Embed Size (px)
Citation preview

& SIR, 2015
J Vasc Interv
http://dx.doi.or
None of the au
From the Obs(A.V.), and RadJD Peron 4190final revision recorrespondenc
CLINICAL STUDY
Feasibility and Safety of Prophylactic Uterine
Artery Catheterization and Embolizationin the Management of Placenta Accreta
Gustavo Izbizky, MD, César Meller, MD, Mario Grasso, MD,Andrea Velazco, MD, Oscar Peralta, MD, Lucas Otaño, MD, PhD,
and Ricardo Garcia-Monaco, MD, PhD
ABSTRACT
Purpose: To evaluate the feasibility and safety of prophylactic uterine artery catheterization and embolization in themanagement of placenta accreta (PA).
Materials and Methods: Retrospective chart review was performed of 95 consecutive patients with prenatal suspicion of PAmanaged in a 10-year period with a strategy that included prophylactic bilateral uterine artery catheterization, delivery of thebaby, uterine artery embolization if indicated, and subsequent surgery. Feasibility was defined as catheterization being possibleto perform, technical success as embolization being possible when indicated and complete stasis of the vessels achieved, andclinical success as no maternal death or major blood loss. Median gestational age at delivery was 36 weeks (interquartile range,24–39 wk).
Results: PA was confirmed in 79 patients (83%). Feasibility was 97% (92 of 95); in three cases (3%), acute early massivehemorrhage forced emergency delivery without catheterization. Embolization was performed in 83 of 92 patients (87%) to theextent of complete stasis; in the remaining nine, it was unnecessary because spontaneous placental detachment was visualizedafter fetal delivery (technical success rate, 100%). There were several complications, including bleeding requiring bloodtransfusion (49%) and bladder surgery (37%), but there were no major complications attributable to the endovascularprocedures. There was one minor complication presumably related to embolization (transient paresthesia and decreasedtemperature of lower limb), with uneventful follow-up. Clinical success rate was 86%, with no maternal deaths, but 14% ofpatients received large-volume blood transfusion.
Conclusions: Prophylactic uterine artery catheterization and embolization in the management of PA appeared to be feasibleand safe in this consecutive series of patients.
ABBREVIATIONS
IIA = internal iliac artery, IQR = interquartile range, PA = placenta accreta, PRBC = packed red blood cell, UAE = uterine artery
embolization
Placenta accreta (PA) is an increasingly common life-threatening condition. It is associated with maternalmortality and morbidity resulting from massive obstetric
Radiol 2015; 26:162–169
g/10.1016/j.jvir.2014.10.013
thors have identified a conflict of interest.
tetrics Service (G.I., C.M., M.G., L.O.), Gynecology Serviceiology Service (O.P., R.G.M.), Hospital Italiano de Buenos Aires,(C1199ACI), Buenos Aires, Argentina. Received April 11, 2014;ceived October 12, 2014; accepted October 13, 2014. Addresse to R.G.M.; E-mail: [email protected]
hemorrhage and surgical morbidity (1–5). Most expertsagree that the perioperative care of patients with suspec-ted PA should be in an institution with the appropriateexpertise and facilities to ensure a multidisciplinaryapproach (3–6). However, the optimal management ofthese patients remains controversial. The use of endo-vascular interventional procedures to reduce hemor-rhage, thereby improving visualization of the surgicalfield and allowing a more controlled hysterectomy (whenindicated), has been described in the managementof obstetric hemorrhage of various causes, but its rolein the management of PA is still a subject of discussion(6–10). Actually, several centers do not support its use,even with the availability of the technology. Different

Volume 26 ’ Number 2 ’ February ’ 2015 163
approaches have been described, including balloonocclusion alone as an adjunct for cesarean hysterectomy,a combination of balloon occlusion and embolization,and prophylactic catheter placement and prehysterec-tomy embolization. Despite being widely practiced, thereis no robust evidence to support temporary balloonocclusion of the internal iliac arteries (IIAs) beforehysterectomy (11). The efficacy of prophylacticbilateral uterine artery catheterization and emboli-zation to reduce surgical bleeding has shown encou-raging results in retrospective series without a controlarm, but current literature about its feasibility and safetyis still scarce (8,9,11–14). Although there is literatureregarding feasibility and safety of embolization ofuterine fibroid tumors, the setting of PA is different formany reasons, including the fact that women with PAmay need an unscheduled delivery mainly as a result ofvaginal bleeding, that embolization in PA frequentlyinvolves additional target organs, and the likelihood ofhigher risk of thrombotic complications because of theprothrombotic state of pregnancy. Therefore, publica-tions of embolization for fibroid tumors may not beadequate to allow extrapolation to the feasibility andsafety of embolization in PA.The aim of the present study was to evaluate the
feasibility and safety of prophylactic selective bilateraluterine artery catheterization and embolization in themanagement of PA in a consecutive series of patientstreated at a single institution.
MATERIALS AND METHODS
The present study was a retrospective chart review of aseries of 95 consecutive patients who were suspectedprenatally to have PA and were managed with the samemultidisciplinary strategy between February 2002 and July2012 at a university hospital. Inclusion criteria weresuspicion of PA based on the presence of ultrasound (US)and/or magnetic resonance (MR) imaging findings and/orthe presence of high risk factors such as previous cesareandelivery and placenta previa in the index pregnancy.Patients were identified from a specific electronic databaseof pregnancies with prenatal suspicion of PA and scheduledfor the multidisciplinary management protocol (Excel 2011;Microsoft, Redmond, Washington). The study wasapproved by the institutional review board.Abnormal placental adherence was confirmed histo-
pathologically and/or clinically after delivery (15–18).Histopathologic confirmation included the spectrum ofaccreta (ie, chorionic villi are implanted on the myome-trium without intervening deciduas), increta (ie, themyometrium is invaded by the placental villous tissue),and percreta (ie, the villi penetrate the entire uterinewall) (16). Clinical assessment of abnormal adherence ofthe placenta was defined as placental attachment to theuterine wall without easy separation (15). For the
purposes of the present study, we used the term PA forthe entire spectrum of abnormal placental adherence.The management of PA in our institution included the
following: prenatal imaging studies (US and MR imag-ing), preoperative multidisciplinary counseling, sched-uled delivery at approximately 36 weeks of gestation,and a staged perioperative protocol including bilateraluterine artery catheterization and angiography, cysto-scopy and bilateral ureteral stent placement, midlinelaparotomy, hysterotomy and delivery of the baby(avoiding the placenta), embolization (unless spontane-ous placental detachment was seen with normal bleedingat the placental site immediately after fetal delivery), andelective hysterectomy if the diagnosis of PA was con-firmed during surgery. Conservative surgery with pres-ervation of the uterus was reserved for false-positivecases or for patients with a focal or small limited area ofaccretism, but our standard of care was hysterectomy.Before treatment, all patients received comprehensivecounseling and provided written informed consent.Preoperative pelvic angiography was performed with a
5-F pigtail catheter in the angiography suite (IntegrisV5000; Philips Medical Systems, Best, The Netherlands)via a percutaneous arterial femoral approach. First, two5-F Cobra-type catheters (Glidecath; Terumo, Tokyo,Japan) were introduced coaxially through bilateralfemoral 5-F introducers (Terumo). Each catheter wasplaced in the anterior trunk of the contralateral IIA.Then, selective bilateral uterine artery catheterizationand angiography were performed with low-osmolarcontrast medium (Hexabrix; Guerbet, Roissy, France).The catheters were advanced further and placed at thelevel of the horizontal portion of each uterine artery.Then, the catheters were fixed to the skin, and thepatient was transferred to the operating room, wherebilateral ureteral stents were placed under cystoscopy.Immediately before surgery, the position of the uterineartery catheter was checked under fluoroscopy with amobile angiography system (BV300; Philips MedicalSystems) located in the operating room.A laparotomy through an infraumbilical incision and a
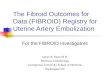
hysterotomy (avoiding the placenta) were then per-formed. After delivery of the baby, if PA was stronglysuspected and spontaneous detachment was not visual-ized, the placenta was left in situ, and free-flow bilateraluterine embolization was performed under fluoroscopywith a mixture of iodine contrast medium and Gelfoampledgets (Pharmacia and Upjohn, Kalamazoo, Michigan)until complete stasis (Fig 1). If preoperative pelvicangiography showed significant uterine vascular supplyfrom the vesical or vaginal arteries, these vessels werealso embolized with the same 5-F catheter. Postemboli-zation angiography was not performed routinely but atthe operator’s discretion. Immediately after embolization,a gynecologist with 10–25 years of experience performeda total or subtotal hysterectomy if PA was strongly sus-pected and spontaneous detachment was not visualized.

Figure 1. (a) Aortogram shows low placental implantation (asterisk) and vascularization originating from the uterine and vesicovaginal
arteries (arrows). The angiogram shows the fetal head (open arrows) and “double-J” formed by catheters (arrowheads). This
angiogram was obtained immediately before bilateral and simultaneous catheterization of both uterine arteries. (b) Postembolization
angiogram after simultaneous contrast agent injection from both hypogastric arteries after delivery (arrows) shows double-J formed by
catheters (arrowheads). Placenta was devascularized after uterine artery and anterior internal iliac trunk free-flow embolization
(asterisk).
Izbizky et al ’ JVIR164 ’ Uterine Artery Catheterization/Embolization for Placenta Accreta
Perinatal and maternal outcomes were recorded (in-cluding maternal age, obstetric history, gestational ageat delivery, maternal morbidity [including blood loss andthe need of transfusions], and neonatal morbidity). Themedian gestational age at delivery was 36 weeks (inter-quartile range [IQR], 34–37 wks), and median follow-upwas 5.8 years (IQR, 3.7–7.7 y).Prophylactic selective bilateral uterine artery catheter-
ization was defined as feasible if it was possible toperform. Technical success of the embolization wasdefined as the possibility of embolization when indicatedand achievement of complete stasis of the vessels.Complications related to endovascular procedures
were categorized as minor and major per Society ofInterventional Radiology clinical practice guidelines(19). Minor complications include events that (i) re-quired no therapy and had no consequences or (ii) re-quired nominal therapy and had no consequences,including overnight admission for observation only.Major complications include events that (i) required the-rapy and minor hospitalization (o 48 h); (ii) requiredmajor therapy, were associated with an unplannedincrease in the level of care, or required a prolongedhospitalization (4 48 h); (iii) resulted in permanentadverse sequelae; or (iv) resulted in patient death. We
defined large-volume blood transfusion as at least 4 U ofpacked red blood cells (3). Clinical success was definedas no maternal death and no major blood loss requiringa large-volume blood transfusion or repeat operation asa result of bleeding. Demographic and clinical character-istics of the patients are shown in Table 1.Data are presented with measures of central tendency
and dispersion according to the distribution, using themean or median and standard deviation or IQR. Forcategoric variables, proportions were used. STATAsoftware (version 8.0; StataCorp, College Station, Texas)was used for data analysis.
RESULTS
PA was confirmed in 79 of 95 patients (83%), 74 basedon histopathology (hysterectomies) and five based onintraoperative clinical assessment. Among the 74 pa-tients with a pathologic diagnosis of abnormal placentaladherence, 20 (27%) were accreta, 18 (24%) increta, and36 (49%) percreta (Table 2). The five patients withclinical diagnosis of PA were managed without hyste-rectomy at the discretion of the attending physi-cian because only a focal area of PA was suspected,

Table 1 . Demographic and Clinical Characteristics
Characteristic Value
Age (y) 35 � 4.4
Gravidity
Median 3
IQR 2–7
Parity
Median 2
IQR 1–5
Previous cesarean section
0 4 (4.2)
1 40 (42.1)
2 30 (31.6)
Z 3 21 (22.1)
Previous uterine curettage
0 68 (72)
1 21 (22)
Z 2 6 (6)
Placental occlusion
Yes 79 (83)
No 16 (17)
Values presented as means � standard deviation where
applicable. Values in parentheses are percentages.
IQR ¼ interquartile range.
Table 2 . Peripartum Management
Characteristic Value
Gestational age at delivery (wk)
Median 36
IQR 24–39
Operative time (min)* 226.7 � 65
Ureteric stent placement 84 (88.4)
Uterine artery catheterization 92 (96.8)
Uterine artery embolization 83 (87.3)
Postoperative length of stay (d)
Median 5
IQR 3–10
Depth of placental invasion
Acretism 20 (27)
Incretism 18 (24)
Percretism 36 (49)
Values presented as means � standard deviation where
applicable. Values in parentheses are percentages.
IQR ¼ interquartile range.
*Operative times calculated from operating room entrance to
the end of surgery.
Volume 26 ’ Number 2 ’ February ’ 2015 165
the placenta could be removed, and none of thesepatients required reoperation or a large-volume bloodtransfusion. In 16 of 95 patients (17%), there was nopostnatal confirmation of PA, and hysterectomy was notperformed (Fig 2).Perioperative management is summarized in Table 2.
A scheduled delivery was achieved in 67% of patients (64of 95), and an unscheduled delivery occurred in 33% of
patients (31 of 95), mainly as a result of vaginal bleeding(25 of 31). Prophylactic selective bilateral uterine arterycatheterization was performed electively in 92 of 95patients (97%; nonemergency group). In the remainingthree patients (3%), acute early massive hemorrhageforced emergency delivery (mean gestational age,26 wk � 6.1), precluding prophylactic uterine arterycatheterization (ie, procedure not feasible). Embolizationwas performed in 83 of 92 patients (87%) who underwentprophylactic bilateral uterine catheterization, withcomplete stasis in all of them; 52 of the 83 patients(63%) did not require embolization of additional arteriesother than the uterine arteries, and embolization of addi-tional arteries was needed in the remaining 31 (37%). Inthe nine patients who did not undergo uterine emboli-zation, the procedure was considered unnecessary be-cause spontaneous placental detachment was observedimmediately after fetal delivery, with normal bleeding atthe placental site. The technical success rate was 100%.The mean contrast agent volume used in the endo-vascular procedure was 130 mL (IQR, 70–170 mL).Ureteric stents were placed in 84 of 95 patients (88.4%);in the other eight (8.4%), technical difficulties precludedstent placement. The remaining three patients (3.1%)belonged to the emergency group. The mean operativetime was 226.7 minutes � 65.Among the 95 patients, there were several surgical and
postoperative complications (Tables 3, 4), which showmaternal and neonatal morbidity, including bleedingrequiring blood transfusion (49%), bladder surgery(37%), and coagulopathy (7.4%). In four patients, repeatoperation before 24 hours was needed: delayed hyster-ectomy was performed in one case, and abdominalbleeding led to hypovolemic shock and required repeatlaparotomy in the other three.There were no major complications directly attribut-
able to the endovascular procedures. One patient (1%)experienced a minor complication consisting of decrea-sed temperature in the right lower limb and mild pares-thesia 6 hours after surgery. Doppler US and multi-detector computed tomographic angiography showednormal, patent vessels. The patient’s symptoms resolvedspontaneously the following morning, and follow-up wasuneventful.A blood transfusion was indicated in 47 patients
(49%): 45 of 79 (57%) in the group with confirmed PAand two of 16 (12.5%) in the group with no PA. Amongthe nonemergency group, 44 of 92 patients (48%)required a transfusion (13 of 92 [14%] required large-volume blood transfusion), and the three patients inthe emergency group needed a transfusion (two [66%]needed a large-volume blood transfusion). The meanamount of blood transfused per patient in the catheter-ized group was 1.4 U.Postoperative length of stay was 4 days (IQR, 4–5 d)
in the 92 nonemergency cases and 7 days (IQR, 6–13 d)in the three emergency cases (P = .01).

Figure 2. Flow chart of patient disposition.
Table 3 . Maternal and Neonatal Morbidity
Characteristic Value
Blood transfusion* 45 (57)
Z 4 U PRBCs 15 (19)
Z 10 U PRBCs 2 (2.5)
Diminished temperature and paresthesia 1 (1.3)
Bladder surgery* 35 (44)
ICU admission* 14 (18)
Coagulopathy* 7 (8.8)
Thromboembolism* 1 (1.3)
Vault hematoma* 2 (2.6)
Reoperation before 24 h*† 4 (5.2)
Delayed hysterectomy* 1 (1.3)
Vesicovaginal fistula* 1 (1.3)
Readmission*‡ 4 (5.2)
Birth weight (g) 2,566 � 783
Neonatal length of stay (d)
Median 4
IQR 2–55
Fetal death 3 (3.1)
NICU admission 56 (61)
Values presented as means � standard deviation where
applicable. Values in parentheses are percentages.
ICU ¼ intensive care unit, IQR ¼ interquartile range, NICU ¼neonatal intensive care unit, PRBC ¼ packed red blood cell.
*Including only the 79 cases of postnatal confirmed placenta
accreta.†In one case, a delayed hysterectomy was performed, and in
the other three, abdominal bleeding led to hypovolemic shock
and needed repeat laparotomy.‡Infections (n ¼ 3) and pulmonary thromboembolism (n ¼ 1).
Izbizky et al ’ JVIR166 ’ Uterine Artery Catheterization/Embolization for Placenta Accreta
There were three fetal deaths, two corresponding tosurgeries before 24 weeks gestation because of maternalcomplications, and the third one was a referral of a
patient with suspected PA and already an intrauterinedeath. There were no maternal deaths. Clinical success inthe catheterized group was 86% (79 of 92). Clinicalfailure included 13 patients who received large-volumeblood transfusion, four of whom needed a repeatoperation within the first 24 hours.
DISCUSSION
The present large series reports the use of prophylacticuterine artery catheterization and embolization togetherwith the surgical management of PA at a single institu-tion. In this multidisciplinary approach, prophylacticuterine artery catheterization proved to be feasible in97% of patients, with no major complications directlyattributable to the endovascular procedures.The literature describes two different types of endo-
vascular interventions to diminish bleeding before hys-terectomy in the management of PA: temporary balloonocclusion of the IIAs (4,7,9–11,14) and bilateralembolization of the uterine vessels (8,9,11–14,20–23).Although balloon placement is widely practiced, highrates of complications related to this procedure havebeen reported, and its benefits have not been clearlydemonstrated (10,11,15). The use of prophylactic bilat-eral uterine artery catheterization and embolization toreduce surgical bleeding in PA has shown encouragingresults in small series, but its safety and feasibility havenot been reported in large series (8,9,11–13,21,23,24).Maternal complications such as groin or retro-
peritoneal hemorrhage, femoral arterial pseudoaneur-ysm, vessel injury, thromboembolic events, abscess, andtissue infarction have been reported with the use of

Table 4 . Maternal and Neonatal Morbidity in Each Subgroup of Patients
Characteristic
Confirmed PA (n ¼ 79) No PA (n ¼ 16)
HT (n ¼ 71) No HT (n ¼ 5) Emergency (n ¼ 3) UAE (n ¼ 7) No UAE (n ¼ 9)
Blood transfusion 40 (56) 2 (40) 3 (100) 0 2 (12)
Z 4 U PRBCs 13 (18) 0 0 0 0
Z 10 U PRBCs 0 0 2 (66) 0 0
Diminished temperature and paresthesia 1 (1.4) 0 0 0 0
Bladder surgery 34 (48) 0 1 0 0
ICU admission 11 (15) 0 3 0 0
Coagulopathy 6 (8) 0 1 0 0
Thromboembolism 1 (1.4) 0 0 0 0
Vault hematoma 1 (1.4) 0 1 0 0
Repeat operation before 24 h* 3 (4.2) 0 1 0 0
Delayed hysterectomy 0 0 1 0 0
Vesicovaginal fistula 0 0 1 0 0
Readmission† 4 (6) 0 0 0 0
Birth weight (g) 2,551 � 778 2,652 � 407 1,085 � 710 2,912 � 347 2,975 � 725
Neonatal length of stay (d)
Median 13 3 45 3.6 4.1
IQR 2–55 2–5 – 3–6 3–6
Fetal death 2 (3) 0 1 (30) 0 0
NICU admission 52 (73) 2 (40) 2 (100) 1 (6) 2 (12)
Values presented as means � standard deviation where applicable. Values in parentheses are percentages.
ICU ¼ intensive care unit; IQR ¼ interquartile range; HT ¼ hysterectomy; NICU ¼ neonatal intensive care unit; PA ¼ placenta accreta;
PRBC ¼ packed red blood cell; UAE ¼ uterine artery embolization.
*In one case, a delayed hysterectomy was performed; in the other three, abdominal bleeding led to hypovolemic shock and needed
repeat laparotomy.†Three cases for infections and one case for pulmonary thromboembolism.
Volume 26 ’ Number 2 ’ February ’ 2015 167
endovascular techniques (9–11,25,26). In a series of 19patients who underwent prophylactic balloon catheterplacement, Shrivastava et al (10) reported a 16% rate ofmajor complications related to the intervention. Inone patient, a groin hematoma developed that wasassociated with occlusive dissection of the IIA, and IIAand femoral artery thrombosis developed as aconsequence of the endovascular procedures in twopatients. Chung et al (26), in a series of 33 patientswho underwent transarterial embolization for post-partum hemorrhage, reported a 27% rate of comp-lications related to the interventional procedure.Buttock pain and transient lower-limb paresthesia werethe most common minor complications. A vaginal fistulaattributed to tissue ischemia developed in one patient;and, at 3 years after the procedure, one patient hadchronic limb paresthesia requiring neurologic treatment.Both these events were regarded as major complications.However, prophylactic catheterization of the PA was notperformed in any of these patients, as therapeuticcatheterization and embolization was required in allprocedures reported in that study (26). Even thoughthe estimated complication rate of the endovascularprocedures has been reported to be as high as 16%–
27% (10,26), we observed no major complicationsrelated to prophylactic intraarterial procedures in thepresent series. Although PA treatment was associated
with major maternal morbidity (Tables 3, 4) and it is notpossible to asseverate that they are not complications orfailures of the interventional radiologic technique, thesurgical technique, or both, it seemed to be unrelated tothe endovascular procedures because the incidence issimilar to those in other series of PA that did not useinterventional radiologic techniques (3). Specifically, wedid not relate the thromboembolism to interventionalradiology because it developed 2 weeks after the surgery,and the vesicovaginal fistula was present in a patientwith no catheterization. One patient experienced a minortransient complication as a consequence of arterialspasm, presumably associated with a mild femoralnerve injury. Similarly to our experience, small seriesof prophylactic embolization of uterine arteries inpatients with PA have shown a low rate of com-plications related to the endovascular procedure(12,13,21) (Table 5) (1,3,5,7,8,10,12–14,20–22,27,28).Some factors, such as the choice of endovasculartechnique (balloon occlusion vs selective embolization)and/or technical resources and operator experience, mayhelp to explain the different complication rates indifferent series. Given that there is no diagnostic testfor PA with 100% accuracy, the low complication ratereported is important when considering patients inwhom prophylactic selective bilateral uterine arterycatheterization is performed but PA is not confirmed

Izbizky et al ’ JVIR168 ’ Uterine Artery Catheterization/Embolization for Placenta Accreta
(approximately 17% in the present series). Importantly,even though the nine patients without imaging suspicionof PA (only clinical suspicion) did not actually have PA,we did not modify our protocol in patients who present ahigh pretest risk (ie, approximately 50% of PA inpatients with two previous cesarean sections and pla-centa previa) irrespective of the test results.Because PA is a life-threatening condition that
requires a multidisciplinary team for proper manage-ment, and because—as reported by our group and others(29,30)—approximately 30%–50% of patients with thiscondition will have an unscheduled delivery, mainly as aresult of vaginal bleeding, one concern is whethercatheter placement and embolization is feasible in stand-ard clinical practice. In our institution, in which staffand technological resources are available around theclock, prophylactic uterine arterial catheterization wasfeasible in 97% of patients.
Table 5 . Series with at Least 10 Cases of Placenta Accreta Reporting
and Blood Loss/Need for Blood Transfusion (1,3,5,7,8,10,12–14,20–22
Study, Year Cases IR Treatment
IR-R
Complic
O’Brien et al, 1996 (1) 109 BC (2 cases) N
Bodner et al, 2006 (7) 6 BC with/without PAE N
22 –
Bretelle et al, 2007 (20) 50 PAE (4 cases) 5
Shrivastava et al, 2007 (10) 19 BC 1
50 –
Mok et al, 2008 (14) 12 BC with or without PAE
Yu et al, 2009 (21) 11 PAE
Hoffman et al, 2010 (27) 29 BC‡
Warshak et al, 2010 (5) 99 BC§ N
Angstmann et al, 2010 (8) 26 BC or PAE|| N
Diop et al, 2010 (13) 17 PAE 5
Sentilhes et al, 2010 (22) 167 PAE N
Sivan et al, 2010 (28) 30 BC with or without PAE 1
Eller et al, 2011 (3) 79 – N
62 BC (9 cases) N
Li et al, 2014 (12) 12 UAE
Present series 95 UAE
BC ¼ pelvic artery balloon catheterization; IR ¼ interventional radiol
blood cells); NR ¼ not reported; PAE ¼ pelvic artery embolization; U
*In two of four cases, with conservative management.†Estimated in patients with estimated blood loss Z 2,500 mL.‡Fourteen of 29 bilateral iliac artery catheters (six common iliac and
balloons were never inflated in seven women, inflated prophylactic
five women.§Inflated only if significant bleeding.||If there was significant hemorrhage, prophylactic pelvic artery ballo
was performed (eight cases).¶One case with bilateral ovarian venous thrombosis 1 day after em
**A total of 25 of 167 patients required 4 5 U packed red blood ce††Minor catheterization-related complications included subcutaneou
[n ¼ 1]) and transient leg ischemia (n ¼ 3), which resolved spontan
The natural prognosis of PA is a potentially cata-strophic scenario (1). The morbidity can be dramatic andincludes disorders associated with massive bleeding suchas disseminated intravascular coagulation, multiple-organ failure, and even death (3). In most patients,hysterectomy is required to stop the bleeding (3). Thestandard of care in patients with prenatal diagnosis ofPA is cesarean section at tertiary-care hospitals withmultidisciplinary teams experienced in this condition (3–6). However, the optimal management remains contro-versial because none of the different strategies describedin the literature—elective hysterectomy or conservativemanagement with or without additional perioperativeinterventions (ie, use of interventional radiologic techni-ques)—were tested in prospective, randomized trials.Although the present study was not designed to establishthe efficacy of prophylactic bilateral uterine arteryembolization in diminishing intraoperative blood loss,
on the Use of Prophylactic Interventional Radiologic Treatment
,27,28)
elated
ations (%) LVBT (%)
Mean Blood
Transfusion (U)
Maternal
Death
R NR 7 7% (8 of 109)
R NR 6.5 No
NR 6.3
0* NR 4.9 No
5.8 NR 10 No
– NR 6.5
0 58 6.6 No
0 27† NR No
7 41.4 NR No
R NR 4.7 (prenatal diagnosis),
6.9 (no prenatal diagnosis)
No
R 46 0.5 (embolization) vs
7.9 (no embolization)
No
.8¶ NR NR No
R 15** NR 0.6%
7†† NR 4 No
R 43 2 No
R 61 5 1.6%
0 58.3 4.8 No
1 19 1.4 (catheterized group),
2 (all cases)
No
ogy; LVBT ¼ large-volume blood transfusion (Z 4 U packed red
AE ¼ uterine artery embolization.
eight internal iliac). Use of the catheters was highly variable: the
ally in two women, and inflated on the onset of hemorrhage in
on catheterization was performed. If not, selective embolization
bolization.
lls.
s hematoma (axillary hematoma [n ¼ 1] and groin hematoma
eously.

Volume 26 ’ Number 2 ’ February ’ 2015 169
it is interesting to note that a mean of only 1.4 U ofblood was transfused in the catheterized group, and only14% of patients who underwent catheterization requiredlarge-volume blood transfusion (3). These figures appearto be lower than in other large series that used differentstrategies in the management of PA, with or withoutcatheterization (Table 5).The present study has some limitations, including its
retrospective nature, the lack of a control group to assessthe effectiveness of the management strategy, the fact thatthe amount of blood loss was estimated rather thanobjectively measured, the fact that the need for transfusionrequirements was left to the discretion of the attendingphysician, the fact that the effects of radiation to motherand newborn were not measured, and the lack of long-term outcome data. Finally, another limitation is that mildevents such as a minor ecchymosis at the puncture site orother unclaimed symptoms may have been underreportedif patients did not notice or report such complaints.In conclusion, in the present series, perioperative
selective bilateral uterine artery catheterization andembolization in the management of PA appeared to bea feasible and safe intervention. The efficacy of thisstrategy for the management of patients with a prenataldiagnosis of PA, as well as its impact on maternaloutcomes, should be tested in larger series and withprospective randomized trials.
REFERENCES
1. O’Brien JM, Barton JR, Donaldson ES. The management of placentapercreta: conservative and operative strategies. Am J Obstet Gynecol1996; 175:1632–1638.
2. Flood KM, Said S, Geary M, Robson M, Fitzpatrick C, Malone FD.Changing trends in peripartum hysterectomy over the last 4 decades. AmJ Obstet Gynecol 2009; 200(6):632.e1.
3. Eller AG, Bennett MA, Sharshiner M, et al. Maternal morbidity in casesof placenta accreta managed by a multidisciplinary care team comparedwith standard obstetric care. Obstet Gynecol. 2011; 117:331–337.
4. Hull A, Resnik R. Placenta Accreta and Postpartum Hemorrhage. ClinObstet Gynecol. 2010; 53(1):228–236.
5. Warshak C, Ramos G, Eskander R, et al. Effect of Predelivery Diagnosis in99 Consecutive Cases of Placenta Accreta. Obstet Gynecol 2010; 115:65–69.
6. Publications Committee, Society for Maternal-Fetal Medicine, BelfortMA. Placenta accreta. Am J Obstet Gynecol 2010;203:430–439.
7. Bodner LJ, Nosher JL, Gribbin C, Siegel RL, Beale S, Scorza W. Balloon-assisted occlusion of the internal iliac arteries in patient with placentaaccreta/percreta. Cardiovasc Intervent Radiol 2006; 29:354–361.
8. Angstmann T, Gard G, Harrington T, Ward E, Thomson A, Giles W.Surgical management of placenta accreta: a cohort series and suggestedapproach. Am J Obstet Gynecol 2010;202:38.e1–e9.
9. Lee JS, Shepherd SM. Endovascular treatment of postpartum hemor-rhage. Clin Obstet Gynecol 2010; 53:209–218.
10. Shrivastava V, Nageotte M, Major C, Haydon M, Wing D. Case-controlcomparison of cesarean hysterectomy with and without prophylacticplacement of intravascular balloon catheters for placenta accreta. Am JObstet Gynecol 2007;197:402.e1–402.e5.
11. Gonsalves M, Belli A. The role of interventional radiology in obstetrichemorrhage. Cardiovasc Intervent Radiol. 2010; 33(5):887–895.
12. Li Q, Yang ZQ, Mohammed W, Feng YL, Shi HB, Zhou X. ProphylacticUterine Artery Embolization Assisted Cesarean Section for the Preven-tion of Intrapartum Hemorrhage in High-Risk Patients. CardiovascIntervent Radiol. 2014; 37:1458–1463.
13. Diop AN, Chabrot P, Bertrand A, et al. Placenta accreta: managementwith uterine artery embolization in 17 cases. J Vasc Interv Radiol 2010;21(5):644–648.
14. Mok M, Heidemann B, Dundas K, Gillespie I, Clark V. Interventionalradiology in women with suspected placenta accreta undergoing caesar-ean section. Int J Obstet Anesth 2008; 17(3):255–261.
15. Eller AG, Porter TF, Soisson P, Silver RM. Optimal managementstrategies for placenta accreta. Br J Oobstet Gynaecol 2009; 116:648–654.
16. Benirschke K, Kaufmann P, Baergen R. Pathology of the humanplacenta, Springer; New York, 5th edition, 2006.
17. Hung TH, Shau WY, Hsieh CC, Chiu TH, Hsu JJ, Hsieh TT. Risk factorsfor placenta accreta. Obstet Gynecol. 1999; 93(4):545–550.
18. Wu S, Kocherginski M, Hibbard J. Abnormal placentation: twenty-yearanalysis. Am J Obstet Gynecol 2005; 192:1458–1461.
19. Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of InterventionalRadiology clinical practice guidelines. J Vasc Interv Radiol 2003; 14(9 Pt2):S199–S202.
20. Bretelle F, Courbière B, Mazouni C, et al. Management of placentaaccreta: morbidity and outcome. Eur J Obstet Gynecol Reprod Biol 2007;133(1):34–39.
21. Yu PC, Ou HY, Tsang LL, Kung FT, Hsu TY, Cheng YF. Prophylacticintraoperative uterine artery embolization to control hemorrhage inabnormal placentation during late gestation. Fertil Steril 2009; 91(5):1951–1955.
22. Sentilhes L, Ambroselli C, Kayem G, et al. Maternal outcome afterconservative treatment of placenta accreta. Obstet Gynecol 2010; 115(3):526–534.
23. Ojala K, Perälä J, Kariniemi J, Ranta P, Raudaskoski T, Tekay A. Arterialembolization and prophylactic catheterization for the treatment for severeobstetric hemorrhage. Acta Obstet Gynecol Scand 2005; 84(11):1075–1080.
24. Alvarez M, Lockwood CJ, Ghidini A, Dottino P, Mitty HA, BerkowitzRL. Prophylactic and emergent arterial catheterization for selectiveembolization in obstetric hemorrhage. Am J Perinatol 1992; 9(5-6):441–444.
25. Heidemann B. Interventional radiology in the treatment of morbidlyadherent placenta: are we asking the right questions? Int J ObstetAnesth 2011; 20(4):279–281.
26. Chung JW, Jeong HJ, Joh JH, Park JS, Jun JK, Kim SH. Percutaneoustranscatheter angiographic embolization in the management of obstetrichemorrhage. J Reprod Med 2003; 48:268–276.
27. Hoffman MS, Karlnoski RA, Mangar D, et al. Morbidity associated withnonemergent hysterectomy for placenta accreta. Am J Obstet Gynecol2010; 202(628):e1–e5.
28. Sivan E, Spira M, Achiron R, et al. Prophylactic pelvic artery catheter-ization and embolization in women with placenta accreta: can it preventcesarean hysterectomy? American journal of perinatology 2010; 27(06):455–461
29. Bowman ZS, Manuck TA, Eller AG, Simons M, Silver RM. Risk factorsfor unscheduled delivery in patients with placenta accreta. Am J ObstetGynecol 2014; 210(3):241.e1–e6.
30. Meller CH, Izbyzky G, Otaño L. Timing of delivery in placenta accreta.Am J Obstet Gynecol 2014; 211:438–439.