Embed Size (px)
Citation preview

From Prep to Polypectomy: Improvements in Colorectal
Cancer Screening Colleen Schmitt, MD, MHS
President, Galen Medical Group
Past President, American Society for Gastrointestinal Endoscopy

Disclosures
• AmSurg Physician Advisory Board
• ABIM, Gastroenterology Specialty Board
• Stockholder, United Health Group, Alexion Pharmaceuticals, AmSurg, Steris, Quintiles
• Corporate Partner, AmSurg
• Board of Directors, GIQuIC Registry
• Board of Trustees, ASGE Foundation

Objectives
• To review the US Multi-Society Task Force 2017 recommendations for CRC screening
• To understand the role of colonoscopy quality metrics in prevention of CRC-related mortality, especially as related to adenoma detection rate
• To identify the split bowel preparation in high quality screening colonoscopy

Background
• CRC screening definition• The process of detecting early-stage CRCs and precancerous lesions in
asymptomatic people with no prior history of cancer or precancerous lesions--Average risk
• Surveillance• Interval use of colonoscopy in patients with previously detected CRC or
precancerous lesions or to detect dysplasia in patients with IBD
• Diagnostic examinations are done for the purpose of evaluating symptoms

Approaches to Screening
• Programmatic (organized) screening• systematic offers of screening, reduction of overscreening, superior
monitoring of quality, and systematic follow-up of testing
• Opportunitistic screening occurs with provider encounter
• U.S. has world’s highest rates of CRC screening (60%)
• U.S. has world’s greatest CRC incidence and mortality reduction• 3-4% per year decrease in incidence
• 30% overall reduction in mortality during 1st decade of this century
Siegel R , Desantis C , Jemal A . CA Cancer J Clin 2014 ; 64 : 104 – 17.Edwards BK , Noone AM , Mariotto AB et al.. Cancer 2014 ; 120 : 1290 – 314 .

Approaches to Screening
Approach Description
Multiple options The relative benefits, risks, and costs of 2 or more options are presented
Sequential testing A preferred test is offered first. If the patient declines then another option is offered.
Risk stratification Colonoscopy is offered to patients predicted to have a high prevalence of advanced precancerous lesions; other tests are offered to patients predicted at low risk.
• There is insufficient evidence to identify one approach as superior.• Patients should understand that colonoscopy is used to evaluate other tests when positive.• Insurance coverage of colonoscopy performed to evaluate other (+) tests may be less than coverage of
primary screening colonoscopy.

Screening Targets
Target Descriptors
Conventional adenomas Dysplasia gradeVillousity
Serrated lesions Sessile serrated polypTraditional serrated adenoma
Early CRC
70% CRC
30% CRC
Advanced adenoma: > 1 cm, HGD, villous elements
Advantage colonoscopy: SSP primarily in proximal colon, flat, few surface vessels

CRC Screening Methods
Method Advantages Disadvantages
Colonoscopy High sensitivity for cancer and all classes of precancerous lesionsSingle session dx and txLong interval between exams
Bowel cleansingRisks
Perforation 0.5/1000Bleeding 2.6/1000Death 2.9/1000
Operator dependence in performance
FIT Noninvasive1-time sensitivity for CRC 79%Fair sensitivity for advanced adenoma (30%)Low 1-time cost ($20)
Annual testPoor/no sensitivity for sessile serrated class
FIT-fecal DNA Noninvasive1-time sensitivity for CRC 92%
Decreased specificity (86%)Higher costs relative to FIT ($500 for MC)
Dex DK, et al. Am J Gastroenterol 2017;112:1016-1030

CRC Screening Methods (Cont.)
Method Advantages Disadvantages
CT Colonography Sensitivity 82-952% for adenoma > 1cm Bowel cleansingPoor performance for lesions < 1cm or SSPExtracolonic lesionsRadiation exposure
Flexible sigmoidoscopy
RCT confirms reduction in CRCLower costMore limited bowel preparationNo sedation
Lower benefit in preventing right-sided CRCLow patient satisfaction
Dex DK, et al. Am J Gastroenterol 2017;112:1016-1030

Quality in Screening Colonoscopy
• Is quality of the exam important?
• What are valid quality metrics in colonoscopy?
• What are the fundamentals of a high quality examination?
• What techniques improve overall quality of the examination?

Why We Should Care About Quality
• Effectiveness of the exam• Detection of cancer and reduce missed CRC rates• Detection of adenomas and serrated lesions• Effective resection of colorectal polyps
• Safety of the exam• Reduce complications• Appropriate screening and surveillance intervals
• Reimbursement• Episodes of care
• Patient centeredKaminski MF , Regula J , Kraszewska E et al. N Engl J Med 2010 ; 362 : 1795 – 803
Corley DA , Jensen CD , Marks AR et al. N Engl J Med 2014 ; 370 : 1298 – 306Abdeljawad K , Vemulapalli KC , Kahi CJ et al. Gastrointest Endosc 2015 ; 81 : 517 – 24 .

Key criteria for Quality Metric
• Evidence-based
• Interpretable
• Actionable
• Tied to key clinical outcome: Interval CRC
• Useful to stakeholders: patients, payers

Quality Determinants of Screening Colonoscopy
Adenoma Detection
• Complete procedure
• Adequate prep
• High quality examination technique
Effective Utilization
• Appropriate indication
• Appropriate screening and surveillance intervals
Rex DK, et al. Gastroenterol 2002;97:1296-308.ASGE Practice Guidelines Gastrointest Endosc 2006;58:S1-S38
Rex DK, et al. Gastrointest Endosc 2015;81:31-53.

Complete Examination: Getting to the Cecum
• USMSTF recommendation for cecal intubation >90% in all cases and >95% in screening cases
Rex DK, et al. Gastrointest Endosc 2015;81:31-53Baxter N, et al. Gastroenterology 2011;140:65-72.
Prove it with PhotoDocumentation

Complete Examination:Bowel Preparation• USMSTF recommends > 85% adequate
• Costs of Poor Bowel Preparation
• Reduced detection of polyps and cancer
• Aborted procedure
• Repeat procedure
• Increased risk for complications
• Lost co-pays and cost of transportation
• Lost days at work
• If not Adequate, then reschedule < 1 year

Play List for Your Colonoscopy Prep
• Take it Easy (The Eagles)
• The Waiting is the Hardest Part (Tom Waits)
• When the Levee Breaks (Memphis Minnie)
• Medley: Highway to Hell then Shook Me All Night Long (AC/DC)
• Ring of Fire
• Back in the Saddle Again
• Tush (ZZ Top)
• Hurts So Good (John Cougar Mellencamp)
• The End (The Doors)
• Friends in Low Places
• Moon River (Henry Mancini)
• Bad Moon Rising (Creedance Clearwater Revival)
• Rolling in the Deep (Adele)
• Pretty on the Inside (Hole)
• Shot in the Dark (Ozzy Ozbourne)
• Boogie in the Butt (Eddie Murphy)
• Way Down in the Hole (Tom Waits)
• Pants on the Ground (Larry Pratt)
• Everything Must Go (Manic Street)
• All Things Must Pass (George Harrison)
• Foggy Bottom Breakdown
• I Can See Clearly Now (Johnny Nash)
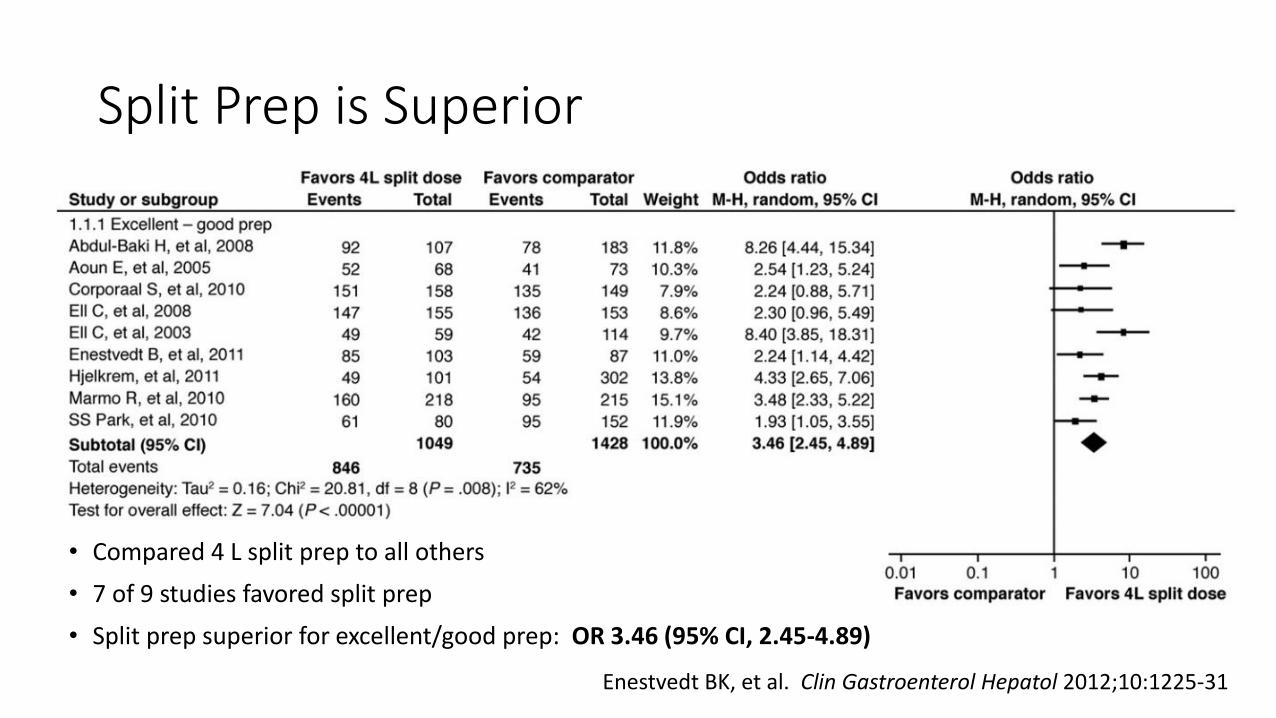
Split Prep is Superior
• Compared 4 L split prep to all others
• 7 of 9 studies favored split prep
• Split prep superior for excellent/good prep: OR 3.46 (95% CI, 2.45-4.89)
Enestvedt BK, et al. Clin Gastroenterol Hepatol 2012;10:1225-31
How to Split Prep
• Use split dose or same day prep
• Begin 2nd dose 4 to 6 hours prior to exam
• Finish prep at least 2 hours prior to exam
• Prep assessment after washing is complete
• Benchmark: Prep deemed adequate >85% cases
• If prep is deemed inadequate (fair, poor) the repeat exam within 1 year

Split Prep Results in Higher ADR
0
5
10
15
20
25
30
35
40
45
% with Adenoma % with Adenoma <10 mm
Chart Title
Split Prep Non-Split Prep
Cohen LB, et al. Aliment Pharmacol Ther 2010;32:637-44.

Complete Examination: Withdrawal Time
> 6 Minutes in (-) Screening
• Technique includes• Adequate distention
• Adequate washing up
• Careful examination behind folds
• Segmental inspection
WT and Interval CRC
ASGE Practice Guidelines Gastrointest Endosc 2006;58:S1-S38Shaukat A, et al. Gastroenterology 2015;149:952-7.

Surveillance Interval
• Surveillance interval correct in > 90% compliant after completing procedure and reviewing the pathology
• Average risk, no adenoma: 10 year
• 1 to 2 small adenomas: 5 years
• > 3 adenomas or adenoma > 10 mm: 3 years
• Piecemeal polypectomy: Depends…

Adenoma Detection Rate
Endoscopist ADRHazard Ration for Interval CRC
(95% CI)Unadjusted Risk
(no. of cases/10,000 person-yr)
7.35-19.05 % 1.00 (reference) 9.8
19.06-23.85 % 0.93 (0.70-1.23) 8.6
23.86-28.40 % 0.85 (0.68-1.06) 8.0
28.41-33.50 % 0.70 (0.54-0.91) 7.0
33.51-52.51 % 0.52 (0.39-0.69) 4.8
Each 1% increase in the ADR is associated with a 5% decrease in the risk of a fatal interval colorectal cancer.
Corley DA, et al. NEJM 2014;870:1298-306.

New Techniques to Improve ADR
• Participation in Registry
• Retroflexion in right colon
• Water immersion and exchange
• High definition white light
Pike I, et al. DDW, 2017Kushnir VM, et al. Am J Gastroenterol 2015;110:415-22.Cadoni S, et al. Endoscopy 2017;49:456-467.Subramanian V, et al. Endoscopy 2011;43:499-505.

New Technologies to Improve ADR

Emerging Technologies

SummaryRecommended Screening for CRC by USMSTF
Tier 1
• Colonoscopy every 10 years
• Annual FIT
Tier 2
• CT colonographyevery 5 years
• FIT-fecal DNA every 3 years
• Flex sig every 5 years
Tier 3
• Capsule colonoscopy every 5 years
Dex DK, et al. Am J Gastroenterol 2017;112:1016-1030

SummaryRecommended Screening for CRC by USMSTF• Average risk screening to begin at age 50 years in non-African Americans
and at 45 years for African Americans
• If up to date and prior screening is negative, consider cessation of screening at age 75 years or when life expectancy < 10 years
• If health allows, consider screening up until age 85 years if no prior screening
• 1st degree relative with CRC or documented advanced adenoma diagnosed <60 years or two 1st degree relatives with CRC and/or documented advanced adenoma – undergo colonoscopy at 5 year intervals beginning 10 years younger than age at which youngest relative was diagnosed, or age 40, whichever is earlier (offer annual FIT testing if decline colonoscopy)
Conclusions
• Split bowel preparation is currently the state-of-the-art approach
• Colonoscopy is the gold standard for CRC screening
• Effective CRC screening requires a commitment to the concept and to the quality of the examination