Embed Size (px)
Citation preview

Fall Service Models -Lessions learned from the FARSEEING project
Jorunn L Helbostad Research group on Geriatrics, Movement and Stroke Department of Neuroscience, Faculty of Medicine,
Norwegian University of Science and Technology, Trondheim Norway, and St. Olav University Hospital, Trondheim Norway,

Acknowledgements
• NTNU – Ather Nawaz – Espen Ihlen – Alan Bourke – Per Bendik Wik – Arnhild Jenssen Nygård
• Municipality of Trondheim
– Kirsti Fossland Brørs – Klara Borgen – Lise Høiberg Knipeberg
• Sintef – Babak Farshchian – Yngve Dahl – Thomas Vilarinho
• University of Bologna
– Lorenzo Chiari – Sabato Mellone
• Rest of the FARSEEING
consortium
• Technology
• Service model – a description of a service
and the components required to deliver that service
• Service
– Implementation of the service model in practice
Service model
Technology

4
Health enabling technology and services
• The tools must be reliable
• The services must be reliable
• The services must meet the requirements for real life use
• New systems should build on the existing health care systems, health information systems, and information management systems
– Ludwig et al. 2012

5
Factors complicating implementation of falls service models in practice
• The technology is still immature or not feasible for older persons
• Lack of agreements and standards for technological platforms
• Failure to take into account the interests of important stakeholders – Patients, care providers, health care organizations, health care
personnel, policy makers, next of kin, government, suppliers

Falls and falls prevention

7
The FARSEEING telemedicine service models
• Fall detection and management – Give immediate and qualified help to older people
following a fall
• Fall risk assessment (proof of concept) – Detect fall risk earlier – Improve decision making for clinicians
• Exercice guidance (proof of concept)
– Increase uptake of interventions – Empower older people to mange own health and
function

Falls and falls prevention

9
Why fall detection and management services?
• Nearly half of those who fall need help
to get up from the floor – Not being able to get up after a fall
increases fear of falling
• 10 % stay on the ground >1 hour • poor prognosis if >12 hours on the
ground

Norway • Low population density
• 2050
– 20% of the population will be >67 years of age
• 2060
– Decrease in number of empolyees per retired person from 5 to 2.5
• Home care services constitute 1/3
of the municipal activity and costs Proportion of people living i areas with low and high population density

TRONDHEIM, NORWAY
• 172 000 inhabitants – 10% >67 years of age
• Public health care system
• Low population density
• Well developed primary
health care system – Home nursing – Public safety alarm service

12
Users of safety alarm services in Norway
Sintef report, 2012
0
20
40
60
80
100
50-66 yrs 67-79 yrs 80-89 yrs 90 yrs and older
Percentage
Reasons for using alarm services • Increased fall risk • Anxiety • Heart disease

13
Today’s safety alarm service in Trondheim
• 3780 safety alarm users
• 83 employees in the safety alarm service
• Use of push button-activated alarms
• ~12 000 activated alarms every month
• ~ 10% of the activated alarms lead to a physical visit

Today’s safety alarm service Trondheim, Norway
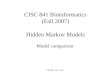
Push-button pendent safety alarm systems and services Pro • Robust technology • Established service • Same service for different
needs
Cons • The alarm only works
indoor • Alarm buttons are not
always worn • The users do not activate
the alarm • Requires a conscious
decision by the user • Dependent on analogue
telephone lines

Existing fall alarm service (Trondheim)
IO1: The user fails to activate the alarm IO2: The user fails to provide status about his condition after activating the alarm IO3: Response time

17
The FARSEEING automatic fall detection system and service model • User centered design
• Take important stakeholders into account
• Develop reliable algorithms for fall detection
• Develop/use technological platforms that can be reused and that can interoperate with other platforms

18
The FARSEEING fall detection and management service model

19
The FARSEEING service model adapted to a residential care setting

The FARSEEING automatic fall detection system

21
Field testing of the FARSEEING service model Aim: Assess experiences with implementing the model Sample • 20 end-users
– Age: 28-103 yrs, mean: 82.5 yrs – Living in residential care facilities – 8 had fallen the past year – All were considered to be at risk of falling – All were users of the today’s alarm service
• 10 care-providers
Assessment • Log books and logs from the server • Weekly follow-up meetings • Focus interviews with care-providers and end-users • Number of elicited alarms


23
Number of falls and triggered alarms • 20 people monitored over 4 weeks
– ~500 monitored days
• 7 falls by 4 people
– 0.42 fall per monitoring month
• Activated alarms
– 1 true positive – 6 falls not detected – 3 false alarms

24
Results Form factor and ergonomics – End-users
• Wearability • Aestetics • Self management
– Care-providers
• Devises that are strapped on are preferable (e.g. watch)
• Devises should be visible

25
Results System feedback and user control • End-users
– Want confirmation that the alarm has been received – Need a system that works in- and outdoor – Want to have the possibility to stop the alarm – Feasibility is more important than safety
• Care-providers – Inappropriate feedback increases anxiety for the end-user – Feedback to end-users should be individualised – False alarms are burdensome for carers and end-users – The end-user’s safety is most important

26
Lessions learned…… • ICT enables moving interventions closer to the users
– Empowering people to take care of own health requires new services
• User privacy – Sharing of data collected in free-living situations raise new challenges
• Introduction of new services raise new ethical questions
• Technology usability and form factors – Feasible to wear over 24 hours a day – Easy to use – Reliable!
• Holistic models vs. fragmented technologies and services – Same technologies and platforms for different purposes – Services than can be used by the same users over time

http://farseeingresearch.eu/ http://profound.eu.com/
Falling can be risky!
Thank you for the attention!

The user centred design process
ISO standard 9241-210