or other lesions more distally. Furthermore, a plain X-ray plus sedimentation rate are considered sufficient to rule out tumors and infections in persons with acute pain and red flags. It seems that, with more modern research and some relief from medicolegal stressors American physicians might also find that needle EMG and ancillary tests detect more “maladies” than spine MRI, with less cost. Today, the important message to colleagues who work in low-resource regions is that they should not feel too compromised when they use the less expensive workup of EDX and X-ray and sedimentation rate instead of the expensive and often unavailable MRI.
A number of common spinal diagnoses can be found on paraspinal EMG, sometimes leading to change in treatment. Failed back surgery syndrome after fusion appears to be more about the surgical technique than the patient, since these patients have higher paraspinal mapping scores than those with good recovery.28 Radiofrequency ablation of the posterior primary ramus is increasingly used to relieve facet joint pain. When it fails to relieve pain, paraspinal mapping EMG can determine whether the procedure was technically adequate at a segment-to-segmental level, allowing clinicians to consider or reject repeating the procedure.12 Other presentations for this course address the use of needle EMG to target spinal injections with improved outcomes.
Unusual disorders are obvious on careful needle EMG, but the examiner needs to be aware of them. The bent spine syndrome, a paraspinal myopathy, sounds clinically a lot like lumbar stenosis, since the patient’s back fatigues with walking or standing. While it can be seen as “whiting out” of the paraspinal muscles on MRI, radiologists almost always miss it. It is more common than one would think. The author has found it often enough on needle EMG when paraspinal mapping results in a “fatty” feel during insertion through the multifidus muscle.10 The hallmark of a paraspinal compartment syndrome, which usually presents as severe back pain after abdominal surgery, is multisegmental sensory loss in the low back. However, paraspinal EMG will also indicate that there is severely increased insertional activity (e.g., 4+ fibrillations) around the edges with decreased or fibrotic findings in the center of the muscle.14 Finally, with a more specific and sensitive paraspinal
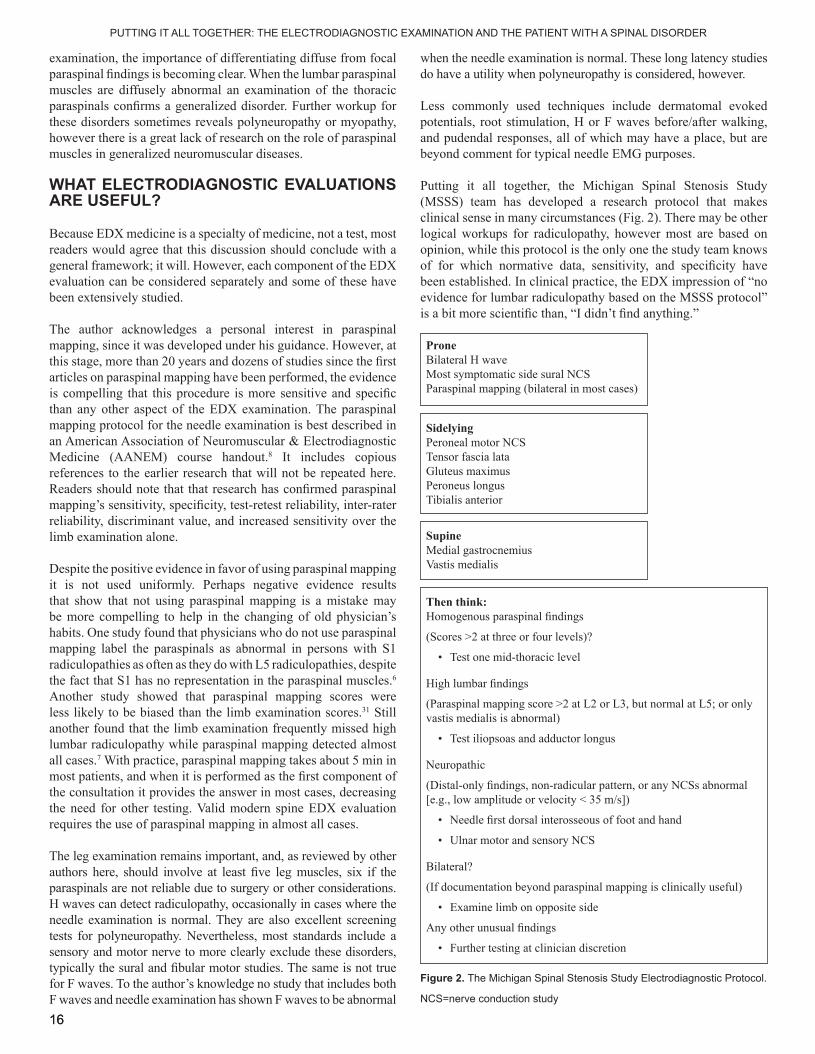
1616
examination, the importance of differentiating diffuse from focal paraspinal findings is becoming clear. When the lumbar paraspinal muscles are diffusely abnormal an examination of the thoracic paraspinals confirms a generalized disorder. Further workup for these disorders sometimes reveals polyneuropathy or myopathy, however there is a great lack of research on the role of paraspinal muscles in generalized neuromuscular diseases.
WHAT ELECTRODIAGNOSTIC EVALUATIONS ARE USEFUL?
Because EDX medicine is a specialty of medicine, not a test, most readers would agree that this discussion should conclude with a general framework; it will. However, each component of the EDX evaluation can be considered separately and some of these have been extensively studied.
The author acknowledges a personal interest in paraspinal mapping, since it was developed under his guidance. However, at this stage, more than 20 years and dozens of studies since the first articles on paraspinal mapping have been performed, the evidence is compelling that this procedure is more sensitive and specific than any other aspect of the EDX examination. The paraspinal mapping protocol for the needle examination is best described in an American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) course handout.8 It includes copious references to the earlier research that will not be repeated here. Readers should note that that research has confirmed paraspinal mapping’s sensitivity, specificity, test-retest reliability, inter-rater reliability, discriminant value, and increased sensitivity over the limb examination alone.
Despite the positive evidence in favor of using paraspinal mapping it is not used uniformly. Perhaps negative evidence results that show that not using paraspinal mapping is a mistake may be more compelling to help in the changing of old physician’s habits. One study found that physicians who do not use paraspinal mapping label the paraspinals as abnormal in persons with S1 radiculopathies as often as they do with L5 radiculopathies, despite the fact that S1 has no representation in the paraspinal muscles.6 Another study showed that paraspinal mapping scores were less likely to be biased than the limb examination scores.31 Still another found that the limb examination frequently missed high lumbar radiculopathy while paraspinal mapping detected almost all cases.7 With practice, paraspinal mapping takes about 5 min in most patients, and when it is performed as the first component of the consultation it provides the answer in most cases, decreasing the need for other testing. Valid modern spine EDX evaluation requires the use of paraspinal mapping in almost all cases.
The leg examination remains important, and, as reviewed by other authors here, should involve at least five leg muscles, six if the paraspinals are not reliable due to surgery or other considerations. H waves can detect radiculopathy, occasionally in cases where the needle examination is normal. They are also excellent screening tests for polyneuropathy. Nevertheless, most standards include a sensory and motor nerve to more clearly exclude these disorders, typically the sural and fibular motor studies. The same is not true for F waves. To the author’s knowledge no study that includes both F waves and needle examination has shown F waves to be abnormal
when the needle examination is normal. These long latency studies do have a utility when polyneuropathy is considered, however.
Less commonly used techniques include dermatomal evoked potentials, root stimulation, H or F waves before/after walking, and pudendal responses, all of which may have a place, but are beyond comment for typical needle EMG purposes.
Putting it all together, the Michigan Spinal Stenosis Study (MSSS) team has developed a research protocol that makes clinical sense in many circumstances (Fig. 2). There may be other logical workups for radiculopathy, however most are based on opinion, while this protocol is the only one the study team knows of for which normative data, sensitivity, and specificity have been established. In clinical practice, the EDX impression of “no evidence for lumbar radiculopathy based on the MSSS protocol” is a bit more scientific than, “I didn’t find anything.”
ProneBilateral H waveMost symptomatic side sural NCSParaspinal mapping (bilateral in most cases)
SidelyingPeroneal motor NCSTensor fascia lataGluteus maximusPeroneus longusTibialis anterior
Then think:Homogenous paraspinal findings
(Scores >2 at three or four levels)?
• Test one mid-thoracic level
High lumbar findings
(Paraspinal mapping score >2 at L2 or L3, but normal at L5; or only vastis medialis is abnormal)
• Test iliopsoas and adductor longus
Neuropathic
(Distal-only findings, non-radicular pattern, or any NCSs abnormal [e.g., low amplitude or velocity < 35 m/s])
• Needle first dorsal interosseous of foot and hand
• Ulnar motor and sensory NCS
Bilateral?
(If documentation beyond paraspinal mapping is clinically useful)
• Examine limb on opposite side
Any other unusual findings
• Further testing at clinician discretion
SupineMedial gastrocnemiusVastis medialis
Figure 2. The Michigan Spinal Stenosis Study Electrodiagnostic Protocol.
NCS=nerve conduction study
PUTTING IT ALL TOGETHER: THE ELECTRODIAGNOSTIC EXAMINATION AND THE PATIENT WITH A SPINAL DISORDER

17
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
17
WHAT DON’T WE KNOW?
There is a whole lot we don’t know. Despite the age-old concept that recovery from radiculopathy occurs proximally-to-distally, there is still no case series following recovery from radiculopathy aside from the author and his colleagues’ 18 month followup on stenosis subjects.13 So, in the face of decades-old folklore that recovery from radiculopathy occurs in the paraspinals and progresses over unknown timeframes down the leg, physicians are unable to characterize neurological recovery from herniation or its relationship to pain and disability. It is suspected that, with modern microdiscectomy, a range of normal for the paraspinals may be found. This information would help detect new lesions in persons who had previous surgery. However, no study has been forthcoming. No credible, validated technique with norms has been devised for the cervical paraspinal muscles, which are much more complex than the lumbar muscles. Even a straightforward comparative study of needle EMG to MRI in diagnosing herniated disk, including asymptomatic control subjects (some of whom will have herniations on MRI), has not yet been initiated.
The big question is whether the information elicited through the EDX examination can change the course of disease. The answer to this question requires prospective trials. These are very difficult to get funded, partly because review groups for spinal disorders typically are comprised of engineers, physiologists, therapists, or surgeons who equate diagnostic EMG with surface EMG. A recent application to the National Institutes of Health went as far as to include a primer on EDX. Still, it was criticized for not accounting the effect of “muscle relaxants” and not looking at fatigue and muscle coordination, none of which have anything to do with diagnostic EMG.24 If the EDX examination is to be shown to be of value policymakers and scientists outside the field need to have a better understanding of exactly what it is.
Notwithstanding the severe limitations of the masked, randomized controlled trials of the 20th century, they do provide a confident justification for EDX in spinal disorders. This document reviews some of that scientific justification, but it goes beyond the gathered facts to impose them within a rational framework.
The danger is to assume—as clinicians, scientists, and policymakers of the 20th century did— that this recursive approach is not scientific. In fact, it is imminently researchable. In a process akin to the development of the English legal system, qualitative studies can probe deep into the myriad details of good practice and find commonalities between expert practitioners. Research trials (even those randomized, controlled trials) can then study the outcomes from pathways of care rather than individual events at single points in time.
Medicine is scientific. For EDX and spinal disorders the best science—the science that embraces the known truth of individual variability—is yet to come. This document sets a framework for that science, and it proposes a place for EDX in the practice of today’s clinicians.
1818
REFERENCES
1. Albert TJ, Balderston RA, Heller JG, Herkowitz HN, Garfin SR, Tomany K, An HS, Simeone FA. Upper lumbar disk herniations. J Spinal Disord 1993;6(4):351-359.
2. Al Nezari NH, Schneiders AG, Hendrick PA. Neurological examination of the peripheral nervous system to diagnose lumbar spinal disk herniation with suspected radiculopathy: a systematic review and meta-analysis. Spine 2013;13:657-674.
3. Barr K. Electrodiagnosis of lumbar radiculopathy. P M R Clin N A 2013;24(1):79-91.
4. Boden S, et al. Abnormal magnetic resonance scans of the lumbar spine in asymptomatic subjects. J Bone Joint Surg 1990;72A:403-408.
5. Cinotti G, Postacchini F, Weinstein JN. Lumbar spinal stenosis and diabetes. Outcome of surgical decompression.bJ Bone Joint Surg Br 1994;76(2):215-219.
6. Haig AJ, Levine JW, Ruan CM, Yamakawa K. Describing paraspinal EMG findings: inadequacy of the single 0-4+ score. Am J Phys Med Rehab 2000;79:133-137.
7. Haig AJ, Yamakawa K, Hudson DM. Paraspinal electromyography in high lumbar and thoracic lesions. Am J Phys Med Rehabil 2000;79(4):336-342.
8. Haig AJ. Paraspinal mapping. American Association of Electrodiagnostic Medicine Workshop Handout (peer reviewed and published as a separate document). Rochester MN: AAEM; 2000. Revised 2005.
9. Haig AJ, Tong HC, Yamakawa KS, Quint DJ, Hoff JT, Chiodo A, Miner JA, Choksi VR, Geisser ME. The sensitivity and specificity of electrodiagnostic testing for the clinical syndrome of lumbar spinal stenosis. Spine 2005;30(23):2667-2676.
10. Haig AJ, Tong HC, Kendall R. The bent spine syndrome: myopathy + biomechanics = symptoms. Spine 2006;6(2):190-194.
11. Haig AJ, Tong HC, Yamakawa KSJ, Quint DJ, Hoff JT, Chiodo A, Miner JA, Choksi VR, Geisser ME. Spinal stenosis, back pain, or no symptoms at all? A masked study comparing radiologic and electrodiagnostic diagnoses to the clinical impression. Arch Phys Med Rehabil 2006;87(7) 897-903.
12. Haig AJ, Smuck M. Paraspinal mapping electromyography to verify radiofrequency facet denervation. Third annual meeting; China Orthopedic Association, Suzhou, China, 2008.
13. Haig AJ, Yamakawa KS, Parres C, Chiodo A, Tong HC. A prospective, masked 18 month minimum follow-up on neurophysiologic changes in persons with spinal stenosis, low back pain, and no symptoms. PM R 2009;1(2):127-136.
14. Haig AJ. Hartigan AG. Quint D. Low back pain after nonspinal surgery: the characteristics of presumed lumbar paraspinal compartment syndrome. PM R 2009;1(4):383-388.
15. Haig AJ, Geisser ME, Tong HC, Yamakawa KS, Quint DJ, Hoff JT, Chiodo A, Miner JA, Phalke VV. Electromyographic and magnetic resonance imaging to predict lumbar stenosis, low-back pain, and no back symptoms. J Bone Joint Surg Am 2007;89(2):358-366.
16. Haig AJ, Yamakawa KSJ, Yarjanian J, Hartigan A. Inter-rater reliability of physiatrists in diagnosing neurogenic claudication under an unconstrained clinical situation. AAPMR 2012.
17. Haig AJ, Park P, Henke P, Yamakawa KSJ, Valdivia J, Tomkins C, Loar S. The reliability of the clinical diagnosis in persons offered surgery for lumbar spinal stenosis. Spine: in press.
18. Hakimi K. Spanier D. Electrodiagnosis of cervical radiculopathy. PM R Clin N Am 24(1):1-12, 2013.
19. Hitselberger WE, Witten RM. Abnormal myelograms in asymptomatic patients. J Neurosurg 1968;28:204-206.
20. Kalichman L, Cole R, Kim DH, et al. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J 2009;9(7):545-550.
21. Knuttson B. Comparative value of electromyographic, myelographic, and clinical-neurological examinations in the diagnosis of lumbar root compression syndrome. Acta Orthop Scand 1961;(suppl 49):1-134.
22. LaBan MM, Grant AE. Occult spinal metastases—early electromyographic manifestation. Arch Phys Med Rehabil 1971;52(5):223-226.
23. Levin KH. Approach to the patient with suspected radiculopathy. Neurol Clin 2012;30(2):581-604.
24. National Institutes of Health. Review of 1R01AR056132-01A1. Denervation in Symptomatic and Asymptomatic Disk Herniation.
25. Plastaras CT, Joshi AB.The electrodiagnostic evaluation of neck pain. Phys Med Rehabil Clin N Am 2011;22(3):429-438, viii.
26. Plastaras CT, Joshi AB. The electrodiagnostic evaluation of radiculopathy. Phys Med Rehabil Clin N Am 2011;22(1):59-74.
27. Shea PA, Woods WW, Werden DH. Electromyography in diagnosis of nerve root compression syndrome. Arch Neurol Psychiat 1950;64:93.
28. Sihvonen T, Herno A, Paljarvi L, Airaksinen O, Partanen J, Tapaninaho A. Local denervation atrophy of paraspinal muscle in postoperative failed back syndrome. Spine 1993;18(5):575-581.
29. Wilbourne AJ, Aminoff MJ. AAEM Minimonograph #32: The electrophysiologic examination in patients with radiculopathies. Muscle Nerve 1988;11(11):1101-1114.
30. Yagci I, Gunduz OH, Ekinci G, Diracoglu D, Us O, Akyuz G. The utility of lumbar paraspinal mapping in the diagnosis of lumbar spinal stenosis. Am J Phys Med Rehabil 2009;88(10):843-851.
31. Yamakawa KSJ, Haig AJ, Geisser ME, Tong HC, Chiodo A, Miner J. The clinician effect on “objective” technical components of the electrodiagnostic consultation. Am J Phys Med Rehabil 2007;86(5):364-372.
PUTTING IT ALL TOGETHER: THE ELECTRODIAGNOSTIC EXAMINATION AND THE PATIENT WITH A SPINAL DISORDER
19
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
19
INTRODUCTION
Lumbar spinal disorders contribute significantly to the health and socioeconomic problems encountered throughout Western countries. A review of the total cost associated with low back pain (LBP) in the United States performed in 2006 revealed it to be in excess of $100 billion per year, two-thirds of which were a result of lost wages and reduced productivity.8 In the setting of rising healthcare costs, clinicians today are faced with choosing among numerous assessment and treatment options for patients presenting with lumbar spinal disorders. Diagnostic studies therefore are optimally used if they: (1) are strongly correlated with clinical presentation and functional disability, (2) critically influence treatment plan decisions, or (3) are predictive of outcomes.
This review will focus mainly on two common disorders of the lumbar spine with neurological manifestations—lumbosacral radiculopathy (LSR) and lumbar spinal stenosis (LSS)—and on two commonly used diagnostic modalities—the electrodiagnostic (EDX) evaluation and magnetic resonance imaging (MRI).
ELECTRODIAGNOSIS
The historical lack of research examining the prognosticating role of EDX medicine and its ability to improve patient outcomes and lower healthcare costs in patients with painful lumbar spine disorders likely led to the exclusion of EDX medicine as one of the decisionmaking variables from the 1994 spine treatment guidelines (published by an agency now known as the Agency for
Healthcare Research and Quality). However, since then, several studies have better established the utility of the EDX examination in the evaluation and management of patients with lumbar spinal disorders.
An accurate diagnosis of radiculopathy is important in implementing appropriate and timely treatments.6 However, in addition to correctly identifying radiculopathies, EDX evaluation also can provide further details regarding the pathology (e.g., an axonal versus a demyelinating lesion) as well as the severity of the diagnosis, which has important implications with prognostication.In patients with a clinically determined diagnosis of LSR, based on history and physical examination, the EDX evaluation was found to be better correlated with clinical symptoms and functional disability than MRI.14 Specificity and sensitivity of the EDX examination and MRI in the diagnostic evaluation of LSR were compared and EDX examination was found to be more specific in predicting physical examination findings and better correlated with muscle weakness than MRI. However, in patients without clear findings of radiculopathy (based on history, physical examination, and/or imaging), an EDX evaluation can perhaps prove most useful in correctly identifying a radiculopathy. Charles Cho and colleagues6 summarize this point best by stating, “In those cases with negative imaging findings or atypical clinical presentations, EDX evaluation is especially useful; whereas, in those with abnormal imaging findings, it serves as a complementary diagnostic role.”
Effective Use of Diagnostic Studies in Optimizing Patient Management
Thiru M. Annaswamy, MD, MA Associate Professor, Department of Physical Medicine & Rehabilitation
University of Texas Southwestern Medical Center at DallasStaff Physician, VA Medical Center
Dallas, TX

2020
LSR is a complex disorder, and hence it has been historically difficult to identify independent predictors of outcome for nonsurgical and surgical treatments in the management of painful radiculopathy.3 LSR can occur from mechanical compression of the nerve root due to various conditions, including herniated lumbar intervertebral disc, spondylolisthesis, stenosis, or facet arthropathy; however, LSR can also occur without direct nerve root compression when there is a stretch injury or chemical irritation of the roots, the latter possibly from the release of phospholipase A2 and other pro-inflammatory substances, leading to nerve root inflammation and edema.1,19
Epidural steroid injection (ESI) has become a very commonly used intervention in the management of lumbosacral radicular pain in the United States.16 Lumbar ESIs (LESI) are widely regarded as effective treatments for LSR, providing improvement in both pain and mobility.17 The utility of needle electromyography (EMG) as a prognostic tool for LESI outcomes has been studied. A review of the literature reveals a few recent studies that have evaluated the ability of needle EMG to predict outcomes after LESI.
In a retrospective study, Fish and colleagues10 examined the predictive value of needle EMG on improvements in pain and functional outcomes following transforaminal ESI (TFESI) in patients with LSR. The Oswestry Disability Index (ODI) for functional outcome and current pain severity were used to evaluate patient responses. A needle EMG examination was performed in a standard fashion by one experienced EDX physician in one laboratory. The standard criteria was that two muscles innervated by two nerves from the same myotomal level needed to be abnormal to achieve a diagnosis of radiculopathy. Positive findings included denervation or reinnervation changes found on needle EMG. Negative radiculopathy was defined as the absence of denervation or reinnervation changes on needle EMG. Subjects had their needle EMG before TFESI at L4 and/or L5, and they had symptomatic pain in only one extremity. Patients with needle EMG-positive radiculopathy had significantly better improvement in ODI scores (7.11±9.5) compared with a negative needle EMG (3.2±17.4; p<0.05). Pain improvement, however, was not significantly different in the positive needle EMG group (1.8±1.2) compared with the negative needle EMG group (1.2±1.2; p<0.05). The limitations of this study included its retrospective design and the lack of clear differentiation as to how many subjects were diagnosed with radiculopathy based on acute findings (e.g., positive sharp waves and fibrillations) as opposed to chronic findings. Another limitation is that multiple regression analysis was not performed to evaluate for other predictors of outcome.
Marchetti and colleagues17 reported results of a retrospective chart review of patients who had LESI (either caudal, interlaminar, or transforaminal) after needle EMG. They found no differences among the needle EMG-positive, needle EMG-negative, and equivocal groups in their response rates to LESI. The mean leg and back pain scores improved significantly in all three groups after undergoing ESI, but there was no significant difference identified in pain improvement post ESI with respect to needle EMG findings. Based on this, the investigators concluded that patients with a negative needle EMG should not be excluded from a trial of LESI. However, there were several limitations
of this study, which were primarily related to its retrospective methodology and its failure to use a multiple regression analysis to evaluate for other independent predictors of outcome.
Cosgrove and collagues studied the EDX examination and other predictors of a successful response to LESIs in patients with LSR.7 Their study was rigorous with the use of prospective study design, multivariate regression analysis, and an objective EDX definition of radiculopathy by including only abnormal spontaneous activity such as positive sharp waves and fibrillation potentials in their determination of abnormality. However, their study included only 16 subjects, and only 1 subject had an abnormal EDX examination consistent with LSR, thereby limiting the judgment on whether the EDX evaluation has strong predictive ability for outcomes after LESI.7
The study by Annaswamy and colleagues3 reported the results of a prospective, multiple regression study evaluating the independent predictive ability of needle EMG in determining outcomes after lumbar interlaminar ESI in patients with clinical LSR, as well as the role of needle EMG findings and their interactions with other psychosocial and functional variables in determining patient response to LESI. Data were collected from more than 80 subjects who had their needle EMG prior to undergoing interlaminar ESI under fluoroscopic guidance at a level as close to the suspected level of pathology as feasible.3 The investigators found that an abnormal needle EMG consistent with the EDX impression of LSR moderately predicted longterm improvement in pain after LESI. Positive EDX evidence of LSR was predictive of statistically significant better improvement in both pain and functional scores when compared with negative EDX evidence of LSR, although the patients with a normal needle EMG also tended to favorably respond to LESI. A regression model, including needle EMG and several other independent predictors, was predictive of pain and functional outcomes. The authors concluded that their findings indicate that needle EMG findings can be a useful tool to identify and select the subset of patients who are more likely to respond more favorably to LESI. This is similar to the conclusion obtained by Fish and colleagues in their retrospective study.10 However, although most of the studies described above suggest that a positive needle EMG is predictive of better outcome than negative a needle EMG, they also suggest that several other variables need to be analyzed and considered when advising patients regarding potential benefits of ESI in the treatment of LSR.3,7,10,17
Needle EMG has also been studied for its outcome prediction after lumbar spine surgery for LSR. Spengler and colleagues used a multiple regression model to analyze the utility of components of preoperative evaluation, including needle EMG, for prediction of operative findings and clinical outcome.22 Only 39% of the total variability in the operative findings could be explained by this regression model. Needle EMG was positive in 70% of those subjects who underwent the study and was one of the predictor variables in the model, but its value as an independent predictor of surgical outcome was not assessed. Another study compared the outcome of patients treated surgically versus those treated nonsurgically and found that an initial needle EMG had no prognostic ability to predict outcome at 5 years, which was influenced mostly by psychosocial factors.9
EFFECTIVE USE OF DIAGNOSTIC STUDIES IN OPTIMIZING PATIENT MANAGEMENT

21
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
21
The above research studies support the prognosticating role of the EDX evaluation in patients with LSR. EDX information can help clinicians more accurately and reliably advise patients regarding the appropriate course of action when choosing among several treatment options including ESI.2 EDX assessment can be useful to help appropriately select patients for ESI as well as to identify patients who may not benefit from nonsurgical management so that they can then be considered for surgical intervention. However, some still contend that EDX medicine’s main strength lies in its ability to diagnose physiologic function of the nerve root, rather than predicting surgical outcomes.4
MAGNETIC RESONANCE IMAGING
MRI is used as a standard tool for initial patient imaging evaluation, even though MRI has been shown to be too sensitive to intervertebral disc abnormality and cannot distinguish between symptomatic and asymptomatic findings.18
One review article looked at 12 different studies intended to identify patients who benefit from ESI.5 Chronic LBP patients with one or more of the following characteristics were studied: sciatica, positive neurogenic signs, lumbar radiculopathy, postlaminectomy pain, and positive radiological findings of spinal stenosis and nerve root compression. Subjects who had positive outcome with ESI (series of three injections at 7-day intervals) had the following characteristics: sciatica, LBP for 6 to 12 months, and positive MRI findings of disc bulge and/or spinal stenosis.
Another study evaluated 149 patients with excellent or poor outcomes after TFESI for LSR caused by herniated disc. They found that disc herniations in the foraminal or extraforaminal zone were associated with better outcomes than disc herniations in the central or subarticular zones. Other MRI findings such as disc degenerative changes, T2-weighted signal changes, Modic change, disc height loss, grade of disc degeneration, and presence of osteophytes were not statistically significant.15
Ghahreman and Bogduk in 2011 reported a study in which they attempted to identify clinical and radiological features that predict response to TFESI for LSR due to disc herniation.11 They analyzed several variables including neurologic symptoms and signs, duration of symptoms, and MRI findings. They found that only an MRI finding of a low grade of nerve root compression correlated with excellent outcomes after TFESI.11
Jensen and colleagues in 2007 published a prospective observational study of 154 patients with sciatica receiving active nonsurgical treatment.12 In the multivariate analyses, broad-based protrusions, extrusions, and male sex were found to be predictive of a good outcome, defined as an absence of sciatic leg pain and a Roland Morris disability score of 3 or less at 14-month followup.12
MRI is useful in the diagnosis of LSS and in determining the neuroanatomy of the spine. However, it is yet unclear how useful MRI is in treatment planning or predicting outcome. Sirvanci and colleagues evaluated 63 patients undergoing surgery for LSS out of which 27 had severe and 33 had moderate central canal stenosis, 11 had severe and 27 had moderate lateral recess stenosis, and 22 had severe and 31 had moderate foraminal
stenosis.21 Functionally, 10 of them were mildly impaired, 13 were moderately impaired, 25 were severely impaired, 12 were crippled, and 3 were bedridden. The authors found no correlation between disability and stenosis scores.21 On the other hand, in Sigmundsson and colleagues’ prospective study looking at predictors of outcome after spine surgery (decompression without fusion) found that an MRI finding of narrow dural sac predicted better improvement in back and absolute leg pain, along with other pre-operative clinical variables.20
Kapural and colleagues evaluated how MRI findings predicted improvement after LESI in patients with LSS. In this retrospective study, improvement in pain scores was correlated with an index that factors in the number of levels stenosed and the severity of stenosis.13 Patients with more than 3 levels affected had the worst outcome with LESI.
The above research studies establish the utility of MRI in patients with LSR and LSS. The anatomic information from an MRI can help clinicians more accurately diagnose patients; however, several other factors including demographic, clinical presentation, and electrophysiological studies need to be weighed in as well before choosing among several treatment options. MRI can be useful to make appropriate patient selection for nonsurgical management options such as ESI or physical therapy, as well as to identify patients who may not benefit from nonsurgical management so that they can then be considered for surgical intervention. However, most agree that MRI’s primary utility lies in its ability to anatomically diagnose the abnormalities in the lumbar spine and the spinal nerves, rather than predicting outcomes.

22
REFERENCES
1. An HS, Anderson PA, Haughton VM, Iatridis JC, Kang JD, Lotz JC, Natarajan RN, Oegema TR, Jr., Roughley P, Setton LA, Urban JP, Videman T, Andersson GB, Weinstein JN. Introduction: disc degeneration: summary. Spine 2004;29(23):2677-2678.
2. Annaswamy TM, Bierner SM, Avraham R. Role of electrodiagnosis in patients being considered for epidural steroid injections. PMR 2013;5(5 Suppl):S96-S99.
3. Annaswamy TM, Bierner SM, Chouteau W, Elliott AC. Needle electromyography predicts outcome after lumbar epidural steroid injection. Muscle Nerve 2012;45(3):346-355.
4. Barr K. Electrodiagnosis of lumbar radiculopathy. Phys Med Rehabil Clin N Am 2013;24(1):79-91.
5. Bogduk N, Brazenor G, Christophides N, Cherry D, Fraser R, Jenkins J. Epidural steroids in the management of low back pain and sciatica of spinal origin. Report of the working party. Sydney: National Health and Medical Research Council; 1993. pp 102-106.
6. Charles Cho S, Ferrante MA, Levin KH, Harmon RL, So YT. Utility of electrodiagnostic testing in evaluating patients with lumbosacral radiculopathy: an evidence-based review. Muscle Nerve 2010;42(2):276-282.
7. Cosgrove JL, Bertolet M, Chase SL, Cosgrove GK. Epidural steroid injections in the treatment of lumbar spinal stenosis efficacy and predictability of successful response. Am J Phys Med Rehabil 2011;90(12):1050-1055.
8. Crow WT, Willis DR. Estimating cost of care for patients with acute low back pain: a retrospective review of patient records. J Am Osteopath Assoc 2009;109(4): 229-233.
9. Falck B, Nykvist F, Hurme M, Alaranta H. Prognostic value of EMG in patients with lumbar disc herniation--a five year follow up. Electromyogr Clin Neurophysiol 1993;33(1):19-26.
10. Fish DE, Shirazi EP, Pham Q. The use of electromyography to predict functional outcome following transforaminal epidural spinal injections for lumbar radiculopathy. J Pain 2008;9(1):64-70.
11. Ghahreman A, Bogduk N. Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation. Pain Med 2011;12(6):871-879.
12. Jensen TS, Albert HB, Sorensen JS, Manniche C, Leboeuf-Yde C. Magnetic resonance imaging findings as predictors of clinical outcome in patients with sciatica receiving active conservative treatment. J Manipulative Physiol Ther 2007;30(2):98-108.
13. Kapural L, Mekhail N, Bena J, McLain R, Tetzlaff J, Kapural M, Mekhail M, Polk S. Value of the magnetic resonance imaging in patients with painful lumbar spinal stenosis (LSS) undergoing lumbar epidural steroid injections. Clin J Pain 2007;23(7):571-575.
14. Lee JH, Lee SH. Physical examination, magnetic resonance image, and electrodiagnostic study in patients with lumbosacral disc herniation or spinal stenosis. J Rehabil Med 2012;44(10):845-850.
15. Lee JW, Choi SW, Park SH, Lee GY, Kang HS. MR-based outcome predictors of lumbar transforaminal epidural steroid injection for lumbar radiculopathy caused by herniated intervertebral disc. Eur Radiol 2013;23(1):205-211.
16. Manchikanti L. Medicare in interventional pain management: a critical analysis. Pain Physician 2006;9(3):171-197.
17. Marchetti J, Verma-Kurvari S, Patel N, Ohnmeiss DD. Are electrodiagnostic study findings related to a patient’s response to epidural steroid injection? Pm R 2010;2(11):1016-1020.
18. Nardin RA, Patel MR, Gudas TF, Rutkove SB, Raynor EM. Electromyography and magnetic resonance imaging in the evaluation of radiculopathy. Muscle Nerve 1999;22(2):151-155.
19. Saal JS. The role of inflammation in lumbar pain. Spine 1995;20(16):1821-1827.
20. Sigmundsson FG, Kang XP, Jonsson B, Stromqvist B. Prognostic factors in lumbar spinal stenosis surgery. Acta Orthop 2012;83(5):536-542.
21. Sirvanci M, Bhatia M, Ganiyusufoglu KA, Duran C, Tezer M, Ozturk C, Aydogan M, Hamzaoglu A. Degenerative lumbar spinal stenosis: correlation with Oswestry disability index and MR imaging. Eur Spine J 2008;17(5):679-685.
22. Spengler DM, Ouellette EA, Battie M, Zeh J. Elective discectomy for herniation of a lumbar disc. Additional experience with an objective method. J Bone Joint Surg Am 1990;72(2):230-237.
EFFECTIVE USE OF DIAGNOSTIC STUDIES IN OPTIMIZING PATIENT MANAGEMENT

23
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
23
INTRODUCTION
Most clinical guidelines on the treatment of low back pain (LBP) are directed to the primary care physician. This brief review attempts to summarize the best available evidence for common treatments utilized in North America. The role of the physician specialist who is evaluating a patient with a complaint of LBP and/or leg pain is to achieve a diagnosis when such is possible as well as to rule out alternative diagnoses that are potentially more serious to the patient when necessary, and then to direct treatment in a logical fashion with consideration of the rational utilization of scarce medical resources. While this goal is easy to state, it can be difficult to achieve in practice due to a number of factors outside the physician’s direct control: insurance factors (or lack of any insurance coverage), doctor-shopping patients, unrealistic expectations from an aging cohort of the population, and media coverage of health and sports topics which convey a message of easy solutions or cure when both may be elusive.
METHODOLOGY
Because of the breadth of this topic, a university research librarian was instructed to narrow the search using a defined search strategy and then refining it based on journal impact factor.
For the search strategy in the PubMed website, randomized controlled trials or observational cohort studies were sought, with meta-analyses or systematic reviews being preferred. In addition, the studies need to involve human subjects only, be only in the English language, and have a time frame inclusive of 1999-2013. The search terms used included: back pain, lumbago, lumbar disc herniation, sacroiliac joint, facet or zygapophyseal joint (lumbar), rehabilitation, interdisciplinary rehabilitation, physical therapy
or manual therapy or acupuncture, core strengthening, epidural steroid injection, interventions or interventional spinal, chronic back pain, chronic pain, sciatica or radiculopathy or lumbar radicular syndrome, acute pain, outcomes, discectomy (surgery), lumbar fusion, laminectomy, post-laminectomy syndrome, and psychological aspects.
The initial search yielded 265 articles; this was reduced by using journal impact factor to narrow the search to 94 citations. (Articles from journals with an impact factor greater than 1.3 were kept.) These citations were then reviewed individually for relevance. An additional 14 citations were eliminated due to nonrelevance to the topic of LBP (e.g., osteoporotic compression fracture, cancer, spinal fracture, children, acupuncture, and whiplash). Further eliminations were made of articles that did not involve patients with LBP (1) or did not involve treatment, etc. The total yield was 58 articles, 3 of which were meta-analyses, and 1 article which was listed as a randomized controlled trial (RCT) of transforaminal epidural steroid injections that did not, in the author’s opinion, meet criteria for classification as an RCT because it did not involve blinding of the subjects or the assessments, and the randomization was described as “patient preference.” This left 54 articles of which all were classifiable as RCTs (Table).
For purposes of analysis, the 54 RCTs as described from the original selection were included. More than 4800 patients in total were included in these 54 studies. The 3 meta-analyses which were found involved spinal manipulation, exercise and work disability, and rehabilitation post-discectomy, and they are not considered further in this analysis, but the reader is referred to those publications for details.1-3
Treatment Options for the Lumbar Spine
Samuel M. Bierner, MD, MRMProfessor of Physical Medicine & Rehabilitation
Director, Residency ProgramUniversity of Texas Southwestern Medical Center
Dallas, TX

2424
TREATMENT OPTIONS FOR THE LUMBAR SPINE
Number Year Author RCT? #Subjects Intervention Notes1 2012 Becker yes 1322 Guidance implementa-
tioncost-effective
2 2012 Bergstrom yes 214 Multidimensional Pain Inventory (MPI-S) adap-tive coper
negative
3 2012 Chan yes 46 aerobics + Physical Therapy (PT)
negative
4 2012 Chen yes 43 functional fascial taping (FFT)
FFT reduced worst pain but did not affect disability or average pain levels
5 2012 Copack yes 48 goal setting military population6 2012 Du Bois yes 506 counseling + Disability
Evaluationworker injury
7 2012 Grunnesjo yes 160 4 treatment options positive8 2012 Jensen yes 351 hospital-based brief v.
multidisciplinary inter-vention
worker injury
9 2012 Macedo yes 172 motor control exercise negative 10 2012 Manchikanti yes 100 caudal Epidural Steroid
Injection (ESI) for lum-bar spinal stenosis (LSS)
LSS
11 2012 Paolucci yes 50 back school Treated subgroups showed improvement in Quality of Life (QOL), disability and pain
12 2012 Parkin-Smith yes 118 Evidence-based Medi-cine (EBM) care
control and treatment groups were similar on outcome measures at 4 weeks
13 2011 Bronfort yes 301 Spinal Manipulative Therapy (SMT) vs Ex-ercise
positive for exercise
14 2011 Cao yes 130 intradiscal injection therapy for discogenic pain
negative
15 2011 Cuesta-Vargas yes 46 manual therapy + PT + deep water running
negative
16 2011 Fiore yes 30 high intensity laser therapy for lower back pain (LBP)
positive
17 2011 McGregor yes 338 2 rehab options after back surgery
negative
Table. The 54 randomized controlled trials included in the literature review

25
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
25
18 2010 Bishop yes 92 chiropractor treatment vs. Usual Care (UC) from family doctor
high drop out rate; usual care was all over the place
19 2010 Goren yes 45 exercise with or without ultrasound LSS
positive for exercise
20 2010 Nielsen yes 60 prehabilitation before disc surgery
positive
21 2010 Shirado yes 210 Nonsteroidal antiinflam-matory drug (NSAID) versus home exercise
positive for exercise
22 2010 Skillgate yes 409 Naprapathy (type of manual therapy)
naprapathic manual therapy was more effective
23 2010 Unsgard-Tondel
yes 109 motor control exercise, sling exercise
negative
24 2009 Berg yes 152 total disc replacement versus fusion 2 yr follow-up
TDR better up to 2 years; no longer term results
25 2009 Dundar yes 65 aquatic exercise versus land based PT
positive effect of aquatic over land based
26 2009 Sertpoyraz yes 40 isokinetic versus regular exercise
negative
27 2008 Bogefeldt yes 160 pragmatic manual therapy
positive effect for return to work
28 2008 George yes 160 Fear Avoidance Beliefs Questionnaire
better predictor of perceived disability
29 2008 Helmhout yes 129 lumbar extensor versus regular PT
negative; male soldiers
30 2008 Newcomer yes 138 Behavioral videotape versus standard
negative
31 2007 Chatzithe-odorou
yes 20 high intensity aerobic exercise versus passive treatment
positive effect for high inten-sity aerobic exercise
32 2007 Critchley yes 212 physiotherapy; back class; spinal stabilization
all 3 interventions were posi-tive for reduced disability
33 2007 Johnson yes 196 Cognitive Behavioral Therapy (CBT) for LBP
negative for benefit; low cost
34 2007 Kool yes 174 function centered con-ditioning versus pain centered
positive for function-centered work rehabilitation
35 2007 Malmivaara yes 94 surgical treatment for spinal stenosis versus therapy
positive effect for surgery, but diminished over 2 years
Number Year Author RCT? #Subjects Intervention Notes

2626
36 2007 Suni yes 106 Lumbar stabilization(neutral zone)
positive effect for lumbar sta-bilization on pain, disability improved in both groups
37 2007 Vad yes 50 Back Rx exercise with cryobrace and pain medication
positive effect on disability at 12 months
38 2006 Kääpä yes 120 multidisciplinary rehab versus PT led exercise (all female subjects)
no significant difference in outcomes; both groups showed benefit at 24 months.
39 2006 Santilli yes 102 chiropractic versus simulated chiropractic
modest positive effect for chiropractic; no effects on QOL or disability; time had interaction effect with treat-ment arms
40 2006 Strong yes 262 psychologist versus lay person counseling for LBP
modest positive effect for both groups
41 2005 Kool yes 174 functional restorative approach versus back school
reduction in work related disability by intervention (function-oriented rehab)
42 2005 Lewis yes 80 individual therapy with manual treatment and spinal stabilization ver-sus group exercise
no significant difference; both groups showed im-provement, but group ap-proach was 40% less expen-sive.
43 2005 Wright yes 111 manipulation, steroid in-jection and back school versus PCP led exercise advice with pamphlet
treatment group showed significant reduction in work disability compared to con-trol
44 2004 Hurley yes 240 interferential therapy; manual therapy alone or combination
no differences between the 3 groups (interferential; manu-al or combination of both)
45 2004 Mayer yes 421 facet injections for segmental rigidity plus exercise; versus exercise only
improvement in ROM after treatment with injections for segmental rigidity; no dif-ferences in pain or disability between groups
46 2004 Ostelo yes 105 behavioral therapy after first -time lumbar sur-gery versus control
no statistically significant dif-ferences
47 2003 Nadler yes 76 overnight heat wrap therapy
effective at reducing stiffness for up to 48 hours and next day pain
48 2003 Storheim yes 93 intensive group physical exercise versus cogni-tive intervention
both groups improved; 18% dropout; exercise group more satisfied with treatment.
Number Year Author RCT? #Subjects Intervention Notes
TREATMENT OPTIONS FOR THE LUMBAR SPINE

27
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
27
Analysis of the frequency of publication of RCTs on the topic of LBP showed a nonlinear increase over time since 1999 (Figure 1). A linear regression analysis showed that 67.5% of the variance (R-squared) was explainable, which was significant (F=24.9, d.f.=12, p<0.0003). Because of the upward sloping curve, a quadratic equation, however, gave the best fit, with a robust standard deviation of residuals (RSDR) equal to 0.9.4 These data imply that the number of randomized studies continues to increase rapidly, for reasons that remain somewhat unclear. While medical expenditures for treatment of LBP have risen over time, the findings from multiple RCTs have not shown uniform results from treatment, as can be seen from perusal of the Table. This may be one reason that the number of published studies continues to grow.
FINDINGS FROM 54 RANDOMIZED CONTROLLED TRIALS
Of the 54 studies examined (published from 1999-2012), 27 showed negative results and 27 showed positive results in at least one treatment or control arm. The median number of subjects in the positive results trials was 106 (CI= 65, 160). In the negative results group, the median number of subjects was 129.5 (CI= 102, 196]. So it does not appear as though the problem with RCTs with negative results stems from inadequate numbers of subjects. The types of treatment which have shown some effectiveness will be reviewed below.
49 2002 Vad no 48 transforaminal ESI ver-sus trigger point injec-tion
they reported significant improvement with TFESI; however, the study was unblinded and randomization was flawed as described.
50 2001 Little yes 311 PCP (primary care) advice to exercise after acute LBP onset; back pamphlet of advice given
no significant differences
51 2001 Mannion yes 148 active exercise therapy for 3 months; muscle reconditioning with machines; low impact aerobics
All 3 interventions were positive for reduced pain and improved muscle strength.
52 2000 Linton yes 243 cognitive behavioral 6 sessions versus usual care
CBT showed improvement in risk of long term disability
53 1999 Kankaanpaa yes 59 12 weeks active rehabil- itation versus passive control
Active rehabilitation was su-perior in pain and disability up to 1 year.
54 1999 Lonn yes 81 active back school ver-sus control
Active back school was ef-fective.
Number Year Author RCT? #Subjects Intervention Notes
Figure 1: Increase in Number of Randomized Controlled Trials on Low Back Pain since 1999
RCT = Randomized control trialsSolid straight black line indicates best fit linear regression; curved solid black line indicates polynomial fit (quadratic equation); dotted black lines indicate 95% confidence interval for linear regression line. Large black dots are data points.
RCTs on Back Pain

28
PHYSICAL EXERCISE AS TREATMENT
Physical exercise helps back pain. This conclusion is clearly supported by several of the RCTs as indicated in the Table. What has not been as clear is what specific type of exercise is superior to any other type. Exercise has been difficult to study as an intervention because there are many different protocols or types of exercise intervention which have been tried, and the differences among them have not reached statistical significance in many of the study designs employed. It appears clear that active exercise is more useful than any type of passive treatment. Exercise instruction can be provided to the patient in several ways, including exercise supervised initially by a physical therapist or through an exercise booklet with instructions from a primary care physician. Both of these methods appear to be effective.5-9
In many of the studies reviewed for this article, the treatment was a mixture of therapies (e.g., exercise and medication, exercise and injection, and back school, etc.). While these multimodal approaches are more realistic and resemble current clinical practices, they make it impossible to tease apart conclusions about what specifically is the effective part of the treatment.10
There is strong evidence that physical exercise is helpful not harmful, and it should be recommended to almost all patients with benign forms of spine disease (e.g., disc or facet pathology, nonspecific back pain, etc.). Spinal stabilization has shown promise as one type of exercise that has published efficacy. Core strengthening (i.e., trunk and abdominal muscles) which promotes spinal stability is a treatment that all physical therapists can teach patients. Aquatic exercise can be useful for some patients, and it may be more effective initially than land-based exercise.11,12
PSYCHOLOGICAL INTERVENTIONS
In the case of chronic LBP, cognitive behavioral strategies can help reduce subsequent disability and improve the patient’s perception of their situation, reducing hopelessness and maladaptive thoughts. At least six sessions of cognitive behavioral treatment have been shown to be more effective than standard treatment (usual medical care) for patients whose pain persists beyond 12 weeks.13
In one study, investigators showed both psychologists and lay counselors had a modest positive impact on disability.14 Treatments aimed at restoration of function as opposed to pain relief have been more effective.15,16 Fear avoidance beliefs appear to play a strong role in the catastrophizing response to chronic pain.17
MANIPULATION THERAPY
Spinal manipulation has some effectiveness, but in some studies it has been combined with other treatments, making it more difficult to assess the impact of the manipulation alone.18 One recent study, however, found exercise to be more effective.19 An earlier study compared active chiropractic with sham treatment, and it showed a modest positive effect for active chiropractic therapy.20
Other varieties of manual therapy, such as napratherapy and pragmatic manual therapy, have been shown effective in two studies.21,22 The author is not personally familiar with these variants of manual therapy, but from the descriptions they are regional variations of manual therapy techniques.
MEDICATION
A home exercise program was shown to be more effective than non-steroidal anti-inflammatory drugs alone.23 Few other studies examined specific medication treatments in relation to each other to determine superiority. In many RCTs, those who received usual medical care were the control group, so medications may have been prescribed as part of that intervention.
PHYSICAL MODALITIES
Passive treatments in general have not shown favorable results. However, there have been some studies which have shown usefulness for specific interventions, such as a Cryobrace combined with back exercise and pain medication.24 As noted previously, such combinations of treatment make it difficult to ascertain the significance of the cold therapy versus other components of the treatment. In an earlier study, an overnight heat wrap was effective at relieving pain and stiffness for up to 48 hours.25 So, it can be concluded that heat and cold may be effective at least in short term relief of back pain symptoms.
SPINE INJECTIONS (INTERVENTIONAL TREATMENT)
The enthusiasm of some spine specialists for use of targeted injection therapies (usually fluoroscopically guided) has not been supported by much high level RCT evidence. In this review, a study by Manchikanti and colleagues compared only local anesthetic injection via caudal technique versus the use of anesthetic and corticosteroid. There was no significant difference between the two groups, with both yielding some benefit in pain reduction.26 This type of finding would cast doubt on the efficacy of corticosteroids at all. The author is aware of studies previous to 1999 that also failed to show efficacy of corticosteroids.
The second study uncovered in this search was problematic in that the subjects and assessors were not blinded, and the randomization was described as “patient preference” which did not appear to be true randomization (i.e., each subject has equal chance of receiving either treatment).27 That study claimed superiority of transforaminal epidural steroid injection over trigger point injection, which served as the control treatment. In this author’s opinion, trigger point injection was a poor choice as a control treatment, and the study design should have included an epidural injection with a single agent (such as local anesthetic) or saline as the control.
Further investigation is needed in this area given the high cost that epidural and other forms of spinal injection may add to the total treatment costs. The Patient-Centered Outcomes Research Institute (PCORI), a federal agency, is currently funding a 3-year study (which is urgently needed given the aging demographics of the nation) to look at long-term outcomes of epidural steroid injections in lumbar spinal stenosis (LSS).28
TREATMENT OPTIONS FOR THE LUMBAR SPINE

29
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
SURGICAL INTERVENTION
The Spine Patient Outcomes Research Trial (SPORT) has been the most significant study of the treatment of the major forms of degenerative lumbar spine disease: disc herniation, degenerative spondylolisthesis, and LSS.29-31 Interested readers should consult the original publications or the Dartmouth website whichsummarizes the results, accessible at: http://www.dartmouth.edu/sport-trial/index.htm.
Although there has been some disagreement about the interpretation of the results for treatment of lumbar disc herniation syndrome, there were clear benefits for surgical treatment, which have been maintained up to 4 years, for the treatment of degenerative spondylolisthesis and spinal stenosis producing neurological syndromes of nerve root impingement.32-35
CONCLUSIONS
Despite its prevalence, LBP has been remarkably resistant to study because of many factors, including the definition of what constitutes the patho-anatomical structures causing the pain, a variety of opinions among practitioners who provide the treatment, and difficulties with outcome measures. Physical measures, such as improvement in spinal range of motion, have for the most part given way to patient-related outcome measurement instruments, such as numerical rating scales or visual analog scales for pain, paper and pencil disability scales, and fear avoidance belief questionnaires.
Acute back pain appears to be responsive to many forms of intervention, including active exercise, physical therapy, manipulation and heat/cold modalities. Because of the benign nature of LBP in most cases, these types of treatment often can be administered inexpensively if patients are motivated to perform exercise at home.
Chronic back pain, by its nature, has exceeded the natural history for soft tissue healing. Psychological dysfunctions are more commonly seen, with depression and anxiety disorder prominent and among the most common. A variety of psychotherapeutic interventions focused on cognitive–behavioral therapies and which emphasize changing the patient’s catastrophizing behavior and thoughts to more productive modes of conceptualizing their problem can be effective. Such treatments can be effective in as few as six sessions.
Further research from the recently formed PCORI should shed more light on the value of epidural steroid injections, at least for the diagnosis of spinal stenosis.
When the clinician is faced with a patient who has persistent neurological symptoms and findings (compatible with lumbar root compression), then surgical intervention is effective especially for lumbar spondylolisthesis and spinal stenosis, and it is likely effective for providing faster relief in lumbar disc herniation with radiculopathy syndrome.
REFERENCES
1. Oesch P, Kool J, Hagen KB, Bachmann S. Effectiveness of exercise on work disability in patients with non-acute non-specific low back pain: Systematic review and meta-analysis of randomised controlled trials. J Rehabil Med 2010;42:193-205.
2. Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review. Spine 2011;36:E825-E846.
3. Rushton A, Wright C, Goodwin P, Calvert M, Freemantle N. Physiotherapy rehabilitation post first lumbar discectomy: a systematic review and meta-analysis of randomized controlled trials. Spine 2011;36:E961-E972.
4. GraphPad Prism version 6.00 for Windows, GraphPad Software, La Jolla, California.
5. Lonn JH, Glomsrod B, Soukup MG, Bo K, Larsen S. Active back school: prophylactic management for low back pain. A randomized, controlled, 1-year follow-up study. Spine 1999;24:865-871.
6. Kankaanpaa M, Taimela S, Airaksinen O, Hanninen O. The efficacy of active rehabilitation in chronic low back pain. Effect on pain intensity, self-experienced disability, and lumbar fatigability. Spine 1999;24:1034-1042.
7. Mannion AF, Taimela S, Muntener M, Dvorak J. Active therapy for chronic low back pain part 1. Effects on back muscle activation, fatigability, and strength. Spine 2001;26:897-908.
8. Critchley DJ, Ratcliffe J, Noonan S, Jones RH, Hurley MV. Effectiveness and cost-effectiveness of three types of physiotherapy used to reduce chronic low back pain disability: a pragmatic randomized trial with economic evaluation. Spine 2007;32:1474-1481.
9. Paolucci T, Morone G, Iosa M, et al. Psychological features and outcomes of the Back School treatment in patients with chronic non-specific low back pain. A randomized controlled study. Eur J Phys Rehabil Med 2012;48:245-253.
10. Grunnesjo MI, Bogefeldt JP, Blomberg SI, Strender LE, Svardsudd KF. A randomized controlled trial of the effects of muscle stretching, manual therapy and steroid injections in addition to “stay active” care on health-related quality of life in acute or subacute low back pain. Clin Rehabil 2011;25:999-1010.
11. Dundar U, Solak O, Yigit I, Evcik D, Kavuncu V. Clinical effectiveness of aquatic exercise to treat chronic low back pain: a randomized controlled trial. Spine 2009;34:1436-1440.
12. Suni J, Rinne M, Natri A, Statistisian MP, Parkkari J, Alaranta H. Control of the lumbar neutral zone decreases low back pain and improves self-evaluated work ability: a 12-month randomized controlled study. Spine 2006;31:E611-E620.
13. Linton SJ, Andersson T. Can chronic disability be prevented? A randomized trial of a cognitive-behavior intervention and two forms of information for patients with spinal pain. Spine 2000;25:2825-2831; discussion 2834.
14. Strong LL, Von Korff M, Saunders K, Moore JE. Cost-effectiveness of two self-care interventions to reduce disability associated with back pain. Spine 2006;31:1639-1645.
15. Kool JP, Oesch PR, Bachmann S, et al. Increasing days at work using function-centered rehabilitation in nonacute nonspecific low back pain: a randomized controlled trial. Archives of physical medicine and rehabilitation 2005;86:857-864.
16. Kool J, Bachmann S, Oesch P, et al. Function-centered rehabilitation increases work days in patients with nonacute nonspecific low back pain: 1-year results from a randomized controlled trial. Archives of physical medicine and rehabilitation 2007;88:1089-1094.

30
17. George SZ, Fritz JM, Childs JD. Investigation of elevated fear-avoidance beliefs for patients with low back pain: a secondary analysis involving patients enrolled in physical therapy clinical trials. J Orthop Sports Phys Ther 2008;38:50-58.
18. Wright A, Lloyd-Davies A, Williams S, Ellis R, Strike P. Individual active treatment combined with group exercise for acute and subacute low back pain. Spine 2005;30:1235-1241.
19. Bronfort G, Maiers MJ, Evans RL, et al. Supervised exercise, spinal manipulation, and home exercise for chronic low back pain: a randomized clinical trial. Spine J 2011;11:585-598.
20. Santilli V, Beghi E, Finucci S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. Spine J 2006;6:131-137.
21. Bogefeldt J, Grunnesjo MI, Svardsudd K, Blomberg S. Sick leave reductions from a comprehensive manual therapy programme for low back pain: the Gotland Low Back Pain Study. Clin Rehabil 2008;22:529-541.
22. Skillgate E, Bohman T, Holm LW, Vingard E, Alfredsson L. The long-term effects of naprapathic manual therapy on back and neck pain—results from a pragmatic randomized controlled trial. BMC musculoskeletal disorders 2010;11:26.
23. Shirado O, Doi T, Akai M, et al. Multicenter randomized controlled trial to evaluate the effect of home-based exercise on patients with chronic low back pain: the Japan low back pain exercise therapy study. Spine 2010;35:E811-E819.
24. Vad VB, Bhat AL, Tarabichi Y. The role of the Back Rx exercise program in diskogenic low back pain: a prospective randomized trial. Arch Phys Med Rehabil 2007;88:577-582.
25. Nadler SF, Steiner DJ, Petty SR, Erasala GN, Hengehold DA, Weingand KW. Overnight use of continuous low-level heatwrap therapy for relief of low back pain. Arch Phys Med Rehabil 2003;84:335-342.
26. Manchikanti L, Cash KA, McManus CD, Pampati V, Fellows B. Fluoroscopic caudal epidural injections with or without steroids in managing pain of lumbar spinal stenosis: one-year results of randomized, double-blind, active-controlled trial. J Spinal Disord Tech 2012;25:226-234.
27. Vad VB, Bhat AL, Lutz GE, Cammisa F. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine 2002;27:11-16.
28. Friedly J. Long term outcomes of lumbar epidural steroid injections for spinal stenosis. Research grant. 2013. Accessed at: http://pcori.org/
29. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA 2006;296:2441-2450.
30. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
31. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. New Engl J Med 2007;356:2257-2270.
32. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine 2008;33:2789-2800.
33. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. New Engl J Med 2008;358:794-810.
34. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surgery (Am) 2009;91:1295-1304.
35. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial. Spine 2010;35:1329-1338..
TREATMENT OPTIONS FOR THE LUMBAR SPINE

31
FUNDAMENTALS OF SPINE CARE FOR THE NON-SPINE PHYSICIAN
Fundamentals of Spine Care for the Non-Spine Physician
CME Questions:
1. The following lumbar spinal diagnoses are all common causes of low back pain EXCEPT:A. Disc herniation.B. Spinal stenosis.C. Sacroiliac joint pain.D. Sciatica.
2. The disease state of the lumbar spine in which history and physical examination is most helpful is which of the following?A. Spinal stenosis.B. Disc herniation.C. Sciatica.D. Sacroiliac joint pain.
3. In diagnosing a lumbar disc herniation, which of the following elements is LEAST helpful?A. Straight leg raise.B. Scoliosis on inspection.C. Sensation loss.D. Weakness on muscle testing.
4. When evaluating a patient for sacroiliac joint pain, a combination of tests gives the optimal sensitivity and specificity. The one test found to be helpful in any of the combinations in literature is the:A. Gaenslen’s test.B. Patrick’s test.C. Sacral sulcus tenderness.D. Gillet’s test.
5. All of the following elements in the evaluation of lumbar spinal stenosis have good specificity EXCEPT:A. Orthopedic comorbidities.B. Bilateral buttock or leg pain.C. Persistent pain when seated.D. Bilateral plantar numbness.
6. The most important unique contribution of EDX to the routine workup of spinal pain is:A. Its sensitivity.B. Its specificity.C. Speed of performance.D. Safety.
7. Mechanical disorders that mimic spinal stenosis include:A. Trochanter pain.B. Sacroiliac pain.C. Facet pain.D. Hip joint pain.E. All of the above.
8. In post-operative cases where paraspinal mapping scores are affected by surgical trauma, which of the following is true?A. The number of limb muscles required for optimal
sensitivity is unchanged.B. Objectivity and sensitivity are significantly
compromised. C. S-1 radiculopathies will be missed. D. A correction can be made by multiplying total score by ½.
9. Electrodiagnosis for lumbar disk herniation: A. Is proven with masked controlled trials.B. Is probably as sensitive as MRI or CT.C. Has the same range of norms for younger as for older
persons.D. None of the above.
10. Which of the following conditions can cause lumbosacral radiculopathy?: A. Lumbar disk herniation.B. Spondylisthesis.C. Lumbar spinal stenosis.D. All of the above.

32
11. Lumbosacral radiculopathy that occurs without direct mechanical compression of the nerve root can be due to all of the following EXCEPT: A. Stretch injury.B. Vasculitis.C. Pro-inflammatory substances.D. Phospholipase A2.
12. In Marchetti et al.’s study, which group responded most favorably to lumbar epidural steroid injections?A. Abnormal needle EMG group.B. Normal needle EMG group.C. Equivocal needle EMG group.D. All groups responded similarly.
13. All of the following are advantages of using MRI as a diagnostic study in the evaluation of lumbar spinal disorders EXCEPT:A. Ability to distinguish between symptomatic and
asymptomatic findings.B. Sensitive to lumbar intervertebral disc abnormalities.C. Contrast-enhanced studies can help identify scar tissue
and neoplastic lesions.D. Patients undergoing MRI are not exposed to radiation.
14. Which of the following locations of lumbosacaral herniated disk is NOT correlated with good outcomes after transforaminal epidural steroid injections?A. Foraminal.B. Posterolateral.C. Anterior.D. Extraforaminal.
15. Which of the following statements about treating acute back pain is true?A. Ibuprofen is more effective than physical therapy.B. Home exercise sheets can be useful for the motivated
patient. C. Needle EMG study of the lower extremities is usually
necessary to define organic pathology.D. Magnetic resonance scan should be obtained within
first 6 weeks.
16. When comparing types of conservative treatment for a patient with 3 months of lumbago, which of the following has been shown to be true?A. Back school is not effective. B. Yoga is superior to lumbar stabilization exercise. C. Fear avoidance beliefs will influence disability. D. Transcutaneous electrical nerve stimulation is superior
to land based exercise.
17. Which of the following statements about the use of physical modalities in back pain treatment is true?A. Transcutaneous electrical nerve stimulation is useful. B. Back bracing has been proven effective. C. Massage therapy is efficacious. D. Overnight heat wrap has shown efficacy for 48 hours.
18. Regarding the use of interventional spinal injection therapy for lumbar spinal stenosis, which of the following is true?A. Corticosteroid injection is necessary for pain relief. B. Transforaminal delivery of medication is superior to
caudal method. C. Epidural steroid injection has proven effectiveness over
other treatments.D. Long term outcomes are unknown.
19. Surgical intervention is supported by evidence-based medicine in which of these scenarios?A. Low back pain of 3 months duration without
neurological involvement.B. Lumbar spinal stenosis that causes leg pain and involves
one or two intervertebral disc levels. C. Multi-level disc bulging and 4 weeks of leg pain. D. Grade 1 spondylolisthesis and no leg pain.
CME QUESTIONS





























