Farmaci innovativi e terapie di associazione: quali ...terapie di associazione: quali opportunità?...
58
Giuse pp e Penno Dipartimento di Medicina Clinica e Sperimentale Farmaci innovativi e terapie di associazione: quali opportunità?
Farmaci innovativi e terapie di associazione: quali ...terapie di associazione: quali opportunità? Dichiarazione esplicita di trasparenza delle fonti di finanziamento e dei rapporti
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Einarson TR et al Cardiovasc Diabetol 2018 17 83
57 articles with 4549481 persons having T2DM 2007 - March 2017
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
BP blood pressure CV cardiovascular CVA cerebrovascular accident HF heart failure hHF hospitalisation for HF HR hazard ratio LDL-C low densityndashlipoprotein cholesterol MI myocardial infarction T2D type 2 diabetes
On average the patients with T2D had a 45 increase in the risk of hHF despite other major risk factors in guideline recommended range or absent
bull In this analysis the risk of hHF in patients with T2D (n=271174) was compared to those without T2D (n=1355870)
bull The following risk factors were either not present or within guideline range HbA1c systolic and diastolic BP LDL-C albuminuria and tobacco use
bull A substantial higher risk for hHF remained among patients who had all the variables within target range
No risk factors
Death
MI
hHF
CVA
HR (95 CI)
106 (100 112)
084 (075 093)
095 (084 107)
145 (134 157)
Risk of event in patients with T2D with no other risk factors out of range compared to patients without
diabetes
Rawshani A et al New Engl J Med 2018 379 633-644
Swedish National Disease Register
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
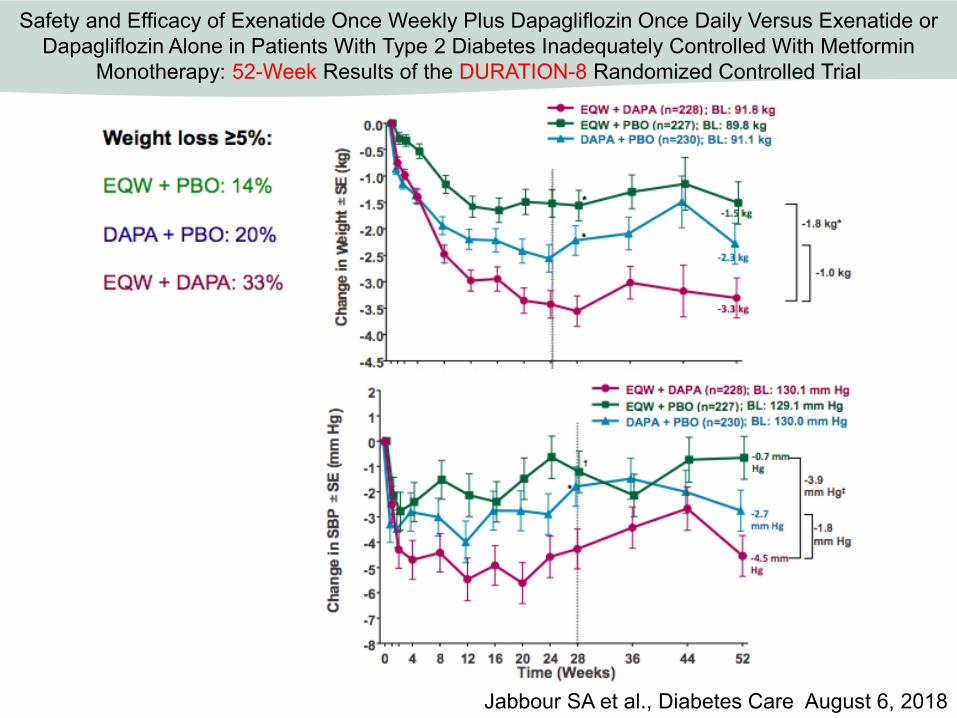
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Dichiarazione esplicita di trasparenza delle fonti di finanziamentoe dei rapporti con soggetti portatori di interessi commerciali
Il sottoscritto Dr Giuseppe Penno
in qualitagrave diModeratore Relatore
ai sensi dellrsquoart 33 sul Conflitto di Interessi pag 17 del Reg Applicativo dellrsquoAccordo Stato-Regione del 5 novembre 2009
dichiarache negli ultimi due anni ha avuto i seguenti rapporti anche di
finanziamento con soggetti portatori di interessi commerciali in campo sanitario
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Einarson TR et al Cardiovasc Diabetol 2018 17 83
57 articles with 4549481 persons having T2DM 2007 - March 2017
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
BP blood pressure CV cardiovascular CVA cerebrovascular accident HF heart failure hHF hospitalisation for HF HR hazard ratio LDL-C low densityndashlipoprotein cholesterol MI myocardial infarction T2D type 2 diabetes
On average the patients with T2D had a 45 increase in the risk of hHF despite other major risk factors in guideline recommended range or absent
bull In this analysis the risk of hHF in patients with T2D (n=271174) was compared to those without T2D (n=1355870)
bull The following risk factors were either not present or within guideline range HbA1c systolic and diastolic BP LDL-C albuminuria and tobacco use
bull A substantial higher risk for hHF remained among patients who had all the variables within target range
No risk factors
Death
MI
hHF
CVA
HR (95 CI)
106 (100 112)
084 (075 093)
095 (084 107)
145 (134 157)
Risk of event in patients with T2D with no other risk factors out of range compared to patients without
diabetes
Rawshani A et al New Engl J Med 2018 379 633-644
Swedish National Disease Register
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Progression of Contents
DIABETES BURDEN TODAY
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Einarson TR et al Cardiovasc Diabetol 2018 17 83
57 articles with 4549481 persons having T2DM 2007 - March 2017
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
BP blood pressure CV cardiovascular CVA cerebrovascular accident HF heart failure hHF hospitalisation for HF HR hazard ratio LDL-C low densityndashlipoprotein cholesterol MI myocardial infarction T2D type 2 diabetes
On average the patients with T2D had a 45 increase in the risk of hHF despite other major risk factors in guideline recommended range or absent
bull In this analysis the risk of hHF in patients with T2D (n=271174) was compared to those without T2D (n=1355870)
bull The following risk factors were either not present or within guideline range HbA1c systolic and diastolic BP LDL-C albuminuria and tobacco use
bull A substantial higher risk for hHF remained among patients who had all the variables within target range
No risk factors
Death
MI
hHF
CVA
HR (95 CI)
106 (100 112)
084 (075 093)
095 (084 107)
145 (134 157)
Risk of event in patients with T2D with no other risk factors out of range compared to patients without
diabetes
Rawshani A et al New Engl J Med 2018 379 633-644
Swedish National Disease Register
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Einarson TR et al Cardiovasc Diabetol 2018 17 83
57 articles with 4549481 persons having T2DM 2007 - March 2017
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
BP blood pressure CV cardiovascular CVA cerebrovascular accident HF heart failure hHF hospitalisation for HF HR hazard ratio LDL-C low densityndashlipoprotein cholesterol MI myocardial infarction T2D type 2 diabetes
On average the patients with T2D had a 45 increase in the risk of hHF despite other major risk factors in guideline recommended range or absent
bull In this analysis the risk of hHF in patients with T2D (n=271174) was compared to those without T2D (n=1355870)
bull The following risk factors were either not present or within guideline range HbA1c systolic and diastolic BP LDL-C albuminuria and tobacco use
bull A substantial higher risk for hHF remained among patients who had all the variables within target range
No risk factors
Death
MI
hHF
CVA
HR (95 CI)
106 (100 112)
084 (075 093)
095 (084 107)
145 (134 157)
Risk of event in patients with T2D with no other risk factors out of range compared to patients without
diabetes
Rawshani A et al New Engl J Med 2018 379 633-644
Swedish National Disease Register
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
BP blood pressure CV cardiovascular CVA cerebrovascular accident HF heart failure hHF hospitalisation for HF HR hazard ratio LDL-C low densityndashlipoprotein cholesterol MI myocardial infarction T2D type 2 diabetes
On average the patients with T2D had a 45 increase in the risk of hHF despite other major risk factors in guideline recommended range or absent
bull In this analysis the risk of hHF in patients with T2D (n=271174) was compared to those without T2D (n=1355870)
bull The following risk factors were either not present or within guideline range HbA1c systolic and diastolic BP LDL-C albuminuria and tobacco use
bull A substantial higher risk for hHF remained among patients who had all the variables within target range
No risk factors
Death
MI
hHF
CVA
HR (95 CI)
106 (100 112)
084 (075 093)
095 (084 107)
145 (134 157)
Risk of event in patients with T2D with no other risk factors out of range compared to patients without
diabetes
Rawshani A et al New Engl J Med 2018 379 633-644
Swedish National Disease Register
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Chart1
Y-Values
4
3
2
1
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
106
006
006
NaN
NaN
084
009
009
NaN
NaN
095
012
011
0
0
145
012
011
Sheet1
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
death
106
4
1
112
006
006
MI
084
3
075
093
009
009
CVA
095
2
084
107
011
012
0
0
HF
145
1
134
157
011
012
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
bull Consider adding the other class (GLP-1 RA or SGLT2i) with proven CVD benefit
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Association for the Study of Diabetes (EASD)
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
bull Consider adding the other class (GLP-1 RA or SGLT2i)
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
HR 078 (95CI 068 090)plt0001
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
aNew onset of macroalbuminuria or a doubling of the serum creatinine level and an eGFR of le45 mlmin173 m2 the need for continuous renal-replacement therapy or death from renal disease bNew or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinine clearance of less than 45 mlmin173 m2
(according to the Modification of Diet in Renal Disease criteria) or the need for continuous renal-replacement therapy c40 eGFR decline renal replacement renal death or new-onset macroalbuminuria dAdjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline glycated hemoglobin eGFR and body-mass index eIncludes fatal and nonfatal events f Composite of CV death or hospitalization for heart failure CI confidence interval CV cardiovascular eGFR estimated glomerular filtration rate GLP-1 RA GLP-1 receptor agonists HR hazard ratio MACE major adverse cardiovascular events MI myocardial infarction QW once weekly1 Marso SP et al N Engl J Med 2016375311ndash322 2 Marso SP et al N Engl J Med 20163751834ndash1844 3 Holman RR et al Article and supplementary appendix N Engl J Med 20173771228-1239 4 Bethel MA et al Presented at ADA 78th Scientific Sessions June 22-26 2018 Orlando FL Poster 522-P 5 Hernandez AF et al Online ahead of print Lancet 2018
MACE
Death from CV causes
Nonfatal MI
Nonfatal stroke
Renal endpoint
Favors placebo
Favors liraglutid
e
LEADER1
Hosp for heart failure
087 (078 097)
078 (066 093)
088 (075 103)
089 (072 111)
087 (073 105)
078 (067 092)a
HR (95 CI)
Favors placebo
Favors semaglut
ide
074 (058 095)
098 (065 148)
074 (051 108)
061 (038 099)
111 (077 161)
064 (046 088)b
HR (95 CI)
Favors placebo
Favors exenatide
QW
091 (083 100)
088 (076 102)
095 (084 109)
086 (070 107)
094 (078 113)
085 (074 098)cd
Favors placebo
Favors albigluti
de
078 (068 090)
093 (073 119)
075 (061 00)e
086 (066 114)e
085 (070 104)f
HR (95 CI) HR (95 CI)
SUSTAIN-62 EXSCEL34 HARMONY5
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
087
01
009
078
015
012
088
015
013
089
022
017
087
018
014
078
014
011
1
0
0
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
087
7
078
097
009
01
Death from CV causes
078
6
066
093
012
015
Nonfatal myocardial infarction
088
5
075
103
013
015
Nonfatal stroke
089
4
072
111
017
022
Hospitalization for heart failure
087
3
073
105
014
018
Renal endpoint (Nephropathy newonset of macroalbuminuria or a doubling of theserum creatinine level and an eGFR of le45 mlper minute per 173 m2 the need for continuousrenal-replacement therapy or death from renaldisease)
078
2
067
092
011
014
1
0
0
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
091
009
008
088
014
012
095
014
011
086
021
016
094
019
016
085
013
011
1
0
0
Sheet1
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
091
7
083
1
008
009
Death from CV causes
088
6
076
102
012
014
Nonfatal myocardial infarction
095
5
084
109
011
014
Nonfatal stroke
086
4
07
107
016
021
Hospitalisation for heart failure
094
3
078
113
016
019
Renal endpoint (defined as 40 eGFR decline renal replacement renal death or new-onset macroalbuminuria Adjusted for age sex ethnicity race region duration of diabetes prior history of CV event insulin use baseline HbA1c eGFR and BMI)
085
2
074
098
011
013
1
0
0
Chart1
Y-Values
7
6
5
4
3
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
078
012
01
093
026
02
075
015
014
086
028
02
085
019
015
2
0
0
Sheet1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
078
7
068
09
01
012
Death from CV causes
093
6
073
119
02
026
Myocardial infarction
075
5
061
09
014
015
Ischemic stroke
086
4
066
114
02
028
Composite of CV death or hospitalisation for heart failure
085
3
07
104
015
019
Renal endpoint (not reported)
2
0
0
1
Chart1
Y-Values
7
6
5
4
3
2
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
074
021
016
098
05
033
074
034
023
061
038
023
111
05
034
064
024
018
1
0
0
Sheet1
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Primary efficacy endpoint
074
7
058
095
016
021
Death from CV causes
098
6
065
148
033
05
Nonfatal myocardial infarction
074
5
051
108
023
034
Nonfatal stroke
061
4
038
099
023
038
Hospitalisation for heart failure
111
3
077
161
034
05
Renal endpoint (New or worsening nephropathy includes persistent macroalbuminuria persistent doubling of the serum creatinine level and a creatinineclearance of less than 45 ml per minute per 173 m2 of body-surface area (according to the Modification of Diet in Renal Disease criteria)or the need for continuous renal-replacement therapy)
064
2
046
088
018
024
1
0
0
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
Hernandez AF et al Lancet 2018 October 2
Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes) a double-blind randomised placebo-
controlled trial
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7) a multicentre
open-label randomised trial
Tuttle KR et al Lancet Diabetes Endocrinol 2018 6 605-617
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
1 Zinman B et al N Engl J Med 20153732117ndash2128 2 Neal B et al N Engl J Med 2017 DOI 101056NEJMoa16119253 Sattar Diabetologia (2013) 56686ndash695 4 Raz I et al Diabetes Obes Metab 2018 httpdxdoiorg101111dom13217
34of patients did not have eCVD
~60of patientsdid not have eCVD
1of patients did not have eCVD
Rates of pts with and without established CVD varied across the three SGLT2i CVOTs
EMPA-REG OUTCOME(N=7020)
CANVAS(N=10142)
DECLARE(N=17160)
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
Chart1
Sales
066
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
034
66 had eCVD
Sheet1
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sales
0
66 had eCVD
1
SUM(D14)
Chart1
Sales
099
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
001
99 eCVD
Sheet1
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sales
0
99 eCVD
1
SUM(D14)
Chart1
Sales
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
06
04
Sheet1
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sales
1
40
0
SUM(D14)
N at risk is the number of subjects at risk at the beginning of the period 2-sided p-value is displayed HR CI and p-value are from cox proportional hazard model CV cardiovascular Dapa dapagliflozin hHF hospitalization for heart failure MACE major adverse cardiac eventWiviott SD et al Online ahead of print N Engl J Med 2018
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
1
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Two-sided p-value is shown for the primary efficacy composite outcome of CV death or hHFCV cardiovascular DAPA dapagliflozin HF heart failure hHF hospitalization for heart failure Wiviott SD et al Online ahead of print New Engl J Med 2018
121110080706
Composite of hHFCV death 417 496 083 (073 095) 0005
Hospitalization for HF 212 286 073 (061 088)
CV death 245 249 098 (082 117)
09
Number of events
DAPA 10 mg(N=8582)
Placebo(N=8578) HR (95CI) p-value
Favors DAPA Favors Placebo
Dapagliflozin and Cardiovascular Outcomesin Type 2 Diabetes
hHF or CV Death
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
CV cardiovascular eCVD established CV disease HF heart failure hHF hospitalized heart failure SGLT-2i SGLT co-transporter 2 inhibitor T2D type 2 diabetesWiviott SD et al Online ahead of print N Engl J Med 2018
078 (063 097)
Hazard ratio(95 CI)
Favors Dapagliflozin Favor Placebo
064 (046 088)
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
073 (055 096)Prior HF
073 (058 092)No prior HF
10 of patients in DECLARE had prior HF
Hazard ratio(95 CI)
hHF by presenceabsence of eCVD hHF by presenceabsence of previous HF
Hospitalization for HF Hospitalization for HF
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Favors Dapagliflozin Favor Placebo
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Chart1
Y-Values
4
2
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
6
0
0
078
019
015
5
0
0
3
0
0
064
024
018
1
0
0
Sheet1
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
ECVD
078
4
063
097
015
019
5
0
0
3
0
0
MRF
064
2
046
088
018
024
1
0
0
Chart1
Y-Values
4
2
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
6
0
0
073
023
018
5
0
0
3
0
0
073
019
015
1
0
0
Sheet1
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
6
0
0
Prior HF
073
4
055
096
018
023
5
0
0
3
0
0
No Prior HF
073
2
058
092
015
019
1
0
0
daggerRenal composite endpoint defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal or CV death (pre-specified secondary outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal disease1 Raz I et al Diabetes Obes Metab 2018201102ndash1110 2 Wiviott SD et al Online ahead of print N Engl J Med 2018 3 Zinman B et al N Engl J Med 20153732117ndash2128 4 Neal B et al N Engl J Med 2017377644ndash657
Placebo (480 Events)Renal CompositedaggerThe patients in the DECLARE12 trial had better baseline renal function than the EMPA-REG OUTCOME3 or CANVAS4 trials
DEC
LAR
E
CAN
VAS
EMPA
-REG
eGFR mean(mLmin173m2)
852 765 741
Micro-macro-albumin-uria ()
302 302 406
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
Overall population
ge90 mLmin173 m2
60 to lt90 mLmin173 m2
lt60 mLmin173 m2
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
050 (034 073)
054 (040 073)
060 (035 102)
Baseline eGFRa
053 (043 066)
InteractionP value = 087
Overall population
eCVD
Multiple Risk Factors
Hazard ratio (95 CI)
Favors Dapagliflozin Favors Placebo
Composite of ge40 decrease in eGFRa to lt60 mLmin173 m2 ESRD or renal deathc
055 (041 075)
051 (037 069)
CV risk
053 (043 066)
InteractionP value = 072
daggerRenal composite endpoint without CV death defined as sustained confirmed eGFR decrease ge 40 to eGFR lt 60 mlmin173m2 using CKD-EPI equation andor ESRD (dialysis ge 90 days or kidney transplantation sustained confirmed eGFR lt 15 mlmin173m2) andor renal death (pre-specified additional renal composite outcome)CV cardiovascular CKD chronic kidney disease Dapa dapagliflozin eGFR estimated glomerular filtration rate ESRD end-stage renal diseaseWiviott SD et al Online ahead of print N Engl J Med 2018
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
Chart1
Y-Values
6
4
3
2
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
053
013
01
05
023
016
054
019
014
06
042
025
1
0
0
Sheet1
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
6
043
066
01
013
gt90
05
4
034
073
016
023
60-90
054
3
04
073
014
019
lt60
06
2
035
102
025
042
1
0
0
Chart1
Y-Values
5
3
2
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
053
013
01
4
0
0
055
02
014
051
018
014
Sheet1
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
X-Values
Y-Values
95 min
95 max
95 min for graph
95 max for graph
Overall
053
5
043
066
01
013
4
0
0
ASCVD
055
3
041
075
014
02
MRF
051
2
037
069
014
018
Verma S Juumlni P Mazer CD The Lancet 2018 in press
These data with dapagliflozin from DECLARE- TIMI 58 extend the benefit of SGLT2i to a broader population of patients for primary and secondary
prevention
Key messages
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of myocardial infarction stroke and cardiovascular death (major adverse cardiovascular events MACE)
stratified by the presence of established atherosclerotic cardiovascular disease
Similar pattern for Myocardial infarction CV death all-cause mortalityNo effect on stroke
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on major adverse cardiovascular events (MACE)
stratified by the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified by the presence of established atherosclerotic
cardiovascular disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on hospitalisation for heart failure and cardiovascular death stratified
by history of heart failure
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trialsMeta-analysis of SGLT2i trials on hospitalization for heart failure stratified by
the eGFR level
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on the composite of renal worsening ESRD or renal death stratified by the presence of established atherosclerotic cardiovascular
disease
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Zelniker TA et al The Lancet 2018 November 10
Meta-analysis of SGLT2i trials on composite of worsening of renal function ESRD or renal death stratified by the eGFR level
SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes a systematic
review and meta-analysis of cardiovascular outcome trials
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Devies MJ et al Diabetologia amp Diabetes Care 2018 October 5
Management of Hyperglycemia in Type 2 Diabetes 2018 A Consensus Report by the American Diabetes Association (ADA) and the European
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Lingway I Endocrine Practice 2017
BASAL INSULIN
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial plasma glucose1 Marathe PH et al J Diabetes 20179320ndash324 2 Blevins T Postgrad Med 2011123135ndash1473 Wilcox G Clin Biochem Rev 20052619ndash39 4 Russell-Jones D Diabetes Obes Metab 20079799ndash8125 Aronoff SL et al Diabetes Spectr 200417183ndash190 6 Meier JJ Nat Rev Endocrinol 20128728ndash742
Increases glucose disposalDecreases hepatic glucose production
Suppresses ketogenesis
Body weight Increases satietyIncreases fatty acid synthesis
Risk of hypoglycemia Glucose-dependent insulin secretionEffects are not glucose-dependent
Neutral effect
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Potential clinical benefits of basal insulin amp GLP1-RAs
Basal insulin GLP-1 RA+
Potential for
FPG reductions
Reduced PPG excursions
Less weight gain
Reduced risk of hypoglycemia
Improvement in CV risk factors amp MACE
Additional A1C reductions
A1C glycated hemoglobin CV cardiovascular FPG fasting plasma glucose GLP-1 RA glucagon-like peptide-1 receptor agonist PPG postprandial glucose1 Gough S et al Diabetes Obes Metab 201517965ndash973 2 Marso SP et al N Eng J Med 2016375311ndash322 3 Marso SP et al N Eng J Med 20163751834ndash1844
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Efficacy outcomes for iGlarLixi and IDegLira
Nuffer W et al Therapeutic Advances in Endocrinology and Metabolism 9 69-79 2018
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
What combinations are availables IDegLira (up to 50 UI18 mg) and iGlarLixi (up to 60 UI20 microg)
What are the main benefits single daily injection robust BG-lowering beyond either insulin or GLP1-RA alone weight neutralityloss similar or reduced risk of hypoglycemia compared with insulin alone
What are the main disadvantages patients may require amounts of insulin or GLP1-RA in a different ratio
Who is a good candidate for insufficient BG control on a combination of OHAs insufficient BG control either on basal insulin or a GLP1-RA alone avoiding addition of prandial insulin
Who is a poor candidate for patients with history of pancreatitis family history of medullary thyroid cancer
Starting IDegLira 16 steps iGlarLixi 15 or 30 steps (if basal insulin lt or gt30 UI)
Adjustmenttitration IDegLira plusmn2 steps every 3-4 days iGlarLixi 2-4 steps weekly adjustments are made based on the insulin not the GLP1-RA component
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Lingway I Endocrine Practice 2017
Rationale for the combination of DPP-4 and SGLT2 inhibition
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
DPP4iSGLT2i + Metformin Provides a Logical Approach to T2DM Treatment Through Complementary Mechanisms
bull DPP4iSGLT2i combination is differentiated from other therapies due to its complementary mechanisms that target multiple disease pathways1
bull DPP4i slow the deactivation of GLP-1 in the circulation resulting in23
bull SGLT2i exert effects on the kidneys to4
Glucose reabsorption
Urinary glucose excretion
Glucagon secretion
αβ
Glucose uptakeGlycogen synthesis
Glucose uptakeGlycogen synthesis
Insulin secretion
Hepatic glucose production
Glucoseuptake
bull Metformin exerts its effects to4
1 DeFronzo RA Diabetes 200958773ndash795 2 Wang A et al BMC Pharmacology 2012 Apr 41223 Drucker DJ Nauck MA Lancet 20063681696ndash1705 4 Paisley AN et al Expert Opin Investig Drugs 201322131ndash140
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Emerging use of combination therapies for the management of type 2 diabetes ndash focus on saxagliptin and dapagliflozin
Yu H et al Diabetes Metabolic Syndrome and Obesity Targets and Therapy 10 337-332 2017
Five completed phase III trials and at least seven trials ongoing
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Pharmacokinetic drug evaluation of empagliflozin plus linagliptin for the treatment of type 2 diabetes
Four completed phase III trials others ongoing
Rizos CV et al Exper Opinion on Drug Metabolism amp Toxicology [Epub ahead of print] 2018
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Ertugliflozin and Sitagliptin the VERTIS Program Three completed phase III trials others ongoing
Reductions from baseline in HbA1c Placebo E5S100 E15S100
Ertugliflozin and Sitagliptin Co-initiation in Patients with Type 2 Diabetes The VERTIS SITA Randomized Study
-04 -16 -17
E5 E15 S100
E5S100 E15S100
Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with T2DM inadequately controlled with metformin The VERTIS FACTORIAL randomized trial
-10-11-11
-15 -15
Placebo E5 E15Efficacy and safety of the addition of ertugliflozin in patients with T2DM inadequately controlled with metformin and sitagliptin The VERTIS SITA2 placebo-controlled randomized study
00 -07 -08
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Additivity in glycemic and pleiotropic effects Reductions from baseline in combination therapy vs either agent alone
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Lingway I Endocrine Practice 2017
Rationale for the combination of SGLT2i and GLP1-RA
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Frias JP et al Lancet Diabetes
Endocrinol September 6 2016
Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with T2DM inadequately controlled with metformin monotherapy (DURATION-8) a 28 week multicentre double-blind phase 3 randomised trial
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Jabbour SA et al Diabetes Care August 6 2018
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Safety and Efficacy of Exenatide Once Weekly Plus Dapagliflozin Once Daily Versus Exenatide or Dapagliflozin Alone in Patients With Type 2 Diabetes Inadequately Controlled With Metformin
Monotherapy 52-Week Results of the DURATION-8 Randomized Controlled Trial
Jabbour SA et al Diabetes Care August 6 2018
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Dulaglutide as add-on therapy to SGLT2 inhibitors in patients with inadequately controlled type 2 diabetes (AWARD-10)
a 24-week randomised double-blind placebo-controlled trial
Ludvik B et al Lancet Diabetes Endocrinol February 23 2018
dulaglutide given as add-on treatment to any of the three available SGLT2 inhibitors (plusmnmetformin)
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Van Baar MJB et al Diabetes Care 41 1543-1556 2018
Expected and demonstrated net effects in combination therapy with SGLT2is in T2DM
All combined effects are expected effects based on single-drug effects except for which are demonstrated net effects in combination studies
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
The effects of GLP-1
receptoragonists are
shown in purple boxes
those of SGLT2
inhibitors in green boxes
and those of both classes
in orangeboxes
Mechanisms of action of GLP-1
receptor agonists and SGLT2
inhibitors
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
Progression of Contents
DIABETES BURDEN TODAY
CONSENSUS ADA-EASD 2018
WHAT THE NEXT FUTURE HOLDS TO US
GLP-1 RA AN UPDATING
SGLT2i AN UPDATING
COMBINATION OF INNOVATIVES
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
copy AstraZeneca 2018
Canagliflozin Renal Outcomes Study ndash Halted Early for Efficacy
bullCREDENCE ndash Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation
bull4400 patients with T2DM and eGFR between 30 to 90 mlmin173 mq on ACE inhibitors or ARBs
bullStudy halted nearly a year sooner = the primary composite endpoint (ESRD doubling of serum creatinine or Cv death) has been achieved
bullSGLT2-i as the first therapy to treat patients with DKD and T2DM in more than 15 years
bullCVD and DKD are inextricably linked in diabetes
CREDENCE Canagliflozin
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
copy AstraZeneca 2018
Superiority in reduction of cardiovascular events for broad range of T2DM
bullREWIND ndash Researching cardiovascular Events with a Weekly INcretin in Diabetes
bullA clinical trial (n 9901) that included a majority of participants who did not have established CV disease in a median follow-up period of more than 5 years
bullOnly 31 of participants had established CVD at baseline
bullDulaglutide significantly reduces major adverse cardiovascular events (MACE) across a broad range of people with T2DM
bullThe 9901 participants had a mean duration of diabetes of 10 years and a mean baseline HbA1c of 73
REWIND Dulaglutide
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity
Diapositiva numero 36
Diapositiva numero 37
Diapositiva numero 38
Diapositiva numero 39
Diapositiva numero 40
Diapositiva numero 41
Diapositiva numero 42
Diapositiva numero 43
Diapositiva numero 44
Diapositiva numero 45
Diapositiva numero 46
Diapositiva numero 47
Diapositiva numero 48
Diapositiva numero 49
Diapositiva numero 50
Diapositiva numero 51
Diapositiva numero 52
Diapositiva numero 53
Diapositiva numero 54
Diapositiva numero 55
Diapositiva numero 56
Diapositiva numero 57
Diapositiva numero 58
copy AstraZeneca 2018
Thank for your attention
Diapositiva numero 1
Diapositiva numero 2
Diapositiva numero 3
Prevalence Rates of CV Comorbidities in Persons With T2DM Results of a Systematic Literature Review
Despite control of known CV risk factors patients with T2D remain at elevated risk of developing HF
Diapositiva numero 6
Diapositiva numero 7
Diapositiva numero 8
Diapositiva numero 9
Diapositiva numero 10
Diapositiva numero 11
Diapositiva numero 12
Earlier studies with diabetes treatments did not definitively show benefit for CV disease and HF GLP-1 RAs are shown to have CV benefits driven by fewer atherosclerotic events
Diapositiva numero 14
Diapositiva numero 15
Diapositiva numero 16
Diapositiva numero 17
Diapositiva numero 18
Representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
Diapositiva numero 20
Diapositiva numero 21
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Dapagliflozin slowed renal disease progression in T2D patients with relatively good baseline renal function
This renal benefitdagger is demonstrated across eGFR subgroups and in patients with and without established CV disease
Key messages
Diapositiva numero 26
Diapositiva numero 27
Diapositiva numero 28
Diapositiva numero 29
Diapositiva numero 30
Diapositiva numero 31
Diapositiva numero 32
Diapositiva numero 33
Diapositiva numero 34
Complementary mechanisms of action that address several of the underlying patho-physiological abnormalities of T2DM without overlapping toxicity