Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Factors associated with early hospital arrival in acute ischemicstroke patients
Esin Kulein Koksal • Sibel Gazioglu •
Cavit Boz • Gamze Can • Zekeriya Alioglu
Received: 7 January 2014 / Accepted: 7 April 2014
� Springer-Verlag Italia 2014
Abstract Early diagnosis and treatment in acute ischemic
stroke are crucial in terms of survival and disability. Many
stroke patients remain disabled because of the treatment
delay. The purpose of this study was to investigate the
factors associated with the early hospital arrival in acute
ischemic stroke patients. 113 patients diagnosed with acute
ischemic stroke were included in this prospective study
performed at the Karadeniz Technical University Medical
Faculty Hospital. Patients’ characteristics and patients’ and
relatives’ emotional and behavioral reactions were com-
pared between early (within 3 h) and late (after 3 h) arrival
groups. 72.6 % of patients arrived at hospital within 3 h
from symptoms onset. Univariate analysis revealed that
history of atrial fibrillation (p = 0.04) and coronary heart
disease (p = 0.02), sudden onset of symptoms
(p = 0.001), loss of consciousness (p = 0.03), recognizing
symptoms as stroke (p = 0.01), seeking immediate medi-
cal attention (p \ 0.001), feelings of fear and panic
(p = 0.001), arriving at hospital by ambulance having
called the emergency medical services (p = 0.04) and
National Institute of Health Stroke Scale (NIHSS) score
(p = 0.001) were associated with hospital arrival within
3 h. A multivariate regression model demonstrated that
recognizing symptoms as stroke (OR, 3.4; 95 % CI,
1.2–9.3) and atrial fibrillation (OR, 4.3; 95 % CI, 1.1–15.7)
were independent factors associated with early arrival. The
role in early arrival at hospital of recognizing symptoms as
stroke and seeking immediate medical attention with
transportation by ambulance emphasize the importance of
public awareness concerning recognizing the symptoms of
stroke and accessing emergency medical assistance.
Keywords Ischemic stroke � Acute � Hospital � Time �Arrival � Early
Introduction
Stroke is the second most important cause of mortality and
the main cause of disability in developed countries [1]. The
most important factors determining the extent of cell
damage in acute ischemic stroke are the duration and
degree of ischemia [2, 3]. When administered within the
first 3 h from onset of acute ischemic stroke symptoms,
intravenous thrombolytic therapy with tissue plasminogen
activator (t-PA) is a treatment of proven benefit [4].
However, it must not be forgotten that the earlier the
treatment is given, the greater the benefit [5, 6]. Interven-
tion by a specialist and starting appropriate treatment as
early as possible have been shown to be associated with
reduced levels of disability [7–9].
Considering the importance of early treatment in acute
ischemic stroke, identifying the factors that may influence
early hospital arrival and increasing public awareness of
these factors may contribute to the success of treatment.
Several studies have investigated factors influencing early
hospital arrival in different countries [2, 3, 10–14]. How-
ever, little is known about factors influencing early hospital
arrival in Turkey and also about the role of emotional and
behavioral reactions to stroke on arrival times at hospital.
The purpose of this study was to investigate the factors
associated with early hospital arrival in acute ischemic
E. K. Koksal � S. Gazioglu (&) � C. Boz � Z. Alioglu
Department of Neurology, Karadeniz Technical University
Medical Faculty, 61080 Trabzon, Turkey
e-mail: [email protected]
G. Can
Department of Public Health, Karadeniz Technical University
Medical Faculty, 61080 Trabzon, Turkey
123
Neurol Sci
DOI 10.1007/s10072-014-1796-3

stroke patients which may contribute to the development of
new strategies for increasing the opportunities of benefiting
from treatment.
Patients and methods
Patients
This prospective study was conducted at the Karadeniz
Technical University Medical Faculty Hospital, which
provides advanced medical care to approximately 4 million
people and serves as a tertiary care center and also a ref-
erence center for the use of t-PA in acute ischemic stroke in
the northeastern part of Turkey. There are approximately
20 other hospitals including community hospitals and pri-
vate clinics in the same region which also provide health-
care to stroke patients. Patients presented directly to our
university hospital emergency department or referred by
other hospitals between 1 May 2011, and 31 January 2012,
with sudden onset of acute focal neurological deficit and
diagnosis of acute ischemic stroke confirmed following
evaluation by a neurologist supported by neuroimaging
were included in the study.
Participants consisted of patients, or relatives of those
patients whose neurological condition was inappropriate
for individual participation and evaluation. Patients and/or
relatives unaware of the times of symptom onset, seeking
medical attention or hospital arrival, who could not recall
their experiences during the event or who had no relatives
available to provide such information (for unconsciousness
patients), who did not present to any hospital within the
first 48 h of symptom onset, who had in-hospital stroke and
patients and/or relatives who refused to participate were
not included.
The ethical committee approved the study, and informed
consent was obtained from each subject.
Data collection
A standardized questionnaire was administered to patients
and/or relatives as soon as possible after arrival at our
hospital. The questionnaire was developed based on the
relevant literature. In order to reduce the possibility of
participants being affected by information that might be
obtained during their stay in hospital, participants were first
asked to what they first attributed the symptoms. They were
immediately afterward asked about their behavioral and
emotional reactions to the stroke and the times of symptom
onset, seeking medical attention and hospital arrival in
order to prevent this information being forgotten over the
intervening period.
Time of stroke onset was defined as when patients or
relatives first noticed the symptoms, duration of seeking
medical attention as the period between awareness of
symptoms and time of seeking medical attention, and time
of hospital arrival as the period between awareness of
symptoms and presentation to any hospital. Since the aim
of the study was to determine the factors influencing early
hospital arrival which means starting early management,
time of hospital arrival was taken as arrival at the first
hospital. However, times to arrival at our university hos-
pital, the reference center for administration of t-PA in
ischemic stroke in our region, were also recorded. The
times given by patients and relatives were also checked
using hospital records and ambulance, consultation or
referral sheets. Patients were assessed in two groups, those
reaching hospital within the first 3 h being classified as
early arrivals and those arriving after 3 h as late arrivals.
Finally, demographic and clinical characteristics and
other factors that might influence the arrival time at hos-
pital were recorded. To that end, patients’ age, sex, level of
education, marital status, employment status, whether or
not the patient lived alone, risk factors for stroke, history of
stroke, mode of onset of stroke (sudden or gradual), where
stroke occurred, whether patients were alone during stroke,
where and when the stroke occurred and symptoms and
signs at stroke onset were recorded. The National Institute
of Health Stroke Scale (NIHSS) was used in assessing
neurological deficits resulting from stroke. In addition, the
ways in which patients sought assistance and were trans-
ported to hospital were recorded. The telephone number for
emergency medical services (EMS) in Turkey is 112,
which is also used to request ambulances. Calling 112 and
transportation by ambulance were therefore assessed as a
single factor. Calling 112 is free of charge in Turkey.
Statistical analysis
All statistical analyses were performed using ‘‘SPSS for
Windows 13.0’’. Main descriptive statistics were presented
as patient number, percentage, mean, standard deviation
and median. After evaluation of the assumption of normal
distribution, Student’s t test and the Mann–Whitney U test
were applied for the comparison of continuous variables
and the Chi square was applied for comparison of cate-
gorical variables. Correlations were tested using Spearman
correlation analysis. Logistic regression analysis was con-
ducted in order to estimate the contribution of the variables
associated with hospital arrival within 3 h on a model
consisting of the variables found to be statistically signif-
icant in the univariate analysis together with the factors
reported in the literature. The model included the variables
age, sex, atrial fibrillation, NIHSS score, recognizing
Neurol Sci
123
symptoms as stroke, using EMS and ambulance and onset
time. Statistical significance was set at a p value of 0.05.
Results
During the study period, 172 patients with acute stroke
were screened for study eligibility; 113 met the criteria for
inclusion, 106 (93.8 %) with ischemic stroke and 7 (6.2 %)
with TIA. Of these, 54 (47.8 %) presented directly to our
university hospital, and 59 (52.2 %) were referred from
other hospitals. Fifty-seven (50.4 %) patients were unable
to provide information personally, therefore data concern-
ing these were given by relatives. The patient population
consisted of 45 (39.8 %) women and 68 (60.2 %) men,
with a mean age of 69 ± 13.4 (27–90).
Median time to seeking medical attention was 15 min
(3–2,580), and median time to arrival at any hospital was
75 min (15–2,640). There was a positive correlation
between time to seeking medical attention and median
hospital arrival time (p \ 0.001). Median time for all our
patients to arrive at our university hospital was 193 min
(15–7,200). Eighty-two (72.6 %) patients arrived at any
hospital within the first 3 h, while 55 (48.7 %) patients
arrived to our university hospital within the first 3 h.
Seventeen (30.9 %) of the 55 patients presenting to our
university hospital in the first 3 h had been referred from
other hospitals. Median time to arrival of those patients
presenting directly to our university hospital was signifi-
cantly shorter than those of referred patients (p \ 0.001).
Seventy-two (63.7 %) patients arrived at the first hospital
by private vehicle, and 41 (36.3 %) by ambulance. Median
time to arrival of those using private vehicles was signifi-
cantly longer than those using ambulances (p = 0.03).
The onset of symptoms was sudden in 100 (88.5 %) of
patients. Mean NIHSS score for all patients was
6.63 ± 5.6. Sixty-four (56.6 %) of the 113 participants
recognized stroke as the cause of their symptoms, 21
(18.6 %) recognized them as something important but
could not determine what, 13 (11.5 %) thought their
symptoms were caused by existing diseases and 15
(13.3 %) reported that they did not think they were any-
thing important. In terms of behavioral responses during
stroke, 72 (63.7 %) individuals immediately sought medi-
cal assistance, while 29 (25.7 %) did not seek assistance
since they thought the symptoms would pass, 6 (5.3 %)
because they were alone, 3 (2.7 %) because it was late and
3 because they thought they had more important things to
do. In terms of emotional responses by patients or their
relatives during stroke, 72 (63.7 %) reported feeling fear or
panic while 41 (36.3 %) remained calm.
Comparison of the demographic characteristics of
patients who arrived at hospital within the first 3 h and those
arriving after 3 h revealed no significant difference between
the groups in terms of age, sex, marital status, employment
status or living alone. There was no significant difference
between the individuals deciding to seek medical attention
in the two groups in terms of age, sex or level of education.
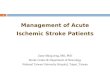
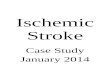
Of the stroke risk factors, history of coronary heart
disease (p = 0.02) and atrial fibrillation (p = 0.04) were
statistically more frequent in the early hospital arrival
group. No significant difference was determined between
Table 1 Comparisons of characteristics between early arrivals
(within 3 h) and late arrivals (after 3 h). Univariate analyses
Characteristics Early arrivals
(B3 h)
(n = 82)
Late arrivals
([3 h)
(n = 31)
p value
Age (mean ± SD) 70.2 ± 13.25 65.77 ± 13.54 0.11
Age [70 (%) 50 (61) 14 (45.2) 0.19
Sex, male (%) 45 (54.9) 23 (74.2) 0.09
Marital status, married
(%)
81 (98.8) 28 (90.3) 0.06
Unemployed (%) 74 (90.2) 26 (83.9) 0.34
Living alone (%) 6 (7.3) 3 (9.7) 0.7
Risk factors (%)
Hypertension 66 (80.5) 24 (77.4) 0.92
Coronary heart disease 25 (30.5) 3 (9.7) 0.02
Atrial fibrillation 28 (34.1) 4 (12.9) 0.04
Hyperlipidemia 28 (34.1) 11 (35.5) 1
Diabetes 19 (23.2) 8 (25.8) 0.96
Congestive heart failure 13 (15.9) 2 (6.5) 0.23
Previous stroke 21 (25.6) 7 (22.6) 0.92
Family history of stroke 29 (35.4) 8 (25.8) 0.45
Smoking 26 (31.7) 13 (41.9) 0.42
Clinical characteristics
NIHSS score
(mean ± SD)
7.6 ± 5.6 4 ± 4.5 0.001
Loss of consciousness
(%)
20 (24.4) 2 (6.5) 0.03
Motor weakness (%) 51 (62.2) 13 (41.9) 0.08
Sudden onset (%) 78 (95.1) 22 (71) 0.001
Recognizing symptoms as
stroke (%)
53 (64.6) 11 (35.5) 0.01
Seeking immediate
medical attention (%)
71 (86.6) 1 (3.2) <0.001
Using EMS- ambulance
transport (%)
34 (41.5) 6 (19.4) 0.04
Alone at onset (%) 19 (23.2) 7 (22.6) 1
Feelings of fear and panic
(%)
60 (73.2) 12 (38.7) 0.001
Onset location, home (%) 69 (84.1) 24 (77.4) 0.57
Onset time, daytime (%) 46 (56.1) 22 (71) 0.22
Onset time, weekend (%) 31 (37.8) 12 (38.7) 1
Bold values indicate significance (p \ 0.05)
Neurol Sci
123

the early and late arrival groups in terms of hypertension,
diabetes, hyperlipidemia, congestive heart failure, previous
history of stroke, cigarette consumption and whether stroke
occurred at night or in the daytime, or at the weekend or
midweek, the place where stroke occurred, and whether or
not the subject was alone at the time of symptom onset.
Sudden onset of symptoms (p = 0.001) and loss of
consciousness (p = 0.03) were more frequent in the early
hospital arrival group. Mean NIHSS score was also higher
in the early arrival group (p = 0.001). No difference was
observed between the two groups in terms of other symp-
toms of stroke, such as speech disturbance, motor paresis,
facial paralysis, vertigo and ataxia, nausea and vomiting,
headache and dysphagia.
Recognizing symptoms as stroke (p = 0.01), seeking
immediate medical attention (p \ 0.001), feelings of fear
and panic (p = 0.001) and using EMS and ambulance
(p = 0.04) rates were higher in the early arrival group
compared to the late arrival group. Table 1 shows the
comparisons of the characteristics of the early and late
arrival groups.
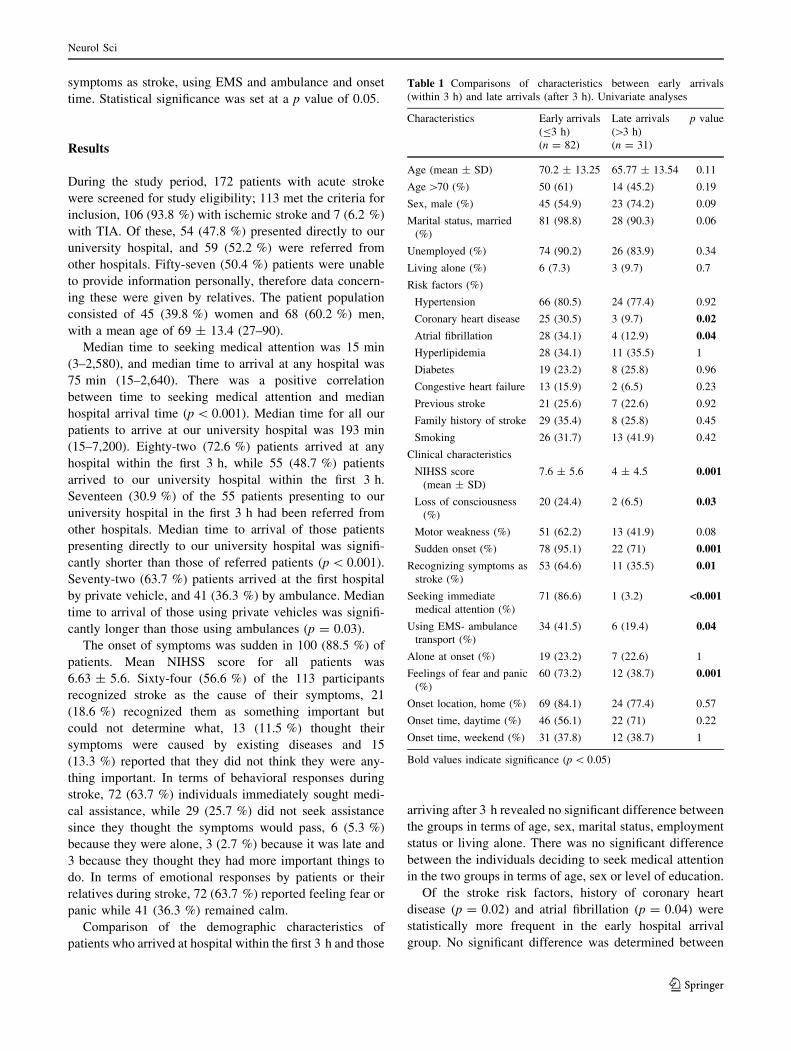
Results from logistic regression analysis indicated that
recognizing symptoms as stroke and atrial fibrillation were
independent factors associated with early arrival at hospi-
tal. Compared with the cases that did not recognize
symptoms as stroke, those cases that recognized symptoms
as stroke were 3.4 times (95 % CI, 1.2–9.3) more likely to
arrive early at hospital. Compared with the patients who
had no atrial fibrillation, those patients with a history of
atrial fibrillation were 4.3 times (95 % CI, 1.2–9.3) more
likely to arrive early at hospital (Table 2).
Discussion
Median arrival time at any hospital in acute ischemic
stroke patients in our study was 75 min, and 72.6 % of
patients arrived at a hospital within the first 3 h. Median
time to arrival at our university hospital, where thrombo-
lytic therapy can be administered, was 193 min, and
48.7 % of patients arrived within the first 3 h. Median time
to arrival at hospital in several studies in the literature
ranges from 1.5 to 16 h, with 12–68 % of patients arriving
hospital within the first 3 h [15]. The high level of early
arrival at a hospital in our study is probably due to the
region not having a wide geographical distribution. This
high level of early arrival determined in our study is
promising in terms of the use of thrombolytic therapy.
However, the median time to arrival at university hospital,
a tertiary health center at which thrombolytic therapy is
administered, of patients referred from other hospitals was
significantly longer compared to that of patients arriving
directly and the rate of arrival at our university hospital
within the first 3 h was lower compared to that of arrival at
any hospital. This may probably be attributed to lack of
sufficient awareness among the public and the health per-
sonnel involved in patient transportation about the impor-
tance of thrombolytic therapy in acute ischemic stroke and
of the institutions where it is available. Raising awareness
on this subject may increase the number of patients arriving
earlier at institutions where thrombolytic therapy is avail-
able and thus having the opportunity to use it.
Time to arrival at hospital in our study increased as time
to seeking medical attention was prolonged, and the rate of
seeking immediate medical attention in the early arrival
group was significantly higher than that of the late arrival
group. Previous studies also reported the importance of
time to seeking medical attention. Chang et al. [16]
reported that time to seeking medical attention represented
45 % of total time to arrival at hospital. Rosamond et al.
[17] reported that time to seeking medical attention was the
most important factor affecting time to arrival at hospital.
Although there are conflicting reports on the influence of
demographic factors on early admission, age, sex, educa-
tion, marital and employment status, living alone, onset
location and time or being alone at onset were not asso-
ciated with early arrival in the present study.
History of coronary heart disease and atrial fibrillation
were more frequent in the early arrival group and atrial
fibrillation was identified as an independent risk factor
affecting early arrival at hospital in the multivariate ana-
lysis in our study. Similar to our results, significant cor-
relations between atrial fibrillation or heart disease and
early arrival at hospital have been reported in the literature
[12, 13]. Patients with cardiac disease generally arriving
early may probably be attributed to higher public aware-
ness of heart disease.
Wester et al. [18] reported that subjects unable to rec-
ognize symptoms as stroke or those who did not seek
assistance within the first hour even if they did identify
them as stroke took longer to reach hospital. Kim et al. [19]
identified perception of symptoms as stroke and knowledge
of thrombolytic therapy as a powerful factor in early arrival
Table 2 Predictors of arrival at hospital within 3 h. Multivariate
analyses
Variable OR (95 % CI) p value
Age [70 1.8 (0.7–4.8) 0.21
Sex, male 0.6 (0.2–2) 0.46
Atrial fibrillation 4.3 (1.1–15.7) 0.02
NIHSS score 1.1 (0.9–1.2) 0.06
Recognizing symptoms as stroke 3.4 (1.2–9.3) 0.01
Using EMS-ambulance transport 1.7 (0.5–5.3) 0.36
Onset time, daytime 0.4 (0.1–1.3) 0.15
Bold values indicate significance (p \ 0.05)
Neurol Sci
123

at hospital. Feldman et al. [20] also reported that recog-
nizing symptoms as stroke was correlated with early arri-
val. We also identified recognition of symptoms as stroke
as an independent factor in early arrival at hospital, a
finding which again emphasizes the importance of educa-
tion concerning stroke related symptoms.
Rates of seeking emergency medical services (EMS) as
the first medical contact in the literature have been reported
at between 16 and 49 %, and rates of transportation by
ambulance or EMS at 16–94 % [15]. In our study 36.3 %
of participants arrived at hospital by ambulance after
calling the EMS. Although these patients had a shorter
arrival time to hospital than those using private vehicles
and higher rates of arrival at hospital within the first 3 h,
using EMS and ambulance was not significant on multi-
variate analysis. Most studies in the literature have reported
a significant correlation between being transported to
hospital by ambulance and early arrival at hospital [10–13,
16–19, 21, 22]. Our study did not investigate the reasons
for not choosing ambulances for transfer, but the low level
determined emphasizes the need for society to be educated
on the importance of EMS and ambulance use in early
arrival at hospital.
Differing results obtained in studies investigating the
factors associate with early arrival at hospital in various
regions are probably due to sociocultural and healthcare
service delivery variations. To the best of our knowledge,
this is the first study to investigate factors associated with
early hospital arrival in acute ischemic stroke patients in
Turkey, including the role of clinical characteristics and
patients’ and relatives’ behavior during acute ischemic
stroke. Previous studies investigating the factors affecting
late arrival at hospital of acute ischemic stroke patients
have examined ischemic and hemorrhagic strokes together,
and the effect of patients’ clinical characteristics and
patients’ and relatives’ behaviors has not been assessed
[23, 24]. There are limitations to this study, however. One
is the small sample size and hospital-based design
involved, which limit the possibility of generalizing the
findings to the entire population. As many patients with
acute stroke admitted to other hospitals and not all patients
with acute stroke referred to our hospital, our study does
not cover all patients with acute stroke in the region.
Another limitation is that the question of to what patients
first attributed their symptoms may have been affected by
their knowledge that they were taking part in a study
concerning stroke or referred patients knowing that stroke
was the reason for their referral. In order to reduce this
possibility to a minimum, we sought to obtain this infor-
mation from participants as soon as possible.
In conclusion, seeking immediate medical attention by
recognizing symptoms as stroke and using EMS and
ambulance for transfer to hospital were identified as the
most significant factors affecting early arrival. Educa-
tional campaigns in order to increase public awareness of
the importance of early treatment in acute ischemic
stroke and associated factors, especially stroke related
symptoms and signs, the role of seeking immediate
medical assistance and using EMS and ambulance for
transfer, may increase the number of patients arriving at
hospital earlier and having the opportunity to receive
early management.
Acknowledgments None.
References
1. Millan M, Davalos A (2006) The need for new therapies for acute
ischaemic stroke. Cerebrovasc Dis 22:3–9
2. Chen CH, Huang P, Yang YH, Liu CK, Lin TJ, Lin RT (2007)
Pre-hospital and in-hospital delays after onset of acute ischemic
stroke: a hospital-based study in southern Taiwan. Kaohsiung J
Med Sci 23:552–559
3. Turan TN, Hertzberg V, Weiss P, McClellan W, Presley R,
Krompf K, Karp H, Frankel MR (2005) Clinical characteristics of
patients with early hospital arrival after stroke symptom onset.
J Stroke Cerebrovasc Dis 14:272–277
4. The National Institute of Neurological Disorders and Stroke rt-
PA Stroke Study Group (1995) Tissue plasminogen activator for
acute ischemic stroke. N Engl J Med 333:1581–1587
5. Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R,
Broderick JP et al (2004) Association of outcome with early
stroke treatment: pooled analysis of ATLANTIS, ECASS, and
NINDS rt-PA stroke trials. Lancet 363:768–774
6. Wardlaw JM, Warlow CP (1992) Thrombolysis in acute ischemic
stroke: does it work? Stroke 23:1826–1839
7. Davalos A, Castillo J, Martinez-Vila E (1995) Delay in neuro-
logical attention and stroke outcome. Cerebrovascular Diseases
Study Group of the Spanish Society of Neurology. Stroke
26:2233–2237
8. Moloczij N, McPherson KM, Smith JF, Kayes NM (2008)
Help-seeking at the time of stroke: stroke survivors’ perspec-
tives on their decisions. Health Soc Care Community
16:501–510
9. Silvestrelli G, Parnetti L, Paciaroni M, Caso V, Corea F, Vitali R,
Capocchi G, Agnelli G (2006) Early admission to stroke unit
influences clinical outcome. Eur J Neurol 13:250–255
10. Derex L, Adeleine P, Nighoghossian N, Honnorat J, Trouillas P
(2002) Factors influencing early admission in a French stroke
unit. Stroke 33:153–159
11. Iosif C, Papathanasiou M, Staboulis E, Gouliamos A (2012)
Social factors influencing hospital arrival time in acute ischemic
stroke patients. Neuroradiology 54:361–367
12. Jin H, Zhu S, Wei JW, Jin H, Zhu S, Wei JW et al (2012) Factors
associated with pre-hospital delays in the presentation of acute
stroke in urban China. Stroke 43:362–370
13. Lacy CR, Suh DC, Bueno M, Kostis JB (2001) Delay in pre-
sentation and evaluation for acute stroke: Stroke Time Registry
for Outcomes Knowledge and Epidemiology (STROKE). Stroke
32:63–69
14. Nowacki P, Nowik M, Bajer-Czajkowska A, Porebska A, Zywica
A, Nocon D, Drechsler H, Safranow K (2007) Patients’ and
bystanders’ awareness of stroke and pre-hospital delay after
stroke onset: perspectives for thrombolysis in West Pomerania
Province, Poland. Eur Neurol 58:159–165
Neurol Sci
123

15. Teuschl Y, Brainin M (2010) Stroke education: discrepancies
among factors influencing pre-hospital delay and stroke knowl-
edge. Int J Stroke 5:187–208
16. Chang KC, Tseng MC, Tan TY (2004) Pre-hospital delay after
acute stroke in Kaohsiung, Taiwan. Stroke 35:700–704
17. Rosamond WD, Gorton RA, Hinn AR, Hohenhaus SM, Morris
DL (1998) Rapid response to stroke symptoms: the Delay in
Accessing Stroke Healthcare (DASH) study. Acad Emerg Med
5:45–51
18. Wester P, Radberg J, Lundgren B, Peltonen M (1999) Factors
associated with delayed admission to hospital and in-hospital
delays in acute stroke and TIA: a prospective, multicenter study.
Seek- Medical-Attention-in-Time Study Group. Stroke 30:40–48
19. Kim YS, Park SS, Bae HJ, Cho AH, Cho YJ, Han MK et al
(2011) Stroke awareness decreases pre-hospital delay after acute
ischemic stroke in Korea. BMC Neurol 11:2
20. Feldmann E, Gordon N, Brooks JM, Brass LM, Fayad PB,
Sawaya KL, Nazareno F, Levine SR (1993) Factors associated
with early presentation of acute stroke. Stroke 24:1805–1810
21. Morris DL, Rosamond W, Madden K, Schultz C, Hamilton S (2000)
Pre-hospital and emergency department delays after acute stroke: the
Genentech stroke presentation survey. Stroke 31:2585–2590
22. Mandelzweig L, Goldbourt U, Boyko V, Tanne D (2006) Per-
ceptual, social, and behavioral factors associated with delays in
seeking medical care in patients with symptoms of acute stroke.
Stroke 37:1248–1253
23. Keskin O, Kalemoglu M, Ulusoy RE (2005) A clinic investiga-
tion into pre-hospital and emergency department delays in acute
stroke care. Med Princ Pract 14:408–412
24. Memis S, Tugrul E, Evci ED, Ergin F (2008) Multiple causes for
delay in arrival at hospital in acute stroke patients in Aydin,
Turkey. BMC Neurol 8:15
Neurol Sci
123