Embed Size (px)
Citation preview
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Sharing knowledge. Sharing hope.
Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MDFebruary 2013
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Disclosures
Janet Brunner, PA-C• I have no relevant conflicts of interest to disclose.
Angela Dispenzieri, MD• I have no relevant conflicts of interest to disclose.
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Objectives:
1) Understand why the Myeloma & Amyloid Forms were combined into one
2) Complete the revised Pre/Post-HCT Plasma Cell Disorder (PCD) forms accurately

CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Plasma Cell Disorder (PCD)-Pre-HCT Data
Form 2016
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Subsequent HCT
Additional options have been added:• Same disease subtype, but without a prior disease
insert completed (begin with Q1)
• Same disease subtype, but there has been a relapse or progression (begin with Q188- Was therapy given?)
• Same disease (begin with Q233)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Plasma Cell Disorders (PCD)
• Additional sub-types have been added• Osteosclerotic myeloma / POEMS syndrome• Light chain deposition disease (LCDD)
• Question about preceding / concurrent PCD• Multiple myeloma (symptomatic)• Smoldering myeloma (asymptomatic)• Monoclonal gammopathy of unknown significance
(MGUS)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
How to report Myeloma and Amyloidosis
• Scenario 1• Patient has smoldering myeloma (asymptomatic) &
amyloidosis. • Report amyloidosis as the primary diagnosis for HCT
(question 1). • Report smoldering myeloma as a concurrent diagnosis
(question 6)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
How to report Myeloma & Amyloidosis
• Scenario 2• Patient has symptomatic myeloma & amyloidosis• Report symptomatic myeloma as the primary
diagnosis for HCT (question 1)• Report amyloidosis as a concurrent diagnosis
(question 6)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
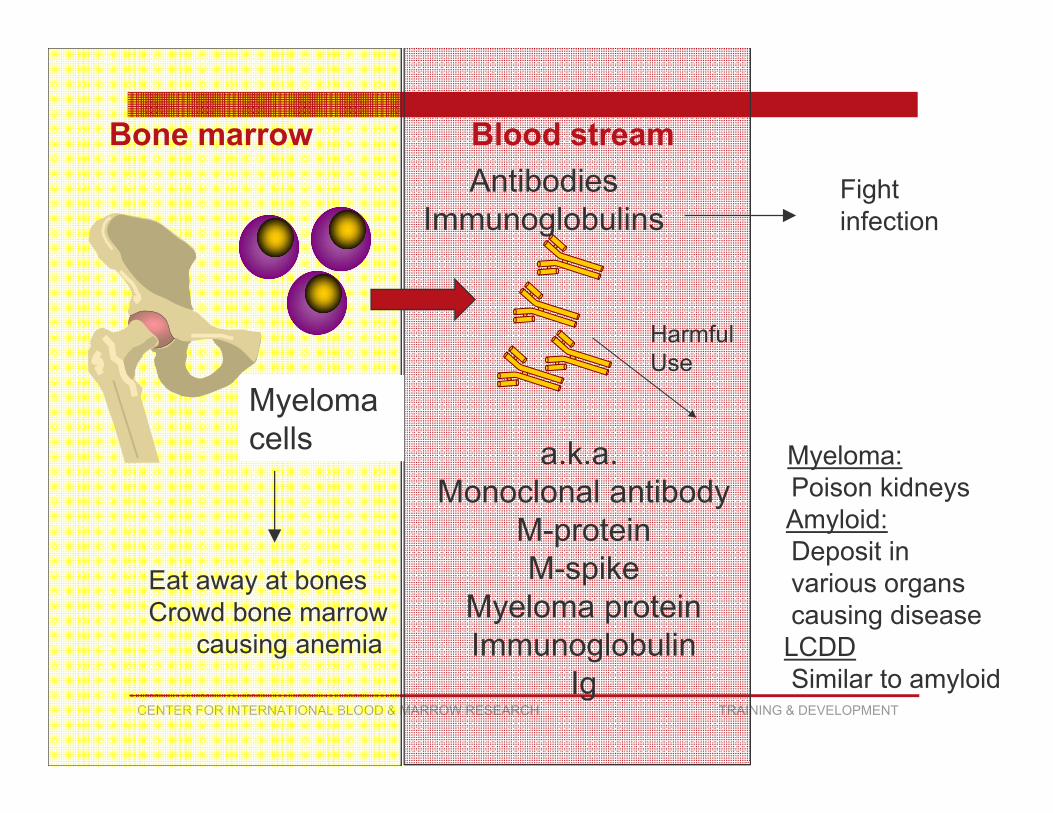
AntibodiesImmunoglobulins
Plasma cells
Bone marrowFight infection
a.k.a. Monoclonal antibody
M-proteinM-spike
Myeloma proteinImmunoglobulin
Ig
HarmfulUse
Myeloma:Poison kidneysAmyloid:Deposit in various organscausing disease
LCDDSimilar to amyloid
Eat away at bonesCrowd bone marrow
causing anemia
Myeloma cells
Blood stream
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
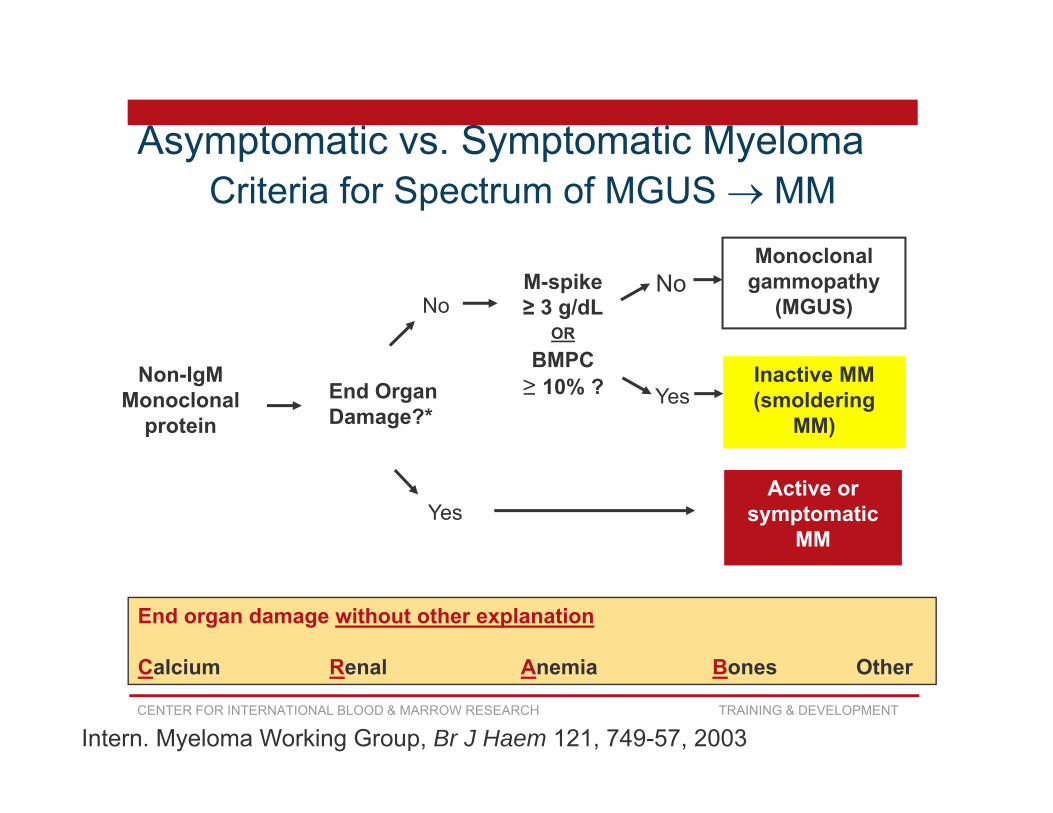
Criteria for Spectrum of MGUS MM
End Organ Damage?*
Non-IgMMonoclonal
protein
End organ damage without other explanation
Calcium Renal Anemia Bones Other
M-spike ≥ 3 g/dL
OR
BMPC ≥ 10% ?
No
Active or symptomatic
MMYes
Monoclonal gammopathy
(MGUS)No
Inactive MM (smoldering
MM)Yes
Intern. Myeloma Working Group, Br J Haem 121, 749-57, 2003
Asymptomatic vs. Symptomatic Myeloma
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
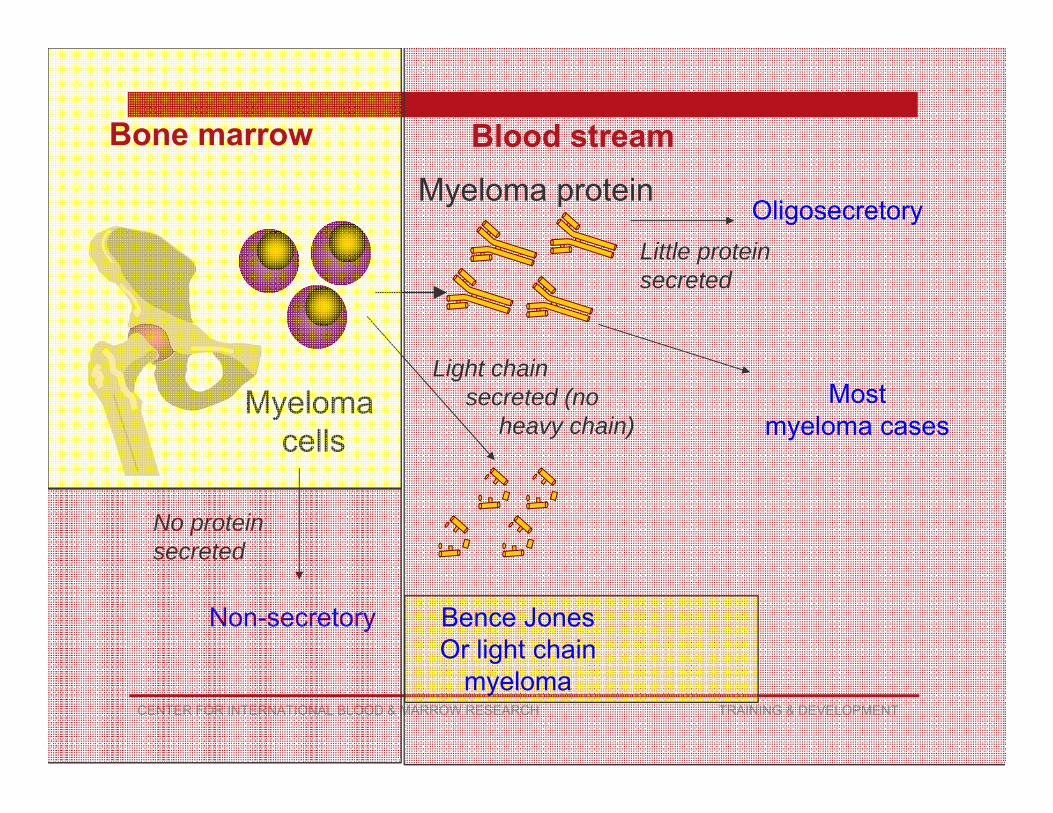
Myeloma protein
Myeloma cells
No protein secreted
Non-secretory
OligosecretoryLittle protein secreted
Bence JonesOr light chain
myeloma
Light chain secreted (no
heavy chain)Most
myeloma cases
Bone marrow Blood stream
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Light chain only myeloma vs. LCDD
Light chain deposition disease (LCDD) is actually very similar to amyloidosis except looks slightly different under microscope
Light chain only myeloma is merely a type of MM (no heavy chain). It may cause light chain cast nephropathy (renal failure)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
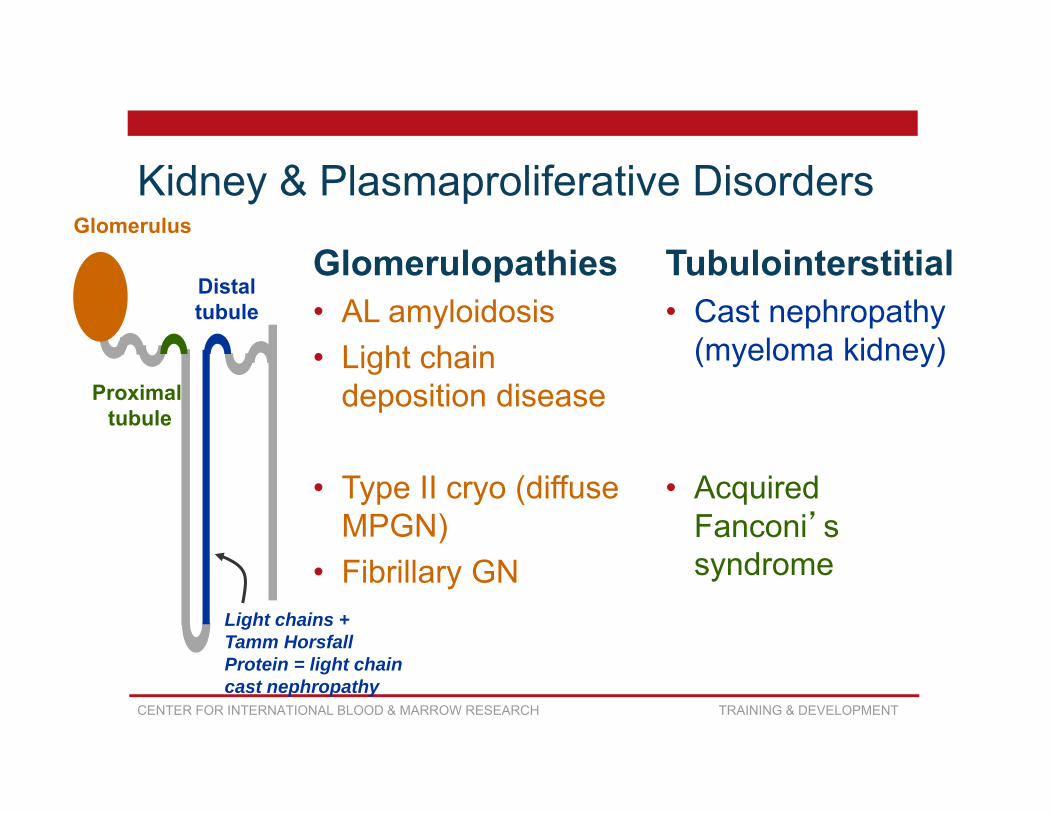
Kidney & Plasmaproliferative Disorders
Glomerulopathies• AL amyloidosis• Light chain
deposition disease
• Type II cryo (diffuse MPGN)
• Fibrillary GN
Tubulointerstitial• Cast nephropathy
(myeloma kidney)
• Acquired Fanconi’s syndrome
Glomerulus
Proximal tubule
Distaltubule
Light chains +Tamm HorsfallProtein = light chain cast nephropathy
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
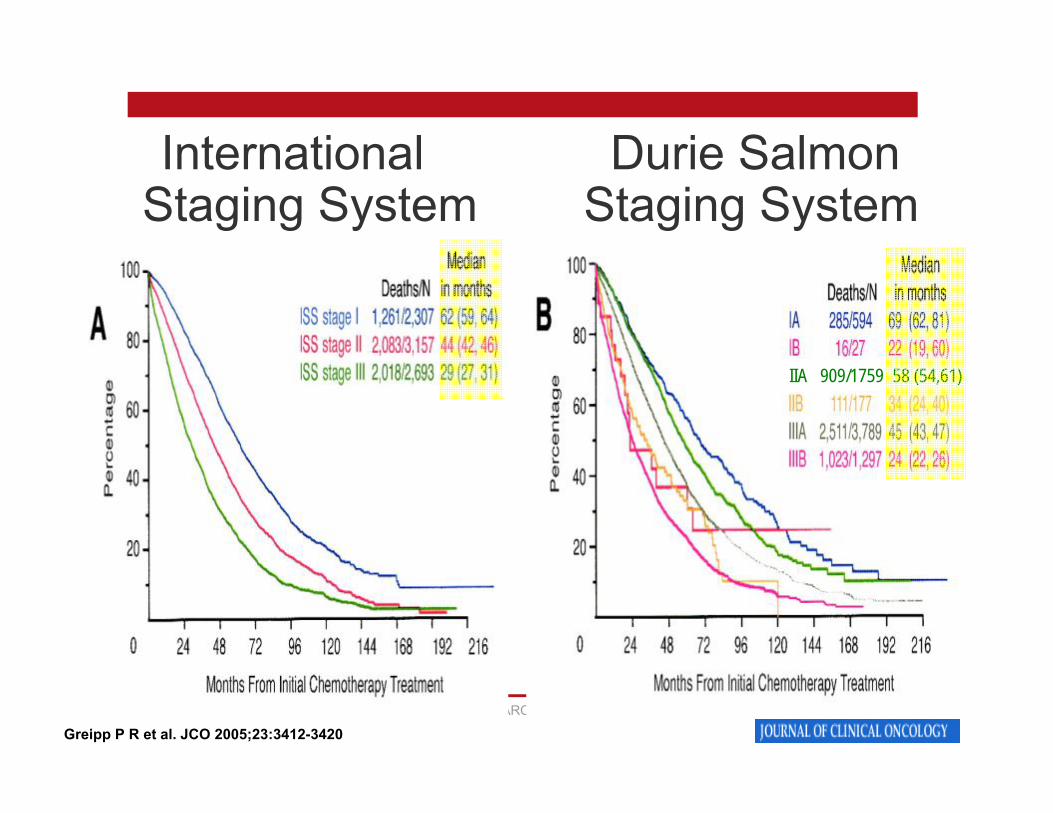
Staging of Myeloma
• Durie-Salmon Staging• Requires hemoglobin, serum calcium, monoclonal
protein & bone survey findings
• International Staging System (ISS)• Requires β2 microglobulin & albumin
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
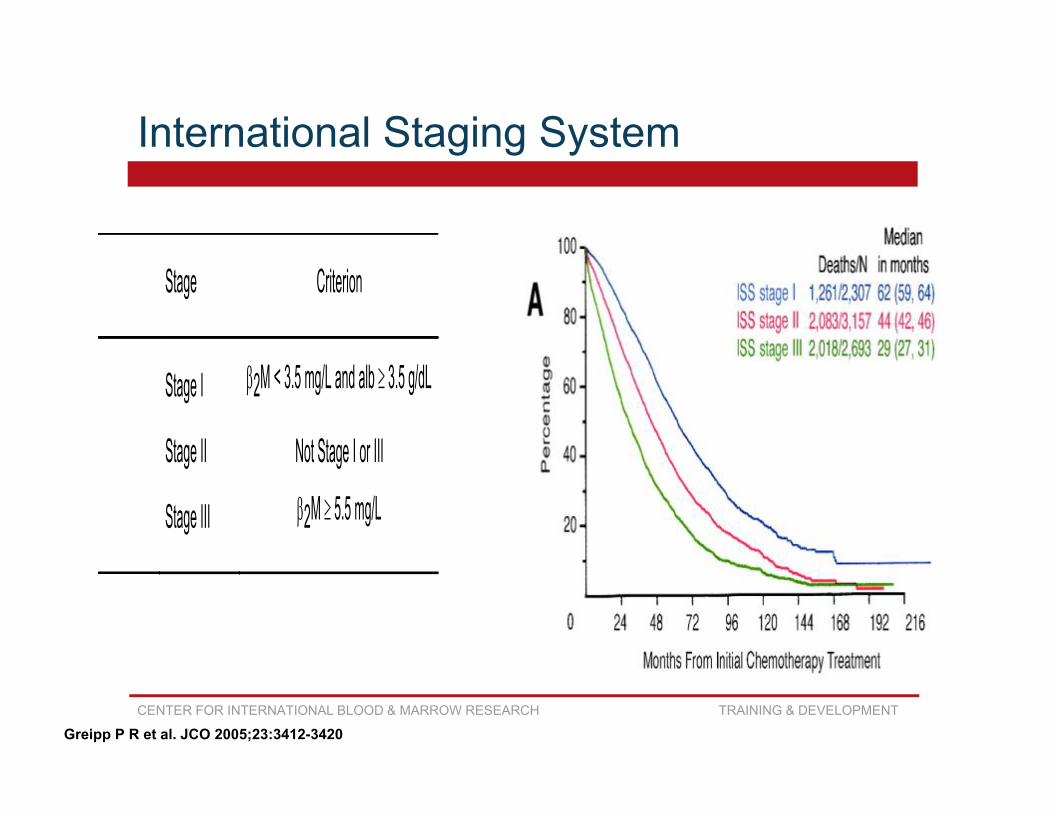
International Staging System
Stage Criterion
Stage I 2M < 3.5 mg/L and alb 3.5 g/dL
Stage II Not Stage I or III
Stage III 2M 5.5 mg/L
Greipp P R et al. JCO 2005;23:3412-3420

CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Durie Salmon Staging System
Stage I Stage III All of the following One or more of the following Hemoglobin > 10.0 g/dL Hemoglobin < 8.5 g/dL Serum calcium < 12 mg/dL Serum calcium > 12 mg/dL On radiograph, normal bone structure or
solitary bone plasmacytoma only Advanced lytic bone lesions
Low M-component production rates High M-component rates IgG < 5 g/dL, IgA < 3 g/dL, or urine IgG > 7 g/dL, IgA > 5
g/L, or urine light M spike on electrophoresis < 4 g/24
hrs chain M spike > 12 g/24
hrs Stage II Fitting neither stage I or III
A: Serum creatinine < 2 mg/dL B: Serum creatinine 2 mg/dL
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Greipp P R et al. JCO 2005;23:3412-3420
International Durie Salmon Staging System Staging System
IIA 909/1759 58 (54,61)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Cytogenetics
• FISH
• Conventional
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
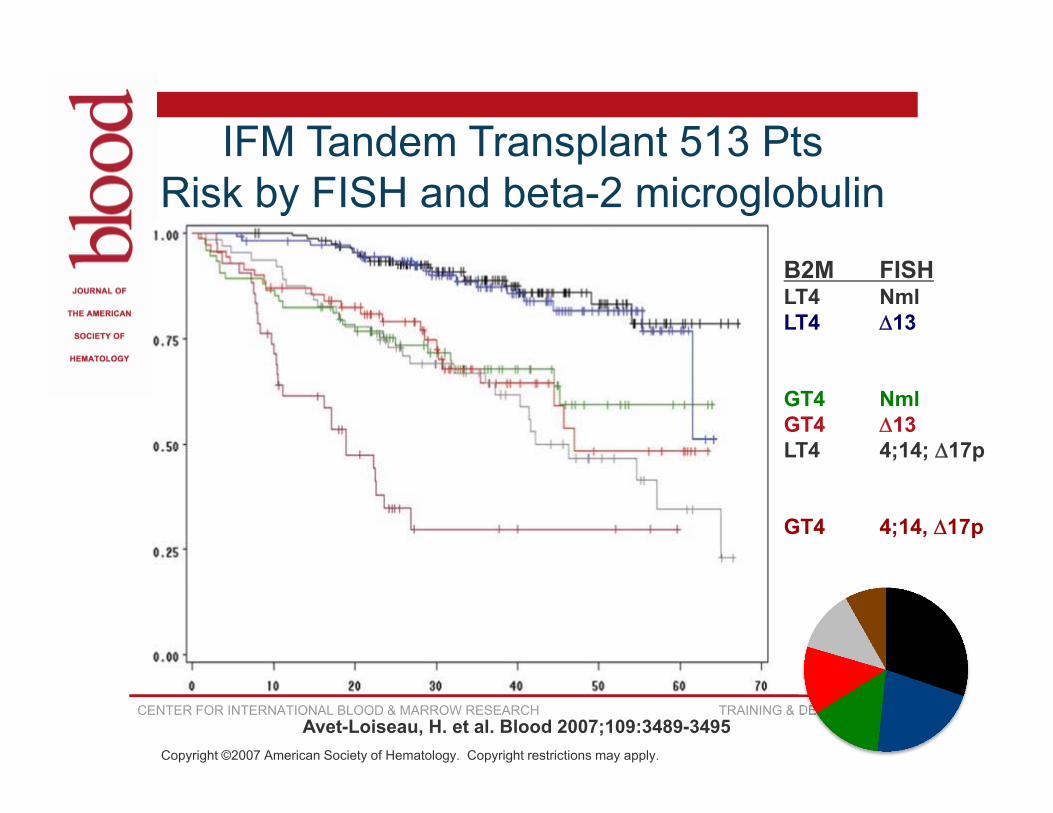
Copyright ©2007 American Society of Hematology. Copyright restrictions may apply.
Avet-Loiseau, H. et al. Blood 2007;109:3489-3495
B2M FISHLT4 NmlLT4 13
GT4 NmlGT4 13LT4 4;14; 17p
GT4 4;14, 17p
IFM Tandem Transplant 513 PtsRisk by FISH and beta-2 microglobulin
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
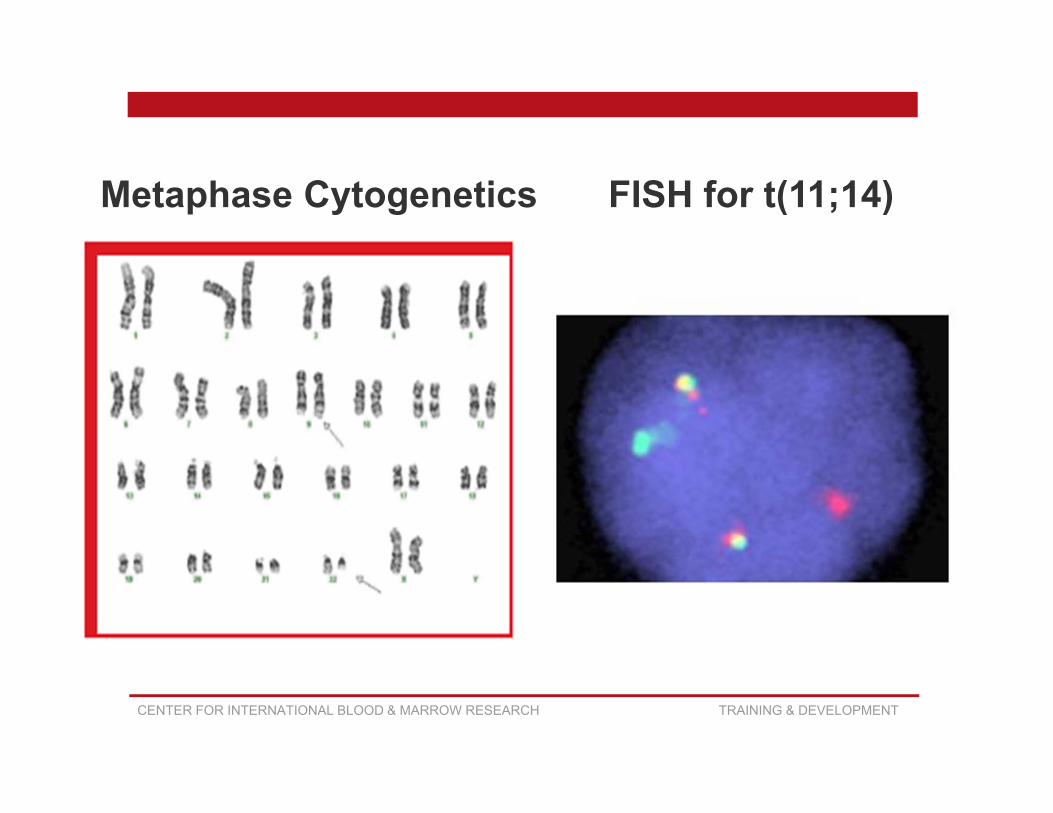
FISH for t(11;14)Metaphase Cytogenetics
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
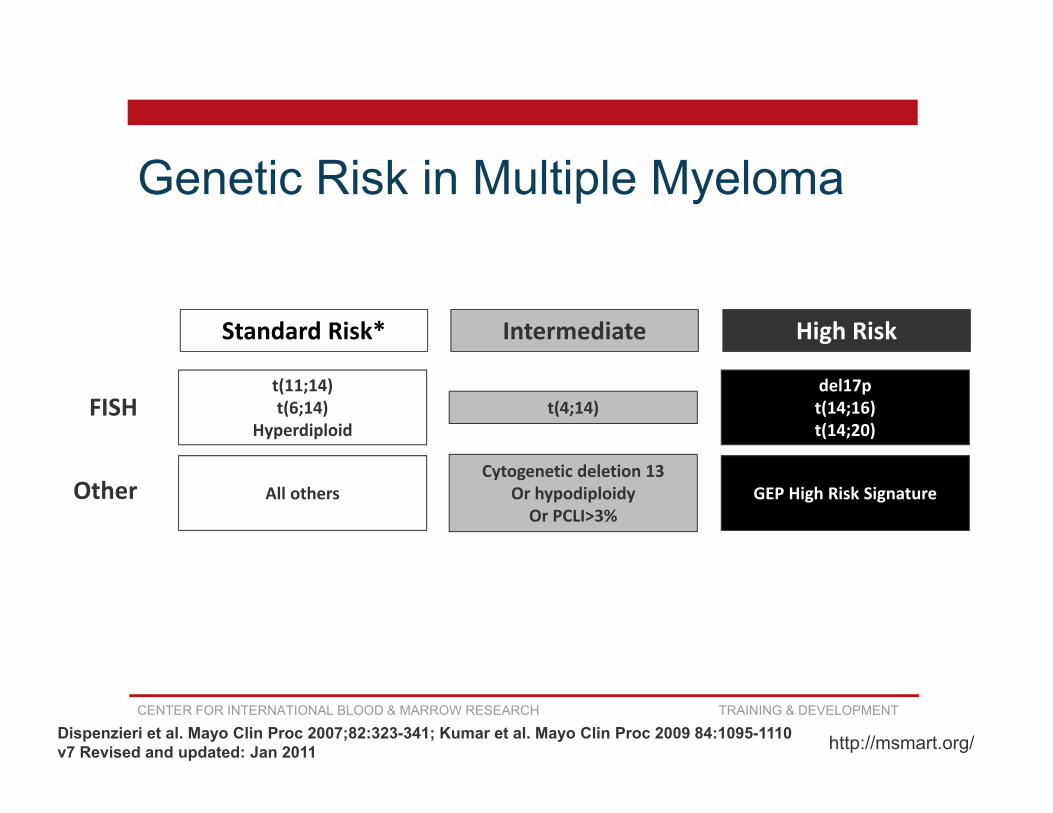
Standard Risk* Intermediate
t(11;14)t(6;14)
Hyperdiploidt(4;14)
All othersCytogenetic deletion 13
Or hypodiploidyOr PCLI>3%
FISH
Other
High Risk
del17pt(14;16)t(14;20)
GEP High Risk Signature
Dispenzieri et al. Mayo Clin Proc 2007;82:323-341; Kumar et al. Mayo Clin Proc 2009 84:1095-1110v7 Revised and updated: Jan 2011 http://msmart.org/
Genetic Risk in Multiple Myeloma
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Laboratory Studies
This section has been expanded to include:• Gene Expression Profile
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
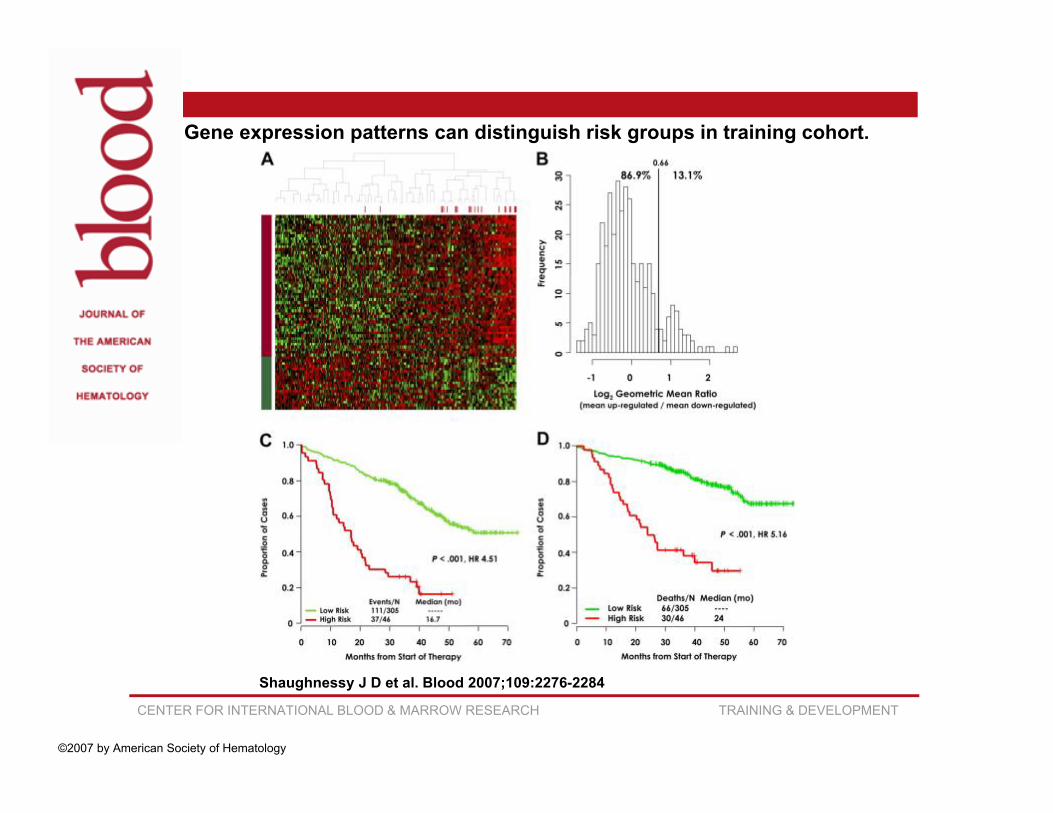
Gene Expression Profiling (GEP)
• Measures activity (the expression) of thousands of genes at once, to create a global picture of cellular function.
• GEP can distinguish between cells that are actively dividing, or show how the cells react to a particular treatment.
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Gene expression patterns can distinguish risk groups in training cohort.
Shaughnessy J D et al. Blood 2007;109:2276-2284
©2007 by American Society of Hematology
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Amyloidosis Section
• Cardiac biomarkers (current)• Brain natriuretic peptide (BNP) and/or N-terminal
prohormone brain natriuretic peptide (NT-proBNP)• Troponin

CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Amyloidosis
• Cardiac biomarkers (revised form)• Brain natriuretic peptide (BNP)• N-terminal prohormone brain natriuretic peptide (NT-
proBNP)• Troponin I• Troponin T• High sensitivity troponin T

CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Cardiac Biomarkers
• BNP- secreted by the ventricles of the heart in response to excessive stretching of heart muscle cells (cardiomyocytes)
• Troponin- integral to muscle contraction in skeletal & cardiac muscle. It is the most specific & sensitive laboratory markers of myocardial cell injury
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
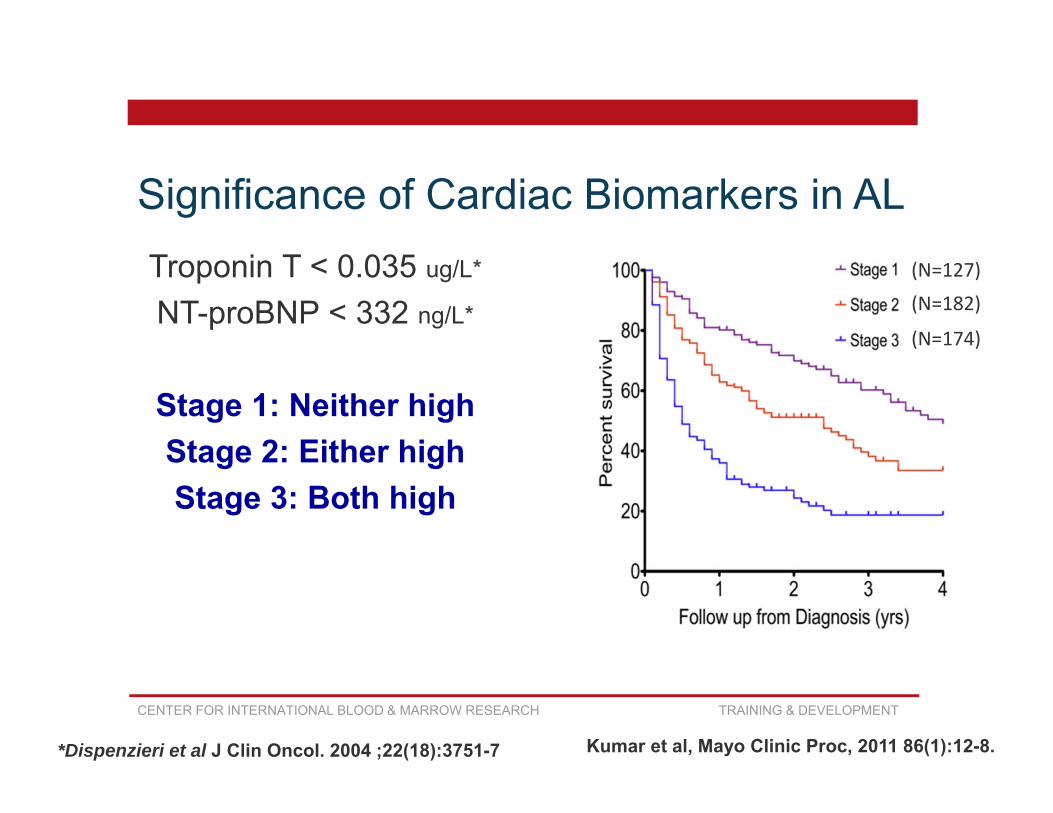
Significance of Cardiac Biomarkers in AL (N=127)
(N=182)
(N=174)
Kumar et al, Mayo Clinic Proc, 2011 86(1):12-8.
Troponin T < 0.035 ug/L*
NT-proBNP < 332 ng/L*
Stage 1: Neither highStage 2: Either highStage 3: Both high
*Dispenzieri et al J Clin Oncol. 2004 ;22(18):3751-7
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
0 12 24 36 48
Time (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
porti
on s
urvi
ving
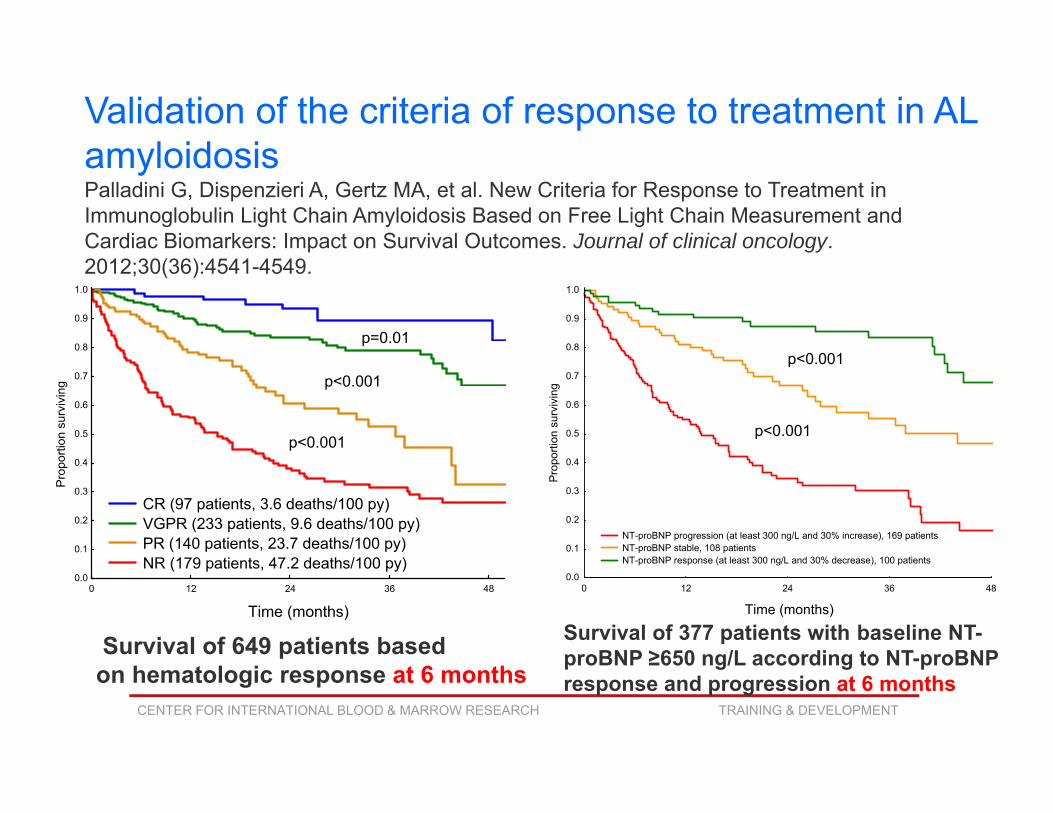
CR (97 patients, 3.6 deaths/100 py) VGPR (233 patients, 9.6 deaths/100 py) PR (140 patients, 23.7 deaths/100 py) NR (179 patients, 47.2 deaths/100 py)
p=0.01
p<0.001
p<0.001
Survival of 649 patients based on hematologic response at 6 months
Validation of the criteria of response to treatment in AL amyloidosis Palladini G, Dispenzieri A, Gertz MA, et al. New Criteria for Response to Treatment in Immunoglobulin Light Chain Amyloidosis Based on Free Light Chain Measurement and Cardiac Biomarkers: Impact on Survival Outcomes. Journal of clinical oncology. 2012;30(36):4541-4549.
0 12 24 36 48
Time (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
porti
on s
urvi
ving
NT-proBNP progression (at least 300 ng/L and 30% increase), 169 patients NT-proBNP stable, 108 patients NT-proBNP response (at least 300 ng/L and 30% decrease), 100 patients
p<0.001
p<0.001
Survival of 377 patients with baseline NT-proBNP ≥650 ng/L according to NT-proBNP response and progression at 6 months
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Pre-HCT Therapy
Added common regimens:• VCD (Bortezomab, cyclophosphamide,
dexamethasone)• RVD/VRD (Bortezomab, lenilidomide,
dexamethasone)• DVD/VDD (Bortezomab, liposomal doxirubicin,
dexamethasone)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Best Response to Therapy
• Near Complete Remission (nCR) added• Serum & urine M-protein detectable by
immunoelectrophoresis (IFE)• Negative SPEP & UPEP• <5% plasma cells in bone marrow.
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Plasma Cell Disorder (PCD) Post-HCT DataForm 2116
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Disease Specificity Determination
• Q1- Was the recipient transplanted for or do they have a history of amyloidosis?
If yes, go to Q2If no, go to Q3 (best response question)
• Q2- Did the recipient have features of multiple myeloma?
If yes, go to Q3If no, go to Q5 (lab studies at best response)
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Laboratory Studies Section
• Lab Studies at Time of Best Response to HCT• Questions 5-33• Completed for both Amyloidosis & Multiple Myeloma
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Hematologic & Organ Evaluation Section
• Questions 32-59
• Completed for Amyloid only patients; or
• Multiple Myeloma patients with a history of or concurrent diagnosis of Amyloid
CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Post-HCT Therapy
• Not using ‘planned’ vs. ‘not planned’ terminology
• Q60- Was therapy given since the date of last report for reasons other than relapse or progressive disease? (include any maintenance and consolidation therapy)

CENTER FOR INTERNATIONAL BLOOD & MARROW RESEARCH TRAINING & DEVELOPMENT
Questions