Embed Size (px)
Citation preview

Daniel I. Feig, MD, PhD, MS
Director, Division of Nephrology
Department of Pediatrics
University of Alabama, Birmingham
Fructose, Uric Acid and Hypertension in Children and Adolescents

Topics for Discussion
• The Obesity Epidemic
• The Sugar Primer
• Fructose
• Biochemical Considerations
• Animal models
• Human studies
• Uric Acid/Hypertension Hypothesis
• What can we do?

The Obesity Epidemic
2017 Estimates
2.7 billion overweight
720 million obese

Sugar and Obesity
Johnson, et al. Am J Clin Nutrit. 2007; 86:899-906.
Mean Annual
Individual Sugar
Intake
1700 1.8 kg
1800 8.1 kg
1900 40.9 kg
2000 70.4 kg
2015 74.6 kg
Men
Women
Sugar Tax
HFCS
WW 2
WW 1

What is Fructose?
Table sugar (Sucrose) is a disaccharide of glucose and fructose.
Naturally occurring fructose is found in honey, fruits and vegetables.
High fructose corn syrup most commonly contains 55% fructose and 45% glucose.
Adolescents consume 72.8 grams per day.

Fructose Metabolism Increases Uric
Acid
Triglycerides

Health Risks of SSBs
Health Professionals F/U: top quartile of SSB intake had 20% increased risk of coronary disease
De Koning et al. Circulation 2012; 123:1735
Meta-analysis of data from 94 countries: each % point increase of caloric intake from sugar associated with 5% increase in T2DM risk
Siegel et al. Diabetes Res Clin Pract 2012; 96:76
Quebec Adiposity and Lifestyle In Youth: 100mL/d increase in SSB associated with insulin resistance and weight increase
Wang et al. Pediatr Obesity 2012; 8:284

Proposed Mechanisms
IMPAIRED SATIETY: animal models suggest fructose consumption suppresses leptin release disruption hypothalamic control of hunger and energy metabolism
Melanson et al. Am J Clin Nutr. 2008; 88:1738S
HIBERNATION METABOLISM: animal and human studies suggest >25% caloric intake from fructose results in decreased energy expenditure and fatty acid oxidation
Stanhope et al. J Clin Invest. 2009; 119:1322
HYPERURICEMIA: dysregulated fructose metabolism results in purine release and uric acid production. Uric acid acts as a vascular toxin causing hypertension and organ damage
Feig et al. New Engl J Med. 2008; 359:1811

It’s the Quantity not the Source
Gm sugar per 6oz serving

Soft Drinks and Hyperuricemia
Wong, et al. Arthritis and Rheumatism. 2008; 59 (1): 109-116.
1-2 servings per day increases sUA
by 1mg/dL

Baseline After 2wks
Metabolic Syndrome (%) 19% 28% P Value
Triglycerides 136 ± 15 193±20 <0.001
HDL Cholesterol 46.5 ± 1.5 44±0.7 <0.001
Insulin resistance (HOMA) 1.7 ± 0.2 2.3±0.2 <0.005 Weight (kg) 84.3 ± 2.3 84.9±0.2 0.130
BMI (kg/m2) 29.0 ± 0.6 29.2±0.1 0.304
24 hr Systolic BP (mm Hg) 126±2 133±2 <0.001
24 hr Diastolic BP (mm Hg) 75 ± 2 81±3 <0.001
Uric acid (mg/dl) 5.2 ± 0.2 6.3±0.8 <0.001
Effect of Fructose (200 g/d) for 2 weeks on Metabolic syndrome in Men: Menorca Study
Perez-Pozo et al. Int J Obes. 2010; 34:454-61

Fructose withdrawal may be helpful
28 patients with CKD II-III, low sweetener diet for 6wks then resume normal diet for 6 more weeks.
Brymora et al.
NDT, 2011
Fructose Summary
Acute Fructose Loading Causes Weight gain
Increased serum uric acid
Onset of metabolic syndrome
Increase in BP
Increase TG
Fructose reduction may reverse symptoms

Fang, J. et al. JAMA 2000;283:2404-2410.
Age-Adjusted CV Mortality Rates by Serum Uric Acid Quartile
NHANES

Rat Model of Hyperuricemia
Normal Rat Uric Acid (0.5-1.4 mg/dl)
Hyperuricemic RatUric Acid (2.7-4.0 mg/dl)
Uricaseinhibitor
Oxonic acid (OA)

Hyperuricemia Induces Hypertension
Watanabe S et al., Hypertension 2002; 40:355-360
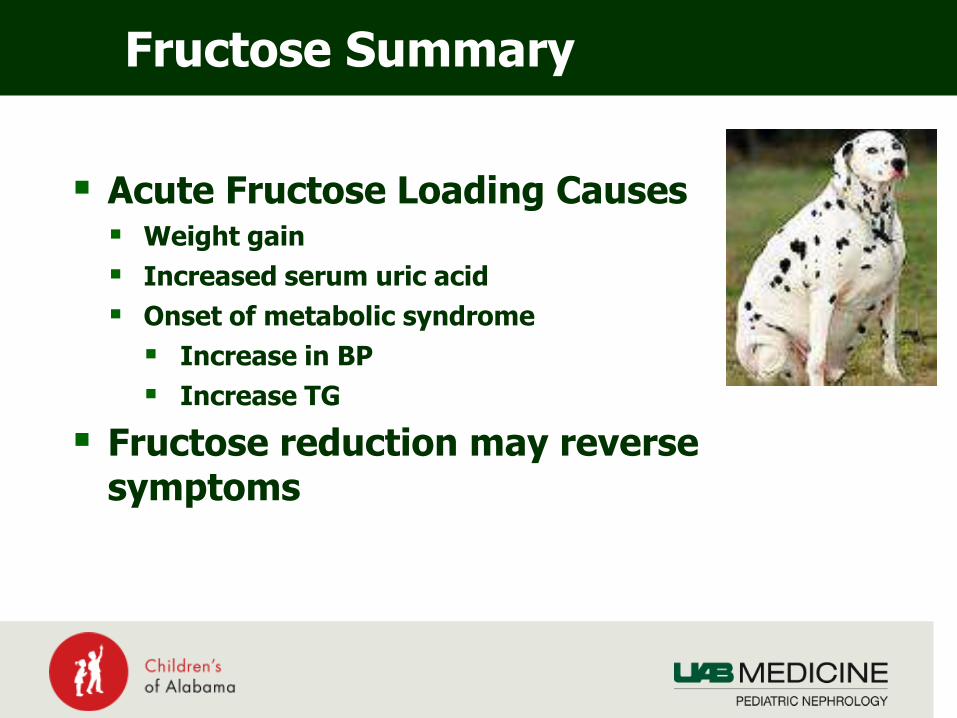
Vascular model of Uric Acid Mediated Hypertension
Phase 1: Reversible Vasoconstriction
Phase 2: Arteriolar Wall Thickening
Uric Acid
Uric Acid
Increased reninDecreased NO
Vascular smoothmuscle proliferation mediated by PDGF and MCP-1
Remains uric acid dependentSodium resistant
Becomes uric acid independentSodium sensitive

Uric acid and Vascular Compliance
Framingham Cohort
Mehta et al. Am J Hypertens. 2015; 28:877

≠
Hyperuricemia in Patients

Serum Uric Acid in Children with Hypertension
Feig and Johnson. Hypertension. 2003; 42; 247-252

Allopurinol for the Treatment of Hypertension in Adolescents
Feig, et al. JAMA. 2008; 300: 942-932.

Effect of Allopurinol on Blood Pressure
Feig et al., JAMA 2008; 300(8):924-32

PHOA Trial: Prevention of Hypertension in Obese Adolescents
60 Adolescents
•BMI >30kg/m2
•Pre-hypertension
•Uric acid >5mg/dL
•No current meds
•Never Rx’d for HTN
Scre
en
an
d R
an
do
miz
e 20 Adolescents, 2 mo Placebo
20 Adolescents, 2 mo Probenecid
20 Adolescents, 2 mo Allopurinol
1 mo f/u
1 mo f/u
1 mo f/u
Soletsky and Feig. Hypertension. 2012; 60:1148-1156.

Uric Acid Reduction in PrehypertensiveAdolescents: Allopurinol vs. Probenecid
End Point Placebo Allopurinol Probenecid
Serum Uric Acid (mg/dl)
Change from baseline
6.3
-0.3
4.1
-2.8 (0.0005)
4.0
-2.7 (0.0026)
24hr Systolic BP (mmHg)
Change from baseline
120.0
+1.9
113.5
-9.2 (0.0008)
113.7
-8.9 (0.0002)
24hr Diastolic BP (mmHg)
Change from baseline
68.7
+1.3
62.4
-6.1 (0.0009)
62.4
-7.3 (0.0006)
Weight (kg)
Change from baseline
99.8
+2.1
98.1
-0.9 (0.039)
93.8
-0.1 (0.03)
Soletsky and Feig. Hypertension. 2012; 60:1148-1156.

Urate Lowering Therapy With ACEi in Children
Assadi et al. J Nephrol 2014; 27:51• 52 hypertensive adolescents• Mean uric acid 6.6mg/dL• Randomized to enalapril vs
+allopurinol• 8wks therapy• ABPM is endpoint
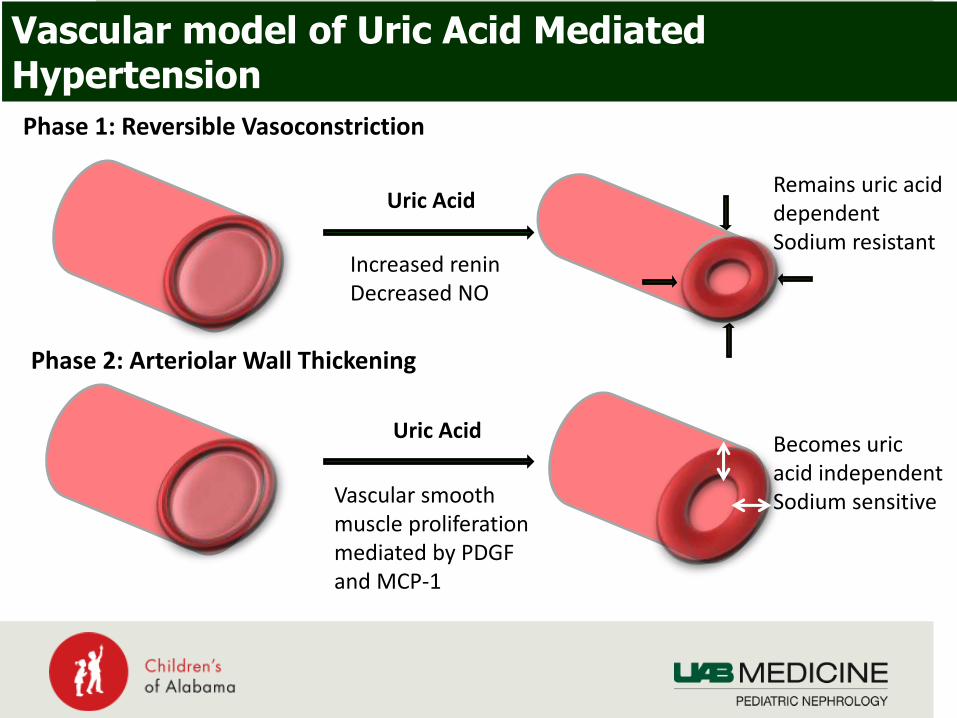
Counter Evidence – BP Urate Lowering Therapy
Forman et al. CJASN 2017; 12:807• 150 patients, mean age 41• Mean sUA 6.1mg/dL• Mean BP:
• Casual 119/77, Control 119/77• ABPM 127/74, Control 121/58
• No change in BP with UrLTDifferences• Older population• Completely normotensive • 79/150 had BP data (53%)• Less Hyperuricemic• Most smokers

Febuxostat in Adults with CKD
Gunawardhana et al. JAHA 2017; 6:e006683• 121 adults• Mean age 53• Mixed renal function
• Normal: 37%• CKD 1-2: 52%• CKD 3-4: 11%
• Hypertensive 100%• No Meds: 28%• 1 Med: 62%• 2 Meds: 9%
No change in BP in whole populationIn Patients with Normal Renal Function, mean decrease of SBP of 6.6mmHg

Influence of UrA on CKD Progression in Young Patients
CKID CohortRodenbach et al., AJKD 2015;66:984

Summary of Human Data
• Uric acid correlates with the development of essential hypertension in children
• Uric acid lowering therapy, regardless of mechanism lowers blood pressure in hypertensive and prehypertensiveadolescents
• Hypertensive effect appear more pronounced in young
• Age, lack of hypertension, severity of CKD attenuate the BP response to uric acid reduction
• Hyperuricemia associated with impaired vascular compliance, consistent with mechanistic studies
• Hyperuricemia is associated with progressive decline in GFR

Conclusions
Sweetener consumption parallels the obesity, metabolic
syndrome and CV disease epidemic
Fructose mediates some of its effects through uric acid
which causes vasoconstriction and vasculopathy
Uric acid mediates hypertension in young patients
Markedly attenuated response in older patients
First line therapy should be dietary fructose reduction
Management of hyperuricemia holds promise as additive
therapy and in prevention but needs more study