Embed Size (px)
Citation preview

Fitness, Fatigue, Disease Activity, and Quality ofLife in Pediatric LupusKRISTIN M. HOUGHTON,1 LORI B. TUCKER,1 JAMES E. POTTS,1 AND DONALD C. MCKENZIE2
Objective. To measure aerobic fitness (maximum oxygen consumption [VO2peak]), fatigue, quality of life (QOL), anddisease activity in young persons with systemic lupus erythematosus (SLE), and to determine an equation for predictingVO2peak from the distance walked in 6 minutes (6MW).Methods. Fifteen young patients ages 12–19 years with SLE participated. VO2 was measured by a graded treadmillexercise test. Submaximal exercise intensity was determined from the ventilatory anaerobic threshold. Submaximalaerobic capacity was measured using the 6MW. Patient questionnaires included measures of fatigue, QOL, and physicalactivity. Physician questionnaires included the Systemic Lupus Erythematosus Disease Activity Index and the SystemicLupus International Collaborating Clinics/American College of Rheumatology Damage Index.Results. Compared with age-matched norms, our patients had moderate impairment in aerobic fitness, with a mean � SDVO2peak of 31.1 � 7.9 ml/minute/kg and a mean 6MW distance Z score of �2.4 � 2.3. The regression equation to predictVO2peak (ml/minute/kg) from 6MW was as follows: 57.1 � [0.038 � distance (meters)] � (�0.35 � maximal heart rate) (R �0.67, P � 0.027). Ten subjects (67%) reported significant fatigue. There was no significant correlation of fatigue with fitnessmeasures. Neither fatigue nor fitness was significantly correlated with disease activity, disease damage, or QOL measures.Conclusion. Young SLE patients have lower aerobic fitness than reference norms. The 6MW may be used as a marker offitness, but it is preferable to determine VO2 with a graded exercise test. Fatigue is a significant symptom in young SLEpatients. The application of fatigue measures in young persons is exploratory. The relationship between fatigue andaerobic fitness is not clear.
INTRODUCTION
The onset of systemic lupus erythematous (SLE) occurs inchildhood or adolescence for �15% of affected individu-als. Young persons with SLE generally have severe diseaseat onset, requiring high-dose corticosteroid and immuno-suppressive drugs for disease control (1–4). A majorityhave organ system disease (kidney, lung, central nervoussystem, heart) either at diagnosis or early in the course oftheir disease (1). The combination of active disease andside effects of corticosteroid treatment, such as weightgain, results in difficulties in normal functioning for chil-dren with SLE. Many children with SLE discontinue their
participation in sports or physical activity at the time ofdiagnosis (4).
Fatigue is one of the most prevalent clinical manifesta-tions of SLE. Fatigue is a nonspecific and highly subjectivesymptom, and perceived severity may be related to psy-chosocial and disease- and treatment-related factors (5).Fatigue can be profound and often affects an individual’sability to function. Several studies have suggested a corre-lation of fatigue with disease activity, pain, mood, andsleep dysregulation (2,3,5–8). A positive correlation be-tween fatigue and fibromyalgia (FM) associated with SLEhas been demonstrated in adults (9). Physical inactivityand deconditioning may also play a role in fatigue andquality of life (QOL) in patients with SLE.
Despite the important role of fatigue in adults with SLE,there have been no studies reporting the incidence offatigue in children with SLE and its impact on their dailylives. In addition, the extent of physical deconditioningand inactivity among children with SLE has not beenstudied. Aerobic fitness diminishes after adolescence andhas a strong positive relationship with general health. Re-cent large cohort studies have confirmed the importance ofexercise capacity in predicting mortality among both menand women (10,11). The role of exercise in children withchronic disease is an area in need of clarification.
Supported by a grant from the British Columbia Chil-dren’s Hospital Telethon.
1Kristin M. Houghton, MD, FRCPC, FAAP, Lori B. Tucker,MD, FAAP, James E. Potts, PhD: British Columbia Children’sHospital, Vancouver, British Columbia, Canada; 2Donald C.McKenzie, MD, PhD: Human Kinetics and University ofBritish Columbia, Vancouver, British Columbia, Canada.
Address correspondence to Kristin M. Houghton, MD,FRCPC, FAAP, K4-123 ABC, 4480 Oak Street, Vancouver,British Columbia, Canada V6H 3V4. E-mail: [email protected].
Submitted for publication June 14, 2007; accepted in re-vised form October 12, 2007.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 59, No. 4, April 15, 2008, pp 537–545DOI 10.1002/art.23534© 2008, American College of Rheumatology
ORIGINAL ARTICLE
537

The purpose of the present study was to measure fitness,fatigue, and QOL in a cohort of young patients with SLE.Our hypothesis was that young patients with SLE wouldhave reduced aerobic fitness compared with referencenorms and that fatigue would be inversely related to aer-obic capacity. The secondary objectives of this study wereto test the use of a modified Kids Fatigue Severity Scale(K-FSS), to examine the relationship between maximaland submaximal exercise tests in our study population,and to determine an equation for predicting maximumoxygen consumption (VO2peak) and ventilatory anaerobicthreshold (VAT) from the distance walked in 6 minutes(6MW) (12).
PATIENTS AND METHODS
Participants. Patients ages 12–20 with a definite diag-nosis of SLE who were followed at the Pediatric Rheuma-tology Program at British Columbia Children’s Hospitalwere invited to participate (13,14). Patients were excludedif they had been diagnosed within the preceding 3 months,were �18 years of age at diagnosis, or had active organsystem disease or treatment morbidity (including renalinsufficiency, pericarditis, pleuritis, serositis, myositis,avascular necrosis) precluding participation in exercisetests. Study assessments occurred between January 2006and March 2007. All patients and caregivers providedassent and consent prior to participation. Ethical approvalwas obtained from the University of British Columbia’sClinical Research Ethics Board and the hospital’s ResearchReview Committee.
Methods. Study participants underwent a clinical as-sessment by a rheumatologist (KMH) the same day as theexercise testing. Assessment included a complete physicalexamination (including tender point count) and data col-lection for age, sex, disease duration, history of previouscardiac or respiratory disease (echocardiogram, electrocar-diogram [EKG], and pulmonary function test results), andcurrent medications.
Anthropometric measures. Height (Harpenden Stadi-ometer, London, England) and body mass (SECA electron-ics, Hamburg, Germany) were measured to the nearest 0.1cm and 0.1 kg, respectively. Body mass index (BMI) wascalculated (kg/m2). Body composition (percent body fat)was estimated from the sum of skinfold measurements ofthe subscapular and triceps region (Baseline Skinfold Cal-iper, AMG Medical, Montreal, Quebec, Canada) accordingto the equation developed by Slaughter et al (15). Obesitywas defined as a BMI or triceps skinfold greater than the95th percentile according to reference data (16).
Fitness measures. Aerobic fitness. Maximal aerobic ca-pacity (VO2peak) is the level of oxygen uptake that cannotbe surpassed with increased exercise intensity. VO2peak
was measured by a graded treadmill exercise test to voli-tional fatigue. Treadmill speed was kept constant at 5km/hour and the grade was increased 2.5% every 2 min-
utes. Open-circuit spirometry was used to determine re-spiratory exchange variables during exercise and was av-eraged over 15-second intervals. Patients breathed througha Hans Rudolph valve (Hans Rudolph, Kansas City, MO).Using a MOXUS Metabolic Cart (AEI Technologies, Pitts-burgh, PA), expired gases were analyzed by O2 and CO2
analyzers (models S-3A and CD-3A, respectively; AEITechnologies). The system was calibrated before each testwith standard gases of known O2 (20.93% and 15.00%)and CO2 (0.03% and 5.02%) concentrations. Volume wascalibrated and verified using a 3-liter syringe (Hans Ru-dolph). Measurements included total test duration,VO2peak (defined as the highest VO2 achieved in any 15-second period), maximal ventilation, peak respiratory ex-change ratio (RER), maximal heart rate (MHR), and percentage-predicted MHR. Blood pressure in the right arm wasmeasured manually at baseline, every 5 minutes duringexercise, and 5 minutes postexercise with a sphygmoma-nometer. A maximal effort was defined as achieving anRER �1.0, or reaching an MHR �195 (17). VO2peak wascompared with American population data (18).
Submaximal exercise intensity was determined by theVAT. VAT, defined as the point at which oxygen supplyno longer meets oxygen demands of exercising muscle, isa surrogate measure of lactate threshold (19). We used thepoint of inflection of the maximal ventilation/VO2, withthe maximal ventilation/CO2 production constant or de-clining as the VAT (20).
Submaximal aerobic capacity is exercise performed be-low the maximal oxygen uptake. Submaximal tests areoften used to predict VO2peak. Submaximal aerobic capac-ity was determined from the 6MW. The walk test wasperformed in our clinic (50-meter measured loop) withstandard encouragement (21). Distance walked in meters,MHR, average HR, and rating of perceived exertion (RPE)were recorded. RPE was recorded as a number value from1 to 10 per the Children’s Effort Rating Scale (22). Refer-ence values for the 6MW were obtained from healthywhite and Chinese populations (23,24). Children of otherSoutheast Asian background or American Indians werecompared with the reference Chinese data, which areslightly lower than the reference data for whites.
Strength. Isometric quadriceps strength of the dominantleg and grip strength were measured with a CITEC hand-held dynamometer (CT 3001; C.I.T. Technics, Groningen,The Netherlands); the best effort of 3 trials was recorded(rectus femoris was measured with the hip and knee flexedat 90° and the ankle supported by the examiner with thedynamometer on the anterior surface of the distal thigh).Results were compared with reference population data(25).
Flexibility. Flexibility of the dominant hamstrings andgastrocnemius muscle groups was measured with a goni-ometer (Incstar Corporation, Stillwater, MN). Popliteal an-gles and ankle dorsiflexion were recorded to the nearestdegree.
Patient questionnaires. The K-FSS was used to assessfatigue. The FSS is a validated questionnaire developed foradults that measures the impact of fatigue on activities of
538 Houghton et al

daily living (12). The questions on the FSS were modifiedso that they were appropriate for children’s language andactivities (Table 1). Scores range from 1 to 7 with higherscores indicative of more fatigue. Fatigue was defined aspresent if the K-FSS score was �3.0 (5).
Habitual physical activity levels were assessed using theHabitual Activity Estimation Scale (HAES). The HAES hasbeen validated in healthy children and children withchronic disease. The Two Days of My Life questionnaireasks children to recall typical weekday and weekend dailyactivity, estimating the time spent inactive (e.g., sleeping),somewhat inactive (e.g., sitting), somewhat active (e.g.,walking), and active (e.g., running) (26). Patients withsummary scores reflecting �3 hours per week of activitywere considered active (27).
QOL was measured with the Child Health Questionnaire(CHQ), a generic validated questionnaire measuring theQOL of children ages 5–17 years. The CHQ child version isa profile measure with 78 questions that measures physicalfunctioning, social and emotional functioning, mentalhealth and behavior, self-esteem, and family functioning.Reference norms are available, with higher scores indica-tive of higher QOL (28).
Disease measures. The Systemic Lupus ErythematosusDisease Activity Index (SLEDAI) was used to assess dis-ease activity (29). The SLEDAI assesses 24 clinical andlaboratory measures of SLE activity with a score range of0–105; a higher score corresponds to higher disease activ-ity. The following activity categories have been defined onthe basis of SLEDAI scores: no activity (SLEDAI � 0), mildactivity (SLEDAI � 1–5), moderate activity (SLEDAI �6–10), high activity (SLEDAI � 11–19), and very highactivity (SLEDAI �20) (30). The Systemic Lupus Interna-tional Collaborating Clinics/American College of Rheuma-tology (ACR) Damage Index (SDI) was used to assess dis-ease damage (31). Items include disease- and treatment-related morbidities. Scores range from 0 to 47 and itemsmust be present continuously for �6 months to be scoredas damage.
Statistical analysis. Descriptive statistics were calcu-lated for fitness measures, fatigue, and QOL. Mean � SDvalues and Z scores are presented. The association be-tween continuous variables was assessed using Pearson’sand Spearman’s correlation coefficients. Linear regressionmodels were used to explore the relationships betweenaerobic capacity and fatigue, QOL, disease activity, anddisease damage. Correlation coefficients of 0.3–0.5, 0.5–0.7, and 0.7–1.0 indicated low, moderate, and high corre-lations, respectively. The 6MW distance, walking MHR,BMI, and SLEDAI scores were correlated with VO2peak andwith VAT to determine which variables to enter into astepwise regression equation to predict VO2 and VAT. Thesignificance level for all tests was set at P values less than0.05, except for determining which variables to enter intostepwise regression, which was set P values less than 0.10.Fisher’s exact test was used for a 2 � 2 contingency table.Statistics were performed using SPSS 15.0 (SPSS, Chicago,IL).
RESULTS
At the time of the study, 32 of the 48 patients with SLEwho were followed in our clinic were eligible to partici-pate. Of these, 15 participated. The majority of patientswho declined cited lack of time as the reason. Sixteenpatients with SLE were excluded (9 patients had activedisease precluding exercise testing, 2 patients were diag-nosed within 3 months of the study closing, and 5 weredeemed ineligible because they were �12 years of age).Demographic, clinical, and disease factors are shown inTable 2. The mean � SD age was 16.5 � 1.9 years. Themean disease duration was 45 � 33 months. All patientswere taking hydroxychloroquine, 10 (67%) were takingprednisone, and 10 (67%) were taking at least 1 noncorti-costeroid immunosuppressant. Disease activity and dis-ease damage were variable (Table 2).
Only 1 patient met our operational definition of obesity.Several patients had a few tender points, but none met theACR criteria for FM (32,33). The clinical cardiorespiratory
Table 1. Kids Fatigue Severity Scale and Fatigue Severity Scale (12)*
Question Modified kids statement Adult statement
1 I don’t feel like doing anything when I amfatigued.
My motivation is lower when I am fatigued.
2 Exercise brings on my fatigue. Exercise brings on my fatigue.3 I am easily fatigued. I am easily fatigued.4 Fatigue interferes with things like walking,
running, or climbing stairs for me.Fatigue interferes with my physical
functioning.5 Fatigue causes frequent problems for me. Fatigue causes frequent problems for me.6 My fatigue makes it hard to do physical
activities for very long.My fatigue prevents sustained physical
functioning.7 Fatigue interferes with things I need to do,
like going to school.Fatigue interferes with carrying out certain
duties and responsibilities.8 Fatigue is among my 3 biggest problems. Fatigue is among my 3 biggest problems.9 Fatigue interferes with my social life
(spending time with friends).Fatigue interferes with my work, family, or
social life.
* Patients choose a number from 1 to 7 corresponding to their level of agreement with each statement (1 � strongly disagree and 7 � strongly agree).
Fitness in Pediatric Lupus 539

examination, EKG, and echocardiogram were normal in allpatients. There were mild diffusion abnormalities on pul-monary function tests in 5 (33%) patients, but all hadnormal oxygen saturation. One patient had mild restrictivelung disease.
Fitness. Fitness measures are shown in Tables 3 and 4.There was a large range in fitness measures, with a mean �SD VO2 peak of 31.1 � 7.9 ml/minute/kg corresponding to amean � SD Z score of �1.75 � 1.16. Five (33%) patientshad Z scores of �2 or lower. Only 2 (13%) patients had aVO2 peak greater than �1 Z score of reference norms (18).
Distance covered during the 6MW was lower than age-,sex-, and ethnicity-matched normative data for white andChinese children (34,35). The mean � SD distance coveredwas 548 � 110 meters, corresponding to a mean Z score of�2.4 � 2.3. Nine (60%) patients had Z scores of �2 orlower.
The mean � SD VAT was 20.1 � 1.3 ml/minute/kg forboys compared with a normative mean value of 22 � 5.0ml/minute/kg (P � 0.51). The mean � SD VAT was 17.0 �5.8 ml/minute/kg for girls compared with a normativemean value of 20.0 � 4.0 ml/minute/kg (P � 0.03) (18).VAT usually corresponds to 60–70% of VO2peak (36–38).
Table 2. Patient demographic, clinical, and disease measures*
Patient Age, years Sex Ethnicity Disease duration, months Medications† SLEDAI SDI
1 16.7 F East Indian 6 1�, 2, 5, 10 4 22 18.5 F Filipino 6 1�, 2, 5, 8, 9 12 23 14.8 F Sri Lankan 43 2, 4 2 04 14.4 F Chinese 22 1�, 2, 6, 9 6 05 17.0 F Chinese 59 2, 6, 7 0 06 17.8 F American Indian 132 1�, 2, 5, 9 12 17 16.6 M Vietnamese 32 1, 2, 4, 11, 12 4 08 17.6 M White 41 2, 7, 13 0 09 16.8 F Chinese 57 1, 2 2 010 14.8 F White 4 1�, 2, 13 2 011 19.6 F Chinese 68 2 0 012 18.6 F White 56 1, 2, 4 5 213 14.0 M Vietnamese 49 1�, 2, 5, 7–9, 11 16 114 12.8 F White 25 1�, 2, 4 16 015 17.1 F Vietnamese 71 2 2 0Mean � SD 16.5 � 1.9 45 � 33Median (range) 4 (0–16) 0 (0–2)
* SLEDAI � Systemic Lupus Erythematosus Disease Activity Index; SDI � Systemic Lupus International Collaborating Clinics/American College ofRheumatology Damage Index.† 1 � prednisone; 1� � �10 gm/day; 2 � hydroxychloroquine; 3 � methotrexate; 4 � azathioprine; 5 � cyclophosphamide; 6 � mycophenolatemofetil; 7 � aspirin; 8 � hydrochlorothiazide; 9 � enalapril; 10 � intravenous immunoglobulin; 11 � amlodipine; 12 � losartan potassium; 13 �naproxen.
Table 3. Fitness measures*
PatientBMI,kg/m2
% bodyfat
VO2 testduration,minutes
VO2peak,ml/kg/mind
VO2peak,% age/
sexpredicted
(18)VO2peakZ score RER
VO2MHR
VAT, ml/kg/min
%VAT
(VAT/VO2)
6MW,meters
6MWZ score
6MWMHR
1 20.0 28.1 8.75 17.5 44 �3.70 1.12 178 11.9 66 470 �4.3 1562 23.2 25.1 25.1 20.5 51 �3.21 0.82 200 9.1 54 575 �1.6 1583 17.5 21.2 21.2 28.4 66 �2.34 0.75 152 ND ND 595 �1.1 1414 22.3 25.4 25.4 33.3 78 �1.55 0.96 203 13.9 36 512 �3.2 1265 19.8 18.1 18.1 29.8 74 �1.69 0.84 196 15.0 48 430 �5.4 1246 35.6 51.7 51.7 21.9 55 �2.98 0.74 180 14.6 67 480 �4.1 1287 20.1 23.0 23.0 34.7 68 �1.71 1.00 171 20.7 54 505 �2.8 1348 21.4 21.3 21.3 38.9 76 �1.27 1.16 181 22.4 53 370 �5.8 1259 18.0 30.4 30.4 32.2 80 �1.29 1.10 181 19.7 45 600 �1.0 11610 22.1 25.7 25.7 38.2 89 �0.76 1.14 206 27.5 55 630 �0.65 12811 19.7 25.4 25.4 30.9 77 �1.51 1.28 193 20.4 57 450 �4.8 13612 20.3 26.7 26.7 24.1 60 �2.62 1.17 160 ND ND 550 �2.3 13413 20.2 18.9 18.9 35.1 66 �1.64 1.09 167 19.4 60 680 �0.17 13214 16.9 23.3 23.3 48.2 119 1.17 0.99 195 41.1 66 814 3.0 14115 24.2 30.4 30.4 33.2 83 �1.13 1.04 197 17.7 52 560 �2.0 139Mean� SD
21.4 � 4.4 26.3 � 7.9 14.7 � 4.6 31.1 � 7.9 72 � 18 �1.75 � 1.16 1.01 � 0.16 184 � 16 17.4 � 5.6 55 � 9 548 � 110 �2.4 � 2.3 135 � 11
* BMI � body mass index; VO2 � oxygen consumption; VO2peak � maximum oxygen consumption; RER � respiratory exchange ratio; MHR � maximalheart rate; VAT � ventilatory anaerobic threshold; 6MW � distance walked in 6 minutes; ND � not determined.
540 Houghton et al

Our patients’ mean percent VAT was 55% � 9%. The VATcould not be determined in 2 patients.
Compared with age-matched norms, rectus femorisstrength was low, with a mean � SD of 185 � 70N corre-sponding to a mean Z score of �2.5 � 1.9 (25). Eight (53%)patients had Z scores of �2 or lower. The mean gripstrength was 107 � 22N. Normative data are available for3-point grip but not grip strength. Flexibility of the ham-strings was suboptimal in all patients, with none havingpopliteal angles �160° (mean � SD 139° � 7°). Achillesflexibility was representative of the adolescent population(mean � SD 10° � 4°).
Results from patient self-report of fatigue, habitual ac-tivity levels, and QOL measures are shown in Table 5. Themean � SD K-FSS score was 3.8 � 1.2. Ten (67%) patientsreported a K-FSS score �3.0, indicating significant fatigue(5). Using the HAES, 8 (53%) children reported a physi-cally active lifestyle. Fatigue and activity level were notrelated (P � 0.38). For the CHQ, normative means areavailable for a reference school-based population and end-
stage renal disease population; the SD is only available forindividual items, not subscales or general scores. The CHQgeneral health perceptions (CHQ-GH) and self-esteemwere lower in our patients with SLE than reference norms.There were no significant differences between our patientsas a group and the reference sample on measures of phys-ical functioning, social and emotional functioning, mentalhealth and behavior, or pain and pain behaviors. Ourpatients had more disruption of family functioning, withlower scores for family activities but not family cohesion.
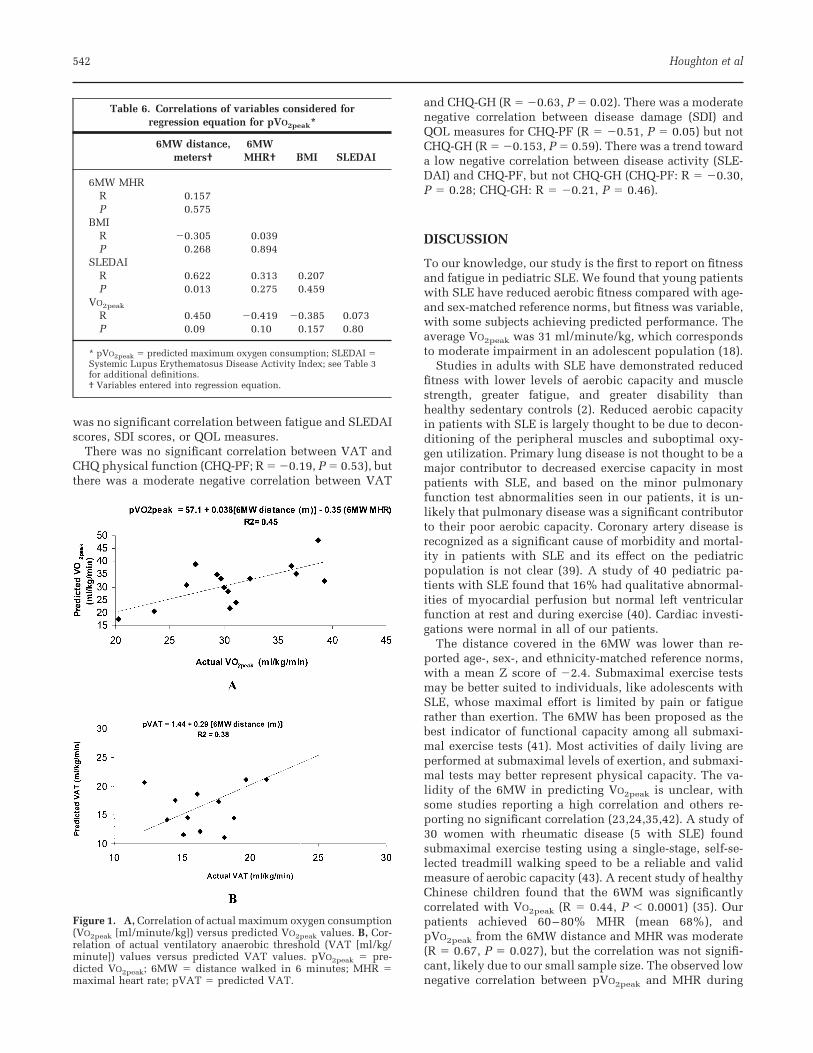
Correlations. VAT showed a moderate positive correla-tion with 6MW distance (R � 0.61, P � 0.026), whereasVO2peak and 6MW distance were positively correlated, butthe correlation was not statistically significant (R � 0.45,P � 0.09). The 6MW distance and MHR were independentvariables in stepwise regression to predict VO2peak. BMIand SLEDAI scores were not significantly correlated withVO2peak and were not entered into the regression equation(Table 6). The regression equation for predicting VO2peak
(pVO2peak) from distance walked and MHR in the 6MWwas as follows: pVO2peak (ml/minute/kg) � 57.1 � [0.038 �distance (meters)] � (�0.35 � MHR) (R � 0.67, P � 0.027,standard error of the estimate [SEE] 6.1) (Figure 1A). Theregression equation for predicting VAT (pVAT) was asfollows: pVAT (ml/minute/kg) � 1.44 � 0.029 [distance(meters)] (R � 0.61, P � 0.1, SEE 4.6) (Figure 1B).
There was no significant correlation of fatigue withVO2peak and VAT (R � 0.01 and 0.10, respectively). Thepresence/absence of fatigue and normal/subnormal VATwas not correlated (P � 0.65 by Fisher’s exact test). There
Table 4. VO2peak norms (18)*
VO2peak
Age, years Girls Boys
12, 13 40.5 � 6.6 49.4 � 8.814, 15 42.9 � 6.2 53.3 � 11.118 40.1 � 6.1 51.0 � 9.5
* Values are the mean � SD. VO2peak � maximum oxygenconsumption.
Table 5. Patient questionnaires: fatigue, habitual activity levels, and quality of life measures*
K-FSS† HAES‡ CHQ-PF CHQ-GH CHQ-SE CHQ-FA CHQ-FC
Present studyPatient 1 4.4 Active 48 59 87 87 85Patient 2 4.4 Nonactive 81 45 58 58 30Patient 3 2.8 Nonactive 89 43 94 94 85Patient 4 3.8 Nonactive 89 79 94 94 85Patient 5 3.8 Nonactive 92 60 64 64 60Patient 6 3.3 Active 89 32 66 66 30Patient 7 4.8 Active 89 57 69 69 60Patient 8 2.7 Active 64 52 80 80 85Patient 9 2.9 Nonactive 96 65 75 75 85Patient 10 6.0 Active 66 34 51 51 60Patient 11 4.2 Nonactive 96 59 62 62 60Patient 12 5.6 Nonactive 66 52 66 66 60Patient 13 2.8 Active 100 66 96 96 85Patient 14 4.4 Active 100 43 46 46 30Patient 15 1.3 Active 96 66 89 89 30Mean � SD 3.8 � 1.2 53% active 84 � 16 54 � 13 73 � 16 54 � 21 62 � 23ReferenceSLE adults, mean � SD 4.6 � 1.5Healthy adults, mean � SD 2.3 � 1.7Reference norms 88 65 82 62 60–85End-stage renal disease 73 49 68 NA NA
* K-FSS � Kids Fatigue Severity Scale; HAES � Habitual Activity Estimation Scale; CHQ � Child Health Questionnaire; PF � physical function; GH �general health; SE � self-esteem; FA � family activities; FC � family cohesion; SLE � systemic lupus erythematosus; NA � not available.† Fatigue was defined as present if K-FSS score was �3.0.‡ Active was defined as �3 hours/week.
Fitness in Pediatric Lupus 541
was no significant correlation between fatigue and SLEDAIscores, SDI scores, or QOL measures.
There was no significant correlation between VAT andCHQ physical function (CHQ-PF; R � �0.19, P � 0.53), butthere was a moderate negative correlation between VAT
and CHQ-GH (R � �0.63, P � 0.02). There was a moderatenegative correlation between disease damage (SDI) andQOL measures for CHQ-PF (R � �0.51, P � 0.05) but notCHQ-GH (R � �0.153, P � 0.59). There was a trend towarda low negative correlation between disease activity (SLE-DAI) and CHQ-PF, but not CHQ-GH (CHQ-PF: R � �0.30,P � 0.28; CHQ-GH: R � �0.21, P � 0.46).
DISCUSSION
To our knowledge, our study is the first to report on fitnessand fatigue in pediatric SLE. We found that young patientswith SLE have reduced aerobic fitness compared with age-and sex-matched reference norms, but fitness was variable,with some subjects achieving predicted performance. Theaverage VO2peak was 31 ml/minute/kg, which correspondsto moderate impairment in an adolescent population (18).
Studies in adults with SLE have demonstrated reducedfitness with lower levels of aerobic capacity and musclestrength, greater fatigue, and greater disability thanhealthy sedentary controls (2). Reduced aerobic capacityin patients with SLE is largely thought to be due to decon-ditioning of the peripheral muscles and suboptimal oxy-gen utilization. Primary lung disease is not thought to be amajor contributor to decreased exercise capacity in mostpatients with SLE, and based on the minor pulmonaryfunction test abnormalities seen in our patients, it is un-likely that pulmonary disease was a significant contributorto their poor aerobic capacity. Coronary artery disease isrecognized as a significant cause of morbidity and mortal-ity in patients with SLE and its effect on the pediatricpopulation is not clear (39). A study of 40 pediatric pa-tients with SLE found that 16% had qualitative abnormal-ities of myocardial perfusion but normal left ventricularfunction at rest and during exercise (40). Cardiac investi-gations were normal in all of our patients.
The distance covered in the 6MW was lower than re-ported age-, sex-, and ethnicity-matched reference norms,with a mean Z score of �2.4. Submaximal exercise testsmay be better suited to individuals, like adolescents withSLE, whose maximal effort is limited by pain or fatiguerather than exertion. The 6MW has been proposed as thebest indicator of functional capacity among all submaxi-mal exercise tests (41). Most activities of daily living areperformed at submaximal levels of exertion, and submaxi-mal tests may better represent physical capacity. The va-lidity of the 6MW in predicting VO2peak is unclear, withsome studies reporting a high correlation and others re-porting no significant correlation (23,24,35,42). A study of30 women with rheumatic disease (5 with SLE) foundsubmaximal exercise testing using a single-stage, self-se-lected treadmill walking speed to be a reliable and validmeasure of aerobic capacity (43). A recent study of healthyChinese children found that the 6WM was significantlycorrelated with VO2peak (R � 0.44, P � 0.0001) (35). Ourpatients achieved 60–80% MHR (mean 68%), andpVO2peak from the 6MW distance and MHR was moderate(R � 0.67, P � 0.027), but the correlation was not signifi-cant, likely due to our small sample size. The observed lownegative correlation between pVO2peak and MHR during
Table 6. Correlations of variables considered forregression equation for pVO2peak*
6MW distance,meters†
6MWMHR† BMI SLEDAI
6MW MHRR 0.157P 0.575
BMIR �0.305 0.039P 0.268 0.894
SLEDAIR 0.622 0.313 0.207P 0.013 0.275 0.459
VO2peak
R 0.450 �0.419 �0.385 0.073P 0.09 0.10 0.157 0.80
* pVO2peak � predicted maximum oxygen consumption; SLEDAI �Systemic Lupus Erythematosus Disease Activity Index; see Table 3for additional definitions.† Variables entered into regression equation.
Figure 1. A, Correlation of actual maximum oxygen consumption(VO2peak [ml/minute/kg]) versus predicted VO2peak values. B, Cor-relation of actual ventilatory anaerobic threshold (VAT [ml/kg/minute]) values versus predicted VAT values. pVO2peak � pre-dicted VO2peak; 6MW � distance walked in 6 minutes; MHR �maximal heart rate; pVAT � predicted VAT.
542 Houghton et al

submaximal exercise is consistent with physiologicchanges associated with fitness training. A reduction ofresting and submaximal HR is a sensitive response totraining, and conversely an increase in resting and sub-maximal HR is seen with detraining and deconditioning.
The most common measure of submaximal exercise in-tensity is VAT. VAT may be related to fatigue and function(19). VAT usually corresponds to 60–70% of VO2peak andis higher in trained individuals (36–38,44). One studyfound a mean � SD VAT of 60% � 9% with slightly lowerratios in older children (44). Exercise above the VAT leadsto increased anaerobic metabolism with lactate accumula-tion and secretion of stress hormones. Patients can usuallyexercise and perform activities of daily living safely belowtheir VAT. A study of 21 women with SLE without car-diopulmonary complications found low aerobic capacityand low VAT, suggesting that a low VAT may contribute tofatigue (45). In a study of women with FM, impaired VATand VO2peak were found; the majority of patients were notable to achieve maximum effort (46).
As a group, our female patients had a lower VAT thanreference norms. The VAT could not be determined in 2patients because of erratic breathing patterns; this problemhas been reported by other researchers (19,47). A lowerVAT may be related to early fatigue, because some activi-ties of daily living may be above an individual’s VAT,leading to an inability to sustain that level of activity.However, we did not find a correlation between presence/absence of fatigue and normal/subnormal VAT in our pa-tients. In clinical practice, exercise prescription using theHR at VAT as a target HR may help guide conditioning andtraining programs. Improvements in VAT are seen beforeVO2peak during aerobic training, and serial exercise testingmay allow monitoring of physical fitness.
We used measures of isometric strength for ease of test-ing and reproducibility in the clinic. However, isometricstrength testing does not give any information on muscularendurance and, therefore, does not necessarily correlatewith aerobic fitness. Anaerobic fitness depends predomi-nantly on nonoxidative energy turnover and is related tolocal characteristics of working muscle groups. Eight(53%) patients demonstrated decreased rectus femorisstrength with Z scores of �2 or lower (25). Anaerobicfitness was not tested in this study, but in future studies itwill be interesting to examine because there is indicationof a positive relationship between functional ability andanaerobic fitness in other pediatric chronic rheumatic dis-ease populations (48).
The K-FSS was used as a measure of fatigue; this is anew measure based on the FSS, which was modified byour group for use in pediatric populations. The FSS is awell-validated questionnaire developed for adults thatmeasures the impact of fatigue on activities of daily living(12). This instrument has been used in a number of studiesof fatigue in adult patients with SLE, and has been shownto be stable over time, sensitive to clinical change, and ableto discriminate between fatigue and depressive symptoms(5,12). Comparisons have not previously been made be-tween pediatric and adult patients with SLE. Mean � SDFSS scores are reported as 4.6 � 1.5 and 2.3 � 1.7 foradults with SLE and healthy adults, respectively. Our av-
erage score of 3.8 was lower than that for adults with SLEbut higher than that for healthy adults. Ten of our patients(67%) reported fatigue as a significant problem. Referencevalues for healthy children are not currently available forcomparison. The reported fatigue had no significant corre-lation with aerobic fitness or QOL measures.
QOL was measured with the CHQ. Our patients hadlower general health perceptions and self-esteem than areference school population, but scored higher than anend-stage renal disease population (28). Our patients hadmore disruption of family functioning, with lower scoresfor family activities, but not family cohesion. Referencevalues for family functioning are not available for otherchronic diseases, but it is intuitive that caring for a childwith chronic illness may disrupt some family activitiesand scheduling. There were no significant differences be-tween our patients as a group and a reference sample onmeasures of physical functioning, social and emotionalfunctioning, mental health and behavior, and pain andpain behaviors. There was a moderate negative correlationbetween measures of physical function and disease dam-age. There was no significant correlation between diseaseactivity and QOL or fatigue. The SLEDAI does not includesubjective symptoms such as fatigue, and this may par-tially explain the low correlation with patient disease ac-tivity, QOL, or fatigue. Use of the SLAM (Systemic LupusActivity Measure) in future studies should be consideredbecause scoring relies on the reporting of symptoms by thepatient rather than objective documentation as required bythe SLEDAI (49).
This study has several limitations. Small numbers ofpatients, enrollment bias, and absence of controls limitgeneralization of our results. Procedural limitations in-clude measures of fatigue and the exercise protocol. TheK-FSS does not have normative data for young persons andits use is exploratory. The same exercise protocol was usedfor all patients to standardize testing, but individual pro-tocols may have allowed for maximal tests in all patients.Two patients (patients 3 and 6) did not achieve a maximaleffort. Not achieving a maximal effort may be due to asubmaximal test or termination of the test prior to exhaust-ing cardiopulmonary reserve, possibly due to mental ormuscular fatigue. The exercise test is a maximal test tovolitional fatigue and should ideally last 8–12 minutes.The standardized protocol was based on studies con-ducted in adults with SLE but underestimated our pa-tients’ fitness, with exercise lasting �15 minutes in 8(53%) patients, thus becoming more of an endurance testthan a maximal test (17). Normative VO2peak data are forwhite children using the Bruce protocol (both speed andslope increase from one stage to the next) (18). Ethnicdifferences may exist and our protocol used a modifiedBalke protocol (fixed speed with slope increase from onestage to the next) (17).
Few randomized control studies have looked at exerciseintervention in the adult SLE population and all havedemonstrated either no effect or a positive effect on fatigueand exercise capacity, with no worsening of disease activ-ity. Supervised cardiovascular training programs reportsignificant improvements in fitness, whereas unsupervisedhome-based interventions report improved measures of
Fitness in Pediatric Lupus 543

fatigue or QOL without significant improvements in aero-bic fitness (50–55). Exercise intervention studies involvingthe pediatric SLE population have not been published.
In summary, children and young persons with SLE havelower aerobic fitness than reference norms. The 6MW maybe used as a marker of aerobic fitness but it is preferable todetermine VO2peak with a graded exercise test. This studyconfirms that fatigue is a significant symptom in youngpatients with SLE. The application of fatigue measures inyoung persons is exploratory. The relationship betweenfatigue and aerobic fitness and QOL is not clear. Futurestudies are needed to determine the validity and utility offatigue measures in young patients and to research theeffects of exercise therapy on fitness, VAT, fatigue, andQOL. Exercise capacity is increasingly recognized as animportant predictor of mortality (10,11). Fitness as mea-sured by VO2peak may emerge as an important outcomemeasure for children and young persons with SLE.
ACKNOWLEDGMENTSThanks to Natalie Taha, BSc, HKinetics, and Astird De-Souza, MSc, HKinetics, for their help with exercise testing.
AUTHOR CONTRIBUTIONS
Dr. Houghton had full access to all of the data in the study andtakes responsibility for the integrity of the data.Study design. Houghton, Tucker, McKenzie, Potts.Acquisition of data. Houghton, Potts.Analysis and interpretation of data. Houghton, Tucker, McKen-zie, Potts.Manuscript preparation. Houghton, Tucker, McKenzie, Potts.
REFERENCES
1. Tucker LB, Menon S, Schaller JG, Isenberg DA. Adult- andchildhood-onset systemic lupus erythematosus: a comparisonof onset, clinical features, serology, and outcome. Br J Rheu-matol 1995;34:866–72.
2. Tench C, Bentley D, Vleck V, McCurdie I, White P, D’Cruz D.Aerobic fitness, fatigue, and physical disability in systemiclupus erythematosus. J Rheumatol 2002;29:474–81.
3. Wysenbeek AJ, Leibovici L, Weinberger A, Guedj D. Fatigue insystemic lupus erythematosus: prevalence and relation to dis-ease expression. Br J Rheumatol 1993;32:633–5.
4. Petty RE, Laxer RM. Systemic lupus erythematosus. In:Cassidy JT, Petty RE, Laxer R, Lindsley C, editors. Textbook ofpediatric rheumatology. 5th ed. Philadelphia: Elsevier; 2005.p. 342–91.
5. Krupp LB, LaRocca NG, Muir J, Steinberg AD. A study offatigue in systemic lupus erythematosus. J Rheumatol 1990;17:1450–2.
6. Zonana-Nacach A, Roseman JM, McGwin G Jr, Friedman AW,Baethge BA, Reveille JD, et al, and the LUMINA Study Group.Systemic lupus erythematosus in three ethnic groups. VI.Factors associated with fatigue within 5 years of criteria di-agnosis. Lupus 2000;9:101–9.
7. McKinley PS, Ouellette SC, Winkel GH. The contributions ofdisease activity, sleep patterns, and depression to fatigue insystemic lupus erythematosus: a proposed model. ArthritisRheum 1995;38:826–34.
8. Tench CM, McCurdie I, White PD, D’Cruz DP. The prevalenceand associations of fatigue in systemic lupus erythematosus.Rheumatology (Oxford) 2000;39:1249–54.
9. Wang B, Gladman DD, Urowitz MB. Fatigue in lupus is notcorrelated with disease activity. J Rheumatol 1998;25:892–5.
10. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood
JE. Exercise capacity and mortality among men referred forexercise testing. N Engl J Med 2002;346:793–801.
11. Gulati M, Black HR, Shaw LJ, Arnsdorf MF, Merz CN, LauerMS, et al. The prognostic value of a nomogram for exercisecapacity in women. N Engl J Med 2005;353:468–75.
12. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fa-tigue severity scale: application to patients with multiplesclerosis and systemic lupus erythematosus. Arch Neurol1989;46:1121–3.
13. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, RothfieldNF, et al. The 1982 revised criteria for the classification ofsystemic lupus erythematosus. Arthritis Rheum 1982;25:1271–7.
14. Hochberg MC, for the Diagnostic and Therapeutic CriteriaCommittee of the American College of Rheumatology. Updat-ing the American College of Rheumatology revised criteria forthe classification of systemic lupus erythematosus [letter].Arthritis Rheum 1997;40:1725.
15. Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Still-man RJ, Van Loan MD, et al. Skinfold equations for estimationof body fatness in children and youth. Hum Biol 1988;60:709–23.
16. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing astandard definition for child overweight and obesityworldwide: international survey. BMJ 2000;320:1240–3.
17. Bar-Or O, Rowland TW. Procedures for exercise testing inchildren. In: Pediatric exercise medicine. Champaign (IL):Human Kinetics; 2004. p. 343–67.
18. Ahmad F, Kavey RE, Kveselis DA, Gaum WE, Smith FC.Responses of non-obese white children to treadmill exercise.J Pediatr 2001;139:284–90.
19. Wasserman K, Whipp BJ, Koyl SN, Beaver WL. Anaerobicthreshold and respiratory gas exchange during exercise.J Appl Physiol 1973;35:236–43.
20. Beaver WL, Wasserman K, Whipp BJ. A new method fordetecting anaerobic threshold by gas exchange. J Appl Physiol1986;60:2020–7.
21. ATS Committee on Proficiency Standards for Clinical Pulmo-nary Function Laboratories. ATS statement: guidelines for thesix-minute walk test. Am J Respir Crit Care Med 2002;166:111–7.
22. Eston RG, Lamb KL, Bain A, Williams AM, Williams JG.Validity of a perceived exertion scale for children: a pilotstudy. Percept Mot Skills 1994;78:691–7.
23. Guyatt GH, Sullivan MJ, Thompson PJ, Fallen EL, Pugsley SO,Taylor DW, et al. The 6-minute walk: a new measure ofexercise capacity in patients with chronic heart failure. CanMed Assoc J 1985;132:919–23.
24. Nixon PA, Joswiak ML, Fricker FJ. A six-minute walk test forassessing exercise tolerance in severely ill children. J Pediatr1996;129:362–6.
25. Beenakker EA, van der Hoeven JH, Fock JM, Maurits NM.Reference values of maximum isometric muscle force ob-tained in 270 children aged 4-16 years by hand-held dyna-mometry. Neuromuscul Disord 2001;11:441–6.
26. Hay JA. Development and testing of the Habitual ActivityEstimation scale. In: Armstrong N, Weisman J, Kirby B, edi-tors. Children and exercise XIX: promoting health and well-being. XIXth International Symposium of Pediatric WorkPhysiology. Exeter (WA): Singer; 1997. p. 125–9.
27. Healthy Active Living Committee. Healthy active living forchildren and youth. Paediatr Child Health 2002;7:339–45.
28. Landgraf JL, Abetz L, Ware JE. The CHQ user’s manual. 1st ed.Boston: The Health Institute, New England Medical Center;1996.
29. Bombardier C, Gladman DD, Urowitz MB, Caron D, ChangCH, and the Committee on Prognosis Studies in SLE. Deriva-tion of the SLEDAI: a disease activity index for lupus patients.Arthritis Rheum 1992;35:630–40.
30. Cook RJ, Gladman DD, Pericak D, Urowitz MB. Prediction ofshort term mortality in systemic lupus erythematosus withtime dependent measures of disease activity. J Rheumatol2000;27:1892–5.
31. Gladman DD, Urowitz MB, Goldsmith CH, Fortin P, Ginzler E,
544 Houghton et al

Gordon C, et al. The reliability of the Systemic Lupus Inter-national Collaborating Clinics/American College of Rheuma-tology Damage Index in patients with systemic lupus ery-thematosus. Arthritis Rheum 1997;40:809–13.
32. Wolfe F. Fibromyalgia. Rheum Dis Clin North Am 1990;16:681–98.
33. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,Goldenberg D, et al. The American College of Rheumatology1990 criteria for the classification of fibromyalgia: report ofthe Multicenter Criteria Committee. Arthritis Rheum 1990;33:160–72.
34. Geiger R, Strasak A, Treml B, Gasser K, Kleinsasser A, FischerV, et al. Six-minute walk test in children and adolescents.J Pediatr 2007;150:395–9.
35. Li AM, Yin J, Yu CC, Tsang T, So HK, Wong E, et al. Thesix-minute walk test in healthy children: reliability and va-lidity. Eur Respir J 2003;25:1057–60.
36. Reybrouck T, Weymans M, Stijns H, Knops J, van der Hau-waert L. Ventilatory anaerobic threshold in healthy children:age and sex differences. Eur J Appl Physiol Occup Physiol1985;54:278–84.
37. Weltman A, Katch VL. Relationship between the onset ofmetabolic acidosis (anaerobic threshold) and maximal oxygenuptake. J Sports Med Phys Fitness 1979;19:135–42.
38. Washington RL, van Gundy JC, Cohen C, Sondheimer HM,Wolfe RR. Normal aerobic and anaerobic exercise data forNorth American school-age children. J Pediatr 1988;112:223–33.
39. Schanberg LE, Sandborg C. Dyslipoproteinemia and prema-ture atherosclerosis in pediatric systemic lupus erythemato-sus. Curr Rheumatol Rep 2004;6:425–33.
40. Gazarian M, Feldman BM, Benson LN, Gilday DL, Laxer RM,Silverman ED. Assessment of myocardial perfusion and func-tion in childhood systemic lupus erythematosus. J Pediatr1998;132:109–16.
41. Solway S, Brooks D, Lacasse Y, Thomas S. A qualitativesystematic overview of the measurement properties of func-tional walk tests used in the cardiorespiratory domain. Chest2001;119:256–70.
42. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM.Two-, six-, and 12-minute walking tests in respiratory disease.Br Med J (Clin Res Ed) 1982;284:1607–8.
43. Minor MA, Johnson JC. Reliability and validity of a submaxi-mal treadmill test to estimate aerobic capacity in women withrheumatic disease. J Rheumatol 1996;23:1517–23.
44. Cooper DM, Weiler-Ravell D, Whipp BJ, Wasserman K.Growth-related changes in oxygen uptake and heart rate dur-ing progressive exercise in children. Pediatr Res 1984;18:845–51.
45. Sakauchi M, Matsumura T, Yamaoka T, Koami T, Shibata M,Nakamura M, et al. Reduced muscle uptake of oxygen duringexercise in patients with systemic lupus erythematosus.J Rheumatol 1995;22:1483–7.
46. Valim V, Oliveira LM, Suda AL, Silva LE, Faro M, Neto TL, etal. Peak oxygen uptake and ventilatory anaerobic threshold infibromyalgia. J Rheumatol 2002;29:353–7.
47. Davis JA, Vodak P, Wilmore JH, Vodak J, Kurtz P. Anaerobicthreshold and maximal aerobic power for three modes ofexercise. J Appl Physiol 1976;41:544–50.
48. Takken T, van der Net J, Helders PJ. Relationship betweenfunctional ability and physical fitness in juvenile idiopathicarthritis patients. Scand J Rheumatol 2003;32:174–8.
49. Liang MH, Socher SA, Larson MG, Schur PH. Reliability andvalidity of six systems for the clinical assessment of diseaseactivity in systemic lupus erythematosus. Arthritis Rheum1989;32:1107–18.
50. De Carvalho MR, Sato EI, Tebexreni AS, Heidecher RT,Schenkman S, Neto TL. Effects of supervised cardiovasculartraining program on exercise tolerance, aerobic capacity, andquality of life in patients with systemic lupus erythematosus.Arthritis Rheum 2005;53:838–44.
51. Tench CM, McCarthy J, McCurdie I, White PD, D’Cruz DP.Fatigue in systemic lupus erythematosus: a randomized con-trolled trial of exercise. Rheumatology (Oxford) 2003;42:1050–4.
52. Daltroy LH, Robb-Nicholson C, Iversen MD, Wright EA, LiangMH. Effectiveness of minimally supervised home aerobictraining in patients with systemic rheumatic disease. Br JRheumatol 1995;34:1064–9.
53. Robb-Nicholson LC, Daltroy L, Eaton H, Gall V, Wright E,Hartley LH, et al. Effects of aerobic conditioning in lupusfatigue: a pilot study. Br J Rheumatol 1989;28:500–5.
54. Ramsey-Goldman R, Schilling EM, Dunlop D, Langman C,Greenland P, Thomas RJ, et al. A pilot study on the effects ofexercise in patients with systemic lupus erythematosus. Ar-thritis Care Res 2000;13:262–9.
55. Clarke-Jenssen AC, Fredriksen PM, Lilleby V, Mengshoel AM.Effects of supervised aerobic exercise in patients with sys-temic lupus erythematosus: a pilot study. Arthritis Rheum2005;53:308–12.
Fitness in Pediatric Lupus 545