Embed Size (px)
Citation preview

February 23, 24 & 25, 2017February 23, 24 & 25, 2017
The HoustonAortic SymposiumAortic SymposiumFrontiers in Cardiovascular Diseases
ROBERTO DI BARTOLOMEO
CARDIAC SURG. DEPT.ST. ORSOLA – HOSPITAL
UNIVERSITY OF BOLOGNA
ROBERTO DI BARTOLOMEO
UNIVERSITY OF BOLOGNA

FINANCIAL DISCLOSURE: NONE
HOUSTON, TEXASHOUSTON, TEXAS

Complex lesions of the thoracic aorta
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Complex lesions of the thoracic aorta
““Pa tholog yofthe a orta sta rting from the a sc e nd ing a orta orPa tholog yofthe a orta sta rting from the a sc e nd ing a orta ora ortic a rc h a nd e xte nd ing d ownwa rd intothe d e sc e nd ing thora c ica ortic a rc h a nd e xte nd ing d ownwa rd intothe d e sc e nd ing thora c ica ortic a rc h a nd e xte nd ing d ownwa rd intothe d e sc e nd ing thora c ica ortic a rc h a nd e xte nd ing d ownwa rd intothe d e sc e nd ing thora c ic
orthora c oa b d om ina la ortaorthora c oa b d om ina la orta ””
ACU TE
Type A a ortic d isse c tion
CHRO N IC
Chronic a ne urysm sType A a ortic d isse c tion
Type B a ortic d isse c tion
Chronic a ne urysm s
Type A a ortic d isse c tion
PAU – AoHa e m a tom a Type B a ortic d isse c tion
PAU – AoHa e m a tom aPAU – AoHa e m a tom a
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

1982 –THE BIRTH OF THE ELEPHANT TRUNK
The problem: 2 patients with mega-aorta
Re fle ctionsof Borst
The problem: 2 patients with mega-aortasyndrome
Idea: “Decided to replace the aortic arch with aH. BORSTH. BORST
Idea: “Decided to replace the aortic arch with along graft, whose free ‘‘elephant trunk’’ extensionwas to be suspended freely in the distal aorta”
1 st stage1 st stage1 st stage1 st stage 2 nd stage2 nd stageCardiac Surgery Dept. – University of Bologna
roberto.dibartolomeo@ unibo.it

TheThe mostmost recentrecent developmentdevelopment ofof thethe classicclassic elephantelephant trunktrunk
techniquetechnique isis thethe combinationcombination ofof anan endovascularendovascular stentstent graftgraft
withwith aa conventionalconventional surgicalsurgical graftgraft forfor hybridhybrid proceduresprocedures ofof
thethe entireentire thoracicthoracic aortaaorta..
ThisThis newnew optionoption waswas termedtermed::ThisThis newnew optionoption waswas termedtermed::
FROZEN ELEPHANTFROZEN ELEPHANTFROZEN ELEPHANTFROZEN ELEPHANTTRUNKTRUNK
Kark M,Haverich A, et al.Kark M,Haverich A, et al. The froze ne le pha nttrunk te c hnique :a ne wThe froze ne le pha nttrunk te c hnique :a ne wtre a tm e ntforthora c ic a ortic a ne urysm stre a tm e ntforthora c ic a ortic a ne urysm s. J Thorac Cardiovasc Surg 2003;. J Thorac Cardiovasc Surg 2003;125:1550125:1550--33

THE TRUNK EVOLUTION
1982
TodayBirth of ET
1992ET modified
Today
ET modifieddistal suture
Crawford-Svensson
2004Branched ET
NeriSvensson
2007FET Hybrid graft 2012
2003Birth of FET
Chavan-HaverichFET Hybrid graft 2012
Branched FET
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
Chavan-Haverich
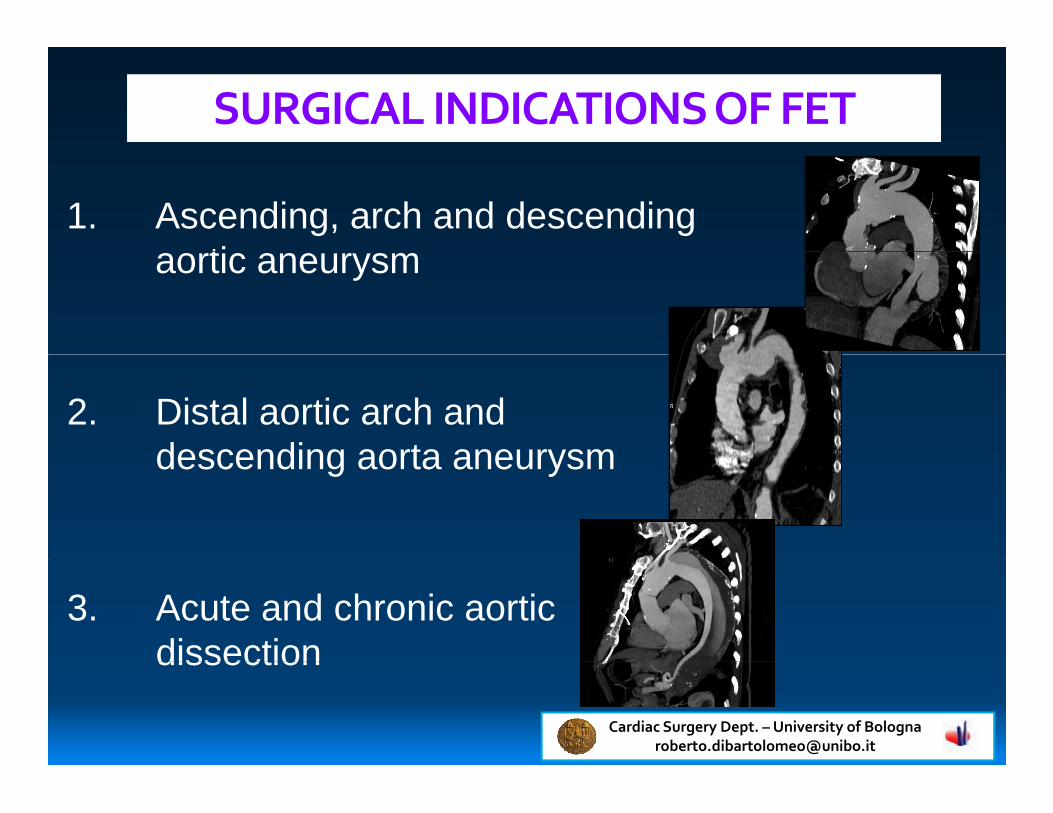
SURGICAL INDICATIONS OF FET
1. Asce nding, arch and de sce ndingaortic ane ury smaortic ane ury sm
2. Distalaortic arch andde sce nding aorta ane ury smde sce nding aorta ane ury sm
3. Acute and ch ronic aorticdisse ction
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
disse ction

Rationale for FET in typeA and B acute dissection
• Type A acute aortic dissections Intimal tear in the arch
Young patients
Malperfusion syndrome
Retrograde dissection
• Type B acute aortic dissection• Type B acute aortic dissection
Impending rupture when TEVAR isnot feasiblenot feasible
Associated with ascending and archaneurysm
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
aneurysm

COMMERCIALLY AVAILABLE STENTED GRAFTSIN EUROPEIN EUROPE
E-vita Open plus - JotecE-vita Open plus - Jotec
Thoraflex - Vascutek
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Currently under investigation
Stanford University, California
Emory Saint Joseph's Hospital, Georgia
Northwestern Memorial Hospital, IllinoisNorthwestern Memorial Hospital, Illinois
Ann Arbor, Michigan
The Mount Sinai Hospital, NewYork
Columbia University Medical Center, NewYork
NewYork-Presbyterian Weill Cornell Medical Center, NewYork
Duke University Medical Center, North Carolina
Cleveland Clinic, Ohio
University of Pennsylvania, Philadelphia University of Pennsylvania, Philadelphia
University of Pittsburgh Medical Center (UPMC), Pittsburgh
Baylor St. Luke’s, Texas
University of Texas-Memorial Hermann Medical Center, Texas University of Texas-Memorial Hermann Medical Center, Texas
The Heart Hospital Baylor Plano, Texas

Aortic anatomy assessmentAortic anatomy assessment
• Myocardial
Organ protection
• Myocardial
• Cerebral
• Visceral
Surgical technique/strategy
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Aortic Disse ction
AORTIC ANATOMY ASSESSMENT
• Intim alflap e ste ntion
•Entry site
Aortic Disse ction
TL
FL
•Re lation true /false lum e n
•Visce ralve sse lsorigin
•Re e ntry
TL
FL
TL
FLFL
•Re e ntry
•• NoNo ove rsizingove rsizing
FL
FL
TL FL
EntryEntryEntry siteEntry site
ReentryReentry ReentriesReentries
EntryEntry

AORTIC ANATOMY ASSESSMENT
CHRONIC
Evaluation of
CHRONICANEURY SMS
Evaluation ofaortic diam e te rs
OVERSIZING: 10OVERSIZING: 10--20%20%
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
OVERSIZING: 10OVERSIZING: 10--20%20%

ORGAN PROTECTION - MYOCARDIAL
C u stodiol®® ModifiedModified BretschneiderBretschneider solutionsolution(Koe hle rChe m ie ,Alsb a c h-Ha e nle in,G e rm a ny)
• H ypothermia(8 -10°C )• 20-25cc/Kgsingle dose
18 0 min (3h)ischemia
S elective infu sion+/-retrograde perfu sion
RCL C
L owL owpressu repressu repressu repressu reP erfu sionP erfu sion(5(5--8 min)8 min) Cardiac Surgery Dept. – University of Bologna
roberto.dibartolomeo@ unibo.it

Antegrade Selective Cerebral Perfusion
ORGAN PROTECTION – CEREBRAL PROTECTION
Antegrade Selective Cerebral PerfusionAxilla ry,b ra c hioc e pha lic a nd c a rotid a rte rie s
400 ml/min(5ml/Kg/min)
1 lt/min
8 0 KgptP max:8 0 mmH g M oderate systemic hypothermia:
26 °C of nasoph.T
Ox
1 lt/minKeepgoodpressu re in the
O xigenator
flowmeter
P artialclamp
A dvantages:
RA
B IOP UM P
>1,5lt/min! :spin/min
flowmeter
• A ntegrade flow• L eftcarotid and leftsu bclavian art.selective cannu lation
RA
D rawbacks:• Two system cerebralperfu sion• N o rightradialarterypressu re• N o rightradialarterypressu re
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

ORGAN PROTECTION – VISCERAL AND SPINALCORD PROTECTION
P max:8 0 mmH g
After Distal Anastomosis
CORD PROTECTION
400 ml/min(5ml/Kg/min)
1 lt/min
8 0 mmH g
KeepgoodP artialclamp
RA
Ox
B IO
Keepgoodpressu re in the
O xigenator
flowmeter
clamp
RAB IOP UM P
>1,5lt/min! :spin/min
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Thoraflex hybrid implantation in …
……

Step-1 FET – Spinal fluid drainage
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Step-2 Guidewire positioning
True Lumen Confirmation by TEE
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Central arterial cannulationStep-3
Ax illary arte ry Carotid arte ry
Brach ioce p h alic trunk
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Step-4
Arterial cannulaArterial cannula
ASCPASCP cannulacannula
ASCP cannulaASCP cannula
Cannulation of epiaorticvessels for antegrade
Di bartolomeo-ASCP Cannulavessels for antegrade
cerebral perfusionDi bartolomeo-ASCP Cannula
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Step-5 Preparation of the distal aorta
False lumenFalse lumen
• Acute /Ch ronic Ao disse ction:re ap p rox im ation of th e TL and FL
• Ch ronic ane ury sm
GuidewireGuidewire
True lumenTrue lumenTrue lumenTrue lumen
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Endoscopy inside the Thoracic AortaStep-6
Before and after stent graft release
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Antegrade introduction of the stent graftStep-7
Th orafle x Hy b rid
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Distal anastomosisStep-8
• Just beyond left subclavian artery• Between left subclavian and left carotid arteryBetween left subclavian and left carotid artery• Between left carotid and brachiocephalic artery• Before brachiocephalic artery
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Restore visceral perfusionStep-9
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Epiaortic vessels reimplantationStep-10
Separated -Thoraflex
AA
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
B

Left subclavian artery reimplantationStep-11
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

Proximal anastomosisStep-12
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
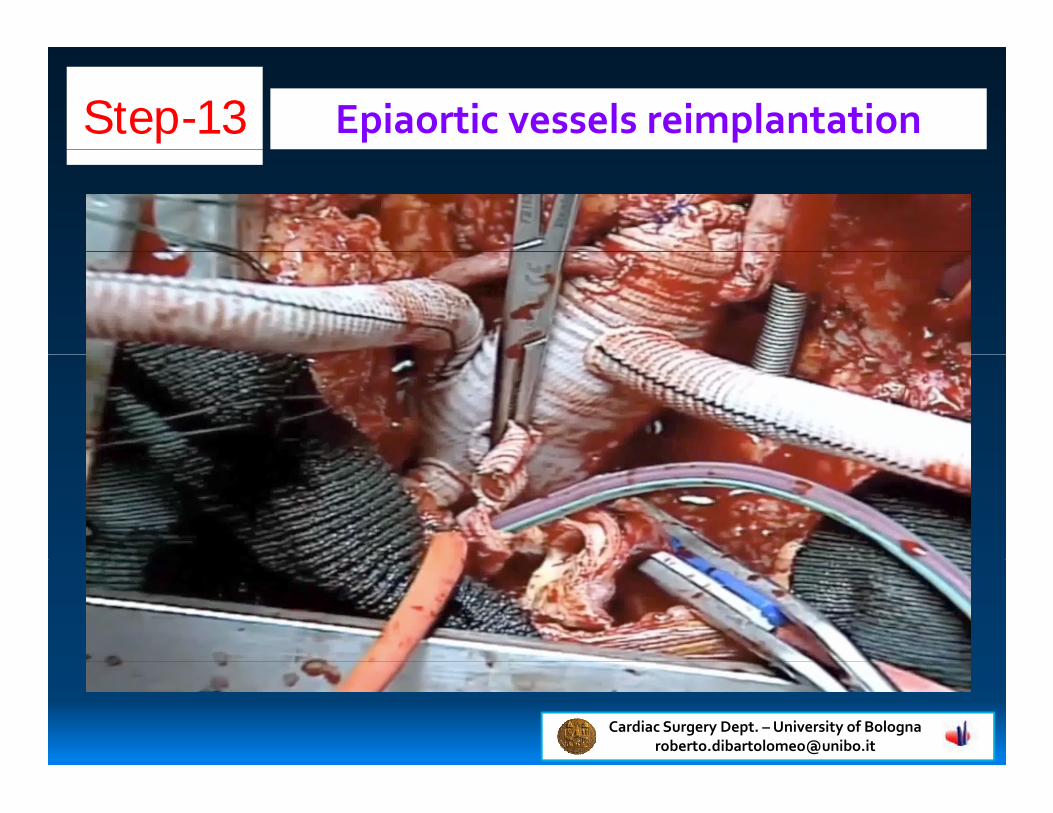
Epiaortic vessels reimplantationStep-13
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it

FET - Features of the 4-branched hybrid graft
Arch BranchesFROM 2007
CollarTO 2012
EndograftSide branch forart. cannulation Endograft
• Reduction of myocardial and lower body ischemia• Pathological regions of the aortic arch can be totally
art. cannulation
• Pathological regions of the aortic arch can be totallyresected (individual arch vessel reimplantation)
• Distal anastomosis can be achieved more proximally in
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
• Distal anastomosis can be achieved more proximally inthe arch

BOLOGNA FET - EXPERIENCE
January 2007 –April 2016
Jotek EVITA: 161 pts Vascutek Thoraflex: 64 pts
Cardiac Surgery Dept. – University of Bolognaroberto.dibartolomeo@ unibo.it
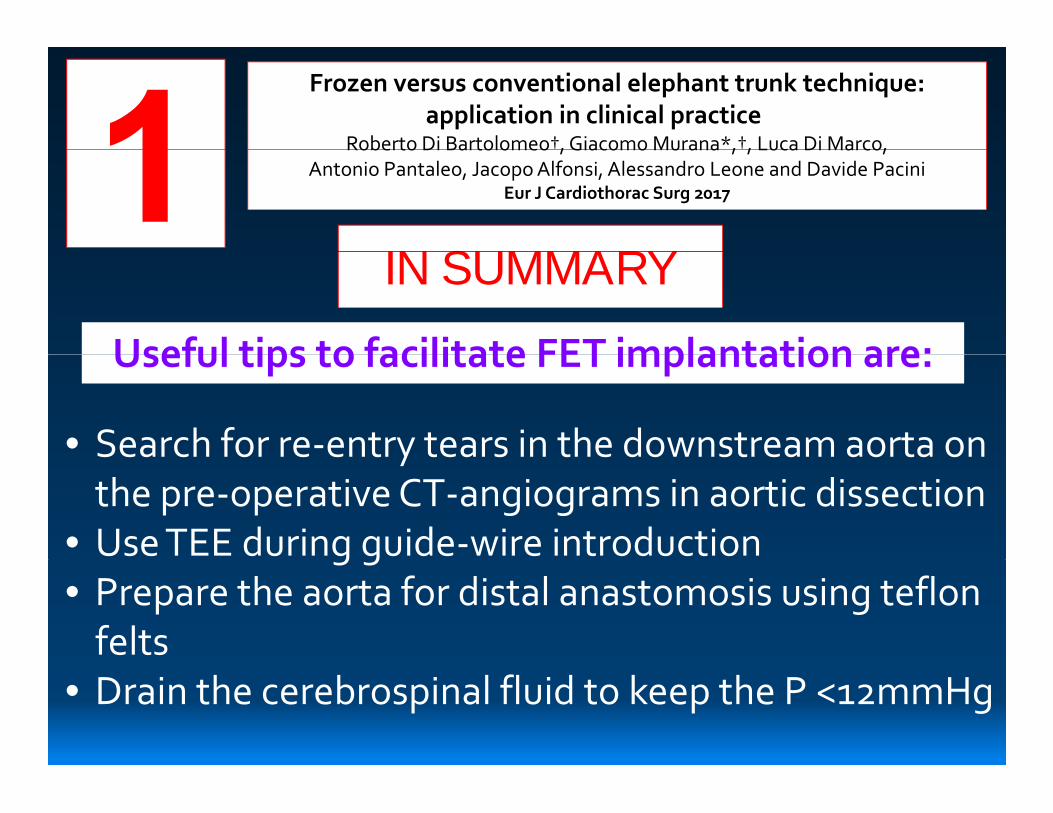
Frozen versus conventional elephant trunk technique:application in clinical practice
Roberto Di Bartolomeo†, Giacomo Murana*,†, Luca Di Marco,
IN SUMMARY
Roberto Di Bartolomeo†, Giacomo Murana*,†, Luca Di Marco,Antonio Pantaleo, Jacopo Alfonsi, Alessandro Leone and Davide Pacini
Eur J Cardiothorac Surg 2017
Useful tips to facilitate FET implantation are:
IN SUMMARY
Useful tips to facilitate FET implantation are:
•Search for re-entry tears in the downstream aorta on•Search for re-entry tears in the downstream aorta onthe pre-operative CT-angiograms in aortic dissection
•Use TEE during guide-wire introduction•Use TEE during guide-wire introduction•Prepare the aorta for distal anastomosis using teflon
feltsfelts•Drain the cerebrospinal fluid to keep the P <12mmHg

Frozen versus conventional elephant trunk technique:application in clinical practice
Roberto Di Bartolomeo†, Giacomo Murana*,†, Luca Di Marco,
IN SUMMARY
Roberto Di Bartolomeo†, Giacomo Murana*,†, Luca Di Marco,Antonio Pantaleo, Jacopo Alfonsi, Alessandro Leone and Davide Pacini
Eur J Cardiothorac Surg 2017
Useful tips to facilitate FET implantation are:
IN SUMMARY
•Look inside the descending thoracic aortaendoscopically before/after release of the stent graft
Useful tips to facilitate FET implantation are:
endoscopically before/after release of the stent graft•Restart systemic perfusion and ‘rewarming’
immediately after completing the distal anastomosisimmediately after completing the distal anastomosis•Avoid stent oversize in aortic dissection•Keep mean systemic pressure >80 mmHg after device•Keep mean systemic pressure >80 mmHg after device
implantation to better perfuse the spinal cord

13-14 November 201713-14 November 2017
…SAVE THE DATE!…SAVE THE DATE!






![PARTE DIARIO - chfutaleufu.com.ar · PARTE DIARIO Estaciones Meteorologicas Lluvia Diaria [mm] Lluvia Mensual [mm] ... ND 5.1 ND ND ND ND 12.8 ND ND ND (Lago Futalaufquen) (Pto Rios)](https://img.dokumen.tips/doc/110x75/5c0da76209d3f23c2a8bb4cf/parte-diario-parte-diario-estaciones-meteorologicas-lluvia-diaria-mm-lluvia.jpg)






















