Embed Size (px)
Citation preview


FOREWORD
In ParkwayHealth, we are acutely aware of our obligation to ensure that we provide the best possible care and achieve the finest clinical outcomes for our patients.
Our Group of hospitals in Singapore - East Shore Hospital, Gleneagles Hospital and Mount Elizabeth Hospital - has long been associated with a reputation for excellent medical care, and are all accredited with the Joint Commission International (JCI), the world's leading standards organisation dedicated to improving quality and safety of health care services.
Our reputation for achieving desired clinical outcomes has propelled us to becoming the leading provider of comprehensive integrated health care services in Asia.
We aspire to be a global leader in value-based integrated health care. Towards this end we continue to invest heavily, not just in equipment and infrastructure, but also in attracting and retaining the best people and developing quality systems focussed on patient safety and clinical excellence.
We believe that it is quality and service that differentiates us from the rest. Quality and service are the foundations on which the reputation of our hospitals was built and we are committed to continuously striving to achieve new heights in these areas.
This inaugural publication is a celebration of our quality and a reflection of the outstanding work that goes on in ParkwayHealth hospitals through our clinical programmes.
My great thanks goes to all the doctors, nurses and staff who have supported the development of the clinical programmes which form the pillars of the wide spectrum of medical services we provide our patients today - from screening and diagnosis, treatment and care, surgery to rehabilitation.
I am very grateful to all of you who have so enthusiastically embraced our core values relating to People, Excellence and Results and who continue to work tirelessly towards ensuring that our patients are delighted by our service and clinical standards.
GROUP CHIEF OPERATING OFFICER'S MESSAGE
Daniel J. Snyder, FACHEGroup Executive Vice President & Group Chief Operating OfficerParkwayHealth

Keeping patients safe and achieving Outstanding Clinical Outcomes.
Three major Institute of Medicine reports in the late 90’s – “The National Roundtable on Healthcare Quality”, “To Err is Human” and “Crossing the Quality Chasm”, highlighted the major deficiencies in the design of the US health care system and sparked off a wave of interest in re-looking health care processes and health care delivery systems across the world. Quality, keeping patients safe, and enhancing clinical outcomes became buzzwords in health care institutions around the world.
In a classic formulation of the dimensions of quality of care almost 40 years ago, Avedis Donabedian described quality as including: structure (viewed as the capacity to provide high quality care), processes (or performance), and outcomes. In general, either processes or outcomes may be valid measures of quality. For an outcome to be a valid measure of quality, it must be closely related to processes of care that can be manipulated to affect the outcome. Likewise, for a process to be a valid measure of quality, it must be closely related to an outcome that people care about.
Valid clinical performance indicators and outcome measures are therefore integral components of a quality management programme. Developing these valid measures of quality are however not always easy. Clinical outcomes are affected by factors such as age, underlying co-morbid conditions, socio-economic background etc, in addition to the training and experience of the attending doctor(s) and the health care team. This variation makes it difficult for health care organisations to do apple-for-apple comparisons of the quality of their care.
Hospitals in Singapore have only recently taken the first steps towards publishing some of their performance measures and clinical outcomes. As the leading private health care group, ParkwayHealth is taking the lead amongst the private hospitals, to publish our quality initiatives (structure), and the indicators of our performance. We believe that this move towards greater transparency in demonstrating the quality of the care we offer our patients will lead to even higher standards and clinical outcomes.
Best practices relating to patient safety and clinical quality should not be limited to individual hospitals or organisations. In this regard, ParkwayHealth Hospitals draw strength in belonging to an integrated network of hospitals spread across Singapore, Malaysia, China and India.
This publication outlines our clinical quality structure and some of the processes we have put in place to reduce risk and improve clinical outcomes. Our clinical programmes are a bold attempt to re-look and rationalise the care we provide such that the health care team can work optimally to ensure outstanding patient care. As the Clinical Programmes develop, we expect to be able to refine some of our outcome indicators even more, so as to be able to truly reflect quality of care and enable us to make valid comparisons with leading institutions around the world.
We are rapidly heading towards a new age where patients insist on being able to make informed decisions about their doctors and the hospitals they will be treated at. We hope that increasing collaboration between hospitals on quality initiatives and a growing willingness to share performance and outcome measures, will result in a huge leap forward in our ability to keep our patients safe and produce outstanding clinical outcomes.
Dr S. ThanasekaranGroup Vice President Quality DivisionParkwayHealth

CONTENTSREFLECTIONS
13 Clinical Quality Scorecard15 Clinical Practice Improvement Programme17 Clinical Safety & Risk Management17 Hospital Occurrence Report (HOR)18 Adverse Outcomes18 The Sentinel Event Review Process19 Clinical Review Programme20 Infection Control21 Occupational Safety and Health22 Joint Commission International Accreditation
Clinical Quality Initiatives
26 Oncology Programme27 Heart & Vascular Clinical Programme28 Transplant & Cellular Therapy Programme30 Neuroscience Programme31 Woman & Children Programme32 Musculoskeletal Programme33 Primary Care & Chronic Diseases Programme35 Surgery Programme
ParkwayHealth Clinical Programmes
04 About ParkwayHealth06 Our Vision06 Our Mission06 Strategic Priorities07 ParkwayHealth Enterprise Strategy Map08 Quality Team & Framework09 ParkwayHealth Quality Week 200710 Service Excellence
Introduction
ON QUALITY
PAGE

ParkwayHealth has attained an international reputation
for providing excellent comprehensive medical care.
About ParkwayHealth

Our Singapore Operations Division runs three of Asia’s premier hospitals, East Shore, Gleneagles and Mount Elizabeth with a combined capacity of more than 1000 beds.
The hospitals are supported by an extensive network of primary care clinics, a full range of diagnostic services plus a state-of-the-art facility that provides surgical supplies sterilisation services.
ParkwayHealth hospitals achieve exceptional clinical outcomes with outstanding service standards. This has been the foundation of our outstanding success in moving ahead to become the leading private sector health provider in this part of the world.
In order to achieve the finest clinical outcomes, ParkwayHealth has continuously invested heavily in the best technology and the best people. ParkwayHealth was the first medical provider in South East Asia to deploy the TomoTherapy® Hi Art System, the most advanced integrated cancer treatment system in the world. It allows doctors to deliver highly accurate radiation doses with precision and can capture real-time images of the targeted tumour immediately before and after the treatment. The Haematology & Stem Cell Transplant Centre that was set up at Mount Elizabeth Hospital in 2004 was another first for the Group. This is one of the few centres in Asia that is able to provide marrow replacement therapy using stem cells for patients with haematological malignancies as well as for patients with blood disorders such as Thalassemia Major. Other areas where ParkwayHealth hospitals have taken on a leadership role include the Adult Living Donor Liver Transplantation programme. We have to date performed more than a 100 such transplants.
With 22 facilities across Asia and growing, ParkwayHealth is poised to set new standards in the quality of care, efficiency and value, integrated health systems can provide.
Breakdown of International Inpatients at ParkwayHealth

Our Vision
Our Mission
Strategic Priorities
The global leader in value-based integrated healthcare.
To make a difference in people’s lives through excellent patient care.
People... to attract, develop, retain engaged employees.
Quality... to achieve the finest clinical outcomes.
Service... to attain the highest levels of service excellence.
Finance... to meet and exceed our financial goals and targets.
Growth... to grow the system per our strategic plans.

ParkwayHealth Enterprise Strategy Map 2008 - 2010
MISSIONTo make a difference in people’s lives through excellent patient care
VISIONTo be the global leader in value-based integrated healthcare
Brand Essence • Community • Innovation • Excellence • Confidence • Global LeadershipValues • People • Excellence • Results

Quality Team and FrameworkParkwayHealth has developed a comprehensive and robust quality framework. Currently, the Quality Division is organised into five teams that look after each critical domain of our quality system:
• Medical Affairs• Quality Management• Clinical Safety & Risk Management• Infection Control • Strategic Clinical Projects
These teams work closely with clinical departments. They oversee, administer and support the following quality programmes and initiatives:
• The Hospital Occurrence System• Clinical Review Programme• Clinical Quality Scorecard• Clinical Practice Improvement Projects• Environmental & Occupational Safety • Clinical Safety & Risk Management Programme• Infection Control Programme• Monitoring of Clinical Outcomes for the 8 Clinical Programmes
In addition the Quality Division is also responsible for Accreditation & Licensing of our Hospitals. Parkway Hospitals in Singapore have the rare distinction of being the only private hospital group fully accredited by Joint Commission International (JCI).
ParkwayHealth Quality Week 2007
The Quality Week is an annual event to reaffirm and reflect on our commitment to clinical quality and keeping patients safe.
A specific theme is selected for each year. The theme for 2007 was “Safety Starts with Me”. The focus was to drive home the 6 international patient safety goals.
The following major themes were discussed at the three hospitals:• East Shore Hospital: Dr Anselm Lee on the topic of “Medication Error in Paediatrics” • Gleneagles Hospital: Dr Yeo Poh Teck on “The Law and the Health Professional” • Mount Elizabeth Hospital: Dr Yeo Khee Quan on “The Modern Nurse: Opportunities and Responsibilities”
The joint closing ceremony included talks by:• Dr Thanasekaran, GVP (Quality & Medical Affairs) & CMO, on “Using Clinical Programmes to Improve Patient Safety”• Ms Leanne Laidler, GVP (Nursing and Academy), on “Providing Safe Nursing Care”
In addition, there was a skit on “Can you understand me?” by the Gleneagles Hospital nursing and rehabilitation team that highlighted the importance of effective communication in a healthcare setting.

Service Excellence
Parkway Hospitals Singapore Overall Hospital Total Experience Index
The OPERATIONS Index is a composite of the overall for 12 Items:1. Registration services 7. Facilities2. Doctor services 8. Meals services3. Nurse services 9. Family Treatment services4. Triage services 10. Housekeeping services5. Other services 11. Discharge services6. Medication services 12. Appointment services
Patient ratings are on a 5-point scale, of which only the top 2 ratings are used for TEI calculation. Hence, the TEI is the percentile mean of the “Excellent” and “Good” ratings given by patients, or their qualified proxies.
The survey methodology is as follows:• Inpatients are interviewed face-to-face in the wards, followed by a phone call to complete the survey on their Discharge experience.• Day Surgery, Outpatient, Ancillary Services and A&E patients are interviewed over the telephone.• Each month, twenty patients from each ward/unit in the three hospitals are randomly selected to be surveyed.
The target for achievement of ParkwayHealth’s TEI in 2007 was 90%. All our hospitals achieved results that were close or above that target. In 2008, the TEI target for the hospitals has been stretched to 93%.
In January 2007, ParkwayHealth engaged, QS-First Pte Ltd, to conduct independent Patient Satisfaction surveys on our patients. QS-First is affiliated to the world renowned Press Ganey company that some of the best hospitals in the USA use.
Patient Satisfaction is tracked through a layered patient experience indexing system. The top-line indicator is the Total Experience Index (TEI).
The TEI is a composite index, calculated from patient ratings of around 16 Items. • 1 Overall Satisfaction Item• 6 Loyalty Items• 12 Operations Items
The LOYALTY Index is a composite index of 6 Items: 1. Medical Treatment2. Coordination of Care3. Service4. Value for Money5. Return6. Recommend

Clinical Quality ScorecardClinical Practice Improvement ProgrammeClinical Safety & Risk ManagementHospital Occurrence Report (HOR)Adverse OutcomesThe Sentinel Event Review ProcessClinical Review ProgrammeInfection ControlOccupational Safety and HealthJoint Commission International (JCI) Accreditation
Clinical Quality Initiatives

Clinical Quality Scorecard
On the enterprise balance scorecard, “Quality” has five measurable domains. These are:
1. To meet or exceed globally recognized clinical outcomes and benchmarks.2. Achieve the finest clinical outcomes.3. Build strong relationships with doctors and other partners.4. Create a climate of open communication.5. Build a reputation for clinical excellence.
Adverse outcome are incidents that had resulted with patient injuries requiring interventions or extended length of stay. Lower Adverse Outcome rates indicate the effectiveness of Clinical Safety measures being implemented in the facility.
Aspirin is known to help in AMI by preventing formation of blood clots and dissolving blood clots already formed causing damage to heart muscles.
Percutaneous Coronary Interventions (PCI) is one of the most effective procedure for opening blocked blood vessels that cause heart attacks.
An evaluation of the LV function checks the effectiveness of left chamber of the heart in pumping blood.
Timely use of antibiotics is known to improve the clinical outcomes of pneumonia caused by bacteria.
Administration of antibiotics within one hour before surgery is known to reduce the risk of wound infections.
MRSA is a highly dangerous and drug resistant bacterium which is known to cause Hospital Acquired Infections. Lower MRSA Rate in facility indicates the effectiveness of infection control measures being implemented.
Lower Blood stream Infection rates in ICU indicate the high level of hygiene & ensure patient safety from dangerous infections in these critical care areas of hospital.
Q1
Q2A
Q2B
Q3
Q4
Q5
Q6A
Q6B
Adverse outcome rate
Aspirin within 2 hours of admission with AMI
PCI within 90 minutes of admission with STEMI
Objective LV assessment for admissions with CCF
Antibiotic Therapy commenced within 4 hours of admission with Bacterial Pneumonia (Q4)
Prophylactic antibiotics 60 minutes before Knee and Hip Replacement Surgery
MRSA (Methicillin Resistant Staphylococcus Aureus)infection rate
Central line-associated BSI in ICU
INDICATOR EXPLANATION
The six indicators are:
Only Domain 1 “To meet or exceed globally recognized clinical outcomes and benchmarks” was measured over the full year in 2007. We started measuring Domain 2 “Achieve the finest clinical outcomes” from our eight Clinical Programmes in the last quarter of 2007. In 2008 we shall be measuring all five domains of quality.
To measure our ability to Exceed Globally Recognised Clinical Outcomes and Benchmarks we use six indicators. These were selected essentially because many international health care quality agencies recognise these indicators as being good markers of quality.
We are convinced that measuring everything we do is the only way to improve quality. You can only manage what you measure. It was with this in mind that our hospitals embarked on the Enterprise Balanced Scorecard project in 2007. The Balanced Scorecard identifies key performance indicators and measurements in our 5 strategic initiatives – People, Quality, Service, Finance and Growth.

The performance of each hospital is measured in these areas and adjusted by an assigned weightages as follows:
An overall maximum score of 5 is allocated to the Clinical Quality Scorecard.
The scorecard is updated on monthly basis & shared with all staff on monthly basis.
The progressive improvement in scores from the first to the last quarter of 2007 demonstrates how measurement changes performance. This change in performance in turn translates into better clinical outcomes and improved patient safety.
Scoring Weightage & Framework
FINAL SCOREBAND
EXCELLENT AVERAGE POOR
Tier 1 40%
Tier 2 30%
Tier 3 30%
Indicator 1 x assigned weightage
Indicator 6 x assigned weightage
Indicator 2 x assigned weightage
Indicator 3 x assigned weightage
Indicator 4 x assigned weightage
Indicator 5 x assigned weightage
Tier 1 Score
+
Tier 2 Score
+
Tier 3 Score
5
4
3
2
1
0Q1 Q2 Q3 Q4
1.72
Group Clinical Quality Scorecard 2007
3.76 4
4.78
REFLECTIONSON QUALITY 13 | 14

Clinical Practice Improvement Programme
To date, our hospitals have submitted a total of ten CPIP projects to the Clinical Quality Poster Competition, organised by the Ministry of Health.
In 2007, the following six CPIP projects were submitted by ParkwayHealth to MOH for this competition. Out of these six projects, the Parkway Laboratory’s project on “Lab Test Turnaround Time” was selected for display at the nation-wide Clinical Quality Poster Competition.
For 2008, we are targeting the following ten CPIP Projects. Out of these ten CPIP Projects nine will be driven by teams from our eight clinical programmes. This will cover the quality improvement initiatives across a wide range of clinical services. In addition to speciality based CPIP’s, a nursing team is also working on improving Tracheostomy care.
PROJECT OBJECTIVE
Surgical Clinical Programme
Oncology Clinical Programme
Transplant & Cellular therapy Clinical Programme
Women and Children Clinical Programme
Neuroscience Clinical Programme
Heart and Vascular Clinical Programme
Musculoskeletal Clinical Programme
Chronic Disease Clinical Programme
Nursing Team
To reduce incidences of needlestick injury to health care worker supporting the OR to zero incidence in 6 months
At least 85% of breast cancer patients will be provided with educational information on diagnosis
To achieve zero defect omission of medication in ward 11 and 13 (Haematology) in 6 months period
Prevention of perineal dermatitis for our encephalopathic patients
To achieve 80% compliance in area of antenatal screening of pregnant women for Group B Streptococcus within six months
Consistent technique and status of transfers of Neurology patients from bed to wheelchair and vice versa
To reduce the Incidences of Haematoma/Bleeding per month
To Achieve in 80% of patients that undergo TKR or THR, to have received pre-operative education of their procedure and what to expect post-operatively, within 6 months
To enhance the efficiency of data recording and the consolidation of results through the use of new technologies
Tracheostomy care
AREA
Radiology (Mount Elizabeth Hospital)
Nursing (East Shore Hospital)
Nursing (Mount Elizabeth Hospital)
Operating Theatre (Gleneagles Hospital)
Laboratory (Parkway Hospitals Singapore)
ME Charter (Mount Elizabeth Hospital)
Computed Radiology Repeat Rate
To reduce IV Line re-insertion rate from 20% to 10% for patients admitted at Ward 4A (Medical-Surgical) within 6 months
Prevention of Central Venous Catheter Infection in Stem CellTransplant Patients
Safe and prompt discharge of post surgical day ward patients at operating theatre
Lab Test Turnaround Time
Follow-up counselling rates of discharged inpatients
FACILITYPROJECT TITLE
The Clinical Practice Improvement Programme (CPIP) is aimed at staff participation and engagement in thinking and contributing directly towards improving patient care processes so that patient safety and clinical outcomes improve.

Showcase Project - Lab Test Turnaround TimeProject OverviewThe project aimed to improve routine lab test results turnaround time for full blood count, renal screen and liver function test. The project aimed to achieve delivering 100% of laboratory test results to the doctors located at Mount Elizabeth Medical Centre within the same day of testing.
Project TeamAdvisor: George Pusavat, CEO, ParkwayHealth Laboratory ServicesTeam Leader: Koh Guat MuiMembers:• Tan Wei How, Lab Systems Manager• Alvin Sim, Lab Operations Manager • Pamela Lim, Lab Business Office Manager• Lana Yap, Lab Business Office Executive• Junaidy Bin Tulus, Lab Despatch Supervisor• MEMC Clinician/Clinic staff
MethodologyThe project team brainstormed on the possible causes. The two main causes were identified to be:• Peak Hours: Too many specimens come at the same time• MEMC Print Reports at 15.45pm, which was not enough
Two intervention(s) were then implemented and the data was analyzed to evaluate the success rate of this project:• Intervention 1 was implemented on 07/05/2007 – One additional shuttle was started from MEH (12:10) to ARC (12:45). This aimed to spread out sample load during peak hours at ARC clinical order entry (COE). • Intervention 2 was implemented on 27/06/2007 – One additional Print job was started at 16:15. This aimed to help in printing of results coming after the existing printing time at 15:45.
ConclusionThe project achieved 98% of set target and the project team will continue to monitor & explore new intervention(s) in order to achieve the goal of delivering 100% lab test results within same day.
110
105
100
95
90
85
1st Intervention: add one additional shuttle run during peak period
2nd Intervention: add one print job
16:15
*Test orders: full blood count, renal screen and liver function set.
% same day (5pm) lab report TAT
%
REFLECTIONSON QUALITY 15 | 16

Categories of HORs received (January - December 2007)
Clinical Safety and Risk Management
Hospital Occurrence Report (HOR)Our quality system is grounded on a Voluntary Hospital Occurrence Reporting System. Staff are encouraged to report any incident that puts patients, staff, doctor, or visitor’s safety at risk regardless whether or not the person suffers an adverse outcome. Near miss reporting is also strongly encouraged. For a voluntary hospital occurrence reporting system to be successful it must:
• Be safe (that is – it must protect staff from blame)• Be simple and convenient to submit reports• Add value (the system must provide feedback and must be seen to serve as a tool for improvement)
Much has been done in recent years to cultivate a “no-blame” culture. Our Internal Reviews and Sentinel Event Reviews are firmly centred on identifying and correcting process failures.
An Electronic Hospital Occurrence Report was successfully implemented in January 2007. This has simplified occurrence reporting for our staff and sped up the routing process.
The number of Hospital Occurrence Reports increased by 55% to 2056 in 2007 against the 1324 Occurrence Reports received in 2006. We see this increase in voluntary reporting as an endorsement of the Hospital Occurrence Reporting System.
Clinical incidents constituted 53% of all HORs raised in 2007.
Non clinical incidents
Clinical incidents
Workplace safety/health
Others
Near miss27%
53%
3%7%
10%

Adverse outcome are incidents that resulted in the patient sustaining an injury, or requiring additional interventions or which resulted in the patient’s length of stay in the hospital having to be extended.
Year 2007 saw a 20% decrease in adverse outcomes in our facilities over year 2006.
Adverse Outcomes
ParkwayHealth hospitals are actively engaged in the national Sentinel Review Programme.
A Sentinel Event is one that results in an unanticipated death or major permanent loss of function, not related to the natural course of the patient’s illness or underlying condition.
All clinical incidents are evaluated using a tool called the Safety Assessment Code (SAC). This tool uses the SEVERITY of the incident and the PROBABILITY of that incident recurring, to compute an overall risk score (1 to 4) for a particular incident. A SAC score of 1 would indicate a catastrophic Incident whilst a score of 4 indicates a relatively minor incident.
The object of the sentinel review is to identify the root causes and the process failures that lead to the occurrence of the incident. The Sentinel Review panel will also make recommendations for process improvements. Targets are set for these improvements to be implemented and adoption and compliance of these new or improved processes is audited.
Defining Sentinel Events Graphically
The Sentinel Event Review Process
Medical Intervention1.Expected Occurrence2.Near Miss
3.Temporary Loss of function
4.Permanent Loss of function
Unexpected
Occurrence
Natural H
istory
Expected Death 5.Unexpected Death Time
Hea
lth S
tate
250
200
150
100
50
0
Abso
lute
Num
bers
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
61 5881 73 78
56
9477
60 7153
73 73 58 65 68 68 66 7181 86 91
7357
110 93 108 108 11599
145120
105 10496
122144
132 133159 159 150
223195 200
223
186
152
2 3 4 6 5 2 2 3 4 7 2 2 4 4 5 6 2 1 4 4 0 2 3 0
HOR / Adverse Events / Adverse Outcomes for Jan 06 - Dec 07, ParkwayHealth
REFLECTIONSON QUALITY 17 | 18

Clinical Review Programme
The Clinical Review Programme complements the Hospital Occurrence Reporting structure that we have. It is designed to pick up adverse events through the review of case notes selected on the basis of occurrences that are referred to as “flags”.
Currently we use four such flags. These are:1. Unplanned Transfer to ICU/HDU/NICU;2. Unplanned Return to Operating Theatre; 3. Unplanned admission from Endoscopy or day surgery within 72 hours;4. Unexpected deaths falling under category 4 and 5. Category 4 includes preventable deaths where steps may not have been taken to prevent it and category 5 deaths include unexpected deaths resulting from medical intervention.
Case notes of these patients are reviewed by a team of trained Reviewers using 24 explicit criteria which indicate the possibility of an adverse event. All preventable adverse events are presented to the next level, the ‘Primary Review’. The Primary Review is conducted every month. Cases validated by Primary Reviewers as “preventable” or potentially “preventable” are escalated to Physician or Nursing peer review committees such as the Medical Quality Assurance or the Nursing Quality Assurance Committees. Where necessary, the Medical Advisory Board may appoint an expert panel to delve deeper into the event and make recommendations for improvement.
To date the Clinical Review Programme has helped us identify some preventable or potentially preventable adverse events and implement process improvements to reduce the risk of similar events recurring.
The CRP helped us to initiate process improvements in following clinical areas in year 2007• Revised Protocols for prevention of aspiration pneumonia.• Revised Protocols for Tracheostomy care.• Revised Protocols for postoperative care of patients who underwent cervical spine surgery. • Revised protocols on Post Partum monitoring.• Revised protocols on the Management of Patients with pre-eclampsia.• Standard Guidelines for stopping anticoagulant therapy prior to surgery.• Revision of Nursing Assessment forms to incorporate history of other medications. (Including over the counter and Herbal Preparations). • Routine ante-natal Group B Streptococcus Screening.
The Clinical Review Process
Medical QACommittee
Medical Advisory Board
Joint Review byQuality Division Chaired
by GVP Quality
Divisional President
PRIMARY REVIEW
FLAGS
1
2
3
45
6
7
8
All Patients
Flags
Quality Review
Primary Review (Validation)
Peer Review
Peak Review
Improvement
Ongoing

Infection Control“Infection Control is Everyone’s Responsibility”
2002 to 2007 Data for Healthcare
Associated MRSA Infection Rate
*NA = Not Available
Healthcare Associated
MRSA Infection Rate
REFLECTIONSON QUALITY 19 | 20
Goals• To protect our patients by preventing or reducing the risk of healthcare associated infections.• To protect our staff and visitors from contracting infections in the hospital.
Infection Control ProgrammeThe key elements of the infection control programme are: • Hand hygiene• Standard (universal) precautions• Transmission-based precautions• Infection Control Surveillance• Safe disposal of Biomedical waste and Sharps
Targeted SurveillanceSurveillance of healthcare-associated infections at ParkwayHealth is priority-directed and targeted, based on the needs and requirements of the organization and health
regulations. The following indicators have been identified for surveillance:
• Device-associated infections in ICUs: a) Central-line associated BSI b) Ventilator-associated pneumonia c) Catheter-associated urinary tract infection• Surgical site infections for Coronary Artery Bypass Grafting (CABG) and Hip Replacement surgery• Healthcare associated MRSA infections• Vancomycin-resistant enterococci (VRE) • Post-operation pneumonia of surgical patients following CABG, Hip Replacement and Organ Transplantation surgery• Timely administration of antibiotic prophylaxis for knee replacement surgery• Timely administration of antibiotics for patients admitted with bacterial pneumonia
Occupational Safety and Health
Occupational safety and health is taken seriously by ParkwayHealth.
The following initiatives were implemented following a gap analysis conducted by external consultants in 2004: • A risk assessment framework • A hazard and spills management programme• A register of hazardous materials/chemicals was established• Surveillance and monitoring of workplace safety
A dedicated Occupational Safety and Health Department was created in year 2004 as a unit within the Quality Division.
This unit is currently engaged in creating awareness among our staff about the new Workplace Safety and Health Act (WSHA), which replaced the Factories Act. This act requires every person at the workplace to take reasonably practicable steps to ensure the safety and health of every workplace and worker. The shift from a prescriptive legislative approach to a performance-based liability regime holds accountable those who create risks to reduce risks at source. The basic premise is that every worker deserves to be protected against safety and health risks.
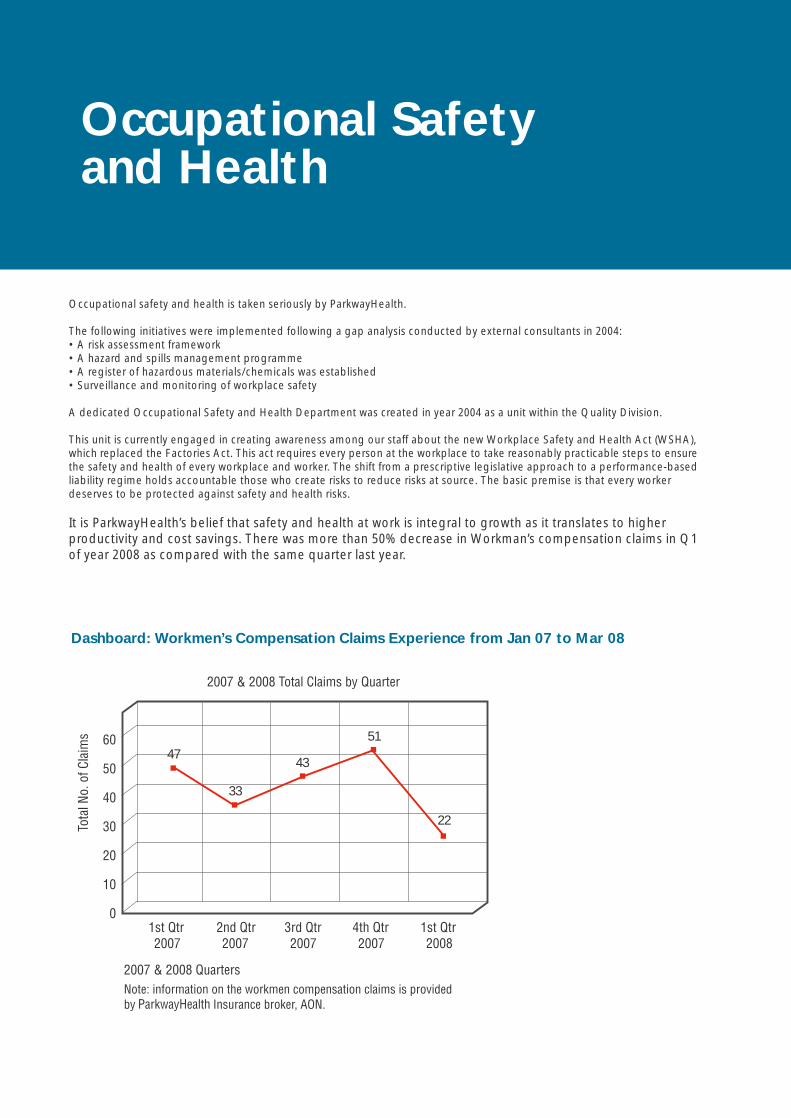
It is ParkwayHealth’s belief that safety and health at work is integral to growth as it translates to higher productivity and cost savings. There was more than 50% decrease in Workman’s compensation claims in Q1 of year 2008 as compared with the same quarter last year.
Dashboard: Workmen’s Compensation Claims Experience from Jan 07 to Mar 08
47
33
43
51
22

An independent, not-for-profit organization, The Joint Commission accredits and certifies more than 15,000 health care organizations and programmes in the United States. Joint Commission accreditation and certification is recognized around the world as a symbol of quality that reflects an organization’s commitment to meet certain performance standards.
Its international arm is known as Joint Commission International (JCI). The mission of Joint Commission International is to continuously improve the safety and quality of care of patients in the international community through the provision of education, consultation services and international accreditation.
Joint Commission International has developed more than 1000 comprehensive standards covering all aspects of patient and staff safety in healthcare organizations. These standards are audited for compliance every 3 years.
All our three hospitals in Singapore have been accredited by Joint Commission International. This gives ParkwayHealth the rare honor of being the only private healthcare group in Asia to have all their hospitals in a country accredited by JCI.
Joint Commission International (JCI) Accreditation
Gleneagles HospitalEast Shore Hospital
Mount Elizabeth Hospital
REFLECTIONSON QUALITY 21 | 22


Oncology ProgrammeHeart & Vascular Clinical ProgrammeTransplant & Cellular Therapy ProgrammeNeuroscience ProgrammeWoman & Children ProgrammeMusculoskeletal ProgrammePrimary Care & Chronic Diseases ProgrammeSurgery Programme
ParkwayHealth Clinical Programmes

The clinical programmes serve as a platform for the provision of excellent patient care. Each clinical programme is lead by a senior healthcare leader who is held responsible for the development of that particular clinical programme and for ensuring that all the elements required to be on the platform for the provision of care in these specialities are in place.
Each clinical programme works with the specialists in the particular programme to decide on the clinical outcome measures they want to use. Since October 2007, each programme is measured on at least two outcome measures. All accredited specialists are welcome to participate in the clinical programmes. The clinical programme initiative promises to be the foundation from which our hospitals can move to even greater heights of clinical quality.
Collaboration with Other Institutions
Innovation and Technology Surveillance
Marketing Support
Clinical Research/Publication
Clinical Outcome Measurement
Committed Core of Physicians
Bundled Cost
Pastoral Core Services
International Patient Services
Clinical Protocols and Defined Care Plans -
Evidence Based Care
Trained and Competent Staff
Equipment/Instruments
Laboratory and Radiology Support
Pharmacy Support
The clinical programmes initiative launched in 2007 is another step forward in our quality journey and marks the beginning of a new era in the provision of a truly integrated and seamless, patient-focused health care.
Lead by senior healthcare leaders each of our eight clinical programmes is designed to be integrated horizontally through all our hospitals in Singapore. A nurse leader assists each Clinical Programme Leader. Each clinical programme will also use Care Co-ordinators to ensure that care is orchestrated around the patient and all the patient needs are met.
SINGAPORE
Oncology
Heart & Vascular
Transplant & Cellular Therapy
Neuroscience
Women’s & Children’s
Primary Care & Chronic Disease
Surgery
Musculoskeletal
ParkwayHealth Day Surgery
& Medical Centre
(PDSMC)
East ShoreHospital
(ESH)
Gleneagles Hospital(GEH)
Mount ElizabethHospital(MEH)
ParkwayPrimary
Care Network
New Hospital
- William A Foster
“Quality is never an accident; it is always the result of high intention,
sincere effort, intelligent direction and skilful
execution; it represents the wise choice of many
alternatives.”
Oncology Programme
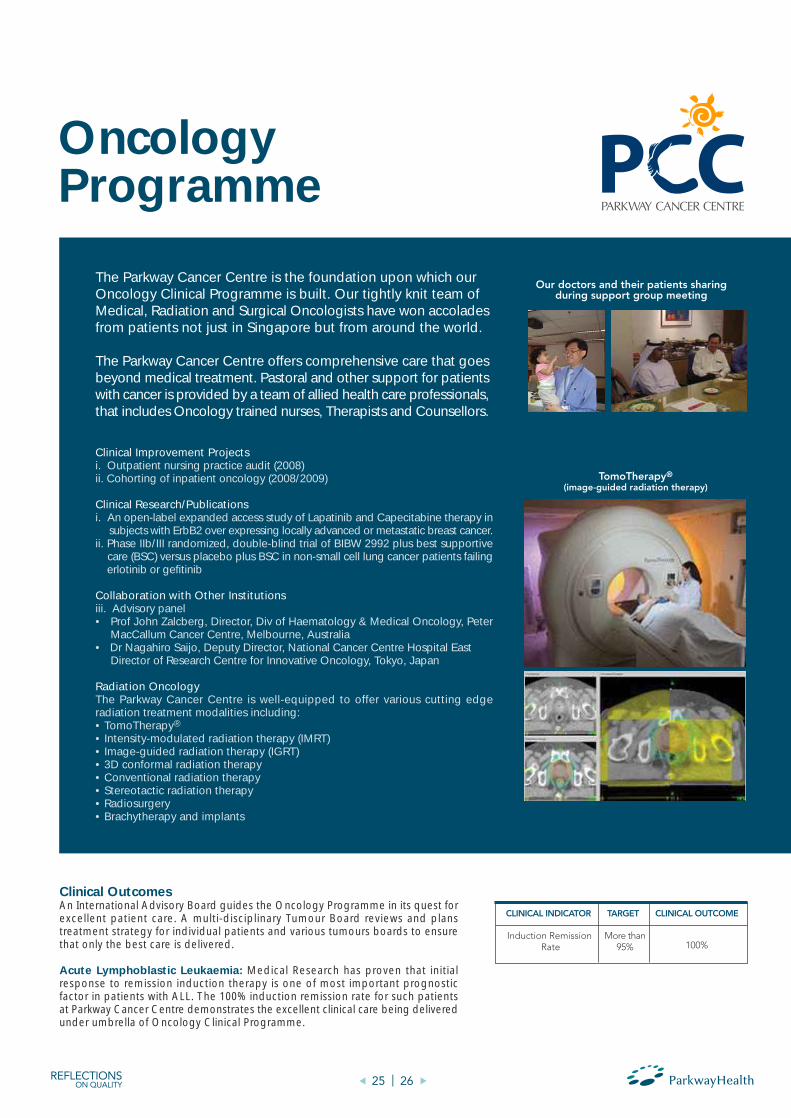
The Parkway Cancer Centre is the foundation upon which our Oncology Clinical Programme is built. Our tightly knit team of Medical, Radiation and Surgical Oncologists have won accolades from patients not just in Singapore but from around the world.
The Parkway Cancer Centre offers comprehensive care that goes beyond medical treatment. Pastoral and other support for patients with cancer is provided by a team of allied health care professionals, that includes Oncology trained nurses, Therapists and Counsellors.
Clinical Improvement Projectsi. Outpatient nursing practice audit (2008)ii. Cohorting of inpatient oncology (2008/2009)
Clinical Research/Publicationsi. An open-label expanded access study of Lapatinib and Capecitabine therapy in subjects with ErbB2 over expressing locally advanced or metastatic breast cancer.ii. Phase IIb/III randomized, double-blind trial of BIBW 2992 plus best supportive care (BSC) versus placebo plus BSC in non-small cell lung cancer patients failing erlotinib or gefitinib
Collaboration with Other Institutionsiii. Advisory panel• Prof John Zalcberg, Director, Div of Haematology & Medical Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia• Dr Nagahiro Saijo, Deputy Director, National Cancer Centre Hospital East Director of Research Centre for Innovative Oncology, Tokyo, Japan
Radiation OncologyThe Parkway Cancer Centre is well-equipped to offer various cutting edge radiation treatment modalities including:• TomoTherapy®
• Intensity-modulated radiation therapy (IMRT)• Image-guided radiation therapy (IGRT)• 3D conformal radiation therapy• Conventional radiation therapy• Stereotactic radiation therapy• Radiosurgery• Brachytherapy and implants
Clinical OutcomesAn International Advisory Board guides the Oncology Programme in its quest for excellent patient care. A multi-disciplinary Tumour Board reviews and plans treatment strategy for individual patients and various tumours boards to ensure that only the best care is delivered.
Acute Lymphoblastic Leukaemia: Medical Research has proven that initial response to remission induction therapy is one of most important prognostic factor in patients with ALL. The 100% induction remission rate for such patients at Parkway Cancer Centre demonstrates the excellent clinical care being delivered under umbrella of Oncology Clinical Programme.

Aquilion ONE can capture the entire heart in 0.35 seconds, providing the perfect view of motion free coronary arteries in exactly the cardiac phase.
Heart & Vascular Clinical Programme
Clinical OutcomesOur clinical outcome scores compare favourably to some of the best centres in the world e.g. Mortality Rate for CABG reported at our facilities was 2.1% as compared to US average of 3% as reported by AHRQ. Similarly, the Surgical Site Infection rate for CABG at ParkwayHealth was 0.9% in comparison with pooled mean rate of 1.25% for USA as reported by NNIS in year 2005.

Transplant & Cellular Therapy Programme
Our Transplant & Cellular Therapy Programme offers both living donor solid organ transplants as well as stem cell transplants for haematological conditions. In addition, targeted stem cell therapy for other conditions such as heart failure is being offered on a Clinical Registry Protocol for no option patients.
Clinical OutcomesRenal Transplant: The Total Number of Renal Transplant cases increased by 87% from 31 in 2006 to 58% in year 2007:
Graph to elaborate depth of Best Response for Targeted Therapy in Multiple Myeloma
Targeted Therapy for Multiple Myeloma (April to Dec 2007):(a) Average time to best response: 2.6 months*(b) Best depth of response to therapy
*Excludes Pending assessment, Stable disease
Data type
Number
Ratio
Total Cases*
9
100%
Stable Partial
Response
3
33.3%
Complete Remission
4
44.4%
Partial Response
1
11.10%
MinimalResponse
1
11.10%
Complete, Partial &
Stable Partial Response
8
88.8%
Year
2007
YearNumber of casesAcute Rejection Rate (%)Graft Survivability(1 Year survival rate)
*Risk Adjusted
2006
31
0*
28
2007
58
0*
NA
Number of Renal Transplant CasesNumber of Cases
70
60
50
40
30
20
10
02006 2007 Year
31
58
Num
ber o
f Cas
es
Best Depth of Response
100
80
60
40
20
0 Observed Response
Perc
ent
Complete, partial, Stable ResponseMinimal
REFLECTIONSON QUALITY 27 | 28

Living Donor Liver Transplant (LDLT):The Asian Centre for Liver Disease at Gleneagles Hospital is the first fully integrated centre for Liver Transplant in Asia. The centre has been instrumental in bringing the latest technological innovations in area of Liver Transplant to Asia. Due to scarcity of cadaveric donors in this part of world, the Living Donor Liver Transplant has evolved as the treatment of choice for patients requiring Liver Transplant. Our Liver Transplant team is lead by eminent Liver Transplant Surgeon Dr K.C. Tan. The Liver Transplant Team is recognized for its exceptional clinical outcomes. A study conducted in 2007 showed an overall 1 year survival rate of more than 80% for our Liver Transplant Patients, which is comparable to some of best Liver Transplant Centre’s around the
world. The centre which successfully performed first adult Living Donor Liver Transplant in South East Asia is also credited with performance of the First Living Donor Liver Transplant on Children in South East Asia. The Liver Transplant Centre achieved a major milestone in year 2007 when it became the first private medical centre in Asia to successfully operate on the 100th Living Donor Liver Transplantation patient. To date, the liver transplant team has undertaken 118 liver transplants. The common causes for liver transplant are hepatitis B, hepatitis C and liver cancer. Patients come mainly from Malaysia, Indonesia and India. The donors are either blood relatives or emotionally related to the recipients, and would have been screened by an independent review committee.

Neuroscience Programme
2. Barthel Indices for Stroke patients:
The Barthel Index is a scoring index composed of 10 different parameters to assess a patient’s activities of daily living and mobility. The Barthel Index is used to objectively measure progress following a stroke.
Mean Barthel Index for Stroke Patients in Ward 12, Mount Elizabeth Hospital:
3. Time–to-CT-Scan for suspected Acute Stroke Patients:
Early diagnosis of stroke patients with CT Scan helps in identifying the site & extent of brain injury and enable care provider to proceed with the best possible treatment modality. This in turn is associated with an improved clinical outcome for the patient:
The Neuroscience programme is designed to provide integrated, holistic care for patients with diseases of the nervous system (brain and nerves).
Neurologists, Neurosurgeons, Pain Management Specialists, Therapists, Speciality Nurses and other health care professionals work together to provide outstanding patient care and clinical outcomes for patients with neurological conditions.
Clinical Outcomes
1. ALOS for Anterior Cervical Discectomy patients:
Our specialists have ready access to a full range of diagnostic and specialised therapeutic instruments and equipment including:
• Computerized Tomography Scan (CT)• Magnetic Resonance Imaging (MRI)• Electroencephalography (EEG)• Electromyography (EMG)• Positron Emission Tomography (PET) Scan• Digital Subtraction Angiography (DSA) • X-Knife Stereotactic Radiosurgery • TomoTherapy®• BrainLab Stereotactic Radiosurgery
Anterior Cervical Discectomy
Target Observed ALOS at Parkway Health
* ALL Outcomes are Non Risk Adjusted
Suspected Acute Stroke Patients
Target Observed Time for CT Scan
at ParkwayHealth
Care of Stroke Patients
REFLECTIONSON QUALITY 29 | 30

The Women and Children programme provides comprehensive clinical services in the following areas:
• Obstetrics including High Risk Pregnancies• Gynaecology• Paediatric Medicine & Surgery• Neonatology• Infertility
Women and Children Programme
In Vitro Fertilization (Mount Elizabeth Hospital):
IVF Centre at Mount Elizabeth Hospital reported a Live Baby Birth Rate of 40% as compared with a rate of 34.4% reported by Centre for Disease Control for USA.
* ALL Outcomes are Non Risk Adjusted
Unexpected Return to OR
Service Score
Conversion Rate to Open Surgery
0.0%
94.5%
0.98%
Less than 1%
90%
Less than 1%
Clinical Indicator
Clinical Indicator Target Clinical Outcome
Live Baby Birth Rate (2006)
Clinical Pregnancy Rate (2007)
Service Score
40%
48%
90.4%
35%
41.8%
90%
Clinical Indicator
Clinical Indicator Target Clinical Outcome
Clinical Outcomes
MIS Laparoscopic Surgery (Cystectomy, Myomectomy, Hysterectomy):

Musculoskeletal Programme
Total Hip Replacement:
The Musculoskeletal Programme covers the entire scope of Orthopaedics – the speciality that deals with diseases and conditions associated with bones, muscles, joints and ligaments.
Orthopaedic Surgeons, Pain Management Specialist, Therapists and Specialist Nurses work together to provide a full range of services.
A comprehensive range of diagnostic and therapeutic options that are available in our hospitals makes for prompt and effective care.
Our facilities reported 0% surgical site infection rate for total hip replacement surgery in comparison with an average rate of 3.3% for Singapore
No. of Patients that are able to Ambulate 4th Post Operative Day
Prophylactic Antibiotics to be administered 0 to 60 min before total knee replacement
More than 90%
100%
Clinical Indicator
Clinical Indicator Target Clinical Outcome
93.8%*
97.8%
No. of Patients that are able to Ambulate 4th Post Operative Day
Surgical Site Infection Rate
70%
Less than 1%
Clinical Indicator
Clinical Indicator Target Clinical Outcome
68.2%*
0.0%
Total Knee & Hip Replacement Surgery - Volume
350
300
250
200
150
100
50
0THR TKR (Unilateral) TKR (Bilateral)
Num
ber o
f Pro
cedu
res
Year 2006Year 2007
Type of Surgery
Clinical Outcomes
Total Knee Replacement:
REFLECTIONSON QUALITY 31 | 32

Age Distribution of Chronic
Proportion of Patients with Multiple Conditions Chronic Distribution Chart
ParkwayHealth has 44 Primary Care Network of clinics across Singapore. Each of these clinics has a dedicated primary care team comprising lead by a Family Physician. Our Chronic Disease Management Program is focused on the three major chronic diseases:• Diabetes• Hypertension• Dyslipidemia
A pilot study comprising 217 patients from seven of our clinics was conducted in the fourth quarter of 2007.
The following observations were made:• There were more men with chronic diseases than women• The mean age of patients was at around 50 years old• More than half of all the patients had two of the three chronic conditions• Hypertension was the commonest of the three chronic conditions• About 75% of patients with chronic diseases were overweight
“Chronic Diseases are those conditions that are permanent, leave residual disability, are caused by non-reversible pathological alteration, require special training of the patient for rehabilitation, or may be expected to require a long period of supervision, observation, or care.”
- World Health Organisation
Primary Care & Chronic Diseases Programme
Sex Distribution of Chronic Diseases
120
100
80
60
40
20
0HT DM LIPID
108 41 92
59 21 39
Num
ber o
f Pat
ient
s
Male Female
Male
Female
Mean
Median
Mode
Clinical Indicator
HT
Clinical Indicator
DM
Clinical Indicator
Lipids
50.6
52
53
51.4
53
53
52
53
53
Lipids 36%
HT 47%
DM 17%
1 Condition 57%
2 Conditions 31%
2 Conditions 12%

Performance indicators to measure the quality of care we provide for patient with these three chronic diseases were developed:
1. Hypertension: It is known that maintaining the Systolic BP below 140 mm Hg and the Diastolic below 90mm Hg decreases the risk of heart disease, renal disease and stokes. Selected Indicator: To achieve Systolic Blood Pressure of 140 or below & Diastolic Blood Pressure of 90 or below for 70% of Hypertensive Patient Population over a period of 3 months.
2. Diabetes: Maintaining good glycaemic control reduces the risks of microvascular and other long term complications of diabetes mellitus. Selected Indicator: HbA1C Level of 7 or less for at least 60% of diabetic patients over 3 months.
3. Dyslipidemia: Refers to lipid abnormalities. High lipid level is associated with high cardiovascular morbidity and mortality. Selected Indicator: LDL Levels to achieve a target of 60% over six months for following categories: • Risk <10% (Patients with 1 Risk Factor) - Target LDL Level <160 over 6 months • Risk 10-20% (Patients with 2 Risk Factors) - Target LDL Level <130 over 6 months • Risk >20% (Patients with 3 or more Risk Factors) - Target LDL Level < 100 over 6 months
Our Chronic Disease Programme has started collecting data for these indicators in January 2008. Outcome data will be available in the third quarter 2008.
Clinical Quality Performance Indicators

Surgery Programme
Our General Surgery Clinical Programme covers the following surgical specialities:
• General Surgery• Minimally Invasive Surgery• Otorhinolaryngology• Ophthalmology• Urology• Plastic surgery
Clinical Outcomes
We currently track surgical outcome in Prostate surgery & Laparoscopic Cholecystectomy. More outcome measurements will be added as the programme develops.
The average length of stay for Laparoscopic Cholecystectomy was reported to be 2.1 days at ParkwayHealth Hospitals. It is interesting to note that this is far better than average length of stay of 4 days for the same procedure as reported by Cleveland Clinic, USA.
TURP
Average Indwelling Catheter Removal time for TURP
Less than 3 days
Clinical Indicator
Clinical Indicator Target Clinical Outcome
2.1 days
MIS Laparoscopic Cholecystectomy
Average Length of Stay 4 days
Clinical Indicator
Clinical Indicator Target Clinical Outcome
2.1 days
Conversion Rate to Open Surgery Less than 1% 0.6%
Laparoscopic Cholecystectomy
470
465
460
455
450
445
440
435Year 2006 Year 2007
Volu
me

Designed and Printed by Four Media Pte Ltd / July 2008
An annual publication for internal circulation by Quality Division, ParkwayHealth.
July 2008
EditorDr S. Thanasekaran
Group Vice PresidentQuality Division
[email protected] Line: (65) 6317 2328
Editorial CoordinatorDr. Sachin GuptaSenior Manager,
Strategic Clinical [email protected] Line: (65) 6317 2398
Parkway Group Healthcare Pte Ltd111 Somerset Road
#15-00Singapore 238164
Company Registration no.: 199303778C
www.parkwayhealth.com
©2008 Parkway Group Healthcare Pte LtdAll rights reserved.
The material in this publication cannot be reproduced whether in part or in whole without the permission of the publisher.

NOTES:
37 | 38 REFLECTIONSON QUALITY

REFLECTIONSON QUALITY 35 | 36
NOTES:

A PARKWAYHEALTH QUALITY DIVISION PUBLICATION
East Shore Hospital321 Joo Chiat PlaceSingapore 427990
Tel: +65 6344 7588
Gleneagles Hospital6A Napier Road
Singapore 258500
Tel: +65 6473 7222
Mount Elizabeth Hospital3 Mount ElizabethSingapore 228510
Tel: +65 6737 2666
ParkwayHealth Primary Care Network20 Bendemeer Road, #01-02/06
Singapore 339914
Tel: +65 6227 7777
ParkwayHealth Day Surgery & Medical Centre363 Balestier RoadSingapore 329784
Tel: +65 6305 7305
www.parkwayhealth.com
JULY 2008





























