Embed Size (px)
Citation preview

From National Health IT to StateUniform Companion Guides
Realities and Opportunities to Make Standards Finally Work
Presented at the HIPAA COW 2008 Fall Conference
Sheboygan, WI – September 19, 2008
Walter G. Suarez, MD, MPHPresident and CEO - Institute for HIPAA/HIT Education and ResearchMember, National Committee on Vital and Health Statistics (NCVHS)
Member, Board of Directors, Health Information Technology Standards Panel (HITSP)

Outline
• Why are we here today?
• Core Health IT and HIE Concepts
• Business Case for NHIN and NHIEs
• A National Coordinated Agenda
• Where Things Stand Today
• Transitioning to State Realities: The Minnesota Statewide
Uniform Companion Guide Development Project
• Take away messages

Why are we here? Some Critical Health Needs and the National HIT Agenda
• Avoidance of medical errors– Up to 98,000 avoidable annual deaths due to medical errors
• Improvement of resource utilization– Up to $300B spent annually on treatments with no health yield
• Acceleration of knowledge diffusion– 17 years for evidence to be integrated into practice
• Reduction of variability in healthcare delivery and access– Access to specialty care highly dependent on geography
• Empowerment of the consumer– Capitalize on growing consumer trend of active health management
• Strengthening of data privacy and protection– HIPAA becomes reality
• Promotion of public health and preparedness– Surveillance is fragmented, and importance to homeland security brings heightened
awareness

Core Concepts

Health IT and HIE - Leading Transformation Factors
• Electronic Health Records
• Personal Health Records
• Interoperable Standards
• Health Information Infrastructure
• Population Health Infrastructure
• Robust Security and Privacy
And…
• A business reason that supports doing all this!

What is “Interoperability”?
“The ability of different information technology
systems and software applications to
communicate, to exchange data accurately,
effectively and consistently, and to use the
information that has been exchanged.”
Source: National Alliance for Health Information Technology, July 2005; “Consensus
Conventions for the Use of Key HIT Terms” Project – ONC/HHS, 2008

“Record” Terms
Source: National Alliance for Health Information Technology, Report to the Office of the National Coordinator for Health Information Technology – Defining Key Health Information Technology Terms, April 28, 2008

“Network” Terms
Source: National Alliance for Health Information Technology, Report to the Office of the National Coordinator for Health Information Technology – Defining Key Health Information Technology Terms, April 28, 2008

RHIO and HIE – Distinguishing and Common Characteristics
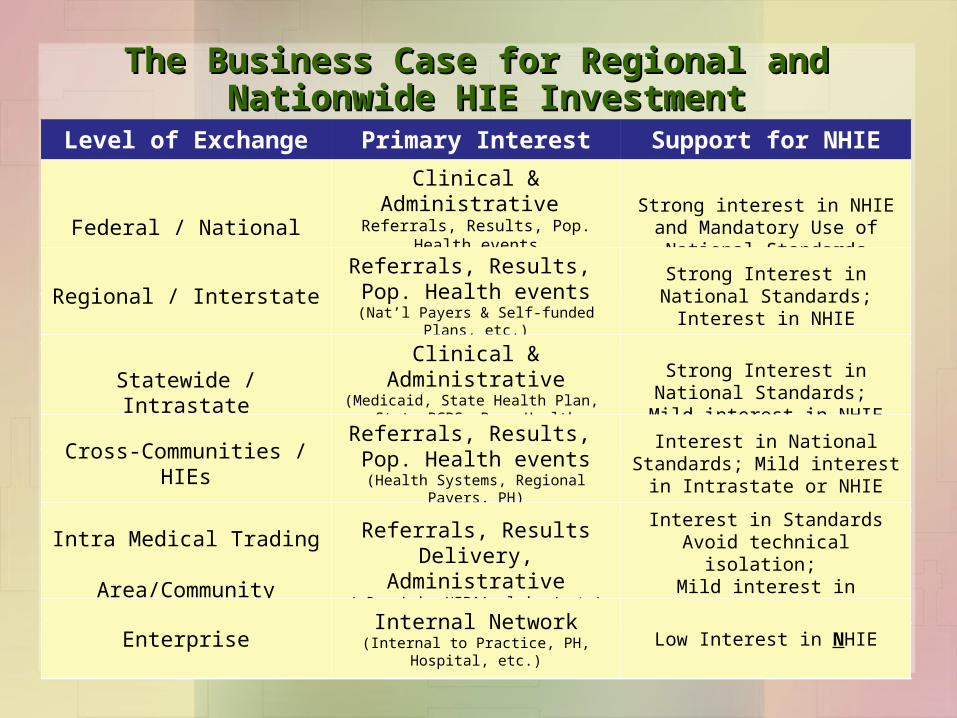
The Business Case for Regional and The Business Case for Regional and Nationwide HIE InvestmentNationwide HIE Investment
Level of Exchange Primary Interest Support for NHIE
Federal / NationalClinical & Administrative Referrals, Results, Pop. Health
events(Medicare, MHS/VA/IHS/SSA etc.)
Strong interest in NHIE and Mandatory Use of National
Standards
Regional / InterstateReferrals, Results, Pop. Health events
(Nat’l Payers & Self-funded Plans, etc.)
Strong Interest in National Standards;
Interest in NHIE
Statewide / IntrastateClinical & Administrative(Medicaid, State Health Plan, State
BCBS, Pop. Health awareness)
Strong Interest in National Standards;
Mild interest in NHIE
Cross-Communities / HIEsReferrals, Results, Pop. Health events
(Health Systems, Regional Payers, PH)
Interest in National Standards; Mild interest in Intrastate or
NHIE
Intra Medical Trading Area/Community
Referrals, Results Delivery, Administrative
(eRx, Lab, HIPAA claims/pmts)
Interest in StandardsAvoid technical isolation;
Mild interest in Intrastate / NHIE
Enterprise Internal Network(Internal to Practice, PH, Hospital, etc.)
Low Interest in NHIE

The National Health IT Strategy

Federal Government Collaborations Among Health IT Initiatives

ONC-Coordinated Federal Health IT Strategic Plan 2008-2012

ONC Health IT Strategic Plan (2008-2012)

National HIT Agenda and Health Information Exchange
PrioritiesPriorities• American Health Information
Community (AHIC)• Business needs and priorities• Use Cases
PrioritiesPriorities• American Health Information
Community (AHIC)• Business needs and priorities• Use Cases
StandardsStandards• Healthcare Information
Technology Standards Panel (HITSP)
• Recognized standards
StandardsStandards• Healthcare Information
Technology Standards Panel (HITSP)
• Recognized standards
NetworkingNetworking• NHIN - network of
networks• Architecture
specifications
NetworkingNetworking• NHIN - network of
networks• Architecture
specifications
PoliciesPolicies• State laws and regulations –• State Alliance for e-Health• State-level Health Information
Exchange• Health Information Security and
Policy Collaboration (HISPC)
PoliciesPolicies• State laws and regulations –• State Alliance for e-Health• State-level Health Information
Exchange• Health Information Security and
Policy Collaboration (HISPC)
CertificationCertification• Certification Commission For
Healthcare Information (CCHIT) Technology
• Criteria development• Testing
CertificationCertification• Certification Commission For
Healthcare Information (CCHIT) Technology
• Criteria development• Testing
AgendaAgenda

• Recommendations to Secretary on overall policy
directions related to Health IT
• Definition of priority areas (breakthroughs)
• Development of Use Cases for harmonization of
standards
• Transitioning to AHIC 2.0
Setting Priorities - AHIC
http://www.ahicsuccessor.org

Networking – NHIN and the NHIEs
• NHIN: the nationwide “Network of Networks”… of Networks– Framework for health information
network service providers
– Interconnecting NHIEs
– Business/Technical Issues: Standards, Sustainability, Security
• NHIEs: Local, state, regional HIEs interoperable with NHIN
http://www.hhs.gov/healthit/healthnetwork/background/

Networking – NHIN and the NHIEs
• Phase 1 (2007) – Prototyping – 4 Consortia
– Core elements of NHIN
• Phase 2 (2008) – Trial Implementations– 15+ sites
– Develop the NHIN HIE Specs
• Phase 3 (2009) - TBD
http://www.hhs.gov/healthit/healthnetwork/background/


Where are States with respect to HIEs?
Sources: Health Information Security and Privacy Collaborative (HISPC); State-level Health Information Exchange (SLHIE); January, 2008

Policies - HISPC• Phase 1 (2006-2007)
– 34 Teams (33 State, Puerto Rico) – 1) Assessments of privacy/security
variations; 2) Analysis of solutions; 3) Develop implementation plans
• Phase 2 (July-Dec 2007) – Each team to implement a
foundational component of their implementation plans
• Phase 3 (2008-2009)– 7 Multistate Collaboratives
developing common, replicable multistate solutions
http://healthit.ahrq.gov/privacyandsecurity

Policies – State-level HIE
http://www.staterhio.org
• Funded by ONC
• Develop reports and tools:– State-level HIE Development Workbook– RHIO Governance roles– Consensus model HIE policies

Policies – State Alliance for eHealth
http://www.nga.org
• National Governors Association’s initiative supported by ONC• Initial work (2006/2007) done through 3 Taskforces:
– Health Information Protection– Health Care Practices– Health Information
Communications and Data Exchange
• Reconfigured Taskforces to focus on:– Privacy and Security– Public Programs Implementation
• Taskforce reports provide severalrecommendations to states on privacy, security, Public program (i.e. Medicaid) roles in HIEs, need for harmonizing cross-state regulations on medical practice

Standards – The Health Information Technology Standards Panel (HITSP)



27HITSP: Enabling interoperability across the health care enterprise
HITSP Information Resources
Please take a copy of the introductory CD-ROM
available at this kiosk or visit our website (www.hitsp.org)
for a downloadable copy of the
CD’s content
Also available on www.hitsp.org
– News, organizational details and information on
upcoming meetings
– HITSP Public Document Library
– Interoperability Specifications (ISs)
and Executive Summaries
– Use Cases
– HITSP Webinars (Free!)
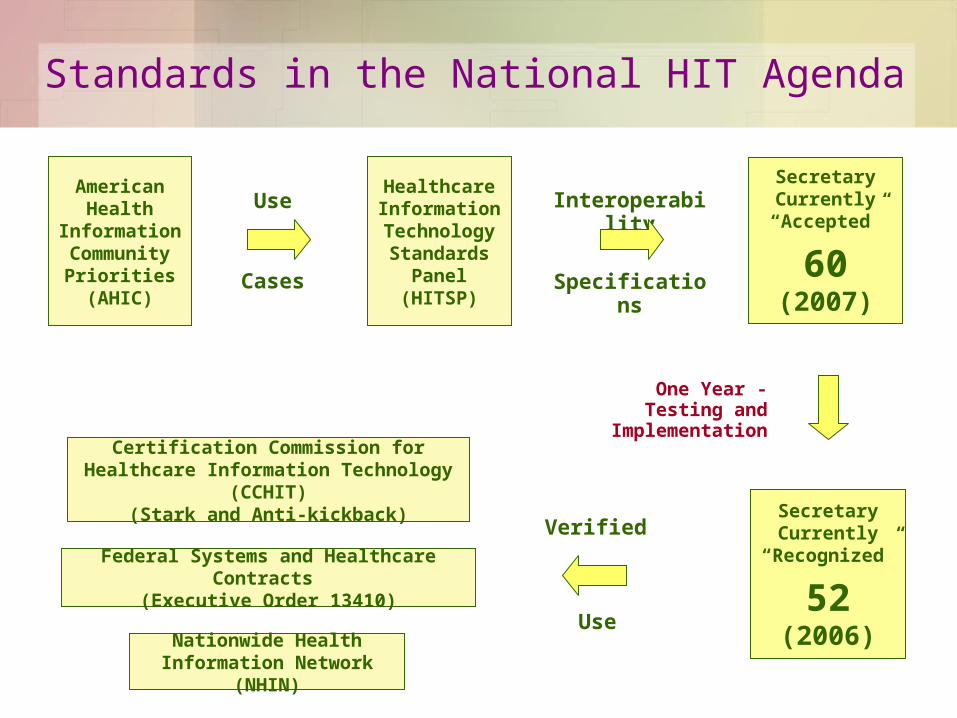
Standards in the National HIT Agenda
American Health
Information Community
Priorities(AHIC)
Healthcare Information Technology Standards
Panel(HITSP)
Nationwide Health Information Network (NHIN)
Certification Commission for Healthcare Information Technology (CCHIT)
(Stark and Anti-kickback)
Use
Cases
Interoperability
Specifications
Federal Systems and Healthcare Contracts (Executive Order 13410)
SecretaryCurrently
“Accepted”
60(2007)
SecretaryCurrently
“Recognized”
52(2006)
One Year -Testing and
Implementation
Verified
Use

Certification – The Certification Commission for Health Information Technology (CCHIT)
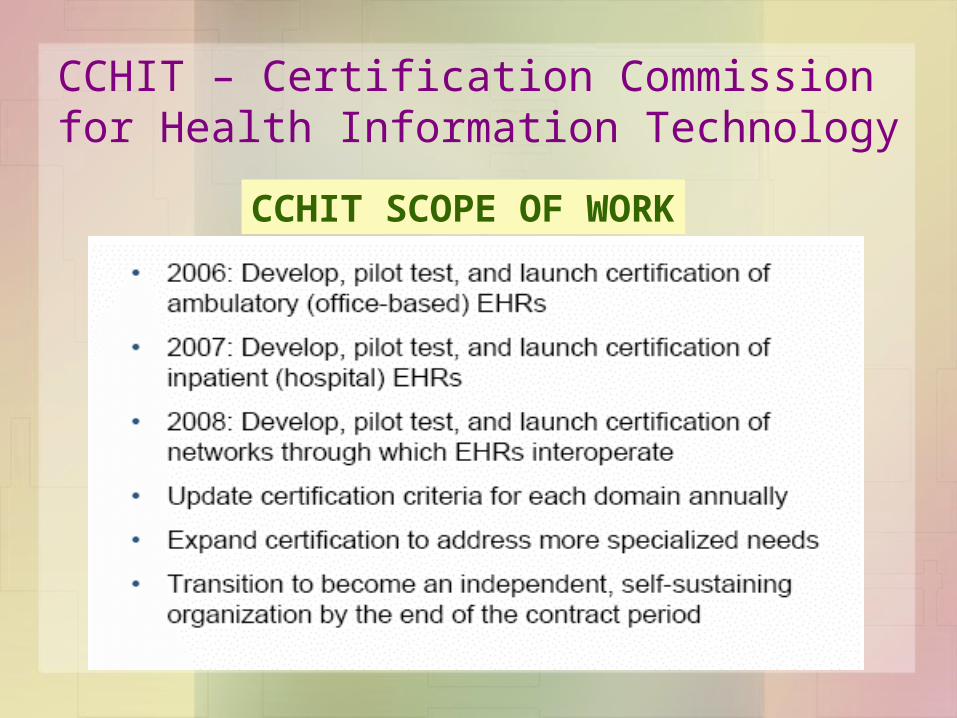
CCHIT – Certification Commission for Health Information Technology
CCHIT SCOPE OF WORK

CCHIT – Certification Commission for Health Information Technology
• Results to-date:
– A total of nine inpatient EHR products have been certified,
representing 36% of the inpatient EHR vendors in the market
• Four additional inpatient EHR product applications were received
recently, bringing total to 50% of the inpatient EHR vendor market
– Over 60 ambulatory EHR products representing more than 35%
of the outpatient EHR vendors in the market
• 14 additional ambulatory EHR product applications recently
received, bringing total to close to 50% of the inpatient EHR
– Moving into specialty areas (i.e., cardiovascular, child health),
network services

NHIN – Completing the Cycle

Transitioning to State Realities: The Minnesota Statewide Uniform
Companion Guide Development Project

• In 2007 the MN Legislature passed a law amending the “MN Health Care Administrative Simplification Act of 1994” (MN Statutes §62J.50 -§62J.61) and requiring the development, adoption and use of state uniform companion guides
• Part of Minnesota’s commitment to the increased use of health IT for both administrative and clinical activities
• Initial set of transactions subject to the new law includes Claims (837P, 837I, 837D, NCPDP), Claim Payment (835), and Eligibility (270/271)
• State law covers all health care providers and group purchasers (health plans, Medicaid, employers and others) doing business in the state; the law requires them to conduct these transactions electronically and use the standard companion guides
Background

• Commissioner of Health, in consultation with the MN
Administrative Uniformity Committee, is charged with
developing state uniform companion guides
• Companion guides are to be based on billing and coding
rules from the Medicare program, but can depart from them
based on state health care industry’s consensus
• Companion guides will be required to be used, along with
the HIPAA Implementation Guides, when conducting any of
the transactions they cover
Background

Summary of State Law
The Minnesota Uniform Companion Guide Development Project

• Part 1 - Requirements for all health care providers and group purchasers to implement uniform electronic transactions
– All group purchasers and health care providers in MN must exchange claims and eligibility information electronically, using the transaction standards prescribed by HIPAA and the companion guides and timelines established by the state law
– Group purchasers may not impose any fee on providers for the use of the transactions prescribed in this legislation
– Direct data entry, web-based methodology allowed, so long as it is consistent with data content component of HIPAA implementation guides and MN uniform companion guides
Summary of State Law(MN Statutes § 62J.536)

• By January 15, 2009, ALL health care providers and group purchasers
in MN must submit/accept the HIPAA electronic eligibility transaction
(270/271)
• By July 15, 2009, ALL health care providers and group purchasers in
MN must submit/accept the HIPAA electronic health care
claim/encounter information transaction prescribed by HIPAA (837s,
NCPDP)
• By December 15, 2009, ALL health care providers and group
purchasers in MN must submit/accept the electronic health care
payment/RA transaction prescribed by HIPAA (835)
Summary of State Law(MN Statutes § 62J.536)

• Part 2 - Requirement for the development and use of single, uniform, statewide companion guides for the identified transactions:
– Each named transaction must use a single, uniform companion guide to the HIPAA implementation guides statewide
– Companion guides to be developed as follows:
• Commissioner of Health, in consultation with MN-ACU develops companion guides at least 12 months prior to the timelines required for transaction
• Commissioner of Health issues a Notice of Proposed Rulemaking requesting industry comments on ‘draft’ companion guides
• Commissioner of Health promulgates rules establishing and requiring group purchasers and health care providers in MN to use the uniform companion guides
Summary of State Law(MN Statutes § 62J.536)

• No group purchaser or health care provider may add or modify the companion guides through their own companion guides or other requirements
• Commissioner shall not require data content that is not essential to accomplishing the purpose of the transaction
• Health care providers also includes dentists, chiropractors, nursing homes, boarding care homes and home care providers
• Other ‘group purchasers’ subject to law includes Workers Compensation and medical component of Auto Insurance
Summary of State Law(MN Statutes § 62J.536)
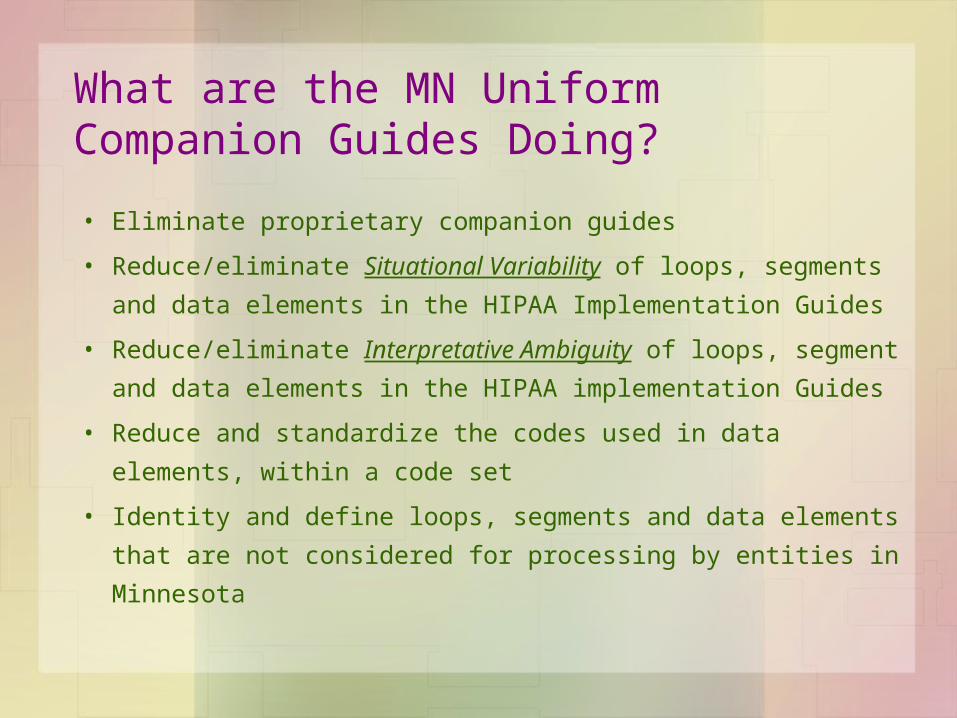
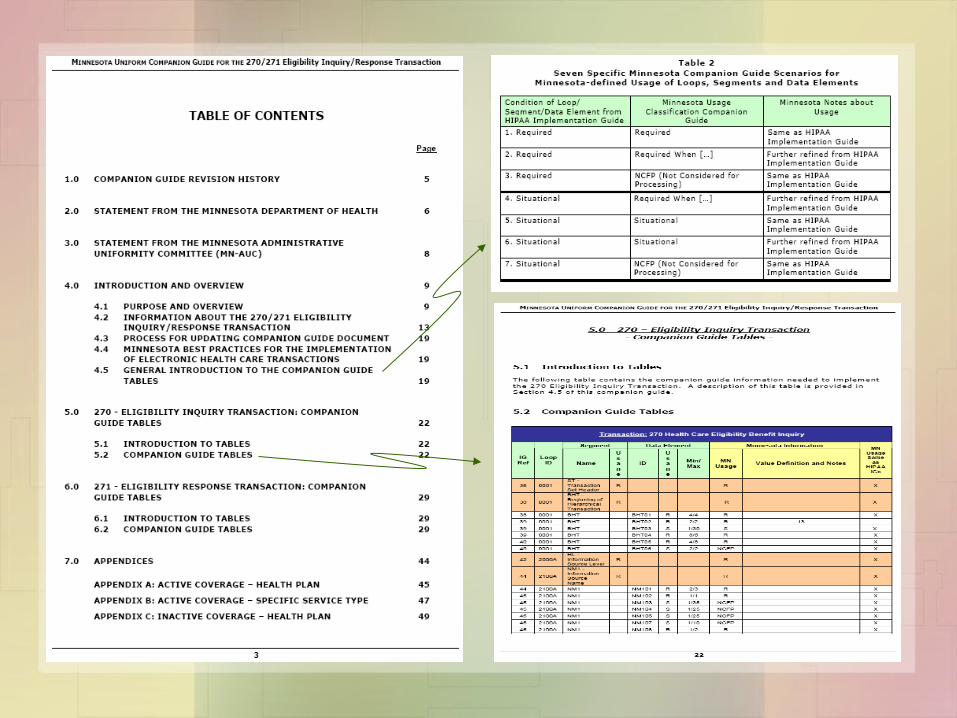
• Eliminate proprietary companion guides
• Reduce/eliminate Situational Variability of loops, segments
and data elements in the HIPAA Implementation Guides
• Reduce/eliminate Interpretative Ambiguity of loops, segment
and data elements in the HIPAA implementation Guides
• Reduce and standardize the codes used in data elements,
within a code set
• Identity and define loops, segments and data elements that
are not considered for processing by entities in Minnesota
What are the MN Uniform Companion Guides Doing?
• Replace HIPAA IGs
• Make implementation inconsistent and incompatible with, or in
violation of the HIPAA Implementation Guides– What is Required by HIPAA IG is Required by MN CG
– What is Not Used in HIPAA IG is Not Used in MN CG
– What is Situational in HIPAA IG is further defined in MN CG
• Disclaimer from the Guide: “… the [companion guide] supplements, but
does not contradict, disagree, oppose, or otherwise modify the HIPAA
Implementation Guide in a manner that will make its implementation by
users to be out of compliance.”
What the MN Uniform Companion Guides are NOT Doing?

• Multiplicity of companion guides and payer-specific requirements
• Providers need to customize transactions on a payer-by-payer basis
• Inconsistencies in transaction requirements significantly increases administrative burden
• Quality of care delivered to consumers is being affected
Why is this Project Important?

Understanding Companion Guides
The Minnesota Uniform Companion Guide Development Project

• A Companion Guide is a document that clarifies,
supplements and further defines specific data content
requirements contained in the Implementation Guides
established for each of the HIPAA transactions
• Generally, companion guides cover four core areas:– Define transaction instructions (EDI information) between trading
partners
– Further define requirement of loops, segments, data elements
– Further define data element content
– Further define data coding used in transaction
What are Companion Guides?

While there is ONE HIPAA Implementation Guide, there are 1000s of companion guides developed by each payer in the market….
1000s of Companion Guides…

Process for DevelopingMN Uniform Companion Guides
The Minnesota Uniform Companion Guide Development Project

• Use MN-AUC Committee and Workgroup Structure
• Establish Companion Guide Development Teams
• Develop Principles and Guidance Document
• Develop Consensus Building Approach and Decision
Making Process Document
• Develop Standard Master Template Companion Guide
Document
• Establish Project Workplan and Timeline
Process for Developing MN Uniform Companion Guides

• Draft of Companion Guide is prepared
• Notice proposing adoption published - 30-day comment period
• Comments are addressed, changes made to guide
• Notice adopting guide is published
• A one-year period of transition for compliance starts
• Six-month into process, technical review is done– Revisions to adopted companion guide are published for public comments
– Notice adopting final revised companion guide for compliance is published
• Compliance starts
• Annual review and update…
Cycle for Companion Guide Development
www.health.state.mn.us/auc



Minnesota Department of HealthMinnesota Administrative Uniformity Committee
MN Companion Guide Project Plan Last Update:January, 2008
Major Milestones/Task Timelines2007-2008
All Companion Guides
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar13 23 01 08 15 22 29 11 18 25 01 08 15 22 29 05 12 19 26 03 10 17 24 31 07 14 21 28 05 12 19 26 02 09 16 23 30 06 13 22 29 05 12 19 26 31
270
/27
12
70
/27
1N
CP
DP
NC
PD
P8
37
D8
37
D8
37
I/83
7P
837
I/83
7P
835
835
Phase I
Pro
jP
roj
Mg
tM
gt Phase II
Develop Principles/Guidance/Templates
Est
ablis
h W
orkg
roup
CollectBaseInfo
CreateTable
Review/Discuss, Reach Consensus
Identify Parking Lot
Issues
Address Parking Lot Issues
Create/Review CG Doc
MergeTable and CG, add
Appendices
SendCG to AUC Ops
Notice Published;Comments due
10/30
CG Group meets to review comments,
update CG as needed
SendCG to AUC Ops
Notice of AdoptionPublished
12/10
Effective Date of Notice:30 days
post publication
Deadline for Implementation of CG by industry: 01/15/2009
Est
ablis
h W
orkg
roup
Collect Base Info
Create Tables
Review/Discuss, Reach Consensus
Firs
t Mee
ting
Identify Parking Lot Issues
Address Parking Lot Issues
Create CG Docs
MergeTables and CGs, add
AppendicesReview Front Matter
SenddraftCGs
to AUC Ops
Complete Drafting and Review of
CGs
Notice (30-day Public Comment)Published
3/31
Companion Guide (CG) DevelopmentE
stab
lish
Wor
kgro
up
Collect Base Info
Create Table
Review/Discuss, Reach Consensus
Firs
t Mee
ting
Identify Parking Lot Issues
Address Parking Lot Issues
Create CG Doc
MergeTable and CG,
add Appendices
Review Front Matter
SenddraftCG to AUC Ops
Complete Drafting and Review of CG
Notice (30-day Public Comment)Published
3/31Coordinate Parking
Lot Issues with 837P/837I Group
Est
ablis
h W
orkg
roup
Collect Base Info
Create Tables
Review/Discuss, Reach Consensus (Round 1)
Identify Parking Lot Issues
Create CG Docs
Form “Parking
Lot Issues Groups”(100 to
500 Work Groups)
Review/Discuss, Reach Consensus (Round 2)
MergeTables and CGs, add Appendices
Complete 100-500 Review Process
Address Parking Lot Issues from 837D
Address Coding Issues
Senddraft
CG to AUC Ops
Notice (30-day Public Comment)Published
3/31
Address Coding Issues
Review CG Front Matter
EO
B W
orkg
roup
E
stab
lishe
d
Collect Base Info Create Tables Review/Discuss, Reach Consensus (Round 1)
Identify, Discuss, Address Parking Lot Issues
Identify, Discuss, Address Coding Issues
Create CG Doc Review/Discuss CG Front Matter
MergeTable and CG
create/add Appendices
2 0 0 7 2 0 0 8
Complete the development of CGs, and Code set Appendices

Minnesota Department of HealthMinnesota Administrative Uniformity Committee
MN Companion Guide Project Plan Last Update:October 15, 2007
Major Milestones/Task Timelines2007-2008
All Companion Guides
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul 01 07 14 21 28 05 12 19 26 02 09 16 23 01 07 14 21 28
270
/27
12
70
/27
1N
CP
DP
NC
PD
P8
37
D8
37
D8
37
I/83
7P
837
I/83
7P
835
835
Pro
jP
roj
Mg
tM
gt Phase II
Deadline for Implementation
of CG by industry:
01/15/2009
Sub
mis
sion
to
AU
C O
psPhase III
Industry Transition, Guide Refinement
Industry Preparedness and Transition
Process for Identification, Review and Adoption of Technical Corrections
CG Periodic
Maintenance
AUC CG Group review comments and update CGs
as needed MD
H R
evie
w -
P
ublis
h N
otic
e of
A
dopt
ion
Deadline for Implementation
of CG by industry:
07/15/2009
Industry Preparedness and Transition
Process for Identification, Review and Adoption of Technical Corrections
Deadline for Implementation
of CG by industry:
07/15/2009
Industry Preparedness and Transition
Process for Identification, Review and Adoption of Technical Corrections
Deadline for Implementation
of CG by industry:
07/15/2009
Industry Preparedness and Transition
Process for Identification, Review and Adoption of Technical Corrections
2 0 0 8 2 0 0 9
Senddraft
CG to AUC Ops
Modify CG as
NeededFrom
AUC Ops Input
Sendfinal
CG to AUC Ops
Notice (30-day Public Comment)Published
7/15
Complete Drafting and Review of CG
Public Comment Period
Sub
mis
sion
to
AU
C O
ps
AUC CG Group review comments and update CGs
as needed MD
H R
evie
w -
P
ublis
h N
otic
e of
A
dopt
ion
Public Comment Period
Sub
mis
sion
to
AU
C O
ps
AUC CG Group review comments and update CGs
as needed MD
H R
evie
w -
P
ublis
h N
otic
e of
A
dopt
ion
Public Comment Period
Sub
mis
sion
to
AU
C O
ps
AUC CG Group review comments and update CG as
needed MD
H R
evie
w -
P
ublis
h N
otic
e of
A
dopt
ion
Public Comment Period
Industry Preparedness and Transition
Process for Identification,
Review/Adoption of Technical Corrections
Deadline for Implementation
of CG by industry:
12/01/2009

• Eligibility (270/271) Companion Guide:
– Completed and adopted by state - December 10, 2007
– Technical revision completed in May 15, 2007
– Implementation date: January 15, 2009 (early voluntary adoption permitted)
• Claim (837P/I/D, NCPDP) Companion Guides:
– Completed and published for comment in March, 2008
– Published notice adopting companion guides in June, 2008
– Technical changes expected to be completed in March, 2009
– Implementation date: July 15, 2009 (early voluntary adoption permitted)
• Claim Payment/RA (835) Companion Guide:
– Under development – expected completion and publication for comment: June, 2008
– Published a Notice of Proposal to Adopt in July, 2008 – Comment Period ended August, 2008
– Currently reviewing and addressing comments, revising companion guide
– Notice adopting final companion guide expected to be published October, 2008
– Six-month technical amendment in April, 2009
– Implementation date: December 1, 2009
• All final guides will be available from the MN AUC website (www.health.state.mn.us/auc)
Status of Project Deliverables

Take Away Message….
So, why is all this important to me?
• National and local initiatives are affecting how you do business in health
care
– Increased dependency on electronic health information, connectivity and
interoperability
• HIPAA still a very important implementation issue
– Upcoming Claim Attachments, 5010, NCPDP D.0 and ICD10 standards
• Industry moving into the adoption and use of clinical information exchanges
– Electronic health records, lab information systems, e-Prescribing
• New and emerging areas in health information
– Personal Health Records – will they become mainstream?
– Clinical decision support systems – increasing dependency on standard, codified
electronic health information

So, why is all this important to me?
• Informed consumers with shifting expectations– Bringing better and more relevant health information to the fingertips of
consumers and improving efficiency of consumer controls over their health information
– Consumers bringing higher expectations on a practice’s ability to maintain and exchange their health information securely and efficiently
– Can my Doctor and I communicate electronically via email and web services?
• Alignment of incentives to adopt health IT– NOW: Pay for Performance – including the adoption of health IT
components such as CPOE
– NEXT: Pay for Conformance – including adopting interoperable, certified health IT products and networks

Thank You
Walter G. Suarez, MD, MPHPresident and CEO
Institute for HIPAA/HIT Education and Research
Alexandria, VAPhone: (952) 221-3841
Email: [email protected]





























