Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:613-619
Detection of HSV1 DNA by in situ hybridisation inhuman brain after immunosuppressionJOHN SALDANHA,*t RICHARD NP SUTTON,* ALISON GANNICLIFFE,*BRIAN FARRAGHER,t RUTH F ITZHAKI*
From the Departments of Virology* and Medical Statistics,t University Hospital ofSouth Manchester,Withington Hospital, Manchester, UK
SUMMARY Human brain cells were examined for the presence of herpes simplex virus type 1 (HSV1)DNA sequences by in situ hybridisation. Viral genome was detected in immunosuppressed patientswith virological evidence of past HSV infection but not in immunosuppressed patients with no suchevidence. In patients who had not been immunosuppressed, no HSV DNA sequences were
detectable.
Over fifty years ago, a model for recurrent herpeticdisease proposed that latent infection occurs in sen-sory ganglia.' More recently, co-cultivation studieshave suggested that latent virus is present both inbrain and ganglia. Subsequently, preliminary studiesin this laboratory2 showed, by molecular hybrid-isation to DNA from brain, that herpes simplex virustype 1 (HSVI) DNA sequences were detectable inpatients with chronic but not acute psychiatric diseaseand also in mice six months after infection withHSV1. Since then, various hybridisation studies haveconfirmed the presence of HSV1 sequences in brainsof humans3 and of mice after experimental infec-tion.4s
It is not known whether latent herpes virus affectshost cell metabolism in a manner comparable tocertain persistent viruses, such as lymphocyticchoriomeningitis virus,6 which can turn off thedifferentiation function of a cell without killing it, oreven whether there is any transcription of the latentherpes genome.7~ Possibly the latter is dormant anddamage to the host cell occurs only when the virus isreactivated following immunosuppression or otherstress. Experimental immunosuppression in micebearing latent HSV1 infection leads to reactivation ofvirus in brain and to transient neurological signs.'0 Inman, such effects cannot be determined experi-mentally but in illnesses such as acute leukaemia,both disease and cytotoxic treatment involve immu-nosuppression.tPresent address: Department of Physiology, Royal Free HospitalSchool of Medicine, Rowland Hill Street, London NW3 2PF, UK.
Present address and address for reprint requests: Dr Ruth F Itzhaki,Molecular Neurobiology Laboratory, Department of OphthalmicOptics, UMIST, PO Box 88, Manchester M60 IQD, UK.
Received 30 May 1985 and in final revised form 24 October 1985.Accepted 2 November 1985
Using in situ hybridisation, we have examinedspecimens of brain (obtained post-mortem) from suchpatients, on all of whom, in life, standard diagnosticvirological investigations had been made. Thus wehave been able to answer the questions: is HSV DNAdetectable in brains from patients who had previouslybeen infected with HSV and who were subsequentlyimmunosuppressed?; is it detectable in those patientsnot infected but immunosuppressed, or infected butnot immunosuppressed?From our studies, the detectability of HSVI DNA
in brain has been linked with evidence of previousinfection and with immunosuppression.
Patients and methods
PatientsTwo groups were examined. In one (A), virological studiesin life had been carried out. It included seven patients withacute myelocytic or lymphoblastic leukaemia. All of thesewere immunocompromised; two had received total bodyirradiation as part of a bone-marrow transplant procedure.In another patient of group A, the clinical presentation andpost-mortem histological findings led to a firm diagnosis ofHSV encephalitis; infectious virus was recovered from athroat swab taken shortly before death but no virus wasrecovered from post-mortem brain specimens. In the secondgroup (B), no studies in life had been possible. These patientshad not been immunocompromised, their diagnoses beingdiverse and unrelated to neurological or psychiatric disease.Although no data on past HSV1 infections were availablefor these patients, it can be assumed that the majority hadsuffered a past infection (80%-90% of humans havedetectable antibodies to HSV1I'1). These patients can there-fore be regarded as "controls" for the immunosuppressedpatients.
LABORATORY METHODSVirological investigationVirus isolation Swabs were taken into virus transport
613
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

614
medium and subsequently inoculated into MRC5 humanfibroblast and BK tissue cultures: viruses were identified byneutralisation tests.Electron microscopy (EM) Material from lesions wasplaced on microscope slides and air-dried. The material waslater re-suspended in distilled water and a drop placed on aformvar-carbon-coated EM grid. The sample was thenstained with 3% phosphotungstic acid (pH 6 5) and exam-ined under the electron microscope (AEI, EM 1801 orME6B). Photographs were taken of all positive samples.Serology With slight modifications, the classicaltechnique12 of complement fixation as applied to the diag-nosis of virus diseases was followed. Tests were carried outin plastic microtitre plates. About three 50% haemolyticdoses (HD50) of complement were used and in the titrationof this, any slight anti-complementariness of the standardPublic Health Laboratory Serivice antigens employed wastaken into account. The primary reaction took place at 4°Covernight. Sensitised red cells were added and the secondaryreaction allowed to proceed for one hour at 37°C. End-points were read by interpolation and sera with titres of lessthan 10 were regarded as negative.
DNA-DNA HYBRIDISATION STUDIESPreparation of viral DNA, Vero and HeLa DNA HSV1nucleocapsids were isolated and purified from Vero cellsinfected with HSV1 at a low multiplicity of infection.13DNA was extracted by lysing nucleocapsids in 2% (w/v)sodium dodecyl sulphate (SDS) at 60°C for 30 minutes andpurified by phenol-chloroform extraction and CsCl gradientultracentrifugation. [3HI-labelled HSV1 and A DNAprobes and [32p]-labelled HSV1 DNA were prepared bynick-translation. 14 Vero and HeLa DNA were prepared by amethod using hot SDS which we devised for extractingDNA from human brain.15Hybridisation In situ hybridisation was carried out by amodification of the method of MacGregor and Varley.16The cells were fixed in ethanol-acetic (3:1), pipetted on togelatine-coated slides and fixed at room temperature. Fol-lowing two washes in 2 x SSC (SSC is 0 15 M NaCl,0 015 M trisodium citrate, pH 7 0), the cells were denaturedin 0-1 N NaOH at 20°C for 3 minutes and dehydrated inethanol. [3H}-HSVI DNA probe (specific activity 1-2 xI07 cpm/,ug) was denatured in 0 1 N NaOH, 50% formamideand 4 x SSC at 0°C for 3 minutes. The pH of the mixturewas then adjusted to neutrality with 0 1 N HCI and heat-denatured, sonicated calf thymus DNA and dextran sul-phate were added to final concentrations of 100,pg/ml and10% respectively. Approximately 1 x 105 cpm of probe in30pl was allowed to hybridise to each slide for 16 hours at37°C. Slides were rinsed in 2 x SSC, 0 1% SDS, followed bywashing in 3 changes of 2 x SSC at 65°C for 1 hour, onewash in 2 x SSC, 01% SDS at room temperature for 10minutes, one wash in 2 x SSC at room temperature for 10minutes, one wash in 5% (w/v) trichloroacetic acid at 4°Cfor 5 minutes and 30 minutes washing in three changes of 2x SSC at room temperature. After dehydration in ethanol,slides were coated with Ilford K5 emulsion diluted with anequal volume of distilled water, exposed at 4°C for 14 days,developed, and stained with Giemsa.Controls for hybridisation methods(1) Purity ofprobe It was essential to ensure that our viral
Saldanha, Sutton, Gannicliffe, Farragher, Itzhaki
* 'it 9< 9t; il; f § z <Rea> ~~~~~~~~~~M,>.;Y.
,4~~~
Fig 1 In situ hybridisation of[3H1JHSVJ DNA to (a)HSV-J-infected Vero cells and (b) uninfected Vero cells.(x 1000.)
DNA isolated from Vero cells was free of cellular DNA con-tamination. We found that the Tm (the melting temperatureof duplex DNA which decreases with increase in mis-matched base-pairs) of the DNA in 0-1 x SSC was 82-50C;this corresponds to 65-5% (G + C) (guanine + cytosine)base-pairs, characteristic of HSVI DNA. To check theabsence of appreciable contamination with cellular DNA,dot blot hybridisation17 was used to compare the blackeningproduced by a dot of Vero cell DNA with that of a series ofHeLa cell DNA samples containing different amounts ofadded HSVI DNA, after hybridisation to ["2PI-labelledHSVI DNA. This showed the contamination level to beequivalent to only 0-01-0-05 viral genomes per cell genome,that is, far too low to produce any false positives onhybridisation.(2) Positive hybridisation control The specificity of theHSVI probe was checked by incubation with Vero cells 48hours after infection with HSVI (multiplicity of infection1-2 plaque-forminig units per cell). The majority of cellsshowed a cytopathic effect and this was consistent with
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

Detection ofHSVI DNA by in situ hybridisation in human brain after immunosuppression
each brain specimen by means of cumulative frequencycurves. These show the percentage of grain counts (per cell)greater than (or less than) any selected grain count level.Appropriate percentiles can be obtained from the curves byinspection.
Results
Fig 2 In situ hybridisation of[3H]-A DNA to human brainnuclei (patient mg). ( x 1000.)
heavy labelling (fig la), whereas tests with uninfected Verocells were negative (fig b), no cell having more than sevengrains.(3) Negative hybridisation controls No grains in excess ofthe background level were found when A DNA was used asprobe (fig 2), or when brain samples found to be stronglypositive when examined by our normal procedure weretested without prior denaturation, or when slides weretreated with DNAase after hybridisation. This indicates thatthe grains detected in our test specimens resulted specificallyfrom hybridisation of [3HI-labelled HSVI probe to com-plementary HSVI DNA sequences within the brain cells.(4) The avoidance of observer bias Clinical and virologicalresults were not disclosed until the hybridisation studies hadbeen completed.
Quantitation of in situ hybridisation and its statisticalanalysisGrains were counted in nuclei only as, in the case of neurons,the cytoplasm was usually poorly defined. At least two sepa-rate experiments were carried out on each sample; in each ofthese, grains were counted in about 200 nuclei from at least10 random fields (that is, over 400 nuclei were examinedfrom each sample). For measurement of background levels,we counted the grains present in areas adjacent to or equiv-alent to those of the cells; values of 0-5 grains per area wereobtained (mean of 3).We examined the distribution of grain counts in cells from
Virological investigationsVirological investigations were carried out on the leu-kaemic patients over many months prior to theirdeaths and many specimens were tested (table 1). TheHSV antibody levels are within our normal range forhealthy adults. The short-term standard treatmentregimes with cytotoxic drugs result in considerablesuppression of cellular immunity but, to a much lesserdegree, in impairment of humoral immunity;immunoglobulin and antibody levels remain normal,although the humoral response to a new antigenicchallenge is reduced."8
In four patients, all with antibody, HSV was recov-ered in tissue culture, or identified by electron micros-copy, or both, in specimens taken from peripheralsites (almost invariably oropharynx). This recovery ofvirus confirms unequivocably that these patients (hb,ab, mg, wf) had a latent HSV infection which wascapable of reactivation. In two patients (mf, pj) therewas serological evidence of past HSV infection but noreactivation of virus was observed. In no instance wasvirus detected in post-mortem brain tissue by inocu-lation of tissue culture or by electron microscopy(results not shown in table 1). In patients mb and psthere was no virological evidence of previous HSVinfection. In three other patients (tw, gh, ts), ante-mortem virological studies could not be performedbut it is reasonable to assume that some or all of theseindividuals must have had previous infection withHSV.1
Hybridisation ofHSVJ DNA to brain specimens(1) HSVI DNA sequences in brain cells Smears ofbrain samples (from the temporal lobe) obtainedpost-mortem were studied by in situ hybridisation
Table 1 Results ofroutine virological tests on patients under study
Patient No of sera Minimum titre Maxinum titre No ofspecimens Number yieldingtested tested HSV
hbt 3 40 80 6 1 *mg 6 80 160 12 3*ab 9 <10 80 28 8*wf 5 40 160 22 3*mf 2 160 >320 9 0pj 5 20 80 21 0mb 3 <10 <10 12 0Ps I <10 <10 1 0
*For technical reasons, these strains could not be typed: it is probable that most, or all, were HSVI.tDiagnosed as having HSV encephalitis.
615
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

Saldanha, Sutton, Gannicliffe, Farragher, Itzhaki
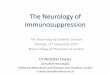
Fig 3 In situ hybridisation of[3H]-HSVi DNA to human brain smears. Small pieces offrozen tissue were smeared onto gelatine-coated slides, fixed in ethanol-acetic acid (3:1) for 20 minutes at 0°C, air-dried and hybridised as describedin Methods. (a) positive neuronal nuclei (patient mg), (b) positive endothelial nuclei (patient mg), (c) negativeneuronal nucleus-arrow (patient pj). Scale bar 6 3 um.
with [3H]-HSV1 probes. The majority of labelled 100- ts gh twP.mf wf ab hbcells were neurons but, in two cases (mg, hb), endo- mthelial cells were also labelled. Figure 3a-c shows pos- 807itive neurons, positive endothelial cells and negative > 80cells. ,
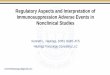
Examination of the cumulative frequency curves 60-(fig 4) indicates differences in median grain counts butmuch more marked are the changes in the distribution a 40-of grain counts at the top two centiles. For this rea- /
Eson, we have rejected the usual significance tests E 20-which examine differences in medians: discrimination u
between positive and negative samples can best be _ _IY//achieved by simple examination of grain count distri- 10 20 30 40 50 60 7(bution, the shape of the whole distribution being the No of grains / nucleusprime indicator. Figure 4 thus shows a clear dis-tinction between cases hb, mg and ab, in which many Fig 4 Percentage cumulative frequency ofnuclei concells have very high grain counts and cases tw, gh and 6 grains or more, plotted against number ofgrains perts, in which few have values above background. In nucleus. The cumulativefrequency curves ofgrains in
caseshb.mg and ab, at least 75% of the nuclei have neuronal nuclei only are shown, exceptfor patient pscases hb, mg and ab, at least 75% of the nuclei have the cumulativefrequency curve ofgrains in endothelia10 or more grains and at least 35% have 20 or more is shown as veryfew neurons were present. For convengrains; these are defined at positive. In cases tw, gh display, experimental points are omitted but all arefitand ts, 90% of the nuclei have 10 or fewer grains; smoothly by the above curves.
ntaining
wherednucleiiience oftted
616
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

Detection ofHSVI DNA by in situ hybridisation in human brain after immunosuppression
Table 2 HSVI DNA sequences in brains ofpatients and controls
Group Patient Immuno- Percentage of cells In situ Virological evidence ofpast HSVcompromised hybridisation infection
with 10 or more with 20 or more summarygrains grains Positive HSV% % serology recovered
A hb - (encephalitis) 92 63 + + + +,I, ab + 85 40 + + + +
mg + 75 35 ++ + +mf +* 68 12 + +wf +* 62 14 + + +pj + 55 7 ? +mb + 44 0
,, ps + 41 7 - -B tw - 10 0 -- NKt NKt
gh _ 10 0 -- NKt NKtts - 0 0 -- NKt NKt
*Including total body irradiation.tNot known.
these are defined as negative.As to the intermediate cases, wf and mf have about
65% of cells with 10 or more grains and about 13%with 20 or more grains; these can be classed as posi-tive. In contrast, in mb and ps, almost 60% of cellshave 10 grains of less and almost none have 20 grainsor more and these can be classed as negative. Case pjremains uncertain.
Table 2 summarises these results.(2) The relation of HSVI DNA sequences in brain toprevious HSV infection HSVI DNA sequences wereclearly detectable in brain tissue from the patient withHSV encephalitis (hb). They were also present inthree patients (ab, mg, wf) with serological evidenceof past HSV infection and with reactivation of virusin the oropharynx, and in one patient (mf) with sero-logical evidence of past infection alone.HSV1 DNA sequences were not present in brain
tissue from two patients with no virological evidenceof past HSV infection (mb, ps). They were not presentin brain tissue from the three patients (tw, gh, ts) withunknown histories of past HSV infection.
There was a statistically signiticant associationbetween the presence of HSV antibodies and the pres-ence of HSV1 DNA sequences in brain tissue (p =0-048, Fisher's exact test). The relationship betweenthe recovery ofHSV from oropharyngeal swabs takenin life and the presence of HSV1 DNA sequences inbrain, although not statistically significant (p =0 143, Fisher's exact test), showed a suggestive trend,in view of the small numbers tested.(3) The relation of HSVI DNA sequences toimmunosuppression HSV1 DNA sequences werepresent in brain from four immunocompromisedpatients (ab, mg, wf, mf) and in one non-immunocompromised patient (hb) with HSV enceph-alitis. They were not- present in three non-immunocompromised patients (tw, gh, ts) or in two
patients with negative histories of past HSV infection(mb, ps).When the patients with negative HSV histories and
the patient with HSV encephalitis were excluded fromanalysis, there was a significant association betweenthe presence of HSV1 DNA sequences in brain tissueand a history of immunosuppression (p = 0-029,Fisher's exact test).
Discussion
We have asked the question "Does immuno-suppression in man result in reactivation of latentHSV in brain tissue?" To answer this, we have pro-duced data which, owing to the present and future useof prophylactic antivirals'9 in patients such as wehave studied, will not be obtainable in future.Our study confirms and extends previous reports
from this laboratory2 and elsewhere3 that latentHSV1 DNA sequences are present in human braintissue in certain cases, and is the first in which clinicaland virological observations of patients have beenmade during life. It indicates that reactivation oflatent virus occurs in immunosuppression; this resultsin a sufficiently high level (that is, in effect, anamplification) of viral DNA in brain to be detectableby in situ hybridisation as well as in recovery of HSV1in throat swabs due to passage of virus distally fromthe ganglia.A novel observation in patients mg and hb, where
the concentration of hybridising sequences (shown bygrain density) was particularly high, was that endo-thelial cells as well as neurons were labelled. Sincelatency is most unlikely to become established in non-neuronal cells, it may be that on reactivation of latentvirus in neurons (for example following immuno-suppression), adjacent non-neural cells become infec-ted but at a level below that detectable by tissue cul-
617
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

618
ture inoculation. In other specimens with somewhatlower grain counts, the concentration of reactivatedvirus may have been insufficient to infect adjacentcells.A recent study by Taylor etal,20 substantiates our
suggestion that immunosuppressiorn-leads effectivelyto "amplification" by reactivation of pre,-existingviral genome, thus increasing its detectability. In 83brain samples from normal individuals and frompatients with Huntington's chorea and schizophrenia,cytomegalovirus DNA was detected by dot-blothybridisation in only one case, this being a normalindividual who had previously been immuno-compromised.20
It is most unlikely that our results are due to thepresence of any sequences in cellular DNA which are
homologous to viral DNA sequences and could there-fore hybridise with probe, giving false positives. Jones(KW) et a12 ' detected sequences homologous toadenovirus 2 genome in human placental tissue butlater22 suggested that pre-existing sequences may
have been amplified owing to the abnormal growthcharacteristics of this tissue. Similar arguments couldapply to the findings of Peden et a123 who used humanplacenta and Puga et a124 who used HeLa and humanleukaemia cell lines and who, by Southern blot,detected homology between the repeated sequences
(the joint regions and the ends) of HSV DNA andcertain intermediate repetitive (G + C) rich cell DNAsequences. However, the latter findings have beenattributed by Jones (TR) and Hyman25 to artefactualhybridisation of G-rich probe (portions of the jointregion comprise over 80% (G + C)) to C-rich humanDNA, on the basis of blocking experiments usingadded poly (U, G).Even if such homologies do exist, a strong argu-
ment against our results reflecting this is that all cellsof a similar type in all our samples would then showa few excess grains, and this is contrary to our
findings. The absence of such hybrids here may be dueto our use of highly stringent conditions and/or thepresence of denatured calf thymus DNA, which con-
tains 35% highly repetitive (G + C)-rich sequencesand could thereby preclude artefactual binding or
binding to homologies by the probe. Alternatively,although in situ hybridisation is a very sensitivemethod for detecting long sequences of DNA such as
the HSV genome, it is insensitive to short sequencesunless the latter are tandemly repeated. Thus, any
homologous cellular sequences which are relativelyshort might not be revealed here even if present inlarge numbers.As to the nature of the latent viral DNA, Rock and
Fraser5 have shown by Southern blot hybridisationthat most or all of the HSV genome is present inlatently infected mouse CNS tissue, possibly in a cir-
Saldanha, Sutton, Gannicliffe, Farragher, Itzhaki
cular or concatenated form. However, a recent studyby Puga et al26 indicates that part of the HSV genomeis rearranged during latency. This would not affect itsdetectability by HSV DNA probe, provided the sizeof the latter were sufficiently small, as it is in our case(approx 100 bases).Our detection of HSV1 genome in the brains of
immunosuppressed patients parallels the results ofKastrukoff et al10 who have shown in latently infec-ted mice, by co-cultivation, that massive immuno-suppression results in a transient infection of theCNS. It should be noted though that studies of ani-mal models may not relate in all aspects with humandisease.27We conclude that immunosuppression in man,
whether iatrogenic (as in our patients) or from natu-ral causes (for example infection28 29 or aging30), maybe associated with reactivation of HSV in the tempo-ral lobes of the brain as well as peripherally. AcuteHSV encephalitis is commonly localised to these lobesand causes serious neuropsychiatric illness. We there-fore speculate that minor degrees of virus reac-tivation, such as we have detected here, could causeless gross but still significant disease, particularly ifreactivation occur repeatedly.
We are greatly indebted to Professor HC MacGregorfor help with in situ hybridisation techniques, Dr HReid for advice on recognition of nerve cell types, DrA Curry for electron microscopy, Dr H Anderson andProfessor BE Tomlinson for brain samples and toMrs R Ward and Mrs DE Monaghan for invaluablehelp.
This work was supported by the Medical ResearchCouncil and the Mental Health Foundation. A pre-liminary report of this work is in press. (Trans Bio-chem Soc.).
References
Goodpasture EW. Herpetic infection with especial refer-ence to involvement of nervous system. Medicine1929;8:223-43.
2 Sequiera LW, Carrasco LH, Curry A, Jennings LC, LordMA, Sutton RNP. Detection of herpes simplex viralgenome in brain tissue. Lancet 1979;ii:609-12.
3 Fraser NW, Lawrence WC, Wroblewska Z, Gilden DH,Koprowski H. Herpes simplex type 1 DNA in humanbrain tissues. Proc Nat Acid Sci USA 198 1;78:6461-5.
4Cabrera CV, Wohlenberg C, Openshaw H, Rey-MendezM, Puga A, Notkins AL. Herpes simplex virus DNAsequences in the CNS of latently infected mice. Nature1980;288:288-90.
s Rock DL, Fraser NW. Detection of HSV- I genome in cen-tral nervous system of latently infected mice. Nature1983;302:523-25.
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from

Detection ofHSVI DNA by in situ hybridisation in human brain after immunosuppression
6Oldstone MBA, Sinha YN, Blount P, et al. Virus-inducedalterations in homeostasis: alterations in differentiatedfunctions of infected cells in vivo. Science1982;218: 1125-7.
'Puga A, Rosenthal JD, Openshaw H, Notkins AL.Homology between murine and human cellular DNAsequences and the terminal repetition of the S com-ponent of herpes simplex virus type 1 DNA. Virology1978;89:102-1 1.
8Tenser RB, Dawson M, Ressel SJ, Dunstan ME.Detection of herpes simplex virus mRNA in latentlyinfected trigeminal ganglion neurons by in situ hybrid-isation. Ann Neurol 1981;11:285-91.
9 Galloway DA, Fenoglio C, Schevchuk M, McDougall JK.Detection of herpes simplex RNA in human sensoryganglia. Virology 1979;95:265-8.
°0Kastrukoff L, Long C, Doherty PC, Wroblewska Z,Koprowski H. Isolation of virus from brain after immu-nosuppression of mice with latent herpes simplex.Nature 198 1;291:432-3.
l Gerdes JG, Smith DS. Recurrent phenotypes and estab-lishment of latency following rabbit keratitis producedby multiple herpes simplex virus strains. J Gen Virol1983;64:2441-54.
12 Bradstreet CMP, Taylor CED. Technique ofcomplement-fixation test applicable to the diagnosis ofvirus diseases. Mon Bull Minist Hith Lab Serv1962;21:96-9.
13Ben-Porat T, Demarchi JM, Kaplan AS. Characterisationofdefective interfering viral particles present in a prepa-ration of pseudorabies virions. Virology 1974;61:29-37.
4Rigby PWJ, Dieckmann M, Rhodes C, Berg P. Labellingdeoxyribonucleic acid to high specific activity in vitroby nick translation with DNA polymerase I. J MolecBiol 1977;113:237-51.
15Saldanha J, Gannicliffe A, Itzhaki RF. An improvedmethod for preparing DNA from human brain. J Neu-rosci Meth 1984;11:275-9.
16 MacGregor HC, Varley JM. Working With Animal Chro-mosomes. Chichester: J Wiley & Sons, 1983:213-26.
17Brandsma J, Miller G. Nucleic acid hybridisation: rapidquantitative screening test of lymphoid cells forEpstein-Barr viral DNA. Proc Nat Acad Sci1980;77:6851-5.
18Dale DC. Defects in Host Defence Mechanisms in Com-promised Patients, In: Rubin RH, Young LS, eds. Clin-ical Approach to Infection in the Compromised Host.New York and London: Plenum, 1981:35-74.
Anderson H, Scarffe JH, Sutton RNP, Hickmott E, Brig-den D, Burke C. Oral acyclovir prophylaxis against her-pes simplex virus in non-Hodgkin lymphoma and acutelymphoblastic leukaemia patients receiving remissioninduction chemotherapy. A randomised double blind,placebo controlled trial. Br J Cancer 1984;50:45-49.
20Taylor GR, Crow TJ, Higgins T, Reynolds G. Search forcytomegalovirus in postmortem brain tissue frompatients with Huntington's Chorea and otherpsychiatric disease by molecular hybridization usingcloned DNA. J Neuropathol Exp Neurol1985;44;2: 176-84.
21Jones KW, Kinross J, Maitland NJ, Norval M. Normalhuman tissues containing RNA and antigens related toinfectious adenovirus type 2. Nature 1979;277:274-9.
22Maitland NJ, Kinross JH, Busuttil A, Ludgate SM, SmartGE, Jones KW. The detection of DNA tumour virus-specific RNA sequences in abnormal human cervicalbiopsies by in situ hybridisation. J Gen Virol198 1;55: 123-37.
23Peden K, Mounts P, Hayward GS. Homology betweenmammalian cell DNA sequences and human herpesvirus genomes detected by a hybridisation procedurewith high-complexity probe. Cell 1982;31:71-80.
24Puga A, Cantin EM, Notkins AL. Herpes simplex virusDNA and mRNA sequences in acutely and chronicallyinfected trigeminal ganglia of mice. Cell 1982;31:81-7.
25Jones TR, Hyman RW. Specious hybridization betweenHerpes Simplex Virus DNA and Human CellularDNA. Virology 1983;131:555-60.
26 Puga A, Cantin EM, Wohlenberg C, Openshaw H,Notkins AL. Different sizes of restriction endonucleasefragments from the terminal repetitions of the herpessimplex virus type 1 genome latent in trigeminal gangliaof mice. J Gen Virol 1984;65:437-44.
27Wildy P, Field HJ, Nash AA. Classical herpes latencyrevisited. In: Mahy BWJ, Minson AC, Darby GK, eds.Virus Persistence. SGM Symposium 1982;33: 133-67.
28Haider S, De Coutinho M de L, Emond RTD, SuttonRNP. Tuberculin anergy and infectious mononucleosis.Lancet 1973;ii:74.
29Bowne TJ, Wedgwood RJ, Ochs HD, Henle W. Transientimmunodeficiency during asymptomatic Epstein-Barrvirus infection. Pediatrics 1983;71:964-7.
30Wedelein C, Bjorkholm M, Holm G, Ogenstad S, Mell-stedt H. Blood T-lymphocyte functions in healthyadults in relation to age. Scand J Haematol1982;28:245-53.
619
by copyright. on M
ay 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.6.613 on 1 June 1986. Dow
nloaded from