Embed Size (px)
Citation preview

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06578
MULTICENTRIC LYMPHOMA
The term multicentric lymphoma is not synonymous with multiple lymph node involvement. Although cats are often described as having multicentric lymphoma, where multiple organ systems are involved, this rarely includes the generalised lymphadenopathy that is often seen in dogs. This category of lymphoma usually includes cats with liver, spleen or peripheral/intra-abdominal lymph node involvement.
Clinical signs range from vague malaise, weight loss or anorexia to more acute signs of liver failure. Radiography and ultrasound examination of the abdomen may indicate changes in the size, shape and echotexture of the parenchymal organs, thus prompting needle aspi-rates in the first instance. It is worth remembering that liver infiltration and/or elevated biochemical parameters do not equate to liver failure and changes may be revers-ible with appropriate treatment. Compromised liver function will require reductions in cytotoxic drug dos-ages and careful monitoring for signs of toxicity.
If generalised lymphadenopathy occurs in cats and lymphoma is suspected, definitive histology is required to avoid misdiagnosis of healthy, younger cats with non-
CO
MP
AN
ION
AN
IMA
L P
RA
CT
ICE
THIS article, the second of two on feline lymphoma, discusses how the disease can present to the veterinarian. Lymphoma is a differential diagnosis for a variety of clinical presentations in cats and can occur in, or spread to, any anatomical site that contains lymphoid tissue. A regionally localised disease must be assumed to have a systemic component unless proved otherwise. Thus, ascribing a disease to a particular anatomical form (ie, mediastinal, alimentary or multicentric) can be difficult and may have led to inaccuracies in reporting of the disease in the literature. In addition to these commonly recognised forms, cutaneous, ocular, central nervous system, tracheal, renal, nasal and pulmonary forms are also recognised. These various anatomical presentations of feline lymphoma may come to be regarded as specific disease entities in their own right as more is learnt about the pathogenesis and biology of feline lymphoid neoplasias, but are currently best considered as manifestations of a disease continuum. Rather than struggling to ascribe an individual case to a particular anatomical form, the clinician should be aware that the main aim of staging is simply to document all areas of involvement. Initial clinical investigations will pertain to the organ system recognised in the presentation of disease, but full staging is always required and should include diagnostic investigation of the whole patient wherever possible. This was discussed further in Part 1, published in the last issue, which reviewed the principles of diagnosis and management in feline lymphoma cases (In Practice, October 2006, volume 28, pp 516-524).
Feline lymphoma
2. Specific disease presentations ALISON HAYES
In Practice (2006) 28, 578-585
specific immune stimulation. Two studies have alluded to this: in the first, lymphadenopathy was reported to regress over time in a group of younger cats diagnosed with lymphoma and presenting with generalised lym-phadenopathy (Mooney and others 1987b) and, in the
Alison Hayes graduated from Glasgow in 1991 and spent five years in mixed and small animal practice in north-west England. She subsequently undertook a three-year Blue Cross residency in oncology at the Animal Health Trust in Newmarket, where she is now a clinical oncologist. She holds the RCVS certificate in veterinary radiology and an MSc in clinical oncology from the University of Birmingham medical school.
Four-year-old female domestic longhaired cat, which presented with signs of upper respiratory stridor and was FeLV-negative. Third eyelid protrusion and reduced retropulsion were noted, which were more marked on the right side. Nasal biopsy confirmed lymphoma and, after complete staging, chemotherapy was commenced with radiation therapy on relapse. Generalised lymphadenopathy is rarely a feature of lymphoma in cats
Submandibular lymphadenopathy in a domestic shorthaired cat of unknown age. Multicentric lymphomas such as this rarely manifest as generalised peripheral lymphadenopathy, which is common in dogs. In this cat, there was marked, localised, unilateral enlargement of the submandibular node (arrow). Picture, Lorraine Fleming
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06 579
second, peripheral lymph node enlargement in 14 cats led to lymphoma in only one cat, with 13 cats undergo-ing spontaneous lymph node regression (Moore and oth-ers 1986). In the latter study, six out of nine cats tested had feline leukaemia virus (FeLV) antigen detected in the blood and had similar histology findings to kittens developing lymphadenopathy following experimental FeLV infection. In addition to histology, immunohisto-chemistry and FeLV antigen detection may be helpful in determining a definitive diagnosis. If there is any ambi-guity, clinical monitoring and re-biopsy is advocated before making treatment decisions.
MEDIASTINAL LYMPHOMA
Mediastinal disease is a common presentation of lym-phoma. Cats are often dyspnoeic, although sometimes this is not recognised by owners. Radiographic changes include an anterior thoracic mass effect with or with-out a pleural effusion. The thymus, mediastinal, pre-sternal and other intrathoracic lymph nodes may all be affected. Lymphadenopathy may be appreciated in the thoracic inlet and lower cervical area. Displacement of the apex beat and dulled lung sounds will be heard on clinical examination. Regurgitation and dysphagia may also be reported by owners. Cytology of pleural fluid is usually supportive of the diagnosis, although histol-ogy is advisable wherever possible, especially in older cats that are FeLV-negative, in which the disease must be differentiated from thymoma, which may be treated surgically.
Ultrasound examination of the thorax facilitates guided fine needle aspiration or core biopsy of abnormal tissue. The presence of pleural fluid can aid ultrasonog-raphy, but due care is needed and thoracocentesis may be required for initial stabilisation before further inves-tigation can take place. In cats, the right second to third or third to fourth intercostal space is a commonly used site for this. Care should be taken to avoid the intercostal vessels along the caudal aspect of the rib, while directing the needle along the thoracic wall to avoid lung trauma. A butterfly catheter or short over-the-needle catheter can be used, with or without extension tubing, and attached to a three-way tap and syringe for short-term drainage. The first fluid that is withdrawn should be placed into EDTA and plain tubes for cellular and bio-chemical analysis.
The mainstay of treatment for mediastinal lymphoma is cytotoxic chemotherapy, although low-dose radiation therapy to consolidate treatment can lead to durable remis-sions (Elmsie and others 1991). Young, FeLV-negative, Siamese cats may be overrepresented, but can respond well to chemotherapy – often achieving complete and durable remissions, allowing treatment to be stopped.
ALIMENTARY LYMPHOMA
Alimentary (or gastrointestinal) lymphoma is frequently seen in cats. The small and large intestines, oral cavity, oesophagus, stomach, mesenteric nodes, pancreas and liver can all be involved. Presenting signs include weight loss, anorexia, lethargy and diarrhoea. Vomiting is not a consistent feature of the disease in cats. Intestinal involvement is generally regarded as a diffuse bowel
disease, but may initially manifest as a solitary, focal mass detectable on abdominal palpation. Alternatively, abdominal palpation can reveal diffuse, cord-like bowel thickening. Abdominal ultrasonography is essential for diagnosis, staging and monitoring, and facilitates guided core and needle biopsy. Bowel thickening, loss of motili-ty and layering, hypoechogenicity and lymphadenopathy are characteristic changes seen on ultrasound examina-tion (Penninck and others 1994).
When the disease presents as diffuse gastrointestinal changes, diagnosis may be achieved by ultrasound-guided needle or endoscopic grab biopsies prior to commencing chemotherapy. For more solitary masses, fine needle aspi-ration or needle-core techniques can be used. A surgical approach is required if definitive diagnosis is not achieved with non-invasive techniques such as Tru-cut style biop-sies or when there is an immediate need to relieve bowel obstruction or intussusception. Superficial grab biopsies obtained endoscopically should be interpreted with cau-tion, as these may underdiagnose lymphoma involving the
Right lateral recumbent (above) and dorsoventral (left) projections of the thorax showing a mediastinal lymphoma in a 10-year-old domestic shorthaired cat. The thoracic air space is almost obliterated by a homogeneous soft tissue opacity which obscures the cardiac silhouette and displaces the trachea dorsally and to the right (arrows). Only the dorsocaudal part of the right lung remains aerated. The disease must be distinguished from thymoma, which may be treated surgically. Ultrasound-guided Tru-cut biopsy can provide a definitive diagnosis
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06580
deeper layers and overestimate the importance of inflam-matory bowel changes seen more superficially.
Treatment can be surgical, medical or a combination of the two. Limitations apply to each form of treatment. Chemotherapy can be used as a first-line treatment if a definitive diagnosis has already been achieved by non-invasive means. However, large, focal mass lesions treated with chemotherapy can result in a full thick-ness defect once malignant lymphoid tissue is lost and close monitoring is required during the initial induction phase. Surgical resection of large areas of bowel does not appear to prolong survival compared with cats treat-ed medically. Chemotherapy is advocated after recovery from surgical diagnostic and therapeutic procedures.
Cats with low-grade gastrointestinal lymphoma have been shown to respond well to a combination of pred-nisolone (10 mg per cat per day) and chlorambucil (15 mg/m2 daily for four days, repeated every three weeks), achieving a median survival time of 22·8 months for the 67 per cent of animals that achieved complete remission (Fondacaro and others 1999). In another study, which did not differentiate the grade of disease, 71 per cent of cats with gastrointestinal lymphoma achieved complete remission with a median survival time of 259 days and an overall median survival time for all cats of 201 days following treatment with a doxorubicin-based, six-drug protocol (Rassnick and others 1999). However, two other
studies have reported outcomes suggesting that cats with gastrointestinal lymphoma may respond less favourably to combination protocols than cats with other forms of the disease. Zwahlen and others (1998) reported that, of 21 cats treated with a doxorubicin-based, six-drug protocol, 38 per cent achieved complete remission with a median survival time of 291 days, and an overall sur-vival time of 280 days for all cats. In the second study, Mahony and others (1995) reported that, of 27 cats treat-ed with cyclophosphamide, vincristine and prednisolone (COP), 33 per cent achieved complete remission, with a median survival time of 213 days for those animals in complete remission and an overall survival time of 50 days.
As with other forms of the disease, the best chemother-apy protocol for gastrointestinal lymphoma is probably yet to be determined. However, from the limited studies to date, it appears that COP alone is probably inadequate for the management of gastrointestinal lymphoma.
RENAL LYMPHOMA
Renal lymphoma is the most common renal tumour in cats and often presents with acute-onset renal insuffi-ciency, anorexia, weight loss and polyuria/polydipsia. Bilaterally enlarged, and sometimes irregular, kidneys can be found on palpation of the abdomen and confirmed radiographically. An apparent unilateral presentation can be encountered, although the disease is considered to be bilateral in all cases. Unsuspected renal involvement can be discovered during ultrasound examination if loss of corticomedullary definition is seen. This can be due to cortical infiltration by neoplastic lymphocytes. The diagnosis must be confirmed with fine needle aspira-tion or Tru-cut style biopsy. There may be an association between renal and nasal lymphoma, and also between renal and central nervous system lymphoma, but this is still unproven.
Treatment for renal lymphoma is always drug-based and can result in a rapid resolution of azotaemia, leav-ing relatively undamaged, functional kidneys. Surgical removal of a kidney for diagnostic purposes should be unnecessary and is not warranted from a therapeutic
Right lateral recumbent projection of the abdomen of a seven-year-old domestic shorthaired cat with renal lymphoma. There is marked enlargement of both kidneys (cranial and caudal pole of each kidney shown by arrows), which has displaced the abdominal contents caudoventrally. These are typical signs of this condition in cats. This cat also had disseminated signs of disease, suggested by the pleural effusion
Lymphoma or IBD?
If there is a relationship between inflammatory bowel disease and lymphoma, it is a contentious one. The pathological classification of feline lymphocytic enteric disease has not yet been fully elucidated. Researchers have found that epitheliotropic intestinal lymphoma, characterised by infiltration of the super-ficial layers with small lymphocytes, can only be reliably differentiated from inflammatory bowel disease by identifying clonality on immunohistochemistry (Carreras and others 2003) and future molecular studies may aid further under-standing. Currently, it is still unclear whether inflammatory bowel disease is a reaction or a precursor to lymphoma. Although it is tempting to regard these two diseases as a continuum of each other, this may prove to be inaccurate. Cats that show a poor response to inflammatory bowel disease therapy should be reviewed, and a diagnosis of lymphoma reinvestigated.
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06 581
perspective. Survival times can be prolonged for cats with renal lymphoma; in one study involving 11 cats with disease confined only to the kidneys and treated with a multidrug protocol, the median survival time was 396 days (Mooney and others 1987a). The degree of azo-taemia should not be regarded as a prognostic indicator in cats with renal lymphoma. It is important to realise that reported median survival times may be unrepre-sentative of renal lymphoma per se, due to the possible link with central nervous system lymphoma and the more guarded prognosis that this carries.
Supportive care is required in cases of renal lympho-ma, especially in the early stages of diagnosis and treat-ment. Cytotoxic drug dose reductions may be necessary in sick patients. Drug doses may be increased after the initial azotaemia has resolved. Special care should be
Right lateral recumbent (above) and ventrodorsal (left) projections of the abdomen of a nine-year-old domestic shorthaired cat with renal lymphoma. Note the asymmetry of the left and right renal silhouettes. The left kidney is enlarged, with an irregular, globoid shape and lies more ventrally than normal (white arrows). The right kidney is also enlarged, but retains its normal shape and position in the right dorsal abdomen (black arrows). Renal involvement is often bilateral, but this may not be clinically apparent, and enlargement may not be symmetrical
Ultrasound image showing a normal feline kidney
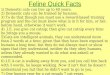
(above left) Ultrasound image from a nine-year-old domestic shorthaired cat showing renal lymphoma in the left kidney prior to treatment. The kidney is enlarged, measuring 50·91 mm along the long axis (normal range 37 to 44 mm). A hypoechoic rim surrounds the kidney, indicating subcapsular fluid and cellular infiltration (white arrows). Poor corticomedullary definition and patchy areas of increased echogenicity give the cortex a mottled appearance (black arrows). This loss of corticomedullary definition raises the suspicion of lymphoma and, although marked in this case, a more subtle appearance without other renal changes should prompt the clinician to consider a diagnosis of lymphoma. (above right) Ultrasound image from the same cat following chemotherapy with cyclophosphamide, vincristine and prednisolone. A marked reduction in renal size can be appreciated, with the kidney now measuring about 41 mm in length. There is also a decrease in the amount of subcapsular fluid and almost normal corticomedullary definition (arrows), although the mottled appearance of the cortex remains at this stage. Renal lymphoma can respond rapidly to chemotherapy without major medical complications; such changes should not necessarily preclude an attempt at induction therapy
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06582
taken with those drugs that require any degree of renal excretion (eg, cyclophosphamide). If used, doxorubicin should be administered with pre- and post-treatment fluid therapy; extreme care should be taken with cats with renal lymphoma, as this drug is nephrotoxic in this species.
CENTRAL NERVOUS SYSTEM LYMPHOMA
Lymphoma can affect the brain or spinal cord either as a main presenting sign or as a sign of progressive disease in cats undergoing treatment. Most cats with central nerv-ous system involvement will also have lymphoma in sites other than the central nervous system. In the past, spinal
Transverse (left) and dorsal (right) T2-weighted magnetic resonance images of the cervical spine of an 18-year-old domestic shorthaired cat with a three-week history of progressive tetraplegia. An extradural lymphoma can be seen as a roughly ovoid, hyperintense, well-defined mass within the vertebral canal and there is marked cord compression. A narrow, hyperintense band between the mass and the cord corresponds to cerebrospinal fluid that is located extradurally; this may respond to chemotherapy as drugs do not have to cross the blood–brain barrier to reach the target site
Bilaterally enlarged kidneys due to renal lymphoma seen at postmortem examination. There are multifocal, nodular lymphomatous infiltrates throughout the cortex, which is swollen. Picture, Mark Bestbier
Fine needle aspirate cytology from a cat with renal lymphoma. Normal lymphocytes have a nuclear diameter approximately the same size as a red blood cell (black arrow). The nucleated lymphocytes (white arrows) have enlarged nuclei, approximately two to four times that of a red blood cell, and scant cytoplasm. Magnification X40. Picture, Mark Bestbier
Histology of a biopsy sample from a cat with renal lymphoma showing an interstitial infiltrate of malignant lymphocytes with a moderate variation in nuclear size and shape. Loss of function can be reversible with prompt treatment. Haematoxylin and eosin, magnification X10. Picture, Mark Bestbier
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06 583
lymphoma may have occurred more commonly, princi-pally in FeLV-positive cats, but lymphoma in the brain was reported less frequently and in older, FeLV-negative cats. Clinical signs of brain involvement include irrita-bility, seizures, circling, blindness, cranial nerve defi-cits and nystagmus. With spinal lymphoma, the onset of signs can be acute or insidious, and focal hyperaesthesia prior to clinical dysfunction has been reported. Paresis and ataxia with a rapidly deteriorating clinical course are common.
Definitive diagnosis can be difficult to achieve and may account for the relative under-reporting of brain involvement. Computed tomography or magnetic reso-nance imaging may detect a focal mass lesion, or a more infiltrative or widespread pattern of change. An accu-rate diagnosis may come from sampling other distant sites that are thought to be involved. Cerebrospinal fluid analysis may demonstrate malignant cells, but negative findings do not rule out lymphoma. The expected high-er incidence of spinal lymphoma compared with lym-phomas in the brain was not seen in a recent review of cases at the Animal Health Trust. This may reflect the changing face of feline lymphoma due to its FeLV/feline immunodeficiency virus associations.
Drug-based protocols for brain lymphoma may achieve less than expected for other forms of lympho-ma, as most conventional cytotoxic drugs have minimal access across the blood–brain barrier. Protocols con-taining cytosine arabinoside have been advocated in an
attempt to access affected areas. However, more success is generally achieved with radiation therapy, usually in conjunction with chemotherapy. Survival times of up to seven months have been reported, but usually the prog-nosis is regarded as poor. Spinal lymphoma is mainly extradural and thus should respond more favourably to drug-based therapies, although parenchymal extension can occur. Surgical decompression of the spine or adju-vant, low-dose radiation therapy may be considered on an individual case basis. Survival is affected as much by disease response to chemotherapy as by the timing of decompression, which can cause permanent neurological damage. Bone marrow analysis may yield a definitive diagnosis without the need for spinal surgery.
OCULAR LYMPHOMA
Ocular lymphoma can be unilateral or bilateral, and can precede the onset of systemic disease in many (but not all) cats. Any part of the eye and retrobulbar space can be affected. The uvea is most commonly affected and can show either diffuse or nodular changes. When other, systemic sites are thought to be involved, they should be sampled to help yield a definitive diagnosis. If an exact aetiology cannot be established, symptomatic treatment for uveitis can be implemented with regular re-evalua-tion. If there is a gross tumour within the eye and other sites are not involved, enucleation can be performed. In
Transcorneal ultrasound scan of lymphoma in the retrobulbar space of a nine-year-old domestic shorthaired cat. An ill-defined, hypoechoic mass in the medial part of the orbit causes indentation of the globe (white arrows). There is also disruption of the hyperechoic line that represents the bony medial wall of the orbit (black arrows). Oral examination revealed a mass in the pterygopalatine fossa, biopsy of which confirmed lymphoma
Eight-year-old Persian cat with ocular changes associated with lymphoma. Diffuse inflammation and thickening of the iris was accompanied by miosis and keratic precipitates on the corneal endothelium
Ocular changes associated with lymphoma in a cat of unknown age. There is localised thickening and inflammation of the iris, most marked between 9 and 12 o’clock
Ocular changes associated with lymphoma in an 11-year-old domestic shorthaired cat. Diffuse inflammation and thickening of the lateral part of the iris can be seen together with distortion of the pupil and a cottage cheese-like deposit in the anterior chamber. Mild corneal oedema can also be appreciated. This cat additionally had retinal detachment and bilateral panuveitis
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06584
experienced hands, aqueocentesis may yield a diagnosis in some cases, thus permitting chemotherapy to be start-ed without sacrificing the eye.
As with other forms of feline lymphoma, when ocu-lar lymphoma is diagnosed, the possibility of systemic disease should prompt the use of adjuvant chemotherapy, although the clinician should be aware that some long-term survivors have been reported following enucleation alone.
TRACHEAL LYMPHOMA
Tracheal lymphoma is an uncommon but well recog-nised form of feline lymphoma. Cats can present with dyspnoea, wheezing, cyanosis, coughing and lethargy (Brown and others 2003). Lesions can be visualised on plain radiography and bronchoscopy will aid collec-tion of material for cytology. Successful treatment with chemotherapy has been reported, although radiation therapy can be used as a primary treatment modality, or as an adjunct to chemotherapy. As systemic disease can be seen at presentation or relapse, it is safest to assume that this form of lymphoma is part of a systemic dis-ease and implement localised treatment as an adjunct to systemic therapy.
NASAL LYMPHOMA
Nasal lymphoma is also well recognised in cats. Affected animals can present with upper respiratory stridor, sneezing, nasal discharge, epiphora, and facial pain or deformation. Deviation or poor retropulsion of the globe should alert the clinician to the possibility of orbital extensions. Although radiographic displacement of midline structures, an increase in soft tissue opac-ity, loss of turbinate detail and bone invasion are all more likely to be seen in cases of nasal neoplasia, these changes are not specific for cancer versus rhinitis or for lymphoma versus any other intranasal neoplasia. As with other forms of lymphoma, careful staging is required. See Part 1 for a discussion of biopsy techniques.
Pre- (above) and post-radiotherapy (below) transverse post-contrast T1-weighted magnetic resonance images of a nasal lymphoma in a 10-year-old domestic shorthaired cat at the level of the caudal nasal cavity. Prior to treatment, a large mass can be seen filling the left nasal cavity, but it does not cross the nasal septum or invade the orbit (white arrow). Fluid is trapped within the left frontal sinus (black arrow). The post-treatment scan shows significant resolution; the soft tissue mass is no longer apparent and the trapped fluid has been allowed to drain. Radiotherapy can be useful for localised disease, as a combined modality treatment or rescue therapy
Treatment can involve either chemotherapy or radia-tion therapy, or a combination of the two modalities. In the author’s experience, long-term survival is achiev-able with radiation therapy alone, and in the absence of systemic involvement this is the preferred method of treatment when available. This is supported by the observations of other authors (Elmsie and others 1991). However, systemic disease, even if absent at presenta-tion, can manifest later in the course of disease and ultimately chemotherapy may be required. Conversely, relapsing nasal lymphoma treated by chemo therapy in the first instance, either due to systemic involvement or owner/vet preference, can be successfully rescued with radiation therapy. When nasal disease extends to the retrobulbar space, radiation of the globe may lead to long-term complications necessitating enucleation. A combined modality approach using chemotherapy to downsize the tumour (neoadjuvant therapy) may allow successful radiation therapy without irradiation of the globe. Repeated sectional imaging to monitor the response to drug-based treatment is essential in such cases prior to commencing chemotherapy.
OTHER FORMS OF LYMPHOMA
Other forms of lymphoma can be diagnosed in cats, either alone or as part of a multicentric presentation. When lymphoma of the lung occurs, it tends to mani-fest as nodular lesions, which are uncommon in dogs. Larnygeal lymphomas can cause respiratory stridor or
Dorsoventral intraoral projection of nasal lymphoma in a nine-year-old domestic shorthaired cat. There is loss of turbinate pattern unilaterally, an increase in soft tissue opacity (arrow) and occlusion of the nostril. The cribriform plate and medial orbital wall are ill-defined (not seen on this radiograph). This cat’s orbital ultrasonogram (see page 583) suggested that the nasal lymphoma had extended into the retrobulbar space. A definitive biopsy can often be obtained without invasive procedures
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from

In Practice ● @B V - ? ) - L â , - * - ? ) - L 20 06 585
Hodgkin’s-like lymphoma
A specific form of feline lymphoma, termed Hodgkin’s-like lymphoma, seems to be emerging. As the term suggests, there are pathological and clinical similari-ties to this specific human form of lymphoma. In people, Hodgkin’s lymphoma tends to affect contiguous lymph nodes in the neck and thorax, and the dis-ease can be slow to progress. Treatment is often based on surgery and radia-tion, rather than systemic drug therapy, which is more commonly associated with non-Hodgkin’s lymphoma. The neoplastic cells (Reed–Sternberg) are in the minority and are found among non-neoplastic lymphocytes.
The feline form of the disease appears to affect older cats, which present with unilateral and often focal cervical or mandibular lymphadenopathy. A mixed population of lymphocytes is recognised with neoplastic cells seeming to be in the minority (Walton and Hendrick 2001). A similar and possibly synony-mous condition has been described by Day and others (1999) as a T cell rich B cell lymphoma. Further work is required to categorise this disease more specifi-cally and document the clinical outcome. In the author’s experience, neoadju-vant chemotherapy prior to localised lymph node excision for cervical lymphad-enopathy has proved rewarding.
dyspnoea. Cutaneous lymphomas can be solitary or dif-fuse, and composed of T or B cells. Solitary cutaneous lymphomas can be cured surgically. In the case of multi-ple cutaneous lesions, or if surgical treatment is not indi-cated, treatment with conventional cytotoxic drugs can be attempted. Plesiotherapy and external beam radiation therapy may be useful as an adjunct to systemic treat-ment or as single modality therapy in areas that are deemed to be non-surgical.
SUMMARY
Lymphoma can present in many different guises, and the clinician should be alert to the possibility of this condi-tion in any cat regardless of age, breed or viral status. Treatment can be rewarding with rapid responses often leading to a reversal of life-threatening situations within hours or days of commencing appropriate therapy in the practice setting. Histological diagnosis and full staging are required to tailor treatment choices to the individ-ual cat. All samples for diagnostic purposes should be obtained before commencing therapy, including gluco-corticoid treatment.
AcknowledgementsThe images for this article were compiled with the help of the Units of Comparative Ophthalmology and Diagnostic Imaging at the Animal Health Trust, with particular thanks to Jane Samson, Ruth Dennis and Fraser McConnell.
ReferencesBROWN, M. R., ROGERS, K. S., MANSELL, K. J. & BARTON, C. (2003) Primary intratracheal lymphosarcoma in four cats. Journal of the American Animal Hospital Association 39, 468-472CARRERAS, J. K., GOLDSCHMIDT, M., LAMB, M., McLEAR, R. C., DROBATZ, K. J. & SORENMO, K. U. (2003) Feline epitheliotropic intestinal malignant lymphoma: 10 cases (1997-2000). Journal of Veterinary Internal Medicine 17, 326-331DAY, M. J., KYAW-TANNER, M., SILKSTONE, M. A., LUCKE, V. M. & ROBINSON, W. F. (1999) T-cell-rich B-cell lymphoma in the cat. Journal of Comparative Pathology 120, 155-167ELMSIE, R. E., OGILVIE, G. K., GILETTE, E. L. & McCHESNEY-GILLETTE, S. (1991) Radiotherapy with and without chemotherapy for localized lymphoma in 10 cats. Veterinary Radiology 32, 277-280FONDACARO, J. V., RICHTER, K. P., CARPENTER, J. L., HART, J. R., HILL, S. L. & FETTMAN, M. J. (1999) Feline gastrointestinal lymphoma: 67 cases (1988-1996). European Journal of Comparative Gastroenterology 4, 5-11MAHONY, O. M., MOORE, A. S., COTTER, S. M., ENGLER, S. J., BROWN, D. & PENNINCK, D. G. (1995) Alimentary lymphoma in cats: 28 cases (1988-1993). Journal of the American Veterinary Medical Association 12, 1593-1598
MOONEY, S. C., HAYES, A. A., MATUS, R. E. & MacEWEN, E. G. (1987a) Renal lymphoma in cats: 28 cases (1977-1984). Journal of the American Veterinary Medical Association 191, 1473-1477MOONEY, S. C., PATNAIK, A. K., HAYES, A. A. & MacEWEN, E. G. (1987b) Generalized lymphadenopathy resembling lymphoma in cats: six cases (1972-1976). Journal of the American Veterinary Medical Association 190, 897-900MOORE, F. M., EMERSON, W. E., COTTER, S. M. & DELELLIS, R. A. (1986) Distinctive peripheral lymph node hyperplasia of young cats. Veterinary Pathology 23, 386-391PENNINCK, D. G., MOORE, A. S., TIDWELL, A. S., MATZ, M. E. & FREDEN, G. O. (1994) Ultrasonography of alimentary lymphosarcoma in the cat. Veterinary Radiology & Ultrasound 35, 299-304RASSNICK, K. M., MAULDIN, G. N., MOROFF, S. D., MAULDIN, G. E., McENTEE, M. C. & MOONEY, S. C. (1999) Prognostic value of argyrophilic nuclear organiser region (AgNOR) staining in feline intestinal lymphoma. Journal of Veterinary Internal Medicine 13, 187-190WALTON, R. M. & HENDRICK, M. J. (2001) Feline Hodgkin’s-like lymphoma: 20 cases (1992-1999). Veterinary Pathology 38, 504-511ZWAHLEN, C. H., LUCROY, M. D., KRAEGEL, S. A. & MADEWELL, B. R. (1998) Results of chemotherapy for cats with alimentary malignant lymphoma: 21 cases (1993-1997). Journal of the American Veterinary Medical Association 213, 1144-1149
Further readingOGILVIE, G. K. & MOORE, A. S. (2001) Feline Oncology. A Comprehensive Guide to Compassionate Care. Trenton, New Jersey, Veterinary Learning SystemsVAIL, D. M. & THAMM, D. H. (2000) Hematopoietic tumours. In Textbook of Veterinary Internal Medicine. Diseases of the Dog and Cat, 6th edn. Eds S. J. Ettinger and E. C. Feldman. Philadelphia, W. B. Saunders. pp 732-747
CORRECTION
Feline lymphoma 1. Principles of diagnosis and management (In Practice, October 2006, volume 28, pp 516-524)On page 522, the dose for vincristine in the bottom table describing the MOPP protocol for rescue therapy should have read 0·025 mg/kg and not as stated. *This service is available to UK members only. Please be ready to quote your membership number
Wouldn’t it be nice if you had free 24-hour
legal advice at the end of a phone?
You do.As a BVA member you can call our free
legal advice line at anytime on
0870 1628 213*
on 16 June 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inpract.28.10.585 on 1 Novem
ber 2006. Dow
nloaded from