Embed Size (px)
Citation preview

Special supplement The Journal of Dental Hygiene 1
ver the last 30 years we havelearned much about the etiol-
ogy progression and treatment ofperiodontal diseases For examplewe know that the accumulation ofdental biofilm can trigger resultantinflammatory and immune responsesDental biofilm contains a vast diver-sity of microbial species some ofwhich have been identified as etio-logic agents for systemic diseases
Risk factors for periodontitis canbe grouped into categories such asmicrobial systemic behavioral andlocal Controlling risk factors isimportant to the management ofperiodontal diseases and is some-thing that should be an overall goalfor every dental hygienist One riskfactor for disease that can be con-trolled in the majority of cases isdental biofilm However control ofdental biofilm is dependent on manyfactors including the knowledge ofthe dental hygienist regarding evi-dence-based strategies for diseaseprevention and treatment
We have an extensive amount ofscientific evidence available to edu-cate every oral health care profes-sional about periodontal diseasesHowever dental practice manage-ment experts report that many clini-cians are not adequately diagnosingdocumenting or monitoring diseasestatus or making treatment recom-
mendations to patients based on evi-dence-based strategies Many ques-tions arise about the best treatmenttechniques products and recom-mendations for patients who havechronic periodontitis or are at risk forthe disease The patient is dependenton the dental hygienist to be at theforefront of prevention It is vital fordental hygienists to have up-to-dateaccurate information so they can edu-cate and make appropriate recom-mendations for the individual patient
This supplement of the Journal ofDental Hygiene includes articles thatwill educate every dental hygienistabout the evidence base for treat-ment of chronic periodontitis DrCharles Cobb is an internationalexpert on dental biofilm and theeffect of nonsurgical methods forremoving biofilm and hard deposits(calculus) on the tooth and root sur-faces He provides a comprehensiveevidence-based review of what den-tal hygienists can expect from non-surgical therapies Drs DavidPaquette and Maria Ryan 2 world-renowned periodontists and I pres-ent a comprehensive paper on theevidence base for the use of locallydelivered antimicrobials Since theirinception 3 decades ago oral healthcare professionals have been utiliz-ing locally delivered antimicro-bialsantibiotics to treat chronic peri-
odontitis Still questions arise abouttheir utility and ability to treat andcontrol this disease This paper pres-ents the clinical evidence for use oflocally delivered antimicrobials inpatient care Finally Dr LarrySweeting Ms Karen Davis and DrCharles Cobb put the evidence intoan action plan for dental hygienistsDr Sweeting and Ms Davis are den-tal clinicians as well as professionalspeakers and consultants Theirpaper discusses the effectiveness ofusing a Periodontal Treatment Pro-tocol to assist in the early diagnosisand treatment of periodontal dis-eases It also discusses insurancecoding vital verbal skills to use withpatients and considerations forimplementation of locally deliveredantimicrobials into a general clini-cal practice
I want to extend sincere apprecia-tion to OraPharma Inc for their sup-port of this supplement OraPharmaInc has been diligent in their goalof conducting evidence-based scien-tific investigations in order to helpall oral health care professionals bet-ter diagnose and treat periodontaldiseases
Rebecca S Wilder RDH BS MSEditor-in-Chief Journal of DentalHygieneRebeccaWadhanet
From the Editor-in-Chief of the Journal of Dental Hygiene
O
This special issue of the Journal of Dental Hygiene wassponsored by an educational grant from OraPharma Inc
This supplement can also be accessed online atwwwadhaorgCE_courses
To obtain two hours of continuing education credit complete thetest at wwwadhaorgCE_coursescourse20
4 The Journal of Dental Hygiene Special supplement
Introduction
Typically the term ldquoperiodontal dis-easerdquo refers to gingivitis and periodonti-tis both common inflammatory diseasesthat involve a variety of pathogenic bac-terial species and an innate host responseto those bacteria1 Gingivitis the mostfamiliar form of inflammatory perio-dontal disease has a high prevalencerate affecting 50-90 of adultsworldwide23 By definition gingivitis islimited to an inflammation that involvesonly the gingival soft tissues ie gingi-val epithelium and subjacent fibrousconnective tissues In spite of its highprevalence rate and worldwide distribu-tion biofilm (plaque)- induced gingivitisis preventable and rather easily reversedby routine oral hygiene measures
Inflammation that extends into thedeeper tissues to involve bone resultingin resorption of tooth supporting bone istermed periodontitis Concomitant withthe loss of bone is the formation of adeepened space between the root of thetooth and the gingiva a periodontalpocket Periodontitis can present as achronic and slowly progressing disease(most common form) or as an aggres-sive disease causing loss of bone over arelatively short period of time Peri-odontitis of advanced severity can resultin tooth mobility occasional pain anddiscomfort (generally associated withabscess formation) impaired ability tomasticate food and eventual tooth loss
Although more common to adultsepidemiologic data indicate that peri-odontitis can also be found in childrenand adolescents45 In the United Stateschronic periodontitis is more prevalentin men than women and in AfricanAmericans Native Americans andMexican Americans than Caucasians267
Various epidemiology studies when
considered in aggregate suggest a pro-gressive decrease in the prevalence ofperiodontitis between the years 1988-20047-11 The more recent of these stud-ies indicate a prevalence rate for mod-erate to advanced periodontitis rangingfrom approximately 5 to 15 for indi-viduals gt 18 years of age9-11 Given thecurrent US Department of Census pro-jections a 5 to 15 prevalence ratetranslates to 11 to 33 million US adultsthat may exhibit periodontitis of moder-ate to advanced severity12 If oneincludes slight severity the prevalencerate for periodontitis increases toapproximately 30 of the US adult pop-
ulation or roughly 65 million individu-als9-12 However all epidemiology stud-ies that have reported on the prevalenceof chronic periodontitis have utilizedpartial-mouth examinations which tendto underestimate prevalence extent andseverity of disease13-15
Microbes and Biofilm
A biofilm is a complex community ofmicroorganisms characterized by theexcretion of an adhesive and protectiveextracellular matrix microbe-to-microbeattachment structural heterogeneity
SupplementSupplement
Abstract
Biofilms are a complex community of microorganisms characterized bythe excretion of an adhesive and protective extracellular matrix microbe-to-microbe attachment structural heterogeneity genetic diversity andcomplex community interactions Bacteria growing in dental biofilmsdisplay an increased tolerance to antibiotics and antimicrobial agentsincluding those used in dentifrices and mouthrinses
The microbial challenge associated with the inflammatory periodontaldiseases induces an immediate inflammatory and immune response inthe host The nature and magnitude of the response has an impact onthe severity and rate of progression of the periodontal disease It is thishost inflammatory-immune response that ultimately leads to the clinicalsigns and symptoms of gingivitis and chronic periodontitis The traditionaltreatment modality of scaling and root planing (SRP) remains the ldquogoldstandardrdquo for the non-surgical management of chronic periodontitisEven clinically successful treatment has a high probability of pocket re-infection Re-infection of periodontal pockets results from residualbiofilms increased tolerance of microbes within a dense mature biofilmto antibiotics reservoirs of bacteria in calculus and reservoirs of bac-teria within the dentinal tubules of infected root surfaces Thus for max-imum effect a combination of scaling and root planing and locally deliv-ered antimicrobials should be considered if non-surgical therapy is thetreatment of choice
Keywords periodontal disease periodontal infection chronic peri-odontitis scaling and root planing dental biofilm
Microbes Inflammation Scaling and Root Planingand the Periodontal ConditionCharles M Cobb DDS MS PhD
Special supplement The Journal of Dental Hygiene 5
genetic diversity and complex commu-nity interactions Dental plaque is amicrobial biofilm (Figure 1) As withany biofilm the constituent microbesare tightly adherent to each other andto an oral substrate by means of anextracellular matrix ie slime layer orglycocalix into which they are embed-ded1617 The microbial populations inbiofilm have 2 strategies that enablethem to successfully survive withintheir community The first is a high rateof reproduction for continued survivaland the second is physiologic adapta-tion to the available environmentalresources or life-supporting capacity ofthe environment18
Biofilms inherently dictate profoundchanges in the behavior of individualmicrobes their relationship to the hostand their response to environmentalconditions19 Indeed oral biofilms asdistinct entities are the causative agentsof biological processes such as dentalcaries periodontal disease and peri-implantitis rather than any singlemicrobe evading the host defense andcausing disease20 Biofilms exhibit char-acteristics that impact the clinical man-agement of inflammatory periodontaldisease For example both altered pat-terns of microbial gene expression andthe composition and density of the
extracellular matrix reduce the suscep-tibility of microbes to antimicrobialagents21-23 Bacteria growing in dentalbiofilms display an increased toleranceto antimicrobial agents including thoseused in dentifrices and mouthrinses24-27
In addition confocal microscopy of insitu established natural biofilms showedthat chlorhexidine only affected theouter layers of cells in 24 and 48 hourplaque biofilms suggesting eitherquenching of the agent at the biofilmsurface or a lack of penetration28 Fur-ther biofilms of oral bacteria are alsomore tolerant of antibiotics (eg amoxy-cillin doxycycline minocycline andmetronidazole) than planktonic cells29-31
In this regard biofilms of Porphy-romonas gingivalis have been shown totolerate 160 times the minimuminhibitory concentration (MIC) ofmetronidazole that was determined forplanktonic cells32
Over 700 species of aerobic andanaerobic bacteria have been identifiedin the human oral cavity3334 Themicrobes grow as complex mixedinterdependent colonies in biofilms andmay achieve considerable thicknessachieving a thickness of 1 mm within96 hours if left undisturbed1617 Oralbiofilms like all microbial biofilmsexhibit a successional colonization with
gram-positive aerobic Streptococcispecies (spp) being the initial coloniz-ers followed in sequence by Actino-myces spp Corynebacterium spp Veil-lonella spp and then in more maturebiofilm a variety of gram-negativeanaerobic microbes such as Treponemaspp Fusobacterium spp Porphy-romonas spp Prevotella spp and Tan-nerella spp173536
As the biofilm is allowed to maturewith concomitant increases in thick-ness the percentage of Gram-negativeanaerobic microbes increases Specificcomplexes of such microbes com-monly cohabit subgingival sites andare consistently associated withinflammatory periodontal diseases35
These putative microbial pathogensinclude Porphyromonas gingivalisTannerella forsythia and Treponemadenticola35
In the human host the transition fromgingivitis to periodontitis does not occurautomatically either in every patient orevery site but depends on 3 factors 1)degree of host susceptibility 2) presenceand numbers of pathogenic bacteria and3) presence and numbers of protectivebacteria36 Pathogenic bacteria exhibitvirulence features that decrease theeffectiveness of the host response byinducing tissue degradation and retard-ing attempts at healing
Host defense mechanisms are im-paired through a variety of mecha-nisms As one example consider thatAggregatibacter (formally Actinobacil-lus) actinomycetemcomitans produces aleukotoxin that alters the cell mem-branes of neutrophils and monocytesand thereby alters chemotactic andphagocytic responses36 Infection withGram-negative anaerobes is accompa-nied by the release of epitheliotoxinsendotoxins leukotoxins collagenasegellatinase elastase fibrinolysins andother proteolytic enzymes37 These bac-terial toxins and enzymes are tissue irri-tants andor cytotoxic and viewed bythe host immune system as foreign pro-teins (Figure 2) The aggregate cellu-lartissue insult activates the hostimmune system locally and is gener-ally visualized at a clinical level asinflammation with all the inherent gin-gival changes eg vasculitis edema andswelling change in tissue color fromwhite-pink to red or red-purple andspontaneous gingival bleeding or bleed-ing on provocation38
Figure 1 Scanning electron microscopic photograph of root associ-ated dental biofilm (plaque) Bar = 10 micron at an original magnifi-cation of 2840x
6 The Journal of Dental Hygiene Special supplement
Role of the HostImmune Response
Bacteria are necessary but not suffi-cient by themselves to produce adestructive periodontal disease Diseaseinitiation and progression requires asusceptible host38 The microbial chal-lenge induces an immediate inflamma-tory and immune response in the hostThe nature and magnitude of theresponse have an impact on the sever-ity and rate of progression of the peri-odontal disease39 Locally bacteria andtheir metabolic byproducts stimulate acellular immune response within theaffected gingiva represented by a denseinfiltration of neutrophils macro-phages and lymphoid cells These cellsand host connective tissue cells withinthe developing inflammatory lesion arestimulated to synthesize and releaseproinflammatory cytokines prosta-noids and proteolytic enzymes eginterleukin-1 (IL-1) interleukin-6 (IL-6) interleukin-8 (IL-8) tumor necro-sis factor-alpha (TNF-α) prostaglandinE2 (PGE2) matrix metalloproteinases38
It is this host inflammatory-immuneresponse that ultimately leads to theclinical signs of gingivitis and chronicperiodontitis and their characteristicfeatures of fibrous connective tissuedegradation resorption of tooth sup-porting alveolar bone and periodontalpocket formation
In contrast to the epidermis of skinthe epithelial lining of the soft tissuewall of a periodontal pocket lacks a stra-tum corneum and stratum granulosumConsequently the pocket epithelium iseasily ulcerated and breached by inva-sive subgingival pathogenic bacteria40
In addition endotoxins and other micro-bial antigens may gain access to theunderlying connective tissues and gin-gival vasculature leading to bacteremiaand endotoxemia There is considerableevidence that the locally produced pro-inflammatory cytokines and prostanoidsgain access to the circulatory system andmay in turn induce the production ofliver-derived markers of a systemicinflammatory reaction such as C-reac-tive protein fibrinogen serum amyloid-A and haptoglobin41-45 Elevations inboth the locally generated inflammatorymediators and systemic markers ofinflammation have been associated withvarious systemic diseases such as ath-
erosclerosis46 cardiovascular disease47
ischemic stroke48 pre-eclampsia49 andpoor glycemic control 50 in diabeticpatients
Risk FactorsAssociated WithDevelopment ofChronic Periodontitis
In addition to the accepted associa-tions of pathogenic microbes to thepathogenesis of inflammatory peri-odontal diseases several genetic andenvironmental risk factors have beenidentified that affect the host response Itis well established that the prevalenceand severity of chronic periodontitisincreases with advancing age poor oralhygiene marginally or poorly controlledtype I and II diabetes and use oftobacco5152 In addition data from twinstudies indicate that about 50 of thepopulation variance in periodontitis canbe attributed to genetic factors5354 Sev-eral studies indicate that genetic poly-morphisms (variations) in a cluster of atleast 3 genes on chromosome 2q13
which control the production of proin-flammatory cytokines may affect thesystemic inflammatory response in asignificant percentage of people withchronic periodontitis5556
Scaling and RootPlaning in the Controlof Chronic Periodontitis
Periodontitis is a chronic and pro-gressive inflammatory disease forwhich there is no known cure It is nowwell-established that periodontitis isnot associated with a single microor-ganism but rather the initiation andprogression of periodontitis is theresult of the hostrsquos immune responseto a consortium of bacteria For peri-odontopathic bacteria to initiate peri-odontitis it is essential that they areable to colonize subgingival pocketsand produce virulence factors thatdirectly damage host tissue Thus amajor goal of nonsurgical periodontaltherapy is to suppress to the extentpossible the subgingival pathogenicmicrobial flora and thereby signifi-
Figure 2Transmission electron microscopic photograph of a nega-tively stained Phorphyromonas gingivalis featuring fimbriae andnumerous surface blebs that likely contain endotoxin Both fimbriaeand endotoxin are potent antigens that solicit a host immuneresponse Original magnification of 35 000x
cantly reduce or eliminate the associ-ated inflammatory lesion
Dental calculus was the original eti-ologic agent associated with develop-ment of chronic periodontitis In the1960s and 1970s it was established thatthe rough irregular surface of dental cal-culus was always covered with a non-mineralized microbial biofilm (Figure3)57-59 In addition to the surface biofilmat least one recent study has identifiedthe presence of several viable periodon-tal pathogens within the mass of dentalcalculus ie Aggregatibacter actino-mycetemcomitans Treponema denticolaand Porphyromonas gingivalis60 Inter-estingly the persistence of Porphy-romonas gingivalis in the subgingivalenvironment following periodontal ther-apy has been associated with progres-sive alveolar bone loss61 In support ofthis observation Offenbacher et al62
recently reported a significant associa-tion between serum immuneoglobulinG (IgG) titers against Porphyromonasgingivalis in patients that exhibit deepPDs (gt 4 mm) and moderate (gt 10 tolt 50) and severe (gt 50) bleeding onprobing
In spite of the fact that calculus canserve as a reservoir for pathogenicmicrobes the role of subgingival cal-culus as an etiologic agent in chronicperiodontitis was relegated to second-ary status once microbial biofilm wasdeclared the primary extrinsic etiologicfactor Thus the need for completeremoval of subgingival calculusbecame a subject for debate63 How-ever the traditional treatment modal-ity of scaling and root planing (SRP)remains the ldquogold standardrdquo for thenonsurgical management of periodon-titis64
The periodontal literature is repletewith studies showing that treatment ofperiodontitis by SRP results in reduc-tions in probing depth (eg a meanreduction of 129 mm for 4-6 mm pock-ets and a mean of 216 mm for pocketsof gt 7 mm) and subgingival bacterialloads and gains in clinical attachment65-
67 Probing depth (PD) reduction is gen-erally greater at sites with deeper ini-tial probing depths The decrease in PDis the result of 2 phenomena shrinkageof the pocket soft tissue wall manifestedas recession of the gingival marginwhich results from a decrease in softtissue inflammation and the inherentedema and gain in clinical attachment
The latter usually accounts for roughlyone-half of the probing depth reduc-tion65-67 In general clinicians shouldevaluate post-SRP healing at 4 to 6weeks following treatment After 6weeks most of the healing has takenplace but repair and collagen matura-tion may continue for an additional 9months6768
Three relevant observations must beconsidered when deciding to use non-surgical therapy as the primary modal-ity for treatment of early to moderatechronic periodontitis First regardingSRP clinicians must be careful wheninterpreting data from published clini-cal trials as they may not accuratelyreflect the private practice setting interms of time skill level severity ofdisease and diversity of patient popu-lation65 For example university-con-ducted clinical trials often use highlyskilled clinicians select patients forlevel of disease and report spending 10minutes per tooth when performingSRP6667 Ten minutes per tooth equatesto about 70 minutes per quadrant It isthe experience of this author that in pri-vate practice a quadrant of SRP may becompleted in approximately 60 minutesregardless of the level of disease and
this allows approximately 10 minutesfor setting of the patient and adminis-tration of anesthetic Greenstein67 hasrightfully noted that decreased timedevoted to SRP in more recent studiesprobably accounts for the diminishedresults reported when to the more clas-sic clinical trials Second one mustremember that microbes embedded ina mature undisturbed subgingivalbiofilm may exhibit an increased toler-ance to antimicrobial agents28-32 Thirdeven when chronic periodontitis istreated successfully the reduction insubgingival pathogenic microbes istransitory SRP of diseased root sur-faces can open dentinal tubules allow-ing invasion by periodontal pathogensinto the exposed tubules and possiblythen serve as a reservoir for re-infec-tion of the pocket6970 Thus the need forfollow-up treatment usually consistingof supra- and subgingival debridementat 3 to 4 month intervals is necessary tomaintain the initially gained beneficialeffects7172 Collectively considered thedistinct probability of less than idealresults from SRP and pocket re-infec-tion by residual microbes is a forcefulargument for the use of adjunctivetreatment modalities in addition to SRP
Special supplement The Journal of Dental Hygiene 7
Figure 3 Scanning electron microscopic photograph of dental cal-culus characterized by a superficial layer of microbial biofilm Bar =10 micron at an original magnification of 1770x
8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

4 The Journal of Dental Hygiene Special supplement
Introduction
Typically the term ldquoperiodontal dis-easerdquo refers to gingivitis and periodonti-tis both common inflammatory diseasesthat involve a variety of pathogenic bac-terial species and an innate host responseto those bacteria1 Gingivitis the mostfamiliar form of inflammatory perio-dontal disease has a high prevalencerate affecting 50-90 of adultsworldwide23 By definition gingivitis islimited to an inflammation that involvesonly the gingival soft tissues ie gingi-val epithelium and subjacent fibrousconnective tissues In spite of its highprevalence rate and worldwide distribu-tion biofilm (plaque)- induced gingivitisis preventable and rather easily reversedby routine oral hygiene measures
Inflammation that extends into thedeeper tissues to involve bone resultingin resorption of tooth supporting bone istermed periodontitis Concomitant withthe loss of bone is the formation of adeepened space between the root of thetooth and the gingiva a periodontalpocket Periodontitis can present as achronic and slowly progressing disease(most common form) or as an aggres-sive disease causing loss of bone over arelatively short period of time Peri-odontitis of advanced severity can resultin tooth mobility occasional pain anddiscomfort (generally associated withabscess formation) impaired ability tomasticate food and eventual tooth loss
Although more common to adultsepidemiologic data indicate that peri-odontitis can also be found in childrenand adolescents45 In the United Stateschronic periodontitis is more prevalentin men than women and in AfricanAmericans Native Americans andMexican Americans than Caucasians267
Various epidemiology studies when
considered in aggregate suggest a pro-gressive decrease in the prevalence ofperiodontitis between the years 1988-20047-11 The more recent of these stud-ies indicate a prevalence rate for mod-erate to advanced periodontitis rangingfrom approximately 5 to 15 for indi-viduals gt 18 years of age9-11 Given thecurrent US Department of Census pro-jections a 5 to 15 prevalence ratetranslates to 11 to 33 million US adultsthat may exhibit periodontitis of moder-ate to advanced severity12 If oneincludes slight severity the prevalencerate for periodontitis increases toapproximately 30 of the US adult pop-
ulation or roughly 65 million individu-als9-12 However all epidemiology stud-ies that have reported on the prevalenceof chronic periodontitis have utilizedpartial-mouth examinations which tendto underestimate prevalence extent andseverity of disease13-15
Microbes and Biofilm
A biofilm is a complex community ofmicroorganisms characterized by theexcretion of an adhesive and protectiveextracellular matrix microbe-to-microbeattachment structural heterogeneity
SupplementSupplement
Abstract
Biofilms are a complex community of microorganisms characterized bythe excretion of an adhesive and protective extracellular matrix microbe-to-microbe attachment structural heterogeneity genetic diversity andcomplex community interactions Bacteria growing in dental biofilmsdisplay an increased tolerance to antibiotics and antimicrobial agentsincluding those used in dentifrices and mouthrinses
The microbial challenge associated with the inflammatory periodontaldiseases induces an immediate inflammatory and immune response inthe host The nature and magnitude of the response has an impact onthe severity and rate of progression of the periodontal disease It is thishost inflammatory-immune response that ultimately leads to the clinicalsigns and symptoms of gingivitis and chronic periodontitis The traditionaltreatment modality of scaling and root planing (SRP) remains the ldquogoldstandardrdquo for the non-surgical management of chronic periodontitisEven clinically successful treatment has a high probability of pocket re-infection Re-infection of periodontal pockets results from residualbiofilms increased tolerance of microbes within a dense mature biofilmto antibiotics reservoirs of bacteria in calculus and reservoirs of bac-teria within the dentinal tubules of infected root surfaces Thus for max-imum effect a combination of scaling and root planing and locally deliv-ered antimicrobials should be considered if non-surgical therapy is thetreatment of choice
Keywords periodontal disease periodontal infection chronic peri-odontitis scaling and root planing dental biofilm
Microbes Inflammation Scaling and Root Planingand the Periodontal ConditionCharles M Cobb DDS MS PhD
Special supplement The Journal of Dental Hygiene 5
genetic diversity and complex commu-nity interactions Dental plaque is amicrobial biofilm (Figure 1) As withany biofilm the constituent microbesare tightly adherent to each other andto an oral substrate by means of anextracellular matrix ie slime layer orglycocalix into which they are embed-ded1617 The microbial populations inbiofilm have 2 strategies that enablethem to successfully survive withintheir community The first is a high rateof reproduction for continued survivaland the second is physiologic adapta-tion to the available environmentalresources or life-supporting capacity ofthe environment18
Biofilms inherently dictate profoundchanges in the behavior of individualmicrobes their relationship to the hostand their response to environmentalconditions19 Indeed oral biofilms asdistinct entities are the causative agentsof biological processes such as dentalcaries periodontal disease and peri-implantitis rather than any singlemicrobe evading the host defense andcausing disease20 Biofilms exhibit char-acteristics that impact the clinical man-agement of inflammatory periodontaldisease For example both altered pat-terns of microbial gene expression andthe composition and density of the
extracellular matrix reduce the suscep-tibility of microbes to antimicrobialagents21-23 Bacteria growing in dentalbiofilms display an increased toleranceto antimicrobial agents including thoseused in dentifrices and mouthrinses24-27
In addition confocal microscopy of insitu established natural biofilms showedthat chlorhexidine only affected theouter layers of cells in 24 and 48 hourplaque biofilms suggesting eitherquenching of the agent at the biofilmsurface or a lack of penetration28 Fur-ther biofilms of oral bacteria are alsomore tolerant of antibiotics (eg amoxy-cillin doxycycline minocycline andmetronidazole) than planktonic cells29-31
In this regard biofilms of Porphy-romonas gingivalis have been shown totolerate 160 times the minimuminhibitory concentration (MIC) ofmetronidazole that was determined forplanktonic cells32
Over 700 species of aerobic andanaerobic bacteria have been identifiedin the human oral cavity3334 Themicrobes grow as complex mixedinterdependent colonies in biofilms andmay achieve considerable thicknessachieving a thickness of 1 mm within96 hours if left undisturbed1617 Oralbiofilms like all microbial biofilmsexhibit a successional colonization with
gram-positive aerobic Streptococcispecies (spp) being the initial coloniz-ers followed in sequence by Actino-myces spp Corynebacterium spp Veil-lonella spp and then in more maturebiofilm a variety of gram-negativeanaerobic microbes such as Treponemaspp Fusobacterium spp Porphy-romonas spp Prevotella spp and Tan-nerella spp173536
As the biofilm is allowed to maturewith concomitant increases in thick-ness the percentage of Gram-negativeanaerobic microbes increases Specificcomplexes of such microbes com-monly cohabit subgingival sites andare consistently associated withinflammatory periodontal diseases35
These putative microbial pathogensinclude Porphyromonas gingivalisTannerella forsythia and Treponemadenticola35
In the human host the transition fromgingivitis to periodontitis does not occurautomatically either in every patient orevery site but depends on 3 factors 1)degree of host susceptibility 2) presenceand numbers of pathogenic bacteria and3) presence and numbers of protectivebacteria36 Pathogenic bacteria exhibitvirulence features that decrease theeffectiveness of the host response byinducing tissue degradation and retard-ing attempts at healing
Host defense mechanisms are im-paired through a variety of mecha-nisms As one example consider thatAggregatibacter (formally Actinobacil-lus) actinomycetemcomitans produces aleukotoxin that alters the cell mem-branes of neutrophils and monocytesand thereby alters chemotactic andphagocytic responses36 Infection withGram-negative anaerobes is accompa-nied by the release of epitheliotoxinsendotoxins leukotoxins collagenasegellatinase elastase fibrinolysins andother proteolytic enzymes37 These bac-terial toxins and enzymes are tissue irri-tants andor cytotoxic and viewed bythe host immune system as foreign pro-teins (Figure 2) The aggregate cellu-lartissue insult activates the hostimmune system locally and is gener-ally visualized at a clinical level asinflammation with all the inherent gin-gival changes eg vasculitis edema andswelling change in tissue color fromwhite-pink to red or red-purple andspontaneous gingival bleeding or bleed-ing on provocation38
Figure 1 Scanning electron microscopic photograph of root associ-ated dental biofilm (plaque) Bar = 10 micron at an original magnifi-cation of 2840x
6 The Journal of Dental Hygiene Special supplement
Role of the HostImmune Response
Bacteria are necessary but not suffi-cient by themselves to produce adestructive periodontal disease Diseaseinitiation and progression requires asusceptible host38 The microbial chal-lenge induces an immediate inflamma-tory and immune response in the hostThe nature and magnitude of theresponse have an impact on the sever-ity and rate of progression of the peri-odontal disease39 Locally bacteria andtheir metabolic byproducts stimulate acellular immune response within theaffected gingiva represented by a denseinfiltration of neutrophils macro-phages and lymphoid cells These cellsand host connective tissue cells withinthe developing inflammatory lesion arestimulated to synthesize and releaseproinflammatory cytokines prosta-noids and proteolytic enzymes eginterleukin-1 (IL-1) interleukin-6 (IL-6) interleukin-8 (IL-8) tumor necro-sis factor-alpha (TNF-α) prostaglandinE2 (PGE2) matrix metalloproteinases38
It is this host inflammatory-immuneresponse that ultimately leads to theclinical signs of gingivitis and chronicperiodontitis and their characteristicfeatures of fibrous connective tissuedegradation resorption of tooth sup-porting alveolar bone and periodontalpocket formation
In contrast to the epidermis of skinthe epithelial lining of the soft tissuewall of a periodontal pocket lacks a stra-tum corneum and stratum granulosumConsequently the pocket epithelium iseasily ulcerated and breached by inva-sive subgingival pathogenic bacteria40
In addition endotoxins and other micro-bial antigens may gain access to theunderlying connective tissues and gin-gival vasculature leading to bacteremiaand endotoxemia There is considerableevidence that the locally produced pro-inflammatory cytokines and prostanoidsgain access to the circulatory system andmay in turn induce the production ofliver-derived markers of a systemicinflammatory reaction such as C-reac-tive protein fibrinogen serum amyloid-A and haptoglobin41-45 Elevations inboth the locally generated inflammatorymediators and systemic markers ofinflammation have been associated withvarious systemic diseases such as ath-
erosclerosis46 cardiovascular disease47
ischemic stroke48 pre-eclampsia49 andpoor glycemic control 50 in diabeticpatients
Risk FactorsAssociated WithDevelopment ofChronic Periodontitis
In addition to the accepted associa-tions of pathogenic microbes to thepathogenesis of inflammatory peri-odontal diseases several genetic andenvironmental risk factors have beenidentified that affect the host response Itis well established that the prevalenceand severity of chronic periodontitisincreases with advancing age poor oralhygiene marginally or poorly controlledtype I and II diabetes and use oftobacco5152 In addition data from twinstudies indicate that about 50 of thepopulation variance in periodontitis canbe attributed to genetic factors5354 Sev-eral studies indicate that genetic poly-morphisms (variations) in a cluster of atleast 3 genes on chromosome 2q13
which control the production of proin-flammatory cytokines may affect thesystemic inflammatory response in asignificant percentage of people withchronic periodontitis5556
Scaling and RootPlaning in the Controlof Chronic Periodontitis
Periodontitis is a chronic and pro-gressive inflammatory disease forwhich there is no known cure It is nowwell-established that periodontitis isnot associated with a single microor-ganism but rather the initiation andprogression of periodontitis is theresult of the hostrsquos immune responseto a consortium of bacteria For peri-odontopathic bacteria to initiate peri-odontitis it is essential that they areable to colonize subgingival pocketsand produce virulence factors thatdirectly damage host tissue Thus amajor goal of nonsurgical periodontaltherapy is to suppress to the extentpossible the subgingival pathogenicmicrobial flora and thereby signifi-
Figure 2Transmission electron microscopic photograph of a nega-tively stained Phorphyromonas gingivalis featuring fimbriae andnumerous surface blebs that likely contain endotoxin Both fimbriaeand endotoxin are potent antigens that solicit a host immuneresponse Original magnification of 35 000x
cantly reduce or eliminate the associ-ated inflammatory lesion
Dental calculus was the original eti-ologic agent associated with develop-ment of chronic periodontitis In the1960s and 1970s it was established thatthe rough irregular surface of dental cal-culus was always covered with a non-mineralized microbial biofilm (Figure3)57-59 In addition to the surface biofilmat least one recent study has identifiedthe presence of several viable periodon-tal pathogens within the mass of dentalcalculus ie Aggregatibacter actino-mycetemcomitans Treponema denticolaand Porphyromonas gingivalis60 Inter-estingly the persistence of Porphy-romonas gingivalis in the subgingivalenvironment following periodontal ther-apy has been associated with progres-sive alveolar bone loss61 In support ofthis observation Offenbacher et al62
recently reported a significant associa-tion between serum immuneoglobulinG (IgG) titers against Porphyromonasgingivalis in patients that exhibit deepPDs (gt 4 mm) and moderate (gt 10 tolt 50) and severe (gt 50) bleeding onprobing
In spite of the fact that calculus canserve as a reservoir for pathogenicmicrobes the role of subgingival cal-culus as an etiologic agent in chronicperiodontitis was relegated to second-ary status once microbial biofilm wasdeclared the primary extrinsic etiologicfactor Thus the need for completeremoval of subgingival calculusbecame a subject for debate63 How-ever the traditional treatment modal-ity of scaling and root planing (SRP)remains the ldquogold standardrdquo for thenonsurgical management of periodon-titis64
The periodontal literature is repletewith studies showing that treatment ofperiodontitis by SRP results in reduc-tions in probing depth (eg a meanreduction of 129 mm for 4-6 mm pock-ets and a mean of 216 mm for pocketsof gt 7 mm) and subgingival bacterialloads and gains in clinical attachment65-
67 Probing depth (PD) reduction is gen-erally greater at sites with deeper ini-tial probing depths The decrease in PDis the result of 2 phenomena shrinkageof the pocket soft tissue wall manifestedas recession of the gingival marginwhich results from a decrease in softtissue inflammation and the inherentedema and gain in clinical attachment
The latter usually accounts for roughlyone-half of the probing depth reduc-tion65-67 In general clinicians shouldevaluate post-SRP healing at 4 to 6weeks following treatment After 6weeks most of the healing has takenplace but repair and collagen matura-tion may continue for an additional 9months6768
Three relevant observations must beconsidered when deciding to use non-surgical therapy as the primary modal-ity for treatment of early to moderatechronic periodontitis First regardingSRP clinicians must be careful wheninterpreting data from published clini-cal trials as they may not accuratelyreflect the private practice setting interms of time skill level severity ofdisease and diversity of patient popu-lation65 For example university-con-ducted clinical trials often use highlyskilled clinicians select patients forlevel of disease and report spending 10minutes per tooth when performingSRP6667 Ten minutes per tooth equatesto about 70 minutes per quadrant It isthe experience of this author that in pri-vate practice a quadrant of SRP may becompleted in approximately 60 minutesregardless of the level of disease and
this allows approximately 10 minutesfor setting of the patient and adminis-tration of anesthetic Greenstein67 hasrightfully noted that decreased timedevoted to SRP in more recent studiesprobably accounts for the diminishedresults reported when to the more clas-sic clinical trials Second one mustremember that microbes embedded ina mature undisturbed subgingivalbiofilm may exhibit an increased toler-ance to antimicrobial agents28-32 Thirdeven when chronic periodontitis istreated successfully the reduction insubgingival pathogenic microbes istransitory SRP of diseased root sur-faces can open dentinal tubules allow-ing invasion by periodontal pathogensinto the exposed tubules and possiblythen serve as a reservoir for re-infec-tion of the pocket6970 Thus the need forfollow-up treatment usually consistingof supra- and subgingival debridementat 3 to 4 month intervals is necessary tomaintain the initially gained beneficialeffects7172 Collectively considered thedistinct probability of less than idealresults from SRP and pocket re-infec-tion by residual microbes is a forcefulargument for the use of adjunctivetreatment modalities in addition to SRP
Special supplement The Journal of Dental Hygiene 7
Figure 3 Scanning electron microscopic photograph of dental cal-culus characterized by a superficial layer of microbial biofilm Bar =10 micron at an original magnification of 1770x
8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 5
genetic diversity and complex commu-nity interactions Dental plaque is amicrobial biofilm (Figure 1) As withany biofilm the constituent microbesare tightly adherent to each other andto an oral substrate by means of anextracellular matrix ie slime layer orglycocalix into which they are embed-ded1617 The microbial populations inbiofilm have 2 strategies that enablethem to successfully survive withintheir community The first is a high rateof reproduction for continued survivaland the second is physiologic adapta-tion to the available environmentalresources or life-supporting capacity ofthe environment18
Biofilms inherently dictate profoundchanges in the behavior of individualmicrobes their relationship to the hostand their response to environmentalconditions19 Indeed oral biofilms asdistinct entities are the causative agentsof biological processes such as dentalcaries periodontal disease and peri-implantitis rather than any singlemicrobe evading the host defense andcausing disease20 Biofilms exhibit char-acteristics that impact the clinical man-agement of inflammatory periodontaldisease For example both altered pat-terns of microbial gene expression andthe composition and density of the
extracellular matrix reduce the suscep-tibility of microbes to antimicrobialagents21-23 Bacteria growing in dentalbiofilms display an increased toleranceto antimicrobial agents including thoseused in dentifrices and mouthrinses24-27
In addition confocal microscopy of insitu established natural biofilms showedthat chlorhexidine only affected theouter layers of cells in 24 and 48 hourplaque biofilms suggesting eitherquenching of the agent at the biofilmsurface or a lack of penetration28 Fur-ther biofilms of oral bacteria are alsomore tolerant of antibiotics (eg amoxy-cillin doxycycline minocycline andmetronidazole) than planktonic cells29-31
In this regard biofilms of Porphy-romonas gingivalis have been shown totolerate 160 times the minimuminhibitory concentration (MIC) ofmetronidazole that was determined forplanktonic cells32
Over 700 species of aerobic andanaerobic bacteria have been identifiedin the human oral cavity3334 Themicrobes grow as complex mixedinterdependent colonies in biofilms andmay achieve considerable thicknessachieving a thickness of 1 mm within96 hours if left undisturbed1617 Oralbiofilms like all microbial biofilmsexhibit a successional colonization with
gram-positive aerobic Streptococcispecies (spp) being the initial coloniz-ers followed in sequence by Actino-myces spp Corynebacterium spp Veil-lonella spp and then in more maturebiofilm a variety of gram-negativeanaerobic microbes such as Treponemaspp Fusobacterium spp Porphy-romonas spp Prevotella spp and Tan-nerella spp173536
As the biofilm is allowed to maturewith concomitant increases in thick-ness the percentage of Gram-negativeanaerobic microbes increases Specificcomplexes of such microbes com-monly cohabit subgingival sites andare consistently associated withinflammatory periodontal diseases35
These putative microbial pathogensinclude Porphyromonas gingivalisTannerella forsythia and Treponemadenticola35
In the human host the transition fromgingivitis to periodontitis does not occurautomatically either in every patient orevery site but depends on 3 factors 1)degree of host susceptibility 2) presenceand numbers of pathogenic bacteria and3) presence and numbers of protectivebacteria36 Pathogenic bacteria exhibitvirulence features that decrease theeffectiveness of the host response byinducing tissue degradation and retard-ing attempts at healing
Host defense mechanisms are im-paired through a variety of mecha-nisms As one example consider thatAggregatibacter (formally Actinobacil-lus) actinomycetemcomitans produces aleukotoxin that alters the cell mem-branes of neutrophils and monocytesand thereby alters chemotactic andphagocytic responses36 Infection withGram-negative anaerobes is accompa-nied by the release of epitheliotoxinsendotoxins leukotoxins collagenasegellatinase elastase fibrinolysins andother proteolytic enzymes37 These bac-terial toxins and enzymes are tissue irri-tants andor cytotoxic and viewed bythe host immune system as foreign pro-teins (Figure 2) The aggregate cellu-lartissue insult activates the hostimmune system locally and is gener-ally visualized at a clinical level asinflammation with all the inherent gin-gival changes eg vasculitis edema andswelling change in tissue color fromwhite-pink to red or red-purple andspontaneous gingival bleeding or bleed-ing on provocation38
Figure 1 Scanning electron microscopic photograph of root associ-ated dental biofilm (plaque) Bar = 10 micron at an original magnifi-cation of 2840x
6 The Journal of Dental Hygiene Special supplement
Role of the HostImmune Response
Bacteria are necessary but not suffi-cient by themselves to produce adestructive periodontal disease Diseaseinitiation and progression requires asusceptible host38 The microbial chal-lenge induces an immediate inflamma-tory and immune response in the hostThe nature and magnitude of theresponse have an impact on the sever-ity and rate of progression of the peri-odontal disease39 Locally bacteria andtheir metabolic byproducts stimulate acellular immune response within theaffected gingiva represented by a denseinfiltration of neutrophils macro-phages and lymphoid cells These cellsand host connective tissue cells withinthe developing inflammatory lesion arestimulated to synthesize and releaseproinflammatory cytokines prosta-noids and proteolytic enzymes eginterleukin-1 (IL-1) interleukin-6 (IL-6) interleukin-8 (IL-8) tumor necro-sis factor-alpha (TNF-α) prostaglandinE2 (PGE2) matrix metalloproteinases38
It is this host inflammatory-immuneresponse that ultimately leads to theclinical signs of gingivitis and chronicperiodontitis and their characteristicfeatures of fibrous connective tissuedegradation resorption of tooth sup-porting alveolar bone and periodontalpocket formation
In contrast to the epidermis of skinthe epithelial lining of the soft tissuewall of a periodontal pocket lacks a stra-tum corneum and stratum granulosumConsequently the pocket epithelium iseasily ulcerated and breached by inva-sive subgingival pathogenic bacteria40
In addition endotoxins and other micro-bial antigens may gain access to theunderlying connective tissues and gin-gival vasculature leading to bacteremiaand endotoxemia There is considerableevidence that the locally produced pro-inflammatory cytokines and prostanoidsgain access to the circulatory system andmay in turn induce the production ofliver-derived markers of a systemicinflammatory reaction such as C-reac-tive protein fibrinogen serum amyloid-A and haptoglobin41-45 Elevations inboth the locally generated inflammatorymediators and systemic markers ofinflammation have been associated withvarious systemic diseases such as ath-
erosclerosis46 cardiovascular disease47
ischemic stroke48 pre-eclampsia49 andpoor glycemic control 50 in diabeticpatients
Risk FactorsAssociated WithDevelopment ofChronic Periodontitis
In addition to the accepted associa-tions of pathogenic microbes to thepathogenesis of inflammatory peri-odontal diseases several genetic andenvironmental risk factors have beenidentified that affect the host response Itis well established that the prevalenceand severity of chronic periodontitisincreases with advancing age poor oralhygiene marginally or poorly controlledtype I and II diabetes and use oftobacco5152 In addition data from twinstudies indicate that about 50 of thepopulation variance in periodontitis canbe attributed to genetic factors5354 Sev-eral studies indicate that genetic poly-morphisms (variations) in a cluster of atleast 3 genes on chromosome 2q13
which control the production of proin-flammatory cytokines may affect thesystemic inflammatory response in asignificant percentage of people withchronic periodontitis5556
Scaling and RootPlaning in the Controlof Chronic Periodontitis
Periodontitis is a chronic and pro-gressive inflammatory disease forwhich there is no known cure It is nowwell-established that periodontitis isnot associated with a single microor-ganism but rather the initiation andprogression of periodontitis is theresult of the hostrsquos immune responseto a consortium of bacteria For peri-odontopathic bacteria to initiate peri-odontitis it is essential that they areable to colonize subgingival pocketsand produce virulence factors thatdirectly damage host tissue Thus amajor goal of nonsurgical periodontaltherapy is to suppress to the extentpossible the subgingival pathogenicmicrobial flora and thereby signifi-
Figure 2Transmission electron microscopic photograph of a nega-tively stained Phorphyromonas gingivalis featuring fimbriae andnumerous surface blebs that likely contain endotoxin Both fimbriaeand endotoxin are potent antigens that solicit a host immuneresponse Original magnification of 35 000x
cantly reduce or eliminate the associ-ated inflammatory lesion
Dental calculus was the original eti-ologic agent associated with develop-ment of chronic periodontitis In the1960s and 1970s it was established thatthe rough irregular surface of dental cal-culus was always covered with a non-mineralized microbial biofilm (Figure3)57-59 In addition to the surface biofilmat least one recent study has identifiedthe presence of several viable periodon-tal pathogens within the mass of dentalcalculus ie Aggregatibacter actino-mycetemcomitans Treponema denticolaand Porphyromonas gingivalis60 Inter-estingly the persistence of Porphy-romonas gingivalis in the subgingivalenvironment following periodontal ther-apy has been associated with progres-sive alveolar bone loss61 In support ofthis observation Offenbacher et al62
recently reported a significant associa-tion between serum immuneoglobulinG (IgG) titers against Porphyromonasgingivalis in patients that exhibit deepPDs (gt 4 mm) and moderate (gt 10 tolt 50) and severe (gt 50) bleeding onprobing
In spite of the fact that calculus canserve as a reservoir for pathogenicmicrobes the role of subgingival cal-culus as an etiologic agent in chronicperiodontitis was relegated to second-ary status once microbial biofilm wasdeclared the primary extrinsic etiologicfactor Thus the need for completeremoval of subgingival calculusbecame a subject for debate63 How-ever the traditional treatment modal-ity of scaling and root planing (SRP)remains the ldquogold standardrdquo for thenonsurgical management of periodon-titis64
The periodontal literature is repletewith studies showing that treatment ofperiodontitis by SRP results in reduc-tions in probing depth (eg a meanreduction of 129 mm for 4-6 mm pock-ets and a mean of 216 mm for pocketsof gt 7 mm) and subgingival bacterialloads and gains in clinical attachment65-
67 Probing depth (PD) reduction is gen-erally greater at sites with deeper ini-tial probing depths The decrease in PDis the result of 2 phenomena shrinkageof the pocket soft tissue wall manifestedas recession of the gingival marginwhich results from a decrease in softtissue inflammation and the inherentedema and gain in clinical attachment
The latter usually accounts for roughlyone-half of the probing depth reduc-tion65-67 In general clinicians shouldevaluate post-SRP healing at 4 to 6weeks following treatment After 6weeks most of the healing has takenplace but repair and collagen matura-tion may continue for an additional 9months6768
Three relevant observations must beconsidered when deciding to use non-surgical therapy as the primary modal-ity for treatment of early to moderatechronic periodontitis First regardingSRP clinicians must be careful wheninterpreting data from published clini-cal trials as they may not accuratelyreflect the private practice setting interms of time skill level severity ofdisease and diversity of patient popu-lation65 For example university-con-ducted clinical trials often use highlyskilled clinicians select patients forlevel of disease and report spending 10minutes per tooth when performingSRP6667 Ten minutes per tooth equatesto about 70 minutes per quadrant It isthe experience of this author that in pri-vate practice a quadrant of SRP may becompleted in approximately 60 minutesregardless of the level of disease and
this allows approximately 10 minutesfor setting of the patient and adminis-tration of anesthetic Greenstein67 hasrightfully noted that decreased timedevoted to SRP in more recent studiesprobably accounts for the diminishedresults reported when to the more clas-sic clinical trials Second one mustremember that microbes embedded ina mature undisturbed subgingivalbiofilm may exhibit an increased toler-ance to antimicrobial agents28-32 Thirdeven when chronic periodontitis istreated successfully the reduction insubgingival pathogenic microbes istransitory SRP of diseased root sur-faces can open dentinal tubules allow-ing invasion by periodontal pathogensinto the exposed tubules and possiblythen serve as a reservoir for re-infec-tion of the pocket6970 Thus the need forfollow-up treatment usually consistingof supra- and subgingival debridementat 3 to 4 month intervals is necessary tomaintain the initially gained beneficialeffects7172 Collectively considered thedistinct probability of less than idealresults from SRP and pocket re-infec-tion by residual microbes is a forcefulargument for the use of adjunctivetreatment modalities in addition to SRP
Special supplement The Journal of Dental Hygiene 7
Figure 3 Scanning electron microscopic photograph of dental cal-culus characterized by a superficial layer of microbial biofilm Bar =10 micron at an original magnification of 1770x
8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

6 The Journal of Dental Hygiene Special supplement
Role of the HostImmune Response
Bacteria are necessary but not suffi-cient by themselves to produce adestructive periodontal disease Diseaseinitiation and progression requires asusceptible host38 The microbial chal-lenge induces an immediate inflamma-tory and immune response in the hostThe nature and magnitude of theresponse have an impact on the sever-ity and rate of progression of the peri-odontal disease39 Locally bacteria andtheir metabolic byproducts stimulate acellular immune response within theaffected gingiva represented by a denseinfiltration of neutrophils macro-phages and lymphoid cells These cellsand host connective tissue cells withinthe developing inflammatory lesion arestimulated to synthesize and releaseproinflammatory cytokines prosta-noids and proteolytic enzymes eginterleukin-1 (IL-1) interleukin-6 (IL-6) interleukin-8 (IL-8) tumor necro-sis factor-alpha (TNF-α) prostaglandinE2 (PGE2) matrix metalloproteinases38
It is this host inflammatory-immuneresponse that ultimately leads to theclinical signs of gingivitis and chronicperiodontitis and their characteristicfeatures of fibrous connective tissuedegradation resorption of tooth sup-porting alveolar bone and periodontalpocket formation
In contrast to the epidermis of skinthe epithelial lining of the soft tissuewall of a periodontal pocket lacks a stra-tum corneum and stratum granulosumConsequently the pocket epithelium iseasily ulcerated and breached by inva-sive subgingival pathogenic bacteria40
In addition endotoxins and other micro-bial antigens may gain access to theunderlying connective tissues and gin-gival vasculature leading to bacteremiaand endotoxemia There is considerableevidence that the locally produced pro-inflammatory cytokines and prostanoidsgain access to the circulatory system andmay in turn induce the production ofliver-derived markers of a systemicinflammatory reaction such as C-reac-tive protein fibrinogen serum amyloid-A and haptoglobin41-45 Elevations inboth the locally generated inflammatorymediators and systemic markers ofinflammation have been associated withvarious systemic diseases such as ath-
erosclerosis46 cardiovascular disease47
ischemic stroke48 pre-eclampsia49 andpoor glycemic control 50 in diabeticpatients
Risk FactorsAssociated WithDevelopment ofChronic Periodontitis
In addition to the accepted associa-tions of pathogenic microbes to thepathogenesis of inflammatory peri-odontal diseases several genetic andenvironmental risk factors have beenidentified that affect the host response Itis well established that the prevalenceand severity of chronic periodontitisincreases with advancing age poor oralhygiene marginally or poorly controlledtype I and II diabetes and use oftobacco5152 In addition data from twinstudies indicate that about 50 of thepopulation variance in periodontitis canbe attributed to genetic factors5354 Sev-eral studies indicate that genetic poly-morphisms (variations) in a cluster of atleast 3 genes on chromosome 2q13
which control the production of proin-flammatory cytokines may affect thesystemic inflammatory response in asignificant percentage of people withchronic periodontitis5556
Scaling and RootPlaning in the Controlof Chronic Periodontitis
Periodontitis is a chronic and pro-gressive inflammatory disease forwhich there is no known cure It is nowwell-established that periodontitis isnot associated with a single microor-ganism but rather the initiation andprogression of periodontitis is theresult of the hostrsquos immune responseto a consortium of bacteria For peri-odontopathic bacteria to initiate peri-odontitis it is essential that they areable to colonize subgingival pocketsand produce virulence factors thatdirectly damage host tissue Thus amajor goal of nonsurgical periodontaltherapy is to suppress to the extentpossible the subgingival pathogenicmicrobial flora and thereby signifi-
Figure 2Transmission electron microscopic photograph of a nega-tively stained Phorphyromonas gingivalis featuring fimbriae andnumerous surface blebs that likely contain endotoxin Both fimbriaeand endotoxin are potent antigens that solicit a host immuneresponse Original magnification of 35 000x
cantly reduce or eliminate the associ-ated inflammatory lesion
Dental calculus was the original eti-ologic agent associated with develop-ment of chronic periodontitis In the1960s and 1970s it was established thatthe rough irregular surface of dental cal-culus was always covered with a non-mineralized microbial biofilm (Figure3)57-59 In addition to the surface biofilmat least one recent study has identifiedthe presence of several viable periodon-tal pathogens within the mass of dentalcalculus ie Aggregatibacter actino-mycetemcomitans Treponema denticolaand Porphyromonas gingivalis60 Inter-estingly the persistence of Porphy-romonas gingivalis in the subgingivalenvironment following periodontal ther-apy has been associated with progres-sive alveolar bone loss61 In support ofthis observation Offenbacher et al62
recently reported a significant associa-tion between serum immuneoglobulinG (IgG) titers against Porphyromonasgingivalis in patients that exhibit deepPDs (gt 4 mm) and moderate (gt 10 tolt 50) and severe (gt 50) bleeding onprobing
In spite of the fact that calculus canserve as a reservoir for pathogenicmicrobes the role of subgingival cal-culus as an etiologic agent in chronicperiodontitis was relegated to second-ary status once microbial biofilm wasdeclared the primary extrinsic etiologicfactor Thus the need for completeremoval of subgingival calculusbecame a subject for debate63 How-ever the traditional treatment modal-ity of scaling and root planing (SRP)remains the ldquogold standardrdquo for thenonsurgical management of periodon-titis64
The periodontal literature is repletewith studies showing that treatment ofperiodontitis by SRP results in reduc-tions in probing depth (eg a meanreduction of 129 mm for 4-6 mm pock-ets and a mean of 216 mm for pocketsof gt 7 mm) and subgingival bacterialloads and gains in clinical attachment65-
67 Probing depth (PD) reduction is gen-erally greater at sites with deeper ini-tial probing depths The decrease in PDis the result of 2 phenomena shrinkageof the pocket soft tissue wall manifestedas recession of the gingival marginwhich results from a decrease in softtissue inflammation and the inherentedema and gain in clinical attachment
The latter usually accounts for roughlyone-half of the probing depth reduc-tion65-67 In general clinicians shouldevaluate post-SRP healing at 4 to 6weeks following treatment After 6weeks most of the healing has takenplace but repair and collagen matura-tion may continue for an additional 9months6768
Three relevant observations must beconsidered when deciding to use non-surgical therapy as the primary modal-ity for treatment of early to moderatechronic periodontitis First regardingSRP clinicians must be careful wheninterpreting data from published clini-cal trials as they may not accuratelyreflect the private practice setting interms of time skill level severity ofdisease and diversity of patient popu-lation65 For example university-con-ducted clinical trials often use highlyskilled clinicians select patients forlevel of disease and report spending 10minutes per tooth when performingSRP6667 Ten minutes per tooth equatesto about 70 minutes per quadrant It isthe experience of this author that in pri-vate practice a quadrant of SRP may becompleted in approximately 60 minutesregardless of the level of disease and
this allows approximately 10 minutesfor setting of the patient and adminis-tration of anesthetic Greenstein67 hasrightfully noted that decreased timedevoted to SRP in more recent studiesprobably accounts for the diminishedresults reported when to the more clas-sic clinical trials Second one mustremember that microbes embedded ina mature undisturbed subgingivalbiofilm may exhibit an increased toler-ance to antimicrobial agents28-32 Thirdeven when chronic periodontitis istreated successfully the reduction insubgingival pathogenic microbes istransitory SRP of diseased root sur-faces can open dentinal tubules allow-ing invasion by periodontal pathogensinto the exposed tubules and possiblythen serve as a reservoir for re-infec-tion of the pocket6970 Thus the need forfollow-up treatment usually consistingof supra- and subgingival debridementat 3 to 4 month intervals is necessary tomaintain the initially gained beneficialeffects7172 Collectively considered thedistinct probability of less than idealresults from SRP and pocket re-infec-tion by residual microbes is a forcefulargument for the use of adjunctivetreatment modalities in addition to SRP
Special supplement The Journal of Dental Hygiene 7
Figure 3 Scanning electron microscopic photograph of dental cal-culus characterized by a superficial layer of microbial biofilm Bar =10 micron at an original magnification of 1770x
8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

cantly reduce or eliminate the associ-ated inflammatory lesion
Dental calculus was the original eti-ologic agent associated with develop-ment of chronic periodontitis In the1960s and 1970s it was established thatthe rough irregular surface of dental cal-culus was always covered with a non-mineralized microbial biofilm (Figure3)57-59 In addition to the surface biofilmat least one recent study has identifiedthe presence of several viable periodon-tal pathogens within the mass of dentalcalculus ie Aggregatibacter actino-mycetemcomitans Treponema denticolaand Porphyromonas gingivalis60 Inter-estingly the persistence of Porphy-romonas gingivalis in the subgingivalenvironment following periodontal ther-apy has been associated with progres-sive alveolar bone loss61 In support ofthis observation Offenbacher et al62
recently reported a significant associa-tion between serum immuneoglobulinG (IgG) titers against Porphyromonasgingivalis in patients that exhibit deepPDs (gt 4 mm) and moderate (gt 10 tolt 50) and severe (gt 50) bleeding onprobing
In spite of the fact that calculus canserve as a reservoir for pathogenicmicrobes the role of subgingival cal-culus as an etiologic agent in chronicperiodontitis was relegated to second-ary status once microbial biofilm wasdeclared the primary extrinsic etiologicfactor Thus the need for completeremoval of subgingival calculusbecame a subject for debate63 How-ever the traditional treatment modal-ity of scaling and root planing (SRP)remains the ldquogold standardrdquo for thenonsurgical management of periodon-titis64
The periodontal literature is repletewith studies showing that treatment ofperiodontitis by SRP results in reduc-tions in probing depth (eg a meanreduction of 129 mm for 4-6 mm pock-ets and a mean of 216 mm for pocketsof gt 7 mm) and subgingival bacterialloads and gains in clinical attachment65-
67 Probing depth (PD) reduction is gen-erally greater at sites with deeper ini-tial probing depths The decrease in PDis the result of 2 phenomena shrinkageof the pocket soft tissue wall manifestedas recession of the gingival marginwhich results from a decrease in softtissue inflammation and the inherentedema and gain in clinical attachment
The latter usually accounts for roughlyone-half of the probing depth reduc-tion65-67 In general clinicians shouldevaluate post-SRP healing at 4 to 6weeks following treatment After 6weeks most of the healing has takenplace but repair and collagen matura-tion may continue for an additional 9months6768
Three relevant observations must beconsidered when deciding to use non-surgical therapy as the primary modal-ity for treatment of early to moderatechronic periodontitis First regardingSRP clinicians must be careful wheninterpreting data from published clini-cal trials as they may not accuratelyreflect the private practice setting interms of time skill level severity ofdisease and diversity of patient popu-lation65 For example university-con-ducted clinical trials often use highlyskilled clinicians select patients forlevel of disease and report spending 10minutes per tooth when performingSRP6667 Ten minutes per tooth equatesto about 70 minutes per quadrant It isthe experience of this author that in pri-vate practice a quadrant of SRP may becompleted in approximately 60 minutesregardless of the level of disease and
this allows approximately 10 minutesfor setting of the patient and adminis-tration of anesthetic Greenstein67 hasrightfully noted that decreased timedevoted to SRP in more recent studiesprobably accounts for the diminishedresults reported when to the more clas-sic clinical trials Second one mustremember that microbes embedded ina mature undisturbed subgingivalbiofilm may exhibit an increased toler-ance to antimicrobial agents28-32 Thirdeven when chronic periodontitis istreated successfully the reduction insubgingival pathogenic microbes istransitory SRP of diseased root sur-faces can open dentinal tubules allow-ing invasion by periodontal pathogensinto the exposed tubules and possiblythen serve as a reservoir for re-infec-tion of the pocket6970 Thus the need forfollow-up treatment usually consistingof supra- and subgingival debridementat 3 to 4 month intervals is necessary tomaintain the initially gained beneficialeffects7172 Collectively considered thedistinct probability of less than idealresults from SRP and pocket re-infec-tion by residual microbes is a forcefulargument for the use of adjunctivetreatment modalities in addition to SRP
Special supplement The Journal of Dental Hygiene 7
Figure 3 Scanning electron microscopic photograph of dental cal-culus characterized by a superficial layer of microbial biofilm Bar =10 micron at an original magnification of 1770x
8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

8 The Journal of Dental Hygiene Special supplement
Clinical Implications
1 The prevalence rate for chronicperiodontitis (slight moderateand advanced severity) is approx-imately 30 of the US adult pop-ulation or roughly 65 million indi-viduals
2 Bacteria growing in undisturbeddental biofilms exhibit a signifi-cant increased tolerance to antimi-crobial agents and antibiotics
3 The transition from gingivitis toperiodontitis does not occur auto-
matically either in every patientor every site but depends on 3factors 1) degree of host suscep-tibility 2) presence and numbersof pathogenic bacteria and 3)presence and numbers of protec-tive bacteria
4 Even when chronic periodontitisis treated successfully the reduc-tion in subgingival pathogenicmicrobes is transitory Thus theneed for follow-up treatment usu-ally consisting of supra- and sub-gingival debridement at 3 to 4month intervals is necessary to
maintain the initially gained ben-eficial effects
5 Due to limitations of SRP and re-infection of the periodontalpocket adjunctive treatmentmodalities may increase the like-lihood of improvement in the peri-odontal condition
Disclosure
Dr Cobb has served as a scientificadvisor and consultant for OraPharmaInc
References
1 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
2 Albandar JM Kingman A Gingival recession gingivalbleeding and dental calculus in adults 30 years of ageand older in the United States 1988-1994 J Periodontol1999 7030-43
3 Albandar JM Rams TE Global epidemiology of perio-dontal diseases an overview Periodontol 2000 2002297-10
4 Loumle H Brown LJ Early-onset periodontitis in the UnitedStates of America J Periodontol 199162608-616
5 Jenkins WM Papapanou PN Epidemiology of periodon-tal disease in children and adolescents Periodontol 200020012616-32
6 Douglass CW Fox CH Cross-sectional studies in peri-odontal disease current status and implications for dentalpractice Adv Dent Res 1993725-31
7 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
8 Brown LJ Oliver RC Loumle H Evaluating periodontal statusof US employed adults J Am Dent Assoc 1990121 226-232
9 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
10 Page RC Eke PI Case definition for use in population-based surveillance of periodontitis J Periodontol 2007 781387-1399
11 Borrell LN Crawford ND Social disparities in periodonti-tis among United States adults 1999-2004 CommunityDent Oral Epidemiol 200836In Press Published articleonline 18-Oct-2007 wwwBlackwell-Synergycom
12 Cobb CM Williams KB Gerkovitch M Is The Prevalenceof Periodontitis in the United States in Decline Periodon-tol 2000 2008 In Press
13 Kingman A Morrison E Loumle H Systematic errors in esti-mating prevalence and severity of periodontal disease JPeriodontol 198859707-713
14 Hunt R Fann S Effect of examining half teeth in a partialperiodontal recording of older adults J Dent Res1991701380-1385
15 Eaton KA Duffy S Griffiths GS Gilthorpe MS JohnsonNW The influence of partial and full-mouth recordings on
estimates of prevalence and extent of lifetime cumulativeattachment loss A study in a population of young malemilitary recruits J Periodontol 200172140-145
16 Listgarten MA Structure of the microbial flora associatedwith periodontal health and diseases in man J Periodon-tol 1976471-18
17 Cobb CM Killoy WJ Microbial colonization in human peri-odontal disease an illustrated tutorial on selected ultra-structural and ecologic considerations Scan Microsc19904675-691
18 Nishihara T Koseki T Microbial etiology of periodontitisPeriodontol 2000 20043614-26
19 Marsh PD Dental plaque as a microbial biofilm CariesRes 200438204-221
20 Caldwell DE Atuku E Wilkie DC et al Germ theory vscommunity theory in understanding and controlling theproliferation of biofilms Adv Dent Res 1997114-13
21 Marsh PD Dental plaque Biological significance of abiofilm and community life-style J Clin Periodontol200532(Suppl 6)7-15
22 Gilbert P Maira-Litran T McBain AJ Rickard AH WhyteFW The physiology and collective recalcitrance of micro-bial biofilm communities Adv Microbial Physiol 200246203ndash255
23 Stewart PS Costerton JW Antibiotic resistance of bacte-ria in biofilms Lancet 2001358135-138
24 Marsh PD Bradshaw DJ Microbiological effects of newagents in dentifrices for plaque control Inter Dent J199343399-406
25 Kinniment SL Wimpenny JWT Adams D Marsh PD Theeffect of chlorhexidine on defined mixed culture oralbiofilms grown in a novel model system J Appl Bacteriol199681120-125
26 Wilson M Susceptibility of oral bacterial biofilms to antimi-crobial agents J Med Microbiol 19964479-87
27 Pratten J Wilson M Antimicrobial susceptibility and com-position of microcosm dental plaques supplemented withsucrose Antimicrob Agents Chemother 1999431595-1599
28 Zaura-Arite E van Marle J ten Cate JM Confocalmicroscopy study of undisturbed and chlorhexidine-treateddental biofilm J Dent Res 2001801436-1440
29 Larsen T Susceptibility of Porphyromonas gingivalis inbiofilms to amoxicillin doxycycline and metronidazole OralMicrobiol Immunol 200217267-271
30 Socransky SS Haffajee AD Dental biofilms difficult ther-apeutic targets Periodontol 2000 20022812ndash55
31 Noiri Y Okami Y Narimatsu M Takahashi Y Kawahara TEbisu S Effects of chlorhexidine minocycline and metron-
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines
idazole on Porphyromonas gingivalis strain 381 in biofilmsJ Periodontol 2003741647-1651
32 Wright TL Ellen RP Lacroix JM Sinnadurai S MittelmanMW Effects of metronidazole on Porphyromonas gingi-valis biofilms J Periodont Res 199732473-477
33 Aas JA Paster BJ Stokes LN Olsen I Dewhirst FE Defin-ing the normal bacterial flora of the oral cavity J Clin Micro-biol 2005435721-5732
34 Paster BJ Olsen I Aas JA Dewhirst FE The breadth ofbacterial diversity in the human periodontal pocket andother oral sites Periodontol 2000 20064280-87
35 Socransky SS Haffajee AD Cugini MA Smith C KentRL Jr Microbial complexes in subgingival plaque J ClinPeriodontol 199825134-144
36 Sbordone L Bortolaia C Oral microbial biofilms andplaque-related diseases Microbial communities and theirrole in the shift from oral health to disease Clin Oral Invest20037181-188
37 Zambon JJ Periodontal diseases Microbial factors AnnPeriodontol 19961879-925
38 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
39 Page RC Kornman KS The pathogenesis of human peri-odontitis an introduction Periodontol 2000 1997149-11
40 Hujoel PP White BA Garcia RI Listgarten MA The den-togingival epithelial surface area revisited J PeriodontRes 20013648-55
41 Ebersole JL Machen RL Steffen MJ Willmann DE Sys-temic acute-phase reactants C-reactive protein and hap-toglobin in adult periodontitis Clin Exper Immunol1997107347-352
42 Noack B Genco RJ Trevisan M Grossi S Zambon JJ DeNardin E Periodontal infections contribute to elevated sys-temic C-reactive protein level J Periodontol 2001721221-1227
43 Amar S Gokce N Morgan S Loukideli M Van Dyke TEVita JA Periodontal disease is associated with brachialartery endothelial dysfunction and systemic inflammationArterioscler Thromb Vasc Biol 2003231245-1249
44 Slade GD Ghezzi EM Heiss G Beck JD Riche E Offen-bacher S Relationship between periodontal disease andC-reactive protein among adults in the AtherosclerosisRisk in Communities study Arch Intern Med20031631172-1179
45 Leivadaros E van der Velden U Bizzaro S et al A pilotstudy into measurements of markers of atherosclerosis inperiodontitis J Periodontol 200576121-128
46 Tonetti MS DrsquoAiuto F Nibali L et al Treatment of peri-odontitis and endothelial function N Eng J Med2007356911-920
47 Kinane DF Lowe GD How periodontal disease may con-tribute to cardiovascular disease Periodontol 2000200023121-126
48 Grau AJ Becher H Ziegler CM et al Periodontal diseaseas a risk factor for ischemic stroke Stroke 200435496-501
49 Siqueira FM Cota LOM Costa JE Haddad JPA LanaAMQ Costa FO Maternal periodontitis as a potential riskvariable for preeclampsia A case-control study J Peri-odontol 200879207-215
50 Hein C Cobb CM Iacopino A Report of an independentpanel of experts of the Scottsdale Project The independ-ent study initiative for collaboration in diabetes cardio-vascular disease and periodontal disease interventionGrand Rounds in Oral-Sys Med 20072(Suppl)2-27
51 Abdellatif HM Burt BA An epidemiological investigationinto the relative importance of age and oral hygiene status
as determinants of periodontitis J Dent Res 198766 13-18
52 American Academy of Periodontology Position paper Epi-demiology of periodontal disease J Periodontol199667935-945
53 Michalowicz BS Aeppli D Virag JG et al Periodontal find-ings in adult twins J Periodontol 199162293-299
54 Michalowicz BS Diehl SR Gunsolley JC et al Evidenceof a substantial genetic basis for risk of adult periodontitisJ Periodontol 2000711699-1707
55 Kornman KS Crane A Wang HY et al The interleukin-1genotype as a severity factor in adult periodontal diseaseJ Clin Periodontol 19972472-77
56 DrsquoAiuto F Parkar M Brett PM Ready D Tonetti MS Genepolymorphisms in proinflammatory cytokines are associ-ated with systemic inflammation in patients with severeperiodontal infections Cytokine 20042829-34
57 Baumhammers A Conway JC Saltzberg D Matta RKScanning electron microscopy of supragingival calculus JPeriodontol 19734492-94
58 Muhleman HR Schroeder HE Dynamics of supragingivalcalculus formation Adv Oral Biol 19641175-203
59 Mandel ID Dental plaque Nature formation and effectsJ Periodontol 196637357-367
60 Calabrese N Galgut P Mordan N Identification of Acti-nobacillus actinomycetemcomitans Treponema denticolaand Porphyromonas gingivalis within human dental cal-culus A pilot investigation J Inter Acad Periodontol20079118-128
61 Chaves ES Jeffcoat MK Ryerson CC Snyder B Persis-tent bacterial colonization of Porphyromonas gingivalisPrevotella intermedia and Actinobacillus actinomycetem-comitans in periodontitis and its association with alveolarbone loss after 6 months of therapy J Clin Periodontol200027897-903
62 Offenbacher S Barros SP Singer RE Moss K WilliamsRC Beck JD Periodontal disease at the biofilm-gingivalinterface J Periodontol 200778(10)1911-1925
63 Robertson PB The residual calculus paradox J Peri-odontol 19906165-66
64 Ryan ME Nonsurgical approaches for treatment of peri-odontal diseases Dent Clin N Am 200549611-636
65 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961443-490
66 Greenstein G Periodontal response to mechanical non-surgical therapy a review J Periodontol 199263118-130
67 Greenstein G Nonsurgical periodontal therapy in 2000 aliterature review J Am Dent Assoc 20001311580-1592
68 Badersten A Nilveus R Egelberg J Effect of nonsurgicalperiodontal therapy I moderately advanced periodontitisJ Clin Periodontol 1981857-72
69 Adriaens PA DeBoever JA Loesche WJ Bacterial inva-sion in root cementum and radicular dentin of periodontallydiseased teeth in humans J Periodontol 198859222-230
70 Giuliana G Ammatuna P Pizzo G Capone F DrsquoAngelo MOccurrence of invading bacteria in radicular dentin of peri-odontally diseased teeth microbiological findings J ClinPeriodontol 199724478-485
71 Listgarten MA A rationale for monitoring the periodontalmicrobiota after periodontal treatment J Periodontol198859439-444
72 Listgarten MA Levin S Schifter CC Sullivan P Evian CIRosenberg ES Laster L Comparative longitudinal study of2 methods of scheduling maintenance visits 2 year dataJ Clin Periodontol 198613692-700
Special supplement The Journal of Dental Hygiene 9
10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

10 The Journal of Dental Hygiene Special supplement
Introduction
Periodontal disease is a commonmixed oral infection affecting the sup-porting structures around the teethWhile 75 of the adult population has atleast mild periodontal disease (gingivi-tis) 20-30 exhibits the severedestructive form (chronic periodontitis)1
Characteristically the disease is silentuntil the advanced stage when patientsmay report symptoms like swelling(abscess) discomfort shifting of thedentition or tooth mobility The clini-cal signs of periodontitis emanate frominflammatory and destructive changesin the gingiva connective tissues alve-olar bone periodontal ligament and rootcementum These signs include the for-mation of periodontal pockets loss ofclinical attachment and resorption ofalveolar bone2
Accordingly periodontitis beginswith a pathogenic shift in the bacterialflora around teeth Gram-negativeorganisms such as Porphyromonas gin-givalis Tannerella forsythia Treponemadenticola and Aggregatibacter (formallyActinobacillus) actinomycetemcomi-tans predominate in the subgingivalspace and organize as a biofilm3 Severalof the gram-negative bacteria in thebiofilm are particularly importantbecause they have been identified asred-complex bacteria (T forsythia Pgingivalis and T denticola) and havebeen linked with important parametersof periodontal diagnosis such as pocketdepth and bleeding on probing3 Thisbacterial biofilm is in direct contact withhost tissues along an ulcerated epithe-lial interface called a periodontal pocketLocally bacteria and their products (eglipopolysaccharide entotoxin) penetratehost periodontal tissues and stimulatehost expression of inflammatory medi-ators like arachidonic acid metabolites(prostaglandin E2) and cytokines (inter-leukin-1)4 These mediators in turn trig-ger local inflammatory and destructivechanges in the tissues
Longitudinal population studies indi-cate that these destructive changes (dis-ease progression) are not continuousover time but appear restricted to ldquoran-dom burstsrdquo of activity confined to shortintervals (6 months or less)5 Risk fac-tors associated with progressive peri-odontitis include smoking diabetesobesity poor plaque control and certaingenetic polymorphisms6-10 In additionresidual or persistent deep probingdepths are associated with periodontitisprogression11 Paulander and coworkersrecently demonstrated that periodontitissubjects with moderate (4-5 mm) anddeep (gt 6 mm) probing depths were 2 to3 times more likely to exhibit alveolarbone loss over 10 years12 Similarly fortooth loss the odds ratio for moderatepockets was 29 (95 CI 19-42) andthe odds for deep pockets was 42 (95CI 24-73) These data imply pocketdepth reduction (or resolution) is a clin-ically important treatment goal toensure stability and maintenance inpatients
ComplementaryMedical-MechanicalTreatment Model withAdjunctiveAntimicrobials
Strategies for treating periodontitisprincipally focus on addressing the etio-logic bacteria or biofilm1314 According tothe mechanical model the bacterial bio-film is disrupted and removed via scalingand root planing (SRP) procedures Thesedebridement procedures can be accom-plished nonsurgically or surgically andboth approaches result in pocket depth(PD) reductions in patients1516 In addi-tion a number of adjunctive chemothera-peutic approaches have been developedtested and approved for use in patientswith chronic periodontitis (Table 1) Theseldquolocally delivered antimicrobialsrdquo followa complementary medical-mechanicaltreatment model since they are used incombination with SRP for enhanced effi-cacy These formulations typically cou-
Abstract
Periodontitis is a common oral infection and inflammatory conditionFollowing treatment residual or persistent periodontal inflammation isassociated with disease progression and tooth loss Cumulative evi-dence from clinical trials and meta-analyses support a complementarymedical-mechanical model that combines locally delivered antimicrobialswith scaling and root planing for the treatment of chronic periodontitisAccordingly greater pocket depth reductions andor attachment levelgains occur in patients treated with adjunctive locally administeredantimicrobials (eg tetracycline chlorhexidine doxycycline and minocy-cline) These responses are clinically relevant because they are accom-panied by a higher probability of patient maintenance or pocket resolu-tion Recent trials also indicate that locally administered antimicrobialsmay enhance the effects of periodontal surgical therapy and may reducethe signs of peri-implantitis The consistency of these findings supportsthe use of locally administered antimicrobials for managing dentalpatients with chronic periodontitis
Keywords periodontitis antibiotics antimicrobials local delivery peri-implantitis scaling and root planing
Locally Delivered AntimicrobialsClinical Evidence and RelevanceDavid W Paquette DMD MPH DMSc Maria Emanuel Ryan DDS PhDRebecca S Wilder RDH BS MS
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines
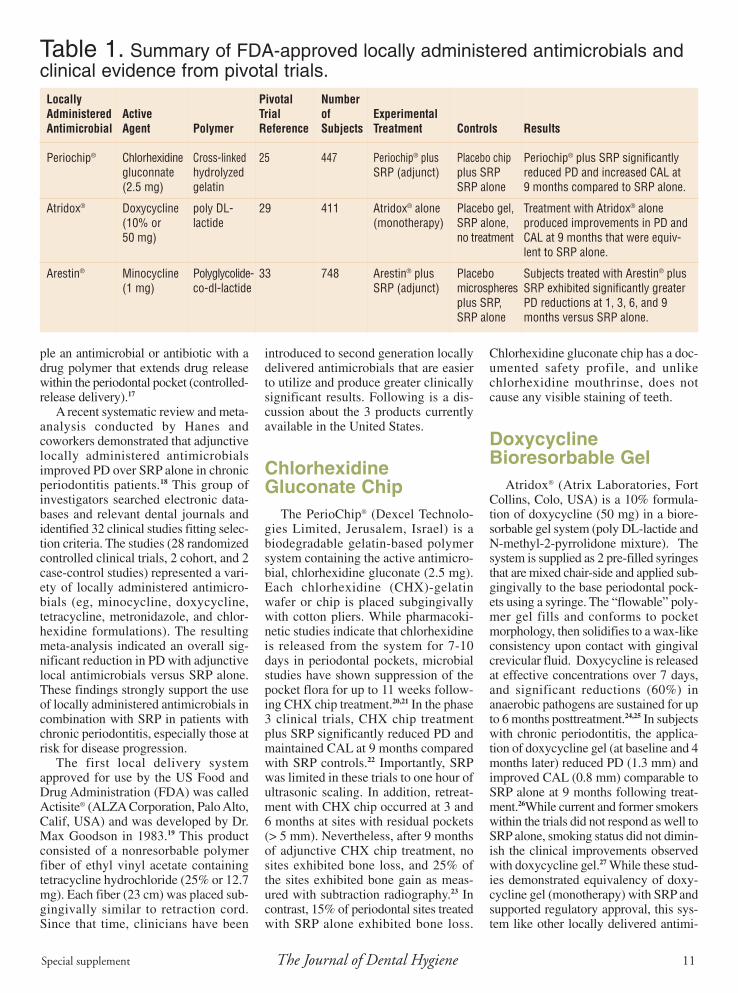
Special supplement The Journal of Dental Hygiene 11
ple an antimicrobial or antibiotic with adrug polymer that extends drug releasewithin the periodontal pocket (controlled-release delivery)17
A recent systematic review and meta-analysis conducted by Hanes andcoworkers demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone in chronicperiodontitis patients18 This group ofinvestigators searched electronic data-bases and relevant dental journals andidentified 32 clinical studies fitting selec-tion criteria The studies (28 randomizedcontrolled clinical trials 2 cohort and 2case-control studies) represented a vari-ety of locally administered antimicro-bials (eg minocycline doxycyclinetetracycline metronidazole and chlor-hexidine formulations) The resultingmeta-analysis indicated an overall sig-nificant reduction in PD with adjunctivelocal antimicrobials versus SRP aloneThese findings strongly support the useof locally administered antimicrobials incombination with SRP in patients withchronic periodontitis especially those atrisk for disease progression
The first local delivery systemapproved for use by the US Food andDrug Administration (FDA) was calledActisitereg (ALZA Corporation Palo AltoCalif USA) and was developed by DrMax Goodson in 198319 This productconsisted of a nonresorbable polymerfiber of ethyl vinyl acetate containingtetracycline hydrochloride (25 or 127mg) Each fiber (23 cm) was placed sub-gingivally similar to retraction cordSince that time clinicians have been
introduced to second generation locallydelivered antimicrobials that are easierto utilize and produce greater clinicallysignificant results Following is a dis-cussion about the 3 products currentlyavailable in the United States
ChlorhexidineGluconate Chip
The PerioChipreg (Dexcel Technolo-gies Limited Jerusalem Israel) is abiodegradable gelatin-based polymersystem containing the active antimicro-bial chlorhexidine gluconate (25 mg)Each chlorhexidine (CHX)-gelatinwafer or chip is placed subgingivallywith cotton pliers While pharmacoki-netic studies indicate that chlorhexidineis released from the system for 7-10days in periodontal pockets microbialstudies have shown suppression of thepocket flora for up to 11 weeks follow-ing CHX chip treatment2021 In the phase3 clinical trials CHX chip treatmentplus SRP significantly reduced PD andmaintained CAL at 9 months comparedwith SRP controls22 Importantly SRPwas limited in these trials to one hour ofultrasonic scaling In addition retreat-ment with CHX chip occurred at 3 and6 months at sites with residual pockets(gt 5 mm) Nevertheless after 9 monthsof adjunctive CHX chip treatment nosites exhibited bone loss and 25 ofthe sites exhibited bone gain as meas-ured with subtraction radiography23 Incontrast 15 of periodontal sites treatedwith SRP alone exhibited bone loss
Chlorhexidine gluconate chip has a doc-umented safety profile and unlikechlorhexidine mouthrinse does notcause any visible staining of teeth
DoxycyclineBioresorbable Gel
Atridoxreg (Atrix Laboratories FortCollins Colo USA) is a 10 formula-tion of doxycycline (50 mg) in a biore-sorbable gel system (poly DL-lactide andN-methyl-2-pyrrolidone mixture) Thesystem is supplied as 2 pre-filled syringesthat are mixed chair-side and applied sub-gingivally to the base periodontal pock-ets using a syringe The ldquoflowablerdquo poly-mer gel fills and conforms to pocketmorphology then solidifies to a wax-likeconsistency upon contact with gingivalcrevicular fluid Doxycycline is releasedat effective concentrations over 7 daysand significant reductions (60) inanaerobic pathogens are sustained for upto 6 months posttreatment2425 In subjectswith chronic periodontitis the applica-tion of doxycycline gel (at baseline and 4months later) reduced PD (13 mm) andimproved CAL (08 mm) comparable toSRP alone at 9 months following treat-ment26While current and former smokerswithin the trials did not respond as well toSRP alone smoking status did not dimin-ish the clinical improvements observedwith doxycycline gel27 While these stud-ies demonstrated equivalency of doxy-cycline gel (monotherapy) with SRP andsupported regulatory approval this sys-tem like other locally delivered antimi-
Locally Pivotal NumberAdministered Active Trial of ExperimentalAntimicrobial Agent Polymer Reference Subjects Treatment Controls Results
Periochipreg Chlorhexidine Cross-linked 25 447 Periochipreg plus Placebo chip Periochipreg plus SRP significantlygluconnate hydrolyzed SRP (adjunct) plus SRP reduced PD and increased CAL at(25 mg) gelatin SRP alone 9 months compared to SRP alone
Atridoxreg Doxycycline poly DL- 29 411 Atridoxreg alone Placebo gel Treatment with Atridoxreg alone(10 or lactide (monotherapy) SRP alone produced improvements in PD and50 mg) no treatment CAL at 9 months that were equiv-
lent to SRP alone
Arestinreg Minocycline Polyglycolide- 33 748 Arestinreg plus Placebo Subjects treated with Arestinreg plus(1 mg) co-dl-lactide SRP (adjunct) microspheres SRP exhibited significantly greater
plus SRP PD reductions at 1 3 6 and 9SRP alone months versus SRP alone
Table 1 Summary of FDA-approved locally administered antimicrobials andclinical evidence from pivotal trials
crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

crobials is conventionally used as an adjunct to SRP inclinical practice
One phase 4 or postmarketing trial investigated theuse of doxycycline gel as an adjunct to SRP and demon-strated incremental benefits when the system was usedin combination with SRP28 Accordingly one arm of theadjunctive use trial involved initiating treatment withultrasonic scaling plus doxycycline gel at baseline andthen isolated SRP at 3 months for those sites with resid-ual pocketing (PD gt 5 mm) The second arm of the studyinvolved SRP alone at baseline and then isolated ultra-sonic scaling and doxycycline gel at those sites withresidual pocketing While both treatment strategies wereequally effective at improving probing depths and clin-ical attachment levels over 6 months responses weregreater on average for the adjunctive doxycycline geltreatment at 3 months compared to SRP alone
Minocycline MicrospheresArestinreg (OraPharma Inc
Warminster Pa USA) is anapproved local delivery systemfeaturing 1mg of minocyclinehydrochloride microencapsu-lated in resorbable polymermicrospheres (polyglycolide-co-dl-lactide) The delivery sys-tem (cartridge and syringe) isdesigned for quick and easyadministration of one unit doseof Arestin subgingivally inperiodontal pockets measuringgt 5 mm with bleeding on probing (BOP) (Figure 1)With this system minocycline hydrochloride is main-tained within pockets for 21 days at concentrations effec-tive against periodontal pathogens The agent may alsoblock collagenases that are implicated in host tissuebreakdown29
The pivotal clinical trials of minocycline microspheresinvolved approximately 750 subjects with generalizedmoderate to advanced chronic periodontitis recruited at 18centers30 Periodontitis subjects meeting inclusion criteriaat baseline were randomized to 1 of 3 treatments 1) scal-ing and root planing (SRP) alone (positive control) 2)SRP plus polymer vehicle (placebo control) or 3) SRPplus minocycline microspheres Full mouth probingexams were performed at baseline (prior to treatment) andat 1 3 6 and 9 months Figure 2 graphs mean probingdepth reductions observed in the 9-month trial for all sub-jects (intent-to-treat population) in the primary analysisAnalyses of covariance adjusting for centers indicatedsignificant-inter-group differences in probing depth reduc-tions at all time points (p lt 0001) In particular subjectstreated with adjunctive minocycline microspheres exhib-ited significantly greater probing depth reductions as com-pared to control subjects treated with SRP alone Whensmokers (Figure 3) or those with advanced periodontitis(mean baseline PD gt 6 mm) (Figure 4) were consideredin secondary analyses again ANCOVA indicated signif-icant probing depth reductions with adjunctive minocy-
Figure 2 Mean probing-depth reductions over ninemonths for periodontitis subjects treated with adjunctiveminocycline microspheres adjunctive vehicle or SRPalone Adapted from Williams et al30
Figure 1 Syringehandle and pre-measured car-tridges for dispens-ing minocyclinemicrospheres
Figure 3 Mean probing-depth reductions over ninemonths for periodontitis subjects who smoke and weretreated with minocycline adjunctive vehicle or SRPalone Adapted from Paquette et al31
Figure 4 Mean probing-depth reductions over ninemonths for advanced periodontitis subjects (mean base-line probing depth gt 6 mm) treated with minocyclineadjunctive vehicle or SRP alone Adapted from Williamset al30
12 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 13
cline microspheres over control treat-ments31 Indeed inter-group differencesin PD reduction were greater amongadvanced periodontitis subjects versusthe overall population
A priori a shift in subject mean prob-ing depth lt 5 mm with treatment wasconsidered a clinically relevant andldquomaintainablerdquo response When regres-sion analyses were performed compar-ing response odds with adjunctiveminocycline microspheres treatmentversus SRP alone the odds ratios forsubjects who smoked or who hadadvanced periodontitis were 206 (95CI 110 385) and 286 (95 CI 145566) respectively32 These data indicatethat patients with advanced periodonti-tis or smokers are 2 to 3 times morelikely to respond and that this increasein odds is clinically relevant Site analy-ses on pocket resolution (posttreatmentPD lt 5 mm) were also designated asmeaningful Again a significantly andconsistently higher percent of pocketswere ldquoresolvedrdquo with adjunctiveminocycline microspheres versus SRPalone for all subjects and smokersrespectively (Table 2)33
A large phase 4 (postmarketing) trialinvolving 2805 patients and 895 dentists
was conducted to evaluate the use ofminocycline microspheres in privatepractices throughout the United States34
Accordingly 1095 patients received 2applications of minocycline micros-pheres (at baseline and 3 months) perprotocol and 1710 patients receivedonly one minocycline microsphereapplication (at baseline) Mean 6-monthpocket depth reductions were 182 and194 mm for the patients receiving oneand 2 minocycline microspheres treat-ments respectively Similar results wereobtained in smokers diabetic patientsand cardiovascular disease patientsAfter one minocycline microspherestreatment 62 of sites had decreasedto less than 5 mm and after 2 treatmentsthe corresponding proportion increasedto 67 This large private practice studydemonstrated that minocycline micros-pheres plus SRP is effective in reducingpocket depth and that efficacy increasedwith retreatment (dose-response)
One recently published trial indicatesthat the effects of flap surgery may beenhanced with adjunctive minocyclinemicrospheres treatment Hellstroumlm andcoworkers recruited 60 periodontitispatients and randomized them to eitherflap surgery plus minocycline micros-
pheres therapy (baseline and weeks 23 and 5) or surgery alone35 At week 25the mean PD reduction from baselinewas 251 mm in the surgery plusminocycline microspheres (test) groupversus 218 mm in the control groupSmokers in the test group had a signifi-cantly greater probing depth reduction(230 mm) as compared to smokers inthe control group (205 mm) In addi-tion the number of sites with probingdepth reductions of 2 mm or more wassignificantly higher in the test groupthan in the control group Henceminocycline microspheres may beadjuncts to both nonsurgical and surgi-cal therapies for patients with moderateto severe chronic periodontitis
These efficacy findings for minocy-cline microspheres have been extendedto peri-implantitis an inflammatoryprocess around one or more osseointe-grated implants in function resulting in aloss of supporting bone and associatedwith a similar pathogenic flora Renvertand coworkers conducted a clinical trial inwhich 32 subjects with peri-implantitis(one implant with PD gt 4 mm bleedingandor exudate on probing and the pres-ence of putative pathogens) randomlyreceived debridement plus minocycline
Baseline PD
TreatmentAll Subjects
Month 1
Month 3
Month 9
Treatment Smokers
Month 1
Month 3
Month 9
5mm
Mino SRPMicro Alone
76 69plt00001
78 71plt00001
75 66plt00001
Mino SRPMicro Alone
73 66plt00001
74 66plt0001
70 61plt00001
6mm
Mino SRPMicro Alone
47 39plt0001
52 48p=001
54 49p=00005
Mino SRPMicro Alone
40 34p=0003
44 41p=017
45 39p=0006
7mm
Mino SRPMicro Alone
22 20p=031
28 23p=001
34 27p=0001
Mino SRPMicro Alone
17 15p=053
22 15p=004
27 20p=004
gt8mm
Mino SRPMicro Alone
10 8p=024
19 14p=002
22 16p=001
Mino SRPMicro Alone
6 3p=009
16 5p=0003
20 12p=004
Table 2 Percentage of periodontal pockets resolving with adjunctiveminocycline microspheres versus SRP Adapted from Paquette et al33
14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

14 The Journal of Dental Hygiene Special supplement
microspheres or debridement pluschlorhexidine gel (02) at baseline 1month and 3 months36 While both treat-ments reduced putative pathogensadjunctive minocycline microsphere treat-ment resulted in significant improvementsin PD compared to chlorhexidine gel at 1month 3 months and 6 months Signifi-cant reductions in bleeding on probingwere also noted for up to 12 months Thisinvestigative group published the resultsfrom a second trial with 30 peri-implanti-tis subjects Again adjunctive minocy-cline microspheres improved PD andbleeding scores whereas the adjunctiveuse of chlorhexidine gel had limitedeffects on bleeding scores37 Anotherinvestigative team Salvi and coworkersalso noted consistent efficacy withminocycline microspheres for treatingperi-implantitis38 Here the investigatorsapplied minocycline microspheres toimplant sites exhibiting bone loss and PDgt 5 mm following a 3-week debridementand hygiene interval While 6 of 31implants were either rescued or exitedfrom the trial because of persistent peri-implantitis all other implants (806)showed significant reduction in both PDand BOP over 12 months with minocy-cline microspheres therapy The investi-gators also examined peri-implantmicroflora using DNA-DNA checker-board hybridization techniques andobserved significant reductions in Aactinomycetemcomitans at 12 months andreductions in ldquored complexrdquo bacteria (Tforsythia P gingivalis and T denticola)for 6 months39 Binary regression analysisshowed that the clinical parameters andsmoking history could not discriminatebetween successfully treated and res-cuedexited implants at any observationtime point In addition failures in treat-ment could not be associated with thepresence of specific pathogens or by thetotal bacterial load at baseline Collec-tively these new data indicate improve-ments in the clinical signs of peri-implan-titis over 12 months with adjunctivelocally administered minocycline
Goodson and coworkers conducted aclinical trial utilizing 124 subjects with
moderate to advanced chronic peri-odontitis Subjects were randomlyassigned to either SRP alone or minocy-cline microspheres and SRP All patientsreceived full-mouth SRP at baseline fol-lowed by treatment with minocyclinemicrospheres if assigned to the SRP andminocycline microspheres group Theexaminer was blinded to the patientrsquostreatment Clinical assessments weremade and plaque samples were collectedat baseline and at Day 30 The resultsdemonstrated that adjunctive minocy-cline microspheres significantly reducedred-complex periodontal pathogens ascompared to SRP alone by one month40
Another investigation conducted byOringer et al41 investigated the effect ofminocycline microspheres on gingivalcrevicular fluid (GCF) levels pyridino-line cross-linked carboxy-terminaltelopeptide of type I collagen (ICTP)and interleukin 1-beta (IL-1) ICTP is abone-specific degradation product andIL-1 is a potent bone-resorptive cyto-kine Forty eight periodontitis patientswere randomized to receive SRP fol-lowed by minocycline microspheres orvehicle Eight healthy individuals servedas a control group Results found apotent short term reduction of ICTP andIL-1 in the SRP plus minocyclinemicrospheres group
Summary andConclusions
Residual or persistent periodontalinflammation is associated with insta-bility of dental tissues (periodontal dis-ease progression and tooth loss) Cumu-lative data from clinical trials andmeta-analyses support a complementarymedical-mechanical model using locallydelivered antimicrobials for treatingchronic periodontitis Overall the clini-cal evidence accrued to date consistentlyshows that when locally administeredantimicrobials are used adjunctively sig-nificantly greater PD reductions andorattachment level gains occur in patientsThese responses are clinically relevant
because they are accompanied by agreater likelihood for patient mainte-nance or pocket resolution Recent trialsalso indicate that locally administeredantimicrobials may enhance the effectsof periodontal surgical therapy and mayreduce the signs of peri-implantitis Theconsistency of these findings supportsthe use of locally administered antimi-crobials for managing dental patientswith chronic periodontitis
Clinical Implications
bull Recent clinical trials indicate thatlocally administered antimicrobialsmay enhance the effects of periodon-tal surgical therapy and may reducethe signs of peri-implantitis
bull Patients with periodontitis exhibitingmoderate (4-5mm) and deep (gt 6mm) probing depths were 2 to 3 timesmore likely to exhibit alveolar boneloss over 10 years
bull A systematic review and meta-analy-sis demonstrated that adjunctivelocally administered antimicrobialsimproved PD over SRP alone inchronic periodontitis patients
bull Patients with advanced periodontitisor smokers are 2 to 3 times more likelyto respond to SRP + minocyclinemicrospheres than to SRP alone
bull Use of minocycline microspheres hasbeen shown to be advantageous whenused as an adjunctive therapy to bothnonsurgical and surgical therapies inpatients with moderate to severechronic periodontitis
bull Adjunctive use of minocyclinemicrospheres has shown a reductionin red-complex periodontal pathogensas compared to SRP alone
Disclosure
Dr Paquette has served as a scien-tific consultant and investigator forOraPharma Inc Dr Ryan and MsWilder are scientific consultants forOrapharma Inc
References1 Albandar J Brunelle JA Kingman A Destructive peri-
odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
2 Flemmig TF Periodontitis Ann Periodontol 1999432-38
3 Socransky SS Haffajee AD Periodontal microbial ecol-ogy Periodontol 2000 200538135-187
4 Offenbacher S Periodontal diseases pathogenesis AnnPeriodontol 19961821-878
5 Socransky SS Haffajee AD Goodson JM Lindhe J Newconcepts of destructive periodontal disease J Clin Peri-
Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 15
odontol 1984 1121-326 American Academy of Periodontology Research Science
and Therapy Committee Tobacco use and the periodon-tal patient J Periodontol 199970 1419-1427
7 Grossi SG Genco RJ Periodontal disease and diabetesmellitus a two-way relationship Ann Periodontol1998351-61
8 Saito T Shimazaki Y Sakamoto M Obesity and peri-odontitis N Eng J Med 1998482-483
9 Ramfjord SP Morrison EC Burgett FG Nissle RR ShickRA Zann GJ Knowles JW Oral hygiene and maintenanceof periodontal support J Periodontol 19825326-30
10 Kornman KS Crane A Wang HY di Giovine FS NewmanMG Pirk FW Wilson TG Jr et al The interleukin-1 geno-type as a severity factor in adult periodontal disease JClin Periodontol 19972472-77
11 Halazonetis TD Haffajee AD Socransky SS Relationshipof clinical parameters to attachment loss in subsets of sub-jects with destructive periodontal diseases J Clin Peri-odontol 198916563-568
12 Paulander J Axelsson P Lindhe J Wennstrom J Intra-oralpattern of tooth and periodontal bone loss between theage of 50 and 60 years A longitudinal prospective studyActa Odontol Scand 200462214-222
13 American Academy of Periodontology Parameter onchronic periodontitis with slight to moderate loss of peri-odontal support J Periodontol 200071853-855
14 American Academy of Periodontology Parameter onchronic periodontitis with advanced loss of periodontalsupport J Periodontol 200071856-858
15 Cobb CM Non-surgical pocket therapy Mechanical AnnPeriodontol 19961450-490
16 Palcanis KG Surgical pocket therapy Ann Periodontol19961589-606
17 Drisko CH Nonsurgical pocket therapy Pharmacothera-peutics Ann Periodontol 19961491-566
18 Hanes PJ Purvis JP Gunsolley JC Local anti-infectivetherapy pharmacological agents A systematic review AnnPeriodontol 2003879-98
19 Goodson JM Holborow D Dunn RL Hogan P Dunham SMonolithic tetracycline-containing fibers for controlled deliv-ery to periodontal pockets J Periodontol 1983 54575-579
20 Soskolne WA Chajek T Flashner M Landau I StabholtzA Kolatch B Lerner EI An in vivo study of the chlorhexi-dine release profile of the PerioChip in the gingival crevic-ular fluid plasma and urine J Clin Periodontol1998251017-1021
21 Stabholz A Sela MN Friedman M Golomb G SoskolneA Clinical and microbiological effects of sustained releasechlorhexidine in periodontal pockets J Clin Periodontol198613783-788
22 Jeffcoat MK Bray KS Ciancio SG Dentino AR Fine DHGordon JM et al Adjunctive use of a subgingival con-trolled-release chlorhexidine chip reduces probing depthand improves attachment level compared with scaling androot planing alone J Periodontol 199869989-997
23 Jeffcoat MK Palcanis KG Weatherford TW Reese MGeurs NC Flashner M Use of a biodegradable chlorhex-idine chip in the treatment of adult periodontitis clinicaland radiographic findings J Periodontol 200071256-262
24 Stoller NH Johnson LR Trapnell S Harrold CQ Garrett SThe pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline comparedto systemically delivered doxycycline in gingival crevicularfluid saliva and serum J Periodontol 1998691085-91
25 Walker CB Godowski KC Borden L Lennon J Nango SStone C et al The effects of sustained release doxycycline on
the anaerobic flora and antibiotic-resistant patterns in sub-gingival plaque and saliva J Periodontol 200071768-774
26 Garrett S Johnson L Drisko CH Adams DF Bandt CBeiswanger B et al Two multi-center studies evaluatinglocally delivered doxycycline hyclate placebo control oralhygiene and scaling and root planing in the treatment ofperiodontitis J Periodontol 199970490-503
27 Ryder MI Pons B Adams D Beiswanger B Blanco VBogle G et al Effects of smoking on local delivery of con-trolled-release doxycycline as compared to scaling androot planing J Clin Periodontol 199926683-691
28 Wennstrom JL Newman HN MacNeill SR Killoy WJ Grif-fiths GS Gillam DG et al Utilisation of locally delivereddoxycycline in non-surgical treatment of chronic peri-odontitis A comparative multi-centre trial of 2 treatmentapproaches J Clin Periodontol 200128753-761
29 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL Berwald B et al Effects of locallydelivered minocycline microspheres on markers of boneresorption J Periodontol 200273835-842
30 Williams R Paquette D Offenbacher S Adams DArmitage G Bray K et al Treatment of periodontitis bylocal administration of minocycline microspheres a con-trolled trial J Periodontol 2001721535-1544
31 Paquette DW Oringer R Lessem J Offenbacher S GencoR Persson GR Williams R Locally delivered minocyclinemicrospheres for the treatment of periodontitis in smokersJ Clin Periodontol 200330787-794
32 Paquette DW Pocket depth reduction as an outcome measureof inflammation and soft tissue changes in Periodontitis trialsJ Int Acad Periodontol 200574 (Supplement)147-156
33 Paquette DW Williams RC Hanlon A Lessem J Clinicalrelevance of adjunctive minocycline microspheres inpatients with chronic periodontitis secondary analysis of aphase 3 trial J Periodontol 200475531-536
34 Lessem J Hanlon A A post-marketing study of 2805patients treated for periodontal disease with Arestin J IntAcad Periodontol 20046150-153
35 Hellstroumlm MK McClain PK Schallhorn RG Bellis L Han-lon AL Ramberg P Local minocycline as an adjunct tosurgical therapy in moderate to severe chronic periodon-titis J Clin Periodontol 200835525-31
36 Renvert S Lessem J Dahleacuten G Lindahl C Svensson MTopical minocycline microspheres versus topical chlorhex-idine gel as an adjunct to mechanical debridement of incip-ient peri-implant infections a randomized clinical trial JClin Periodontol 200633362-9
37 Renvert S Lessem J Dahleacuten G Renvert H Lindahl CMechanical and repeated antimicrobial therapy using a localdrug delivery system in the treatment of peri-implantitis arandomized clinical trial J Periodontol 200879836-44
38 Salvi GE Persson GR Heitz-Mayfield LJ Frei M Lang NPAdjunctive local antibiotic therapy in the treatment of peri-implantitis II clinical and radiographic outcomes Clin OralImplants Res 200718281-5
39 Persson GR Salvi GE Heitz-Mayfield LJ Lang NP Antimi-crobial therapy using a local drug delivery system (Arestin)in the treatment of peri-implantitis I Microbiological out-comes Clin Oral Implants Res 200617386-93
40 Goodson JM Gunsolley JC Grossi SG Bland PS Otomo-Corgel J Doherty F Comiskey J Minocycline HCl micros-pheres reduce red-complex bacteria in periodontal dis-ease therapyJ Periodontol 2007781568-79
41 Oringer RJ Al-Shammari KF Aldredge WA Iacono VJEber RM Wang HL et al Effects of locally deliveredminocycline microspheres on markers of bone resorptionJ Periodontol 2002 73835-842
16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

16 The Journal of Dental Hygiene Special supplement
Introduction
Hujoel et al1 estimated a 31decrease in the prevalence of periodon-titis between the years 1955 and 2000Further these authors estimate an addi-tional 8 decrease by the year 2020 Inspite of the decreased use of smokingtobacco2 better understanding of thepathogenesis of periodontal diseasesand more refined and goal directed ther-apies there remains evidence that den-tistry is not consistently achieving atimely diagnosis and appropriate andtimely treatment of existing periodonti-tis34 Although the evidence is limitedthere is a strong suggestion that use of aperiodontal probe for diagnosis andrecording of periodontal status in treat-ment records in general dental practiceshas yet to achieve the level of a routineand consistent habit5-9 Indeed McFallet al8 determined that except for radi-ographs most private practice patientrecords were so deficient in diagnosticinformation that periodontal status couldnot be established It should be self-evi-dent that treatment requires a definitivediagnosis ie a disease cannot be ade-quately treated unless first diagnosedIn this regard it is interesting to notethat at least one study has reported a dis-connect between dentistsrsquo perception oftreatment rendered and actual treatmentas recorded in patient records10 As anexample prophylactic procedures out-number periodontal procedures by aratio of 2011112 and yet the prevalence ofchronic periodontitis (slight moderateand severe) is estimated to range from alow of 7 (aged gt 18 years)13 up to 35(aged gt 30-90 years)14 of the US adultpopulation
Cobb et al3 compared the pattern ofreferral of periodontitis patients in 1980vs 2000 using patient record data from3 geographically-diverse private peri-odontal practices Results showed thefollowing trends occurring over the 20-year time span decreased use oftobacco increase in the percentage ofcases exhibiting advanced chronic peri-
odontitis with a concomitant decreasein the percentage of mild-moderate dis-ease cases increase in the average num-ber of missing teeth per patient andincrease in the average number of teethscheduled for extraction per patient Asimilar study by Docktor et al4 based onpatient records from 3 private peri-odontal practices located within a majormetropolitan area reported the follow-ing 74 of referred cases were con-sidered advanced periodontitis ofwhich 30 were treatment planned forextraction of 2 or more teeth periodon-tal treatment provided by the general
dental office did not vary because ofdisease severity and the average num-ber of periodontal maintenance vis-itspatientyear in the general dentaloffice was less than the standard of careaccording to severity of disease eg68 of advanced periodontitis casesreported between 0 and 2 periodontalmaintenance visits per year rather thanthe recommended every 3 monthsViewed in aggregate the trendsreported by Cobb et al3 and Docktor etal4 support the assertion that timelydiagnosis and appropriate and timelytreatment of chronic periodontitis have
AbstractA sequence of interrelated steps is inherent to effective periodontaltreatment early and accurate diagnosis comprehensive treatment andcontinued periodontal maintenance and monitoring A primary goal ofperiodontal therapy is to reduce the burden of pathogenic bacteria andthereby reduce the potential for progressive inflammation and recur-rence of disease Emerging evidence of possible perio-systemic linksfurther reinforces the need for good periodontal health In the privatepractice setting the treatment of patients with periodontal disease is bestaccomplished within the structure of a uniform and consistent Peri-odontal Treatment Protocol (PTP) Such a protocol would reinforceaccurate and timely diagnosis treatment needs based on a specificdiagnosis and continual assessment and monitoring of outcomes Thisis best achieved if everyone in the practice setting has a general under-standing of the etiology of periodontal diseases the benefits of treat-ment and potential consequences of nontreatment Communicationskills and patient education are vital components of effective therapysince slight and even moderate stages of the disease often have fewnoticeable symptoms to the patient Accurate documentation and report-ing of procedures for dental insurance reimbursement coupled withscheduling considerations assist general practice settings in effectivelymanaging the increasing volume of patients that can benefit from earlydiagnosis and treatment of periodontal diseases This article presentsthe essential elements of a PTP including diagnosis treatment planningimplementation of therapy assessment and monitoring of therapy insur-ance coding introduction of the patient to periodontal therapy andenhanced verbal skills In addition considerations for implementation ofadjunctive local delivery antimicrobials is presented
Key Words periodontal diseases periodontal diagnosis treatmentprotocol periodontal maintenance periodontal assessment patienteducation
Periodontal Treatment Protocol (PTP) for the General Dental PracticeLarry A Sweeting DDS Karen Davis RDH BSDH Charles M Cobb DDS PhD
Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 17
not significantly improved over time Amajor reason for the reported scarcity oftimely diagnosis and appropriate treat-ment may be the lack of a well-estab-lished office protocol for the diagnosistreatment maintenance and monitor-ing of periodontal disease and involve-ment of the patient through educationObviously this requires dedication ofenergy resources effective communi-cation skills and a change in practicephilosophy
The PeriodontalTreatment Protocol(PTP)
Diagnosis
Regardless of recent advances in ourunderstanding of the etiology and patho-genesis of the periodontal diseases theassessment of traditional clinical param-eters remain the foundation for peri-odontal diagnosis15 Generally such clin-ical parameters include probing depth(PD) bleeding on probing (BOP) clin-ical attachment level (CAL) degree offurcation involvement extent of gingi-val recession tooth mobility and plaquescore Clinicians typically utilize theresults from the periodontal exam radi-ographs and the patientrsquos medical anddental histories to establish a diagnosisand evolve a goaldiagnosis-directedtreatment plan It has been clearlydemonstrated that different interpreta-tions of the same diagnostic informationcan have a dramatic impact on treatmentdecisions16 For this reason a standard-ized approach to periodontal assess-ments and a working protocol as to treat-ment parameters would fill a logicalneed in the average general practice set-ting However due to extensive over-laps in most classification systems anystandardized approach is subject to vari-ations in both clinical assessments (egvariations in probing depth among cli-nicians) as well as the interpretationthereof
All effective treatment protocolsbegin with a thorough and timely diag-nosis Six-point probing to measure PDand BOP is the standard of care Basedon the needs of the patient current radi-ographs should be evaluated to deter-mine the location and percentage of bone
loss The presence location and extentof furcation invasions should be noted aswell as the location of the gingival mar-gin or CAL Also the patientrsquos age is animportant factor especially in cases ofrapidly progressing disease and deter-mining overall long-term prognosis
A modified version of the AmericanAcademy of Periodontology (AAP)proposed guidelines for a comprehen-sive periodontal examination is pre-sented in Table 117 However withrespect to a functional PTP for the gen-
eral dental practice only the followingprincipal diagnostic criteria can beaddressed age PD CAL BOP toothmobility furcation involvement andpercentage of radiographic bone loss Itmust be emphasized that these criteriarepresent the minimal parameters fordetermining a periodontal diagnosisThere are many other important risk andmodifying factors that will impactdevelopment and progression of diseaseand all such factors must be taken intoconsideration when establishing a defin-
Assessment of medical history
Assessment of dental history
Assessment of periodontal risk factors1 Age2 Gender3 Medications4 Presence of plaque and calculus (quantity and distribution)5 Smoking6 RaceEthnicity7 Systemic disease (eg diabetes)8 Oral hygiene9 Socioeconomic status and level of education
Assessment of extraoral and intraoral structures and tissues
Assessment of teeth1 Mobility2 Caries3 Furcation involvement4 Position in dental arch and within alveolus5 Occlusal relationships6 Evidence of trauma from occlusion
Assessment of periodontal soft tissues including peri-implant tissues1 Color2 Contour3 Consistency (fibrotic or edematous)4 Presence of purulence (suppuration)5 Amount of keratinized and attached tissue gingiva6 Probing depths7 Bleeding on probing8 Clinical attachment levels9 Presence and severity of gingival recession
Radiographic evaluation of alveolar bone loss bone density furcationsroot shape and proximity etc
Table 1 Modified Version of the AmericanAcademy of Periodontology Suggested Guidelinesfor a Comprehensive Periodontal Examination18
18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

18 The Journal of Dental Hygiene Special supplement
itive diagnosis and a diagnosis-driventreatment plan18
Age is of relative value in thatadvanced amounts of periodontaldestruction at an earlier age tend to indi-cate a more aggressive form of peri-odontitis In contrast chronic periodon-titis may slowly progress towardsseverity over several years or decadesYoung age combined with moderate tosevere bone loss presents a tenuouslong-term prognosis and requires moreaggressive therapy compared to theolder patient presenting with a chronicform of periodontitis19
Probing depth (PD) is defined asthe distance from the gingival marginto the base of the gingival crevice20 Theperiodontal pocket represented by aprobing depth gt 3 mm is the principlehabitat for gram-negative anaerobicpathogenic bacteria20 Deeper pocketstend to represent more extensivedestruction of the underlying periodon-tium and therefore a potentially greaterpathenogenic burden
Clinical Attachment Level (CAL) isdefined as the distance from the CEJ tothe base of the probable crevicepocketIn cases of gingival recession the amountof recession is added to the PD to yieldthe total amount of CAL Although moredifficult to obtain it is a better measure ofthe total extent of damage to the under-lying periodontium20-22
Mobility is best measured by theblunt end of 2 instruments alternatingpressure in a facial-lingual direction andan apical direction to assess abnormalmovement of the tooth Simplyassessed Grade I mobility is slightlymore than normal Grade II is moder-ately more than normal Grade III issevere mobility facial-lingually plus api-cal displacement23 Mobility patterns aresuggestive of possible occlusal traumasevere inflammation andor loss of sup-porting alveolar bone
Furcations represent bone lossbetween the roots of multi-rooted teethA deeply invasive furcation lesion is theequivalent of a poor long-term progno-sis for the involved tooth Simply put aGrade 1 furcation involvement is incip-ient bone loss only a Grade 2 is partialloss of bone producing a cul-de-sac aGrade 3 is total bone loss with through-and-through opening of the furcationand a Grade 4 is similar to a Grade 3 butwith gingival recession that visuallyexposes the furcation opening24
Radiographic Evidence of BoneLoss is best determined with adequateand current radiographs17 most typicallya full-mouth periapical survey includingvertical bite-wings or a panographicradiograph supplemented with verticalbite-wings and selected periapical filmsBy definition true periodontitis does notbegin until bone loss occurs25 Radi-ographic evaluation of the distributionand severity of bone loss bone densityroot anatomy and approximation to otherteeth provides specific information thatwill help in determining a proper diag-nosis treatment plan and prognosis
Bleeding on Probing (BOP) is asimple assessment of the inflammatorystatus of the gingiva1526 In patients withdeeper pockets andor loss of clinicalattachment the chances of disease pro-gression are greater as the percentage ofbleeding sites increase27 Converselylack of BOP is highly correlated withstability and a lack of inflammation28
This latter statement however does notapply to smokers as they tend to bleedless when compared to nonsmokers withequal amounts of disease29
In addition to the usual clinicalparameters the clinician is well advisedto consider other risk factors and theirpotential impact on the development andprogression of plaque-induced peri-odontal diseases18 Risk factors that aresometimes overlooked in the diagnosistreatment plan and prognosis equationinclude among others diabetes smok-ing osteoporosis compromised immunesystem drug-induced gingival condi-tions hormonal changes and geneticsPatients at risk for periodontal diseaseare often allowed to ldquoslip between thecracksrdquo during a routine visit becausethey may be in the early stages of thedisease Risk factors increase a patientrsquoschance of developing periodontitis Thepresence of one or more of these riskfactors may also indicate a benefit fromspecialty referral in some patients
Case Types and PeriodontalDiagnosis
As part of a PTP it is necessary toestablish diagnostic guidelines that willprovide a framework for organizing thetreatment needs of the patient Guide-lines are not meant to replace clinicalknowledge or skills nor do they imply aone-size-fits-all treatment plan for peri-
odontal disease It is recognized thateach dental practice setting is differentConsequently guidelines are intendedto be used in a manner that best meetsthe needs of the specific patient
Generally speaking plaque-inducedperiodontal diseases have historicallybeen categorized into gingivitis versusperiodontitis based upon whether attach-ment loss has occurred The 1999 Inter-national Workshop for Classification ofPeriodontal Diseases21 reclassified theplaque-induced periodontal diseases into7 different classifications In considera-tion of a working PTP that addressesonly the common periodontal diseasesthis paper will address health gingivitischronic periodontitis (formerly adultperiodontitis) and aggressive periodon-titis (formerly early-onset periodontitis)The first 7 entries in Table 2 (see backcover) constitute a set of clinical criteria(PD BOP percent bone loss toothmobility degree of furcation involve-ment and CAL) that will facilitate dif-ferentiation of health from gingivitis andbetween the various levels of severityof chronic periodontitis Further Table 2can aid the clinician in differentiatingbetween chronic and aggressive peri-odontitis
Some practice settings may prefer asystem of ldquoPeriodontal Case Typesrdquo forpurposes of diagnosis and record keep-ing Table 3 presents the diagnostic clin-ical criteria as applied to Case Types forhealth gingivitis chronic periodontitis(slight moderate and severe) andaggressive periodontitis These criteriaand Case Types are generally appropri-ate but should be considered as guide-lines only and not as a definitive diag-nosis As mentioned before there arenumerous modifying and risk factors toconsider prior to evolving a diagnosisand a diagnosis-driven treatment plan
Treatment Planning
Development of a logical and prop-erly sequenced treatment plan is a deriv-ative of the periodontal assessment anddiagnosis Periodontal therapy is diag-nosis-driven and to the extent possibleshould address all modifying factors andrisk factors that impact development andprogression of plaque-induced peri-odontal disease An overview of a typi-cal periodontal treatment plan is pre-sented in Table 430
PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

PD BOP Bone Mobility Furcations CAL VisualCase Type (mm) (YesNo) Loss () (Grade) (Grade) (mm) Inflammation
0 (Health) 0-3 No 0 None None 0 No
I (Gingivitis) 0-4 Yes 0 None None 0 Yes (localized orgeneralized)
II (Slight Chronic Periodontitis)dagger 4-5 Yes 10 I 1 1-2 Yes (localized orgeneralized)
III (Moderate Chronic Periodontitis)dagger 5-6 Yes 33 I and II 1 and 2 3-4 Yes (localized orgeneralized)
IV (Severe Chronic Periodontitis)dagger gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized orgeneralized)
V (Aggressive Periodontitis)dagger_ gt 6 Yes gt 33 I II or III 1 2 3 or 4 gt 5 Yes (localized or(age is significant factor) generalized)
Localized disease is defined as lt 30 of sites are involved and generalized disease infers gt30 of sites are involved21
dagger Specialty referral may be indicated for additional treatment beyond initial therapydagger_ Specialty referral should be considered
Table 3 Clinical Criteria Assigned to Periodontal Case Types of Health Gingivitis Chronic Periodontitis (slight moderate and severe)and Aggressive Periodontitis
Sequence of Major Phases
1 Address acute periodontal problems andor pain
2 Review and update medical and dental histories
3 Assessment of systemic risk factors and refer for medical consultation as needed
4 Extraoral examination
5 Oral cancer evaluation
6 Assessment of periodontal risk and modifying factors
7 Periodontal examination to include dental implants
8 Dental examination to include occlusal relationships and dental implants
9 Radiographic examination
10 Establish a definitive diagnosis
11 Generate a diagnosis-driven periodontal treatment plan and sequence of treatment
12 Determine required adjunctive restorative prosthetic orthodontic andor endodontic treatments andsequence
13 Execute Phase I therapy (aka anti-infective or nonsurgical therapy) with consideration given to adjunc-tive use of chemotherapeutic agents
14 Re-evaluation (assessment) of Phase I therapy
15 If end-points are not achieved consider selective retreatment need for surgical therapy specialty refer-ral or use of adjunctive diagnostic aides eg microbial genetic medical lab tests etc
16 Determine interval for periodontal maintenance and continued assessment of periodontal status
Table 4 General Overview of the Major Steps in a Typical PeriodontalTreatment Plan3
Special supplement The Journal of Dental Hygiene 19
Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Implementation of Therapy
There are a wide variety of treatmentoptions to be considered when con-fronted with gingivitis or chronic oraggressive periodontitis However thor-ough scaling and root planing (SRP) isstill considered the gold standard in peri-odontal therapy Beyond SRP no onetreatment modality is the answer inevery case However the clinician musthave specific endpoints or goals thattherapy should achieve If such end-points are not achieved then therapymust be re-evaluated and a decisionmade concerning retreatment or spe-cialty referral for consideration of moreadvanced therapy options Treatmentoptions that should be consideredinclude30
bull Patient education including plaquecontrol and counseling in manage-ment of periodontal and systemicrisk factors
bull Scaling and root planing
bull Consideration of adjunctive chemo-therapeutic agents eg locally orsystemically administered antibi-otics and host response modifica-tion agents
bull Re-evaluation
bull Consideration of referral to a spe-cialist is an option that must be con-sidered for both legal and ethicalreasons31 There are a variety of rea-sons to consider referral to a peri-odontist such as SRP in the pres-ence of extreme amounts of dentalcalculus or SRP with complicationsof systemic disease gingival over-growth andor inflammatory hyper-plasia resective surgery regenera-tive procedures for soft and hardtissues periodontal plastic surgeryocclusal therapy pre-prosthetic sur-gery dental implants managementof perio-systemic complicationsphobic patients requiring conscioussedation etc
Periodontal Maintenance Therapy and Continual Assessment
In general data suggests that patientswho have undergone definitive therapyfor either localized or generalized peri-
odontitis should be managed by peri-odontal maintenance (PM) performedat an interval of 3 months for an indefi-nite period of time following active ther-apy32 The 3-month interval is critical(and the standard of care for moderateand severe chronic periodontitis andaggressive periodontitis) as it has beenrepeatedly shown to be effective inreducing disease progression preserv-ing teeth and controlling the subgingi-val bacterial burden33-35 Nonetheless thePM schedule should be individualizedand tailored to meet the needs of eachpatient Factors such as home care pre-vious level of disease tendency towardrefraction stability indicators etcshould be used in making this assess-ment More fragile patients may needintervals of 2 months or less and con-versely patients intercepted in early dis-ease states who demonstrate consistentstability may need less frequent inter-vals of 4-6 months Regardless of theinterval between appointments the peri-odontal status of each patient should bere-evaluated at every maintenanceappointment Only through close moni-toring can disease recurrence be detectedand the maintenance interval adjustedaccordingly Continual assessment of theperiodontium during maintenanceaffords the best opportunity for assur-ing long-term stability or providinginterceptive care3435
Insurance Coding
The American Academy of Peri-odontologyrsquos Parameters of Care 200036
and the American Dental AssociationrsquosCurrent Dental Terminology37 are avail-able to clinicians to guide decision-mak-ing related to providing therapeutic peri-
odontal treatment and subsequentreporting of services for insurance reim-bursement In terms of nonsurgical peri-odontal therapy familiarity with dentalinsurance codes provides a clear methodto document treatment and select appro-priate procedures to maximize insurancereimbursement for the patient
Table 5 presents a modified descrip-tion of the ADA insurance codes mostcommonly used in Phase I periodontaltherapy (aka anti-infective therapy ornonsurgical therapy) The descriptionsare intended to reveal distinctive differ-ences between procedures and guide theclinician in reimbursement procedures
To simplify decisions made bypatients dental insurance should bereferred to as ldquoreimbursementrdquo ldquobene-fitrdquo or ldquoassistancerdquo by the clinician andother staff members rather than ldquocover-agerdquo since the word implies completeMost patients with dental insurance willfind it necessary to supplement what-ever insurance benefit they receivetoward lifetime periodontal care asmany plans have contract limitations forthe percentage of reimbursement asso-ciated with various procedures andorthe length of time those benefits applyFor example limitations of some insur-ance plans assign benefits for PM fol-lowing SRP but only for 24 months fol-lowing active therapy As anotherexample exclusions found in otherinsurance plans assign benefits for SRPfor generalized periodontal disease butnot for localized infection Manypatients are reticent to proceed withtreatment unless their insurance willldquopay for itrdquo Consequently it is advan-tageous for practices to have clear expla-nations about the reality of dental insur-ance Figure 2 presents a sampleexplanation of dental insurance that can
Figure 2 Facts about dental insurance to share with patients
Understanding Dental Insurance1 Dental insurance is a contractual agreement between the employer
and insurance company The percentage of reimbursement variesgreatly dependent upon the premiums paid for a particular plan andlimitations of the agreement
2 Maximum payable benefits around $1000 - $1500 commonly foundtoday with dental insurance plans are almost identical to the annualmaximum benefit of dental insurance plans 40 years ago
3 Dental insurance is a benefit designed to help defray the costs ofquality dental care but is not all-inclusive of what an individual mayneed or desire to obtain optimal dental health for a lifetime
20 The Journal of Dental Hygiene Special supplement
Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 21
CodeNumber Treatment Procedure DescriptionD0180 Comprehensive Indicated for new or established patients showing signs or symptoms of
Periodontal Evaluation periodontal disease and for patients with risk factors such as smokingor diabetes It includes evaluation of periodontal conditions probing andcharting evaluation and recording of the patientrsquos dental and medicalhistory and general health assessment It may include the evaluationand recording of dental caries missing or unerupted teeth restorationsocclusal relationships and oral cancer evaluation
D1110 Adult Prophylaxis Includes the removal of plaque stain and calculus from tooth structuresand is intended to control local irritation to gingival tissues thereby preventing disease initiation
D4355 Full Mouth Debridement Initial removal of plaque and calculus that interfere with the ability toto Enable Comprehen- perform a comprehensive oral evaluation This preliminary procedure is sive Evaluation and generally followed by a comprehensive periodontal evaluation forDiagnosis diagnosis and subsequent therapeutic periodontal procedures
D4341 Scaling and Root Involves therapeutic treatment of 4 or more periodontally involved teethPlaning per quadrant through definitive removal of subgingival plaque biofilm andGeneralized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant inclusive
of updated periodontal charting and radiographs for reimbursement
D4342 Scaling and Involves therapeutic treatment of 1 to 3 periodontally involved teeth perRoot Planing quadrant through definitive removal of subgingival plaque biofilm andLocalized per root preparation in order to halt the disease from progressing therebyQuadrant creating an opportunity for healing To be reported per quadrant with
identification of specific teeth being treated inclusive of updated peri-odontal charting and radiographs for reimbursement
D4381 Localized Delivery of Subgingival insertion of antimicrobial medications of a therapeutic con-Antimicrobial Agents via centration into periodontal pockets that are released over a sufficienta Controlled Release length of time in order to suppress the pathogenic burden and are Vehicle into Diseased intended to enhance the clinical results of scaling and root planing aloneCrevicular Tissue To be reported per tooth identifying multiple treatment sites per tooth if
indicated inclusive of a narrative describing systemic considerations forreimbursement such as tobacco usage diabetes or heart disease
D4999 Unspecified Periodontal In the absence of a specific ADA code for complete periodontalProcedure by Report re-assessment following definitive periodontal therapy this procedure
code is being utilized to determine healing response and future treat-ment recommendations
D4910 Periodontal Maintenance Follows the completion of active therapy to treat periodontal infectionfor the lifetime of the dentition or implant replacements and includesremoval of plaque biofilm and calculus from supra and subgingival sur-faces It may also include site specific scaling and root planing for areasof localized disease recurrence It is intended to keep periodontal dis-eases under control therefore a patient may move from active therapyto periodontal maintenance and back to active therapy andor referralduring the lifetime of the dentition or implant replacements It is not syn-onymous with prophylaxis and is required at varying intervals to man-age periodontal diseases and modify risk factors To be reported byboth general and periodontal practices on patients having undergoneactive therapy irrespective of where the procedure is performed Cur-rent periodontal charting documenting the patientrsquos on-going periodon-tal status should be submitted for reimbursement
Table 5 Modified Description of ADA Insurance Codes Commonly Used for Phase I Periodontal Therapy (aka anti-infective therapy or nonsurgical therapy)
22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

22 The Journal of Dental Hygiene Special supplement
be shared with patients assisting them inmaking independent decisions abouttreatment regardless of the insurancereimbursement schedule
Patient Education and Introduction to Periodontal Therapy
Effective implementation of theaforementioned concepts requiresexpertise in effective patient educationand introduction of periodontal therapyso that patients are prepared to makewise health decisions Being proficientin SRP procedures has little value to thepatient who assumes they are visitingthe dental hygienist for a ldquoroutine clean-ingrdquo This is particularly true if thepatient already has a developing or exist-ing periodontal infection and does notunderstand the need for therapeuticintervention Chronic periodontal dis-eases often provide few noticeablesymptoms especially in earlier stagesof development Thus the need foreffective communication education andlistening skills are of particular impor-tance to todayrsquos dental patient
The incidence of moderate andsevere generalized chronic periodonti-tis in the US appears to affect only 5to 15 of the adult population whereasslight disease affects approximately 35of the adult population131438 Thus mostnew patients and even many existingpatients will ultimately be diagnosedwith periodontal diseases To be effec-tive at enrolling patients into active ther-apy everyone in the practice setting musthave a basic understanding of the etiol-ogy of periodontal diseases treatmentoptions consequences of nontreatmentand direct benefits of therapy Patientsare more motivated to accept treatmentrecommendations when a clear diagno-sis has been established they are giventhe opportunity to see infection in theirown mouths their questions have beenanswered and they understand the valueof treating periodontal infection in rela-tion to their overall health
Many clinicians inform patients oftheir periodontal status while workingin their mouths with sharp instrumentsor give a summary of findings at the endof the visit Most patients are visuallearners Consequently patients need tosee the condition of their own mouthAt the beginning of every appointment
during data collection and tissue assess-ment the patient should be provided amirror to visualize with the clinician theevidence of periodontal disease cariesgingival recession tooth mobility fur-cation involvement etc (Figure 1) Dur-ing periodontal probing the patientshould hear the pocket measurements asdata is being collected and recorded Ina similar manner during examination ofthe radiographs the patient should beshown evidence of permanent bone lossand contrast that to areas without boneloss Involving the patient in the dis-covery process visually and audibly is apowerful tool to help patients take own-ership in their own health
This is also an opportune time for theclinician to introduce adjunctive thera-pies to the patient such as the use oflocally delivered antimicrobials andother agents For example the cliniciancan communicate that locally deliveredantimicrobials have been on the US mar-ket for many years and have been shownto be a safe effective treatment optionImportant information to conveyincludes the ease of application the highpotency of the drug at levels that willkill bacteria it does not affect the rest ofthe body and there is no need for anadditional appointment to remove theproduct since the agent biodegradesEducating the patient to all of their treat-ment options is vital to clear and evi-dence-based communication
Enhanced Communication Skills
Each clinician will develop hisherown style of case presentation for peri-odontal therapy and will individualizethe message to different patients How-ever there is significant advantage ifthe entire office staff has continuity inkey words that are used when dis-cussing periodontal therapy withpatients Equally important is the avoid-ance of minimizing messages such asldquojust a little bit of bleedingrdquo or ldquoa littlebone lossrdquo or ldquojust a little bit ofplaquerdquo It is advisable to use languagethat does not trivialize conditions thatare not yet severe Terms such as ldquoslight
bleedingrdquo ldquoearly bone lossrdquo or ldquoslightplaquerdquo accurately describe findingswithout overstating them Periodontaldisease is a bacterial infection leading toa host immune response that is charac-terized by inflammation and degrada-tion of periodontal tissues22 Wheninforming patients of periodontal dis-ease using the word ldquoinfectionrdquo is morepowerful than ldquogum inflammationrdquo andcan create a sense of urgency regardingtreatment The word ldquohemorrhagerdquoindicates heavy bleeding and implies acondition outside healthy parametersWhen the patientrsquos gingival tissueshemorrhage easily upon provocationldquohemorrhagerdquo rather than ldquobleedinggum tissuerdquo should be verbalized to thepatient The words ldquoscaling and root
Figure 1 Dental hygienist showing patient periodontal conditions inpatientrsquos own mouth
Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Special supplement The Journal of Dental Hygiene 23
Where to use locally delivered antimicrobials Pockets gt 5 mm with bleeding on probing (BOP)
bull The locally delivered antimicrobial may be used atthe time of scaling and root planing (SRP) or at there-evaluation appointment 4-6 weeks following SRPIf used first at the re-evaluation appointment the sitemust have additional SRP to remove biofilm and harddeposits that may have re-accumulated
Residual pockets of gt 5 mm with BOP or any site gt 6mm following initial SRPbull Determined at re-evaluation appointmentbull If gt 4 residual pockets in a given quadrant then con-
sider either retreatment (SRP) with locally deliveredantimicrobial or surgical intervention
Sites treatment planned for osseous graftingbull Locally delivered antimicrobial placed 3 weeks prior
to surgical procedure Periodontal abscess Probing depth at the distal-facial line-angle of 2nd
molars related to 3rd molar extractions where surgicalintervention will yield a compromised result
Ailingfailing dental implants (peri-implantitis) where sur-gical intervention is not indicated or will yield a compro-mised result
Grade II furcation involvements (shallow or deep) whensurgical intervention is not planned
Who might benefit from use of locally deliveredantimicrobials Periodontal maintenance
patients with isolatedprobing depths of gt 5 mmthat exhibit BOP or anypocket gt 6 mm (Figure 3)
Patients wanting to avoidperiodontal surgery
High risk surgery patientsbull Poorly controlled (brit-
tle) diabetic patientsbull Patients with a history
of recent or recurrentcoronary or cere-brovascular events
bull Patients with a compromised immune system due todisease or medications
bull Kidney dialysis patientsbull Heavy smokers (gt12 packday)bull Patients with physical disability that impacts oral
hygiene efficiencybull Mentally handicapped patients
Patientrsquos with marginal oral hygiene that is not likely toimprove and thereby represent a poor surgical risk
Please note that locally applied antimicrobials may needto be placed more than one time to achieve the desiredresult
How to apply locally delivered antimicrobials For optimal effect from locally delivered antimicrobials
the following must be achievedbull Oral hygiene instructions and patient compliance
regarding the necessary oral hygiene procedures ietooth brushing use of interdental hygiene aids suchas dental floss and proxabrushes and use of antimi-crobial oral rinses
bull Supragingival scaling and polishingbull Definitive subgingival SRP (generally under local
anesthesia)bull Place locally delivered antimicrobial according to
manufacturerrsquos directions For example in the caseof minocycline microspheres place one pre-meas-ured dose per pocket If the tooth has 2 pockets thatneed local delivery 2 full doses should be adminis-tered
bull The pocket should be as biofilm and deposit free aspossible prior to insertion
bull Insert the locally delivery product to the base of thepocket In the case of minocycline microspheres thetip should be placed as far into the pocket as possi-ble before activatingthe syringehandle(Figures 4 and 5)
Addendum If probing depths are lt 4
mm the clinician shouldconsider a conventionaladult prophylaxis coupledwith oral hygiene recom-mendations andor rein-forcementbull If the patient exhibits
multiple probingdepths of 4 mm a peri-odontal maintenanceinterval of 3-4 monthsshould be considereduntil it can be deter-mined if the patientrsquosperiodontal status isstable andor improv-ing
Guide for Use of Locally Delivered Antimicrobials
Figure 3 Pre-treatmentclinical presentationshowing PD of 6 mm
Figure 4 Initial Inser-tion of the pre-meas-ured tip for adminis-tration of minocyclinemicrospheres
Figure 5Tip place-ment to base ofpocket for administra-tion of minocyclinemicrospheres
24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

24 The Journal of Dental Hygiene Special supplement
References1 Hujoel PP Bergstroumlm J del Aguila MA DeRouen TA A hid-
den periodontitis epidemic during the 20th century Com-munity Dent Oral Epidemiol 2003311-6
2 Mendez D Warner KE Adult cigarette smoking preva-lence Declining as expected (not as desired) Am J PubHealth 200494251-252
3 Cobb CM Carrara A El-Annan E et al Periodontal refer-ral patterns 1980 versus 2000 A preliminary study J Peri-odontol 2003741470-1474
4 Dockter KM Williams KB Bray KS Cobb CM Relation-ship between pre-referral periodontal care and peri-odontal status at time of referral J Periodontol2006771708-1716
5 Bader JD Rozier G McFall WT Jr Sams DH GravesRC Slome BA Ramsey DL Evaluating and influenc-ing periodontal diagnostic and treatment behaviors ingeneral practice J Am Dent Assoc 1990121720-724
6 Cury PR Martins MT Bonecker M De Araujo NS Inci-dence of periodontal diagnosis in private dental practiceAm J Dent 200619163-165
7 Heins PJ Fuller WW Fries SE Periodontal probe use ingeneral practice in Florida J Am Dent Assoc 1989119147-150
8 McFall WT Jr Bader JD Rozier G Ramsey D Presenceof periodontal data in patient records of general practi-tioners J Periodontol 198859445-449
9 Brown LJ Johns BA Wall TP The economics of peri-odontal diseases Periodontol 2000 200229223-234
10 Helminen SE Vehkalahti M Murtomaa H Dentistsrsquo per-ception of their treatment practices versus documentedevidence Int Dent J 20025271-74
11 Blair C The economic impact of the under diagnosis ofperiodontal disease in general practice Triage 2005121-25
12 American Dental Association Survey Center 1999 Surveyof Dental Services Rendered Chicago IL American Den-tal Association 1999
13 Borrell LN Burt BA Taylor GW Prevalence and trends inperiodontitis in the USA The NHANES 1988 to 2000 JDent Res 200584924-930
14 Albandar JM Brunelle JA Kingman A Destructive peri-odontal disease in adults 30 years of age and older in theUnited States 1988-1994 J Periodontol 19997013-29
15 Armitage GC Periodontal diseases Diagnosis Ann Peri-odontol 1996137-215
16 Papapanou PN Wennstrom JL Sellen A Hirooka H Gron-dahl K Johnsson T Periodontal treatment needs assessedby the use of clinical and radiographic criteria CommunityDent Oral Epedimiol 199018113-119
17 American Academy of Periodontology Parameter on com-prehensive periodontal examination J Periodontol200071(Suppl)847-848
18 Krebs KA Clem DS III American Academy of Periodon-tology Guidelines for the management of patients withperiodontal diseases J Periodontol 2006771607-1611
19 Novak KF Goodman SF Takei HH Determination of prog-nosis In Newman MG Takei H Klokkevold PR CarranzaFA eds Clinical Periodontology 10th ed PhiladelphiaSaundersElsevier 2006 pp 614-625
planingrdquo may sound confusing topatients or imply discomfort The wordsldquoperiodontal therapyrdquo are effectivesemantic choices when informingpatients about necessary periodontaltreatment ldquoWe now knowrdquo are wordsthat can introduce patients to new ideasor treatment options to explain whyinformation may be different than whatthey have heard in the past or expectedto hear at their current visit ldquoHaltingrdquoor ldquoarresting diseaserdquo can be used todescribe a measurable goal for treatingperiodontal diseases that should beobtained through intervention ldquoDailydisease controlrdquo communicates to thepatient that they share in the role in theeffective removal of plaque bacteriabeyond what it achieve through peri-odontal treatment
Even though some states requirewritten consent effective communica-tion between the clinician and the patientis the important consideration ofinformed consent39 not the completionof a form Therefore deliberate seman-tic choices should be shared by all mem-bers of the office staff to optimizepatient understanding of their periodon-tal conditions
Suggestions forImplementation of aPeriodontal Treatment Protocol in the General Practice Setting
bull General dentists and dental hygien-ists should schedule a meeting withreferring periodontists and theirdental hygienists to share philoso-phies of periodontal treatment andestablish clarity for referrals
bull Schedule a team meeting workshopto bring all office staff up-to-dateregarding periodontal assessmentsdiagnosis case types periodontalrisk factors individualized treat-ment of periodontal diseases con-sequences of nontreatment (toothloss and possible systemic involve-ment) and the value of periodontalmaintenance
bull Establish continuity of the verbalskills and terminology the officestaff will utilize to communicateeffectively to patients about peri-odontal conditions
bull Include assessments and diagnosisof periodontal diseases in all newpatient visits routine prophylaxisappointments and ongoing peri-odontal maintenance to insure nopatient is overlooked regardingdiagnosis of developing periodontaldisease or recurring disease
bull Select appropriate ADA InsuranceProcedure Codes for reporting peri-odontal procedures in order to max-imize the patientrsquos benefit
bull Share insurance information withpatients to assist them in reducingtheir dependence on dental insur-ance benefits thereby enablingthem to make independent healthdecisions related to treatment ofperiodontal diseases
Disclosure
Dr Sweeting Ms Davis and DrCobb are scientific advisors forOraPharma Inc
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines
20 Carranza FA Camargo PM The periodontal pocket InNewman MG Takei H Klokkevold PR Carranza FA edsClinical Periodontology 10th ed Philadelphia Saun-dersElsevier 2006 pp 434-451
21 Armitage GC Development of a classification system forperiodontal diseases and conditions Ann Periodontol199941-6
22 American Academy of Periodontology Position paperDiagnosis of periodontal diseases J Periodontol2003741237-1247
23 Carranza FA Takei HH Clinical diagnosis In NewmanMG Takei H Klokkevold PR Carranza FA eds ClinicalPeriodontology 10th ed Philadelphia Saunders Elsevier 2006 pp 540-560
24 Carranza FA Takei HH Bone loss and patterns of bonedestruction In Newman MG Takei H Klokkevold PRCarranza FA eds Clinical Periodontology 10th edPhiladelphia SaundersElsevier 2006 pp 452-466
25 Armitage GC Clinical evaluation of periodontal diseasesPeriodontol 2000 1995739-53
26 Haffajee AD Socransky SS Lindhe J Kent RL OkamotoH Yoneyama T Clinical risk indicators for periodontalattachment loss J Clinical Periodontol 199118117-125
27 Claffey N Egelberg J Clinical indicators of probing attach-ment loss following initial periodontal treatment inadvanced periodontitis patients J Clin Periodontol199522 690-696
28 Lang NP Adler R Joss A Nyman S Absence of bleedingon probing ndash an indicator of periodontal stability J ClinPeriodontol 199017714-721
29 Muller HP Stadermann S Multivariate multilevel models forrepeated measures in the study of smoking effects on the
association between plaque and gingival bleeding ClinOral Invest 200610311-316
30 American Academy of Periodontology Position paperGuidelines for periodontal therapy J Periodontol2001721624-1628
31 American Dental Association Principles of ethics and codeof professional conduct January 2005 Available athttpwwwadaorgprofpraclawcodeindexasp AccessedAugust 28 2008
32 American Academy of Periodontology Position paper Peri-odontal maintenance J Periodontol 2003741395-1401
33 Greenwell H Bissada NB Wittwer JW Periodontics ingeneral practice Perspectives on periodontal diagnosis JAm Dent Assoc 1989119537-541
34 Hirschfeld L Wasserman B A long-term survey of toothloss in 600 treated periodontal patients J Periodontol197849225-237
35 Tonetti MS Muller-Campanile V Lang NP Changes in theprevalence of residual pockets and tooth loss in treatedperiodontal patients during a supportive maintenance careprogram J Clin Periodontol 1998251008-1016
36 American Academy of Periodontology Parameters of careJ Periodontol 200071 847-880
37 American Dental Association Current Dental Terminology2007-20083-27
38 American Academy of Periodontology Position paper Epi-demiology of periodontal diseases J Periodontol2005761406-1419
39 American Academy of Periodontology American Acad-emy of Pediatric Dentistry Guideline for periodontaltherapy Pediatr Dent 2005-200627(7 Reference Man-ual)197-201
Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines

Case Slight Moderate AdvancedIndicator Healthy Gingivitis Periodontitis Periodontitis Periodontitis AggressiveRefractory
Pocket Deptha lt 3 mm lt 4 mm 4 - 5 mm 5 -6 mm gt 6mm gt 6mm
Bleeding Upon No Yesb Yesb Yesb Yesb Yesb
Probing
Six-Point Yes Yes Yes Yes Yes YesProbing
Bone Loss None None lt 10 lt 33 gt 33 gt 33
Tooth None None None lt Grade II lt Grade III lt Grade IIIMobilityc
Furcationd None None lt Grade I lt Grade II lt Grade IIIIV lt Grade IIIIV
Clinical None None 1 - 2 mm CAL 3 - 4 mm CAL gt 5 mm CAL gt 5 mm CALAttachmentLoss (CAL)e
Other No Only gingival Signs of inflammation Signs of inflammation Signs of inflammation Signs of inflammationinflammation tissues affected may be present including may be present including may be present including may be present including
by the bull Edema bull Edema bull Edema bull Edemainflammatory bull Redness bull Redness bull Redness bull Rednessprocess bull Suppuration bull Suppuration bull Suppuration bull Suppuration
bull Alveolar bone level is bull Alveolar bone level is bull Alveolar bone level is bull Same clinical signs asbull No alveolar 3 - 4 mm from CEJ 4 - 6 mm from CEJ bull gt 6 mm from CEJ advanced but includes
bone loss bull Radiographic bone loss bull Radiographic bone loss bull Radiographic bone loss adolescents orbull Localized or present present present young adults
generalized bull Localized or generalized bull Localized or generalized bull Localized or generalized bull Localized or generalizedbull Rapid cycles of disease
progression
Assessment bull Prophy bull Prophy bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150 bull Comp Oral Eval D0150bull OHI bull OHI bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180 bull Comp Perio Eval D0180
bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274 bull Four bitewings D0274bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277 bull Eight bitewings D0277bull FMX D0210 bull FMX D0210 bull FMX D0210 bull FMX D0210bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330 bull Panoramic Film D0330
bull Full Mouth Debride D4355 bull Full Mouth Debride D4355 bull Full Mouth Debride D4355bull Occlusal Analysis D9950 bull Occlusal Analysis D9950 bull Occlusal Analysis D9950
bull Specialty Referral bull Specialty Referral
Active bull Prophy bull Prophy bull Quadrant SRP D4341 bull Quadrant SRP D4341 bull Quadrant SRP D4341Therapy bull OHI bull OHI - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Specialty ReferralAntimicrobials Antimicrobials Antimicrobials
bull OHI D1330 bull OHI D1330 bull OHI D1330bull Specialty Referral bull Specialty Referral bull Specialty Referralbull Other Treatments bull Other Treatments bull Other Treatments
Ongoing 6 Months 6 Months bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910 bull Perio Maintenance D4910Maintenance bull Prophy bull Prophy - 346 months - 346 months - 346 months - 346 months
bull OHI bull OHI bull OHI D1330 bull OHI D1330 bull OHI D1330 bull OHI D1330bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381 bull Locally Administered D4381Antimicrobials Antimicrobials Antimicrobials Antimicrobials
bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342 bull Localized SRP D4342- UR UL LR LL - UR UL LR LL - UR UL LR LL - UR UL LR LL
bull Other Treatments bull Other Treatments bull Other Treatments bull Host Modulation
copyOraPharma Inc 2008aExcluding gingival overgrowth and recessionbBleeding upon probing may not be present in individuals with periodontal disease who are smokersc Tooth Mobility Grade I Slightly more than normal Grade II Moderately more than normal Grade III Severe mobility faciolingually and mesiodistally combined with vertical displacement Adaptedfrom Newman MG Takei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
d Furcation Grades Grade I Initial attachment loss with most of the bone still intact in the furcation No radiographic changes seen Grade II The bone defect is definite horizontal bone loss that doesnot extend all the way through Vertical bone loss may also be present There is an opening into the furca with a bony wall at the deepest portion Grade III Bone is lost across the whole width of thefurcation so no bone is attached to the furcation roof Grade IV Bone loss across the furcation accompanied with gingival recession at the furcation is clinically visible Adapted from Newman MGTakei H Klokkevold PR Carranza FA Carranzarsquos Clinical Periodontology 10th ed Philadelphia PA Elsevier 2006
eAdapted from Armitage GC Development of a classification system for periodontal diseases and conditions Ann Periodontol 1999 4(I)1-6
Adapted from Periodontal Diagnostic Guidelines copyOraPharma Inc 2008
Table 2 Periodontal Diagnostic Guidelines