Embed Size (px)
Citation preview

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 1
CASE REPORT OPEN ACCESS
Frontoethmoidal mucocele with unilateral proptosis: Case series
EE Afiadigwe, AI Apakama, G Obasikene, JU Obah, SNN Nwosu
ABSTRACT
Introduction: Mucocele may occur in any of the paranasal sinuses but the frontal sinus is the commonest followed by the ethmoidal sinuses. Frontoethmoidal mucocele is a disfiguring benign condition with good prognosis when treated promptly but associated with both orbital and intracranial complication if neglected. The current treatment of choice is functional endoscopic sinus surgery (FESS) which is still being developed in many low and middle income nations leaving external frontoethmoidectomy as the available treatment of choice. Case Report: We report two cases of frontoethmoidal mucocele with orbital involvement jointly managed in our center between January 2011 and February 2013 and reviewed the literature. They were one male and one female, both presented with unilateral proptosis and had external frontoethmoidectomy with good outcome. Conclusion: Non-axial proptosis is a serious complication of frontoethmoidal mucocele. External frontoethmoidectomy is an effective treatment of choice especially for massive late presenting lesions as ours, where FESS is still at the developmental stages.
Keywords: Frontoethmoidectomy, Frontoethmoidal mucocele, Proptosis
EE Afiadigwe1, AI Apakama2, G Obasikene1, JU Obah1, SNN Nwosu2
Affiliations: 1Department of ENT, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria; 2Depart-ment of Ophthalmology, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria.Corresponding Author: Dr. EE Afiadigwe, Department of ENT, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria; Email: [email protected]
Received: 05 January 2020Accepted: 06 June 2020Published: 02 July 2020
CASE SERIES PEER REVIEWED | OPEN ACCESS
How to cite this article
Afiadigwe EE, Apakama AI, Obasikene G, Obah JU, Nwosu SNN. Frontoethmoidal mucocele with unilateral proptosis: Case series. J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.
Article ID: 100002Z18EA2020
*********
doi: 10.5348/100002Z18EA2020CS
INTRODUCTION
A paranasal sinus mucocele is a cystic epithelial lesion containing mucus, usually slow growing with expansive and osteolytic features that can involve surrounding structures such as orbit and intracranial cavity [1]. The frontal sinus is the commonest site, followed by the ethmoid, the maxillary and lastly the sphenoid sinuses. Though relatively rare, it usually affects adults and very rarely children. The two most frequent causes of frontal mucoceles are: inflammatory changes and post-traumatic or iatrogenically induced scarring of the nasofrontal duct [2]. Frontoethmoidal mucocele will cause visual impairment and blindness when management is delayed [3].
Frontoethmoidal mucoceles have been traditionally treated by external frontoethmoidectomy (Lynch–Howarth operation) or an osteoplastic flap operation but this is fast being replaced by endoscopic sinus surgery (ESS) especially in developed world. Most centers in resource constrained countries, like ours lack either the facilities or skills for ESS, or both, yet in others it is only evolving. As such, the commonly available treatment remains external frontoethmoidectomy, especially for large mucoceles.
The aim of this paper is to report our experience with huge frontoethmoidal mucocele with late presentation in a resource constrained nation and to review the literature.

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 2
CASE SERIES
Case 1A 54-year-old man presented with 3 years history of
left-sided frontal swelling, 2½ years history of protrusion of the left eyeball, and 2 years history of intermittent headache and facial fullness. There was a preceding history of nasal congestion. He was referred to us from the ophthalmologist to whom he presented for his blurred vision.
On examination there was a left forehead mass, medial to the left eye, boggy to touch with bony defect and proptosis of the left eye, which was displaced outwards, downwards, and laterally (Figure 1). Anterior rhinoscopy revealed left polypoidal lesion obstructing both the inferior and middle meatus with thick mucosecretions.
The ophthalmic examination documented a cystic mass on the superomedial part of the left orbit. The ipsilateral eye was hypotropic with 15 degree exotropia. The visual acuity was 6/9, right eye (RE), 6/9, left eye (LE). There was diplopia on left gaze but visual fields were within normal limits.
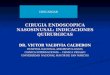
Computed tomography (CT) scan (Figure 2) showed a large isodense soft tissue mass arising from the left ethmoidal sinus involving the frontal sinus and eroding through the upper medial and superior walls of the orbit. Partial erosion of the left frontal bone inner table was noted but no intracranial extension. The left eye was displaced inferiorly and anteriorly.
A diagnosis of frontoethmoidal mucocele was made and patient worked up for left external frontoethmoidectomy using modified Lynch–Howarth approach.
The surgeries were performed under general anesthesia (GA). External frontoethmoidectomy operation was performed under GA. The procedure offered direct access to both the ethmoidal and frontal sinuses with excision of the mucocele and exenteration
of the diseased mucosa. The sinuses were drained using size 24 Foley’s catheter which we further fenestrated for more efficient drainage of the ethmoidal sinuses. It was introduced from the nasal cavity up to the frontal sinus and served as nasofrontal stent as well. The stent which was serially shortened were left in place for six weeks before removal to avoid premature stenosis. They were both followed up for three years without any complaint.
Intraoperatively, the anterior and medial walls of the ethmoid sinus were found eroded. The entire cavity was filled with dark purulent secretions, mucopyocele extending into the frontal sinus obliterating the tables. The procedure was well tolerated and the patient was discharged on the fifth postoperative day after removal of sutures and shortening of the nasal stent. The patient’s six weeks postoperative appearance is as in Figure 3.
Figure 1: Preoperative appearance of case 1.
Figure 2: CT scan showing left sided well circumscribed soft tissue mass with lateral displacement of the orbit.
Figure 3: Postoperative photograph of case 1.

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 3
Case 2A 64-year-old woman presented with left painless
frontal swelling of 11 years duration, protruding left eye ball of 8 years duration. There were preceding histories of recurrent watery rhinorrhea, sneezing bouts associated with allergy more than 10 years before the onset of the presenting complaints.
The patient also had history of recurrent headache and blurring of vision for which she visited two separate ophthalmic centers without relief. She later presented to a prayer house where her condition deteriorated contrary to the earlier promises. The mass kept increasing in size with left eye displacement.
On examination, left superomedial orbital mass, cystic with areas of bone deficit measuring about 8 by 8 cm with non-axial proptosis of the left eye were noted with visual acuity of 6/12 RE and light perception RE. The LE was severely displaced forwards, downwards, and laterally (Figure 4).
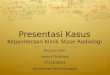
Computed tomography scan showed an expansive non-enhancing hypodense mass involving the left frontal and ethmoidal sinuses as well as orbital cavity displacing the left globe anteriolaterally (Figure 5).
A diagnosis of left frontoethmoidal mucocele was made. External frontoethmoidectomy was performed as in the first case and was well tolerated. She was discharged home seventh day postoperatively. Her postoperative appearance was remarkably improved (Figure 6) and her left visual acuity improved to hand movement. Both patients were followed up for three years without any complaint.
DISCUSSION
Mucoceles can be primary or secondary. A primary mucocele starts with formation of a cyst from a goblet cell gland and grows to expand the sinus. Secondary mucocele results from obstruction of the ostium of the sinus. The obstruction may be due to (i) chronic sinusitis and mucosal edema, (ii) surgical or non-surgical injury, and (iii) tumors pressing on the drainage channel [4–6]. The patients in our series developed mucocele secondary to chronic sinusitis. Paranasal mucoceles predominantly affect the frontal sinus (60–65%), followed in frequency by the ethmoidal (20–30%), maxillary (10%), and sphenoid (2–3%) sinuses [7]. Many other researchers have also reported predominance of frontal sinus involvement, but in a study by Murat et al. in Turkey, the maxillary sinus was the most frequently affected of eighteen (18) patients (n = 9, 50%) [8]. A long-standing untreated mucocele can become infected, forming a mucopyocele, putting the patient at risk for meningitis/cerebritis, orbital cellulitis, and osteomyelitis [8, 9].
Clinical aspects of mucoceles affecting the frontal sinus were primarily described by Langenbeck, in 1819
Figure 4: Preoperative photograph of case 2.
Figure 5: CT scan showing left frontoethmoidal expansile soft tissue mass displacing the orbit laterally. Figure 6: Postoperative appearance of case 2.

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 4
and Berthon proposed surgical drainage of this type of lesion in 1880. The term mucoceles was introduced by Rollet in 1896 and the first histopathological description was made by Onodi in 1901 [1]. Mucocele affects all age groups but it is more common in third and fourth decade of life according to previous researchers [10–12]. While agreeing that no age is immune to development of mucoceles, Prajapati et al. found fourth to seventh decade to be the peak range [13]. Our patients are in the fifth and sixth decade of life respectively. Most researchers reported equal sex distribution [14–16], though Agbara et al. recorded slight male preponderance (M:F= 1.1:1) [17].
Frontoethmoidal mucocele is relatively uncommon in Nigeria. Usually unilateral but bilateral disease has been reported in Nigeria [3, 18]. Only two cases of frontoethmoidal mucocele were seen in our center within a two year period of this study, thus supporting the relative rarity of these lesions in Nigeria. Also our patients fall within the reported age bracket.
Mucocele is a cystic lesion of the epithelial recover layer that affects the paranasal sinuses, contains thick mucus, and has slow growth and expansive characteristics. Its etiology has not been fully defined yet, but it is believed that it is caused by obstruction of the drainage ostium of affected paranasal sinus owing to chronic processes of rhinosinusitis (infectious or allergic), nasosinusal polyposis, craniofacial trauma, previous surgery, benign tumors (osteomas, bone fibrous dysplasia), or malignant neoplasms [19, 20]. Development of mucocele in children with cystic fibrosis of the pancreas and chronic sinusitis has been reported thereby suggesting the hypothesis that intrinsic factors that alter the production of mucus may play a role in the development of these lesions [21]. Madani’s series however did not implicate cystic fibrosis in any of their pediatric cases [8]. That mucocele develop as a complication of chronic rhinosinusitis has been collaborated by a study by Fasunla and Nwaorgu in Ibadan, Nigeria [19]. Like in our study, all our patients presented with initial history of nasal congestion which were unfortunately neglected or trivialized. Mucocele can also be a complication of nasal surgeries. Busaba and Salman reported a large series of ethmoidal mucocele as a late complication of endoscopic ethmoidectomy some of which were actually treated by external approach [20].
There are various theories in the pathogenesis of mucocele like pressure erosion, cystic degeneration of glandular tissue, and active bone resorption and regeneration [22]. Active bone resorption and regeneration theories are supported by greater number of evidence. A number of bone resorbing factors have been found in mucocele mucosa like prostaglandin E2 (PGE2), leukotrienes, hydroeicosatetraenoic acids (HETEs), and a range of cytokines. Also increased levels of interleukin-α (IL-α), IL-1β and tumor necrosis factor-α (TNF-α), vascular adhesion molecules, endothelial leukocyte antigen, e-selectin, and intracellular adhesion molecule (I-CAM) are found in mucocele lining in comparison with normal controls. In normal situation, new bone formation
is balanced by osteolysis. In mucocele, the balance is just tipped in favor of osteolysis facilitating expansion of lesion [22].
Presentation depends upon the site and size of mucocele, and degree of bone erosion. Due to close proximity of the ethmoids to the orbits, majority of these mucoceles have intraorbital extensions giving rise to superior nasal/orbital palpable mass, proptosis, and diplopia. They can also extend into the nasal cavity or intracranially [23].
Since mucocele expands in the direction of least resistance, frontal mucocele tends to erode the thin bone of the superior orbital wall extending into the orbit and displacing the globe inferiorly. Majority therefore present to the ophthalmologist with ocular symptoms such as diplopia, ptosis, proptosis, and epiphora due to displacement of globe [14, 24]. Orbital symptomatology is influenced by the specific area of bone erosion. Thus in a large frontoethmoidal mucocele the clinical picture varies according to whether bone erosion occurs anteriorly or along the orbital roof near the apex. In the later situation the condition may present at the early stage with blurring of vision or defect in the visual field [25]. Loo et al. reported that frontoethmoidal mucocele was second to rhinosinusitis in ear, nose, and throat (ENT) diseases causing ocular manifestation [26].
In our environment patients usually present after a long delay as they would usually have consulted the traditional or spiritual healers and quacks before coming to the specialist thereby increasing the likelihood of orbital and/or intracranial extension. Commonly these patients present more with ophthalmic symptoms which include periorbital swelling, proptosis, diplopia, epiphora, visual impairment, strabismus, and orbital cellulitis. Orbital cellulitis could occur if in long-standing case, the mucocele ruptures and spills into the orbit or as a complication of surgery. In our case study, all our patients presented with proptosis as well as periorbital swelling similar to the study of Ajaiyeoba et al. at Ibadan, Nigeria [27].
Consequently, these patients usually present to the ophthalmologist first before presenting to the otorhinolaryngologist. An unsuspecting ophthalmologist may further delay the patient. In this study, our first patient presented to ENT clinic 3 years after presentation to an ophthalmologist while the second came to us 11 years after first encounter with an ophthalmologist in a different center. Worse still in our environment patients regard all sorts of eye professionals as ophthalmologists, these are not surgeons and may delay the patient on false hopes.
Computed tomography (CT), pre- and post-contrast, is currently the diagnostic method of choice for paranasal sinus pathology. On the basis of three-dimensional reconstructions, the localization and extent of a mucocele can be precisely determined and possible bone erosion can be diagnosed. Moreover, the surgeon obtains important information on the individual anatomy of

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 5
the frontal sinus and the other paranasal sinuses. This knowledge is an important prerequisite for planning surgical interventions [2, 28, 29]. However magnetic resonance imaging (MRI) may be helpful whenever there is extension beyond the sinus boundaries and in differentiating mucocele from meningoencephaloceles and other expansile sinonasal lesions [30].
Treatment of mucocele is surgical. The goals of surgery are eradication of the mucocele with minimal morbidity and prevention of recurrence. Gupta et al. observed that surgical approaches are based on the size, location, and extent of the mucocele [31]. Surgical approaches could involve an external approach (Lynch–Howarth frontoethmoidectomy) or osteoplastic flap with sinus cavity obliteration [24]. The patients in our series both had successful frontoethmoidectomy, also all the 12 patients in a ten (10) year review in Southwestern Nigeria and all had similar external approach [32]. Endoscopic drainage has been advocated so as to allow preservation of the frontal sinus mucosa and maintenance of a patent frontal recess [33].
Open surgery remains a valid procedure in frontal mucoceles with orbital and/or cranial extension or osteomyelitis, and in developing world where only few centers have facilities for endoscopic nasal surgery [34]. Late presentation and extensive disease favor radical approach [19]. Both patients in our series presented late and had orbital extension thereby favoring radical procedure.
External approach is indicated in cases where the anatomical extent of the disease or previous surgery restricts visualization and access to the frontal sinus. If the mucocele of the frontal sinus cannot be accessed through an endonasal access and if a lasting drainage function thus cannot be guaranteed, an extranasal, transfacial procedure is indicated [2]. Some researchers have actually found combined endoscopic and open approach very useful in some of their patients [35, 36].
However, in the developed world with modern facilities and expertise, FESS is the current treatment of choice. Its advantage being that morbidity and mortality are reduced, no external incision is involved and endoscopic examination can be performed for regular follow-up of these patients.
There is need for multidisciplinary approach in the management of non-thyroid unilateral proptosis irrespective of the method to be used [37]. In both cases the ophthalmologists and the otorhinolaryngologists worked together to optimize outcome.
CONCLUSION
Frontoethmoidal mucocele is a relatively rare benign lesion that presents with painless periorbital swelling usually neglected until it becomes massive and disfiguring. When treatment is delayed it can lead to very serious ophthalmic and neurosurgical
complications. Though currently FESS is the advocated and common procedure in developed world, external approach of frontoethmoidectomy (Lynch–Howarth approach) remains relevant in developing nations due to one or combination of the following: late presentation, unavailability or scarcity of the equipment, the long learning curve, and cost of the maintenance. Due to late presentation our patients presented with massive mucocele with orbital extension and were managed successfully with external frontoethmoidectomy. More importantly this paper joins many of its kind to advocate for prompt and appropriate referral and multidisciplinary cooperation in management of frontoethmoidal mucocele.
REFERENCES
1. de Oliveira Vicente A, Chaves AG, Takahashi EN, Akaki F, Sampaio AA, Matsuyama C. Mucocele frontoetmoidal: Relato de casos e revisão da literatura. Rev Bras Otorrinolaringol 2004;70(6):850–4.
2. Constantinidis J, Steinhart H, Schwerdtfeger K, Zenk J, Iro H. Therapy of invasive mucoceles of the frontal sinus. Rhinology 2001;39(1):33–8.
3. Ologe FE, Odebode TO, Owoeye JFA, Eletta PA. Ophthalmic manifestations of fronto-ethmoidal mucocoeles: A report of five cases. Afr J Med Med Sci 2003;32(2):209–14.
4. Kochhar LK, Chaudhry S, Kumar A. Frontoethmoidal mucocele: A case report. Med J Armed Forces India 1995;51(4):290–1.
5. Dragan K, Zoran P, Dragan M, Miloš T, Nikola Ž, Staša K. Clinical analysis and surgical treatment of frontal sinus mucoceles: 10 years experience of seven cases. Srpski Arhiv za Celokupno Lekarstvo 2017;145(11–12):618–22.
6. Jevtovic A, Belic B, Stojanovic J. Combined surgical approach in the treatment of oculo-orbital complications of frontal sinus mucocele: A case report. Serbian J Exp Clin Res 2019.
7. Park CM, Stoffella E, Gile J, Roberts J, Herford AS. Osteoplasty flap technique for repair of latent (30-year) post-traumatic frontal sinus mucocele: Case report and review of the literature. J Oral Maxillofac Surg 2012;70(9):2092–6.
8. Bockmühl U, Kratzsch B, Benda K, Draf W. Paranasal sinus mucoceles: Surgical management and long term results. [Article in German]. Laryngorhinootologie 2005;84(12):892–8.
9. Knopman J, Sigounas D, Huang C, Kacker A, Schwartz TH, Boockvar JA. Combined supraciliary and endoscopic endonasal approach for resection of frontal sinus mucoceles: Technical note. Minim Invasive Neurosurg 2009;52(3):149–51.
10. Di Cicco M, Costantini D, Padoan R, Colombo C. Paranasal mucoceles in children with cystic fibrosis. Int J Pediatr Otorhinolaryngol 2005;69(10):1407–13.
11. Capra GG, Carbone PN, Mullin DP. Paranasal sinus mucocele. Head Neck Pathol 2012;6(3):369–72.
12. Obeso S, Llorente JL, Rodrigo JP, Sánchez R, Mancebo G, Suárez C. Paranasal sinuses mucoceles. our experience in 72 patients. [Article in Spanish].

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 6
Acta Otorrinolaringol Esp 2009;60(5):332–9.13. Prajapati V, Khilnani AK, Gami G, Bhalodiya N,
Gupta D. Fronto-ethmoidal mucoceles: A study of 25 cases. Int J Otorhinolaryngol Head Neck Surg 2017;3(1):112–5.
14. Catalano P, Schlewet M. Frontal sinus mucocele after osteoplastic flap surgery: Case report. Arch Clin Med Case Rep 2017;1(3):67–75.
15. Arrué P, Kany MT, Serrano E, et al. Mucoceles of the paranasal sinuses: Uncommon location. J Laryngol Otol 1998;112(9):840–4.
16. Jacobson AL, Lawson W, Biller HF. Bilateral pansinus mucocele with bilateral orbital and intracranial extension. Otolaryngol Head Neck Surg 1982;90(4):507–9.
17. Rowland A, Chukwudi OA, Joseph OO, Albert OU. Frontocele: Experience from a resource challenged environment. Egyptian Journal of Ear, Nose, Throat and Allied Sciences 2016;17(1):31–7.
18. Odebode TO, Ologe FE, Segun-Busari S, Nzeh DA. Recurrent bilateral fronto-ethmoidal mucocoele with intracranial extension: A case report. West Afr J Med 2005;24(3):268–71.
19. Fasunla JA, Nwaorgu OGB. Adult chronic rhinosinusitis: Spectrum of clinical features in a tertiary health institution and literature review. East Cent Afr J Surg 2011;16(1):12–8.
20. Busaba NY, Salman SD. Ethmoid mucocele as a late complication of endoscopic ethmoidectomy. Otolaryngol Head Neck Surg 2003;128(4):517–22.
21. Evans C. Aetiology and treatment of fronto-ethmoidal mucocele. J Laryngol Otol 1981;95(4):361–75.
22. Pradhan B. Endoscopic marsupialization of fronto ethmoidal mucocele. Nepalese Journal of ENT Head and Neck Surgery 2014;3(2):29–30.
23. Khong JJ, Malhotra R, Wormald PJ, Selva D. Endoscopic sinus surgery for paranasal sinus mucocoele with orbital involvement. Eye (Lond) 2004;18(9):877–81.
24. James E, Dutta A, Swami H, Ramakrishnan R. Frontal mucocele causing unilateral proptosis. Med J Armed Forces India 2009;65(1):73–4.
25. Sen DK, Puri ND, Majid A. Fronto-ethmoidal mucocele as a cause of unilateral proptosis. Indian J Ophthalmol 1979;27(2):45–8.
26. Loo JL, Looi ALG, Seah LL. Visual outcomes in patients with paranasal mucoceles. Ophthalmic Plast Reconstr Surg 2009;25(2):126–9.
27. Ajaiyeoba A, Kokong D, Onakoya A. Clinicopathologic, ophthalmic, visual profiles and management of mucoceles in blacks. J Natl Med Assoc 2006;98(1):63–6.
28. Singh J, Velankar H, Dabholkar Y, Bhalekar S. Frontoethmoidal mucocele with unilateral proptosis. Otorhinolaryngology Clinics: An International Journal 2011;3(2):125–8.
29. Kennedy DW. Prognostic factors, outcomes and staging in ethmoid sinus surgery. Laryngoscope 1992;102(12 Pt 2 Suppl 57):1–18.
30. Morsy MA, Khan A, Chemla ES. Prosthetic axillary-axillary arteriovenous straight access (necklace graft) for difficult hemodialysis patients: A prospective single-center experience. J Vasc Surg 2008;48(5):1251–4, 1254.e1.
31. Gupta P, Sharma A, Singh J, Ojha T. Giant frontoethmoidal osteoma with orbital involvement: A rare case report with review of literature. Romanian Neurosurgery 2017;31(4):540–4.
32. Fasina O, Okoh SS. Paranasal sinus mucoceles in a tertiary center, Southwestern Nigeria: A 10-year review of ophthalmic features, management, and outcome. J Clin Sci 2018;15(4):183–5.
33. Kuhn FA, Javer AR. Primary endoscopic management of the frontal sinus. Otolaryngol Clin North Am 2001;34(1):59–75.
34. Pace-Asciak P, Hathorn IF, Sunkaraneni V, Chen R, Habib A, Javer AR. Balloon dilatation for the frontal sinus. Otolaryngol Neck Surg 2012;147(2 Suppl):P107.
35. Serrano E, Klossek JM, Percodani J, Yardeni E, Dufour X. Surgical management of paranasal sinus mucoceles: A long-term study of 60 cases. Otolaryngol Head Neck Surg 2004;131(1):133–40.
36. Caylakli F, Yavuz H, Cagici AC, Ozluoglu LN. Endoscopic sinus surgery for maxillary sinus mucoceles. Head Face Med 2006;2:29.
37. Jeyasakthy S, Norasnieda MS. Diplopia secondary to a frontoethmoidal mucocoele. Brunei Int Med J 2019;12(1):35–7.
*********
Author ContributionsEE Afiadigwe – Conception of the work, Design of the work, Acquisition of data, Interpretation of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
AI Apakama – Conception of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
G Obasikene – Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
JU Obah – Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
SNN Nwosu – Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related

Journal of Case Reports and Images in Otolaryngology, Vol. 1, 2020.
J Case Rep Images Otolaryngol 2020;1:100002Z18EA2020.www.ijcriotolaryngology.com
Afiadigwe et al. 7
to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone.
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Conflict of InterestAuthors declare no conflict of interest.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Copyright© 2020 EE Afiadigwe et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.
Access full text article onother devices
Access PDF of article onother devices