Embed Size (px)
Citation preview
1
1.RESEARCH TOPIC
Restorative Benefits of Paediatric Ward as a Play Environment in Nigerian Hospital
2. RESEARCH AIM
The aim of this study is to investigate the restorative benefits inherent with play
activities in a paediatric hospital setting.
3. RESEARCH OBJECTIVES
The following objectives are formulated, to achieve the stated aim.
i. To identify the problems patients and caregivers are facing due to lack of
play and activities in a hospital ward;
ii. To observe the benefits of play using “loose parts” as it affects children and
improves their restoration towards a feeling of well being; and
iii. To develop a guideline as to how future paediatric hospital settings will be
designed to provide restoration based on children's preferences.
4. ASSUMPTION
There is growing evidence that stress and anxiety has attracted attention from
researchers, health care provider, and designers. Which shows that hospitalized children
are faced with psychological challenges which affect their hospital stay? This is as a
result of their new and unfamiliar settings, which add stress and in return delay their
restoration (Dise-Lewis, 1988; Varni and Katz, 1997; Varni, Rappaport, and Talbot,
1991).
It isfor now an assumption that if the paediatric ward can be changedinto a play
environment, where patients can play with elements and materials from the theory of
2
“loose parts” under monitoring in line with hospital and medical protocol. It can
improveon a child's ability in coping with stress, and to adjust their emotional state,
social connection, physical development, trust and acceptance of routine medication.
5. RESEARCH QUESTIONS
i. Why would a paediatric ward being conceived as a play environment have
an effect on patients psychologically, and improve on their feeling of well
being?
ii. What are the measures taken in providing children with play experience in
the paediatric ward?
iii. How would children perceive the hospital ward, looking at setting as a play environment?
6. RESEARCH BACKGROUND
Most of the present paediatric ward settings in Nigerian hospitals deliver health care in
relation to protocols and medical norms. The hospital only considers pathogenic
approach in the format of biomedical treatment of illness and control of the spread of
disease. With emphasis on the provision of equipment and facilities that adds
functionality to some extent, but psychologically inefficient to improving the well being
of patients. The formal introduction of western medicine in Nigeria was dated back to
the 1860s, when the sacred heart hospital was established by the Roman Catholic
missionaries in western Nigeria. The first set of catholic priests arrived in Abeokuta on
the 29th of June 1880 and the first catholic missionary sisters on the 3rd of March 1886.
It was at that time that health care delivery entered Nigeria, by meeting the medical
needs of the communities, especially children at the mission homes. The missionaries
were the first health visitors to bring western medicine to Nigeria, they played a vital
task in providing modern health care in Nigeria inthe 1960s, they operate about 40% of
the total number of missions based hospitals (Manuwa,1971).
3
The mission also played a vital role in the training and education of medical personnel
and with further advanced training abroad; these were based in areas that they have
religious influence and other activities. By 1954, almost all the hospitals were operated
by the Catholicmissionaries, the Roman Catholic with the Sudan interior mission
operated other facilities in the northern part of the in the country which remain as part
of health care facilities up to the 1990s (Manuwa, 1971).
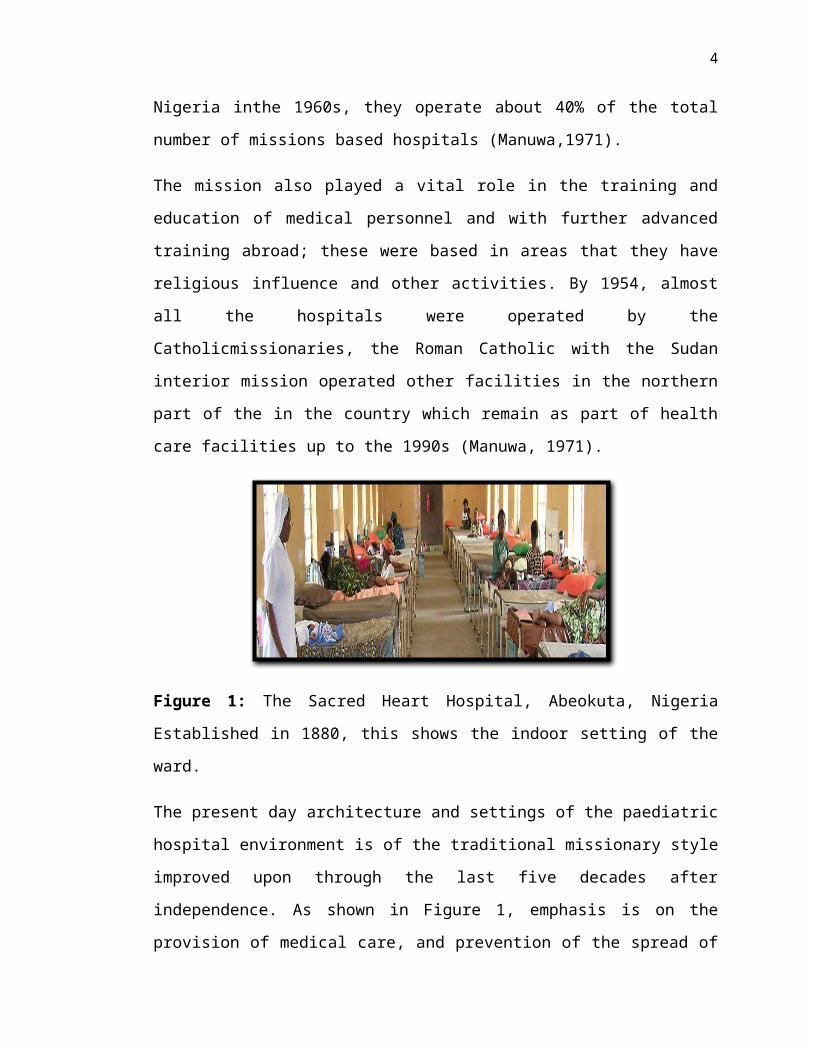
Figure 1: The Sacred Heart Hospital, Abeokuta, Nigeria Established in 1880, this
shows the indoor setting of the ward.
The present day architecture and settings of the paediatric hospital environment is of the
traditional missionary style improved upon through the last five decades after
independence. As shown in Figure 1, emphasis is on the provision of medical care, and
prevention of the spread of disease. As such the environment is more for treatment and
housing of medical equipment, beds, cabins, hangers, nurses’ station, and aisle for
movement, toilets and bathrooms, doctors call rooms, dressingroom.As such the
spaceprovided and distance from one bed to the next does not allow for room and
spaces, especially in the children’s ward for free movement and play activities.
There is a lack or minimal consideration givento other environmental and physical
features that naturally improvethe healing process and patients feeling of well-
being.This shows enough reason for caregivers, hospital management and designers to
start looking for avenue of changing the present hospital settings with features and
conditions for creating a restorative environment(Monjour and Yisong, 2012).
4
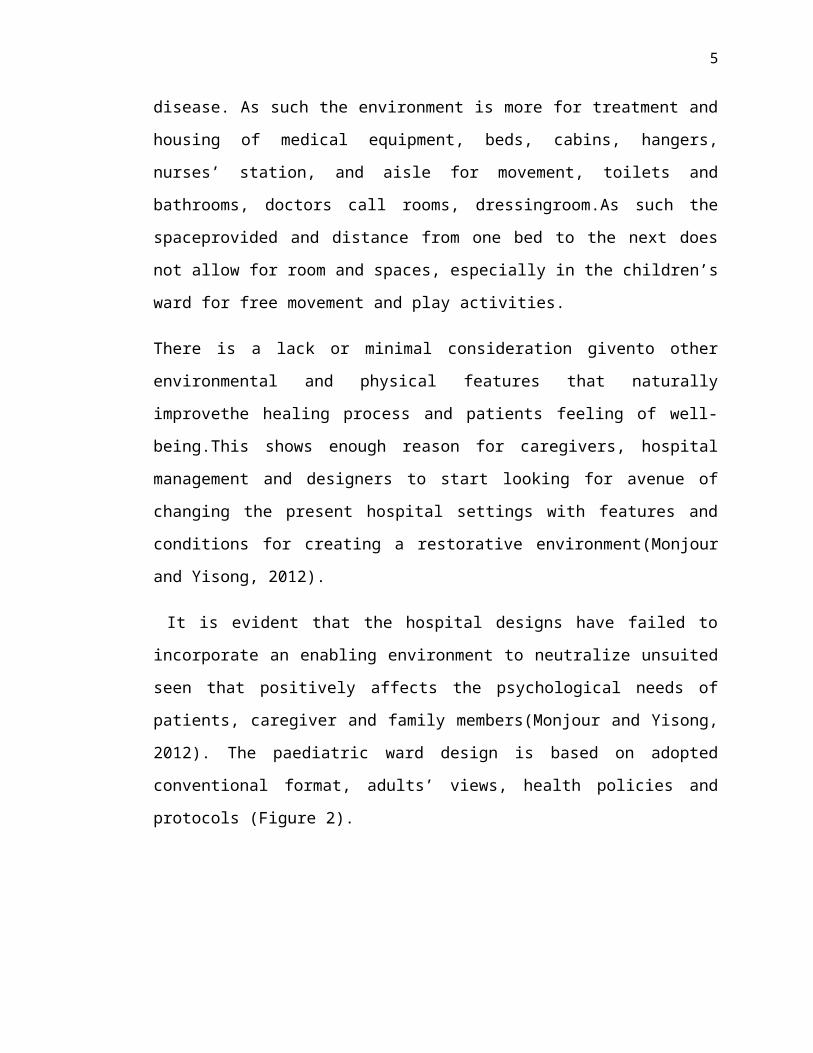
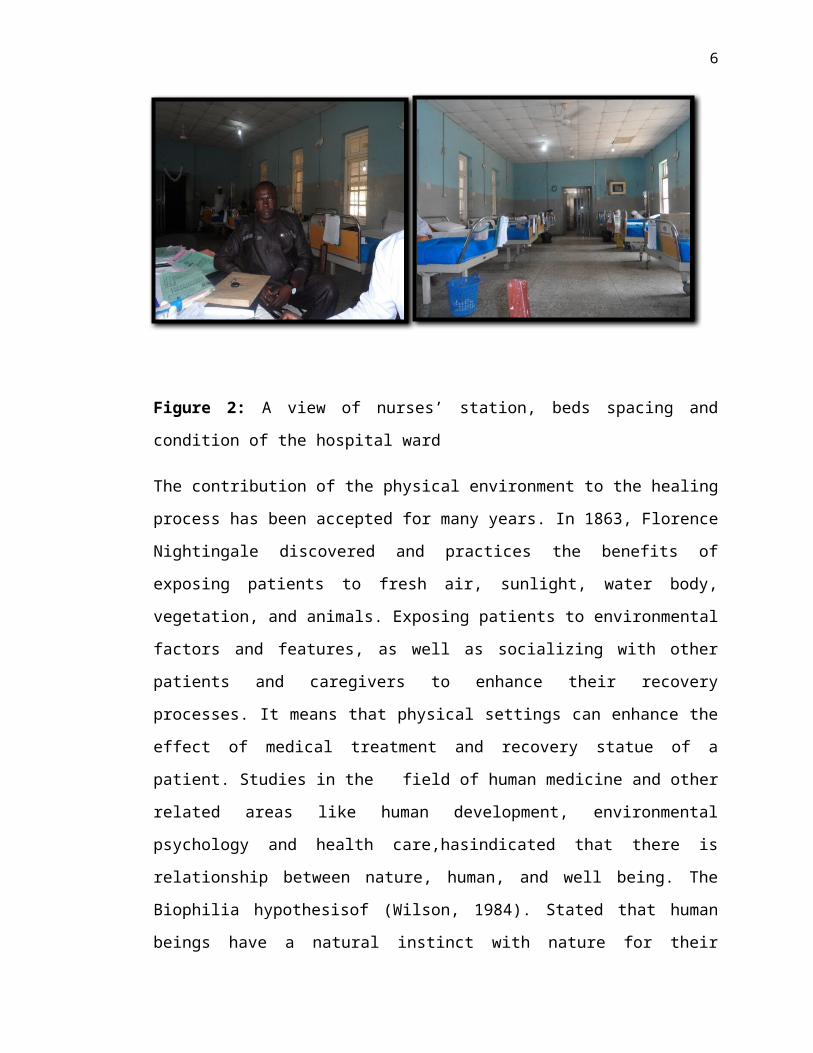
It is evident that the hospital designs have failed to incorporate an enabling
environment to neutralize unsuited seen that positively affects the psychological needs
of patients, caregiver and family members(Monjour and Yisong, 2012). The paediatric
ward design is based on adopted conventional format, adults’ views, health policies and
protocols (Figure 2).
Figure 2: A view of nurses’ station, beds spacing and condition of the hospital ward
The contribution of the physical environment to the healing process has been accepted
for many years. In 1863, Florence Nightingale discovered and practices the benefits of
exposing patients to fresh air, sunlight, water body, vegetation, and animals. Exposing
patients to environmental factors and features, as well as socializing with other patients
and caregivers to enhance their recovery processes. It means that physical settings can
enhance the effect of medical treatment and recovery statue of a patient. Studies in the
field of human medicine and other related areas like human development,
environmental psychology and health care,hasindicated that there is relationship
between nature, human, and well being. The Biophilia hypothesisof (Wilson, 1984).
Stated that human beings have a natural instinct with nature for their psychological,
emotional and spiritual needs (Derr and Kellert, 2012). Human desire for natural
settings has been established by much research work, which shows that nature offers an
avenue for a feeling of well-being and re-cooperating from the effect of acquired stress
5
(Joye and van den Berg, 2011). A further study on health outcome and feeling of well-
being is the Antonorsky’ssalutogenic concept, an approach to health. The emphasis here
is that well-being has a relationship with human activities, social relationship andwith a
strong belief and good will from family and friends human health can improvetowards
feeling of well-being (Dunleavy et al, 2012).
7. PROBLEM STATEMENT
The thought of conceptualizing a paediatric ward as a play environment is to
fosterrestoration to hospitalized children in Nigerian paediatric hospital wards. This can
be attained by changing the present hospital ward settings with positive distraction, such
as play activities for paediatric patients as part of their normal hospital ward.This is as a
result of lack of provision of any kind of features or settings that can improve on
children’s coping skills and distract their attention in a positive manner.As children are
taken to hospital, they noticed that the environment is different and away from their
home and school environment,which is familiar and give them room for playfulness,
and to a new environment that is unknown and unfriendly. They are highly introduced
to different foreign objects and different, unfamiliarpeople potentially causing them
considerable fear, stress and anxiety. For a child with a vivid imagination, anything can
be terrifying.The usual practice is set of personnel all dressed up neatly in white
uniforms with hypodermic injections with needles for blood draw, temperature
thermometers and weight measurement scales or posture still for scanning and X-ray
test. As such, they consider the hospital environment threatening and they can develop
additional stress and trauma during a doctor's appointment orhospitalization (Said,
2006).
Children need an environment that can direct their attention away from pain and
anxiety, which can be achieved by exploring the use of structured playusing elements
from loose partsto enhance children's performance. In connection to the
childrenphysical, cognitive and social functioning.Despite the many positive research
carried out in developed economies around the worldson improving children
6
hospitalization.In relation to minimizing their stress, painful experience and reducing
their length of hospital stay (i) it is evident that such efforts in the Nigerian paediatric
health care environment have not been givenmuch priority, and (ii) the climatic
condition in the study area does not allow an enabling environment to employ finding
from studies conducted in other developed economies around the world such as
Malaysia in the areas of garden and landscapemostly outside the ward. Because of the
shorter periodof raining season within a year, and lack of enough water provision which
makes it very expensive to maintain either a garden or landscape in almost all the
hospital environment.
Playing in an organized setting in an indoor environment can be used to replace the
outdoor play features that are found in gardens and landscape environments. And
children need not to come out into the harsh whether to play.The provisions of synthetic
loose parts indoors can be used to trigger their attention positively to attain the needed
objective of restoration in relation to their healing. The hospitalenvironment and
settings should be able to assist with their restoration towards improving their physical,
social, and cognitive development.This forms the three main features of human
development which expands during the process of human growth.The physical
development involves physical growth and maturation which include gross motor skills,
which involves large muscles of the legs and arms that are used in running and walking,
and fine motor skills which have to do with fingers, toes, eyes and other parts like the
brainthose are used for activities such as drawing, writing, grasping objects, throwing
and catching. The cognitive development is linked to changes in person ability to reason
which involves stages such as a sensory motor stage, the pre operational stage, concrete
operational stage and the formal operational stage. And the social development is linked
to the changes that occurs as a result of person ability to control his or her feelings. The
three areas of development are different in a way, but they work together and influence
each other.The physical development of the brain, allows cognitive advancement to
progress and think of a solutions in different ways, and the same cognitive involvement
gives room for better social and emotional feelings (Mcdevitt and Ormrod, 2004).
7
A child's health care environment restoration can be defined as stress reduction in an
unthreatening environment which allows for physical movement and exercise (Ulrich,
2002). It is as a result of locomotion, physical and social interaction of person with the
features and element of the environment. Which can be explored through play, as play
is the most important activity in the lives of children and as a medium of interaction
with their environment. On the other hand, healing or restorationis defined “as the
casual relationship of man with the environment, the cause is the physical elements and
the natural forces of the environment” (Said, 2006). Studieshave shownthat restorative
environment is conceived as places that provide an avenue for recovering from stress,
and renewal of health, and the ability to focus attention (Hipp and Ogunseitan, 2011).
The health benefits of restorative environment are highlighted by the attention
restorative theory (ART) of Kaplan and Kaplan (1989) and Kaplan (1995).The
theorymaintains that coming in contact with the natural environment has the ability to
improve patient’s cognitive attention, which promotes human interpersonal and social
functioning.The theory argued that an experience in an environment which is
compatible with one's preferencecan enhance physical, psychological and social
wellbeing especially when there is amount of time spent in that environment (Hansen-
Ketchum et al, 2011).
The participants in this study explainthat places in nature or activities that providedthem
with the sense of feeling like being away from the stress of modern life.Relayson
participant preferences which include a chance for unstructured play, view of water
bodies and quietness among others. Further studies on the restorative environment as
explained by (Said, 2008).“Is that the restorative environment, restorative garden,
therapeutic landscape, therapeutic garden, healing garden, healing landscape, often
refers to the same thing and carry a similar meaning, which means, recovery from
illness, diseases, injury, or other impairment.”
Studies in paediatric nursing have shown that medical protocol and the hospital settings,
increase stress and negativehealth effect on children. They show signs of
aggressiveness, fear of pain, emotional regression, loss of appetite and sleep which
further result in adding more illness (Nandineni, 2013).Such problems were due to
8
factors like fear of illness, new environment, and changes in their usual activities.
Anxiety has been reported to be the most stress related child’s experience, many
developing nations such as Nigeria, have their peculiar problems which increases the
level of anxiety experience among hospitalized children. Examples are lack of proper
funding, high poverty level and implementation of few conducted research. A
compilation of the causes of child hospital stress by Coyne (2006) in(Jolley, 2006).
Found the following as the causes of stress during children hospitalization.
(i) Separation from family and friends:Disruption to the family routine, normal
activities, peer relationships, school achievement;
(ii) Being in an unfamiliar environment:fear of the unknown, strange
environment,professionals, noisy ward, and bright lights at night, hot
environment, inadequate play facilities,and food;
(iii) Receiving investigations and treatments: Fears of operations, needles,
mistakes in treatment, harm to body, pain, dying; and
(iv) Loss of self-determination: loss of independence, restricted activities,
lacking control over personal needs, lacking control over sleeping and
waking time, lacking control over food / meal times, lacking control over
timing of procedures.
Because of the extended family system practiced around the study area in Nigeria.
Where people stay together in a large family house and children grow up among many
age groups and peers, it is very difficult for a child to cope with isolation as a result of
being sick. Being in a different environment, and not use to eating or sleeping alone
without their siblings and friend. Fear of the unfamiliar and unforeseen, not able to play
at will among peers and move around at the child’s own time. Such situations may add
up to his worries and additional stress during hospital stay.
Another study by Wilson et al. (2010) concurred that children felt lonely and scared in
the absences of their siblings in the hospital environment. They are afraid of routine
experiences and unknown possibilities. It's evident from studies that stress has a natural
9
attachment to hospital stay, an experience which can accumulate and accelerate patient's
sickness. Children respond to these fears by requesting to have parents nearby, having
familiar objects with them in the hospital or asking to go home.
Feeling of Stress and anxietycan be minimized in the cause of children hospital stay,
when children physical and social environment relates to their perception of assumed
hospital settings (Adams et al, 2010). Same study has shown that when children are
involved in studies about matters that concern them, theirneeds will be further
identified, elaborated and taken into consideration. “Play is a child's way of establishing
authentic relationship with the social and physical world” (Moore, 1986). It is important
that children play spaces are transformable, providing “loose parts”, which are items or
materials that children can move, adopt, control, change, and manipulate within their
play (Derr and Kellert, 2012). They are essential elements of a rich childcentred play
environment, which can enhance restoration, with regard to stress, their emotional state,
social connection, physical development, trust and acceptance of routine medication.
To be able to find out the level of awareness, and to investigate on how children are
coping with stress in Nigerian paediatric hospital settings. A preliminary survey was
conducted on 15th January, 2013, atAbubakar Tafawa Balewa University teaching
Hospital Bauchi. 49 questions were given to caregivers with the Nurses as respondents
(male = 10, female = 39). The question is on their level of awareness as caregivers
about the benefits of restoration for hospitalized children. The questions are, (i) Can
play activities enhance patients feeling towards restoration, (91%) are aware of the
effect of the play on hospitalized children, (ii) Can play environment fascinate patients
to behave like healthy children, (81%) believe that it is possible, (iii) Can the ward
viewed as a play environmentto make children feel at home, (89%) agreed, and (iv) Can
play environment, improve on child psychological well-being, (93%). Based on the
analysed result, it shows that there is a greater level of awareness on the part of the
nurses, the majority of the Nurses reported to understand the advantages ofin
cooperatingplay and play activities in the paediatric settings.From another result of
preliminary study, with mothers as respondents, it shows that the greater percentage of
hospitalized children as at the time of the survey are 75% boys and 25% female, from
10
the age of 6 years of 16years which make (57%) of the patient population, on their
length of hospital stay, (62%) have been hospitalized for three weeks. As to their mood
and behaviour during admission, (37%) reported to be in a depressed mood. On the
question of whether the environment can influence changes with regards to their child's
attitude, behaviour, and response to medication, (97%) responded positively as they
equally believe that play can distract and motivates a child when in an environment that
will enable them the chance to be involved in play, especially with their peers.
From the result of the preliminary study, it showed that children do not have the means
of benefitting from any features in the ward environment. As a result, they lack the
needed means of distractions which can improve on their restoration process since their
hospital ward only offers a pathogenesis approach toward medication. This is because
the design and setting of the ward are inclined towards the provision of medical care,
and prevention of the spread of disease.Further discussion with hospital staffs, shows
that the research will be of relevance to the present hospital environment. The
contribution drove from the preferred physical environment towards restoration, and
positive trend towards a feeling of wellness had been pointed by many researchers
(Abbas and Ghazali, 2010). “That the physical environments also contributetowards a
better quality of life not only for the patients, careers and staffs but also the visitors.”
The availability of positive means of distraction can reduce the level of complainingto
the caregivers and equally reduced on their work stress. Having in mind that researches
with children in a hospital context are has a lot of difficulties.Results of similar studies
was conducted by (Bishop and Said, 2012). Lamented on issues that bother around
qualitative research with children, part of it is lack of cooperation from the medical
personals and professionals in the medical circle in accepting this type of research work
looking at it from the point of their professional ethics. Other challenges are associated
with getting the right sample population and for the person conducting the research; he
is faced with the problem of getting ethical approval, having access to the patients at the
appropriate time and the conditions attached to medical protocols. Despite the barrier
between medical norms and play activities in the hospital environment, and if the
research on the restorativeness of play to children is established, then there should be a
way to blind the hospital norms and play together to benefit the hospitalised children.
11
8. RESEARCH GAP
Research on the causes and benefits of restoration, in healthcare environment had been
approached from different perspective of the study.As compiled by Sachs(2013).
Environmental healthcare research that involvestherapeutic,restoration and healing and
is concentrated on the provision of outdoor facilities. Few out of the many studies are
listed in the Table 1.
This shows that most of the researches undertaken are concentrated on the outdoor
environment. Studies in the field of psychological benefits of nature to man have
focused less on the indoor environment(Bringslimark et al,2009).This is a gap that
needs to be attended a research attention, especially in developing countries like
Nigeria, where health institutionscannot maintained a garden or landscape as a result of
finances that will be involved. studyby(Derr and Kellert, 2012).Further stated that less
emphasis is given to indoor environments. Where children activities that involves their
physical, social, and cognitive as well as healing usuallytake place in an indoor
environment, under protection in a conducive atmosphere.
It is evident that stress and anxiety are caused as a result of children's hospitalization
and the need for them to adapt to their new environment, routine and medical
procedures. Moreover, the causes of stresses to children during hospitalization are all
found within the indoor hospital environment. That is why the study tends to look at
how to provide a remedy within the indoor area, not outdoors where restoration can
have an effect after stress and related anxiety has been acquired. The approach in this
study is to provide an avenue fora child’s restoration by looking at the ward as a play
environment in a different dimension from most research and studies on in
therestoration in outdoor environment.
12
Table 1: Selected areas of previousstudies thatcentred on childrenrestorationand their
ability toplayin a paediatric hospital setting during hospitalization
STUDIES IN RELATED FIELD
FINDINGS UNIT OF ANALYSIS
CONTEXT PARAMETERS
Building a model of Holistic Healing environment for children Hospital.Fiona de Vos.2006
- Patients require adequate food and sleep.- Freedom of being part of the decision.- To have a sense of security.- Social support from caregivers and peers.- To be provided with positive distraction, so as to be engaged and have their mind off their sickness.- Freedom of choice, mobility and routine.- Changing the environment settings to make it less stressful.
Children's hospital of Westchester medical centre (WMC) and its replacement. The new Maria Fareri children's hospital (MFCH) in Valhalla New York.
-Children's hospital as holistic healing environment.-Comparing the existing and new hospital.-Understanding the impact of the environment on people.
Garden as a restorative environment for children in Malaysian Hospital.(Said, 2006). Ismail bin Said2006.
- From the findings, it is evident that children interact more actively with the play equipment provided in the Garden than with the plant.- Children preferred manipulating play equipment to the one that is non manipulating.- The conclusion here is that the garden properties that foster restoration process are as a result of the play with features and equipment of the garden.
6 -12 years Children's hospital in Batu Pahat and Segamat hospital both in Malaysia.
-Properties and attributes of garden.-Determining behavioural response in the ward.-Determine change of behaviour with experience attribute of the garden.
Play and playfulness among hospitalized children(Ryan, 2011). Katherine S. Ryan2011
- Study shows that children do play during their hospitalization.- They find ways to play without the help of child life support, parent or other health care worker.- It shows that playfulness usually increases as from admission to the time of discharge.
-Hospital paediatric environment and home play environment.
-How does play occur among hospitalized children?-Evaluate play in hospital and home.
From their perspective children and young people’s experience of a paediatric hospital environment and its
Findings show that understanding what constitutes a child friendly environment are feeling of well-being, person environment fit, and environmental congruence.
6 – 19 years Paediatric hospital environment.
-Children participatory research.-Physical environment to
13
relationship to their feeling of well-being(K. G. Bishop, 2008). Katherine G. Bishop2008
well-being.-Participatory research for design
9. THEORETICAL FRAMEWORK
In recent decades, various studies on health carehave focused on the effect of the
hospital environment in reducing negative experience of hospitalization of patients,
especially children (Monti et al., 2012). Based on research findings, hospital
environmental settings can positively enhance patients'behaviour, stress coping abilities
and improve on their feeling of well being. Furthermore changes in healthcare
environmental settings, giving consideration to users' preferencescan improve on
patientoutcome (Ulrich, 1984; Venderber and Reuman, n.d;Davidson, 1994; Cesario,
2009; Adams et al., 2010;Monti et al., 2012). Facilitates recovery, reduces pain,
improve acceptance of medication and shorten length of hospital stay (Ulrich, 2002).
The study ofthe human needs of nature in an environment is all centredon the Biophilia
concept of Edward O. Wilson. He stated that “The inherent human affinity to affiliate
with natural system and process” (Wilson, 1984).Wilson added that Biophilia is seen as
“The predictable fantasies and response of individuals from early childhood onward. It
cascades into a repetitive pattern of culture across most or all societies, a consistency
often noted in the literature of anthropology” Hedescribes Biophilia as a rule found due
to stimulation, as a result of contact with nature or representation of nature, which cover
the physical, psychological and cognitive benefits. More recent study by (Kellert et al,
2008). Have further elaborate the study to include human activities such as learning,
physical and social experience which can improve on the relationship between human
and their natural environment. The “Biophilia hypothesis and supporting research tell us
that as a species; we are still powerfully responsive to nature forms, processes, and
patterns” (Ulrich, 1993; Kellert et al., 2008).
The perceptionof the restorative benefits of having contact with nature is very old, study
by Ulrich (1984).Tested the effect of window views on hospital patient health outcome,
14
where he noted that patients that have their rooms with windows viewing an outdoor
landscape feature.Withtrees and lawns uses less medication and have a shorter length of
hospital stay. Than those that have their windows focused on viewing an outdoor brick
walling. Before undertaking that research, he conducted a preliminary finding using less
stressed patients that viewed images that portrays natural settings.This shows that the
images of natural settings have a positive emotional shift than those that viewed images
of urban settings. This is to show that viewing natural settings improves one'sbehaviour,
coping abilities from fear and anxiety. Another study by (Moore, 1981).Show similar
evidence, where he recorded 24% of additional sickness increase among inmates whose
prison cells are viewing the prison courtyard, than those whose views are directed to the
farmland.The human linkage with nature is natural, which applied to children. Lack of
access to this natural connection can cause a possible disorder to children physical,
cognitive and social behaviour, such barrier from nature can be as a result of child's
hospitalization. Children are confined within hospital ward environments, which pay
much attention to treatment of sickness, with less effort towards their psychological
well being.
Theories on human development can serve as a guide, and stimulate further inquiry or
research about human cognitive development, behaviour, emotional state and social
interaction with other human in an environment. The history of human psychology
cannot be written without discussing the contribution of the psychoanalytic theories of
(Sigmund Freud; 1856-1939). “He postulated that personality development involves a
series of psychosexual stages. Each stage poses a unique conflict that must be resolved
before passing to the next stage. He proposed the 3 stages of being.The id: which seeks
self gratification? The superego: This seeks what is morally proper. The ego: This is the
rational mediator between the id and superego”.
For Freud, the stages from birth to age 7 years were more important to the development
of the basic personality structure, which he said are of two types and referred to as
periods, latency and genital? Latency period corresponds to the middle childhood years,
where children suppress most of their sexual feelings and become interested in games,
sports, and friendship, boys’ associates with their boys counterpart and girls with girls,
15
sexual reawakening occurs at puberty. The genital period is where young people begin
to experience romantic feelings, emotions and desires to have a satisfactory sexual
relationship. His emphasis is on the environment, not biology or heredity, the principal
factor in mental health and illness. He is famous for formulating psychosexual stages
and therapeutic “technique to bring unconscious thought and feelings to conscious
experience.”
In contrast to Freud’s views, psychiatrist, Miller thought that relationship are the central
needs of human life, and problems are caused by relationship disconnection. She states
that personality growth occurs within a relationship and that an infant responds to the
emotion of caregivers. The goal is to continue to form intimate relationships not for
anatomy or individualism (Miller and Stiver, 1997). Erik Erikson (1902-1994) built his
psychosocial stages of development;his own findings were that personality continues to
develop over the entire life span. His views emphasis on successes, greatness, and
human potentials, his main concern is the psychosocial development of a person within
a social context. This context can be related to paediatric hospital ward, making the
environment conducive for hospitalized children.To be involved with their peers in a
play activity this will result into physical and social interaction. As a result, they will
not miss that stage of development due to illnessand hospitalization. Erikson developed
8 major stages of development with the 9th theory published by his wife which he
passed through before his death. Each stage poses a unique development task and crises
which individual must resolve, he prefers the term (opportunity). The stage that
involves this study is the Industry vs. Inferiority confusion. 6years to stage of puberty.
Children are at this stages are inquisitive and more Curious about how things are made,
formed or work, they want to try and bring out a new thing. They develop a sense
developing out of what they imagined, mastery and competence (Erikson, 1968a).
Another theory that deals with human development is the Behavioural theory, as the
name implies. It is concerned with the observable behaviour of people, “what they
actually do or say”. Behavioural theory are as a result of responding that separated the
environment into units called stimuli, interest is how people learn to behave in a
particular way. Those that formulated the theories are Ivan Pavlov; (1849-1936).John
16
Watson; (1878-1958). B. F. Skinner; (1904-1990).“Says that people do not go through
distinct stages, but do go through a continuous process of behavioural change, due to
respond to environmental influences called external stimuli”. The process whereby an
activity or event strengthens the probability of another activity or event occurring,
e.g.Gift can encourage a child’s school performance. “A psychologisthas understood
that human behaviour is not simply a mechanical process, which involves the bringing
together two activities or events that happen to occur in a context closely in time.
Organisms do not pair events in a vacuum, the environmental context is critically very
important. From cognitive learning perspective, organism only learns when events
violate their expectations”(Watson and Tharp, 2001).
The “third force in psychology in reaction to the established psychoanalysis and
behaviourism is termed humanistic psychology” Human are different from all other
beings, that they can intervene, control and change their destinies, and be able to modify
their environment to suit the way of life. They take a holistic approach, one that views
the human condition in its totality, and each human made-up is more than a collection
of physical, social and psychological components (Maslow, Frager, & Fadiman, 1970).
Abraham Maslow (1908- 1970) and Carl Rogers (1902-1987).“They are concerned with
maximizing the human potentials for self direction and freedom of choice”; (Maslow et
al, 1970; and Rogers, 1970). The Maslow key concept is the hierarchy of needs; he felt
that human beings have certain basic needs that they must meet before they can fulfil
their other developmental needs. The “fundamental needs are food, water and sex, other
needs that focused on belongings are love and self esteem and the need to realize ones
unique potentials to the fullest which he termed self actualization” (Maslow et al.,
1970). Such stated goals in the case of children can be achieved through play, because it
is an avenue for them to explore their potentials. “The goal of humanistic therapy is to
help a person become more self actualized, that is to guide the client to self directed
change. Building self esteem along the way, in contrast to psychoanalysis and behaviour
modification which are directed more by therapists”.
Cognitive psychologist is interested in the “cognitive structures and processes that allow
a person to mentally represent an event that goes on in the environment”.Jean Piaget;
17
(1896-1980). Piaget’s concentrated on changes that occur in the child mode of thought.
Central is the cognitive stage in development, which sequential period in the growth or
individual ability to think, to gain knowledge, self awareness, and awareness of the
environment (Piaget, 1964). Children engage in a continual interaction with their
environment, they act on, transform and modify the world in which they live. In turn
they are shaped and altered by the consequences of these interactions. This interaction
leads to a new perception of the world and the new organization of knowledge.
Basicallyhe saw development as Adaptation, children gradually modify their repertoire
of behaviour to meet environmental demand, by interacting with their environment
during playand other activities, and children construct a series of schemas (concept or
model) for coping with their world. (Schemas are cognitive structures, which people
construct to deal with their environment). Adaptation involves two processes, which are
assimilation and accommodation. Assimilation is the process of taking in new
information and interpreting it to confirm with the current model of the world.
Accommodations is the process of changing one schema to the reality of the world
(Rathunde and Csikszentmihalyi, 2006). A balance between the two is equilibrium.
Another cognitive theory is that of Albert Bandura, “cognitive learning which occurs as
a result of watching other people, we learn new responses without first having the
opportunity to make the responses ourselves”. This process is termed “cognitive
learning” (it is also termed, as observational learning, social learning, and social
modelling) (Bandura, 1975). Further cognitive research is the socio-cultural theory;
“where children socialize to think of themselves as being part of a group or community,
rather than an individual at odds with those in the vicinity” (Views regarding cognitive
and language development). Lev Vygotsky (1896- 1937) is known for his Sociocultural
theory of psychological development. “He assumes that the development of the
individual is determined by the activity group”. The “child will interact with another
person, assimilate the social aspect of the activity and take that information and
internalize it. In this way social values become personal values”(Vygotsky, 1978).
Vygotsky theory “provides a developmental perspective on how such mental functions
as thinking, reasoning, and remembering are facilitated through language.And how
many functions are anchored in the children interpersonal relationship”.
18
Furthermore, other important theory that elaborates on children is theory of play.
“Theoriesof play were first developed during the 18th and 19th centuries”, they show that
“play relates to healing in the physical environment. And there is a relationship between
children and the environment. Play means movement, locomotion, or mobility, play
permits children to learn through experimentation. Means to facilitate children to
explore and manipulate the environment”(Kellert, 2008).
A play which is the most important activity in the lives of children, sometimes more
than eating and sleepingplay is the work, the occupation of childhood, “an
activitypursued without ulterior purpose and on the whole with the enjoyment or
expectation of enjoyment”(English & English, 1958). It aids child’s psychosocial
development (Erikson, 1993). Piaget defines play as “assimilation, child’s efforts to
make the environmental stimuli match his or her own concept”(Piaget, 1962).
According to Cobb,“Play perception is a kind of temporal scanning, a translation of
spatial into temporal pattern”(Cobb, 1959).“Play as an activity which is positively
valued, self motivated, freely chosen, and engaging”(Garvey and Kramer, 1989). Scales
et al. (1991) called play “that is absorbing activity in which young children participated
with enthusiasm and abandon”. According to Mcdevitt and Ormrod (2004) that
“movement is the very centre of children’s life, through movement they perceived a lot
of information about the environment” meaning that children can move and learn about
their environment through play. And of a more recent was study by Said (2006) where
he portrayed play as the physical contact with the environment, and social interaction
with peers. This is possible through a medium where children can have access to play,
and play activities especially in a hospital context.
Other related theories are: Thesurplus energy (Schiller et al, 1967 and Spencer, 1895)
states that “play is the result of surplus energy that exists because the young are freed
from responsibilities, done by the parents”, while Curtis (1915) states that active play is
necessary to get “rid of the surplus”, because children don’t need to expend their energy
on obtaining food, shelter, or provide for living, so the left over energy is being used to
play. They focused on play as a way to recuperate from fatigue experienced from hard
work. In other words, plays restore energy and provide more benefits to the body than

19
idleness. The pre-exercise theory Groos (1985) posits that “play is the necessary
practice of behaviour, which is essential to the later survival”. Examples include playful
fighting of animal or rough and tumble play of children are essential the practice of
skills that will later aid their survival in the future.
Other additional current theories are: Psychoanalytic theory by (Buhler, 1930); Freud,
1937) “they describe play as defensive, as well as adaptations in dealing with anxiety”.
And the Sociocultural theory of Vygotkys, “states that play actually facilitates cognitive
development, children not only practice what they already know, they also learn new
things”. Playing is a behaviour that children participate to explore and learn in their
environment, play develops a number of skills, including fine and gross motor skills,
sensory knowledge, exploring of different roles, development of language skills and
development of social skills, cognitive skills, problem solving and thinking skills. The
value of play is to help children understand the world around them, all children need to
play. The “impulse to play is innate”, the play is a biological, psychological, and social
necessity, and is fundamental to the healthy development and well being of individual
and communities, which can be achieved through complete play cycle during childhood
(Social services directorate - children’s services, 2012).
10. UNDERPINNING
The research underpinnings to this study area are the Psycho-physiological Stress
Reduction Framework by Ulrich (1999) and the Theory of Loose Parts by Nicholson
(1971).
10.1. Psycho-physiological stress reduction framework involves two theories: Attention
Restorative Theory (ART) by Kaplan and Kaplan (1989) states that compatibility is
from the quality of a setting that fits and supports one’s inclinations or purpose, and the
kind of activity supported, encouraged or demanded by the settings (Herzog et al,
2003). In a hospital setting, child associated outdoor space to play it is compatible with

20
children needs because they get the sense of freedom by playing at their own pace, and
time. Therefore, nature matters to children well- being (Whitehouse et al., 2001).
Stress coping reduction theory, SCRT (Ulrich, 1999) proposes that stress is mitigated,
when a person perceives un-threatening natural environment, and the environment
affords him or her following factors;
- Sense of security; to feel secure, children and caregivers from intruders and
other factors related to their environment.
- Sense of control; to have control over their situation, coping with hospitalization
stress and anxiety.
- Social support; emotional support, in form of play from caregivers and peer’s.
- Physical movement and exercise; movement is play of children, and engage with
others in play.
- Access to nature and other positive distraction; having contact with nature, as
play is part of children natural needs.
The theory shows that play relates to restoration in the physical environment, and there
is relationship between children and the features of the environment. Because both
theory deals with the adaptations of human psychological and physiological response
capabilities to natural environment (Persons and Hartig, 2000). People tend to prefer the
natural environment than the built environment, reviewed by (Knopf, 1987); (Hartig,
1993; Ulrich, 1993). An example of such theories that relates to play in stress reduction
is the study of influence of forest topography and vegetation on the physical activity of
playing and motor development of young children. In terms of children environment
interaction, the theories views environment as a source of sensory stimulation and
feedback that triggers the cognitive functioning of the children through play.(Fjørtoft,
2004)
10.2 The theory of “loose parts” by (Nicholson, 1971) posits that loose parts are items
or materials that children and young people can move, adopt, control, change, and
manipulate within their play. He said that “in any environment, the degree of creativity

21
and inventiveness is directly proportional to the number of variables in it”. A beach is a
good example of loose parts environment, with plenty of moveable and adoptable
materials, i.e. sand, water, rock, shell, (that is why children can be able to play for hours
on a beach). Other examples are pine cones, stones, grass, straw, cushions, blankets,
sand, logs, paper, ropes, balls, baskets, crates, boxes, seedpods, fabrics, etc. Children
are drawn to new, interesting and novel items, and have a natural drive and the ability to
decide on what to do with them in their play. (Leave a pile of loose parts, let children
knows they can use them, and keep adults intervention to a minimum). Loose parts are
springboards for play, and are essential elements of a rich child-cantered play
environment which can enhance restoration.
11. Scope of study
The study is about human psychology, in relation to the perceived physical
environment, that includes factors and features that may enhance children restoration in
ahospital context. Observing children, physical, social and cognitive development, the
study will investigate the restorative benefits of play, using loose parts in hospital
settings. Through children’s perception on how their hospital settings should be
arranged, looking at the ward as play environment.
The unit of analysis is the middle childhood paediatric patients; middle childhood is
generally regarded as age range of 6 to 12 years. Studies that have contributed to our
learning and understanding of child development at this period of human development
are Piaget, Erikson, and Harighurst (Piaget, 1962). Explain middle childhood as a stage,
where a child develops a new form of thinking, which he term as stage of concrete
operations. Where logic structures how children understands the relationship in their
settings. One of the major ideas is the concept of reversibility; this is the idea that some
changes can be undone by reversing to an earlier action (Erikson, 1993). Refers to
middle childhood as the most decisive stage, where division of labour occurs. “Stage of
inferiority and confusion where childrenare curious on how things work, they develop a
22
sense of mastery and competence” (Havighurst, 1972). His finding divides the age of
middle childhood into three different stages, which he termed “thrust out of home, into
the peer group, a physical thrust into games and work requiring neuromuscular skills,
and a mental thrust into adult concept, logic, symbols and communication”. At this
stage, human development is of importance, and has relevance to later behaviour,
during adolescence and adulthood. The age range for this refers to children of school
age period. This can be looked at as a period of a child’s learning, adapting to new rules
and routines from new people in a new environmental setting.
The study will be undertaken in two different paediatric wards of Abubakar Tafawa
Balewa University Teaching Hospital in Bauchi. The reason for selecting this hospital is
because it is one of the state specialist hospitals that were built about four decades ago,
and have undergone different phases of administration and development. As a result, it
is now upgraded to university teaching hospital, but nevertheless the system of medical
treatment and procedures have not taken psychological benefits of healing into much
consideration.The result of the study will be applied alongside the conventional medical
routine and protocol in relation to the treatment of patients in the paediatric ward in all
the related hospital in Nigeria.
12. SIGNIFICANCE OF STUDY
The significance of this study is to be able to address the problem statement and
research gap which are being outlined in the earlier part of this research proposal.
i. The study will add to the existing body of knowledge that features and
factors in an environment, which relates with children basic need such as
play, can improve on the child’s performance. Physically, cognitively,
socially, and their ability to cope with stress and anxiety during
hospitalization.
ii. The study will point out the importance of the need for positive distraction
as a vital component of development and surviving skills as anadult in later
wider world.
23
iii. In terms of policies and future designs, it would reveal the importance of the
ward as a restorative environment, from the child's perception as a model for
future development.
iv. A model based on the child's perception and responses on a hospital ward as
a play environment will be used to establish the importance of
restorativealongside medical treatment in the hospital environment. The
model could be proposed to the relevant authorities, for use in future design
and settings of paediatric hospital ward.
13. RESEARCH DESIGN AND VARIABLES
The aim of the research is to investigate the restorative benefits of a paediatric ward as a
play environment, in the context of present day Nigerian paediatric hospital ward. It
will investigate the benefits of play activities using the elements of “loose parts” by
(Nicholson, 1971). In a paediatric ward as a (independent variable) looking at the ward
features like space, size, and form on children’s performance, as a result play activities
and their level of incline positive behaviour physically, socially and cognitively, as the
(dependent variables). It is an established knowledge that play is innate in children, and
very important for a child to undergo a complete cycle of play before adulthood (Perry
et al., 1997). As such, there is a need for children in a hospitalized environment, without
access to any means of positive distraction to benefit from play during their hospital
stay. The anticipated change of feeling from fear full, depression, to a more cheer full,
coping to routine medical procedure is the important consideration in this study.
Play activities during childhood is related to various physical and psychological benefits
leading to research with different approaches to improve on children physical activity
(Active healthy kids Canada, 2010) (AHK).Theconcepts of play activities enlist,
“leisure, occupational, commuting”, which are either structured or unstructured. The
study will look at structured leisure play, which is more inclined toward providing a
change(Tobin et al, 2013).
24
The lack of positive distraction as a prominent feature of the ward, in the form of
structured activities that would improve on patient behaviour in the environment, can be
accessed through thecaregivers, mother by the use of interview questionnaire. The data
will then be analyzed to establish the level of problems encountered as a result of
limitations to providing the needed setting that can improve on patients’ psychological
wellbeing.
For the benefits of play using “loose parts” towards children’s restoration, data would
obtain by means of structured observation as a main tool employing the systematic and
planned procedure. Information about the physical environment and human behaviour
can be directly recorded without anticipating account of others. The observer may be
able to see what participants cannot, it can provide an environment and behaviour of
those that cannot speak for themselves or take part in an interview or complete a
questionnaire.Examples are babies and young children (Taylor, 1984). This relates to
this study as it tends to look at children of middle childhood, it can be used to check
information obtained from another source like interview questionnaire. Data concerning
the duration, the unit of analysis involved, the context in which the behaviour occurs,
and to text pre- existing theories like the loose parts as it is mostly used in children
learning environment,by using “hypothetico-deductive” method(Sapsford and Jupp,
2006).
The third objective will be a participatory method, which involves children showing
their preference through sketch drawings. They would be required to sketch play
element and features on how their hospital ward should be designed as a play
environment. Part of the method will involve, Watcha clip – Draw – and tell. The
explanation of what they draw will be attached to each drawing transcript and analyse
using Nvivo. Data will be collected from children in the controlled experiment ward,
and from children in other ward, this is to get a deeper understanding on children's
preference respond.
25
.
.Figure. 3: VARIABLES AND PARAMETERS
To achieve the stated objectives, the under-listed stages would be followed.
i. Define the study background, related theories on restoration, and the effect
of play on child development.
ii. Define the criteria for types of structured play, materials and elements for
children’s restorative environment.
iii. To undertake a field survey, and data collection.
iv. To analyze the responses of caregivers on play value in an environment such
as a hospital, using descriptive data analysis.
26
v. To analyze the observational behaviour and activities of children, in-terms of
physical activities, social interaction, and cognitive development using
inferential data analysis.
vi. To analyze the perceptual preference responses of children, looking at how
they prefer the wards as a play environment using descriptive data analysis.
vii. To synthesize the needed criteria for a restorative hospital ward for
children’s performance, this can contribute to their coping skills, and
response to routine medication.
viii. Documentation of research findings on the restorative benefits of a
paediatric ward as a play environment, then conclusion of study.
27
Figure 4: Research operational frameworks
14. ANTICIPATED FINDINGS
The study will draw attention to the restoration and its benefits, inherent with play in a
structured children setting, such as hospital context.
i. Positive response to child’s coping ability to hospital stress, anxiety, and
medication routine.
ii. Adapting to changing circumstances.

28
iii. Freedom for physical activities, social interaction and cognitive
development.
Expected findings from this research, will en-lighten us on the need for a
restorativepaediatric hospital ward environment, and form a model for future paediatric
hospital ward environment design.
Fig. 5: showing positive feelings of well being as a result of play in a hospital ward
References
Abbas, M. Y., & Ghazali, R. (2010). Healing environment of paediatric wards. Procedia Social and Behavoiral Science, (5), 658–667.
Active healthy kids canada, A. (2010). Healthy attitudes start ealier than you think the active healthy kids canada report card on physical activity for children and youth. Toronto.
Adams, A., Theodore, D., Goldenberg, E., McLaren, C., & McKeever, P. (2010). Kids in the atrium: comparing architectural intentions and children’s experiences in a
29
pediatric hospital lobby. Social Science & Medicine (1982), 70(5), 658–667. http://doi.org/10.1016/j.socscimed.2009.10.049
Akanidomo, R. D., & Hannah, B. .(n.d.).psychological issues in paediatric surgery.Bandura, A. (1975). Social learning and personality development (Vol. 14).Holt,
Rinehart and Winston New York. Retrieved from http://library.wur.nl/WebQuery/clc/475285
Bandura, A., & McClelland, D. C. (1977).Social learning theory. Retrieved from http://www.jku.at/org/content/e54521/e54528/e54529/e178059/Bandura_SocialLearningTheory_ger.pdf
Bishop, K. G. (2008). From Their Perspectives: Children and Young People’s Experience of a Paediatric Hospital Environment and Its Relationship to Their Feeling of Well-being. University of Sydney.
Bishop, K., & Said, I. (2012). The Experience of Completing Qualitative Participatory Research in a Paediatric Setting: A Cross Cultural Comparison. Procedia - Social and Behavioral Sciences, 38, 73–80. http://doi.org/10.1016/j.sbspro.2012.03.326
Bringslimark, T., Hartig, T., & Patil, G. G. (2009).the psychological benefits of indoor plants: A critical rewiev of the experimental literature. Journal of Environmental Psychology, 29, 422–433.
Buhler, K. (1930).The Mental Development of the Child.A Summary of Modern Psychological Theory.The Mental Development of the Child.A Summary of Modern Psychological Theory. Retrieved from http://www.cabdirect.org/abstracts/19302702439.html
Cesario, S. .K. (2009).designing healthcare environments: part I Basic concept principle and issues related to evidence based design. The Journal of Continuing Education in Nursing, 40(6), 280–89.
Cobb, E. (1959). The ecology of imagination in childhood.Daedalus, 88(3), 537–548.Curtis, H. S. (1915). Education through play.The Macmillan Company.Davidson, A. W. (1994). Banking on the environment to promote human wellbeing: In
A.D.Seidel (Ed) Banking on design? In OK: EDRA (pp. 62–66). Oklahoma city.Derr, V., & Kellert, S. R. (2012).making children environment “R.E.D”. Restarative
environmental design and its relationship with sustainable design.Journal of Children and Youth Environment.
Dise-Lewis, J. E. (1988). The life events and coping inventory: an assessment of stress in children. Psychosomatic Medicine, 50(5), 484–499.
Dunleavy, A., Kennedy, L. A., & Vaandrager, L. (2012). Wellbeing for homeless people: a Salutogenic approach. Health Promotion International. http://doi.org/10.1093/heapro/das045
English, H. ., & English, A. .(1958). a comprehensive dictionary of psychological psychoanalytic terms. New york: David Mckay.
Erikson, E. H. (1993). Childhood and society. WW Norton & Company.Fjørtoft, I. (2004). Landscape as playscape: The effects of natural environments on
children’s play and motor development. Children Youth and Environments, 14(2), 21–44.
Freud, A. (1937). the ego and mechanism of defense. New york: International universities press.
30
Garvey, C., & Kramer, T. L. (1989).The language of social pretend play.Developmental Review, 9(4), 364–382. http://doi.org/10.1016/0273-2297(89)90035-X
Groos, K. (1985). the play of animals play and instinct In J.S. Bruner, A. Jolly, K. Sylva (Ed) play its role in development and evolution. penguin books.
Hall, G. S. (1908). Youth: Its education, regimen, and hygiene. D. Appleton.Hansen-Ketchum, P. A., Marck, P., Reutter, L., &Halpenny, E. (2011).Strengthening
access to restorative places: Findings from a participatory study on engaging with nature in the promotion of health.Health & Place, 17(2), 558–571. http://doi.org/10.1016/j.healthplace.2010.12.014
Hartig, T. (1993).Nature experience in transactional perspective.Landscape and Urban Planning, 25(1–2), 17–36. http://doi.org/10.1016/0169-2046(93)90120-3
Havighurst, R. J. (1972). Developmental Tasks and Education, (3rd ed.). Longman Group United Kingdom.
Herzog T.R., Colleen, Maguire P., &Nebel M.B. (2003).Assessing the restorative components of environments.Journal of Environmental Psychology, 23(2), 159–170. http://doi.org/10.1016/S0272-4944(02)00113-5
Hipp, J. A., &Ogunseitan, O. A. (2011).Effect of environmental conditions on perceived psychological restorativeness of coastal parks.Journal of Environmental Psychology, 31(4), 421–429. http://doi.org/10.1016/j.jenvp.2011.08.008
Jolley, J. (2006). Commentary on Coyne I (2006) Consultation with children in hospital: children, parents’ and nurses’ perspectives. Journal of Clinical Nurisng 15, 61–71. Journal of Clinical Nursing, 15(6), 791–793. http://doi.org/10.1111/j.1365-2702.2005.01465.x
Joye, Y., & van den Berg, A. (2011). Is love for green in our genes? A critical analysis of evolutionary assumptions in restorative environments research.Urban Forestry & Urban Greening, 10(4), 261–268. http://doi.org/10.1016/j.ufug.2011.07.004
Kaplan, R., & Kaplan, S. (1989). The Experience of Nature: A Psychological Perspective (1st ed.). Cambridge University Press.
Kaplan, S. (1995). The urban forest as a source of psychological well-being. Seattle: University of Washington Press.
Kellert, R. S., Heerwagen, J. H., &Mendor, M. (2008).Biophilic Design: The Theory, Science, and Practice of Bringing Buildings to Life. Retrieved from http://bettercities.net/article/biophilic-design-theory-science-and-practice-bringing-buildings-life
Kellert, S. . (2008). Dimension, elements and attributes of boiphilic design: In S.R. Kellert, J.H. Heerwagen and M.L. Mendor. (Ed). biophilic design : the theory, science and practice of bringing building to life. John wiley and sons.
Kemph, J. P. (1969). Erik H. Erikson. Identity, youth and crisis. New York: W. W. Norton Company, 1968. Behavioral Science, 14(2), 154–159. http://doi.org/10.1002/bs.3830140209
Knopf, R. C. (1987). Humanbehaviour cognition and effect on the natural environment In D. stokols and Altman (Ed) (Vol. 1). New york: John wiley.
Lazarus, M. (1883).Uber die Reize des Spiels, von Prof.Dr. M. Lazarus. Berlin: F. Dümmler.
31
Maslow, A. H., Frager, R., & Fadiman, J. (1970).Motivation and personality (Vol. 2).Harper & Row New York. Retrieved from http://www.chaight.com/Wk%2015%20E205B%20Maslow%20-%20Human%20Motivation.pdf
Mcdevitt, T., &Ormrod, J. (2004).Physical, Cognitive and Social-Emotional Human Development. Retrieved May 12, 2013, from http://voices.yahoo.com/physical-cognitive-social-emotional-human-development-586971.html
Miller, J. B., &Stiver, I. P. (1997).The healing connection: How women form relationships in therapy and in life. Beacon Press Boston. Retrieved from http://www.getcited.org/pub/100229212
Mitchell, E. D., Mason, B. S., & Davis, J. E. (1934).The theory of play.American Journal of Physical Medicine & Rehabilitation, 13(4), 267.
Monjour, M., & Yisong, Z. (2012). Health Providers perception of design factors related to physical environment in hospital. Journal of Environmental Psychology, 32, 362–370.
Monti, F., Agostini, F., Dellabartola, S., Neri, E., Bozievic, L., &pocecco, M. (2012).pictorial intervention in a paediatric environment: effect on parental affective perception of the unit. Journal of Environmental Psychology, 32, 216–224.
Moore, E. O. (1981). A Prison Environment’s Effect on Health Care Service Demands.Journal of Environmental Systems, 11(1), 1–1. http://doi.org/10.2190/KM50-WH2K-K2D1-DM69
Moore, R. C. (1986). Childhood’s Domain: Play and Place in Child Development. Chidren Environment Quarterly, 4(1).
Nandineni, R. D. (2013). behavioral study of children in paediatric hospitals: a design perspective. In ICEEBS 2013. Hong kong China.
Nicholson, S. (1971). How not to cheat children: the theory of “loose parts,” 63, 30–35.Perry, C. L., Sellers, D. E., Johnson, C., Pedersen, S., Bachman, K. J., Parcel, G. S., …
Cook, K. (1997). The Child and Adolescent Trial for Cardiovascular Health (CATCH): Intervention, Implementation, and Feasibility for Elementary Schools in the United States. Health Education &Behavior, 24(6), 716–735. http://doi.org/10.1177/109019819702400607
Persons, R., & Hartig, T. (2000).Environmental psychophysiology. In Cacioppo, J.T; Tassinary, L.G and Beratson, G.G. eds Handbook of psychophysiology. cambridge: University press.
Piaget, J. (1962). Play dreams and imitation in childhood. New york: W.W.Norton and company.
Piaget, J. (1964). Part I: Cognitive development in children: Piaget development and learning. Journal of Research in Science Teaching, 2(3), 176–186.
Rathunde, K., & Csikszentmihalyi, M. (2006). The developing person: An experiential perspective. Handbook of Child Psychology. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/9780470147658.chpsy0109/full
Rogers, C. (1970). R.(1970). Carl Rogers on Encounter Groups.New York, Harper and Row.
Ryan, K. S. (2011). Play and Playfulness Among Hospitalized Children: A Mixed Method Analysis. Texas Woman’s University.
32
Sachs, N. (2013). Exploring the connection between nature and health. Retrieved from http://www.healinglandscapes.org/blog/
Said, I. (2006).Garden as restorative environment for hospitalized children.Universiti Teknologi Malaysia.
Said, I. (2008).Garden as restorative environment for hospitalized children.Sapsford, R., &Jupp, V. (2006).Data collection and analysis. SAGE Publications
Limited. Retrieved from http://books.google.com.br/books?hl=pt-BR&lr=&id=ojz9rFCGGnoC&oi=fnd&pg=PP1&dq=%22data+collection+and+analysis%22&ots=ndhzN8yDhT&sig=mN00zwlPXxouNEoQes-WZFRkEHw
Scales, B., Almy, M., Nicolopulou, A., & Erin-Tripp, S. (1991). defending play in the lives of children. In B.Scales, M. Almy, A. Nicolopulou and S. Erin-Tripp eds play and the social context of development in early care and education. New york: teachers college Columbia University.
Schiller, F., Wilkinson, E. M., & Willoughby, L. A. (1967).On the Aesthetic Education of Man: In a Series of Letters. Edited and Tr., with an Introduction, Commentary and Glossary of Terms, by Elizabeth M. Wilkinson and LA Willoughby. Clarendon Press.
social services directorate -childrens services, discinfo@devongovuk. (2012, August 24). Play Theory. Retrieved May 17, 2013, from http://www.devon.gov.uk/de/text/index/childrenfamilies/eycs/eycs-childcareproviders/eycs-childcareproviders-play/disc-newpage-26.htm
Spencer, H. (1895). The principles of psychology (Vol. 4). D. Appleton.Taylor, S. E. (1984). Social cognition.Addison Wesley publishing co.Tobin, D., Nadalin, E. J., Munroe-Chandler, K. J., & Hall, C. R. (2013).Children’s
active play imagery.Psychology of Sport and Exercise, 14(3), 371–378.Ulrich, R. S. (1984). View through a window may influence recovery from surgery.
Science (New York, N.Y.), 224(4647), 420–421.Ulrich, R. S. (1993). Biophilia, biophobia, and natural landscape: In S.R Kellert, E.O.
wilson. (Ed)The Biophilia hypothesis.washington DC: Island Press.Ulrich, R. S. (1999). Effect of garden on health outcomes: theory and research in
healing gardens: thereapeutic benefits and design reccommendation. New york: John wiley and sons.
Ulrich, R., S. (2002). Health Benefits of Gardens in Hospitals.In Plants for People International Exhibition Floriade 2002.Centre for Health Systems and Design Colleges of Architecture and Medicine, Texas A & M University College State, TX 77843.
Varni, J. W., & Katz, E. R. (1997).Stress, social support and negativity in children with newly diagnosed cancer: A prospective transactional analysis, (6), 267–278.
Varni, J. W., Rappaport, L. ., & Talbot, D. (1991).Effect of stress, social support and self esteemto depression in children with limb differences.Archives of Physical Medicine and Rehabilitation, 72, 1053–1058.
Venderber, S., &Reuman, D. (n.d.).Windows view and health status in hospital therapeutic environment.Journal of Architectural and Planning Research, 4, 120–133.
33
Vygotsky, L. (1978). Interaction between learning and development.Readings on the Development of Children, 34–41.
Watson, D. L., & Tharp, R. G. (2001). Self-Directed Behaviour: Self-Modification for Personal Adjustment (8th Ed.). Wadsworth Publishing.
Whitehouse, S., Varni, J. W., Seid, M., Cooper, M. C., Ensgerg, M. J., & Jacobs, J. . (2001). Evaluating a child's hospital garden environment: utilization and consumer satisfaction. Journal of Environmental Psychology, 21, 301–314.
Wilson, E. O. (1984). Biophilia: The human bond with other species. Cambridge, MA: Harvard university of Washington.
Wilson, M. E., Megel, M. E., Enenbach, L., & Carlson, K. L. (2010). The voices of children: stories about hospitalization. Journal of Pediatric Health Care: Official Publication of National Association of Pediatric Nurse Associates & Practitioners, 24(2), 95–102. http://doi.org/10.1016/j.pedhc.2009.02.008
Wundt, W. (n.d.).Die Psychologie in kampfumsDesein (psychological struggle for existence).