Embed Size (px)
Citation preview

FAR EASTERN UNIVERSITY - DR. NICANOR REYES MEDICAL FOUNDATION
Medical JournalEditor-in-Chief
POLICARPIO B. JOVES JR., MD, MPH, MOH, FPAFP
Associate EditorMACARIO F. REANDELAR JR., MD, MSPH, FPAFP
FAR EASTERN UNIVERSITY - DR. NICANOR REYES MEDICAL FOUNDATION
BIOCHEMISTRY & NUTRITIONMari-Ann B. Bringas, MD, DPAAB
HUMAN STRUCTURAL BIOLOGYLeona Melodia T. Matheus, MD, FPCS,FPSGS
MICROBIOLOGY & PARASITOLOGYCerelyn E. Dacula, MD, MSc, DPPS
CLINICAL LAB./PATHOLOGYCheryl May A. Cabrera, MD, MPM, FPSP
CHILD HEALTHEva I. Bautista, MD, MSc, FPPS
COMMUNITY & FAMILY MEDICINEJenell O. Naldo, MD, MPH, FPAFP
OBSTETRICS & GYNECOLOGYLylah D. Reyes, MD, MSc, FPOGS
OPHTHALMOLOGYAngelico L. Alejo, MD, DPBO
RADIOLOGYMa. Theresa M. Bisquera, MD, FUSP, FPCR
SURGERYOmar O. Ocampo, MD, FPCS, FPSCRS, FPSGS, FPALES
ANESTHESIOLOGYKhristine I. Ramos, MD, FPSA
PHARMACOLOGYAbraham Daniel C. Cruz, MD, MSPH
PHYSIOLOGYRonald Allan G. Cruz, MD, FPSP
OTORHINOLARYNGOLOGY-HEAD & NECKSURGERYCecile C. Cobangbang, MD, FPSOHNS
INTERNAL MEDICINEEleazar P. Daet, MD, FPCP, FPCC
SCHOOL OF RESPIRATORY THERAPYCesar Ayes M. Ong, MD, FPPS, FPAPP, MHPEd
SCHOOL OF NUTRITION & DIETETICSFelina P. Calimbo, RND, MPH
SCHOOL OF NURSINGBenilda V. Medallo, RN, MAN
GENERAL EDUCATIONRose Marie Mendoza, ChE, PhD
EDITORIAL CONSULTANTS
REY H. DE LOS REYES, MD, MHA, FPOGSDean, School of Medicine
NOLAN E. PECHO, MD, MBAH, FPCSChief of Clinics
MAGDALENA F. NATIVIDAD, RMT, MSPH, PhDDean, School of Medical Technology
TITA Y. CRUZ, RN, MAN, EdDDean, School of Nursing
EDITHA C. DIZON, MD, FPARMDean, School of Physical Therapy
REY MELCHOR F. SANTOS, MD, MHA, FPCS, FACS, FPSGS, FPALESChairman, Research Development Office
PIO T. ESGUERRA, MD, FPCP, FPCCP, DIHDean, School of Respiratory Therapy
MARITES V. SINGH, RND, PhDDean, School of Nutrition & Dietetics
ROSALINDA C. SOLEVILLA, RPh, PhDDean, School of Pharmacy
MARCELINO E. MENDOZA, MD, FPCR, FUSPDean, School of Radiologic Technology
SCHOOL OF MEDICINE
SCHOOL OF RADIOLOGIC TECHNOLOGYNestor Q. Galvez, RRT, MPH
SCHOOL OF PHYSICAL THERAPYLeonilo F. Pallasigui, MRS, PT, PTRP, ACE-CPT
SCHOOL OF PHARMACYRobert Paul S. Lim, RPh
SCHOOL OF MEDICAL LABORATORY SCIENCESherwin N. Reyes, RMT, MSc, ISID

EDITORIAL AND BUSINESS COMMUNICATIONS
Submission of Contributions
All manuscripts and correspondence should be addressed to the Editor in Chief.
All articles are subject to editorial revision. Neither the Editorial Board nor the publisher acceptresponsibility for the views and statements of the authors, and clearances, such as permission fromsuperiors and patients for publication of pictures, should be obtained whenever necessary.
All scientific papers and other manuscripts submitted become the property of the FEU MedicalJournal and will not be returned unless a written request is directed to the Editor in Chief with thereasons for such request.
Manuscripts
Manuscripts should be typewritten on one side of the paper only, with double spacing and liberalmargins. References should be placed at the end of the article, numbered in the order of appearance inthe paper, and should conform to the usual style, viz., author’s last name and initials, title of article,periodical’s name in standard abbreviation, volume number, page and date of publication. Referencesto books should include author, title, edition, publisher, city and year of publication and page of reference.
Illustrations
Illustrations accompanying manuscripts should be numbered, provided with suitable legends, andmarked lightly on the back with author’s name. Author should indicate on the manuscript theapproximate position of tables and text figures. Tables should be typed on separate sheets of paper, notin the next, with one table to a page. Captions of the tables should be brief and clear.
Photographs should be distinct, black and white on glossy paper, and drawings done in black ink,properly captioned. The Journal will defray the cost of no more than (4) cuts per article, while the excesswill have to be paid by the author. Color photographs may also be published by special arrangements.
Reprints
Twenty-five reprints are furnished free to the authors, from whom reprints should be obtained.Orders for additional reprints may be arranged with the Business Manager.
All editorial contents of the Journal are covered by copyright and may not be reprinted withoutpermission. Reproduction of articles for commercial purposes will not be permitted.
Advertisements
Advertisements of ethical pharmaceutical products will be given space. Advertisements from otherfirms will be allowed provided that final approval for such shall be given by the Editorial Board.

FEU-NRMF Medical JournalVolume 23 Number 2 December, 2017
Contents
Original Research
Chocolate Agar Plate Modification with Seed Extract from Cacao Tree(Theobroma cacao L.) in Culturing Haemophilus influenza 37
Wilniel Bryan F. Calibuso, Ryan Kenneth G. Canoy, Bernadette Jia M. Cruz,Anne Beatrize U. Cua, Bonn Joseph H. Dedace, Ray Arden G. Demotica,Anjunelle S. Esquivel, Bryan E. Napuaga, Chellie Mae D. Serrano,Maria Corina O. Velasco and Alicia A. Aldave
Case Reports
Cesarean Scar Pregnancy: "A Rarity No More?" A Report of 2 Cases 46Denise Elaine A. Reyes, MD
A Rare Case of an Ovarian Epithelial Tumor in a Pre-menarchal Adolescent Girl 56Justin W. Ng Sinco, MD
Iridocorneal Endothelial (Ice) Syndrome 62Ferdinand N. Valbuena Jr., MD
Squamous Cell Carcinoma of the Temporal Bone 70Josef Carlo Angbue Te, MD; Bernardo D. Dimacali, MD;Nathaniel W. Yang, MD and Jose Roberto V. Claridad, MD

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 37
Chocolate Agar Plate Modification with Seed Extract fromCacao Tree (Theobroma cacao L.) inCulturing Haemophilus influenza*
Wilniel Bryan F. Calibuso, Ryan Kenneth G. Canoy, Bernadette Jia M. Cruz, Anne Beatrize U. Cua,Bonn Joseph H. Dedace, Ray Arden G. Demotica, Anjunelle S. Esquivel, Bryan E. Napuaga,
Chellie Mae D. Serrano, Maria Corina O. Velasco and Alicia A. Aldave
Background: Isolation and identification of certain genus and species of bacteria can be done through growthin a culture medium. One example of such medium is Chocolate Agar Plate (CAP), a non-selective mediawherein certain enrichment factors are added to promote or enhance growth of some fastidious bacteria.Haemophilus influezae are small, non-motile gram negative coccobacilli, and are fastidious by nature. Theyrequire factors for growth such as Heme factor and Nicotine Adenine Dinucleotide factor. These requirementsare provided in CAP to support its growth. Theobroma cacao is a small evergreen tree that is readilyavailable in the Philippines. In many studies, it was proven that cacao has inhibitory effects to bacteria butnot the genus Haemophilus.Objectives: This study involved the cultivation of a purer culture of H.influenzae through the replacement ofthe inhibitory agent bacitracin with crude extract of cocoa to see if the modified chocolate agar plate iscapable of producing results equal to the standard or greater in terms of suppressing the growth of othercontaminant bacteria thus promoting growth of purer culture of H. influenzae.Methods:Theobroma cacao seeds were ground and extracted via ethanolic extraction then subjected to rotaryevaporation that yielded the crude extract and incorporated to the CAP as the experimental plates, BacitracinCAP served as the control. Three concentrations are prepared from the Theobroma cacao crude extract. Fourorganisms were used. Haemophilus influenza, as the organism in focus in the study and other organismswhich are the usual undesired organisms. The organisms were inoculated on both the plates and observed forthe growth and number of colonies.Results:Modified CAP with seed extract from cacao tree with the concentration of 3%, 5% and 10% have notshown selectivity to Haemophilus influenza because of having a significant difference to the standard Bacitracinchocolate agar plate.Conclusion: The researchers have concluded that the modified CAP with seed extract from cacao tree withthe concentration of 3% and 5 % have not shown selectivity to Haemophilus influenzae while 10% of cacaomodified CAP have not shown its selectivity as well but was able to show how increasing concentration ofcocoa extract affect the growth of the selected organism.
Key words: Theobroma cacao, chocolate apgar plate, Haemophilus influenza, bacitracin chocolate apgar plate
Isolation and identification of certain genus andspecies of bacteria can be done through growth in aculture medium. One example of such medium is
ABSTRACT
Chocolate Agar Plate (CAP). It is a non-selectivemedia wherein certain enrichment factors are addedto promote or enhance growth of some fastidiousbacteria. Examples include the genus Neisseria andgenus Haemophilus. In order to have a selective CAPwherein the growth of genus Haemophilus ispromoted while the growth of genus Neisseria and* From the School of Medical Laboratory Science

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201738
other contaminant bacteria like Escherichia coli,Kleibsiella sp., Proteus sp ., and Pseudo sp. issuppressed, bacitracin is added. However, in somestudies it is found that bacitracin cannot totally inhibitthe growth of these contaminant bacteria. Growth ofother contaminant bacteria in the medium can lead tofalse diagnosis in the clinical setting, providinginaccurate and invalid detection of the actual causeof bacterial infection.
Theobroma cacao Linnaeus family Malvaceaeisa small evergreen tree that is readily available in thePhilippines. It is mainly used for the production ofchocolate products. Aside from it being used as aningredient for producing chocolates, it is also prizedfor its medicinal and aphrodisiacal properties. Healthbenefits include antioxidant activity, cardiovascularprotection, skin health, stimulants (though less powerfulcompared to caffeine), and antibacterial effect. Inmany studies, it was proven that cacao has bactericidalor inhibitory effects to many genus and species ofbacteria including Neisseria sp., Escherichia coli,Kleibsiella sp., Proteus sp., and Pseudomonas sp.but not the genus Haemophilus. This study involvesthe cultivation of a purer culture of Haemophilusinfluenzae through the replacement of the inhibitoryagent bacitracin with powdered beans of cacao to seewhether or not the modified chocolate agar plate iscapable of producing results equal to the standard oreven greater in terms of suppressing the growth ofother contaminant bacteria thus promoting growth ofpurer culture of H. influenzae.
Reviews of Related Literature
Genus Theobroma Linnaeus, Local name: Cacao.Cacao is widely scattered in cultivation at low andmedium altitudes but is nowhere spontaneous in thePhilippines. It was introduced from Mexico. This is asmall tree growing from 3 to 5 meters in height. Theleaves are oblong-obovate to oblong, and 15-40centimeters in length with pointed tip and roundedbase. The flowers are solitary or fascicled on the trunkand branches, yellowish or nearly white and about 1centimeter in diameter. The fruit is oblong, 10-15centimeters long, prominently wrinkled, yellow orpurplish. The seeds are numerous and embedded inwhitish pulp. According to Wehmer, the leaves containan alkaloid, theobromine. Caffeine, etc. the wall andpulp of the fruit contain arabinose and galactose; thepulpy flesh; the enzymes: protease invertase, raffinase,
cesease and oxidase. The mesocarp and seeds containtheobromine and caffeine.1
According to Medical Microbiology 4th Ed. byMusher, bacteria of the genus Haemophilus are small,non-motile gram negative bacilli and coccobacilli, andare fastidious by nature. The genus Haemophilusrequires factors, characteristically, for growth suchas, Heme (X factor) and Nicotine Adenine dinucleotide(NAD or V factor). These growth requirements areused in the clinical setting to identify suspect organismsto the species level. Haemophilus sp. grows best ata temperature between 35ºC and 37ºC, at a slightlyalkaline pH of 7.6. Laboratory growth ofH. influenzae is typically achieved in 5% CO2atmospheric conditions on chocolate blood agar, whichprovides the previously mentioned X and V factors.2
The composition of chocolate agar and the bloodagar is the same and the only difference is thepreparation of Chocolate agar, the red blood cellsare lysed. As stated on Manual of ClinicalMicrobiology. 9th ed. by Murray (2007). The lysis ofRBC during the heating process releases intracellularcoenzyme Nicotinamide Adenine Dinucleotide (NADor V Factor) into the agar for utilization by fastidiousbacteria (the heating process also inactivates growthinhibitors). Hemin (factor X) is available from non-hemolyzed as well as hemolyzed blood cells. Themost common species that require this enrichedmedium for growth include: Neisseria gonorrhoeae,Neisseria meningit idis and Haemophilus sp.Neither of these species is able to grow on SheepBlood Agar.3
After conducting considerable investigations byWollgastet. Al (2004) found that cocoa polyphenolsare anthocyanins, catechins, procyanidins, and somephenolic acids have been identified in the unfermentedviolet seedlings of the fruit of Theobroma cacaoLinnaeus. It is as well stated that flavan-3-olsepicatechin, cathechin, and oligomeric and polymericprocyanidins are the main component of cocoapolyphenols.4
According to the article made by the U.S.Chocolate Manufacturers Association, Researcheshave been focusing on the chemical composition ofcocoa, as indicated in the article that there arepolyphenols which include flavanols such as catechin,epicatechin, and pro-cyanidins, as they are the sourceof antioxidants. Also of note are the tannins presentin cocoa, which can also be antioxidants and can assistwith both heart and digestive health.5 Tannins whichare present in cocoa showed an antibacterial activity

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 39
in a study conducted by Scalbert, et al. (1991) in thefollowing mechanisms including the deprivation of theneeded substrate for microbial growth, the inhibitionof extracellular enzymes, and iron deprivation as well.6
Cocoa mass extract is intended to provide acomposition against periodontal bacteria as stated ina study conducted by Morinaga, et al. (2005), whichhas a high safety property without showing any sideeffects and exhibits an excellent effect of killingperiodontal bacteria without affecting the growth ofnon-pathogenic indigenous microorganisms in the oralcavity, and foods, drinks and mouth washers againstperiodontal bacteria. The active ingredient againstperiodontal bacteria found on the Cocoa mass extractis found to be polyphenols originating in the cocoafraction or free fatty acids. It is preferable that theabove-described free fatty acids contain at least onemember selected from palmitic acid, stearic acid, oleicacid and linoleic acid to show its antibacterial activity.7
The study conducted by Nsor-Atindanaet. Al(2012) entitled as "Quantification of Total PolyphenolicContent and Antimicrobial Activity of Cocoa(Theobroma cacao L.) Bean Shells" evaluated thetotal Phenolic Compound Content (PC) and biologicalactivity of Cocoa Bean Shell (CBS). Proximatecompositions of the dry matter (CBS) wereinvestigated, while the antimicrobial activity was ofCBS phenolic extracts in 80% acetone, ethanol,methanol and water performed by paper disk diffusionand micro broth dilution methods against 4 bacterialstrains (Stapylococcus aureus, Escherichia coli,Salmonella, Bacillus cereus). It showed that CBSconsisted of mainly dietary fiber (60%), followed byprotein (16.93%), fat (6.87%), polyphenols (4.85%)and moisture (3.73%). The extracts inhibition zonesdiameter against the tested strains ranged from 16.1to 9.19 (mm) and were all significantly higher (p<0.05)than the negative control. The minimum inhibitoryconcentration ranged from 0.78 TPmg/mL to2.58TPmg /mL.
In a study by Singh, et al. (2015) conducted toidentify the antibacterial property of the Theobromacacao plant. The cocoa leaf, seeds and pod werestudied for the estimation of medicinal properties thatthey contain and the focus was screening foranticancer ability. The antimicrobial assay by agar welldiffusion method of cocoa seeds showed zone ofinhibition against pathogens Serrati amarcescens,Staphylococcus aureus, Salmonella sp. andShigelladysenteriae. Furthermore, antioxidant assaywas performed using DPPH radical scavenging assay.
The samples were then tested for cytotoxicity assayagainst MG63 osteosarcoma cell lines and activecompounds were identified by doing Gaschromatography and Mass spectroscopy (GCMS). Thestudy showed that the extracts contain certaincompounds which can be the reason of the biologicalactivities present in the extracts. Meaning, there is agreat chance for them to be used as antimicrobial drugwith further purification and proper processing.9
According to Adika C. (2013) in a study conductedat the University of Ghana, This study tested the anti-plasmodial activities of crude methanol extract ofnatural cocoa powder. The anti-plasmodial activity ofthe crude methanol natural cocoa extract could bemainly due to its ability to enhance erythrocytemembrane integrity and protect from parasite invasion.Erythrocyte membrane integrity enhancementinhibited sorbitol-induced haemolysis of infectederythrocytes. The direct effects of the bioactiveingredients of extract on the intracellular parasite couldhave contributed the inhibition of sorbitol-inducedhaemolysis of infected erythrocytes. The effect ofcocoa extract on RBC membrane is said to beprotective.10
MATERIALS AND METHODS
Research Design
The approach used by the researchers was thruexperimental designs. The method is a direct controlof the things being studied and/or manipulated. It wasdone in the laboratory for the purpose of the study.
The experimental subjects were divided into twomajor groups: the experimental group and the positivecontrol group. The experimental group was composedof the cacao ground and mixed with the media. (Figure1)
Sample Preparation
The cacao fruit was harvested from 7 year oldtrees on the month of October in Barangay Kabulusan,Pakil, Laguna. The sample was harvested from thetree located at the backyard of the residents' houseon October 1, 2016 and was brought to Fairview,Quezon City. The cacao fruit was opened to get thebeans, which were washed and air dried for four days.The dried beans were ground into powder form, andwere set for ethanolic extraction.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201740
Figure 1. Research design
Ethanolic Extraction
The powdered bean sample was mixed with aconcentration of 95% ethanol with 1:2 ratio for threedays with stirring of a clean spatula 3 times a day, andwas filtered 3 times. Now the sample was ready forcrude extraction.
Crude Extraction
The ethanolic extract of cocoa bean was subjectedto rotary evaporation at 40ºC with a reduced pressureand spun at a speed of 100 rpm. Then, the crudesample was stored at 1-6ºC before it was used.
Cacao Chocolate Agar Medium Preparation
For the 3% Cacao Chocolate Agar Plate (CCAP)that was prepared, the weight of agar needed wasmeasured to produce a 500 ml solution. The agar wasadded to the flask containing 230 ml of distilled water,while mixing, another 230 ml of distilled water wasadded. The sample was mixed until i t washomogenous. The solution was autoclaved for 15
minutes at 121ºC with 15 psi. The solution afterautoclave was allowed to cool for 15 minutes, then 25ml of horse blood was added. After the addition ofhorse blood, the media was reheated at 56ºC until themedia turned brown, which indicates the lysis of thehorse blood. It was allowed to cool for another 5minutes before the 15 ml of cocoa extract was added.Then the media was placed on the plate and allowedto solidify, it was then placed in the refrigerator of thelaboratory before use.
For the 5% Cacao Chocolate Agar Plate (CCAP)that was prepared, the weight of agar needed wasmeasured to produce a 500 ml solution. The agar wasadded to the flask containing 225 ml of distilled water,while mixing, another 225 ml of distilled water wasadded. The sample was mixed until i t washomogenous. The solution was autoclaved for 15minutes at 121ºC with 15 psi. The solution afterautoclave was allowed to cool for 15 minutes, then25ml of horse blood was added. After the addition ofhorse blood, the media was reheated at 56ºC until themedia turned brown, which indicates the lysis of thehorse blood. It was allowed to cool for another 5minutes before the 25 ml of cocoa extract was added.Then the media was placed on the plate and allowedto solidify, it was then placed in the refrigerator of thelaboratory before use.
For the 10% Cacao Chocolate Agar Plate (CCAP)that was prepared, the weight of agar needed wasmeasured to produce a 500 ml solution. The agar wasadded to the flask containing 215 ml of distilled water,while mixing, another 210 ml of distilled water wasadded. The sample was mixed until i t washomogenous. The solution was autoclaved for 15minutes at 121ºC with 15 psi. The solution afterautoclave was allowed to cool for 15 minutes, then 25ml of horse blood was added. After the addition ofhorse blood, the media was reheated at 56ºC until themedia turned brown, which indicates the lysis of thehorse blood. It was allowed to cool for another 5minutes before the 50 ml of cocoa extract was added.Then the media was placed on the plate and allowedto solidify, it was then placed in the refrigerator of thelaboratory before use.
Bacitracin Chocolate Agar Medium Preparation
For the Bacitracin Chocolate Agar Plate (BCAP)that was prepared, the weight of agar needed wasmeasured to produce a 500 ml solution. The agar wasadded to the flask containing 240 ml of distilled water,

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 41
while mixing, another 235 ml of distilled water wasadded. The sample was mixed until i t washomogenous. The solution was autoclaved for 15minutes at 121ºC with 15 psi. The solution afterautoclave was allowed to cool for 15 minutes, then25ml of horse blood was added. After the addition ofhorse blood, the media was reheated at 56ºC until themedia turned brown, which indicates the lysis of thehorse blood. It was allowed to cool for another 5minutes before the addition of 363.63mg of bacitracin.Then the media was placed on the plate.
Inoculation of Bacterial Strains
To test for its selectivity and its ability to culturethe desired bacteria, the inoculum should contain thepure culture of the desired bacteria (H. influenzae)together with the pure culture of undesired organismsthat grows on normal Chocolate Agar Plate such asEscherichia coli and Pseudomonas aeruginosa.Streptococcus pneumoniae represents the grampositive organisms.
Sample size
The researchers used a non-probability purposivesampling where they used the colonies within theprimary/mother plate at the 4th streak which has themost isolated colonies and chose the colonies whichbest describes each organism in theory.
Data Analysis and Technique
Data Analysis Technique
In order to determine the quantitative differencesbetween the two groups (experimental and control),t-test will be used. Three trials were made perconcentration and there was a control group made.
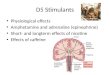
The growth and colony count of Escherichia coliin different concentrations of CCAP. With Escherichiacoli as to 3% of the concentration of CCAP, the growthof the three trials have shown moderately heavy growthand all showing gram negative bacilli and as to its colonycount with the result of 151, 167, and 170 respectivelyand with the average of 163 colonies. With Escherichiacoli as to 5% of the concentration of the CCAP, thegrowth of the three trials have shown moderately heavygrowth on the first plate and a moderate growth on thesecond and third trials and all showing gram negativebacilli and as to its colony count with the result of 143,
157, and 117 respectively and with the average of 139colonies. With Escherichia coli as to 10% of theconcentration of the CCAP, the growth of the threetrials have shown light growth and all showing gramnegative bacilli and as to its colony count with the resultof 14, 8, and 11 respectively and with the average of 11colonies.
With Escherichia coli as to BCAP, the growth ofthe three trials have shown light growth and allshowing gram negative bacilli and as to its colony countwith the result of 6 on all plate and with the averageof 6 colonies. (Table 1)
Figure 1. Escherichia coli on 3%, 5%, and 10% cacao extractchocolate agar plate respectively
Table 1. Growth and colony count of Escherichia coli on3%, 5% and 10% Cacao Chocolate Agar Plate and
Bacitracin Chocolate Agar Plate
Table 2. Growth and colony count of Pseudomonasaeruginosa on 3%, 5% and 10% Cacao Chocolate
Agar Plate and Bacitracin Chocolate Agar Plate

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201742
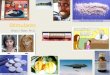
Figure 2. Pseudomonas aeruginosa on 3%, 5%, and 10% cacaoextract chocolate agar plate respectively
The growth and colony count of Pseudomonasaeruginosa in different concentrations of CCAP.With Pseudomonas aeruginosa, as to 3% of theconcentration of CCAP, the growth of the three trialshave shown moderately heavy growths on two platesand a light growth in one plate, and all showing gramnegative bacilli and as to its colony count with theresult of 126, 67, and 114 respectively and with theaverage of 102 colonies. With Pseudomonasaeruginosa as to 5% of the concentration of CCAPthe growth of the three trials have shown moderatelyheavy growths on two plates and a light growth in oneplate, and all showing gram negative bacilli and as toits colony count with the result of 125, 125, and 95respectively and with the average of 115 colonies. WithPseudomonas aeruginosa as to 10% of theconcentration of CCAP the growth of the three trialshave shown a light growth in all plates, and all showinggram negative bacilli and as to its colony count withthe result of 5, 7, and 8 respectively and with theaverage of 7 colonies.
With Pseudomonas aeruginosa as to BCAP, Thegrowth of the three trials have shown light growthand all showing gram negative bacilli and as to itscolony count with the result of 3, 2, 3 respectively andwith the average of 3 colonies.(Table 2)
Table 3. Growth and colony count of Streptococcuspneumoniae on 3%, 5% and 10% Cacao Chocolate
Agar Plate and Bacitracin Chocolate Agar Plate
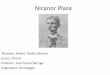
Figure 3. Streptococcus pneumoniaeon 3%, 5%, and 10% cacaoextract chocolate agar plate respectively
The growth and colony count of Streptococcuspneumoniae in different concentrations of CCAP.
With Streptococcus pneumoniae as to 3% of theconcentration of CCAP the growth of the three trialshave shown moderately heavy growths on two platesand a moderate growth in one plate, and all showinggram positive cocci and as to its colony count withthe result of 146, 98, and 135 respectively and withthe average of 126 colonies. With Streptococcuspneumonia as to 5% of the concentration of CCAPthe growth of the three trials have shown moderatelyheavy growths on one plate and a light growth in twoplates, and all showing gram positive cocci and as toits colony count with the result of 61, 115, and 64respectively and with the average of 80 colonies. WithStreptococcus pneumoniae as to 10% of theconcentration of CCAP the growth of the three trialshave shown light growths on all plates, and all showinggram positive cocci and as to its colony count withthe result of 7, 6, and 9 respectively and with theaverage of 7 colonies.
With Streptococcus pneumoniae as to BCAP,The growth of the three trials have shown light growthand all showing gram positive cocci and as to its colonycount with the result of 4 numbers of colony. (Table3)
Table 4. Growth and colony count of Haemophilusinfluenzaeon 3%, 5% and 10% Cacao Chocolate Agar Plate and
Bacitracin Chocolate Agar Plate

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 43
Figure 4. Haemophilus influenzaeon 3%, 5%, and 10% cacaoextract chocolate agar plate respectively
The growth and colony count of Haemophilusinfluenza in different concentrations of CCAP. WithHaemophilus influenzae as to 3% of theconcentration of CCAP the growth of the three trialshave shown moderately heavy growths on one plateand a moderate growth in one plate, and all showinggram negative bacilli and as to its colony count with
the result of 67, 91, and 52 respectively and with theaverage of 70 colonies. With Haemophilus influenzaeas to 5% of the concentration of CCAP, the growthof the three trials have shown moderately heavygrowths on two plates and a light growth in one plate,and all showing gram negative bacilli and as to itscolony count with the result of 115, 54, and 68respectively and with the average of 79 colonies. WithHaemophilus influenzae as to 10% of theconcentration of CCAP the growth of the three trialshave shown a light growth in all plates, and all showinggram negative bacilli and as to its colony count withthe result of 16, 25, and 18 respectively and with theaverage of 20 colonies. With Haemophilus influenzaeas to BCAP, the growth of the three trials have shownmoderate growth and all showing gram negative bacilliand as to its colony count with the result of 55, 84, 69respectively and with the average of 69 colonies.(Table 4)
Table 5. Summary of Statistical Result

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201744
Data Interpretation
Considering the characteristics of the organismas to gram staining, there are no difference ascompared to the theoretical and the control made inthis research. Having almost all of the result acceptingthe alternative hypothesis that there is a significantdifference between the standard media and themodified media, only the Haemophilus influenzae in10% cocoa chocolate agar plate has a negative valueIn which it means that the growth of the Haemophilusis lesser than the standard. From the given results onlyHaemophilus influenzae in 3% cocoa chocolate agarplate showed no significant difference to the standardmedia. (Table 5)
CONCLUSION AND RECOMMENDATIONS
Conclusion
The researchers concluded that the modifiedchocolate agar plate (CAP) with seed extract fromcacao tree with the concentration of 3% and 5% havenot showed selectivity to Haemophilus influenzaewhile 10% of cacao modified chocolate agar plateshowed its selectivity as well but was able to showhow increasing concentration of cocoa extract affectsthe growth of the selected organism. The modificationwith 3% and 5% cacao seed extract was not effectivein inhibiting undesired organisms like Escherichia coli,and Pseudomonas aeruginosa, but with 10% cacaoseed extract, it showed its effectiveness in inhibitingundesired organisms, which can be found in Bacitracinchocolate agar plate. There was reduced growth ofthe undesired organisms mentioned in the medium withits different concentration. Therefore, the modifiedchocolate agar plate medium with 10% cacao seedextract has a significant difference compared tobacitracin chocolate agar plate. Furthermore, theincreasing concentration of the cacao extract modifiedmedium showed its significant difference comparedto one another, giving rise to new information with itsantibacterial ability.1. To add other undesired organism that still grows
on BCA like Neisseria sp., Klebsiellasp. andProteus sp.
2. To perform PCR for confirmation of bacteriapresent on the medium
3. To perform test with an increase in the number ofduplicates for both experimental and control
4. To perform experiment with higher concentrationand lesser increment of cacao extract
5. To be performed by a professional in the field ofmicrobiology
6. To be tested with other strain of ATCC7. To know the exact constituents from the produced
extracts
Recommendation
In the experiment conducted, the researcherswere able to culture H. influenzae in their medium.The modified medium that the researchers made wasable to reduce the growth of the common undesiredorganisms of the standard medium.
The authors recommend that future researcherson the following be made to improve this study:
REFERENCES
1. Quisumbing E. Medicinal plants of the Philippines. 1st ed.Ann Arbor, Michigan: University Microfilms International;1979.
2. Musher D. Haemophilus Species [Internet]. Ncbi.nlm.nih.gov. 1996 [cited 11 January 2017]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK8458/
3. Murray P. Manual of clinical microbiology. 9th ed.Washington, D.C: ASM Press; 2007.
4. Wollgast J. The contents and effects of polyphenols inchocolate [Internet]. 1st ed. Germany: Insti tute ofNutritional Sciences; 2004 [cited 4 January 2017]. Availablefrom: http://geb.uni-giessen.de/geb/volltexte/2005/2239/pdf/WollgastJan-2005-06-10.pdf
5. Medicinal Benefits of Theobroma cacao: ContemporaryStudies of Chocolate as a Health Food and the HistoricalUse of Cacao in Healing [Internet]. Chocolate Class -Multimedia Essays on Chocolate, Culture and the Politicsof Food. 2016 [cited 14 January 2017]. Available from:https://chocolateclass.wordpress.com/2016/05/10/medicinal-benefits-of-theobroma-cacao-contemporary-studies-of-chocolate-as-a-health-food-and-the-historical-use-of-cacao-in-healing/
6. Scalbert A. Antimicrobial properties of tannin [Internet].1st ed. Great Britain: Pergamon Press; 1991 [cited 13 January2017]. Available from: https://www.researchgate.net/publication/223084771_Antimicrobial_ properties_of_tannin
7. Morinaga & Co., Ltd. Use of antibacterial componentextracted from cacao mass for inhibiting the growth ofperiodontal bacteria. Japanese; US 20050152852 A1, 2005.
8. Nsor-Atindana J, Zhong F, Mothibe K, Bangoura M, LagnikaC. Quantification of total polyphenolic content andantimicrobial activity of cocoa (Theobromacacao L.) BeanShells [Internet]. 1st ed. Jiangsu, China: State KeyLaboratory of Food Science and Technology; 2012 [cited 19January 2017]. Available from: http://www.worldcocoafoundation.org/wp-content/uploads/files_mf/nsoratindana2012.pdf

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 45
9. Singh N, Datta S, Dey A, Chowdhury A, Abraham J.Antimicrobial activity and cytotoxicity of Theobroma cacaoextracts [Internet]. 1st ed. Tamil Nadu, India: Der PharmaciaLettre; 2015 [cited 17 January 2017]. Available from: http://www.scholarsresearchlibrary.com/articles/antimicrobial-activity-and-cytotoxicity-of-theobroma-cacao-extracts.pdf
10. Adika C. In vitro effects of natural cocoa extract onerythrocyte membrane and asexual erythrocytic stage ofplasmodium falciparum [Internet]. 1st ed. Ghana: Universityof Ghana; 2013 [cited 5 January 2017]. Available from: http://ugspace .ug .edu .gh /b i t s t r eam/123456789/5250/1 /CHRISTOPHE RADIKA_InVitro Effects of Natural CocoaExtracton Erythrocyte Membraneand Asexual ErythrocyticStage of Plasmodium Falciparum_2013.pdf
11. Alean J, Chejne F, Rojano B. Degradation of polyphenolsduring the cocoa drying process. Journal of Food Engineering[Internet]. 2016 [cited 7 January 2017];189:99-105.Available from: http://www.sciencedirect.com/science/article/pii/S0260877416302059
12. Albertini B, Schoubben A, Guarnaccia D, Pinelli F, DellaVecchia M, Ricci M, et al. Effect of fermentation and dryingon cocoa polyphenols. J Agric Food Chem [Internet]. 2015[cited 14 January 2017];63(45):9948-53. Available from:http://pubs.acs.org/doi/abs/10.1021/acs.jafc.5b01062?journal Code =jafcau&
13. Saldaña M, Zetzl C, Mohamed R, Brunner G. Extraction ofmethylxanthines from guaraná seeds, maté leaves, and cocoabeans using supercritical carbon dioxide and ethanol. J AgricFood Chem [Internet] . 2002 [cited 14 January2017];50(17):4820-26. Available from: http://pubs.acs.org/doi/abs/10.1021/jf020128v
14. Mars, Incorporated. An improved method for extractingcocoa procyanidins. US; WO 2001093690 A2, 2001.
15. Perry W, Lightbown J, Mussett M, Humphrey J. TheInternational Standard for Bacitracin [Internet]. PubMedCentral (PMC). 1953 [cited 12 January 2017]. Availablefrom: https:/ /www.ncbi.nlm.nih.gov/pmc/articles/PMC2542050/

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201746
Cesarean Scar Pregnancy:"A Rarity No More?" A Report of 2 Cases*
Denise Elaine A. Reyes, MD
Cesarean scar pregnancy is the rarest form of ectopic pregnancy. In the Philippines, little is known aboutits incidence and occurrence. However, increasing rates worldwide is now being documented and isclosely being associated with the increasing cesarean section rates. This paper reports two cases ofcesarean scar pregnancy who both presented with vaginal bleeding. The first case is a Gravida 6 Para 5(5005), while the second case is a Gravida 3 Para 2 (2002), who were diagnosed early by ultrasonographybut managed differently. The first case was managed by hysterectomy, on the other hand, the second casewas managed conservatively by laparoscopic excision of the cesarean scar pregnancy. Close follow upwith serial beta-hCG monitoring was done for the second case until normalization of its level. This paperintends to raise awareness of the increasing incidence of cesarean scar pregnancy, its pathophysiology,different options in the diagnosis and management, Recommendations were made to decrease the incidenceof cesarean section, thereby, lowering the occurrence of cesarean scar pregnancy.The incidence of cesarean scar pregnancy has increased due to early and accurate diagnosis byultrasonography. Several factors would tend to affect its management, identifying these factors wouldtailor fit the management according to the needs of the patient.
Key words: Ectopic pregnancy, cesarean scar pregnancy (CSP), cesarean section
Ectopic pregnancies comprise 1 to 2% of allpregnancies and cesarean scar pregnancy is the rarestform. It accounts for 6.1% of all ectopic pregnancieswith a history of at least one previous cesarean sectionscar and an incidence rate of approximately 1:1800 to1:2216.1 Due to its rarity, there are still no evidence-based standards of practice creating a dilemma forits diagnosis and management. With delayed detection,it may lead to massive hemorrhage, uterine ruptureand other life threatening complications. But over thepast 5 years, there has been a substantial increase inthe number of cesarean section scar pregnancy
ABSTRACT
* From the Department of Obstetrics and Gynecology
published in the English literature. This may reflect areal increase in its incidence because of the risingcesarean section rates worldwide, wherein 72% ofcesarean scar pregnancy can occur in women whohave had two or more cesarean sections. Moreover,increasing use of transvaginal ultrasound yieldsincreased diagnosis of its entity; and another reasonmight be contributed by changes in operativetechniques on uterine surgeries.2 In the Philippines,little is known about its incidence and natural history.Philippines Obstetrics and Gynecology Society(POGS) statistics shows there are about 9,365 casesof ectopic pregnancies reported in 5 years (2010-2016), however, no report of cesarean scar pregnancywas ever recorded. This paper intended to promoteawareness on the increasing incidence of cesarean

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 47
scar pregnancy locally and worldwide, i tspathophysiology, as well as with the diagnosis andmanagement options. It is worthwhile to stir awarenessand develop schemes to identify such cases, ascomplications arising from this condition may bringabout life threatening outcomes.
This report aimed to discuss 2 cases of cesareanscar pregnancy diagnosed early by ultrasound imagingand managed differently.
THE CASE
The first case is a 37 years old, Gravida 6 Para 5(5-0-0-5), 7 6/7 weeks age of gestation, married,admitted due to vaginal bleeding. Last menstrual periodwas on November 15, 2016 and previous menstrualperiod on October 15, 2016.
She experienced the usual signs and symptoms ofpregnancy such as cessation of menses, easyfatigability, nausea and vomiting on the first month ofmissed period (December 2016). On the same month,self-pregnancy test was done revealing a positiveresult. No consult, laboratory tests nor intake ofprenatal vitamins was done.
Two days prior to admission, patient experiencedprofuse vaginal bleeding with no associated passageof meaty material. She also experienced crampyhypogastric pain, vomiting, body malaise and dizziness.No medications were taken and nor consult was done.
Few hours prior to admission, still with the abovesymptoms, she experienced chills and frontotemporal
Figure 1. Transabdominal ultrasound initially done showing the gestational sac anterior to the uterine cavity.Cervix also noted to be empty.
headache. Patient self-medicated with Amoxicillin 500mg per orem and Mefenamic acid 500 mg, single dose,which did not offer relief.
The persistence of the symptoms prompted consultat this institution where transvaginal ultrasound wasdone (Figures 1 & 2) which revealed a live fetus withgood cardiac and somatic activities, compatible to 9weeks and 1 day age of gestation by crown rumplength. However, it was located at the previouscesarean section scar within the anterior isthmicportion with no subchorionic hemorrhage. The residualanterior myometrium measured 0.88 cm. with absenceof healthy myometrial wall between the bladder andgestational sac. Color flow mapping showed abundantperipheral color and circular blood flow surroundingthe sac. Unremarkable bilateral ovaries with corpusluteum on the left. She was then diagnosed withEctopic Pregnancy, T/C Cesarean Scar Pregnancy at9 weeks and 1 day and was admitted.
Past medical history and family history were non-contributory to the present condition.
Menarche at fourteen years old. Subsequentmenses were regular, seven day duration, moderatein flow, not associated with dysmenorrhea.
She had her coitarche at 17 years old with onesexual partner. Her partner had four previous sexualpartners and is currently in a monogamous relationship.
The patient is a Gravida 6 Para 5 (5-0-0-5).The first and second pregnancies were delivered
by normal spontaneous delivery to term babies withbirthweights of approximately 2,500 to 2,600 grams.Third pregnancy was delivered by Low Segment

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201748
Figure 2. CRL measured 24.16 mm, equivalent to 9 weeks and 1 day with good cardiac and somatic activities
Cesarean Section due to fetopelvic disproportion at ahospital with a birthweight of 2,700 grams. Her fourthand fifth pregnancies were then delivered by repeatLow Segment Cesarean Sections, with no fetomaternalcomplications.
Patient used depot medroxyprogesterone acetate(DMPA) from 2005-2009 as a method ofcontraception.
Pertinent Physical Examination
Patient is conscious, coherent, not incardiorespiratory distress with stable vital signs.Abdomen with previous midline scar, flat, soft, nomass, non tender. On speculum examination, cervix isclean looking with minimal bleeding per os. Internalexamination revealed a closed cervix, no cervicalmotion tenderness, uterus slightly enlarged, noabdominal mass palpated, non-tender, no adnexal massnor tenderness. Admitting diagnosis was G6P5(5-0-0-5), Cesarean Section Scar pregnancy, 9 weeks,Unruptured, Previous Cesarean Section III (1x forFetopelvic disproportion). She was scheduled for TotalAbdominal Hysterectomy.
Complete blood count and urinalysis revealed mildanemia and urinary tract infection. Two units of packedred blood cell were transfused prior to operation andanother two units were secured for possibleintraoperative transfusion. Prophylactic antibiotic wasgiven 1 hour prior to operation. Possible involvementof the urinary bladder prompted referral to aUrogynecologist for co-management.
Intraoperatively, there was no hemoperitoneum,the uterus was slightly enlarged which measured 7.5cm
x 6.5cm x 5cm with numerous varicosities at theisthmic portion. A bulging mass which measured 5.0cmx 4.0cm at the previous cesarean section scar wasnoted and was adherent to the bladder. After ligationof the round ligaments, uteroovarian ligaments, anduterotubal attachments, the vesicouterine peritoneumwas dissected downwards to separate the bladder fromthe uterine wall. The products of conception wereexpelled at its implantation site with a note of thinmyometrial tissues with a thickness of 1 mm (Figure3). Completion of the hysterectomy procedures withbilateral fimbriectomy were performed afterwards.Methylene blue instillation was done to determine ifthe bladder was injured during dissection. A small rentwas seen thus cystorrhaphy was performed. Estimatedblood loss was 1,100 cc. She was transfused with 2more units of packed red blood cell. Patient toleratedthe procedure well and was discharged on the ninthhospital day with indwelling Foley catheter.
Grossly the uterus measured 10.0cm x 4.5cm x2.5cm. On cut section, the endometrium measured1.2cm to 1.3cm thick while the myometrium measured1.7cm to 2.4cm thick. There are irregularly shapedbrown-black tissues on the left isthmic area, whichmeasured 4.3cm x 2cm x 1.9cm and 4.0cm x 2.3cm x2.0cm. The larger tissue seen was occupying almost80% of the isthmus. Histopathologic examination ofthe specimen confirmed a cesarean scar pregnancy.
Patient followed up one week after discharge withcomplaints of urinary leakage. Voiding cystogramconfirmed the presence of vesicovaginal fistula.Urinary catheter was retained for another month.Removal of IFC was done per patient's request afterone month and she has been asymptomatic since then.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 49
Figure 3. Conceptus noted to be implanted anterior to themyometrium, with a thin membrane separating from the urinarybladder
The second case is a 33 years old, Gravida 3 Para2 (2-0-0-2), 7 5/7 weeks age of gestation, married,admitted due to vaginal spotting. Last menstrual periodwas on May 1, 2016 with a previous menstrual periodon April 2017.
Three weeks prior to admission, patientexperienced vaginal spotting accompanied by nauseaand vomiting but with no associated hypogastric pain.No medications taken, no consult was done.
Two weeks prior to admission, self-pregnancy testdone which revealed a positive result. Still, no consult,laboratory tests nor intake of prenatal vitamins wasdone.
Few hours prior to admission, still with vaginalspotting, she experienced low back pain. Patientconsulted at a secondary hospital where completeblood count and urinalysis were done which showednormal results. Transvaginal ultrasound revealedpregnancy uterine 8 weeks by crown-rump length,however, the gestational sac containing a yolk sac withan embryo with good cardiac activity was noted atthe lower uterine segment. Color mapping showedblood flow from the anterior low segment, suspicious
of a cesarean scar pregnancy. Ectopic pregnancyprobably at the cesarean section scar was thenconsidered, hence, she was transferred at ourinstitution.
Past medical history, family history andgynecologic history were non-contributory to thepresent condition.
She had her coitarche at 28 years old with fourprevious sexual partners. Sexual history of her husbandwas unknown to the patient.
The patient is a Gravida 3 Para 2 (2-0-0-2). Herfirst pregnancy was delivered by low segmentcesarean section due to cephalopelvic disproportionto a term living boy weighing 2,800 grams with nofeto maternal complications. Second pregnancy wasdelivered by repeat low segment cesarean section last2015.
Pertinent physical examination showed a patientwho is conscious, coherent, ambulatory with normalvital signs. Abdomen is flat, with previous transversesuprapubic scar, soft, no palpable mass, nortenderness. Speculum examination revealed a cleanlooking cervix with minimal discharge. On internalexamination, cervix is firm and closed, with no cervicalmotion tenderness, uterus slightly enlarged, non tender,no adnexal mass nor tenderness. Repeat transvaginalultrasound was done which revealed single, livepregnancy at 8 weeks and 3 days by crown rumplength with good cardiac activity described as anirregularly shaped gestational sac with embryo andyolk sac measuring 6.0cm x 5.78cm x 7.82cmseemingly implanted at the anterior lower uterinesegment, probably in the previous cesarean scar. Theanterior myometrial wall thickness measures 0.24cm.A subchorionic hemorrhage was noted beneath theanterior myometrial wall (Figures 4, 5, & 6). Admittingdiagnosis was Gravida 3 Para 2 (2-0-0-2), EctopicPregnancy, 7 weeks and 5 days, T/C Cesarean Scarpregnancy, unruptured, Previous Low SegmentCesarean Section II (1x- Cephalopelvic Disproportion).She was then referred to a ReproductiveEndocrinology and Infertility specialist for diagnosticlaparoscopy with possible exploratory laparotomy withwedge resection or excision of the conceptus or totalabdominal hysterectomy.
Complete blood count and urinalysis revealednormal results. Serum beta-hCG was elevated at 198,289.18 mIU/ml. One unit of packed red blood cellwas secured for possible intraoperative use. Pre-operative antibiotic was given 1 hour prior to theoperation.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201750
Figure 4. Endocervical canal is empty. Gestational sac with anembryo and a yolk sac is seemingly located within the cesareanscar anterior to the uterus.
Figure 5. Gestational sac approximately measuring 6.0cm x 5.78cm x 7.82cm exhibiting circumferential flow on initial colormapping.
Figure 6. CRL: 1.77 cm and yolk sac of 0.313 cm. With good cardiac activity at 174 bpm
Diagnostic laparoscopy was done.Intraoperatively, there was no hemoperitoneum. Theliver, spleen and subdiaphragmatic areas were smoothand grossly normal. The uterus was enlarged to 12weeks' size with a 3.0cm x 2.0cm x 6.0cm highlyvascularized mass protruding at the serosal surfaceof the lower uterine segment. The uterovesicalperitoneum was opened by blunt and sharp dissectionseparating it from the anterior uterine surface usingmonopolar scissors, the product of conception wereexpelled. Evacuation was done. The edges of themyometrium were sutured. Hemostasis was achievedand the specimen was secured for histopathexamination. Estimated blood loss was 1,400 cc.Repeat hemoglobin revealed severe anemia with a

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 51
Figure 7. Cystic mass at the lower uterine corpus with increased vascular flow
hemoglobin count of 63 g/L thus three units of packedred blood cell were transfused. Repeat CBC afterblood transfusion showed improved hemoglobin count.Patient was then discharged improved on herpostoperative day 3. Histopathologic results confirmedcesarean scar pregnancy.
Patient consulted one week postoperative withcomplaints of minimal vaginal bleeding. Speculumexamination revealed clean looking cervix with minimalbleeding per os, internal examination revealed a closedcervix, uterus slightly enlarged, non-tender, no adnexalmass nor tenderness. Repeat transvaginal ultrasoundwas done which showed an irregular structurecontaining irregular cystic areas and strong vascularflow seemingly encroaching the endometrium withinthe lower uterine segment with the impression of agestational trophoblastic disease versus arteriovenousmalformation (Figure 7). Observation with frequentfollow up was done with weekly B-HCG monitoringwhich revealed decreasing values until normalizationand resolution of the vaginal bleeding.
Repeat transvaginal ultrasound was done after onemonth and was unremarkable.
DISCUSSION
Ectopic pregnancy comprises 1% to 2% of allpregnancies and is currently the leading cause ofpregnancy-related deaths during the first trimester,accounting for 10% of all maternal deaths.3
Among all types of ectopic pregnancy, cesareanscar pregnancy (CSP) is the rarest form accounting
for 6.1% of all ectopic pregnancies in women whohad at least one cesarean delivery and a rate of 0.15%in women with a previous cesarean section regardlessof the number of cesarean sections done. Recently,there is an increasing trend of CSP.
In a 2002 study, Fylstra, et al. noted only 19 casesof cesarean scar pregnancy have been reported inthe English medical literature since 1966.
However, two years later, on a 2004 study, theysearched for case reports done after 2002, and found66 new case reports in a span of two years. Then arecent 2012 survey of the literature found 751 casereports. From these statistics, the incidence appearsto be on the rise.19
In another study, from 1978 to 2001, only 19cases of CSP have been reported, 155 cases werereported in 2006 and in 2011, it rapidly increased to751. Jurkovic et al in 2003 estimated a prevalenceof 1:1800 in their local population of women attendingthe early pregnancy assessment unit5, while a recentcase series estimates an incidence of 1:2260 of allpregnancies.18
What could have caused the increasing incidenceof cesarean scar pregnancy?
The strongest association of CSP is attributed tothe increasing incidence of cesarean section ratesworldwide. Over the last few decades, cesareansection (CS) rates have continued to rise. In the UK,the CS rate increased from 12 to 29% between theyear 1990 and 2008 as documented by Betran, et al.(2007). In the USA, in the year 2011, one in threewomen delivered by cesarean section, whereas inChina the CS rates have risen from 2% in 1985 to 36-

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201752
58% in 2010 and in Brazil from 15% in 1970 to even80% in the private sector in 2004.8 Overall, thesestatistics has a common denominator of an increasingtrend of cesarean section.
Without question, cesarean section is truly a life-saving procedure for women with placenta previa orobstructed labor and genuinely indicated for cases ofantenatal or intrapartum fetal distress. Even womenwith breech or twin pregnancy can reap the benefitof this procedure, albeit, the large majority of themwill do well without a cesarean section.9 Even ifproven life-saving, but if performed without properindications, it may lead to consequences such asplacental abnormalities like placental accretasyndromes and placenta previa, in addition to cesareanscar pregnancy. All of which may lead to lethalcomplications for both the mother and the fetus.
In the recent years, several studies haveemphasized the rise in the occurrence of CSPsworldwide which coincides with the increase in therates of cesarean scar section potentially making thema dangerous combination. Over the past three decades,rates of cesarean sections have been on the rise despitethe ideal rate of 10-15% that has been set by the WorldHealth Organization (WHO) in 1985 at Fortaleza,Brazil.10 The inflation of cesarean section rates havebeen attributed to several factors which includecesarean delivery on request, decreased number ofpatients who are willing to subject themselves onVaginal Birth after Cesarean Section (VBAC),decreased vaginal births of breech presentation, andincreased prevalence of high risk pregnancies suchas advanced maternal age and subjective indicationssuch as non-reassuring fetal status and arrest incervical dilatation.11
According to statistics from the United NationsInternational Children's Emergency Fund (UNICEF),despite efforts made by the World Health Organizationand other world administrations, the cesarean sectionrates are still on the rise even locally in the Philippines.From the available Philippine data gathered byUNICEF(2003), CS rate was at the minimum of 7%.As the year 2008 and 2009 approaches, it showed anincreasing trend from 7% to 10-11% respectively. Byyear 2013, a decline to a rate of 9% was observed,however, by year 2016 the highest recorded rate at11.2% was noted.
Five year statistics of cesarean section rates takenfrom Philippine Obstetrics and Gynecological Society(POGS) showed an increasing trend from 2011 andreached its peak by the year 2014 at 38%. By the
year 2015, it was reduced to at least 31%, but stillcomprises about one third of all deliveries made duringthe year 2015.
The primary cesarean section rates in FEU-NRMFinstitution also showed an increasing trend. It had asteady rate from year 2012 to 2014 and a remarkabledecline was noted on year 2015 at 17.07%. Even so,from the year 2015 to 2016 it showed an extensiverise to 26.36%, the highest recorded Primary CesareanSection rate in the Institution. The primary cesareansection will most likely deliver via repeat cesareansection, as well. Increasing probability of a CSP andits other consequences.
With the availability and access to imaging studiesfor diagnosing different kinds of diseases, CSpregnancy is now better recognized and earlierdiagnosed.
Just like in these 2 cases of cesarean scarpregnancy, the diagnosis was made promptly throughtransvaginal sonography and managed earlypreventing life-threatening complications.
Another factor that has contributed to itsoccurrence is the change in operative techniques ofclosing the uterus through a single layer techniquerather than a double or multiple layer which is thecommon practice from the past. Single layertechnique is associated with the development of aphenomenon known as a 'niche'. A 'niche' describesthe presence of a hypoechoic area within themyometrium of the lower uterine segment, reflectinga discontinuation of the myometrium at the site of aprevious CS, providing a ground for the implantationof a conceptus.6
Yazicioglu, et al. (2006) made a significant studyamong 98 patients where they used two differenttechniques in closing the uterus during cesareansection. One technique was closing the single layerfull-thickness of the uterus including the endometriallayer and the other was multiple layer split-thicknessclosing wherein he excluded the closing of theendometrial layer. The results revealed lower ratesof formation of cesarean scar defect among thosewho underwent mul t ip le layer c losure . Theexplanation is that single layer uterine closure maynot be able to guarantee an accurate alignment ofuterine edges, therefore, increasing the chances ofCS defect formation.7
In both patients, there was no previous ultrasoundprior to pregnancy to note for any presence of "niche"and the manner of uterine closure during the previouscesarean sections was unknown.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 53
Cesarean scar pregnancy is the invasion of theconceptus on the myometrium of a previous cesareansection scar. Its etiology still remains a controversyand still subjected for argumentative debates. Themost plausible theory suggests that the blastocystenters into the wall through a microscopic dehiscenttract, which may have been created through a traumathat occurred in association with a cesarean sectionor any other uterine surgery such as dilatation andcurettage (Cheng, et al. 2003), or even followingmanual removal of the placenta (Fylstra, 2002). InVitro Fertilization could also represent a raremechanism (Seow, et al., 2000, 2004), or CSP caneven occur in the absence of any previous uterinesurgery (Hamilton, et al., 1992).5
The most common manifestation of cesarean scarpregnancy is painless, vaginal bleeding. However,there are no specific clinical signs that may pointdirectly to CSP. In a study by Silver et al., presentingsymptoms of CSP observed in 57 pregnant women,37% are asymptomatic, 38% have painless vaginalbleeding, 16% had painful vaginal bleeding, and 9%experienced abdominal pain without vaginal bleeding.13
In these two cases, both presented with vaginalspotting or bleeding. The first case had an associatedhypogastric pain while the second case presented withlow back pain, representing a myriad of its presentingsymptoms, in which, at an early pregnancy, can easilybe mistaken as a form of abortion.
Cesarean scar pregnancy was first recognized in1978 by Larsen and Solomon as a postabortalhemorrhage due to what the authors called a uterinescar sacculus. Since then, cases have been reportedleading to better understanding of its occurrence. Dueto the rarity of its existence in the past, there existsno specific guidelines created for its diagnosis andmanagement. It has been often misdiagnosed asincomplete abortion, abortion in progress and patientsmistakenly undergo curettage leading to life threateninghemorrhage. Diagnosis of CSP requires a high indexof suspicion, especially, when upon ultrasonography,no intrauterine gestational sac can be identified,therefore, pregnancy of unknown location is suspected.Usual differential diagnoses for CSP is cervical ectopicpregnancy, placenta accreta and abortion in progressor incomplete abortion.14
The gold standard for the diagnosis of CSP istransvaginal ultrasonography (TVUS) with anaccuracy rate of 89%. The diagnosis is based onfinding a gestational sac at the site of the previouscesarean section scar in the presence of an empty
uterine cavity and cervix, as well as a thin myometriumadjacent to the bladder.15
In these 2 cases, the CSP were diagnosed earlyand both fulfilled the criteria mentioned above. Theuterus were both empty with the endometrium clearlydemonstrated, the cervical canals were both empty torule out cervical pregnancy or abortion in progressand lastly the gestational sac is located in the anteriorpart of the isthmic portion of the uterus, embeddedand surrounded by the myometrium.
Management of CSP still remains controversialbecause of the lack of evidence-based standards forits treatment. Management options cater to individualpatients depending on gestational age, fetal viability,severity of symptoms, serum hCG levels andultrasonography findings. Options vary: conservativeusing either medical and surgical approach, if thewoman is still desirous of pregnancy or radicalinvolving surgical removal of the uterus. In the medicalapproach several agents can be used, one of which isMethotrexate, which can be administered systemicallyor locally. It can be injected directly to the sac alongwith potassium chloride into the fetal heart, but ethicalconsideration is an issue with the risk of uterine rupturein the subsequent pregnancies.16 Other nonsurgicalapproach can be through uterine artery embolization(UAE). Undoubtedly, the non-surgical interventionsare less invasive and has lesser complications,however, its downside is that it requires longer timeframe for follow up until normalization of hCG levelsand serial ultrasonographic monitoring for theshrinkage of the sac. Surgical interventions are alsoreliable, usually laparotomy and resection of ectopicsac along with previous scar tissue is done and in skilledhands, laparoscopic excision alone would suffice.Serial hCG monitoring is usually done in medical andconservative surgical management, for the reason thatdecline of hCG levels is longer in CSP since thegestational sac is implanted on a fibrous tissue.Therefore, resorption of hCG takes longer. As withthe second case, the patient is still desirous of futurepregnancies, hence, a more conservative approachwas done. Due to the size of the gestational sac, aswell as the presence of cardiac activity, Methotrexatewas not an option. Conservative surgical laparoscopicexcision was the best option. Recurrence of CS scarpregnancy is stil l possible in the subsequentpregnancies thus an earlier surveillance is required torule it out.
Many of the post treatment complications reportedin the literature review were due to the clinicians

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201754
unknowing that increases in hCG concentrations couldbe expected with the treatment, as Dr. Timor-Tritschnoted.
"Many secondary treatments were triggered notby bleeding, but by the observation of a post-treatmentincrease the hCG cycle and vascularity," he said. "Thetreatments often resulted in escalation of the criticalsituation and often hysterectomy." Furthermore, headded "Knowledge of the naturally occurring increaseof the hCG volume in blood vessels with a slowresolution could have avoided a secondaryresolution."19
As with the second case, her hCG levels remainedhigh on the few weeks postoperatively but graduallydeclined to normal levels. Through observation andknowledge of the natural pattern of hCG in CSP, overtreatment was avoided.
In contrast, for patients who are not desirous forfuture pregnancies, total abdominal hysterectomy canbe done.17 In the first case, the patient is multigravida,G6P5, thus the decision to do total abdominalhysterectomy was the most optimal choice, as it givesthe best access to the pelvic structures, more controlledoperative field and lesser operative time and bloodloss.
RECOMMENDATIONS
There are several factors that contribute to theoccurrence of cesarean scar pregnancy. The strongestassociation is having previous cesarean sections.Therefore, measures must be taken to control the risein cesarean section rates worldwide. The followingare the recommendations this paper intends to imparton how to decrease the incidence of cesarean scarpregnancy:
1. Strict adherence to correct indications forperforming cesarean sections
2. Trial of labor or vaginal birth after cesarean section(VBAC) of patients who had one previous lowsegment cesarean section and fulfill the criteriafor VBAC
3. Breech vaginal delivery for multiparous women4. Closing of the uterus in two to three layers to
lessen the phenomenon of niche formation5. Accurate reporting of the specific types of ectopic
pregnancies for a more accurate and detailedstatistics of CSP in the Philippines
In the Philippines, several tertiary hospitals havegiven case reports on their encounters with cesareanscar pregnancy. However, these reports are notreflected in the incidence rates due to inaccuratereporting. This paper, therefore, hopes to createawareness to the increasing probability of thiscondition happening to every Filipino woman who hasundergone cesarean sections in the past or those withother risk factors. Without accurate reporting, wefurther subject these patients to the life threateningoutcomes that cesarean scar pregnancy may bring.With accurate reporting, on the other hand, we promotewomen's health to fulfill the fifth millenniumdevelopmental goal, which is to improve maternalhealth because cesarean scar pregnancy is not a rarityanymore.
Cesarean scar pregnancy, a previously rare entity,now occurring more than ever, should be recognized,reported and most importantly prevented.
REFERENCES
1. Srinivas M, Ragupathy K, Ndumbe F. Case Reports inObstetrics and Gynecology 2013: 525187. 2. Dilemma inthe Management of Caesarean Scar Pregnancy. Reprod SystSex Disord, 2014
2. Ash A, Smith A, Maxwell D. Caesarean scar pregnancy.BJOG 2007; 114: 253-63.
3. Sepilian, et al. Successful conservative management ofcervical pregnancy: a case series. Arch Gynecol Obstet May2010 ;Tulandi T, Lau S. Methotrexate treatment of tubal andinterstitial pregnancy. Fertil Steril 1999; 72:207, Falk SJ,Barbieri RL, Literature Review Jan 2010
4. Seow K-M, Huang L-W, Lin YH, Yan-Sheng Lin M, Tsai Y-L, Hwang J-L. Cesarean scar pregnancy issues in management.Ultrasound ObstetGynecol 2004; 23: 247-53.
5. Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R, etal. First-trimester diagnosis and management of pregnanciesimplanted into the lower uterine segment cesarean sectionscar. Ultrasound Obstet Gynecol 2003; 21: 220-7.
6. Uittenbogaard LB, Hehenkamp WJK, Bro lmann HAM,Mol BWJ, Huirne JAF. VU University Medical Centre,Amsterdam, The Netherlands; Why do niches develop incaesarean uterine scars? Hypotheses on the aetiology ofniche development
7. Yazicioglu F, et al. Eur J Obstet Gynecol Reprod Biol 2006;124: 32-6.
8. Barros, et al. 2011; Deng, et al., 2014; Feng, et al., 2014;Osterman and Martin, 2014
9. Hofmeyer, et al., 2015; Roberts, et al., 2015; Vlemmix, etal., 2015
10. Saleh AM, et al. J Perinat Med. 201611. Barber EL, Lundsberg LS, Belanger K, Pettker CM, Funai
EF, Illuzzi JL. Indications contributing to the increasingcesarean delivery rate. Obstet Gynec 2011; 118(1): 29-38.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 55
12. Gibbons L, Belizan JM, Lauer JA, Betran AP, Merialdi M,Althabe F. The Global Numbers and Costs of AdditionallyNeeded and Unnecessary Cesarean Sections Performed perYear: Overuse as a Barrier to Universal Coverage
13. Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY,et al. Maternal morbidity associated with multiple repeatcesarean deliveries. Obstet Gynecol 2006; 107: 1226-32.
14. Koruglu M, Kayhan A, Soylu FN, Erol B, Schmid-TannwaldC, Gurses C, Karademir I, et al. MR imaging of ectopicpregnancy with an emphasis on unusual implantation sites.Jpn J Radiol
15. Timor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T,Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy
16. Nagi JB, Helmy S, Ofili-Yebovi D, Yazbek J, Sawyer E,Jurkovic D. Reproductive outcomes of women with aprevious history of cesarean ectopic scar pregnancy. HumReprod 2007; 22(7): 2012-5.
17. Kanat-Pektas M, Bodur S, Dundar O, Bakir VL. Systematicreview: What is the best first-line approach for cesareansection ectopic pregnancy?. Taiwanese J Obstet Gynecol2016; 55(2): 263-9.
18. Nankali A, Ataee M, Shahlazadeh H, Daeichin S. Surgicalmanagement of the cesarean scar ectopic pregnancy: A casereport. Case Reports Obstet Gynecol 2013; 525187
19. Melville M. Cesarean scar pregnancies emerge in wake ofincreased cesareans - Medscape - Apr 06, 2012.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201756
A Rare Case of an Ovarian Epithelial Tumor in aPre-menarchal Adolescent Girl*
Justin W. Ng Sinco, MD
This is a case of a 10-year-old female who presented with a sudden, sharp, stabbing, non- radiating,progressive hypogastric pain. This was not associated with any other symptom. The abdomen was soft,but tender at the lower abdomen. There was a palpable and tender right adnexal cystic mass. Ultrasoundrevealed a large, cystic right adnexal mass. Hence, the consideration was an Ovarian New Growth (ONG).Germ cell tumors are the most common type of ovarian tumors in this age group, hence, serum markerswere measured, such as Beta-HCG and serum AFP, which were normal. A definitive diagnosis was madeby histopathology. The patient underwent surgery with frozen section for immediate identification of overtlymalignant cells, especially because germ cell tumors were ruled out. A mucinous cystadenoma (MCA) withbenign features was seen in the right ovary along with an atypical proliferative mucinous tumor in the leftovary, also known as a borderline malignant tumor.As the left ovary showed atypical cells and was at risk for malignancy; it was resected along with thefallopian tube. The right ovary was retained. Peritoneal fluid cytology was negative for malignant cells,hence the patient was discharged well and advised close follow-up.
Abdominal pain is a fairly common presentingsymptom and is present in a myriad of diseases.Hence, an accurate description of the pain and acomplete physical examination are necessary in dealingwith it. The abdomen is a large body cavity housingmany vital organs. In order to differentiate the causesof abdominal pain, it has been traditionally divided intoquadrants to narrow down the organ involved, as eachquadrant represents the organs seen in those areas.Even more specific, the abdomen can be divided into9 areas - bilateral hypochondriac, lumbar and iliac,and the epigastric, umbilical and hypogastric regions.In this case, the patient complained of hypogastric painalong with tenderness at different sites - the righthemiabdomen and left upper quadrant.
ABSTRACT
* From the Department of Child Health
Apart from the location of the abdominal pain, theage and sex of the patient need to be taken intoaccount. Majority of the cases of abdominal pain canbe treated medically. However, when the cause ofabdominal pain is difficult to assess, surgical andgynecological consults are warranted. Besides,imaging assists in determining the cause of abdominalpain.
Numerous rapid physical and psychologicalchanges brought about by changes in hormonalsecretion and patterns occur during adolescence.Adolescence is divided into three stages - the early,middle and late adolescence that occurs at 10 to 13,14 to 17 and 18 to 21 years of age, respectively.1 Inadolescent females, though uncommon, abdominal painmay be ovarian in origin, which present withhypogastric pain. Ovarian tumors in children andadolescents are uncommon, constituting only 10% -20% of all ovarian malignancies2, and only 1% of all

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 57
childhood malignancies. Ten to thirty percent of allchildhood and adolescent ovarian tumors aremalignant.1 The clinical picture of ovarian tumors oftenoverlap and it is difficult to differentiate one from theother. As such, tumor markers and hormones can assistin narrowing down the differential diagnoses.Definitive diagnosis, however, requires ahistopathologic examination of the tumor. And thus,appropriate treatment can be initiated, if warranted,along with patient education and clinical monitoring.
Ovarian new growths, especially mucinous ones,are often unilateral. This is the first reported case ofbilateral ovarian new growths in the pediatricpopulation in our institution.
Objective
This report aims to discuss a rare case of anepithelial ovarian tumor in a 10-year-old pre-menarchalgirl.
THE CASE
K.E. is a 10-year-old premenarchal girl whopresented with a sudden and progressive, non-radiating hypogastric pain, minimally relieved bywarm compress a few hours prior to admission. Thiswas associated with 1 episode of non-bilious, non-projectile vomiting of previously ingested food.There was no loose stools nor fever. Upon physicalexamination, the patient was conscious, coherent,with signs of some dehydration, with stable vitalsigns, and with Tanner stage 2. The abdomen wasflabby, soft, with direct tenderness on the right upper,lef t upper and r ight lower quadrants , wi thnormoact ive bowel sounds and no reboundtenderness. There was no costovertebral angletenderness, nor renal bruits heard. There was apalpable, tender cystic mass at the right adnexa upondigital rectal examination. There were no signs ofprecocious puberty or virilization. She is a diagnosedcase of mild, intermittent allergic rhinitis as well,and is on isoniazid therapy because of pulmonarytuberculosis exposure.
The above physical examination findings pointedto an either surgical or gynecologic cause for theabdominal pain - such as an abdominal or pelvic mass,and/or acute appendicitis. In order to identify thestructure/s involved, a whole abdominal ultrasound wasdone and showed a large (25.1cm x 6.4cm x 20.3cm),
multi-loculated cystic mass in the right adnexa, likelyto be ovarian in origin.
The admitting diagnoses were nulligravid; OvarianNew Growth (ONG); some dehydration, mild; allergicrhinitis, mild intermittent; pulmonary tuberculosisexposure, on 2nd month ongoing treatment. The goldstandard in diagnosing ONG is histopathology.However, in order to differentiate its cellular origin orcomponents, serum β-human chorionic gonadotrophin(β-hCG) and alpha-fetoprotein (AFP) were measured.Both serum markers were normal in K.E.
Acute appendicitis was also a consideration. Theblood counts showed leukocytosis with neutrophilicpredominance. The urinalysis showed trace ketonuriaprobably because of dehydration or stress broughtabout by the vomiting. At this point, however,appendicitis could not yet be totally ruled out.
The scheduled operation was delayed because thepatient had wheezes on the right apical lung whenbrought down to the operating room. This was treatedwith Salbutamol nebulization along with Budesonidenebulization. The patient underwent exploratorylaparotomy; peritoneal fluid cytology; left salpingo-oophorectomy with frozen section of the left ovary;right oophorocystectomy with frozen section on the4th hospital day. Intra-operative gross examinationshowed an unenlarged and grossly normal uterus andnormal right fallopian tube. The right ovary had a 15cmx 8cm x 5cm cystic mass with a smooth capsule andthe left ovary had an 8cm x 7cm x 3cm cystic mass.Frozen section of the right ovarian cyst showed"benign" histomorphologic features consistent withmucinous cystadenoma (MCA). Inadvertent ruptureof the cyst showed serous fluid. The right ovarian cystwall had a smooth inner capsule, with capsularthickness of 0.3cm - 0.5cm. The frozen section of theleft ovary, on the other hand, showed atypicalproliferative mucinous tumor. Lymph node dissection,left, was hence performed to rule out lymphatic spread.For complete surgical staging, cytology of theperitoneal washing was performed, which wasnegative for malignant cells. Surgery service didelective appendectomy because mucinous tumors maybe appendiceal in origin. The patient tolerated theprocedure well.
The final surgical pathology report showed:1) Atypical proliferative mucinous tumor, left ovary,2) negative for tumor: lymphovascular space,omentum, left external iliac lymph node, left internaliliac lymph node, left obturator lymph node,3) mucinous cystadenoma and cystic follicles, right

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201758
ovary, 4) chronic inflammation, appendix, and5) congestion and acute and chronic inflammation,omentum.
In the presence of normal serum AFP and β-hCG,and the absence of precocious puberty or signs ofvirilization, an epithelial ovarian tumor could indeedbe a likely diagnosis. In the patient, the right ovariancyst was indeed large at presentation causing theabdominal pain.
The final diagnoses were nulligravid; ONG,bilateral with frozen section of Right Ovarian Cyst -"Benign" Mucinous Cystadenoma, Frozen section ofleft ovary - Atypical Proliferative Mucinous Tumor;Reactive Airway Disease; Some dehydration, mild -corrected; Allergic Rhinitis, mild, intermittent; PPTB,exposure - 2nd month ongoing treatment; s/pExploratory Laparotomy, Peritoneal Fluid Cytology,Left Salpingooophorectomy with frozen section, Rightoophorocystectomy; with frozen section, left lymphnode dissection; Infracolic Omentectomy,Appendectomy.
DISCUSSION
Abdominal pain is a common but non-specificpresenting symptom of many diseases. Often,abdominal pain is due to a disease that can be treatedmedically such as gastroenteritis or acid peptic disease.However, the abdomen is a large cavity housing amyriad of organs, and as such, abdominal pain mayindeed be an alarming symptom to both the patientand the clinician. Pain receptors in the abdomenrespond to mechanical and chemical stimuli. Thesevisceral receptors are located on serosal surfaces,within the mesentery and within the walls of hollowviscera, and these receptors transmit the pain tocorresponding areas on the abdomen - bilateralhypochondriac, lumbar and iliac, and the epigastric,umbilical and hypogastric regions.
In K.E., the abdominal pain was at the hypogastricarea, and the palpable mass was at the right adnexa.Indeed, the hypogastrium in female patients isimportant because this area houses the reproductiveorgans - uterus, fallopian tubes, and ovaries - and assuch, imaging is important to determine the specificstructure/s involved. A whole abdominal ultrasoundwas done because of its convenience (ease of use,does not require sedation, and lack of ionizingradiation), high sensitivity (92%) and affordability3,4
and showed a large multilocular cystic mass likely to
be ovarian in origin. There is the likelihood that thismay be malignant, especially in premenarchal girls whoare less likely to have benign follicular cysts secondaryto hyperstimulation of the follicles or epithelium byFSH and LH.
Ovarian tumors in children are relativelyuncommon, with an estimated incidence of 2.6 casesper 100,000 girls per year.2 Ovarian malignancies arerare in children and adolescents as compared to adults,but are the most common genital tumor, accountingfor 60-70% of all gynecologic malignancies in this agegroup. Germ cell tumors (GCTs) are the most commontype of ovarian tumor in children followed by surfaceepithelial stromal tumors, and sex cord-stromal tumors.In the Philippines, the incidence of ovarian tumors is18.6/100,000 women-years.5 In FEU-NRMF, for thepast 5 years, the authors had 155 patients with ovariannew growth, and only 4 of these were in the pediatricpopulation.
Regardless of the type of tumor, abdominal painis the most common presenting symptom along witha palpable abdominal or pelvic mass. Often, largeadnexal masses also present with abdominaldistention. The symptomatology and radiographicfindings of adnexal masses are often non-specific.2
However, some ovarian tumors produce specifictumor markers that can aid in narrowing the diagnosis.Since germ cell tumors are most common in youngergirls, AFP and β-hCG were assayed in this patient.Examples of GCTs such as immature teratoma andyolk sac tumors produce AFP; choriocarcinoma anddysgerminoma produce β-hCG. In this patient, bothAFP and β-hCG were normal. This tumor, thus, couldbe a sex cord-stromal tumor or an epithelial tumor.
Ancillary laboratory studies were done to rule outother co-morbidities or complications. Diffuseabdominal tenderness is a sign of an acute abdomen,so surgical diseases should still be considered. Acomplete blood count with platelet count was donebecause acute appendicitis could still be likely.Urinalysis was also done because sterile pyuria maybe present in acute appendicitis as well. In our case,there was leukocytosis with neutrophilicpredominance, often seen in appendicitis, but therewas no pyuria.
The patient then underwent exploratory laparotomywith frozen section of both ovaries, as previouslydescribed. The right ovary showed a benign mucinoustumor, and incidentally, the left ovary was enlarged aswell, showing an atypical proliferative mucinous tumor.Epithelial tumors are rare in premenarchal girls since

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 59
these tumors are usually secondary to hormonalstimulation. Epithelial tumors in children are usuallyof the mucinous (15-25%) or serous (20-50%)subtype.6 Benign MCAs are likely to be large atpresentation, averaging to 16-20cm. Mucinousepithelial tumors often occur unilaterally, especiallywhen primarily ovarian in origin. A large retrospectiveseries and an SEER database analysis showed thatup to 79% of mucinous tumors are unilateral.7,8 Thistype of tumor is benign. On the other hand, atypicalproliferative ovarian tumors, also known as borderlineovarian tumors (BOTs), are named as such becausethese tumors show some features of malignancy suchas nuclear atypia and stratification of the columnarepithelium, but without destructive stromal invasion.9
Mucinous ovarian tumors have a distinctcytogenetic profile from the other tumors of the ovary.These types of tumors have been associated withmutations of the KRAS gene that stimulate cellgrowth. Mutations in genes that inhibit cell growthusually associated with breast and ovarianmalignancies such as the BRCA 1 and 2, and p53genes occur less frequently in mucinous ovariantumors. Mucinous tumors also express E-cadherinmore frequently than serous tumors, and expressN-cadherin less frequently than serous tumors.10
The vast majority of mucinous borderline tumors(MBTs) have an excellent prognosis. However, thereis a risk for recurrence in the form of carcinoma.11,12
Hence, the left ovary along with its fallopian tube wasresected. Up to 75% of BOTs are diagnosed at FIGOstage I, i.e. confined to the ovaries. Local guidelinesrecommend, though, to assess the ipsilateral lymphnodes, the omentum and the peritoneal washings.Peritoneal implants are very uncommon in cases ofmucinous borderline tumors (MBTs) (15%). Trueenough, the related lymph nodes, omentum andperitoneal washings were negative for malignant cells.Current guidelines also recommend that patients withsuspicious ovarian masses should undergo totalabdominal hysterectomy with bilateral salpingo-oophorectomy or, unilateral salpingo-oophorectomywith frozen section for young patients wanting topreserve fertility with FIGO stage IA disease.4
However, a review done in 2006 evaluated the risk ofrecurrence for serous and non-serous BOTs, includingmucinous BOTs. Ninety one out of the 121 cases weremucinous. The 10-year disease-free survival rate ofthose with MBTs who underwent conservative surgerywas 57.4%, but no tumor-related deaths. Hence,conservative surgery can be done for non-serous
tumors.13 In contrast, benign MCAs in perimenarchalgirls do not possess this risk. A review of 6 cases ofMCA in perimenarchal girls in 2006 observed that onfollow-up ranging from 2.4 to 5 years, there was noevidence of recurrence.10 If the cyst is benign,therefore, there is room for conservative surgery tomaintain fertility, so the right ovary and fallopian tubewere retained.
Because of the risk for recurrence, follow-up mustbe done and should include ultrasound of the pelvicorgans and CA-125 levels, as this tumor marker isproduced by epithelial tumors and is useful to monitorrecurrence. Current recommendations do not supportthe use of CA-125 to diagnose a tumor as it is non-specific. Additionally, CA19-9 might be more specificfor mucinous tumors. Once every four months follow-up is recommended for the first two years, then onceevery six months for the next three to five years, thenannually.12
Now that the symptoms have been alleviated, andthe risk for recurrence evaluated, the issue of thereproductive function of the patient needs to beaddressed. Indeed, the ovaries are vital in the physicaland sexual maturation of women, as well asreproduction. It has long been postulated that womenare born with a limited number of oocytes, and theseare responsible for fertility. These oocytes are spentgradually throughout a woman's life. Hence, femalereproductive aging has been proposed to proceed asan ongoing decline in ovarian reserve, determined byremaining ovarian follicles. However, studies haveconcluded that the reproductive function and aging ofwomen who have had unilateral oophorectomy remainnormal - menopause occurred earlier but did not occurprematurely (i.e. occurring before 40 years old).14,15
In fact, a retrospective review of females whounderwent unilateral oophorectomy and ovarian-sparing surgery during childhood and ovarian functionconcluded that unilateral oophorectomy does not affectage of menarche, and it even appears to maintainmenstrual regularity with less incidence ofdysmenorrhea.16 Literature review did not reveal thatunilateral salpingo-oophorectomy adversely affectedfecundability and pregnancy outcomes.
SUMMARY
This is indeed an unlikely case wherein bothovaries of a pre-menarchal girl were affected withdifferent degrees of mucinous neoplasia - a benign

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201760
one on the right, and a borderline one on the left.Though it is yet to be fully understood, the factorscontributing to the development of a BOT on theleft ovary might affect the right ovary as well. Aspediatricians, holistic treatment of the patient isimportant because they are in the frontlines - avanguard against harm. Again, ovarian tumors,though rare in childhood, do occur and they mayhave grave implications for the child and the familybecause some of these tumors have to be removedalong with the whole ovary, as what happened tothe patient. Though unilateral oophorectomy has noeffec t on reproduct ive funct ion, mal ignantrecurrence can still occur especially since the rightovary was spared. The reproductive ability mayeventually be affected.
There has been little study on the psychologicalimpact of ovarian resection in children, but the
authors can probably surmise that it is as emotionallytaxing as it is in adults. Fortunately, this was arelat ively benign case and not a ful l-blownmalignancy; as previously stated, benign ovariantumors in childhood are the less common type.
The role of the pediatrician is vital not only intreating patients but also in divulging importantinformation regarding the medical condition, the mass,the surgical procedure, the impact on reproductive lifeand its psychological effects. The pediatrician isalways faced with the challenge of effectivelycommunicating the illness and its complications to thepatient and parents. Awareness, therefore, of this rarebenign epithelial tumor and borderline tumor gives aglimmer of hope for the physician as well as thefamilies of patients with ovarian tumors, because in aworld where events are usually downhill, everyoneneeds a bit of good news every now and then.
Figure 1. Transabdominal ultrasound showing a large, multiloculated cystic mass on the right adnexa, likely to be ovarian inorigin
Figure 2. Intraoperative gross findings - (a) both ovaries were cystically enlarged, (b) right ovary measured 15cm x 8cm x5 cm, and the (c, d) left ovary measured 8cm x 7cm x 3cm.
Appendix

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 61
Figure 3. Cut section of the left ovary showing atypicalproliferative mucinous tumor. There is stratification of thecolumnar epithelium with nuclear atypia, without stromal invasion
REFERENCES
1. Kliegman RM, Stanton BF, St. Geme JIW, Schor NF, BehrmanRE. Nelson's Textbook of Pediatrics 20th edit ion,Philadelphia: Elsevier, 2016.
2. Heo SH, Kim JW, Shin SS, Jeong SI, Lim HS, Choi YD, LeeKH, Kang WD, Jeong YY, Kang HK. Review of OvarianTumors in Children and Adolescents: Radiologic-PathologicCorrelation, 7 April 2014.
3. Smorgick N, Maymon R. Assessment of adnexal masses usingultrasound: a practical review. Int J Womens Health 2014; 6:857-63.
4. Philippine Obstetrical & Gynecological Society, SGOPTreatment Guidelines, 2012.
5. Philippine Obstetrical and Gynecological Society, ClinicalPractice Guidelines on Myoma and Adnexal Masses, 2010.
6. Lobo R, Gershenson D, Lentz G, Valea F. ComprehensiveGynecology, 7 ed., Philadelphia: Elsevier, 2017.
7. Riopel MA, Ronnett BM and Kurman RJ. Evaluation ofdiagnostic criteria and behavior of ovarian intestinal-typemucinous tumors: atypical proliferative (borderline) tumorsand intraepithelial, microinvasive, invasive and metastaticcarcinomas. Am J Surg Pathol 1999; 23(6): 617-35.
8. Boger-Megiddo I, Weiss NS. Histologic subtypes andlaterality of primary epithelial ovarian tumors. GynecolOncol 2005.
9. Silverberg S, Bell D, Kurman R, Seidman J, Prat J, RonnetB, and e. al. Borderline ovarian tumors: key points andworkshop summary. Hum Pathol 2004; 8(35): 910-7.
10. Sri Paran T, Mortell A, Devaney D, Pinter A, Puri P.Mucinous cystadenoma of the ovary in perimenarchalgirls. Pedia Surg Int 2006; 22(3): 224-7.
11. Hauptmann S, Friedrich K, Redline R, Avril S. Ovarianborderline tumors in the 2014 WHO classification: evolvingconcepts and diagnostic criteria. Virchows 2017; 470(2): 125-42.
12. Abascal-Saiz A, Sotillo-Mallo L, de Santiago J, Zapardiel I.Management of borderline ovarian tumours: a comprehensivereview of the literature. Ecancer medical science 2014;403(8).
13. Yokoyama Y, Moriya T, Takano T, et al. Clinical outcomeand risk factors for recurrence in borderline ovarian tumours.Br J Cancer 2006; 94(11): 1586-91.
14. Wilkosz P, Greggains G, Tanbo T, Fedorcsak P. Femalereproductive decline is determined by remaining ovarianreserve and age. 2014; PLoS One, 9(10): e108343.
15. Thomas-Teinturier C, El Fayech C, Oberlin O, PacquementH, Haddy N, Labbe M, Veres C, Guibout C, Diallo I, DeVathaire F. Age at menopause and its influencing factors in acohort of survivors of childhood cancer: earlier but rarelypremature. Hum Reprod 2013; 2(28): 488-95.
16. Zhai A, Axt J, Hamilton E, Koehler E, Lovvorn H. Assessinggonadal function after childhood ovarian surgery. PediatrSurg 2012; 6(47): 1272-9.
17. Brown J, Frumovitz M. Mucinous tumors of the ovary:Current thoughts on diagnosis and management. 29 April2014. [Online]. Available: doi: 10.1007/s11912-014-0389-x.[Accessed 19 July 2017].

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201762
Iridocorneal Endothelial (ICE) Syndrome*
Ferdinand N. Valbuena Jr., MD
This is a case of a 50 year old female who presented with blurring of vision on the left eye. This wasaccompanied by on and off eye pain, and foreign body sensation. Previous consults were done wherein thepatient was given topical ophthalmic lubricants. However, due to the progression of the blurring of vision,patient sought consult at FEU-NRMF. Ophthalmologic examination revealed a visual acuity of 20/20 onthe right eye and counting fingers at 3ft on the left eye, cornea was hazy and iris abnormalities seen on theleft eye. Intraocular pressure at initial consult was within normal on the right eye and elevated on the lefteye. Patient was then referred to External Disease & Cornea as well as Glaucoma service for furtherevaluation and management. A clinical impression of Iridocorneal Endothelial Syndrome and secondaryglaucoma was made. She was managed medically with pressure lowering agents and hypertonic salinesolution. A month from initial consult, visual acuity improved and decrease in corneal edema was noted.However, the patient was unable to return for subsequent follow-up and came back complaining of eye painand progressive blurring of vision. Surgical management was then planned to control the intraocularpressure and reduce corneal edema. The patient eventually underwent a glaucoma filtering surgery(trabeculectomy) which successfully controlled and maintained intraocular pressure within normal levels.After controlling the IOP, Corneal transplantation (penetrating keratoplasty) pupilloplasty and cataractextraction was then done 6 months post-trabeculectomy. Currently, visual acuity on the left eye was 5/200improved to 20/63 on pinhole and maintained IOP within normal levels without the aid of IOP-loweringmedications.
The eyes are one of the most sensitive anddelicate parts of the human body. Although many maydisregard signs and symptoms that do not affect theirdaily activities, any significant decrease in clarity willprompt patient to seek eye consult. This symptommay be a result of various ocular disease entities,ranging from structural defects (e.g. interferencesin the ocular media) to dysfunctions in image
ABSTRACT
*From the Department of Ophthalmology
processing (e.g. abnormalities in visual center in thebrain). It should be assessed and managed by adoctor equipped with knowledge of the anatomy andphysiology of vision, and instruments in examiningthe eyes in complete detail.
Since the initials 'ICE' fit both the term iridocornealendothelial syndrome and the first letter of each ofthe three component entities, ICE syndrome was thesuggested term and is now the most commonly usedfor this disorder. The clinical findings in ICE syndromevary from patient to patient. Historically, it issubdivided into essential (progressive) iris atrophy,Chandler syndrome, and Cogan-Reese (iris-nevus)syndrome. It is syndrome with a broad spectrum of

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 63
clinical manifestations that share a commonfundamental pathophysiological basis wherein thereis migration of abnormal corneal endothelial cells ontothe iris. The loss of cells often leads to corneal swelling,distortion of the iris and pupil. The cell movement mayalso block the aqueous outflow of the eye causingsecondary glaucoma.
Topical pressure lowering agents are first linetherapy for patients with elevated intraocular pressurefrom secondary glaucoma in the setting of ICEsyndrome. Topical hypertonic saline solutions can alsobe utilized to improve the corneal edema bydehydrating the cornea. However, surgical therapy forcontrolling IOP through a filtering procedure is thedefinitive management to maintain IOP at normallevels. Corneal decompensation similarly may betreated surgically to replace the abnormal endothelialcells and improve corneal function. Although majorityof eyes undergoing surgical therapy for ICE syndromehad favorable outcomes, it is not without its risks (e.g.need for multiple procedures for IOP control and graftfailure).
THE CASE
The Patient
This is a case of a 50 year-old female, vendor,presently residing in Caloocan, who presented at theFEU-NRMF Ophthalmology out-patient department
with a chief complaint of blurring of vision of the lefteye.
History started 9 months prior to consult whenthe patient experienced intermittent left eye pain andforeign body sensation. No associated blurring ofvision or eye redness was noted. The patient soughtconsult at a nearby clinic and was prescribed topicalophthalmic lubricants. In the interim, she still noted onand off eye pain, but now with accompanying cloudingof vision on the left eye.
Past Medical History
The patient is a known hypertensive for 10 yearsand is maintained on Amlodipine 5mg and Losartan50mg. There was no history of diabetes, tuberculosis,ocular trauma, hospitalizations or operations. Noknown allergy to food and drugs was elicited.
Family History
Her father is a known hypertensive and her motheris a known diabetic. Her brother also has a history ofasthma. No history of any blinding disease in her familywas noted.
Physical Examination
On examination, eyelashes are evenly distributed,no matting, no discharge. The conjunctiva was non-hyperemic. Patient had a dirty looking sclera. Ocularexamination findings are presented in Table 1.
Table 1. Ocular examination findings on first consult
Right Left
Visual Acuity 20/20 Counting Fingers at 3ft
External Exam(See Figure 1) • No matting of lashes • No matting of lashes
• No discharge • No discharge• Non-hyperemic conjunctiva • Non-hyperemic conjunctiva• Dirty-looking sclera • Dirty-looking sclera• Pupils 2-3 mm, regular border, • Polycoria, non reactive to light reactive to light and accommodation
Fundoscopy (+) ROR, clear media, Unremarkable dull ROR, hazy media, other structuresnot well appreciated
Slit Lamp Exam Unremarkable Hazy cornea, polycoria, AC deep,(Figure 2) (-) cells & flares, lens: NO3 NC3
Tonometry (mmHg) 16 mmHg 33 mmHg
Ocular Motility Full on all cardinal gaze positions Full on all cardinal gaze positions
Gonioscopy PTM on all quadrants Peripheral anterior synechiae (superotemporal)

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201764
With the salient features of unilateral increasedintraocular pressure (IOP) associated with cornea andiris abnormalities in a 50-year-old female, the clinicalimpression of Iridocorneal-endothelial (ICE) syndromewith secondary glaucoma was made. She was thenreferred to the External Disease and Cornea serviceas well as the Glaucoma service for further evaluationand management. The patient was managed medicallyto control the increased IOP and address the cornealedema. A combination of timolol maleate andbrimonidine tartrate, and sodium chloride eye dropswere started. One month from her initial consult, visualacuity improved to 20/70 on the left eye. Intraocularpressure was maintained at normal levels. However,she was unable to return for subsequent follow-up.She was then seen 4 months later, complaining of eyepain and progressive blurring of vision. Visual acuity
Figure 1. External Exam of the patient
Figure 2. Slit lamp examination of the left eye shows cornealedema, iris atrophy, and pupillary anomalies, ranging fromdistortion to polycoria
was hand movement on the left eye. The cornea wasedematous and IOP at 22mmHg. The initial plan ofthe External Disease and Cornea service was to docorneal transplantation (penetrating keratoplasty),pupilloplasty and lensectomy with or without IOL butIOP was uncontrolled hence she was referred backto Glaucoma service for possible trabeculectomy.(Table 2)
Trabeculectomy was eventually performed.Although visual acuity remained at hand movementwith good light projection for the left eye, the patient'seye pain was greatly reduced. Intraocular pressurewas successfully controlled and maintained at less than15mmhg even after 6 months after surgery. (Figure3)
Table 2. Ocular examination showing progression
1 month from initial consult 4 months from initial consult 4 ½ months from initial consult
VA OS: 20/70 VA OS: Hand Movement with VA OS: Hand movement with good
Slit Lamp Exam: Decreased good light projection light projection
corneal edema Slit Lamp Exam: Edematous cornea Slit Lamp Exam: Edematous cornea
IOP OS: 15mmHg IOP OS: 22mmHg IOP OS: 20mmHg
Figure 3. Trabeculectomy of the left eye showing a diffuse midto high-rise mildly vascular filtering bleb
After controlling the IOP, the next step was toaddress the corneal edema. Corneal transplantation(PKP) pupilloplasty and cataract extraction was thendone 6 months post-trabeculectomy (Figure 4).
A week after the procedure, the patient's visualacuity improved from hand movement prior tooperation to counting fingers improved to 20/100 with

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 65
Figure 4. Penetrating keratoplasty, pupilloplasty and cataract extraction.A) Suturing of the sclera fixation ring/ Flieringa ring, B) Trephination of diseased cornea, C) Diseased corneaexcised, D) Pupilloplasty, E)Open sky extracapsular cataract extraction, F) Donor cornea sutured using Nylon10-0 16 simple interrupted sutures, G) Testing for leaks.
+10diopter lens, cornea is still slightly edematous butwith clear graft, iris was already seen at the periphery,and IOP was maintained at normal levels. One monthafter the operation, visual acuity improved to 5/200and 20/63 on pinhole, cornea is clear and IOPmaintained within normal. (Figure 5)
Figure 5. Post-penetrating keratoplasty, pupilloplasty and cataractextraction. First photo 1 week post-op, second photo 1 monthpost-op. (Table 3)
Table 3.
1 week Post-op 1 month Post-op
Visual Acuity: OS - Counting Fingers at 3 ft Visual Acuity: OS - 5 / 200 improved toSlit Lamp: Cornea is still slightly edematous, 20/ 63 on pinholeiris is in the periphery, aphakia, (+) cells/flares, Slit Lamp: Clear cornea, iris is in the periphery,no epithelial defect aphakia, no cells/flares, complete epitheliazation,IOP: OS- 9 mmHg (+)fibrosis of the anterioir and posterior capsule
IOP: OS- 16 mmHg
The patient is currently maintained on topicalantibiotics and steroids and is on regular follow-up.Intraocular pressure is stable at normal levels withoutthe aid of IOP-lowering eye medications,
Differential Diagnosis
The clinical aspects of the ICE syndrome aredistinct however there are some anterior segmentdiseases that may mimic it and that may be complicatedby the same issues such as corneal edema andglaucoma. Among them, corneal endothelial disorderssuch as posterior polymorphous dystrophy (PPMD)and iris disorders such as Axenfeld-Rieger syndrome(Table 4).

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201766
Table 4. Comparing the general characteristics of eachdifferential diagnosis for ICE syndrome
Posterior Polymorphous Dystrophy
Posterior Polymorphous Dystrophy is anautosomal dominant endothelial corneal dystrophy thatmay have variable amounts of corectopia, cornealedema, iridocorneal adhesions, and can present withboth angle-closure or open-angle glaucoma. Theeasiest differentiating factor is that PPMD is inheritedand is bilateral, whereas ICE syndrome is sporadicand unilateral.5
Axenfeld-Rieger Syndrome
Another disease that may be difficult to distinguishfrom ICE syndrome is Axenfeld-Rieger syndrome. Infact, even the pathogenesis of this syndrome is similaras the iris and iridocorneal angle alterations seen inAxenfeld-Rieger syndrome are also caused by a layerof endothelial cells. The only difference is that inAxenfeld-Rieger syndrome they are not secondary tothe migration but rather to the presence of a primordialendothelial layer. Axenfeld-Rieger syndrome is abilateral, heterogeneous congenital condition that is isautosomal dominant in most cases, but can also occursporadically, and may include developmentalabnormalities in the anterior chamber angle, iris, andtrabecular meshwork. Corectopia, polycoria, ectropionuveae, posterior embryotoxon, and increasedintraocular pressure are common ophthalmologicfindings with ARS.
DISCUSSION
Iridocorneal-Endothelial Syndrome (ICE)syndrome is a unique ophthalmic disorder that involvesan irregular corneal endothelium that can lead tovarying degrees of corneal edema, iris atrophy, andsecondary angle-closure glaucoma. It is generallyconsidered to have three major variations: Chandler'ssyndrome, progressive (essential) iris atrophy, and theCogan-Reese syndrome. Clinical distinction betweeneach subtype can be made based on uniquecharacteristics. However, each can result insubstantial visual impairment from glaucomatous opticneuropathy and / or corneal edema. Clinically, thecorneal endothelium has been described to have a"hammered silver" appearance in ICE syndromepatients (Figure 6). It is said that the normalendothelial cells have been replaced with a moreepithelial-like cell with migratory characteristics. Thealtered endothelium then migrates posteriorly, movingbeyond the Schwalbe's line, onto the trabecularmeshwork, and at times, onto the peripheral iris.Contraction of this tissue within the anterior chamberangle and on the iris results in the high peripheralanterior synechiae (PAS) (Figure 7) and iris changesthat is characteristic of ICE syndrome shown in theMembrane Theory of Campbell (Figure 8). Secondaryangle-closure glaucoma is a consequence of high PAS,but can at times occur without overt synechiaebecause the advancing corneal endothelium canfunctionally close the angle without contraction.1
Figure 6. Slit-lamp view showing the hammered-silverappearance of a corneal endothelial abnormality in a patient withICE syndrome

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 67
Figure 7. Gonioscopic view of Peripheral anterior synechia(PAS):Adhesions between iris and trabecular meshwork. PAS mayreduce outflow of aqueous humor and may lead to raisedintraocular pressure
The true etiology of ICE syndrome is not wellunderstood. In one study, an underlying viral infectionwith Herpes simplex virus (HSV) leads to a low gradeinflammation at the level of the corneal endothelium.PCR evidence shows that HSV DNA is present in asubstantial percentage of ICE syndrome cornealspecimens. Tissue samples cut from positive ICEsyndrome specimens yielded negative results whenretested after the endothelial layer was removed.These findings indicate that localization of HSV DNAis within the endothelium, the tissue primarily involvedin the pathogenesis of the ICE syndrome.4
The condition is sporadic and unilateral, affectsindividuals between 20 and 50 years of age and occursmore often in women.7 Patients present with differingdegrees of pain, decreased vision, and abnormal irisappearance. The vision may be decreased fromcorneal edema. As the syndrome progresses,
Figure 8. Membrane theory of Campbell of ICE syndromeA: Extension of the membrane from the corneal endothelium over the anterior chamber angle and onto the irisB: Contraction of the membrane, creating peripheral anterior synechiae and corectopiaC: Thinning and atrophy of iris in quadrants away from the corectopiaD: Hole formation in an area of atrophy (in progressive iris atrophy), ectropion uvea in the direction of the corectopia, and nodules in the area of the membrane (in Cogan-Reese syndrome)

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201768
symptoms of blurred vision and pain may persistthroughout the day. Patients also may present with achief complaint of an irregular shape or position ofthe pupil (corectopia), or they may describe a darkspot in the eye, which may represent hole formation(polycoria) or atrophy of the iris. Various degrees ofiris atrophy characterize each of the specific clinicalentities.2 In our patient's case, she presented with a 9month long history of on and off eye pain and foreignbody sensation with accompanying blurring of vision.When the patient sought consult in our institution, thecornea was already edematous.
In a study comparing the clinical variants ofIridocorneal-Endothelial Syndrome, the most commonvariant was Chandler's syndrome and also the onepresenting with more severe edema. Progressive irisatrophy and Cogan-Reese syndrome had worsesecondary glaucoma. In Iris-Nevus Syndrome (Cogan-Reese Syndrome), the extent of iris atrophy tends tobe less severe. Nodules that are tan and pedunculatedmay appear on the anterior iris surface. The cornealedema is predominant and typical feature of Chandler'ssyndrome with minimal or no iris stromal atrophy.While in the Progressive (Essential) Iris Atrophyvariant of ICE syndrome, formation of an iridal holeis the hallmark finding along with marked corectopia,polycoria, and ectropion uveae (Figure 9)
Table 9. Side by side comparison of the patient's left eye fromthe clinical variants of ICE syndrome
The primary aim in patients with ICE syndrome isto reduce corneal edema and glaucoma. Thus adiagnosis of ICE syndrome must be considered inyoung to middle-aged, most often females, who have
unilateral glaucoma, iris anomalies, and cornealedema.5
Aqueous suppressant medications tend to beeffective in controlling the IOP, while outflow-associated medications are less effective. Cornealedema may often be controlled using hypertonic salinesolutions. Reduction of the elevated IOP may lessenthe degree of corneal edema. If the IOP level remainsuncontrolled despite medical treatment, surgicaltherapy with a filtering procedure may be necessary.A trabeculectomy with antifibrotic agents (mitomycin-C or 5-fluorouracil) or a glaucoma drainage device(aqueous shunt) have been found to be effective incontrolling IOP in ICE syndrome patients.2 A studycomparing trabeculectomy versus GDD did notdemonstrate clear superiority of one glaucomaoperation over the other and that there are other factorsthat must be considered when selecting a surgicalprocedure, including the surgeon's skill and experiencewith both operations, the patient's willingness toundergo repeat glaucoma surgery, and the plannedsurgical approach if failure occurs.8 In the case ofour patient, Trabeculectomy with mitomycin-C wasdone. Primary trabeculectomy with MMC offersmoderate surgical success in patients with ICEsyndrome, with success rates of 94% at 6 months,82% at 12 months, 71% at 36 months, and 60% at 60months. Similarly, corneal decompensation can betreated surgically when medical management fails.Penetrating keratoplasy (PKP) or endothelialkeratoplasty can be implemented to replace theabnormal corneal endothelial cells and improve cornealfunction. At times, both a filtering and cornealtransplant procedure are necessary which wassimilarly done to the patient.1,5
It has been presumed that a filtering bleb needssufficient time to develop properly. Although therearen't much studies tackling the interval between doingtrabeculectomy prior to corneal transplantation, onecan assume that inflammation associated with cataractsurgery, as concluded in one study, curtails the sameprocess of the proper development of a filtering bleband that an interval between trabeculectomy andcataract extraction of 6 months or less was associatedsignificantly with reoperation for glaucoma.9
Prognosis of ICE syndrome patients depends onwhether complications develop. Commoncomplications include glaucomatous optic neuropathywith extensive vision loss if left untreated and cornealdecompensation.. A study reviewing the clinical courseof 12 patients which underwent penetrating

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 69
keratoplasty for corneal edema associated with theiridocorneal endothelial syndrome. The grafts remainedclear in 10 patients (83%). The prognosis ofpenetrating keratoplasty in the iridocorneal endothelialsyndrome appears to be very favorable in the majorityof eyes. However, a study about graft survival andIOP control of patients with ICE syndrome aftercorneal transplantation demonstrated graft failure afterkeratoplasty for ICE syndrome at a mean duration of4 years in one-third of patients and that additional IOP-lowering treatment was required in 37.9%.10
In summary, ICE syndrome is a unique ophthalmicdisorder with a broad spectrum of clinicalmanifestations that may vary from patient to patient.It has attracted our attention both from the enigma ofits pathogenesis and the challenges in its diagnosisand treatment. Distinction requires a thorough history,examination and knowledge of the pertinent findingsthat will direct us to our diagnosis. Excellent short-term outcomes have been reported in the eyes thatunderwent surgical procedures to control IOP andmaintain corneal clarity. However, long-term prognosisis guarded in light of the risk of failure of cornealtransplantation and glaucoma surgery. Thus,importance of regular follow-up is also emphasized.
REFERENCES
1. Glaucoma. Basic and Clinical Science Course (BCSC).American Academy of Ophthalmology 2010-2011;142-4.
2. Yanoff M, Duker J. Ophthalmology 4th edition. 2014; 1095-96.
3. Chang PC, Soong HK. Prognosis for penetrating keratoplastyin iridocorneal endothelial syndrome, March 1993.
4. Alvarado JA, Underwood JL, Green WR, et al. Detection ofherpes simplex viral DNA in the iridocorneal endothelialsyndrome. Arch Ophthalmol 1994; 112(12): 1601-9.
5. External Disease and Cornea. Basic and Clinical ScienceCourse (BCSC). American Academy of Ophthalmology,2010-2011; 344-5.
6. Wilson MC, Shields MB. A Comparison of the ClinicalVariations of the Iridocorneal Endothelial Syndrome. ArchOphthalmol 1989; 107: 1465-8.
7. Sacchetti M, Mantelli F. Diagnosis and management ofiridocorneal endothelial syndrome. BioMed ResearchInternational. 2015.
8. Chandran P, Rao HL, Mandal AK. Outcomes of primarytrabeculectomy with mitomycin-C (MMC) in eyes withglaucoma secondary to iridocorneal endothelial (ICE)syndrome. J Glaucoma. 2016.
9. Chen PP, Weaver YK. Trabeculectomy function after cataractextraction. October 1998.
10. Quek DT, Wong CW. Graft failure and intraocular pressurecontrol after keratoplasty in iridocorneal endothelialsyndrome. Am J Ophthalmol 2015.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201770
Squamous Cell Carcinoma of the Temporal Bone*
Josef Carlo Angbue Te, MD; Bernardo D. Dimacali, MD;Nathaniel W. Yang, MD and Jose Roberto V. Claridad, MD
This is a case of a 39 year old, female with recurrent left ear discharge accompanied by otalgia for 3months. The patient was initially assessed as Diffuse Otitis Externa and Chronic Suppurative Otitis Mediawith Aural Mass.Otic and oral antibiotics were given but failed to treat the condition. Tissue biopsy of the aural mass wasdone and revealed histologic sections of tissue fragments harboring sheets of atypical squamous cellsinvading the stroma. Computed Tomography of the Temporal Bone was requested and showed ill-definedsoft tissue density in the left periauricular region which extends into the external auditory canal with noextensions to the middle ear cavity with considerations of infectious versus neoplastic process.Resection of the Left Temporal Bone, Excision of the Left Parotid Tumor, Left Mandibular Condylectomy,Radical Neck Dissection on the left and Reconstruction of the defect using Pectoralis Major MyocutaneousFlap were done. Final histopathology results revealed Squamous Cell Carcinoma, mild to moderately-differentiated.
Malignancy of the ear canal, middle ear andtemporal bone is a rare entity representing less than2% of all head and neck malignancies.6,7,11 It isprimarily a disease of older adults with peak incidencein the seventh decade of life. These tumors pose majorchallenges to the clinician in terms of diagnosis, stagingand management.2
Patients with such disease initially presentwith infection of the ear. A delay in diagnosis usuallyoccurs due to its non specific ear symptoms such asin external and middle ear disease.2,6 The condition isusually diagnosed when tumor size is alreadyprominent and this worsens the prognosis. Tumorprogression is usually sudden and can affect thepreauricular soft t issues, the parotid gland,temporomandibular joint and the mastoid bone.
ABSTRACT
Squamous cell carcinoma is a common malignancyin all head and neck tumors, however the usual riskfactors involving Squamous cell carcinoma are notrelated to the Squamous cell carcinoma of the temporalbone. Although Squamous cell carcinoma has beenthe most studied and reported of malignant tumors ofthe ear and temporal bone, there is lack of consensusin staging and best treatment modalities due to theabsence of prospective randomized studies.5,6
This case report aims to present a case of aTemporal bone Squamous Cell Carcinoma on a 39 yearold female. More specifically, it aims to describe theclinical features of the case, present the diagnostic,histopathologic and management options of the case.
THE CASE
A 39 year old female patient presented at the OPDwith a three month history of otalgia and yellowishotorrhea. The patient started experiencing itchinessof the left ear. She also experienced otalgia and tinnitus* From the Department of Otolaryngology - Head and Neck Surgery

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 71
after manipulation of the left ear using cotton buds.Greenish to yellowish otorrhea on the left ear soondeveloped one week after the initial presentation. Shesought consult at a private ENT practitioner whodiagnosed her with Otitis Externa. She was prescribedwith Polymyxin Neomycin Fluocinolone otic drops andwas advised to clean her ears using a cotton soakedhydrogen peroxide three times daily for a week.Symptoms worsened with increased severity of theear pain, now associated with postauricular swelling.The patient went to another ENT practitioner and wasprescribed with Ciprofloxacin otic drops and oralantibiotics three times daily for 1 week, which providedtemporary relief.
Seven weeks prior to admission, progression ofsymptoms was noted and induration of the swellingincreased. Upon follow-up with the same hospital,otoscopy of the left ear showed an aural mass. Oticdrops were continued and oral antibiotic was shiftedto Co-Amoxiclav three times a day for 2 moreweeks. Four weeks prior to consult, worsening ofthe symptoms prompted consult to a private ENTphysician and otic drop was shifted to Ciprofloxcinwith Dexamethasone. The patient was advised toundergo tissue biopsy of the aural mass whichrevealed Squamous Cell Carcinoma, welldifferentiated.
Computed Tomography of the Temporal Boneshowed ill-defined soft tissue density in the leftperiauricular region extending into the external auditorycanal with no gross extension to the middle ear cavityconsidering infectious versus neoplastic process(Figures 1 & 2).
Two weeks prior to admission with progression ofsymptoms and increased induration of the postauricularmass on the left ear extending superiorly andposteriorly, she then consulted the ENT-HNS OPDof FEU-NRMF Medical Center.
The head and neck examination showed moderatepostauricular swelling on the left ear with erythematousborders. On palpation, the swelling was tender withrise of local temperature, there was fluctuance withoutcrepitus. Upon otoscopy, the right ear was patent withintact tympanic membrane while the left ear showedbrown rubbery material totally occluding the canal withfoul smelling discharge. There were palpable cervicallymph nodes at the pre-auricular area and level II onthe left. Intra-oral examination was unremarkable.There was no facial weakness nor asymmetry. Thepatient was advised to undergo resection of thetemporal bone with reconstruction.
Figure 1. Computed Tomography of the Temporal Bone with ill-defined soft tissue density in the left periauricular region extendinginto the external auditory canal (arrow), consider infectious versusneoplastic process. Mild erosive changes seen along thesuperficial wall of the left mastoid bone (circle). The left tympanicmembrane is not definitely identified.
Figure 2. Computed Tomography of the Temporal Bone showsintact ossicles (arrow) with no extensions to the middle ear.
One week prior to admission, with worsening ofsymptoms, post auricular swelling extended moreposteriorly (Figures 3 & 4). There was no facialweakness nor asymmetry. Working impression wasSquamous Cell Carcinoma of the temporal bone, leftear. She was scheduled for the operation henceadmission.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201772
Figure 3. A whitish rubbery mass on the external auditorycanal, left ear(a) 1 week prior to surgery(b) upon admission shows extension on mass 1 week apart
Figure 4. Postauricular induration, left ear(a) 1 week prior to surgery(b) upon admission shows increased induration 1 week later
On the 2nd hospital day resection of the temporalbone was done. Intraoperatively, a whitish massencroaching beyond the external auditory canal wasobserved. Careful dissection of the mastoid area wasdone. Upon drilling using burr tips, soft tissue tumorwas noted along the mastoid including the mastoidantrum and epitympanum. Further drilling wasperformed to identify the facial nerve however thesoft tissue was seen invading the facial nerve henceit was sacrificed. Otic capsule was noted to be spared.Excision of the Parotid gland with mandibularcondylectomy and unilateral radical neck dissection(SCM, EJV, SAN, cervical LN I-V) including the leftsubmandibular glands proceeded (Figures 5 & 6). An
8.6cm x 9.6cm defect was noted after resection ofthe external ear (Figure 7). The left pectoralis majormyocutaneous flap was used to repair the defect(Figure 8). Primary closure with two Jackson-Prattdrains was done. Pressure dressing was applied atthe repaired flap area. She was referred to Psychiatryfor evaluation of body image. The patient wasdischarged after 4 days (Figure 9).
Postoperative histopathologic examination of thetissue revealed Squamous cell carcinoma, well tomoderately differentiated with 7cm in greatestdiameter of tumor size. There were also tumor in theleft parotid gland, external ear, middle ear, cervicallymph nodes (Figure 10). The left submandibular gland,
Figure 5. (a) Resection of the external ear, (b) Posteriorportion shows tumor cells invading the periauricular area
Figure 6. (c) Excision of the parotid gland including themandibular condylewith malignant soft tissue invasion.(d) Radical neck dissection (SCM, EJV, SAN, cervical LN I-V)including the left submandibular gland

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 73
Figure 7. Resection defect measuring 8.6cm x 9.6cm.
Figure 8. Estimation of flap and tunneling of the pectoralismajor flap over the skin of the supraclavicular region
Figure 9. 4th post operative day, recepient site
concha, mandibular condyle, external jugular vein andspinal accessory nerve were negative of tumor. At 1week follow-up, removal of sutures from the flap siteand donor site was done, the patient remainedasymptomatic, there were no signs of flap necrosis orcontracted wound. She was referred to Oncologyservice(s) for postoperative chemotherapy andradiotherapy.
DISCUSSION
Malignant tumors of the external auditory canal,middle ear and temporal bone are rare, accountingfor less that 2% of all tumors of the head and neck.6,7,11
Squamous cell carcinoma is the most common type oftumor in the external auditory canal, middle ear andtemporal bone. These tumors pose major challengesto the clinician in terms of diagnosis, staging andmanagement due to anatomic location and other vitalstructures in proximity.2 The incidence of SCCmalignancy of the temporal bone is higher in womenthan in men, approximately 1:1,000,000 and0.8:1,000,000 respectively per year. Though it affectsall ages, the peak incidence is during the seventhdecade.2 To date, the exact cause of temporal bonecarcinoma remains unclear. A number of risk factorshave been proposed however they are still difficultto assess due to the rarity of the disease. Humanpapilloma virus (HPV) has also been isolated in thetemporal bone but its exact role is still unclear.Tobacco use and alcohol consumption can alsocontribute as it is the most common risk factor forall squamous cell carcinoma of the head and neck;others inc lude choles tea toma, chlor inateddisinfectant and ultraviolet light (UVB), but all thisare still subject to further studies.
While there is a lack of data for optimal tumortreatment, Koppany et al correlates higher treatmentsuccess and survival rate for the early diagnosis ofthe disease. Squamous cell carcinoma of the temporalbone initially presents with non specific symptomsincluding ear discharge and otalgia which are mostcommon.2,6 Due to the lack of specific clinicalmanifestations, diagnosis and detection of thismalignancy is difficult.2 Many otolaryngologists wouldoften misdiagnose the patient specially in its earlystages. The similarity of ear infections like otitisexterna and chronic suppurative otitis media contributeto the misdiagnosis. Due to the complex anatomy ofthis tumor the pattern of spread is difficult to predict.

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201774
Figure 10.(a) normal squamous keratinize epithelial cells(b) well-differentiated squamous cell carcinoma, characterized by sheets of individual cell(c) keratinization, and keratin pearl formation.(c) large cells with pleomorphic, hyperchromatic nuclei.
Tumors usually originate from the skin around theauricle may extend along the soft tissues of the neckand temporal bone. In this patient’s presentation, theexternal ear and auricle remained to be intact and freefrom lesions. Additionally, chronic and recurringinfections thought to proceed tumor development leadto decreased follow-up motivation resulting intofurther delay in diagnosis. Examination of the ear canreveal an exophytic or polypoidal mass that can beulcerated or with granulation.2 Cranial nerve deficitsare always a late sign of tumor spread and leads tofacial spasms and palsies. Endoscopy of thenasopharynx and larynx is indicated for thosesuspected of having a malignancy in the head andneck. Cervical lymphadenopathy must be assessed asit has major implications for the patients prognosis.2,5,11
Similarly in the present case, the patient experienced
a 3 month history of otalgia with associated otorrheaand was treated as an infection however topical andsystemic antibiotic were not effective. A brownishrubbery mass was later seen thru otoscopy that bleedsupon suctioning. Facial palsy was not present in thepatient at the time of surgery.
As with any other tumors, histological confirmationof the primary lesions is still the gold standard for thediagnosis of this malignancy.1,2 Biopsy of the palpablelymph nodes is also indicated for aiding tumor stagingand treatment planning. Computed Tomography (CT)has been established as the initial diagnostic imagingof choice as it is a reliable demonstrator of bonyerosions of the external auditory canal and temporalbone, often the first sign of local spread of the disease.However there may be difficulty in differentiating fluidand inflamed mucosa from tumor in the middle ear

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 2017 75
and mastoid distinguishing inflammation from tumorwhere there is no adjacent bony erosion anddetermining the anterior soft tissue extension on thetumor.2,3,6 Tissue biopsy of the aural mass in this patientalready established. Squamous cell carcinoma andextensions to the external auditory canal seen usingComputed Tomography of the temporal bone fourweeks prior to surgery.
In one case from Arriaga, et al. CT failed to detectthe spread of tumor through the anterior canal wallthat occurred without bony erosion. Tumor can spreadanteriorly via the cartilagenous fissures of Santoriniand the bony foramen of Huschke without evidenceof erosion. These can result inunderestimation of the extent of the disease in theinfratemporal fossa, the mastoid cavity and the carotidcanal. Magnetic resonance imaging can becomplimentary to Computed Tomography by offeringadditional information on the soft tissue extent.2,3,6,10
This malignancy of the temporal bone is uncommonand leads to few studies and literature. Without anyuniversally accepted staging system, Arriaga et alsuggested a staging system in the 1990, which hassince entered the literature as the Pittsburgh StagingSystem. The system allows staging, treatment planningand evaluation outcomes. T1 tumors are those thatare limited to the external auditory canal without anybony erosion or evidence of soft tissue extension. T2are classified as tumors limited within the externalauditory canal with bony erosion (not full thickness)and/or radiographic finding consistent with less than0.5cm soft tissue involvement. T3 are tumors erodingthe osseous external auditory canal (full thinkness)with less than 0.5cm soft tissue involvement, or tumorsinvolving the middle ear and/or mastoid, or patientswith facial nerve involvement. T4 are those that havetumor eroding the cochlea, petrous apex, medial wallof the middle ear, carotid canal, jugular foramen anddura, or with more than 0.5cm soft tissue involvement.Both lymph node (N1) and metastasis (M1) areconsidered very poor prognostic signs.1-3,5,11,13 Tumorstaging and anatomical extent were the primary factorsinfluencing the prognosis.8
Temporal bone malignancies should always bemanaged by a multidisciplinary team. The options aresurgical resection, radiotherapy with or withoutchemotherapy or a combination of both.1,10,13 Theframework for surgical planning are identification ofthe sites and subsites of tumor growth and saferesection of margins; careful assessment of potentialhidden tumor diffusion is also taken into account. The
goal of the surgery is to eliminate disease and achievea negative margin to minimize morbidity andmortality. Complete tumor resection (lateral boneresection) with en bloc excision has remained to bethe preferred initial treatment modality.1,3,7,8,10,13,15 Theen bloc excision includes removal of the cartilaginousand bony canal along with the tympanic membrane,periauricular soft tissues, the parotid gland (with orwithout facial nerve reservation), and neck nodesI-V1,8,10,13,15, mandibular condyle is also excised toprevent osteoradionecrosis when the patient is subjectto postoperative radiotherapy.3 The surgicalmanagement will always leave a sizeable defect andthe patient would nonetheless undergo a flapreconstruction. Free tissue transfer is the goldstandard in modern reconstruction. The patient had a8.6cm x 9.6cm notable defect on the left auriculararea which was repaired using pectoralis majormyocutaneous flap. The patient was preoperativleycategorized as stage 2 using the Pittsburgh stagingsystem with the support of computed tomographyresults. Intraoperative findings however suggest thatthe middle ear was also affected with extensions tothe mastoid, epitympanum and facial nerve.Histopathologic tissue results were also postive forthe parotid glands and one out of thirteen cervicallymph nodes. The patient instead was correctlycategorized as stage 4 and was referred to oncologyservices. All patients are recommended to receiveradiotherapy after surgery to both the primary site andipsilateral neck. This increases the overall survival ratecompared to radiotherapy alone.1,10 However someliterature suggested that radiotherapy is only indicatedfor those in advanced stages (T3-T4).13 Synchronouschemotherapy has shown to enhance the effect ofradiotherapy.2 In some studies chemotherapy did notimprove survival rates but only yielded better paincontrol.1 Chemotherapy is not routinely used norrecommended because distant metastasis areinfrequent in this kind of tumors.10 It is only reservedfor cases with residual diseases, unresectable T4tumors and M stage diseases.1
CONCLUSION
The presented case of a 39 year old female diagnosedwith Temporal bone Squamous Cell Carcinoma, leftear, emphasized the need for early diagnosis, properaggressive surgical intervention and postoperativeradiotherapy with possible chemotherapy. The true

Far Eastern University - Dr. Nicanor Reyes Medical Foundation Medical Journal, Vol. 23, No. 2 - July - December 201776
condition must be recognized clinically as early aspossible if presented with otorrhea and otalgia withaural mass that does not regress in size nor relievethe symptoms despite continuous otic and oralantibiotics. Early suspicion of malignancy indicatesfurther work-up either with tissue biopsy or ComputedTomography to prevent unnecessary spread of tumorand preoperative planning. Squamous cell carcinomais known to be an aggressive type of tumor, a delay indiagnosis and surgical intervention would likely affectthe patient prognosis. The primary treatment modalityis lateral bone resection with en bloc excision followedby a flap reconstruction of the initial defect.Radiotherapy after resection of tumor is indicated notonly for advanced stages but for T1 tumors.Chemotherapy is recommended only for patients withresidual disease, unresectable tumors and those withdistant metastasis. There is an increased 5 yearsurvival rate for patients with T1-T2 undergoing lateralbone resection with postoperative radiotherapy whilethere is still 50% 5 year survival rates for those patientwith T3 tumors given the same management and T4tumors yield a poorer prognosis.
REFERENCES
1. Lavielle JP, Delande C, Kunst H, Deveze A, Magnan J,Schmerber S. Management of carcinoma of the temporalbone. Mediterr J Otol 2005; 2: 00-00.
2. Sethi N, Michalopoulos K, Bajaj Y, Sood S, Khan MI.Squamous cell of the temporal bone. TheOtorhinolaryngologist 2011; 3(3): 104-10.
3. Gillespie MB, Francis HW, Chee N, Eisele DW. Squamouscell carcinoma of the temporal bone:a radiographic-pathologiccorrelation. Arch Otolaryngol Head Neck Surg 2001;127:803-7.
4. Rahaman W, Sheikh R, Mohammed H, Dogan ZA. Squamouscell carcinoma of the external ear in child. DOI.ORG.10.4236.IJOHNS.2015.45057
5. Visnyei K, Gill R, Azizi E, Culliney B. Squamous cellcarcinoma of the external auditory canal: A case report andreview of the literature. DOI: 10.3892/ol.2013.1241
6. Zhen S, Fu T, Qi J. Diagnosis and treatment of carcinoma inexternal auditory canal. DOI.ORG,10.1016,J. JOTO.2014.12.004
7. Martinez-Devesa, Barnes ML, Milford CA. Malignanttumors of the ear and temporal bone: A study of 27 patientsand review of their management, DOI 10.1055/s-2007-992766.
8. Mazzoni A, Zanoletti E, Marioni G, Martini A. En bloctemporal bone resections in squamous cell carcinoma of theear. Technique, principle and limits. Acta Oto-Laryngologica136(5): 425-32.
9. Nam SJ, Yang CJ, Chung JW. A case of squamous cellcarcinoma in the external auditory canal previously treatedfor verrucous carcinoma. J Audiol Otol 2016; 20(3): 183-6.
10. Ogawa K, Nakamura K, Hatano K, et al. Treatment andprognosis of squamous cell carcinom of the external auditorycanal and middle ear: a multi-institutional retrospectivereview of 87 patients. DOI:10.1016,J.Ijrobp.2007.01.052
11. Boamah H, Knight G, Taylor J, Palka K, Ballard B.Squamous cell carcinoma of the external auditory canal: acase report. DOI:10.1155,2011,615210
12. House JW, Brackmann DE. Facial nerve grading system.Otolaryngol Head Neck Surg 1985; 93146
13. A. Mazzoni, G. Danesi, E. Zanoletti. Primary squamouscell carcinoma of the external auditory canal: surgicaltreatment and long-term outcomes. Acto Oto-LaryngologicaIta 2014; 34: 129-37.
14. Zhang B, Tu G, Xu G. Squamous cell carcinoma of temporalbone: reported on 33 patients. Otolaryngol Head Neck Surg1999 8; 21(5): 461-6.
15. Kunst H, Lavieille JP, Marres H. Squamous cell carcinomaof the temporal bone: results and management. Otol Neurotol2008; 29(4): 549-52.