Embed Size (px)
Citation preview

Faculty Highlights | 1

Dean of the School of PharmacyDr. Mohamad Rahal
SOP Newsletter Editor–in-ChiefDr. Dalal Hammoudi
Contributors to this issue (In alphabetical order)
FacultyDr. Sahar Abou RidaDr. Nour ChamsineDr. Michelle CherfanDr. Nermine ChoumaneDr. Hadi DassoukiDr. Sahar HaydarDr. Razan MhannaDr. Bouchra MouhtadiDr. Nisreen MouradDr. Sylvia SaadeDr. Samar Younes
StudentsRawane BarakatIqbal Fahs
Graphic DesignerHiba Haj Omar
Letters to the editor, questions, comments, and requests should be kindly addressed to:
Dr. Dalal Hammoudi, RPh, MSc, PhDSchool of Pharmacy;Lebanese International UniversityBekaa Campus, Khyara, LebanonTel: 961 8 640930/1/2; Ext [email protected]
About the School of PharmacyOne of the highly ranked private schools of pharmacy nationwide, the Lebanese International University School of Pharmacy maintains an elegant reputa-tion for innovative educational programs and skillful training through both degrees it offers, the BPharm and PharmD. Over the past few years the School has strived establish a structure which enables our graduates to become an added quality to the healthcare system.
The School focuses on clinical pharmacy, community outreach, and training on the optimal use of medication therapy through didactic as well as clerkship/internship courses. Today, our School is acknowledged by private, public, and international institutions.
Our graduates attain high success rate in the national pharmacy examination (colloquium), and are highly recognized by national and international pharmaceutical companies.
The SOP Newsletter, published tri-annually, delivers drug and health information news from the School’s Faculty members and highlights some of the School’s events.
© 2016 BY THE LEBANESE INTERNATIONAL UNIVERSITY SCHOOL OF PHARMACY

EDITOR’S NOTEDear Readers,According to the American Journal of Pharmaceutical Education, successful recruitment and development of pharmacy faculty members is essential now more than ever. Such task is achievable through a number of activities, including continuing professional development, peer evaluation, seminars, teaching and learning workshops, preceptor skill improvement, research, as well as written communications. Several studies have also recognized the impact of pharmacy newsletters, both among community and hospital pharmacists. These periodicals serve as an effective means of communication, for keeping abreast of pharmaceutical advances, and for “life-long” learning process within the pharmacy profession.
While the School of Pharmacy at the Lebanese International University strives to promote pharmacy education and mentor competent pharmacy graduates, SOP Newsletter was established to aid in providing information to the School teaching community and students. The purpose of our publication, since the first issue in April 2013, was to highlight new knowledge that fosters the appropriate use of drugs and improves patient outcomes at individual and societal level. Through variety of information presented, focus is on the enduring role of the pharmacist, as the specialized drug consultant to the physician, and the advisor to the public on multiple health issues.
In the following pages, I invite you to share some of new pharmacy advances and research pointed out by our faculty. Beside these, a group of events through which the School communicates with the broad pharmacy sectors and seeks community outreach, is described in the SOP Newsletter. It also features a calendar of upcoming events that will be soon tackled by the School.
The SOP Newsletter is still on the start, but definitely improving with your suggestions and comments as well as your participation. Enjoy reading the Spring 2016 issue!
Dalal Hammoudi, PhDAssistant Professor and ChairSOP Newsletter Editor-in-Chief
IN THIS ISSUE EDITORIAL NOTE
4 SOP PARTICIPATION IN 75TH FIP CONGRESS
6 OSIMERTINIB: NEW DRUG OF THE MONTH
8 UPDATES IN CARDIOVASCULAR DISEASE
10 A NEW CLINICAL TOOL FOR CROHN’S DISEASE
11 MEPOLIZUMAB: A NEW MEDICATION FOR ASTHMA
13 PEDIATRIC ANEMIA IN LEBANON
15 ANTIBIOTIC UPDATES
16 PATIROMER: A NEW TREATMENT FOR HYPERKALEMIA
24 STUDENTS CORNER
27 SAINT JUDE FUNDRAISING CAMPAIGN
28 CONTINUING EDUCATION SESSIONS
29 55TH ICAAC VISIT TO NEW OPL PRESIDENT
30 SOP GALA DINNERS
32 PHARMACY UNION ACTIVITIES
33 18TH CONGRESS OF SCIENTIFIC ASSOCIATION OF COLLEGES OF PHARMACY IN THE ARAB WORLD
34 23RD OPL CONGRESS
35 PRESIDENT’S AND DEAN’S LISTS
36 50TH ASHP SOP SOCIAL LIFE
UPCOMING EVENTS

4 SOP Newsletter | February 2016 | 5
SOP PARTICIPATES IN 75TH
ANNUAL FIP CONGRESS AT DUSSELDORF, GERMANYThe School of Pharmacy at the Lebanese International University is a member of the International Phar-maceutical Federation Academic Institutional Membership (FIP AIM). Represented by the Dean, Dr. Mo-hamad Rahal, and Dr. Marwan Akel, the School participated in the FIP 75th World Congress of Pharmacy and Pharmaceutical Sciences, from September 29th till October 3rd, 2015, in Dusseldorf, Germany. Over 3,000 pharmacists and pharmaceutical scientists from 111 countries attended the congress, the theme of which was “Better practice — science based, evidence driven”.
In this premier international pharmacy event, ex-perts from around the globe meet, learn, share and exchange views. A varied and rich program was featured in the congress, addressing prob-lems and achievements of the pharmacy profes-sion via lectures, plenary sessions, poster exhibi-tions and leadership meetings.
Like each year at the FIP World Congress of Phar-macy and Pharmaceutical Sciences, the FIP AIM hosted a Deans’ Forum, inviting all representative deans from the membership to meet each other and discuss current and relevant topics in an in-ternational arena. Dr. Rahal participated in this year’s forum, entitled “Integrating science and practice into the pharmacy/pharmaceutical edu-cation”. AIM members, deans and academic lead-ers discussed, debated and shared how pharmacy and pharmaceutical sciences education institu-tions are transforming their programs towards achieving better health.
During the forum, inter-professional education, leadership in pharmacy, and integration of research within education and practice were discussed. Academic issues were highlighted in round tables and recommendations were drawn. Moreover, quality assurance of pharmacy education made the theme of a dynamic international workshop. Dr. Rahal communicated his experience and expectations through different sessions of the forum. The strategic planning for the future focused on coordination between AIM members, including exchange of faculty and organization of regular meetings and webinars.
As part of the academic/community scientific sessions of the congress, Dr. Marwan Akel delivered an oral presentation discussing the findings of his study: “An overview of kidney stone disease in Lebanon”.
Dr. Akel also represented LIU in the “FIP working group on pharmacists’ role in harm reduction”. The objectives of this group are to collect available ev-idence for the role and impact of pharmacists and their associations in harm reduction programs on national and regional levels, and to support phar-macists involvement in such activities.
Most of the sessions where interactive, and al-lowed participants to exchange and expose their ideas in their fields of expertise. Moreover, field visits to international pharmaceutical companies and sections’ dinners were organized. The social side, meeting with fellows and friends from differ-ent pharmacy sectors, complemented the diverse congress program.
Faculty Highlights | 7 6 SOP Newsletter | February 2016
Moreover, for patients with swallowing problems, the tablet can be placed in a container with 50 ml of non-carbonated water and stirred till dis-persed, and then drank or administered through a naso-gastric tube.
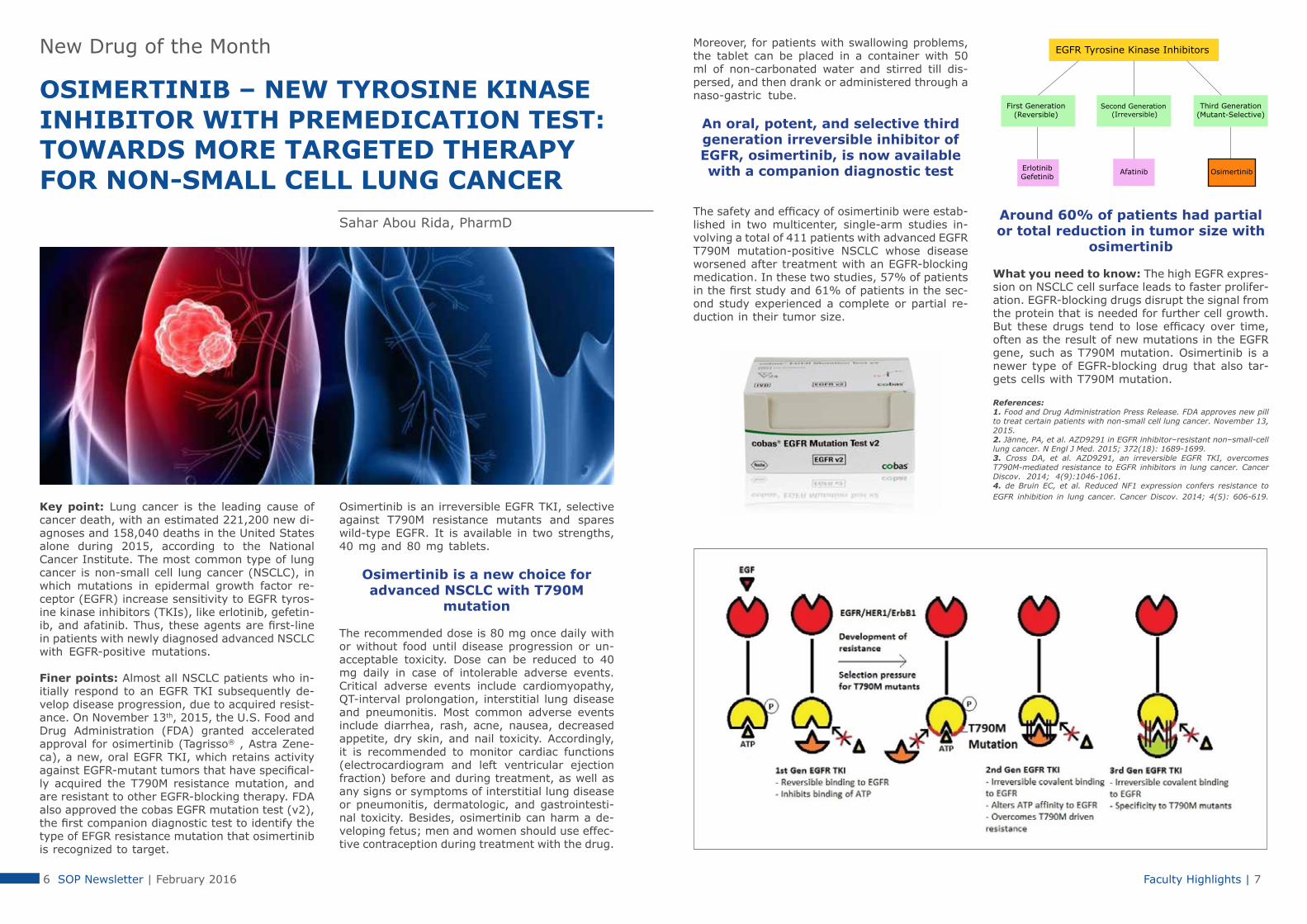
An oral, potent, and selective third generation irreversible inhibitor of EGFR, osimertinib, is now available with a companion diagnostic test
The safety and efficacy of osimertinib were estab-lished in two multicenter, single-arm studies in-volving a total of 411 patients with advanced EGFR T790M mutation-positive NSCLC whose disease worsened after treatment with an EGFR-blocking medication. In these two studies, 57% of patients in the first study and 61% of patients in the sec-ond study experienced a complete or partial re-duction in their tumor size.
Around 60% of patients had partial or total reduction in tumor size with
osimertinib
What you need to know: The high EGFR expres-sion on NSCLC cell surface leads to faster prolifer-ation. EGFR-blocking drugs disrupt the signal from the protein that is needed for further cell growth. But these drugs tend to lose efficacy over time, often as the result of new mutations in the EGFR gene, such as T790M mutation. Osimertinib is a newer type of EGFR-blocking drug that also tar-gets cells with T790M mutation.
References: 1. Food and Drug Administration Press Release. FDA approves new pill to treat certain patients with non-small cell lung cancer. November 13, 2015.2. Jänne, PA, et al. AZD9291 in EGFR inhibitor–resistant non–small-cell lung cancer. N Engl J Med. 2015; 372(18): 1689-1699.3. Cross DA, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014; 4(9):1046-1061.4. de Bruin EC, et al. Reduced NF1 expression confers resistance to EGFR inhibition in lung cancer. Cancer Discov. 2014; 4(5): 606-619.
New Drug of the Month
OSIMERTINIB – NEW TYROSINE KINASE INHIBITOR WITH PREMEDICATION TEST: TOWARDS MORE TARGETED THERAPY FOR NON-SMALL CELL LUNG CANCER
Sahar Abou Rida, PharmD
Key point: Lung cancer is the leading cause of cancer death, with an estimated 221,200 new di-agnoses and 158,040 deaths in the United States alone during 2015, according to the National Cancer Institute. The most common type of lung cancer is non-small cell lung cancer (NSCLC), in which mutations in epidermal growth factor re-ceptor (EGFR) increase sensitivity to EGFR tyros-ine kinase inhibitors (TKIs), like erlotinib, gefetin-ib, and afatinib. Thus, these agents are first-line in patients with newly diagnosed advanced NSCLC with EGFR-positive mutations.
Finer points: Almost all NSCLC patients who in-itially respond to an EGFR TKI subsequently de-velop disease progression, due to acquired resist-ance. On November 13th, 2015, the U.S. Food and Drug Administration (FDA) granted accelerated approval for osimertinib (Tagrisso® , Astra Zene-ca), a new, oral EGFR TKI, which retains activity against EGFR-mutant tumors that have specifical-ly acquired the T790M resistance mutation, and are resistant to other EGFR-blocking therapy. FDA also approved the cobas EGFR mutation test (v2), the first companion diagnostic test to identify the type of EFGR resistance mutation that osimertinib is recognized to target.
Osimertinib is an irreversible EGFR TKI, selective against T790M resistance mutants and spares wild-type EGFR. It is available in two strengths, 40 mg and 80 mg tablets.
Osimertinib is a new choice for advanced NSCLC with T790M
mutation
The recommended dose is 80 mg once daily with or without food until disease progression or un-acceptable toxicity. Dose can be reduced to 40 mg daily in case of intolerable adverse events. Critical adverse events include cardiomyopathy, QT-interval prolongation, interstitial lung disease and pneumonitis. Most common adverse events include diarrhea, rash, acne, nausea, decreased appetite, dry skin, and nail toxicity. Accordingly, it is recommended to monitor cardiac functions (electrocardiogram and left ventricular ejection fraction) before and during treatment, as well as any signs or symptoms of interstitial lung disease or pneumonitis, dermatologic, and gastrointesti-nal toxicity. Besides, osimertinib can harm a de-veloping fetus; men and women should use effec-tive contraception during treatment with the drug.
Faculty Highlights | 9 8 SOP Newsletter | February 2016
WILL ANDEXANET ALFA BE THE FIRST REVERSAL AGENT FOR RIVAROXABAN AND APIXABAN? Sahar Haydar, PharmDKey point: Over the past decade, rivaroxaban, apixaban, and endoxaban have emerged as orally active, di-rect factor Xa inhibitors. They are indicated for stroke prophylaxis in patients with nonvalvular atrial fibrillation, treatment and prevention of deep vein thrombosis and pulmonary embolism, and the prevention of venous thrombosis after orthopedic surgery. Unlike bleeding caused by warfarin, which can be reversed using low-dose vitamin K1, there is no available agent to reverse bleeding or stop anticoagulant effects of oral factor Xa inhibitors.
Andexanet alfa reverses bleeding due to factor Xa inhibitors minutes after injection and without serious adverse effects
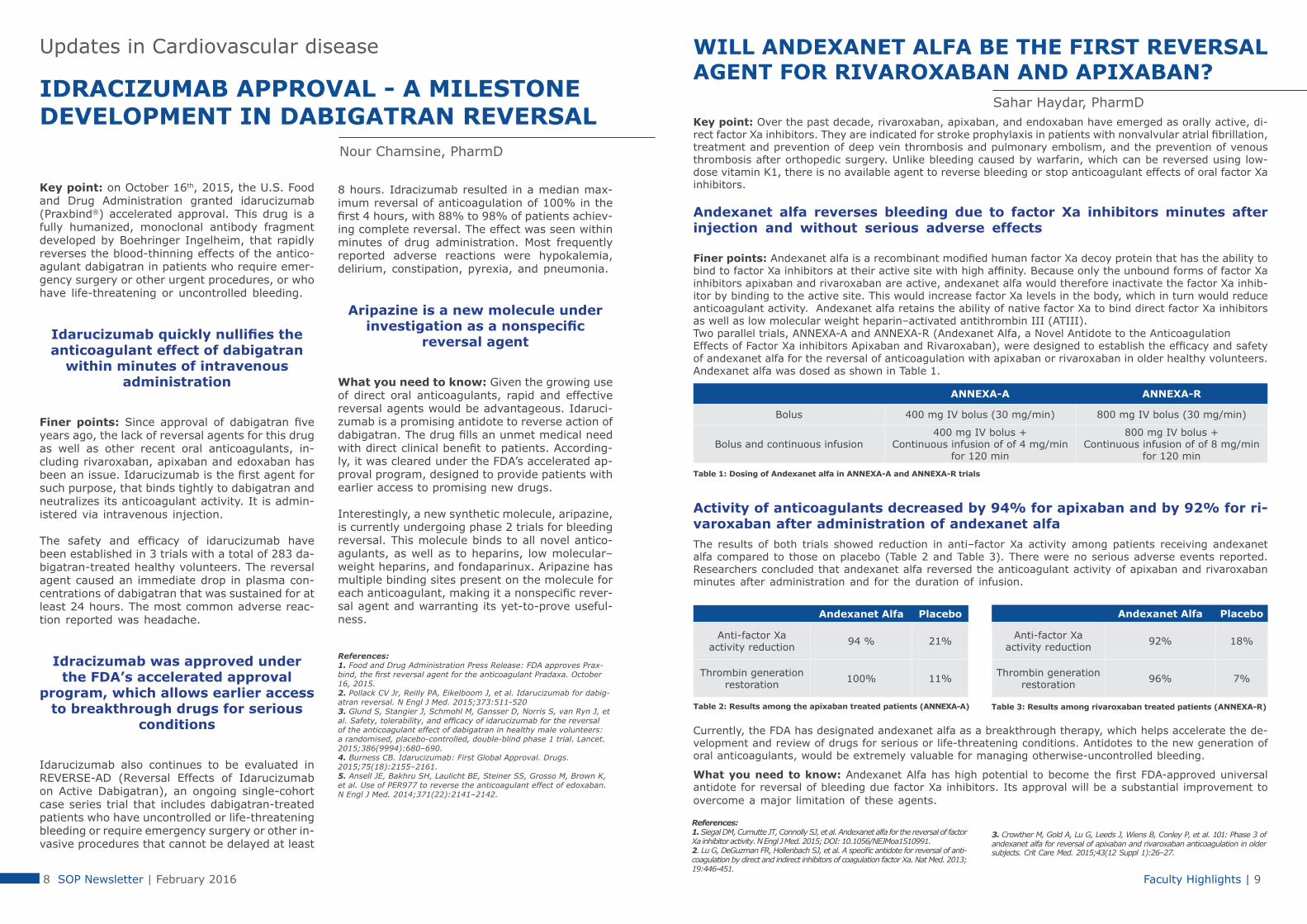
Finer points: Andexanet alfa is a recombinant modified human factor Xa decoy protein that has the ability to bind to factor Xa inhibitors at their active site with high affinity. Because only the unbound forms of factor Xa inhibitors apixaban and rivaroxaban are active, andexanet alfa would therefore inactivate the factor Xa inhib-itor by binding to the active site. This would increase factor Xa levels in the body, which in turn would reduce anticoagulant activity. Andexanet alfa retains the ability of native factor Xa to bind direct factor Xa inhibitors as well as low molecular weight heparin–activated antithrombin III (ATIII).Two parallel trials, ANNEXA-A and ANNEXA-R (Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of Factor Xa inhibitors Apixaban and Rivaroxaban), were designed to establish the efficacy and safety of andexanet alfa for the reversal of anticoagulation with apixaban or rivaroxaban in older healthy volunteers. Andexanet alfa was dosed as shown in Table 1.
ANNEXA-A ANNEXA-R
Bolus 400 mg IV bolus (30 mg/min) 800 mg IV bolus (30 mg/min)
Bolus and continuous infusion400 mg IV bolus +
Continuous infusion of of 4 mg/min for 120 min
800 mg IV bolus +Continuous infusion of of 8 mg/min
for 120 min
Table 1: Dosing of Andexanet alfa in ANNEXA-A and ANNEXA-R trials
Activity of anticoagulants decreased by 94% for apixaban and by 92% for ri-varoxaban after administration of andexanet alfaThe results of both trials showed reduction in anti–factor Xa activity among patients receiving andexanet alfa compared to those on placebo (Table 2 and Table 3). There were no serious adverse events reported. Researchers concluded that andexanet alfa reversed the anticoagulant activity of apixaban and rivaroxaban minutes after administration and for the duration of infusion.
Andexanet Alfa Placebo
Anti-factor Xa activity reduction 94 % 21%
Thrombin generation restoration 100% 11%
Table 2: Results among the apixaban treated patients (ANNEXA-A)
Currently, the FDA has designated andexanet alfa as a breakthrough therapy, which helps accelerate the de-velopment and review of drugs for serious or life-threatening conditions. Antidotes to the new generation of oral anticoagulants, would be extremely valuable for managing otherwise-uncontrolled bleeding.
What you need to know: Andexanet Alfa has high potential to become the first FDA-approved universal antidote for reversal of bleeding due factor Xa inhibitors. Its approval will be a substantial improvement to overcome a major limitation of these agents.
Andexanet Alfa Placebo
Anti-factor Xa activity reduction 92% 18%
Thrombin generation restoration 96% 7%
Table 3: Results among rivaroxaban treated patients (ANNEXA-R)
References:1. Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity. N Engl J Med. 2015; DOI: 10.1056/NEJMoa1510991.2. Lu G, DeGuzman FR, Hollenbach SJ, et al. A specific antidote for reversal of anti-coagulation by direct and indirect inhibitors of coagulation factor Xa. Nat Med. 2013; 19:446-451.
3. Crowther M, Gold A, Lu G, Leeds J, Wiens B, Conley P, et al. 101: Phase 3 of andexanet alfa for reversal of apixaban and rivaroxaban anticoagulation in older subjects. Crit Care Med. 2015;43(12 Suppl 1):26–27.
Updates in Cardiovascular disease
IDRACIZUMAB APPROVAL - A MILESTONE DEVELOPMENT IN DABIGATRAN REVERSAL Nour Chamsine, PharmD
Key point: on October 16th, 2015, the U.S. Food and Drug Administration granted idarucizumab (Praxbind®) accelerated approval. This drug is a fully humanized, monoclonal antibody fragment developed by Boehringer Ingelheim, that rapidly reverses the blood-thinning effects of the antico-agulant dabigatran in patients who require emer-gency surgery or other urgent procedures, or who have life-threatening or uncontrolled bleeding.
Idarucizumab quickly nullifies the anticoagulant effect of dabigatran
within minutes of intravenous administration
Finer points: Since approval of dabigatran five years ago, the lack of reversal agents for this drug as well as other recent oral anticoagulants, in-cluding rivaroxaban, apixaban and edoxaban has been an issue. Idarucizumab is the first agent for such purpose, that binds tightly to dabigatran and neutralizes its anticoagulant activity. It is admin-istered via intravenous injection.
The safety and efficacy of idarucizumab have been established in 3 trials with a total of 283 da-bigatran-treated healthy volunteers. The reversal agent caused an immediate drop in plasma con-centrations of dabigatran that was sustained for at least 24 hours. The most common adverse reac-tion reported was headache.
Idracizumab was approved under the FDA’s accelerated approval
program, which allows earlier access to breakthrough drugs for serious
conditions
Idarucizumab also continues to be evaluated in REVERSE-AD (Reversal Effects of Idarucizumab on Active Dabigatran), an ongoing single-cohort case series trial that includes dabigatran-treated patients who have uncontrolled or life-threatening bleeding or require emergency surgery or other in-vasive procedures that cannot be delayed at least
8 hours. Idracizumab resulted in a median max-imum reversal of anticoagulation of 100% in the first 4 hours, with 88% to 98% of patients achiev-ing complete reversal. The effect was seen within minutes of drug administration. Most frequently reported adverse reactions were hypokalemia, delirium, constipation, pyrexia, and pneumonia.
Aripazine is a new molecule under investigation as a nonspecific
reversal agent
What you need to know: Given the growing use of direct oral anticoagulants, rapid and effective reversal agents would be advantageous. Idaruci-zumab is a promising antidote to reverse action of dabigatran. The drug fills an unmet medical need with direct clinical benefit to patients. According-ly, it was cleared under the FDA’s accelerated ap-proval program, designed to provide patients with earlier access to promising new drugs.
Interestingly, a new synthetic molecule, aripazine, is currently undergoing phase 2 trials for bleeding reversal. This molecule binds to all novel antico-agulants, as well as to heparins, low molecular– weight heparins, and fondaparinux. Aripazine has multiple binding sites present on the molecule for each anticoagulant, making it a nonspecific rever-sal agent and warranting its yet-to-prove useful-ness.
References:1. Food and Drug Administration Press Release: FDA approves Prax-bind, the first reversal agent for the anticoagulant Pradaxa. October 16, 2015.2. Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumab for dabig-atran reversal. N Engl J Med. 2015;373:511-5203. Glund S, Stangier J, Schmohl M, Gansser D, Norris S, van Ryn J, et al. Safety, tolerability, and efficacy of idarucizumab for the reversal of the anticoagulant effect of dabigatran in healthy male volunteers: a randomised, placebo-controlled, double-blind phase 1 trial. Lancet. 2015;386(9994):680–690. 4. Burness CB. Idarucizumab: First Global Approval. Drugs. 2015;75(18):2155–2161. 5. Ansell JE, Bakhru SH, Laulicht BE, Steiner SS, Grosso M, Brown K, et al. Use of PER977 to reverse the anticoagulant effect of edoxaban. N Engl J Med. 2014;371(22):2141–2142.

Faculty Highlights | 11 10 SOP Newsletter | February 2016
In low risk patients who do not achieve remission, recommendations include an assessment of drug levels for immunosuppressive therapy, with consideration given to an anti-TNF therapy. For moderate- to-high risk patients not in remission, treatment options were similar to those recommended as initial therapy. The decision tool also suggests treatment recommendations for patients in remission for both low risk and moderate/high risk patients.
The AGA noted that this tool is only a starting point, as there is a future opportunity to create tools that focus on both treating the underlying disease and providing psychosocial care to the patient. Moreover, they noted that with the recent push towards providing better value in health care, future tools should include quality indicators and cost utility analyses to better help select therapies that provide value to patients and to society. In patients receiving treatments such as azathioprine, steroids, methotrexate, and/or anti-TNF, extensive education should be provided about their proper and safe use.
What you need to know: A new Crohn’s disease clinical decision support tool was released by the AGA to help clinicians assess and stratify patients and determine effective therapies for disease management based on evidence-based treatment recommendations. It is available at: http://campaigns.gastro.org/algorithms/IBDCarePathway/.
Reference:Sandborn WJ. Crohn’s disease evaluation and treatment: clinical decision tool. Gastroenterology 2014;147: 702–05.
FDA-APPROVES MEPOLIZUMAB FOR PATIENTS WITH SEVERE ASTHMA
Updates in Respiratory Disorders
Sylvia Saade, PharmD
Key point: The World Health Organization esti-mates that over 235 million people live with asth-ma worldwide. For many of these patients, ex-isting therapies can provide adequate symptom control if used appropriately. However, approxi-mately 5% of patients with severe asthma cannot achieve symptom control with existing therapies. On the 4th of November, 2015, the FDA approved mepolizumab (Nucala®), a humanized monoclonal antibody, as add-on maintenance treatment for patients with severe asthma aged 12 years and older, and with an eosinophilic phenotype.
Finer points: Severe asthma is defined as “asth-ma which requires treatment with high dose in-
haled corticosteroids (ICS) plus a second control-ler (and/or systemic corticosteroids) to prevent it from becoming ‘uncontrolled’, or which remains ‘uncontrolled’ despite this therapy”. Severe asth-ma patients are also often categorized by long-term use of oral corticosteroids (OCS). In a subset of severe asthma patients, the over-production of eosinophils is known to correlate with severity and frequency of exacerbations. Interleukin-5 (IL-5) is the major cytokine responsible for growth, differ-entiation, recruitment, activation, and survival of eosinophils. Mepolizumab is a humanized IL-5 an-tagonist produced in Chinese hamster ovary cells, and it reduces the production and survival of eo-sinophils by inhibiting IL-5 signaling.
Updates in Gastroenterology
A NEW TOOL FOR IDENTIFICATION, ASSESSMENT, AND INITIAL MANAGEMENT OF CROHN’S DISEASE
Key point: The treatment of Crohn’s disease is in evolution. Historically, patients were treated based on clinical symptoms. In recent years, it was understood that symptomatic response and remission alone are insufficient to ensure that underlying inflammation has resolved. More recently, data support the use of both symptomatic remission and endoscopic remission as treatment goals for patients with the disease.
Finer points: To help clinicians better assess and treat patients with Crohn’s disease, the American Gastroenterological Assocaiation (AGA) released a clinical decision support tool in September, 2014. This tool was created using a rigorous review process and is based on current evidence and AGA’s practice guideline for the management of Crohn’s disease. This tool incorporates assessments for inflammatory status, comorbidities, and disease- and therapy-related complications, as well as treatment recommen-dations based on patient risk and remission status.
According to the decision tool, patients should be classified as low risk or moderate-to-high risk, with treatments assigned according to risk status.
Low risk patients Moderate-to-high risk patients
• Age at initial diagnosis > 30 years • Limited anatomic involvement • No perianal and/or severe rectal disease • Superficial ulcers • No prior surgical resection • No stricturing and/or penetrating behavior
• Age at initial diagnosis < 30 years • Extensive anatomic involvement • Perianal and/or severe rectal disease • Deep ulcers • Prior surgical resection • Stricturing and/or penetrating behavior
Treatment options have also evolved based on evidence from controlled trials. Treatment options were modified from mesalamine and antibiotics for low-risk patients and steroids, azathioprine, and metho-trexate for moderate-to-severe disease, to budesonide, steroids and azathioprine for low-risk patients, and biologic therapy with tumor necrosis factor (TNF) antagonists (ideally in combination with azathi-oprine) and integrin antagonists for high-risk patients. Therapeutic drug monitoring is applied to help guide decision making in patients treated with biologic agents who lose response.
Initial treatment includes the following:
Low risk patients
Ileum and/or proximal colon — none to minimal systemic symptoms• Budesonide 9 mg per day with or without azathioprine• Tapering course of prednisone with or without azathioprine Diffuse or left colon — none to minimal systemic symptoms• Tapering course of prednisone with or without azathioprine
Moderate-to-high risk patients
Moderately severe Crohn’s disease• Use anti-TNF monotherapy over no therapy or thiopurine monotherapy• Use anti-TNF + thiopurine over thiopurine monotherapy or anti-TNF monotherapy• Use methotrexate for patients who do not tolerate purine analog in combination with anti-TNF• Combination therapy with an immunosuppres- sant and an anti-TNF should be considered for patients requiring a 2nd or 3rd biologic agent
Michelle Cherfan, PharmD, MSc

Faculty Highlights | 13 12 SOP Newsletter | February 2016
PREVALENCE AND RISK FACTORS OF PEDIATRIC IRON DEFICIENCY ANEMIA IN LEBANON
Updates in Pediatrics
Razan Mhanna, PharmD
What you need to know: For patients with severe asthma aged 12 years and older, and with an eo-sinophilic phenotype, mepolizumab is the first anti-IL-5 treatment. It is administered as 100 mg every four weeks by SC injection in upper arm, thigh or abdomen. Mepolizumab is not approved for use in patients with other eosinophilic conditions or for emergency treatment of acute bronchospasm or status asthmaticus, but is being investigated in eosinophilic chronic obstructive pulmonary disease (COPD) and eosinophilic granulomatosis with polyangiitis (EGPA).
References:1. Food and Drug Administration Press Release. FDA approves Nucala to treat severe asthma. November 4, 2015.2. Ortega HG, Liu MC, Pavord ID, Brusselle GC, FitzGerald JM, Chetta A, Humbert M, Katz LE, Keene ON, Yancey SW, and Chanez P. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014; 371:1198-1207.3. Ortega H, Chupp G, Bardin P, Bourdin A, Garcia G, Hartley B, Yancey S, Humbert M. The role of mepolizumab in atopic and nonatopic severe asth-ma with persistent eosinophilia. Eur Respir J. 2014; 44: (1) 239-241.4. Pavord ID, Kom S, Howarth P, Bleecker ER, Buhl R, Kene ON, Ortega H, Chanez P. Mepolizumab for severe eosinophilic asthma (DREAM): a mul-ticentre, double-blind, placebo-controlled trial. Lancet. 2012; 380, 9842: 651-659.
The safety and efficacy of mepolizumab were es-tablished based on data from three clinical stud-ies: A phase II 52-week dose-ranging and exac-erbation-reduction trial in subjects with asthma with a history of two or more exacerbations in the previous year despite regular use of high-dose ICS plus an additional controller(s) with or with-out OCS; and two Phase III confirmatory trials (MENSA and SIRIUS trials). Mepolizumab was ad-ministered every 4 weeks in all 3 trials as add-on to background treatment. All subjects continued their background asthma therapy throughout the duration of the trials.
A total of 711 subjects with asthma were studied in the 2 confirmatory trials. They were required to have blood eosinophils of greater than or equal to 150 cells/mcL at screening (within 6 weeks of dosing), or blood eosinophils of greater than or equal to 300 cells/mcL within 12 months of en-rollment.
Mepolizumab is a humanized IL-5 antagonist which reduces the
production and survival of eosinophils by inhibiting IL-5 signaling
The MENSA (Mepolizumab as adjunctive therapy in patients with severe asthma) study was a 32-week double-blind, double-dummy, placebo-con-trolled, parallel group multicentre study that ran-domized and treated 576 patients with severe asthma, who had experienced frequent exacerba-tions despite treatment with high dose ICS plus at least one other controller medication. Patients were randomized to receive either mepolizumab
75 mg intravenous (IV), 100 mg subcutaneous (SC), or placebo every four weeks.
For the primary endpoint of reduction in exacer-bations, defined as worsening of asthma requiring use of systemic corticosteroids and/or hospitaliza-tion, both mepolizumab treatment arms showed a statistically significant reduction in frequency of clinically significant asthma exacerbations com-pared to placebo (75 mg IV, 47%, P<0.001; 100 mg SC, 53%, P<0.001). For endpoints of lung function, time to first exacerbation, quality of life, and asthma control, both mepolizumab arms generated improvement across all measures com-pared to placebo.
In addition, a second phase III study, SIRIUS (Steroid Reduction with Mepolizumab Study), was a 24-week double-blind, placebo-controlled, par-allel group multicentre study designed to evalu-ate mepolizumab 100 mg SC, every 4 weeks in comparison to placebo in reducing daily OCS use while maintaining asthma control. Results showed that patients on mepolizumab 100 mg SC were able to achieve a 50% median overall reduction from baseline in their maintenance OCS dose dur-ing weeks 20-24 compared to 0% with placebo (P =0.007), while maintaining asthma control. Pa-tients receiving mepolizumab also reported a sig-nificant improvement in their asthma control and their quality of life. Patients receiving mepolizum-ab also had a significant reduction (P<0.001) in their eosinophil count throughout the duration of the study.
Mepolizumab treatment decreases asthma exacerbations, improves quality
of life and produces better asthma control
In both studies, most common adverse events were headache, nasopharyngitis, bronchitis, si-nusitis, fatigue and asthma. Injection site reac-tions (pain, redness, swelling, itching, or burning) were higher in the mepolizumab groups.
Faculty Highlights | 15 14 SOP Newsletter | February 2016
Antibiotic UpdatesNEW METAL ANTIMICROBIALS CAN BE EFFECTIVE AGAINST RESISTANT BACTERIA Key point: Although current infection rates are declining, invasive methicillin-resistant Staphylo-coccus aureus (MRSA) infections are responsible for increasing mortality. However, new research has uncovered a new group of antibiotics with sig-nificant antimicrobial activity against both S. au-reus and MRSA.
Finer points: According to a recent study, the potential new antibiotics are unlike contemporary antibiotics because they contain iridium, a sil-very-white transition metal. New transition met-al complexes do not easily breakdown, rendering them important for delivery of antibiotics to the sites where they are needed to fight infection.
In mice models, the incorporation of iridium with antimicrobials results in direct toxicity on bacteria and
lowers doses of antibiotics needed
Silver is proposed to alter cellular processes that keep bacteria alive, such as metabolism, internal iron levels, and ability to form bonds between vital proteins. Researchers also found that silver works to increase the amounts of oxygen present in bac-teria – which often cannot handle high levels of oxygen and thus will be killed. Moreover, in a tox-icity measurement performed on mice up to 48 hours after treatment, it was noted that levels of silver in the blood did not persist for more than two days, and did not cause any adverse effects
on kidneys or liver. Only low concentrations of sil-ver were needed to get antibiotics to work effec-tively.
The addition of silver can also reduce the amount of antibiotics; in fact, adding a small amount of silver corresponded to a two-fold decrease in anti-biotic dose needed to eradicate the infection. This is likely because the silver makes the antibiotic’s role easier; it simply needs to kill bacteria after silver weakens them.
What you need to know: The uses of silver in addition to antibiotics are quite promising. Noth-ing has yet been established about role in hu-mans, but the study concluded that the release of these silver-complexed antimicrobials at the site of infection could prove very useful.
Reference: Karpin GW, Morris DM, et al. Transition metal diamine complexes with antimicrobial activity against Staphylococcus aureus and methicillin-re-sistant Staphylococcus aureus (MRSA). Med Chem Commun. 2015;6: 1471-1478.
Nermine Choumane, PharmD
Key point: Iron deficiency (ID) the most com-mon single nutritional deficiency worldwide, and iron deficiency anemia (IDA) in infancy remains of great concern, due to its damaging effects on infant growth, cognition, and behavioral as well as neural development.
Finer points: In preterm infants, term infants and preschoolers (1-3 years), iron demand is particularly high, so deficiency occurs when the stores are exhausted and tissue supply is compro-mised. According to the American Academy of Pe-diatrics (AAP), ID prevalence is 4% for 6 months infants, 12% for 12 months infants, and ranges between 6.6-15.2% among children 1-3 years old. The WHO global database on anemia estimates a prevalence of 46.6% among preschoolers in East-ern Mediterranean region, which is much higher than that estimated in America (29.3%) and Eu-rope (21.7%). In areas geographically close to Lebanon, prevalence varies from 20% to 67%.
Developmental defects, lowerintelligence quotient, abnormal
motor and socio-emotional function, and altered behavioral and neural growth are only some
of the consequences of iron deficiency in infants
According to American Family Physician, ID risk groups include: premature babies or those with low birth weight, babies with early introduction of cow milk (before one year of age), exclusively breastfed or regular formula-fed babies not re-ceiving iron fortification (above six months of age) and children who have special needs (with chronic infections or restricted diets). Iron deficient tod-dlers not only have a lower mean developmental quotient at initial testing, but also have a lower intelligence quotient in adolescence, abnormal motor and socio-emotional function, as well as al-tered behavioral and neural development and re-ports of cerebral thrombosis.
Among studied Lebanese infants, incidence of iron deficiency
anemia was moderate
A study, recently published in the International Journal of Pharmacy Practice, was undertaken by the School of Pharmacy at the Lebanese Interna-tional University, to investigate the incidence and
risk factors of pediatric IDA. The study was a six-month, prospective, multicenter, cross-sectional survey involving pediatrics departments of three Lebanese hospitals. Preterm to term infants aged 6 to 24 months were included; infants with blood disorders, chronic infections, congenital immuno-deficiency and mental or congenital growth retar-dation were excluded.
Key associated risk factors were prolonged exclusive breastfeeding,
low income, rural residency, mothers’ low education, and
inadequate iron supplementation in both infants and mothers
Among 520 screened infants, a total of 100 pa-tients were selected. Thirty-seven percent of pa-tients were anemic, with hemoglobin levels <11g/dL. Significant risk factors for IDA were: exclu-sive breastfeeding for more than 6 months (95% confidence interval [CI], 1.03-8.9; P=0.043), low family income (95% CI, 0.19-0.98; P= 0.045), ru-ral residency (95% CI, 0.0509-0.064; P<0.001), inadequate maternal iron supply (95% CI, 1.01-8.26; P=0.05), low maternal education level (95% CI, 0.07-0.88; P=0.03), and lack of infant iron supply (95% CI, 1.39-8.41; P=0.007).
What you need to know: The AAP recommends 1mg/kg/day of oral iron supplementation at 4 months of age for breastfed infants until comple-mentary foods are introduced. Universal screen-ing for hemoglobin or hematocrit, once between 9 and 12 months and again between 15 and 18 months, is also recommended in populations with high prevalence of IDA. In Lebanon, with moder-ate incidence of IDA and multiple contributing fac-tors, screening measures as well as raising IDA awareness among families should be considered.
References:1. Baker R, and Greer F. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics. 2010; 126: 1040-1050. 2. The global prevalence of anemia in 2011. World Health Organization. 3. Mhanna R, Rahal M, Iskandarani M and Hammoudi D. Incidence and risk factors associated with iron deficiency anemia among hospitalized Lebanese infants. Int J Pharm Pract. 2015;doi:10.1111/ijpp.12236.
Faculty Highlights | 17 16 SOP Newsletter | February 2016
Updates in PsychiatryDO INCREASED TELEVISION VIEWING AND LOW PHYSICAL ACTIVITY AFFECT THE COGNITIVE FUNCTION OF YOUNG ADULTS?
Key point: Physical inactivity and sedentary lifestyle are emerging trends worldwide, and may lead to accelerated aging, numerous diseases, and an overall decline in the quality of life. Television watching has been linked not only to increased cardiovascular risk factors, but also to other behavioral patterns, including social inactivity and poor diet.
Finer points: To determine the effect of high television viewing and low physical activity on cognition, young adults aged 18-30 years, from four US cities were enrolled in the Coronary Artery Risk Develop-ment in Young Adults (CARDIA) study. The study was prospective and carried out from March 25th, 1985, to August 31st, 2011. A total of 3247 participants completed the study.
The participants were followed through visits every 2- 5 years over a period of 25 years. Physical activity was assessed using the Physical Activity History Questionnaire at each visit. Low physical activity was characterized by having a level of activity less than sex-specific baseline quartile for more than two-thirds of the visits. Television watching was assessed by asking participants about the number of hours they spent watching television during a day. A high television viewing was characterized by spending 3 or more hours per day watching TV for more than two-thirds of the visits. Three tests were done at the 25th year: the Digit Symbol Substitution Test (DSST), to assess processing speed and executive function; the Stroop test, to assess executive function; and the Rey Auditory Verbal Learning Test (RAVLT), to as-sess verbal memory. Results are shown in the table below:
(%) Poor Cognitive Performance TV Viewing PatternTest
14.3Low to moderate TV viewingDSST
27.4High TV viewing
12Low to moderate TV viewingStroop test
21.4High TV viewing
19.1Low to moderate TV viewingRAVLT
27.1High TV viewing
Bouchra Mouhtadi, PharmD
Patiromer is made in powder form consisting of smooth, spherical beads. It is mixed with 90 mL of water and taken once daily with food. It is not absorbed and acts within the gastrointestinal tract by binding to potassium in exchange for calci-um, primarily in the colon. The potassium is then excreted from the body through the normal ex-cretion process. Patiromer should not be used as an emergency treatment for life-threatening hyper-kalemia because of its delayed onset of action.
In the clinical trials, most adverse reactions were mild to moderate in intensity, including constipation, hypomagnesemia, diarrhea, nausea, abdominal dis-comfort, and flatulence. Patiromer can bind to many other orally administered medications, which could decrease their absorption and reduce their effec-
tiveness; therefore, a boxed warning recommends taking it and any other orally administered medica-tion at least six hours apart.What you need to know: Patiromer is the first new medication for the treatment of hyperkalemia in more than 50 years. It will provide doctors and patients with a new option for daily treatment of hyperkalemia, and may be chronically used to keep potassium levels in the target range.
References:1. Food and Drug Administration Press Release. FDA approves new drug to treat hyperkalemia. October 21, 2015.2. Weir MR, Bakris GL, Bushinksy DA, et al. Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors. N Engl J Med. 2015;372:21-221.3. Bakris GL, Pitt B, Weir MR, et al. Effect of patiromer on serum potas-sium level in patients with hyperkalemia and diabetic kidney disease: The AMETHYST-DN randomized clini cal trial. JAMA. 2015;314(2):151-161.
PATIROMER: A NEW MEDICINE FOR HYPERKALEMIA TREATMENT SINCE MORE THAN 50 YEARS
Updates in Metabolic Disorders
Samar Younes, PharmD
Key point: On October 21st, 2015, the U.S. Food and Drug Administration (FDA) approved pati-romer (Veltassa®, Relypsa Inc. California), a non-absorbable potassium binder, for the treatment of hyperkalemia.
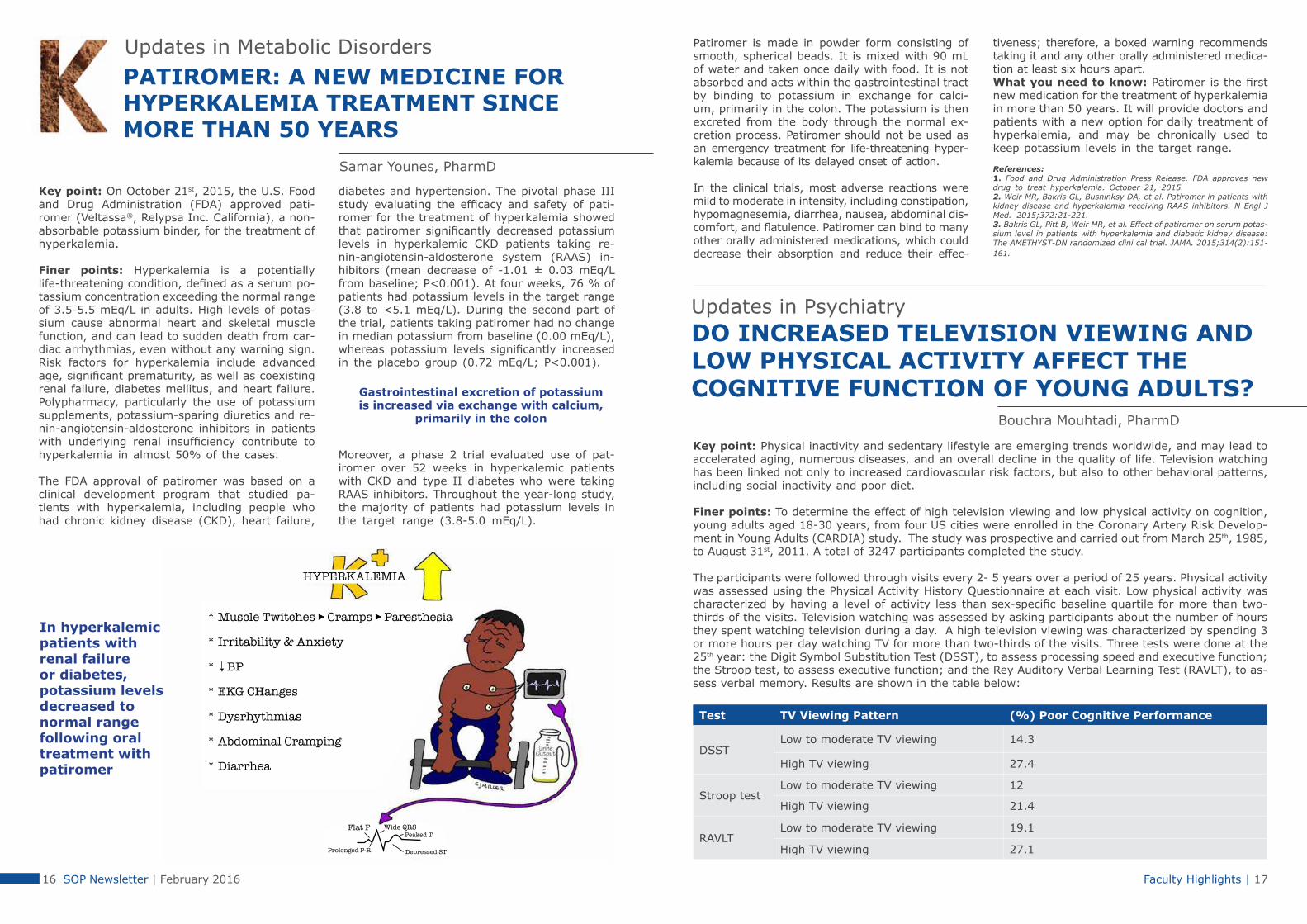
Finer points: Hyperkalemia is a potentially life-threatening condition, defined as a serum po-tassium concentration exceeding the normal range of 3.5-5.5 mEq/L in adults. High levels of potas-sium cause abnormal heart and skeletal muscle function, and can lead to sudden death from car-diac arrhythmias, even without any warning sign. Risk factors for hyperkalemia include advanced age, significant prematurity, as well as coexisting renal failure, diabetes mellitus, and heart failure. Polypharmacy, particularly the use of potassium supplements, potassium-sparing diuretics and re-nin-angiotensin-aldosterone inhibitors in patients with underlying renal insufficiency contribute to hyperkalemia in almost 50% of the cases.
The FDA approval of patiromer was based on a clinical development program that studied pa-tients with hyperkalemia, including people who had chronic kidney disease (CKD), heart failure,
diabetes and hypertension. The pivotal phase III study evaluating the efficacy and safety of pati-romer for the treatment of hyperkalemia showed that patiromer significantly decreased potassium levels in hyperkalemic CKD patients taking re-nin-angiotensin-aldosterone system (RAAS) in-hibitors (mean decrease of -1.01 ± 0.03 mEq/L from baseline; P<0.001). At four weeks, 76 % of patients had potassium levels in the target range (3.8 to <5.1 mEq/L). During the second part of the trial, patients taking patiromer had no change in median potassium from baseline (0.00 mEq/L), whereas potassium levels significantly increased in the placebo group (0.72 mEq/L; P<0.001).
Moreover, a phase 2 trial evaluated use of pat-iromer over 52 weeks in hyperkalemic patients with CKD and type II diabetes who were taking RAAS inhibitors. Throughout the year-long study, the majority of patients had potassium levels in the target range (3.8-5.0 mEq/L).
Gastrointestinal excretion of potassium is increased via exchange with calcium,
primarily in the colon
In hyperkalemic patients with renal failure or diabetes, potassium levels decreased to normal range following oral treatment with patiromer

Faculty Highlights | 19 18 SOP Newsletter | February 2016
A MINIMALLY INVASIVE LIQUID BIOPSY FOR CANCER DETECTION
Key point: Conventional means of cancer diag-nosis can involve numerous types of scans and in-vasive methods like surgical biopsies, but a new method of identifying the disease may involve nothing more than a simple prick of a finger.
Finer points: In recent years, it was discovered that platelets take up protein and RNA molecules from cancer tumors and may have a role in tumor growth and metastasis. Hence, the researchers at the Umea University in Sweden in collaborations with researchers from the Netherlands and the United States aimed to investigate whether RNA from tumors carried in platelets could be used to identify and classify common cancer types.
According to the study published in Cancer Cell, investigators developed a new RNA test of blood platelets that can detect, classify and determine the location of cancer in the body by analyzing a blood sample equivalent in size to just a single drop of blood. Blood samples from 283 individu-als were studied of which 228 patients had some form of cancer and 55 showed no evidence of can-cer. By comparing the blood samples RNA profiles,
researchers could identify the presence of cancer with 96% accuracy and the type of cancer with 71% accuracy in organs like the lungs, pancreas, brain, liver, and colon. In 39 patients where can-cer had been detected early, they were able to identify and classify the cancer with 100% accura-cy. The test is based on the discovery that cancer tumors “educate” blood platelets by altering the platelets’ RNA profile. Thus, analyzing the mRNA profiles of tumor-educated platelets provides di-agnostic information about the tumor’s type and location.
What you need to know: While the technique is not perfect, the results show that blood platelets could constitute a complete and easily accessible blood-based source for sampling. If further trials validate this “ liquid biopsy”, the test promises to be used for blood-based cancer diagnosis, treat-ment and monitoring.
Reference:Myron G. Best, Nik Sol, Irsan Kooi, et al. RNA-Seq of Tumor-Educated Platelets Enables Blood-Based Pan-Cancer, Multiclass, and Molecular Pathway Cancer Diagnostics. Cancer Cell. 2015; 28 (5): 666-676.
Interesting News
Nermine Choumane, PharmD
The results for DSST and STROOP test were signif-icant. After adjustment for age, race, sex, smok-ing, educational level, alcohol use, body mass in-dex, and hypertension the results of the RAVLT test were not significant.
Watching television for 3 hours or more a day in young adulthood,
coupled with low levels of physical activity, may lead to
poorer cognitive function
Individuals with low physical activity were 47% more probable to do poorly on the DSST than those with moderate-high physical activity. In combination, individuals with low physical activity and high TV viewing were almost twice as likely to perform poorly on the STROOP test and DSST than those with high physical activity and low TV watching.
What you need to know: High levels of televi-sion viewing might lead to poorer cognitive per-formance in midlife. The study adds evidence to the growing consensus that there is a link be-tween lifestyle factors and cognitive aging. An active lifestyle is important for keeping the brain healthy, even for young and middle-aged adults.
References: 1. Hoang T, Reis J, Zhu N, Jacobs D, Launer L, Whitmer R, et al. Effect of early adult patterns of physical activity and television viewing on midlife cognitive function. JAMA Psychiatry. 2015;2; doi: 10.1001/jamapsychiatry.2015.12236.2. Warren T, Barry V, Hooker S, Sui X, Church T, & Blair S. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010; 42(5): 879-885.
An active lifestyle is important for keeping the brain healthy, even for young and middle-aged adults

Faculty Highlights | 21 20 SOP Newsletter | February 2016
According to recent research, it is suggested that the best bee’s honey is made by Apis mellifera, and its overall composition differs according to the flowers on which the bee feeds. Although honey contains about 200 substances, its general chemical composition is as follows:
Average composition of honey (Nutritional value per 100 g)
Component Average content
CarbohydratesFructoseGlucoseSucroseOther SugarsDietary Fiber
82.4 g38.5 g31 g1 g11.7 g0.2 g
Fat 0 g
Protein 0.3 g
Water 17.1 g
Vitamins Riboflavin (Vitamin B2)Niacin (Vitamin B3)Pantothenic acid (Vitamin B5)Pyridoxine (Vitamin B6)Folate (Vitamin B9)Vitamin C
0.038 mg0.121 mg0.068 mg0.024 mg0.002 mg0.5 mg
MineralsCalciumIronMagnesiumPhosphorusPotassiumSodiumZinc
6 mg0.42 mg2 mg4 mg52 mg4 mg0.22 mg
Since Stone Age, honey has been an important source of carbohydrates and a widely available sweeten-er. However, with time its use expanded from a nutritional supplement to further treat several ailments. When it comes to the traditional uses of honey, several civilizations employed it mostly for the treatment of wounds and diseases of the gut. Of notice are the following:
Civilization Most common uses of honey
Ancient India
- Benefits those with weak digestion- Treats irritating cough, eye diseases, insomnia, skin disorders, anemia, cardiac pain and palpitation- Keeps the teeth and gums healthy - Prevents cataract
Ancient Egypt - Treats wounds
Ancient Greece
- Treats gout and certain nervous disorders- Hippocrates prescribed it: o To treat pain, acute fevers, thirst, baldness, wounds, constipation, cough, sore throat and eye diseases o To prevent and treat scars o As topical antiseptic and contraceptive
Arabs
- Prophet Muhammad (peace be upon him) recommended the use of honey for the treatment of diarrhea - Avicenna used it as a remedy for tuberculosis
HONEY: AN EXTRAORDINARY THERAPY WITHIN EVERYONE’S REACH
Alternative Medicine Corner
Nisreen Mourad, PharmD
Whether it is called “َعَســل” in Arabic, honey in English or miel in French and Spanish, they all refer to one of the most prized and treasured natural products that has been widely used throughout history for its therapeutic effects. In fact, honey has had a valued place in traditional medicine for centuries, where the first written reference to its use was on a Sumerian tablet going back to 2000-2100 BC, then later it was used by Ancient Egyptians, Chinese, Greeks, Romans and Arabs till today.

Faculty Highlights | 23 22 SOP Newsletter | February 2016
THE PHARMACIST ROLE IS CHANGING TO HELP BETTER MAINTAIN YOUR HEALTH
TALK TO YOUR PHARMACIST!THIS IS A CROSSWOD PUZZLE ADDRESSING MAJOR INFORMATION PATIENTS SHOULD CONSULT ABOUT WITH THIER PHARMACISTAcross:1. Tell your pharmacist about any of these supplements you are taking so they can help you prevent drug interactions4. Besides your community pharmacy, pharmacists also work here to help patients5. Your pharmacist can help you determine if you are at risk to develop this chronic condition, and help you manage it if you do8. Pharmacists raise this in the community towards drugs and diseases10. Ask your pharmacist to help you discover the best therapy for these common complaints that can cause itchy eyes, a runny nose and sneezing11. Regular amounts of this activity improves your general health, increases energy and decreases stress13. You don’t need one of these to visit your pharmacist15. This type of disease is one of the leading causes of death for men and women16. Wash these often to avoid spreading germs, colds and flu17. Your pharmacist can work with this other health care provider to make sure you’re taking the right medications Down:2. Keep that new year’s resolution! Your pharmacist can give you some good tips on how to quit this habit3. Don’t throw it out! Bring this type of unused medication to your local pharmacy for safe disposal6. You can get this from your pharmacist if you are interested in learning about non-prescription products7. All pharmacists are interested in helping patients stay ________9. Some pharmacists do this type of work to help discover new medications12. Many pharmacists can give you one of these to help protect you against flu14. You can come here anytime to ask questions about your health or pick up your prescriptions
Answers
1. Vitamins2. Smoking3. Expired4. Hospital5. Diabetes6. Advice7. Healthy8. Awareness9. Research10. Allergies11. Exercise12. Vaccine13. Appointment14. Pharmacy15. Heart16. Hands17. Doctor
As science progressed, laboratory and clinical investigations on honey proved its role in mod-ern medicine as well. Currently, honey is known to act both as bacteriostatic and bactericidal to about 60 species of aerobes and anaerobes, gram-positive and gram-negative bacteria in-cluding Pseudomonas aeruginosa, Acinetobacter spp., Helicobacter pylori and community-associ-ated Methicillin-resistant Staphylococcus aureus (MRSA). In contrary to conventional antibiotics, honey is not associated with resistance and can be used continuously. In addition to its antibac-terial effects, honey has antifungal properties on some species of Aspergillus, Candida albicans, dermatophytes and Penicillium, as well as antivi-ral effects on herpes, rotavirus and rubella virus. Furthermore, honey has anti-inflammatory effects (reducing the activities of both cyclooxygenase-1 and -2, and inhibiting TNF-α), antioxidant proper-ties (with remark that the darker the honey, the higher its antioxidant capacity) and finally antileu-kemic and anticarcinogenic activities against var-ious cancer cell line and tissues, such as breast, colorectal, renal, prostate, endometrial, cervical and oral cancer.
Because of all of these properties, a branch of al-ternative medicine called “Apitherapy” has been recently developed, offering therapies based on
honey. In fact, nowadays honey is most common-ly used for wound healing, treatment of various dermatologic diseases (such as eczema, psoriasis and dandruff), ophthalmological conditions (such as keratitis, conjunctivitis and corneal injuries) and gastrointestinal infections (such as gastri-tis, duodenitis and gastric ulceration). In diabe-tes, honey is known to stimulate insulin secretion thus reducing glucose levels while elevating the hemoglobin concentration and improving the lipid profile, consequently reducing cardiovascular risk factors. Indeed, many compounds in honey have promising effects in the treatment of various car-diovascular diseases.
With such varied biological and pharmacological properties, honey has proved to be a remarka-ble natural substance with diverse uses, and, no doubt, other unseen effects that are yet to be dis-covered, warranting further experimentation.
References: 1. Eteraf-Oskouei T, Najafi M. Traditional and modern uses of natural honey in human diseases: A review. Iran J Basic Med Sci. 2013; 16: 731-742.2. Ahmed S, Othman NH. Honey as a potential natural anticancer agent: A review of its mechanisms. Evid Based Complement Alternat Med. 2013; article ID 829070.3. Ediriweera ER, Premarathna NY. Medicinal and cosmetic uses of bee’s honey-A review. Ayu 2012; 33 (2): 178-182.4. Bogdanov S, Jurendic T, Sieber R, Gallmann P. Honey for nutrition and health: A review. Am J College Nutr. 2008; 27: 677–689.
Hadi Dassouki, RPh, MSc
Students Corner | 25 24 SOP Newsletter | February 2016
UPDATES TO THE GUIDELINES OF ANTIRETROVIRAL AGENTS IN HIV-1-INFECTED ADULTS AND ADOLESCENTS
Rawane Barakat, PharmD Candidate
ROLE OF PHARMACISTS IN IMPROVING ADHERENCE IN ACS PATIENTS Iqbal Fahs, PharmD Candidate
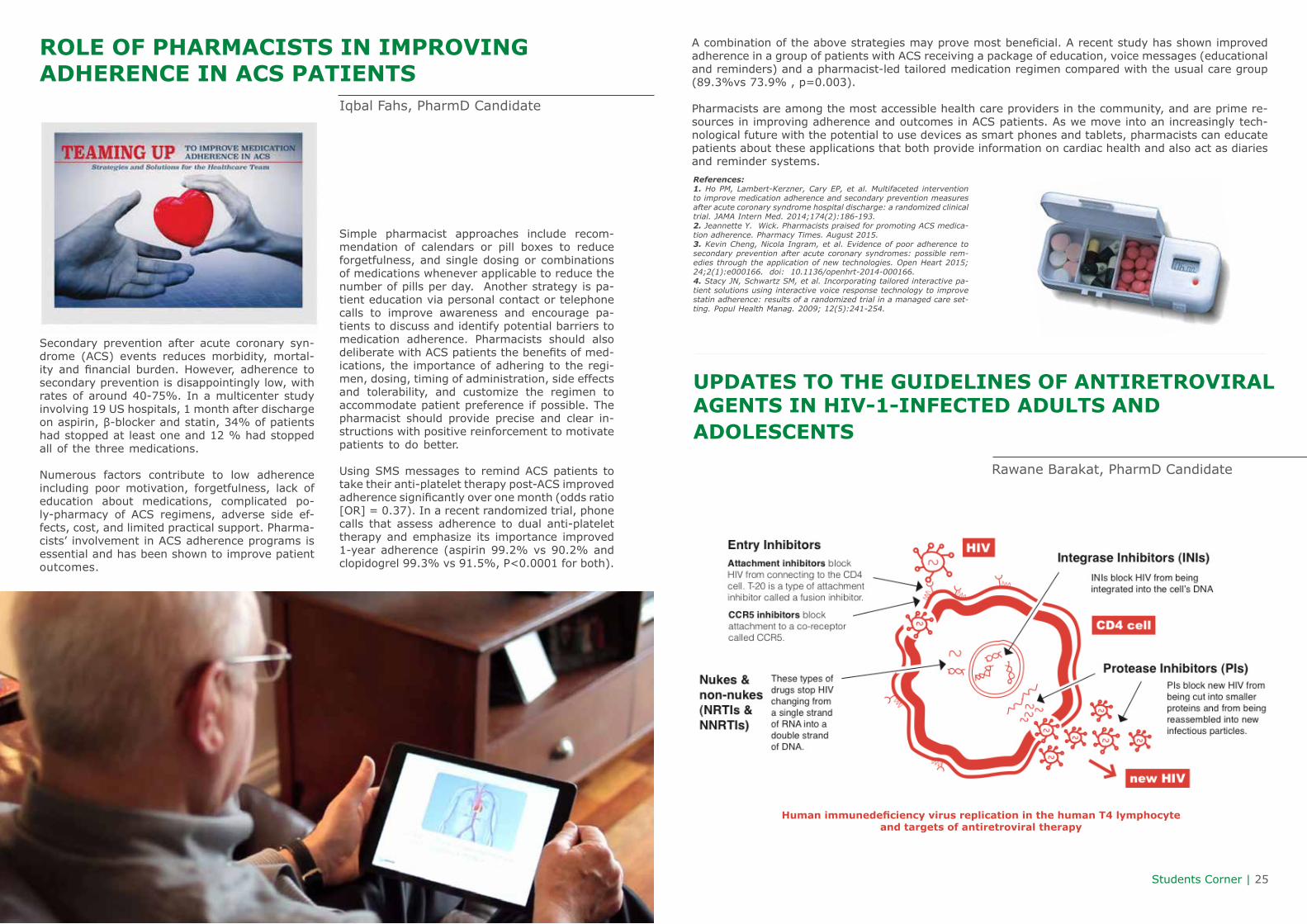
Secondary prevention after acute coronary syn-drome (ACS) events reduces morbidity, mortal-ity and financial burden. However, adherence to secondary prevention is disappointingly low, with rates of around 40-75%. In a multicenter study involving 19 US hospitals, 1 month after discharge on aspirin, β-blocker and statin, 34% of patients had stopped at least one and 12 % had stopped all of the three medications.
Numerous factors contribute to low adherence including poor motivation, forgetfulness, lack of education about medications, complicated po-ly-pharmacy of ACS regimens, adverse side ef-fects, cost, and limited practical support. Pharma-cists’ involvement in ACS adherence programs is essential and has been shown to improve patient outcomes.
Simple pharmacist approaches include recom-mendation of calendars or pill boxes to reduce forgetfulness, and single dosing or combinations of medications whenever applicable to reduce the number of pills per day. Another strategy is pa-tient education via personal contact or telephone calls to improve awareness and encourage pa-tients to discuss and identify potential barriers to medication adherence. Pharmacists should also deliberate with ACS patients the benefits of med-ications, the importance of adhering to the regi-men, dosing, timing of administration, side effects and tolerability, and customize the regimen to accommodate patient preference if possible. The pharmacist should provide precise and clear in-structions with positive reinforcement to motivate patients to do better.
Using SMS messages to remind ACS patients to take their anti-platelet therapy post-ACS improved adherence significantly over one month (odds ratio [OR] = 0.37). In a recent randomized trial, phone calls that assess adherence to dual anti-platelet therapy and emphasize its importance improved 1-year adherence (aspirin 99.2% vs 90.2% and clopidogrel 99.3% vs 91.5%, P<0.0001 for both).
A combination of the above strategies may prove most beneficial. A recent study has shown improved adherence in a group of patients with ACS receiving a package of education, voice messages (educational and reminders) and a pharmacist-led tailored medication regimen compared with the usual care group (89.3%vs 73.9% , p=0.003).
Pharmacists are among the most accessible health care providers in the community, and are prime re-sources in improving adherence and outcomes in ACS patients. As we move into an increasingly tech-nological future with the potential to use devices as smart phones and tablets, pharmacists can educate patients about these applications that both provide information on cardiac health and also act as diaries and reminder systems.References:1. Ho PM, Lambert-Kerzner, Cary EP, et al. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: a randomized clinical trial. JAMA Intern Med. 2014;174(2):186-193.2. Jeannette Y. Wick. Pharmacists praised for promoting ACS medica-tion adherence. Pharmacy Times. August 2015.3. Kevin Cheng, Nicola Ingram, et al. Evidence of poor adherence to secondary prevention after acute coronary syndromes: possible rem-edies through the application of new technologies. Open Heart 2015; 24;2(1):e000166. doi: 10.1136/openhrt-2014-000166.4. Stacy JN, Schwartz SM, et al. Incorporating tailored interactive pa-tient solutions using interactive voice response technology to improve statin adherence: results of a randomized trial in a managed care set-ting. Popul Health Manag. 2009; 12(5):241-254.
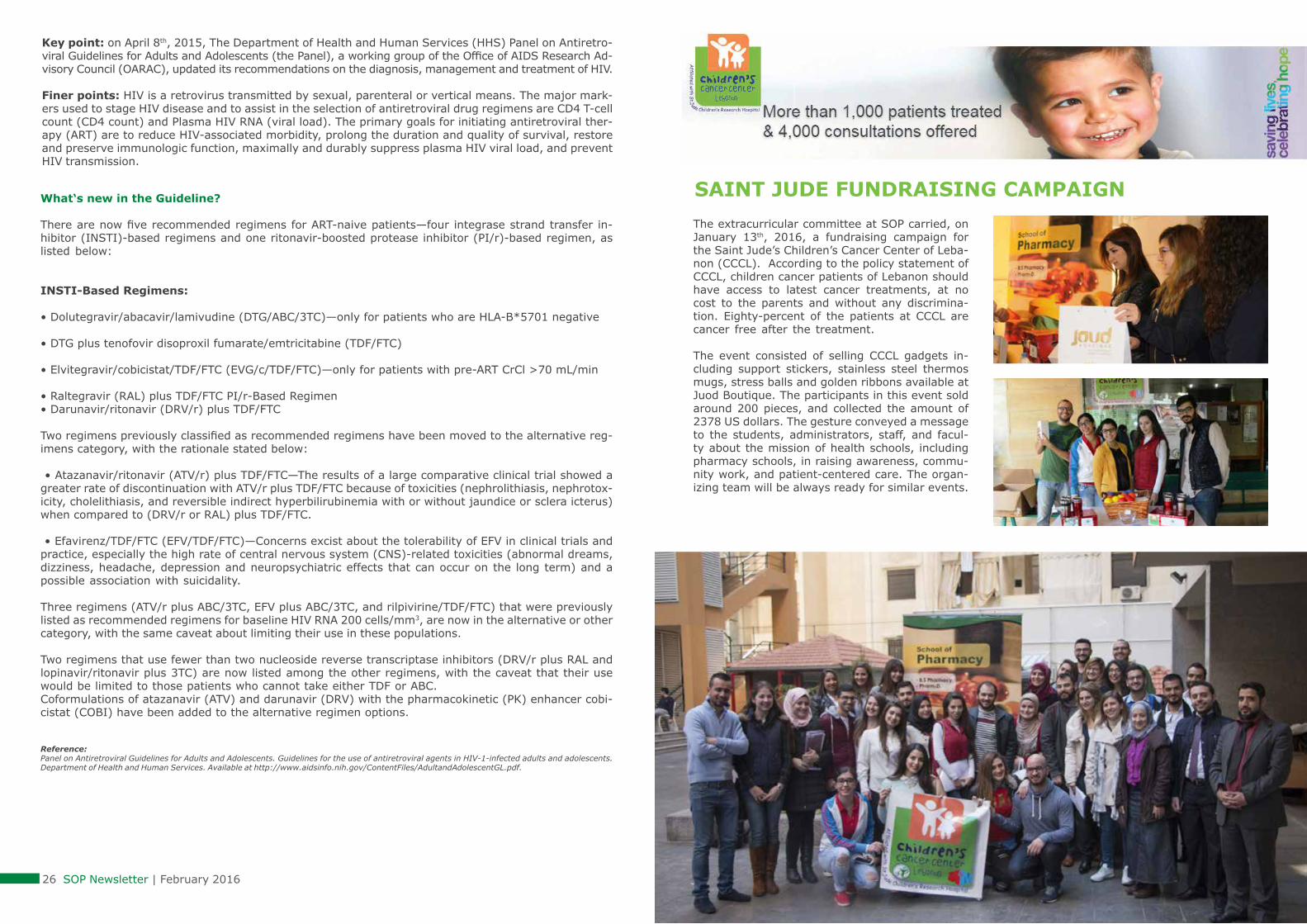
Human immunedeficiency virus replication in the human T4 lymphocyte and targets of antiretroviral therapy
Students Corner | 27 26 SOP Newsletter | February 2016
What‘s new in the Guideline?
There are now five recommended regimens for ART-naive patients—four integrase strand transfer in-hibitor (INSTI)-based regimens and one ritonavir-boosted protease inhibitor (PI/r)-based regimen, as listed below:
INSTI-Based Regimens:
• Dolutegravir/abacavir/lamivudine (DTG/ABC/3TC)—only for patients who are HLA-B*5701 negative
• DTG plus tenofovir disoproxil fumarate/emtricitabine (TDF/FTC)
• Elvitegravir/cobicistat/TDF/FTC (EVG/c/TDF/FTC)—only for patients with pre-ART CrCl >70 mL/min
• Raltegravir (RAL) plus TDF/FTC PI/r-Based Regimen • Darunavir/ritonavir (DRV/r) plus TDF/FTC
Two regimens previously classified as recommended regimens have been moved to the alternative reg-imens category, with the rationale stated below:
• Atazanavir/ritonavir (ATV/r) plus TDF/FTC—The results of a large comparative clinical trial showed a greater rate of discontinuation with ATV/r plus TDF/FTC because of toxicities (nephrolithiasis, nephrotox-icity, cholelithiasis, and reversible indirect hyperbilirubinemia with or without jaundice or sclera icterus) when compared to (DRV/r or RAL) plus TDF/FTC.
• Efavirenz/TDF/FTC (EFV/TDF/FTC)—Concerns excist about the tolerability of EFV in clinical trials and practice, especially the high rate of central nervous system (CNS)-related toxicities (abnormal dreams, dizziness, headache, depression and neuropsychiatric effects that can occur on the long term) and a possible association with suicidality.
Three regimens (ATV/r plus ABC/3TC, EFV plus ABC/3TC, and rilpivirine/TDF/FTC) that were previously listed as recommended regimens for baseline HIV RNA 200 cells/mm3, are now in the alternative or other category, with the same caveat about limiting their use in these populations.
Two regimens that use fewer than two nucleoside reverse transcriptase inhibitors (DRV/r plus RAL and lopinavir/ritonavir plus 3TC) are now listed among the other regimens, with the caveat that their use would be limited to those patients who cannot take either TDF or ABC.Coformulations of atazanavir (ATV) and darunavir (DRV) with the pharmacokinetic (PK) enhancer cobi-cistat (COBI) have been added to the alternative regimen options.
Reference: Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
Key point: on April 8th, 2015, The Department of Health and Human Services (HHS) Panel on Antiretro-viral Guidelines for Adults and Adolescents (the Panel), a working group of the Office of AIDS Research Ad-visory Council (OARAC), updated its recommendations on the diagnosis, management and treatment of HIV.
Finer points: HIV is a retrovirus transmitted by sexual, parenteral or vertical means. The major mark-ers used to stage HIV disease and to assist in the selection of antiretroviral drug regimens are CD4 T-cell count (CD4 count) and Plasma HIV RNA (viral load). The primary goals for initiating antiretroviral ther-apy (ART) are to reduce HIV-associated morbidity, prolong the duration and quality of survival, restore and preserve immunologic function, maximally and durably suppress plasma HIV viral load, and prevent HIV transmission.
SAINT JUDE FUNDRAISING CAMPAIGNThe extracurricular committee at SOP carried, on January 13th, 2016, a fundraising campaign for the Saint Jude’s Children’s Cancer Center of Leba-non (CCCL). According to the policy statement of CCCL, children cancer patients of Lebanon should have access to latest cancer treatments, at no cost to the parents and without any discrimina-tion. Eighty-percent of the patients at CCCL are cancer free after the treatment.
The event consisted of selling CCCL gadgets in-cluding support stickers, stainless steel thermos mugs, stress balls and golden ribbons available at Juod Boutique. The participants in this event sold around 200 pieces, and collected the amount of 2378 US dollars. The gesture conveyed a message to the students, administrators, staff, and facul-ty about the mission of health schools, including pharmacy schools, in raising awareness, commu-nity work, and patient-centered care. The organ-izing team will be always ready for similar events.

SOP Events & Activities | 29 28 SOP Newsletter | February 2016
SOP PARTICIPATES IN THE ANNUAL ICAAC AT SAN DIEGO, CALIFORNIA – NETWORKING WITH THE WORLD’S EXPERTS IN INFECTIOUS DISEASES
SOP VISITS THE NEWLY ELECTED PRESIDENT OF OPL
The newly elected president of the Order of Pharmacist of Lebanon (OPL), Dr. George Sili, was visited by the Dean, Dr. Mohamad Rahal, and Faculty from SOP, to congratulate him and the new members of the Order council for their recent election during November, 2015, and wish them excellence in their new appointment.
Dr. Sili acknowledged SOP Faculty for their pleasant gesture, emphasizing on the continuous collabo-ration that should persist between SOP and OPL, especially with SOP’s great input into different OPL committees and events. He also appreciated the high standards that SOP graduates show, and their reflection of a good image of their School and University. He presented his future plans for improvement of the pharmacy profession in Lebanon.
SOP, represented by Dr. Dalal Hammoudi, participated in the 55th Interscience Conference on Antimicrobial Agents and Chemotherapy joined with the International Congress of Chemotherapy and Infection (ICAAC/ICC 2015), during September 18 – 21th , 2015, at San Diego, California.
Antibiotic resistance, advances in new antibiotic develop-ment, and antibiotic stewardship were the main themes of the annual meeting. Through poster and slide sessions, symposia, and Meet-the-Expert sessions, ICAAC/ICC 2015’s scientific program showcased the most notable names and recent discoveries from all disciplines of the infectious dis-ease community. Dr. Hammoudi presented a poster from her research on carbapenem resistance in Lebanon.
SOP PARTICIPATES IN A CONTINUING EDUCATION HALF-DAY AND GATHERING FOR PHARMACISTS AT AL-KHAYYAL HOTEL, RAYAK, BEKAA
The Continuing Education (CE) Committee at the Order of Pharmacists of Lebanon (OPL) organized a half-day at Al-Khayyal Hotel, Rayak, Bekaa, on September 12th, 2015. The activity was organized in presence of OPL former president, Dr. Rabih Hassouneh, who stressed on importance of CE and its coverage of different Lebanese regions. SOP actively participated in the program by three lectures presented by our faculty.
Dr. Bahia Chahine delivered a lecture on psoria-sis treatment and recent advances, while Dr. Sha-hanz Al Masri lectured on common ear disorders often seen in community practice and their man-agement. “Constipation: It is time for the bowel to move” was the subject of a third presentation by Dr. Marwan Akel. The attendees were involved in case discussions and asking questions at the end of each lecture, and CE credits were allocated.
SOP CONTRIBUTIONS TO CONTINUING EDUCATION SESSIONS AT THE AUDITORIUM OF THE LEBANESE ORDER OF PHARMACISTS
As part of their several contributions to Continuing Education (CE) program of the Order of Pharma-cists of Lebanon (OPL), SOP faculty delivered two lectures at the auditorium of the OPL, Cornich-El-Nahr, Beirut.
Dr. Jihan Safwan presented a CE lecture on No-vember 5th, 2015, entitled: “Community Practice: Uncomplicated Cystitis Treatment”. Dr. Safwan fo-
cused on appropriate antimicrobial regimens for urinary tract infection, in light of the increased antimicrobial resistance of urinary pathogens. Moreover, she discussed the importance of min-imizing “collateral damage” associated with the use of third-generation cephalosporins and fluoro-quinolones. The lecture was concluded by raising awareness towards having pharmacists actively engage with other clinicians to select the suitable treatment for acute uncomplicated cystitis.
“It is Bedtime” was the title of another CE lecture delivered by Dr. Marwan Akel, on November 18th, 2015. Dr. Akel discussed sleep problems, high-lighting their effect on health and on other diseas-es, with 30-40% of adults reporting symptoms of insomnia. He described the available behavioral, non-pharmacological and pharmacological ap-proaches for insomnia management, pointing out the essential safety concerns of the various drug classes, herbals, and supplements used for this purpose.

SOP Events & Activities | 31 30 SOP Newsletter | February 2016
NINTH PROMOTION OF SOP BEKAA CAMPUS GRADUATES CELEBRATED IN A GALA DINNERIn commemoration of its ninth promotion of grad-uates, the School of Pharmacy at Bekaa Campus cordially organized a gala dinner at Park Hotel, Chtoura, on November 13th, 2015. LIU president, H.E. Mr. Abdul Rahim Mourad, represented by Be-kaa Campus Academic Director, Dr. Ahmad Faraj, former President of the Lebanese Order of Phar-macists, Dr. Rabih Hassouneh, and other Order personnel, LIU Vice President, Dr. Samir Abou Nassif, LIU Provost, Dr. Ali Tarabay, administrative personnel from LIU Bekaa, Bekaa Campus Coun-cil, pharmacists and hospital directors attended the dinner, together with the Dean, Dr. Rahal, graduates, and their instructors.Speakers were presented by Dr. Samar Younes, Assistant Dean of SOP at Bekaa Campus, who highlighted the success continuously attained by SOP, which was possible through collaboration of its team and encouragement from the University. Graduates’ speech was delivered by Mohamad Henduas, PharmD candidate, who mentioned that SOP graduates at LIU have the goal of being mod-el pharmacists, and expressed gratitude for the University in creating an atmosphere conductive of learning and success.The Dean addressed the graduates, congrat-ulating their achievements, while pointing out the challenges they will face as they move from academia into their career, and asking them to maintain their smile and their hard work. He also expressed thankfulness to hospitals and pharma-cists who were fully cooperative throughout the training programs developed by SOP.Dr. Faraj expressed the President’s joy in witness-ing the graduates ripe the fruits of their previous endeavors. Moreover, he stressed on role of both University education and professional work by OPL
in maintaining strong backgrounds and innovation in the pharmacy profession.The last speech was delivered by Dr. Hassouneh, who appreciated the role SOP plays in advancing pharmacy education in Lebanon, through par-ticipation in continuing education programs and preparations for the national colloquium examina-tions. The dinner was concluded by a celebration cake and graduates presenting a trophy to the Dean to cherish his notable support during their years of study.
SOP AT BEIRUT CAMPUS CELEBRATES ITS ELEVENTH PROMOTION OF GRDAUATES IN A GALA DINNERLike in Bekaa, SOP at Beirut Campus also celebrated the 2015 promotion of pharmacy graduates in a gala dinner at Coral Beach Hotel and Resort, Beirut, on December 18th, 2015. The dinner was a friendly gathering for LIU administration, School graduates and Faculty, newly elected President of the Order of Pharmacists of Lebanon (OPL), Dr. George Sili, and the new Order council members.
Dr. Marwan Akel welcomed the guests and intro-duced the speakers. The graduates’ speech was delivered by Pharmacist Sanaa Al Khatib, who re-minded her colleagues of difficulties they had to face during their study years, and the fruition of such efforts later after graduation. Following speeches were by the Dean, Dr. Moham-ad Rahal, who congratulated the graduates, ask-ing them to maintain hard work, creativity, and professionalism in their future tasks with patients; then Dr. Sili who mentioned the notable achieve-
ments of SOP over the past years, and announced the willingness of OPL to maintain cooperation with the School, as usual. LIU President, H.E. Mr. Abdul Rahim Mourad, congratulated the new Pres-ident and members of OPL council, and highlight-ed success of the School in national colloquium examinations and in various work fields. Finally, SOP Faculty presented a trophy of appre-ciation to the former Dean’s assistant, Mrs. Siba Matar, who was leaving the School for personal and family obligations.

SOP Events & Activities | 33 32 SOP Newsletter | February 2016
Pharmacy Union ActivitiesBREAST CANCER AWARENESS, LECTURE ON PHARMACIST ROLE IN COMMUNITY, AND PALESTINE ISSUE
Pharmacy Union students at SOP, Bekaa Campus, participated in a campaign on breast cancer aware-ness organized by the School of Arts and Sciences. Under the slogan “Best Protection, Early Detection”, students stood up and united to form the pink solidarity badge carrying the awareness message for early detection of breast cancer. Furthermore, Pharmacy Union members distributed educational brochures on early detection of breast cancer.
Pharmacy Union members also invited to Bekaa Campus Dr. Asmaa Saliba Abi Nasr, consultant to the President of the Lebanese Order of Pharma-cists, to deliver a lecture entitled: “The Pharma-cist as A Health Security Guard: Where are We Now?”. In her presentation, Dr. Abi Nasr focused on the role of pharmacists in healthcare, and the strength they have to improve health outcomes for patients as well as to advance their own pro-fession.
To illustrate her ideas, Dr. Abi Nasr cited examples from real cases to encourage students to concen-trate on patient counseling and adequate revision of medical data when they move on from Univer-sity to practice their profession.
Apart from health and pharmacy-related activ-ities, Pharmacy Union, in collaboration with “Al Ghad Al Afdal Club”, organized the event “Pal-estine is Our Case”, in synchronization with the Palestinian “Rock Revolution”. Faculty members, administration, and students from Bekaa Campus gathered in remembrance of the event. Fifth year pharmacy student and Pharmacy Union member, Tarek Al Jinani, delivered a speech in tribute of the Palestinian issue.
DR. RAHAL PARTICIPATES IN THE 18TH CONGRESS OF THE SCIENTIFIC ASSOCIATION OF COLLEGES OF PHARMACY IN THE ARAB WORLD AT AL-KHARTOUM, SUDAN
The Dean of the School of Pharmacy, Dr. Mohamad Rahal, participated in the 18th Congress of the Sci-entific Association of the Colleges of Pharmacy in the Arab World that was held between 18th and 20th of November, 2015, at Omdurman Islamic University, Al-Khartoum, Sudan. The theme of the conference was: “Sudan Initiative: Harmonization of Pharmacy Education and Practice”, and it brought together key professionals in pharmacy and pharmaceutical sciences from Arab and other countries, as well as deans of pharmacy schools from the Arab World.
Major conference tracks included pharmaceutical education (curriculum development, quality as-surance and accreditation) and pharmacy practice updates, in addition to workshops on pharmacy research and regulatory drug affairs. Recommen-dations of the conference were to seek improve-ment in pharmacy education in the Arab World, through unified curricula and continuing education programs, and to deal with challenges that face the pharmacy profession in the region.

SOP Events & Activities | 35 34 SOP Newsletter | February 2016
BEKAA CAMPUS HONORS DISTINGUISHED PHARMACY STUDENTS ON PRESIDENT’S LIST AND DEAN’S LIST
Three distinguished students on the President’s list (semester Grade point Average, GPA, above 4 with a minimum of 12 credits) and 25 students on the Dean’s list (semester GPA above 3.5 with a minimum of 12 credits) from SOP were honored in a celebration at Bekaa Campus on December 11th, 2015, in presence of faculty, administrative personnel, and students’ parents.
Dr. Mohamad Rahal, Dean of the School, addressed the honorees expressing the pride they give to the university through their accomplishment and ded-ication. He encouraged them to keep the same pace, reminding them that success is not a desti-nation, but rather a journey. Honorary certificates were presented to the students by Dr. Rahal and the Administrative director of Bekaa Campus, Mr. Bassem Hazime.
SOP AT 23RD CONGRESS OF OPL – PARTICIAPTION BY FACULTY AND STUDENTS
Faculty and students from SOP at LIU participated in the 23rd annual congress of the Order of Pharmacists of Lebanon (OPL), that was held in the period from 16th to 18th of October, 2015, at Biel, Beirut. This year’s theme was: “Connecting Science to Practice”, and under this title, our faculty have presented several con-tinuing education lectures and chaired several sessions. Alcohol dependence, dealing with drug abusers, antimi-crobial resistance, obesity management, and pharmacy practice safety pearls were presented by Doctors Jihan Safwan, Zeinab Abbas, Malak Alame, Dalal Hammoudi, Marwan Akel and Sylvia Saade.
Student participation was also remarkable this year, with students from different Lebanese schools of phar-macy joining a student session for career orientation. Students from SOP had their print in this session, chaired by pharmacists working in different sectors. These professionals discussed various career choices with the students, shared with them their experience, and answered the students’ questions.

36 SOP Newsletter | February 2016
SOP PARTICIPATES IN THE ASHP MIDYEAR CLINICAL MEETING ND EXHIBITION - “THE WORLD’S LARGEST GATHERING OF PHARMACISTS”
Like every year, SOP participated the 50th American Society of Health-system Pharmacists (ASHP) Mid-year Clinical Meeting and Exhibition, at New Orleans, Louisiana, on December 6-10th, 2015. More than 22,000 pharmacists, residents, pharmacy students, and industry representatives from over 40 countries attended the meeting. They took advantage of the wide range of educational sessions, special events, and networking opportunities offered.
Doctors Fadi Hdeib, Jihan Safwan, and Faraj Saade from SOP attended the conference, and presented posters from 17 studies realized by PharmD candidates. The studies revolved around various topics, in-cluding meningitis in Lebanese population, vaccine awareness, pharmacotherapy of Parkinson’s disease, urinary tract infections in hospitalized patients, pharmacist interventions in arthritis, multidrug resistant pathogens, drug abuse, hemodialysis-related electrolyte abnormalities, bariatric surgery and hyperten-sion. A group of posters also addressed some conditions related to pregnancy, like gastrointestinal and urinary ailments, immunization and smoking in Lebanese pregnant females, gestational diabetes, gesta-tional hypertension, and folic acid deficiency.
Faculty also attended numerous grand lectures discussing updates in pulmonary diseases, infections, endocrine disorders, new technologies of drug manufacturing, and others.
SOP Social LifeThe SOP family would like to congratulate our colleagues: • Dr. Mariam Dabbouss and Dr. Fouad Sakr for having their newborn twins.• Mrs. Siba Matar, Former Dean’s assistant, for her marriage.• Dr. Jihan Safwan and Dr. Faraj Saade for their marriage.• Mrs. Faten Boukarroum, for joining SOP family as the newly recruited Dean’s assistant.• The Dean, Dr. Mohammad Rahal, and his family for their Omra visit to Mekka.
SOP is currently preparing for the following two events:
• The eleventh annual pharmacy day, which will be held on Friday, May 27th, 2016, at Beirut Campus, Blocks D and F, and it will address the theme of over-the-counter drugs.
• The first International conference which coincides with the 19th congress of the Association of Colleg-es of Pharmacy in the Arab World, between October 18th and 20th, 2016, at Bekaa Campus, Khyara. The theme of the conference will be: “Advancing Pharmacy Horizons: Integrating Education, Practice, and Research”, and will host national and international speakers, who will present and discuss latest pharmacy updates.






























