Embed Size (px)
Citation preview

Functional and Prognostic Significance ofExercise-Induced Ventricular
Arrhythmias in Patients With SuspectedCoronary Artery Disease
Abdou Elhendy, MD, PhD, Krishnaswamy Chandrasekaran, MD,Bernard J. Gersh, MB, ChB, DPhil, Douglas Mahoney, MSc, Kelli N. Burger, BSc, and
Patricia A. Pellikka, MD
Our aims were to assess (1) the relation between exer-cise-induced ventricular arrhythmia (VA) and myocar-dial wall motion abnormalities during exercise echocar-diography in patients with suspected coronary arterydisease (CAD), and (2) the effect of this relation onoutcome. We studied the clinical and prognostic signif-icance of exercise-induced VA in 1,460 patients (meanage 64 � 10 years; 867 men) with intermediate pretestprobability of CAD and no history of previous myocar-dial infarction or revascularization who underwent ex-ercise echocardiography. Exercise-induced VA occurredin 146 patients (10%). Compared with patients withoutVA, those with VA had a greater prevalence of abnor-mal exercise echocardiographic findings (48% vs 29%, p� 0.001) and ischemia on exercise echocardiography(39% vs 22%, p � 0.001), greater increase in wallmotion score index with exercise (0.14 � 0.28 vs 0.06� 0.18, p <0.0001), and a greater percentage of ab-
normal segments with exercise (21 � 30% vs 9 � 19%,p <0.0001). During follow-up (median 2.7 years), car-diac death and nonfatal myocardial infarction occurredin 36 patients. In multivariate analysis of combinedclinical and exercise stress test variables, independentpredictors of cardiac events were exercise-induced VA(chi-square 4.7, p � 0.03) and exercise heart rate (chi-square 18, p � 0.0001). The percentage of abnormalmyocardial segments with exercise echocardiographywas the most powerful predictor of VA (chi-square 31, p� 0.0001) and cardiac events (chi-square 15, p �0.0001). In patients with suspected CAD, exercise-in-duced VA is associated with a greater risk of cardiacdeath and nonfatal myocardial infarction. This risk isattributed to the relation between VA and the extent andseverity of left ventricular functional abnormalities withexercise. �2002 by Excerpta Medica, Inc.
(Am J Cardiol 2002;90:95–100)
The clinical and prognostic significance of exercise-induced ventricular arrhythmia (VA) varies mark-
edly among previous studies.1–12 For healthy asymp-tomatic subjects, exercise-induced VA has beenshown not to be related to an adverse prognosis,1,2
whereas for patients with known or suspected coro-nary artery disease (CAD), there is a discrepancy inpublished reports regarding the relations among exer-cise-induced VA, myocardial functional abnormali-ties, and prognosis.3–12 No data are available regard-ing the relation between exercise-induced VA and leftventricular wall motion abnormalities (WMAs) duringexercise. Echocardiography is an excellent techniquefor evaluating left ventricular function in patients atrest and during exercise.13 Moreover, transient WMAsduring exercise echocardiography are a highly specificmarker of myocardial ischemia and a predictor offuture cardiac events.14–17 Therefore, exercise echo-cardiography is well suited to evaluating the func-
tional significance of exercise-induced VA. The aimof this study was to assess the relation between exer-cise-induced VA and myocardial WMAs during exer-cise in patients with intermediate pretest probability ofCAD and to assess whether exercise-induced VA isassociated with an increased risk of cardiac events.
METHODSThe study included 1,460 patients referred for ex-
ercise echocardiographic evaluation of CAD. Patientswere selected if they had an intermediate pretest prob-ability of CAD (25% to 70%). Estimation of pretestprobability of CAD was based on previously pub-lished data by Diamond and Forrester18 according togender and age. The risk factors considered werethose used by Patterson and Horowitz19 (see Appen-dix). Patients were excluded if they had a history ofprevious myocardial infarction, previous revascular-ization, CAD documented on angiography, or leftbundle branch block, or if they declined participationin research. No patient was referred for evaluation ofarrhythmias. The study was approved by our institu-tional review board. Of the 1,460 patients, 867 weremen and 593 were women (mean age 64 � 10 years).Chest pain or dyspnea, or both, were the reasons forreferral for 1,283 patients (88%).
From the Division of Cardiovascular Diseases and Internal Medicineand the Section of Biostatistics, Mayo Clinic, Rochester, Minnesota.This study was supported by the Mayo Foundation, Rochester,Minnesota. Manuscript received December 5, 2001; revised manu-script received and accepted March 22, 2002.
Address for reprints: Patricia A. Pellikka, MD, Division of Cardio-vascular Diseases and Internal Medicine, Mayo Clinic, 200 First StreetSW, Rochester, Minnesota 55905.
95©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 90 July 15, 2002 PII S0002-9149(02)02428-1

Symptom-limited treadmill exercise testing wasperformed according to the Bruce protocol in 91% ofpatients, the Naughton protocol in 4%, and the mod-ified Bruce protocol in 5%. Workload was measuredby metabolic equivalents. Two-dimensional echocar-diographic images were obtained from the parasternaland apical windows at rest and immediately afterexercise.
Both digitized and videotaped images were inter-preted for each patient.20 Regional wall motion wasassessed semiquantitatively by an experienced echo-cardiographer13 unaware of the clinical information. Wallmotion in patients at rest and after exercise was scoredfrom 1 through 5, according to a 16-segment model.21
The wall motion score index was determined for pa-tients at rest and after peak exercise as the quotient ofthe sum of the segmental scores divided by the num-ber of visualized segments. The development of newor worsening wall motion was considered indicativeof myocardial ischemia. A WMA present at rest andunchanged with exercise was classified as fixed. Ex-ercise echocardiographic results were defined as ab-normal if ischemia or fixed WMAs were present.17
The percentage of abnormal segments was calculatedas the number of abnormal segments divided by thenumber of visualized segments, multiplied by 100%.Exercise electrocardiograms were classified into 3categories: (1) positive for ischemia—horizontal ordownsloping ST-segment depression of �1 mm at 80ms after the J point or �0.1 mV elevation persisting80 ms after the J point, (2) nondiagnostic—abnormalbaseline ST segment, and (3) negative for ischemia—absence of criteria described for the first 2 categories.Exercise-induced VAs were classified as complex(couplets, bigeminy, trigeminy, or multiform ventric-ular extrasystoles) or frequent ventricular ectopic ac-tivity (�5 ventricular premature contractions/min),nonsustained ventricular tachycardia (�3 consecutiveventricular premature contractions during episodeslasting �30 seconds), sustained ventricular tachycar-dia, or ventricular fibrillation that occurred duringexercise or during recovery.
Follow-up was obtained by mailed questionnairesand scripted telephone interviews. Events were veri-fied by contacting the patients’ primary physicians andreviewing medical records and death certificates. Theend points were the occurrence of “hard” cardiacevents, defined as nonfatal myocardial infarction andcardiac death. Unexplained sudden death was consid-ered cardiac death. Myocardial infarction was definedaccording to usual clinical, electrocardiographic, andenzymatic criteria. Patients who had coronary revas-cularization (angioplasty or coronary artery bypasssurgery) before other events were censored at the timeof revascularization.
Statistical analysis: Continuous variables were re-ported as mean � SD, and categorical variables aspercentages. Univariate and multivariate associationsof clinical and exercise echocardiographic variableswith the end point were assessed in the Cox propor-tional-hazards framework. All univariate predictorswere considered for the multivariate model. Variables
were selected in a stepwise forward selection mannerwith entry and retention set at a significance level of0.05. The results were summarized as risk ratios withcorresponding 95% confidence intervals. The associ-ation of exercise-induced VA with clinical, exercisetesting, and echocardiographic variables was assessedin multiple modeling steps by using logistic regres-sion. The first step consisted of fitting a multivariablemodel of only clinical data. Variables selected fromthe first step were used as baseline risk factors, andexercise electrocardiographic and hemodynamic vari-ables were added in a stepwise forward selectionmanner. Variables selected from the first 2 steps werethen used as a baseline risk model, and echocardio-graphic variables were added in a stepwise forwardselection manner.
RESULTSExercise-induced VA occurred in 146 patients
(10%). Among these patients, the most severe grade ofarrhythmia was frequent ventricular premature con-tractions in 53 patients, complex ventricular prema-ture contractions in 52 patients, and nonsustained ven-tricular tachycardia in 41 patients. None had sustainedventricular tachycardia or ventricular fibrillation dur-ing or after exercise. Clinical features of patients withand without VA are listed in Table 1. Exercise stresstest and echocardiographic features of patients withand without VA are shown in Table 2.
Exercise echocardiography: Patients with VA had agreater prevalence of abnormal stress echocardio-graphic findings (rest or stress-induced WMAs) andischemia (stress-induced new or worsening WMAs)detected on echocardiography (Figure 1). The preva-lence of abnormal exercise echocardiograms was 59%(24 of 41) in patients with ventricular tachycardia and44% (46 of 105) in patients with other VAs (p �0.11). The prevalence of resting WMAs was not sig-nificantly different between groups. Rest, exercise,and change in wall motion score indexes and thepercentage of abnormal and ischemic segments duringexercise were significantly greater in patients withthan without VA (Figure 2). In patients without rest-ing WMAs, VA was still associated with a greaterprevalence of ischemia (29% vs 15%, p �0.001) anda greater proportion of ischemic segments on exerciseechocardiography (10 � 19% vs 4 � 12%, p �0.0003). Among patients with ischemia on exerciseechocardiography (exercise-induced WMAs), isch-emic electrocardiographic changes occurred in 97 of286 patients without VA (34%) and in 21 of 57patients with VA (37%) (p � 0.7).
Predictors of exercise-induced VAs: Univariate pre-dictors of exercise-induced VA are presented in Table3. In a multivariate analysis model of clinical andexercise stress test variables, age and percentage ofabnormal segments with exercise echocardiographywere significantly associated with the occurrence ofexercise-induced VA (Table 3). Figure 3 demonstratesthe multiple-step incremental model for the prediction
96 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 JULY 15, 2002

of VA. In the clinical model, advanced age and malegender were predictive of VA (chi-square 27.3). In theexercise electrocardiographic model, a higher exerciseheart rate was additive to clinical parameters. Restingejection fraction and percentage of ischemic segmentswere additive to the clinical and exercise electrocar-diographic model in the prediction of VA (chi-square60 vs 47).
Cardiac events: Sixty-two patients underwent cor-onary revascularization at a median time of 165 daysafter exercise echocardiography and were censored atthe time of revascularization. Patients who underwentrevascularization had a greater prevalence of ischemiaon echocardiography (61% vs 22%, p �0.001), exer-
cise-induced angina (23% vs 7%, p�0.0001), and ischemic electrocar-diographic changes (53% vs 15%, p� 0.001) than patients without revas-cularization. Exercise-induced VAoccurred in 11% of patients (7 of 62)with and in 10% of patients (139 of1,398) without subsequent revascu-larization (p � 0.73). Hard cardiacevents occurred in 36 patients (12died of cardiac causes and 24 hadnonfatal myocardial infarctions).These events occurred at a median2.7 years (range 1 day to 7.8 years)after exercise echocardiography.Clinical, exercise stress test, andechocardiographic variables, univari-ately associated with an increasedrisk of cardiac death and myocardialinfarction, are listed in Table 4.
Predictors of cardiac events in themultivariate analysis model: In themultivariate analysis of the com-bined clinical and exercise stress testvariables, independent predictors ofcardiac events were exercise-inducedVA (chi-square 4.7, p � 0.03) andexercise heart rate (chi-square 18, p� 0.0001). When echocardiographicvariables were added to the model,VA was no longer predictive of car-diac events. Independent predictorsof cardiac death and myocardial in-farction in the latter model were thepercentage of abnormal segmentswith exercise echocardiography (chi-square 15, p � 0.0001) and exerciseheart rate (chi-square 13, p �0.0003).
DISCUSSIONIn this study, we evaluated the
relation between exercise-inducedVA and left ventricular WMAs asassessed by echocardiography in1,460 patients with suspected CAD.Patients with intermediate pretestprobability of CAD were studied be-
cause the prognostic value of exercise-induced VAhas not been previously assessed in this population.Studies have shown that stress-imaging techniques aremost useful in the prognostic stratification of patientswith intermediate probability of CAD.22
Our study showed that exercise-induced VA isassociated with a greater prevalence and extent ofmyocardial WMAs during exercise: WMAs were de-tected in 48% of patients with and in 29% of patientswithout VA (p � 0.001). The prevalence and extent ofexercise-induced myocardial ischemia (defined as newor worsening WMAs with exercise) were significantlygreater in patients with than without VA, as indicatedby a larger percentage of ischemic segments with
TABLE 1 Clinical Features of Patients With and Without Ventricular Arrhythmia
Clinical Features
Ventricular Arrhythmia
p Value0 (n � 1,314) � (n � 146)
Mean age (yrs) (mean � SD) 63 � 10 67 � 8 0.001Men 772 (59%) 95 (65%) 0.1Reason for referral 0.5
Evaluation of chest pain or dyspnea 1,159 (88%) 124 (85%)Preoperative assessment before noncardiac surgery 25 (2%) 5 (3%)Positive or nondiagnostic exercise ECG results 47 (4%) 5 (3%)Evaluation because of risk factors for CAD 83 (6%) 12 (8%)
Hypercholesterolemia* 764 (58%) 74 (51%) 0.08Cigarette smoking 664 (51%) 81 (55%) 0.3Systemic hypertension 646 (49%) 81 (55%) 0.2Diabetes mellitus 138 (11%) 13 (9%) 0.5�-blocker therapy 220 (17%) 23 (16%) 0.8Calcium antagonist therapy 296 (23%) 26 (18%) 0.2
*Defined as total cholesterol value �200 mg/dl or requirement for cholesterol-lowering medication.ECG � electrocardiographic.
TABLE 2 Exercise Stress Test and Echocardiographic Data of Patients With andWithout Ventricular Arrhythmia
Hemodynamic Variables
Ventricular Arrhythmia
p Value0 (n � 1,314) � (n � 146)
Resting heart rate (beats/min) 75 � 13 72 � 12 0.009Exercise heart rate (beats/min) 147 � 22 147 � 21 1Resting systolic blood pressure (mm Hg) 137 � 21 142 � 19 0.006Exercise systolic blood pressure (mm Hg) 184 � 28 188 � 29 0.06Change in systolic blood pressure (mm Hg) 47 � 24 46 � 27 0.8Exercise rate pressure product 27,227 � 6,248 27,743 � 6,053 0.3Workload (METs*) 8.6 � 2.8 8.4 � 2.6 0.4Rest ejection fraction (%) 60% � 6.2% 57% � 8.1% 0.001Rest wall motion score index 1.06 � 0.18 1.13 � 0.3 0.0005Exercise wall motion score index 1.11 � 0.25 1.27 � 0.42 0.0001� Wall motion score index† 0.06 � 0.18 0.14 � 0.28 0.0001Percentage of abnormal segments at rest 5 � 14 11 � 22 0.0005Percentage of abnormal segments with exercise 9 � 19 21 � 30 0.0001Percentage of ischemic segments 6 � 14 14 � 23 0.0001Angina during the test 96 (7%) 12 (8%) 0.7ECG response 0.1
Ischemic changes 210 (16%) 28 (19%)Nondiagnostic electrocardiogram 274 (21%) 39 (27%)No ECG changes 830 (63%) 79 (54%)
*1 MET � 3.5 ml of oxygen per kilogram of body weight per minute.†Difference between the regional wall motion score index in patients after exercise and at rest.Values are expressed as mean � SD or number (%).Abbreviation as in Table 1.
CORONARY ARTERY DISEASE/EXERCISE-INDUCED VENTRICULAR ARRHYTHMIAS 97

exercise in patients with VA (Figures 1 and 2). Exer-cise-induced myocardial WMAs have been reported tobe highly specific for significant CAD.13,14 Thus, it isprobable that exercise-induced VA is associated witha greater prevalence of CAD in this particular popu-lation.
Predictors of exercise-induced VAs: In the multiple-step incremental model for predicting exercise-induced VA, clinical predictors were advanced ageand male gender. The increased incidence of exercise-induced VA with aging is consistent with previousstudies.23 The association with male gender may beexplained by the greater prevalence or severity ofCAD in men. Among exercise variables, a greaterexercise heart rate was predictive of VA. Althoughthis variable was not significant in the univariate anal-ysis, it was significant in the incremental model,
which adjusts for the differences in agebetween patients with and without VA.Echocardiographic variables providedincremental data for the prediction ofVA. Both resting left ventricular func-tion and the severity of exercise-induced ischemia were predictive ofVA, because both the resting ejectionfraction and the percentage of ischemicsegments added significantly to theclinical and exercise model.
The association between exercise-induced VA and WMAs can be ex-plained—at least in part—by the arrhyth-mogenic effect of myocardial isch-emia.24,25 The increased sympathetic ac-tivity and circulating catecholamines duringexercise can induce myocardial ischemiaand alter electrical activity, thereby trigger-ing arrhythmias in the ischemic myocardi-um.2 Another possibility is that mechanicaldysfunction, as a consequence of myocar-dial ischemia, contributes to electrical insta-
bility during exercise by mechanisms such as myo-cardial stretch.
Cardiac events: During a median follow-upperiod of 2.7 years, hard cardiac events occurredin 36 patients (2.5%). VA was associated with asignificantly increased risk of cardiac death andmyocardial infarction in the univariate analysis(p �0.05). In a multivariate analysis model ofclinical and exercise stress test variables, exer-cise-induced VA was independently predictiveof cardiac events. When echocardiographicvariables were added to the model, VA was nolonger predictive of cardiac events. Therefore,the increased risk of cardiac events in patientswith VA is dependent on the association be-tween VA and exercise WMAs. When exercisestress testing is performed without an imagingmethod, such as echocardiography or myocar-dial perfusion scintigraphy, the occurrence ofVA in patients with suspected CAD should beinterpreted as a predictor of cardiac events. Theevent rate in this study was low. Coronary re-
vascularization may have improved outcome. Never-theless, revascularization was performed in similarpercentages of patients with and without VA.
Role of exercise echocardiography: The percentageof abnormal segments during exercise echocardiogra-phy was the most powerful independent predictor ofhard events in the multivariate analysis model. Thisfinding confirms the value of exercise echocardiogra-phy in the risk stratification of patients with suspectedCAD, as previously demonstrated.15–17 Because pa-tients with exercise-induced VA had a greater percent-age of abnormal segments with exercise, one mayassume that the increased risk of hard events associ-ated with VA is related to the association between VAand WMAs and, presumably, to the extent and sever-ity of the underlying CAD and left ventricular dys-function during exercise.
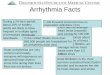
FIGURE 1. Prevalence of abnormal resting echocardiograms, exercise-inducedischemia (new or worsening WMAs), and abnormal exercise echocardiograms(fixed or ischemic WMAs) in patients with (open bars) and without (solid bars) ex-ercise-induced VA. *Significance at p � 0.001.
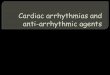
FIGURE 2. Percentage of abnormal segments at rest and during exerciseand percentage of ischemic segments (new or worsening WMAs) in pa-tients with (open bars) and without (solid bars) exercise-induced VA.*Significance at p <0.0001.
98 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 JULY 15, 2002

Comparison with previous studies: Previous studiesof exercise-induced VA have been conducted in eitherasymptomatic patients with low probability of CAD orhigh-risk patients, such as those with previous myo-cardial infarction, or in a heterogeneous populationwith known or suspected CAD. This may explain theconflicting results regarding the significance of VAamong previous studies. In asymptomatic healthy per-sons, exercise-induced VA was not a predictor ofadverse prognosis.1,2
However, a recent study by Jouven and colleagues23
indicated that this might not be thecase during long-term follow-up. Theinvestigators examined the prognosticimplications of exercise-induced VAin a cohort of �6,000 men withoutknown or suspected cardiovasculardisease. After 23 years of follow-up,the risk of death from cardiovascularcauses was increased by a factor of�2.5 among men who had frequentventricular depolarizations during ex-ercise. This increased risk persisted af-ter adjustment for other risk factorsand ischemic electrocardiographicchanges. It is possible that ischemiawas underestimated in that study be-cause it was evaluated by electrocardi-ography without a concomitant imag-ing technique. Therefore, the actualcontribution of ischemia to the in-creased risk in patients with exercise-induced VA might have been underes-timated.
Calkins26 suggested in his editorialcomments that the risk associated withexercise-induced VA in asymptomaticpatients is too great to be ignored andthat additional diagnostic testing, suchas echocardiography, should be imple-
mented. In our study, exercise echocardiog-raphy provided information regarding thereason for the association between VA andcardiac events, because patients with VAhad a greater prevalence and severity ofmyocardial ischemia.
A controversy exists about the relationsamong exercise-induced VA, structural andfunctional abnormalities, and prognosis forpatients with known or suspected CAD.3,12
Few studies have evaluated the relationbetween exercise-induced VA and myo-cardial perfusion abnormalities. Margo-nato et al11 reported an association be-tween VA and reversible defects in theinfarct zone after myocardial infarction.Marieb et al9 reported that for 383 patientswith and without previous myocardial in-farction, exercise-induced VA was associ-ated with a greater prevalence of revers-ible thallium-201 perfusion defects andprovided independent prognostic informa-
tion beyond that provided by thallium stress tests. Incontrast, Schweikert et al10 reported that exercise-in-duced VA was not associated with short-term mortal-ity or angiographic severity of CAD, although it wasassociated with a greater likelihood of thallium perfu-sion defects. The present study is the first to evaluatethe relation between exercise-induced VA and WMAswith echocardiography. The study was conducted in ahomogeneous population in which stress testing wasshown to provide the largest increment in prognosticstratification.
TABLE 3 Clinical, Exercise Stress Test, and Echocardiographic Predictors ofExercise-induced Ventricular Arrhythmias
PredictorWald
Chi-square p ValueOdds Ratio(95% CI)
UnivariateClinical
Age 17 0.0001 1.48 (1.22–1.79)*History of chest pain 4.3 0.04 0.64 (0.42–0.68)Resting systolic blood pressure 6.4 0.01 1.1 (1.0–1.22)*Resting heart rate 8.3 0.004 0.82 (0.74–0.90)*
Exercise stress testNo significant variables�
EchocardiographicRest ejection fraction 16.8 0.0001 0.60 (0.48–0.82)*Exercise WMA 21.1 0.0001 2.25 (1.59–3.18)New WMA (ischemia) 20.9 0.0001 2.3 (1.61–3.29)Percentage of abnormal segments with exercise 41.1 0.0001 1.65 (1.42–1.92)†Percentage of ischemic segments 30.1 0.0001 1.79 (1.45–2.2)†Exercise wall motion score index 37.3 0.0001 4.09 (2.6–6.4)‡� Wall motion score index§ 20.7 0.0001 4.77 (2.44–9.36)‡
MultivariateAge 10 0.0015 1.36 (1.13–1.64)*Percentage of abnormal segments with exercise 31 0.0001 1.57 (1.34–1.84)†
*Per 10-U increment; †per 25% increment; ‡per 1-U increment.§Difference between the regional wall motion score index in patients after exercise and at rest.�Variables considered included workload, electrocardiogram positive for ischemia, exercise rate-
pressure product, achievment of 85% of the age-predicted maximum heart rate, exercise heart rate,exercise systolic blood pressure, and angina during exercise test.
CI � confidence interval.
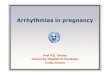
FIGURE 3. Multiple-step incremental multivariate analysis model for the predic-tion of exercise-induced VA (see text for details). ECG � electrocardiogram;Echo � echocardiogram; EF � ejection fraction; HR � heart rate.
CORONARY ARTERY DISEASE/EXERCISE-INDUCED VENTRICULAR ARRHYTHMIAS 99

APPENDIXIntermediate pretest probability: No chest pain: men with 3 risk factors*
if aged �50 years; atypical chest pain: women aged �60 years, men aged �40years, typical angina pectoris: women aged �50 years, men aged �30 years.
1. Busby MJ, Shefrin EA, Fleg JL. Prevalence and long-term significance ofexercise-induced frequent or repetitive ventricular ectopic beats in apparentlyhealthy volunteers. J Am Coll Cardiol 1989;14:1659–1665.2. Fleg JL, Lakatta EG. Prevalence and prognosis of exercise-induced nonsus-tained ventricular tachycardia in apparently healthy volunteers. Am J Cardiol1984;54:762–764.3. Califf RM, McKinnis RA, McNeer JF, Harrell FE Jr, Lee KL, Pryor DB,Waugh RA, Harris PJ, Rosati RA, Wagner GS. Prognostic value of ventriculararrhythmias associated with treadmill exercise testing in patients studied withcardiac catheterization for suspected ischemic heart disease. J Am Coll Cardiol1983;2:1060–1067.4. Yang JC, Wesley RC Jr, Froelicher VF. Ventricular tachycardia during routinetreadmill testing. Risk and prognosis. Arch Intern Med 1991;151:349–353.5. Specchia G, LaRovere MT, Falcone C, Campana C, Traversi E, Caizzi V, DeServi S. Cardiac arrhythmias during exercise-induced myocardial ischaemia inpatients with coronary artery disease. Eur Heart J 1986;7:45–52.6. Sami M, Chaitman B, Fisher L, Holmes D, Fray D, Alderman E. Significanceof exercise-induced ventricular arrhythmia in stable coronary artery disease: acoronary artery surgery study project. Am J Cardiol 1984;54:1182–1188.7. Henry RL, Kennedy GT, Crawford MH. Prognostic value of exercise-inducedventricular ectopic activity for mortality after acute myocardial infarction. Am JCardiol 1987;59:1251–1255.8. Nair CK, Thomson W, Aronow WS, Pagano T, Ryschon K, Sketch MH.Prognostic significance of exercise-induced complex ventricular arrhythmias in
coronary artery disease with normal and abnormal leftventricular ejection fraction. Am J Cardiol 1984;54:1136–1138.9. Marieb MA, Beller GA, Gibson RS, Lerman BB,Kaul S. Clinical relevance of exercise-induced ventric-ular arrhythmias in suspected coronary artery disease.Am J Cardiol 1990;66:172–178.10. Schweikert RA, Pashkow FJ, Snader CE, MarwickTH, Lauer MS. Association of exercise-induced ven-tricular ectopic activity with thallium myocardial per-fusion and angiographic coronary artery disease in sta-ble, low-risk populations. Am J Cardiol 1999;83:530–534.11. Margonato A, Mailhac A, Bonetti F, Vicedomini G,Fragasso G, Landoni C, Lucignani G, Rossetti C, FazioF, Chierchia SL. Exercise-induced ischemic arrhyth-mias in patients with previous myocardial infarction:Role of perfusion and tissue viability. J Am Coll Car-diol 1996;27:593–598.12. Tsuji H, Iwasaka T, Sugiura T, Shimada T, Naka-mori H, Kimura Y, Inada M. Relationship betweenredistribution on exercise thallium-201 scintigraphyand repetitive ventricular premature beats in patientswith recent myocardial infarction. Am Heart J 1991;121:1679–1684.13. Armstrong WF, Pellikka PA, Ryan T, Crouse L,Zoghbi WA. Stress echocardiography: recommenda-tions for performance and interpretation of stress echo-cardiography. J Am Soc Echocardiogr 1998;11:97–104.14. Marwick TH, Nemec JJ, Pashkow FJ, Stewart WJ,Salcedo EE. Accuracy and limitations of exercise echo-cardiography in a routine clinical setting. J Am CollCardiol 1992;19:74–81.15. McCully RB, Roger VL, Mahoney DW, Karon BL,Oh JK, Miller FA Jr, Seward JB, Pellikka PA. Outcomeafter normal exercise echocardiography and predictors
of subsequent cardiac events: follow-up of 1,325 patients. J Am Coll Cardiol1998;31:144–149.16. Olmos LI, Dakik H, Gordon R, Dunn JK, Verani MS, Quinones MA, ZoghbiWA. Long-term prognostic value of exercise echocardiography compared withexercise 201Tl, ECG, and clinical variables in patients evaluated for coronaryartery disease. Circulation 1998;98:2679–2686.17. Arruda AMM, Das MK, Roger VL, Klarich KW, Mahoney DW, Pellikka PA.Prognostic value of exercise echocardiography in 2632 patients � 65 years ofage. J Am Coll Cardiol 2001;37:1036–1041.18. Diamond GA, Forrester JS. Analysis of probability as an aid in the clinicaldiagnosis of coronary-artery disease. N Engl J Med 1979;300:1350–1358.19. Patterson RE, Horowitz SF. Importance of epidemiology and biostatistics indeciding clinical strategies for using diagnostic tests: a simplified approach usingexamples from coronary artery disease. J Am Coll Cardiol 1989;13:1653–1665.20. Attenhofer CH, Pellikka PA, Oh JK, Roger VL, McCully RB, Shub C,Seward JB. Is review of videotape necessary after review of digitized cine-loopimages in stress echocardiography? A prospective study in 306 patients. J Am SocEchocardiogr 1997;10:179–184.21. Schiller NB, Shah PM, Crawford M, De Maria A, Devereux R, FeigenbaumH, Gutgesell H, Reichek N, Sahn D, Schnittger I, Silverman NH, Tajik AJ.Recommendations for quantitation of the left ventricle by two-dimensional echo-cardiography. J Am Soc Echocardiogr 1989;2:358–367.22. Shaw LJ, Hachamovitch R, Heller GV, Marwick TH, Travin MI, IskandrianAE, Kesler K, Lauer MS, Hendel R, Borges-Neto S, et al, for the Economics ofNoninvasive Diagnosis (END) Study Group. Noninvasive strategies for theestimation of cardiac risk in stable chest pain patients. Am J Cardiol 2000;86:1–7.23. Jouven X, Zureik M, Desnos M, Courbon D, Ducimetiere P. Long-termoutcome in asymptomatic men with exercise-induced premature ventricular de-polarizations. N Engl J Med 2000;343:826–833.24. Sung RJ, Huycke EC, Lai WT, Tseng CD, Chu H, Keung EC. Clinical andelectrophysiologic mechanisms of exercise-induced ventricular tachyarrhythmias.Pacing Clin Electrophysiol 1988;11:1347–1357.25. Reinke A, Michel D, Mathes P. Arrhythmogenic potential of exercise-induced myocardial ischaemia. Eur Heart J 1987;8:119–124.26. Calkins H. Premature ventricular depolarization during exercise [editorial].N Engl J Med 2000;343:879–880.
*Risk factors considered are systemic hypertension, smoking, diabetesmellitus, hypercholesterolemia, and resting electrocardiographic ab-normalities. Data from Patterson and Horowitz.19
TABLE 4 Univariate Association of Clinical, Exercise Stress Test, andEchocardiographic Variables With Risk of Cardiac Death and NonfatalMyocardial Infarction
Variable Wald Chi-square p Value Risk Ratio (95% CI)
ClinicalAge 4 0.04 1.48 (1.00–2.16)*Resting systolic blood pressure 4.9 0.3 1.22 (1.00–1.34)*
Exercise stress test85% of age-predicted heart rate 8.5 0.004 0.37 (0.19–0.72)Exercise heart rate 18 0.0001 0.74 (0.66–0.82)*Change in systolic blood pressure 6.3 0.01 0.87 (0.77–0.97)*Exercise rate pressure product 10.4 0.001 0.2 (0.07–0.52)†Workload 9 0.003 0.82 (0.72–0.93)Exercise-induced ventricular arrhythmia 4.2 0.04 2.5 (1.05–6.12)
EchocardiographicRest ejection fraction 19.1 0.001 0.48 (0.35–0.66)*Exercise WMA 9.7 0.002 2.8 (1.47–5.44)New WMA (ischemia) 5.1 0.02 2.19 (1.11–4.32)Percentage of abnormal segments 23 0.0001 1.8 (1.4–2.3)‡Percentage of ischemic segments 5.4 0.02 1.6 (1.08–2.39)‡Exercise wall motion score index 22 0.0001 5.68 (2.74–11.8)§� Wall motion score index� 4.5 0.03 4.38 (1.12–17.1)§
*Per 10-U increment; †per 100-U increment (parameters analyzed on natural logarithm scale); ‡per25% increment; §per 1-U increment.
�Difference between regional wall motion score index in patients after exercise and at rest.Abbreviation as in Table 3.
100 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 JULY 15, 2002