Embed Size (px)
DESCRIPTION
Citation preview

01
September-November 2012
A pUbLICAtIoN For prImArY CAre pHYSICIANS
mICA (p) 242/03/2012
A HOLISTIC APPROACH TO
BREAST CANCER
reverSINg oSteoporoSIS
FIx THE LEAk: UrINArY
INCoNtINeNCe
HIgH HEELS ANd YOu: A podIAtrISt’S
perSpeCtIve
03
editor’s notecontents
THE gP BuZZ EdITORIAL TEAm:Lee Wei Kit Jessie tay
Celine ong
AdVISORY PANEL:Associate professor thomas Lew
Associate professor Chia Sing JooAssociate professor Chin Jing Jih
dr Chong Yew Lamdr tan Kok Leong
Joe Hau
We value your feedback on how we can enhance the content of gp buzz. please send in your
comments and queries to [email protected]
© All rights reserved. No part of this publication may be reproduced
or transmitted in any form by any means without prior consent from the publisher.
the biological make-up of males and females are distinct and unique, which explains the complexity of the health
challenges and issues impacting men and women today.
In conjunction with the nation-wide Breast Cancer Awareness Month in October 2012, this issue of GP BUZZ is dedicated to all women (the daughters, mothers and grandmothers) as we unravel the health concerns of the female community.
In Singapore, Breast Cancer is the most common cancer amongst women, with over 1,500 diagnoses every year between 2005 to 2009*. The good news is that Cancer is no longer a death sentence so long as we take active steps to reduce our risks.
Our cover story (Pg 6) on Breast Cancer presents the strides that Tan Tock Seng Hospital Breast Clinic is already making towards establishing a multi-disciplinary treatment approach to combat this disease. We share the story of one Breast Cancer survivor’s treatment journey and the importance of regular screening for early diagnosis and timely treatment. We also pay tribute to our dedicated TTSH Breast Cancer
A dedication to All Women
Support Group Care Advocates for their tireless work and passion in helping patients cope with the healing process (Pg 11). Our Healthy Recipe also features a delicious low-fat, low salt option for cancer patients (Pg 35).
In addition to Breast Cancer, we also feature other pressing health challenges associated with womanhood and share real-life accounts of recovery by our patients. Learn about reversing the effects of osteoporosis (Pg 16), the prevalence of high cholesterol and heart disease in young women (Pg 23), angle closure glaucoma (Pg 12) and urinary incontinence (Pg 26).
Our team of Allied Health Professionals also bring to you a podiatrist’s perspective on prolonged wearing of high heels (Pg 29), managing a healthy diet plan (Pg 20) and targeted exercises for battling those love handles (Pg 32).
We hope you can draw inspiration from the knowledge shared in this issue and help take proactive steps to care for the wonderful women amongst us.
Happy reading!
The GP Buzz Editorial Team
IN EVERY ISSuE
03 editor’s note
04 in the news
05 CMe CALendAr
32 fitness
35 heALthy reCipe
IN THIS ISSuE
06 A Holistic Approach to Breast Cancer
11 Keeping Abreast
12 Angle Closure Glaucoma – An Ocular Emergency
16 Reversing Osteoporosis
20 The Truth About Carbohydrates
23 Understanding Cholesterol and Heart Disease
26 Fix the Leak: Urinary Incontinence
29 High Heels and You: A Podiatrist’s Perspective
September-November 2012
11
29
3216
* Source: the Singapore Cancer registry, Interim Annual registry report, trends in Cancer Incidence in Singapore, 2005-2009 by the Health promotion board, Singapore.
04 05
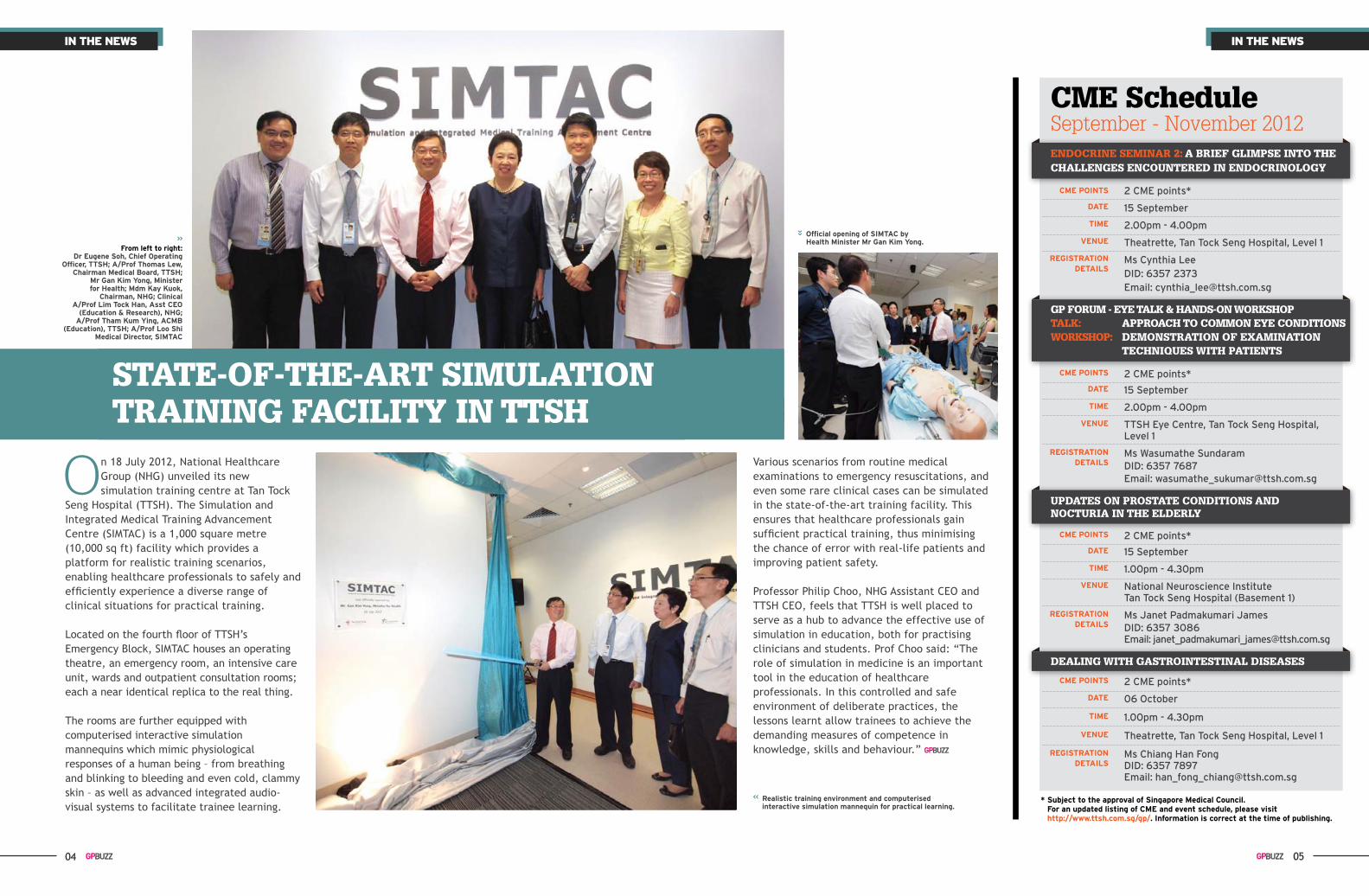
on 18 July 2012, National Healthcare Group (NHG) unveiled its new simulation training centre at Tan Tock
Seng Hospital (TTSH). The Simulation and Integrated Medical Training Advancement Centre (SIMTAC) is a 1,000 square metre (10,000 sq ft) facility which provides a platform for realistic training scenarios, enabling healthcare professionals to safely and efficiently experience a diverse range of clinical situations for practical training.
Located on the fourth floor of TTSH’s Emergency Block, SIMTAC houses an operating theatre, an emergency room, an intensive care unit, wards and outpatient consultation rooms; each a near identical replica to the real thing.
The rooms are further equipped with computerised interactive simulation mannequins which mimic physiological responses of a human being – from breathing and blinking to bleeding and even cold, clammy skin – as well as advanced integrated audio-visual systems to facilitate trainee learning.
CmE Schedule September - November 2012
CMe points
dAte
tiMe
VenUe
reGistrAtion detAiLs
CMe points
dAte
tiMe
VenUe
reGistrAtion detAiLs
CMe points
dAte
tiMe
VenUe
reGistrAtion detAiLs
CMe points
dAte
tiMe
VenUe
reGistrAtion detAiLs
2 CME points*
15 September
2.00pm - 4.00pm
Theatrette, Tan Tock Seng Hospital, Level 1
Ms Cynthia LeeDID: 6357 2373Email: [email protected]
2 CME points*
15 September
2.00pm - 4.00pm
TTSH Eye Centre, Tan Tock Seng Hospital, Level 1
Ms Wasumathe SundaramDID: 6357 7687Email: [email protected]
2 CME points*
06 October
1.00pm - 4.30pm
Theatrette, Tan Tock Seng Hospital, Level 1
Ms Chiang Han FongDID: 6357 7897Email: [email protected]
2 CME points*
15 September
1.00pm - 4.30pm
National Neuroscience Institute Tan Tock Seng Hospital (Basement 1)
Ms Janet Padmakumari JamesDID: 6357 3086Email: [email protected]
ENdOCRINE SEmINAR 2: A BRIEF gLImPSE INTO THE CHALLENgES ENCOuNTEREd IN ENdOCRINOLOgY
gP FORum - EYE TALk & HANdS-ON WORkSHOPTALk: APPROACH TO COmmON EYE CONdITIONSWORkSHOP: dEmONSTRATION OF ExAmINATION TECHNIquES WITH PATIENTS
dEALINg WITH gASTROINTESTINAL dISEASES
uPdATES ON PROSTATE CONdITIONS ANd NOCTuRIA IN THE ELdERLY
Various scenarios from routine medical examinations to emergency resuscitations, and even some rare clinical cases can be simulated in the state-of-the-art training facility. This ensures that healthcare professionals gain sufficient practical training, thus minimising the chance of error with real-life patients and improving patient safety.
Professor Philip Choo, NHG Assistant CEO and TTSH CEO, feels that TTSH is well placed to serve as a hub to advance the effective use of simulation in education, both for practising clinicians and students. Prof Choo said: “The role of simulation in medicine is an important tool in the education of healthcare professionals. In this controlled and safe environment of deliberate practices, the lessons learnt allow trainees to achieve the demanding measures of competence in knowledge, skills and behaviour.”
STATE-OF-THE-ART SImuLATION TRAININg FACILITY IN TTSH
IN THE
NEWS
IN THE
NEWS
from left to right: dr eugene soh, Chief operating
officer, ttsh; A/prof thomas Lew, Chairman Medical Board, ttsh;
Mr Gan Kim yong, Minister for health; Mdm Kay Kuok,
Chairman, nhG; Clinical A/prof Lim tock han, Asst Ceo
(education & research), nhG; A/prof tham Kum ying, ACMB
(education), ttsh; A/prof Loo shi Medical director, siMtAC
official opening of siMtAC by health Minister Mr Gan Kim yong.
realistic training environment and computerised interactive simulation mannequin for practical learning.
* subject to the approval of singapore Medical Council. for an updated listing of CMe and event schedule, please visit http://www.ttsh.com.sg/gp/. information is correct at the time of publishing.
in the newsin the news
06 07
the Breast Clinic at Tan Tock Seng Hospital (Breast Clinic@TTSH)
was established in 2009 with the vision to improve the treatment outcomes and enhance the healing journey of our patients.
Two years into its establishment, the Breast Clinic@TTSH achieved same day imaging for up to 50% of our patients, reaching our target of cutting down diagnosis to within two weeks of first consultation. This was an important milestone as it reduced patients’ anxieties, especially for those found with benign tumours.
The team continues to work at increasing this percentage of
diagnosis within two weeks of first consultation.
The next milestone would be to continuously improve the treatment outcomes for our breast cancer patients.
early Screening is ImportantThe nation-wide BreastScreen Singapore programme (modeled after the Australian national screening programme), celebrates its 10th anniversary this year. Although Singapore is one of the only countries in Asia with a nation-wide screening programme to identify more patients at an early stage, we still struggle to reduce mortality caused by breast cancer.
Disclaimer: The workflow depicted may vary with the individual patient’s condition and is not a standard workflow.
GP / Polyclinic refers patient to The Breast Clinic.
1 week Post-operation.Patient returns for follow-up. Surgeon will also present the proposed post-operation treatment plan.
On the same day patient will see:- Surgeon- Breast Care Nurse- Radiation Oncologist (if necessary)- Medical Oncologist (if necessary)
Patient arrives for appointment, where Mammogram and Ultrasound are done before seeing Surgeon.
Surgeon reviews the results with patient and Trucut Biopsy is done if necessary.
Another appointment is scheduled to review Biopsy results.
Appointment is fixed and patient is informed.
Breast Clinic retrieves referral letters on weekly basis. Surgeon-on-duty will screen each referral letter to decide if patient needs Mammogram or Ultrasound.
Mammogram or Ultrasound is booked on the day patient arrives for first appointment at The Breast Clinic. Surgery
Clinic receives referral letter from TTSH Contact Centre.
Surgeon advises surgery. Patient will also meet with Plastic surgeon if necessary.
1 week Post-operation.The Breast Tumour Board meeting is held in the morning. Multi-disciplinary specialists are present to discuss each patient’s case and to propose the most suitable treatment plan according to each patient’s condition.
Specialists will then go to their allocated Consultation Rooms to see patients whose treatment plan will involve their discipline.
Surgery
1 week 3 days - 1 week 1-2 weeks 1 week
What you don’t see...
Figure 1:the new visit flow for patients at the breast Clinic@ttSH
cover storycover story
We recognise that the low screening rates of 30-40% is the main reason affecting mortality and with other centres in Singapore still seeing symptomatic patients at a late stage. Another possible reason is the failure to provide appropriate and timely treatment.
A recognised process for treatmentThe Breast Clinic@TTSH developed a seamless and
A HOLISTIC APPROACH TO
holistic patient visit flow which shortened the time from diagnosis to treatment for patients (refer to Figure 1). Major studies have shown that multi-disciplinary management improves survival rates in patients.
Many of the elements highlighted in the new patient visit flow meet the international criteria (required for certification of breast centres) and is proof
that the centre is optimally equipped to treat breast cancer patients. These practices have been adopted widely in countries such as the United States (National Accreditation of Breast Centres) and Europe (EUSOMA).
patient-centred treatment As much as we are striving for clinical excellence, we understand that each breast cancer patient is unique as conditions and needs would

08 09
vary. Given the vast expanse of medical knowledge and the variety of treatments needed for each breast cancer patient, a single medical professional will not have the full capability of treating this disease.
The Breast Clinic@TTSH conducts regular multi-disciplinary team (MDT) meetings where all clinicians in varied specialities come together to discuss the management of each breast cancer patient; share medical knowledge of each patient’s tumour characteristic; and the patient’s psychosocial uniqueness. With our breast cancer patients, there is not just one standard protocol or a pathway but a unique treatment angle for each.
The emphasis of MDT is on collaborative decision-making and treatment planning. The concept of a multi-disciplinary forum to share knowledge among clinicians from different disciplines is not new to oncology.
Holistic Approach to recoveryAt the Breast Clinic@TTSH, we adopt a holistic approach
Dr Chen Jia Chuan, JulianaDr Juliana Chen is the Clinical Director and Consultant at The Breast Clinic@TTSH. She did her post-graduate fellowship training at NSW Breast Cancer Institute at Westmead Hospital Australia. Dr Chen is also actively involved in the TTSH Breast Cancer Support Group.
References 1. The requirements of a specialist breast unit, EUSOMA, Eur J Cancer 36(2000) 2288-22932. Certification of breast centres in Germany: proof of concept for a prototypical example of quality
assurance in multidisciplinary cancer care, Brucker SY, Bamberg M, Jonat W et al, BMC Cancer 2009, 9:228
3. Multidisciplinary breast centres in Germany: a review and update of quality assurance through benchmarking and certification, Wallwiener M, Bruker SY, Wallwiener D. The Steering committee, Arch Gyanecol Obstet 2012, 1671-1683
4. Developing and measuring a set of process and outcome indicators for breast cancer. Stordeur S, Vrijiens F, Devriese S et al. The Breast 21(2012): 253-260
5. Cancer multidisciplinary Team Meeting: Evidence, Challenges and the Role of Clinical Decision Support Technology. Patkar V, Acosta D, Davidson T et al International Journal of Breast Cancer 2011
the Multi-disciplinary Breast team
With our breast cancer patients,
there is not just one standard protocol or
a pathway but a unique treatment
angle for each.
cover storycover story
to healing. This has been highlighted in the international breast centre accreditation which places emphasis on outreach activities not just to the general public but also to the cancer survivors.
Through support group activities and programmes for our breast cancer patients, we aim to further enhance and care for their health and well-being. We hope to support and transit our patients from their treatment and ease them back into their normal lives.
While we forge ahead for more effective treatment outcomes for breast cancer, regular breast screenings are still pivotal to the timely and successful treatment of this condition.
As GPs (General Practitioners) taking on the important role in primary care, you are uniquely poised in encouraging women to do their regular breast checks and go for timely breast screenings and seek early treatment. Early detection can improve breast cancer outcomes and survival rates.
10 11
New Lease Of Life After breast CancerGloria was healthy for most of her 48 years until April 2010, when she found out that she had contracted Stage Two cancer in her right breast.
It was a chance observation after a shower that she noticed in the bathroom mirror that the size of her breasts were uneven. Upon self-examination, the mother-of-two felt a hard lump in her right breast. Concerned, she made an appointment immediately for a mammogram at Sengkang Polyclinic in May 2010.
The results of the mammogram were not encouraging, and Gloria visited Tan Tock Seng Hospital (TTSH) for detailed tests.
At the Breast Clinic in TTSH, Gloria underwent a thorough mammogram, ultrasound and biopsy. She received her results within the same day and it was confirmed that she had Stage Two breast cancer, and that a mastectomy was required.
An operation date was set in mid-July. However, the day before the surgery, Gloria decided to take a chance on a friend’s recommendation to seek treatment from a Chinese physician instead, and cancelled the surgery.
“I was so scared. All I wanted was to remove the cancer from my body as soon as possible, but at the same time, I was terribly afraid of surgery and how I would look like after the procedure.”
For the next few months, Gloria underwent a regime of taking traditional Chinese medication and did not seek further treatment at the hospital.
“My friends who knew that I had cancer and was taking herbs all told me I was looking better. However, I knew deep down that the cancer in my body was still there.”
In late October 2010, Gloria returned to TTSH for treatment and saw Adj Asst Prof Patrick Chan, Chief of Specialty and Senior Consultant at The Breast Clinic@TTSH.
I knew I did not have much time left to spare. I wanted a doctor whom I
could have confidence in treating my condition.
By November, Gloria underwent a full mastectomy on her right breast with reconstruction. The operation was a success and she experienced little pain post-surgery. However, Gloria still had to undergo chemotherapy and radiation therapy to clear the cancer entirely from her body.
It was a trying time emotionally and physically for Gloria as she struggled to cope with the side effects of fatigue, nausea, and hair loss from the chemotherapy and radiotherapy. She was also very conscious of the physical loss of her right breast.
It was at this time that Gloria got involved in the TTSH Breast Cancer Support Group, which is coordinated by the doctors, nurses and staff of the Breast Clinic.
Currently, Gloria is cancer-free and enjoying life with her new-found friends she has made from the TTSH Breast Cancer Support Group. Apart from regular meet up sessions with them, Gloria has learnt to make time for regular exercises such as qi gong, zumba and yoga.
She is now always ready to lend a listening ear and share advice with other breast cancer patients. “Be positive and look on the bright side. You are not alone in this journey.”
The TTSH Breast Cancer Support Group was initiated by clinical staff and has garnered continuous support from our members through their active involvement and participation in the outreach activities.
Members with common interests were brought together to work towards the goal of supporting women in their battle against breast cancer. Apart from the creation of social platforms for our patients and survivors, the handmade crafts from our past activities and workshops also helped raise money for the Breast
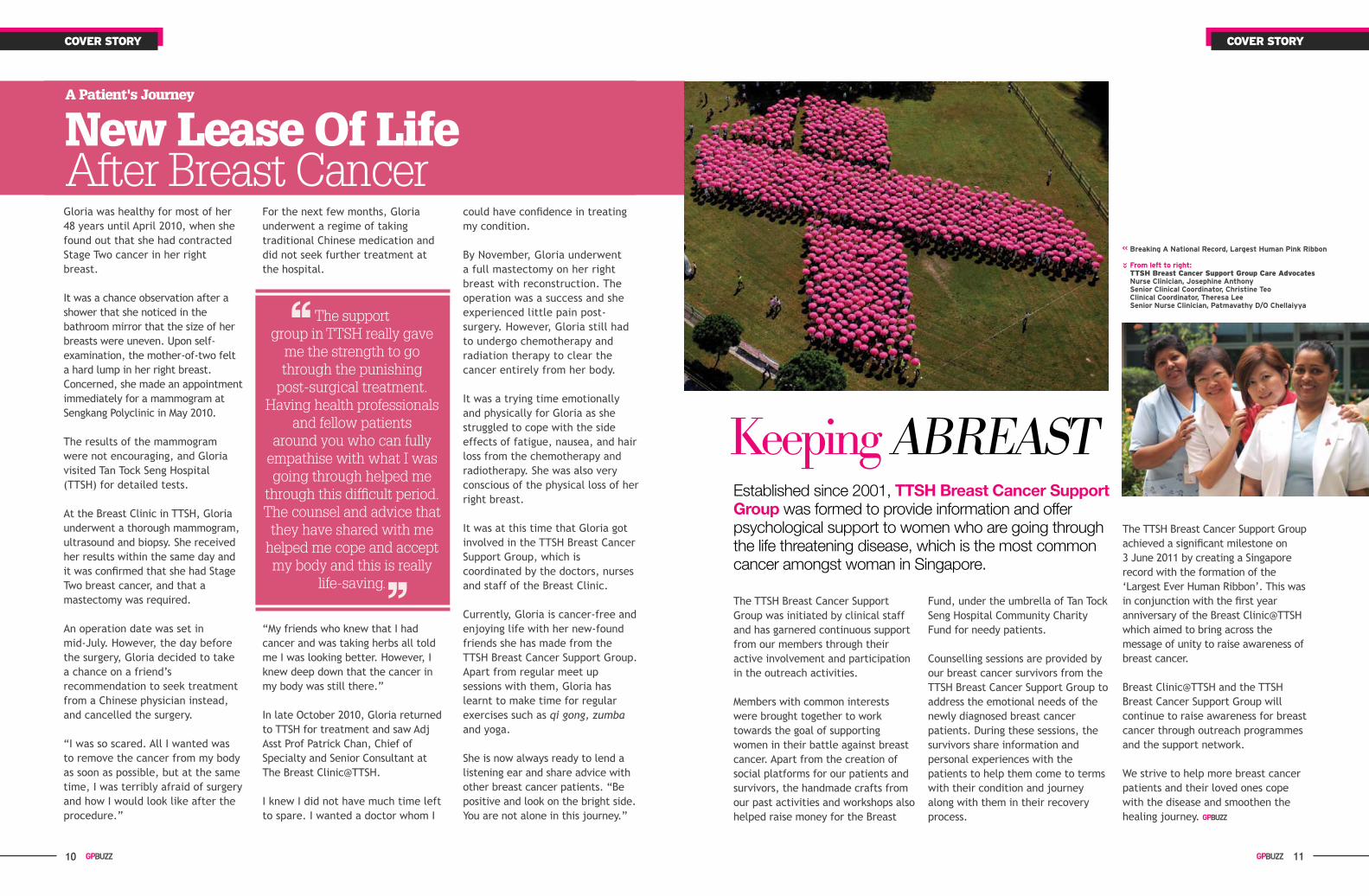
Keeping ABREASTEstablished since 2001, TTSH Breast Cancer Support Group was formed to provide information and offer psychological support to women who are going through the life threatening disease, which is the most common cancer amongst woman in Singapore.
Fund, under the umbrella of Tan Tock Seng Hospital Community Charity Fund for needy patients.
Counselling sessions are provided by our breast cancer survivors from the TTSH Breast Cancer Support Group to address the emotional needs of the newly diagnosed breast cancer patients. During these sessions, the survivors share information and personal experiences with the patients to help them come to terms with their condition and journey along with them in their recovery process.
The TTSH Breast Cancer Support Group achieved a significant milestone on 3 June 2011 by creating a Singapore record with the formation of the ‘Largest Ever Human Ribbon’. This was in conjunction with the first year anniversary of the Breast Clinic@TTSH which aimed to bring across the message of unity to raise awareness of breast cancer.
Breast Clinic@TTSH and the TTSH Breast Cancer Support Group will continue to raise awareness for breast cancer through outreach programmes and the support network.
We strive to help more breast cancer patients and their loved ones cope with the disease and smoothen the healing journey.
Breaking A national record, Largest human pink ribbon
from left to right:ttsh Breast cancer support Group care Advocatesnurse Clinician, Josephine Anthonysenior Clinical Coordinator, Christine teoClinical Coordinator, theresa Leesenior nurse Clinician, patmavathy d/o Chellaiyya
cover storycover story
A Patient's Journey
the support group in ttSH really gave
me the strength to go through the punishing
post-surgical treatment. Having health professionals
and fellow patients around you who can fully
empathise with what I was going through helped me
through this difficult period. the counsel and advice that they have shared with me
helped me cope and accept my body and this is really
life-saving.
12 13
Angle Closure Glaucoma
– An Ocular EmergencyAcute angle closure glaucoma is one of the most common of all ocular
emergencies which affects the Asian population, especially elderly Chinesewomen. As it is potentially sight threatening, a correct diagnosis
with immediate institution of appropriate treatment measures is critical to ensure the best possible outcome.
glaucoma, according to statistics compiled by the World Health Organisation,
remains the second most common cause of blindness worldwide after cataract. The majority of this sight-threatening glaucoma is of the open angle type, an asymptomatic disease that slowly but surely robs the individual of sight while often remaining undetected until a late stage. As a result, this characteristic has earned it the moniker ‘The silent thief of sight’. In Asia, however, the narrow angle type of glaucoma is prevalent and associated with a much more dramatic clinical presentation.
Acute angle closure glaucoma (AACG) is one of the most common ocular emergencies, and is characterised by very high intraocular pressures (IOP). Also potentially sight threatening, the success of its treatment rests on early interventional measures aimed at reducing the IOP as rapidly as possible.
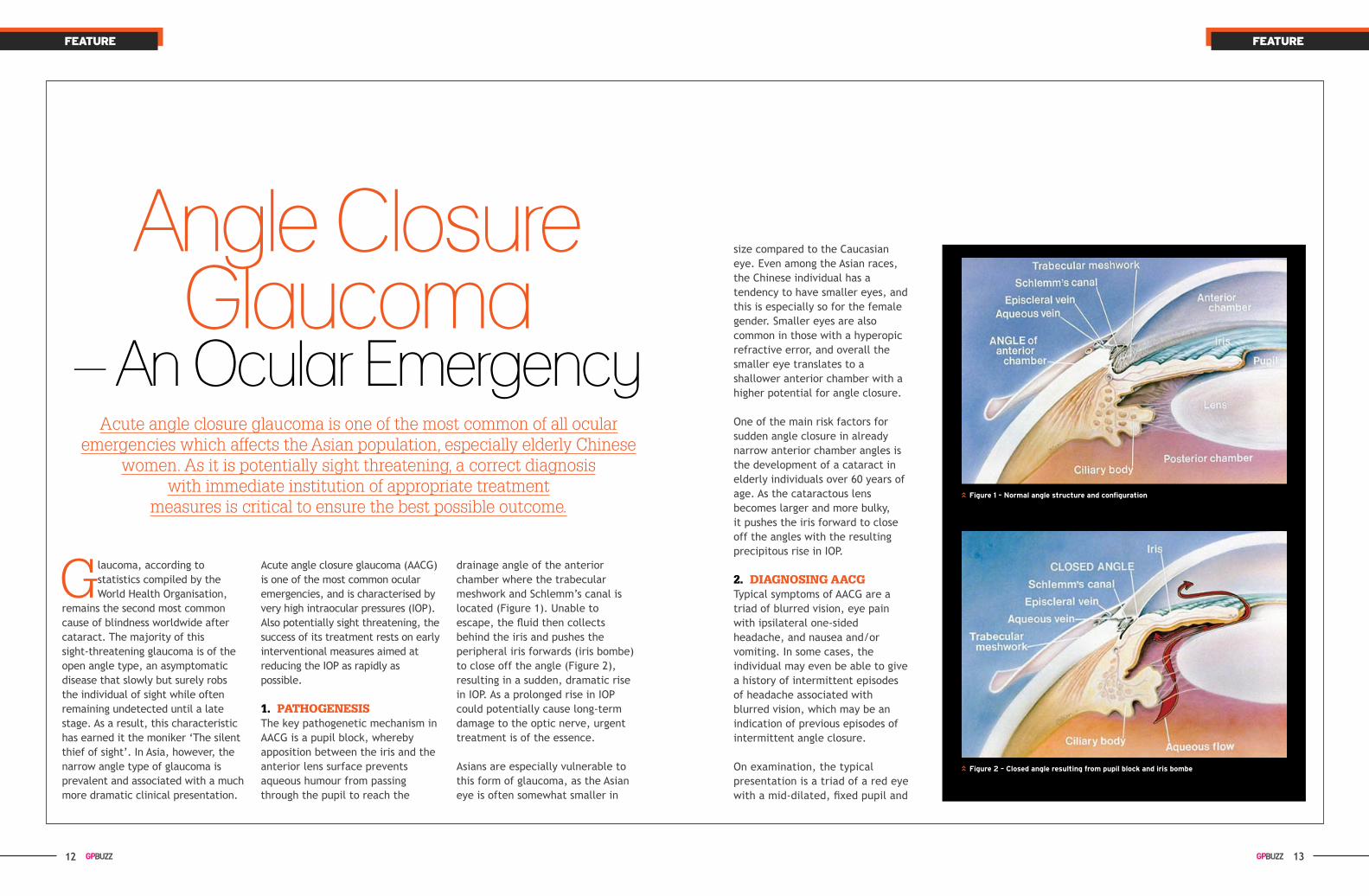
1. PATHOgENESISThe key pathogenetic mechanism in AACG is a pupil block, whereby apposition between the iris and the anterior lens surface prevents aqueous humour from passing through the pupil to reach the
drainage angle of the anterior chamber where the trabecular meshwork and Schlemm’s canal is located (Figure 1). Unable to escape, the fluid then collects behind the iris and pushes the peripheral iris forwards (iris bombe) to close off the angle (Figure 2), resulting in a sudden, dramatic rise in IOP. As a prolonged rise in IOP could potentially cause long-term damage to the optic nerve, urgent treatment is of the essence.
Asians are especially vulnerable to this form of glaucoma, as the Asian eye is often somewhat smaller in
size compared to the Caucasian eye. Even among the Asian races, the Chinese individual has a tendency to have smaller eyes, and this is especially so for the female gender. Smaller eyes are also common in those with a hyperopic refractive error, and overall the smaller eye translates to a shallower anterior chamber with a higher potential for angle closure.
One of the main risk factors for sudden angle closure in already narrow anterior chamber angles is the development of a cataract in elderly individuals over 60 years of age. As the cataractous lens becomes larger and more bulky, it pushes the iris forward to close off the angles with the resulting precipitous rise in IOP.
2. dIAgNOSINg AACgTypical symptoms of AACG are a triad of blurred vision, eye pain with ipsilateral one-sided headache, and nausea and/or vomiting. In some cases, the individual may even be able to give a history of intermittent episodes of headache associated with blurred vision, which may be an indication of previous episodes of intermittent angle closure.
On examination, the typical presentation is a triad of a red eye with a mid-dilated, fixed pupil and
feAturefeAture
figure 1 – normal angle structure and configuration
figure 2 – Closed angle resulting from pupil block and iris bombe

14 15
Dr Vernon YongDr Vernon Yong is the Deputy Director and Senior Consultant at the National Healthcare Group Eye Institute @ Tan Tock Seng Hospital. Dr Yong underwent a one-year fellowship at the Lions Eye Institute in Perth Australia. His interests are in treating an aging population for glaucoma and population screening.
Dr Jeanne OgleDr Jeanne Ogle is a Principal Resident Physician at the National Healthcare Group Eye Institute @ Tan Tock Seng Hospital. She obtained her Fellowship from the Royal College of Surgeons (Edinburgh) and also holds a Masters Degree in Ophthalmology from the National University of Malaysia. Her area of interest is glaucoma and in addition to clinical work, she is also involved in teaching optometrists, medical students, and advanced diploma nursing students.
The pain on the right side of her head was unbearable and so Madam How Suet Keng, 69, admitted herself to the Emergency Department of Tan Tock Seng Hospital (TTSH) on the Sunday evening of 2 August 2009. That day, apart from the throbbing pain in her head that extended down to her nose, Madam How complained of redness and blurred vision in the right eye.
As a full time homemaker, Madam How’s time was divided between household chores and ferrying her grandson to and from childcare. In her leisure time, she would join her friends from the neighbourhood in Woodlands for a karaoke singing session.
In 2008, however, Madam How’s life was disrupted by perpetual
Worsening headachescan mean something
serious. In the case ofmadam How Suet Keng,
serious consequences could have followed if
she had not sought treatment in time.
headaches on the right side of her head, which she thought were caused by the hot and humid temperature in Singapore. She did not pay very much attention to this since the pain was relieved by over-the-counter painkillers or medications prescribed by her General Practitioner (GP). However, the headache on the right side of her head took a turn for the worse. At night and in the dark, she also complained of seeing sudden sparks of red light.
Finally, after much persuasion from her daughter and on the recommendation of her GP, Madam How visited TTSH on 2 August 2009. In the Emergency Department, she was found to have acute angle closure glaucoma and cataract in the right eye. Appropriate medications were quickly administered before laser peripheral iridotomies were
done in both eyes on the same day resulting in quick relief of her headache.
Upon more detailed checks and follow-up by Dr Leonard Yip, Senior Consultant of the National Healthcare Group Eye Institute @ Tan Tock Seng Hospital, Madam How’s intraocular pressure in the right eye remained high despite the treatment given. Dr Yip then went on to recommend combined cataract and glaucoma drainage surgery for Madam How.
Post surgery, Madam How’s recovery and rehabilitation journey was smooth. She was advised to wear an eye-shield while asleep at night for the first week, avoid carrying heavy items, and also avoid any water from splashing into her eye.
On the day after the surgery, Madam How came back to TTSH for a follow-up and Dr Yip found that her intraocular pressure was well under control. Madam How now only visits TTSH every six months for regular check-ups since she has made a full recovery. She has resumed her usual lifestyle and rejoined her karaoke mates for her weekly singing sessions.
When asked about what she gleaned from this episode, Madam How said: “Do not ignore headaches and minor aches and see a doctor early. For glaucoma patients, treat the condition early when it is still not a big issue”. “My neighbour who was formerly a white collar professional before his retirement is now blind since he did not seek timely treatment.” Madam How added.
figure 3 – A patent laser peripheral iridotomy (arrow)
a hazy, oedematous cornea. The peripheral iris is often in a forward-bowed (bombe) configuration, evidence of the underlying pupil block mechanism. In addition, the eye would likely be ‘rock-hard’ to palpation because of the very high IOP.
3. EmERgENCY TREATmENT mEASuRES
In an ocular emergency, immediate referral to an eye specialist for
further management is warranted and the mainstay of treatment is a laser peripheral iridotomy (Figure 3), which alleviates pupil block and re-establishes aqueous outflow, thereby resulting in a drop in the IOP.
4. CONCLuSIONAACG is an ocular emergency that we need to be vigilant for in our ageing population given its propensity for affecting Chinese females aged 65 years and above. As it is potentially treatable, a correct diagnosis and rapid appropriate intervention is critical to ensure the best possible visual outcome.
feAturefeAture
Saved From
Blindness By Timely Treatment
A Patient's Journey
16 17
It is estimated that there are approximately 1.6 million hip fractures in the
world today. This epidemic would increase to over six times by the year 2050. This implies a heavy health bill to both the rich and poor nations, not to mention the resultant morbidity and mortality.
osteoporosis LAndscApe in sinGAporeOsteoporosis is a bone and endocrine disease in which there is reduction of density and quality (micro-architecture) of the bone, leading to fragility of the skeleton. The bones then have a propensity for fracture. The bones that are likely to fracture include the hip, the spine and the wrist.
Post-menopausal women and both elderly men and women are most susceptible. The World Health Organisation considers osteoporosis second only to cardiovascular disease as a global healthcare
reverSINg oSteoporoSIS
problem. This is very pertinent to Singapore.
The Ministry of Health has stated that the prevalence of osteoporosis in Singapore is very much similar to that of Europe and USA. In the three decades since the 1960’s, the number of osteoporotic hip fractures has increased five-fold from 75 cases to 403 cases per 100,000 population in women over the age of 50 years and this figure will set to increase with the ageing Singapore population.
Some 800 to 900 osteoporotic hip fractures occur annually in Singapore. Approximately one in five patients died within one year of the fracture, and one in three became wheelchair bound or bedridden.
why women Are more prone to osteoporosisThe prevalence of osteoporosis is higher in women. This is due to the fact that women are generally smaller than men. Women
usually have a lower peak bone mass to start with.
Men do most of the heavy manual and physical work. Heavyweight bearing and muscular activities lead to denser bones. Moreover, women at menopause (usually between 45-52 years), have their oestrogen and progesterone levels drop fast. It is possible that menopausal women lose up to a fifth of their bone mass five to seven years after menopause. This often leads to the development of osteoporosis.
In men, however, testosterone levels are maintained up to 70 years; therefore men generally develop osteoporosis much later.
effects of osteoporosisMost people believe that osteoporosis is benign and is part of the normal ageing process. This is not true as the osteoporosis can potentially limit the mobility of the
patient, lead to disabilities or even cause death.
Statistics have shown that about one in five persons will die within the year of sustaining an osteoporotic hip fracture and one in three will become wheelchair-bound or bed-ridden.
The possible effects of osteoporosis are: i. hip frActuresThese are serious effects of osteoporosis. If untreated, pain, loss of mobility, malunion, leg shortening and deformity can develop. The mortality rate of hip fracture patients in their advanced age and with comorbidities is 20% within a year of the diagnosis. 30% of them would be wheel-chair or bed-bound.
Surgery is recommended to fix the fractures or to replace the femoral component of the hip joint (Figure 1 and 2). The patient would however be subjected to anaesthetic and operative risks.
feAturefeAture
osteoporosis (the “brittle bone” condition) has now silently become a global health problem. It is called the ‘silent’ disease
because the inexorable bone loss comes with no symptoms.
18 19
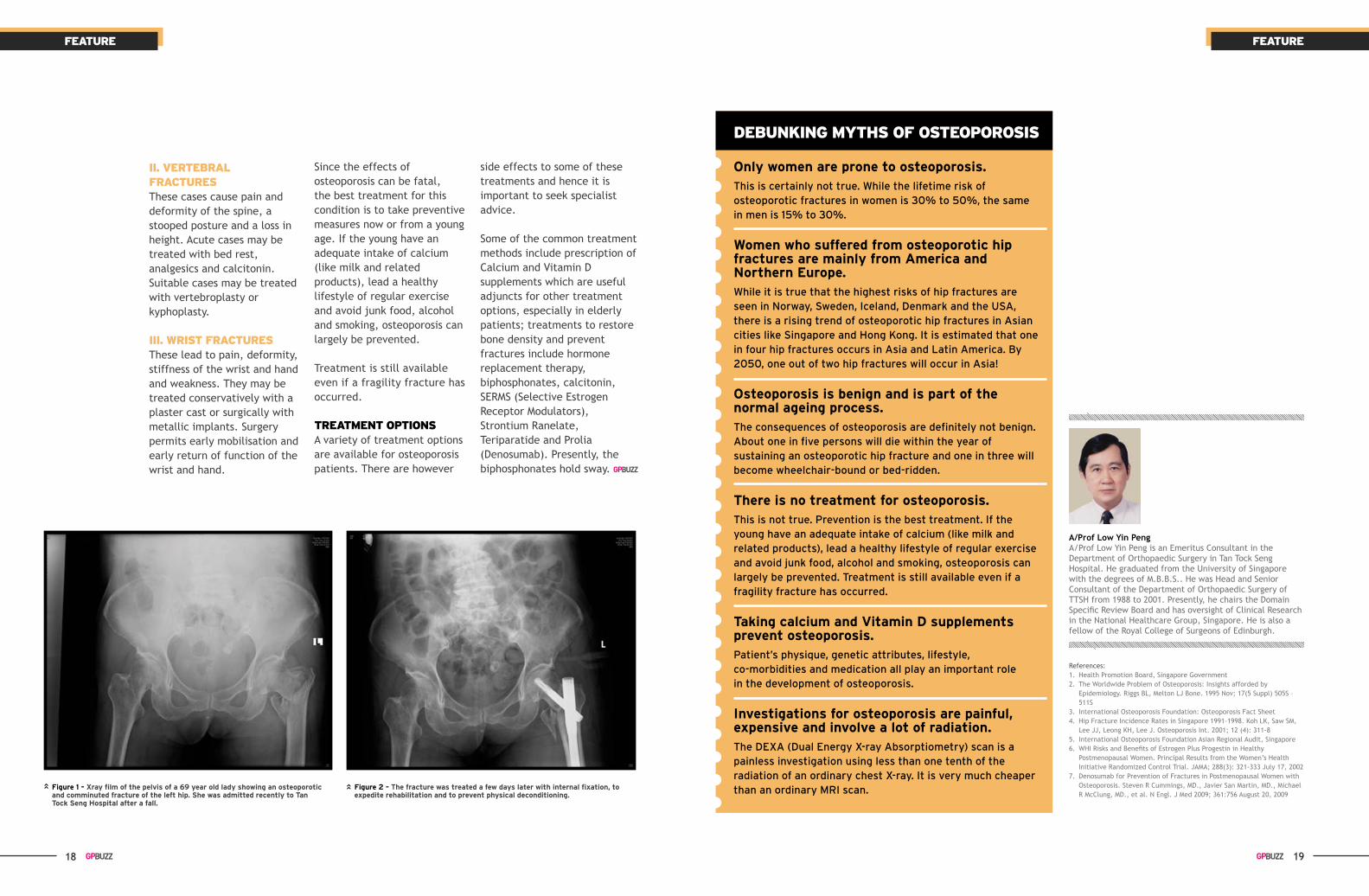
figure 1 – Xray film of the pelvis of a 69 year old lady showing an osteoporotic and comminuted fracture of the left hip. she was admitted recently to tan tock seng hospital after a fall.
figure 2 – the fracture was treated a few days later with internal fixation, to expedite rehabilitation and to prevent physical deconditioning.
ii. verteBrAL frActures These cases cause pain and deformity of the spine, a stooped posture and a loss in height. Acute cases may be treated with bed rest, analgesics and calcitonin. Suitable cases may be treated with vertebroplasty or kyphoplasty.
iii. wrist frActuresThese lead to pain, deformity, stiffness of the wrist and hand and weakness. They may be treated conservatively with a plaster cast or surgically with metallic implants. Surgery permits early mobilisation and early return of function of the wrist and hand.
Since the effects of osteoporosis can be fatal, the best treatment for this condition is to take preventive measures now or from a young age. If the young have an adequate intake of calcium (like milk and related products), lead a healthy lifestyle of regular exercise and avoid junk food, alcohol and smoking, osteoporosis can largely be prevented.
Treatment is still available even if a fragility fracture has occurred.
treAtment optionsA variety of treatment options are available for osteoporosis patients. There are however
side effects to some of these treatments and hence it is important to seek specialist advice.
Some of the common treatment methods include prescription of Calcium and Vitamin D supplements which are useful adjuncts for other treatment options, especially in elderly patients; treatments to restore bone density and prevent fractures include hormone replacement therapy, biphosphonates, calcitonin, SERMS (Selective Estrogen Receptor Modulators), Strontium Ranelate, Teriparatide and Prolia (Denosumab). Presently, the biphosphonates hold sway.
References:1. Health Promotion Board, Singapore Government2. The Worldwide Problem of Osteoporosis: Insights afforded by
Epidemiology. Riggs BL, Melton LJ Bone. 1995 Nov; 17(5 Suppl) 505S – 511S
3. International Osteoporosis Foundation: Osteoporosis Fact Sheet4. Hip Fracture Incidence Rates in Singapore 1991-1998. Koh LK, Saw SM,
Lee JJ, Leong KH, Lee J. Osteoporosis Int. 2001; 12 (4): 311-85. International Osteoporosis Foundation Asian Regional Audit, Singapore6. WHI Risks and Benefits of Estrogen Plus Progestin in Healthy
Postmenopausal Women. Principal Results from the Women’s Health Initiative Randomized Control Trial. JAMA; 288(3): 321-333 July 17, 2002
7. Denosumab for Prevention of Fractures in Postmenopausal Women with Osteoporosis. Steven R Cummings, MD., Javier San Martin, MD., Michael R McClung, MD., et al. N Engl. J Med 2009; 361:756 August 20, 2009
deBunkinG myths of osteoporosis
only women are prone to osteoporosis. This is certainly not true. While the lifetime risk of osteoporotic fractures in women is 30% to 50%, the same in men is 15% to 30%.
women who suffered from osteoporotic hip fractures are mainly from America and northern europe.While it is true that the highest risks of hip fractures are seen in Norway, Sweden, Iceland, Denmark and the USA, there is a rising trend of osteoporotic hip fractures in Asian cities like Singapore and Hong Kong. It is estimated that one in four hip fractures occurs in Asia and Latin America. By 2050, one out of two hip fractures will occur in Asia!
osteoporosis is benign and is part of the normal ageing process. The consequences of osteoporosis are definitely not benign. About one in five persons will die within the year of sustaining an osteoporotic hip fracture and one in three will become wheelchair-bound or bed-ridden.
there is no treatment for osteoporosis. This is not true. Prevention is the best treatment. If the young have an adequate intake of calcium (like milk and related products), lead a healthy lifestyle of regular exercise and avoid junk food, alcohol and smoking, osteoporosis can largely be prevented. Treatment is still available even if a fragility fracture has occurred.
taking calcium and Vitamin d supplements prevent osteoporosis. Patient’s physique, genetic attributes, lifestyle, co-morbidities and medication all play an important role in the development of osteoporosis.
investigations for osteoporosis are painful, expensive and involve a lot of radiation. The DEXA (Dual Energy X-ray Absorptiometry) scan is a painless investigation using less than one tenth of the radiation of an ordinary chest X-ray. It is very much cheaper than an ordinary MRI scan.
A/Prof Low Yin PengA/Prof Low Yin Peng is an Emeritus Consultant in the Department of Orthopaedic Surgery in Tan Tock Seng Hospital. He graduated from the University of Singapore with the degrees of M.B.B.S.. He was Head and Senior Consultant of the Department of Orthopaedic Surgery of TTSH from 1988 to 2001. Presently, he chairs the Domain Specific Review Board and has oversight of Clinical Research in the National Healthcare Group, Singapore. He is also a fellow of the Royal College of Surgeons of Edinburgh.
feAturefeAture
20 21
what are carbohydrates and why are they essential for us?
Carbohydrates break down into sugars to provide an important source of energy for our bodies, especially our brain. Without adequate carbohydrates in our diet, we may experience fatigue, suffer from poor mental function and have decreased stamina and endurance.
The complex and unrefined carbohydrates are often rich in fibre, vitamins, carotenoids, phytochemicals and trace minerals like calcium and potassium which are essential for health.
how did the fad of low carbohydrate diets for weight loss come about?
The obsession with eating minimal amount of carbohydrates for weight loss originated in 1872. Dr William Harvey, an English surgeon, recommended a diet with minimal carbohydrates and mostly protein to William Banting in order to lose weight. Banting subsequently lost 20kg from an initial 90kg in a year, and had continued weight loss. Although Harvey was criticised for the lack of scientific theory, the public was fascinated and quickly adopted this diet for rapid weight loss. In the 1990s, this low carbohydrate diet was once again made famous with the Atkins diet, the Zone diet and the Carbohydrate Addict’s diet, which practiced a similar regime.
why do low carbohydrate diets lead to initial weight loss?
When there are insufficient carbohydrates obtained from the diet, the body sugar stores known as glycogen are broken down to glucose to maintain normal blood sugar levels for daily activities. Since glycogen is made up of glucose units bound together by water molecules, the breakdown of glycogen leads to excretion of water, resulting in rapid initial weight loss.
The Truth About
Carbohydrateswith the increasing number of people
becoming overweight, a desperate search for an instant method to shed the excess
weight arises. Low carbohydrate diets have become increasingly popular even though carbohydrates are an essential part of our diet to provide energy, vitamins, minerals
and fibre. in the long run, such a diet is unsustainable, ineffective for weight
loss and can be damaging to the body. Know the truth about this fad diet,
its associated controversies, and learn healthy eating habits.
Hunger is also suppressed because the carbohydrates are often replaced by protein which provides higher satiety. Appetite is further decreased as the process of ketosis or accumulation of ketones in the blood occurs as the body begins to burn fat.
A low carbohydrate diet often eliminates the fatty and sugary foods which are high in calories, leading to a substantial decrease in calorie intake and thus weight loss.
is this method of dieting healthy?
In the long run, low carbohydrate diets are not recommended for losing weight.
This is because as time passes, the diet becomes unsustainable, ineffective and can be damaging to the body.
Prolonged ketosis can lead to symptoms of headache, mental fatigue and bad breath.
When the suppression of appetite from ketosis subsides, cravings may result and any carbohydrates or sugary foods eaten quickly restore glycogen stores and the water associated with it, thus putting back the weight that was lost initially.
During exercise, fatigue quickly sets in if a consistent lack of dietary carbohydrates has resulted in depleted glycogen stores of energy.
Reducing carbohydrates may also cause one to avoid intake of fruits, wholegrains and sometimes vegetables which can lead to constipation due to the lack of fibre. These foods also contain soluble fibre which help reduce high cholesterol levels and are shown to reduce high blood pressure when combined with a reduced sodium intake. They also contain essential vitamins and minerals which can lead to deficiencies if one persists in such a diet.
When one decides to have a low carbohydrate diet, they inevitably replace the carbohydrates with proteins, commonly animal proteins. Meats, poultry or dairy are higher in
saturated fat and cholesterol which raises the low-density lipoprotein (LDL) cholesterol levels.
For people who suffer from gout, excessive intake of protein foods increases the intake of purine, which may aggravate gout flares. In people with diabetes, a very high protein diet can accelerate the progression of diabetic renal disease. Additional protein also increases the urinary loss of calcium, leading to osteoporosis.
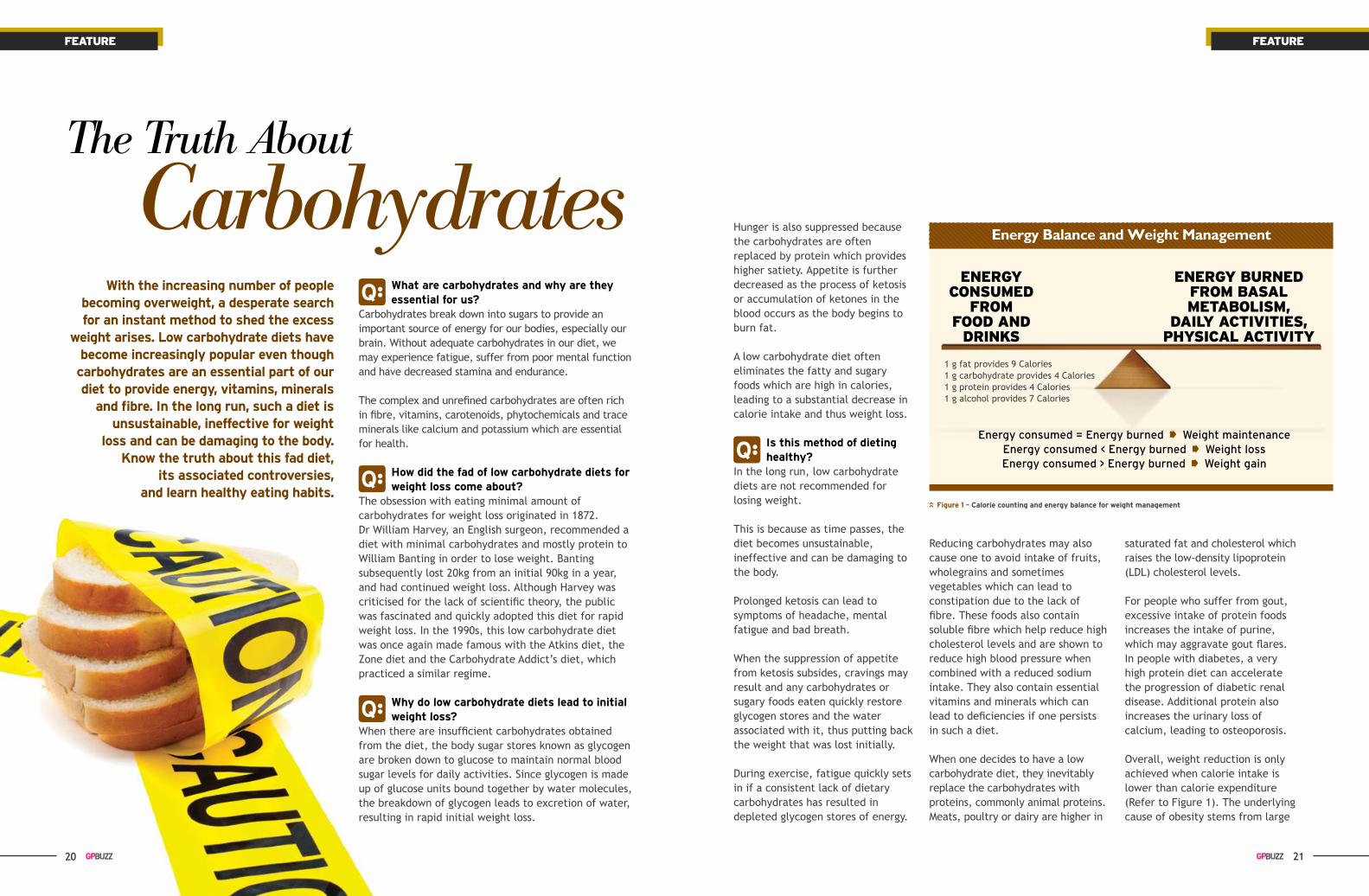
Overall, weight reduction is only achieved when calorie intake is lower than calorie expenditure (Refer to Figure 1). The underlying cause of obesity stems from large
Q
Q
Q
Q
feAturefeAture
enerGy consumed
from food And
drinks
Energy Balance and Weight Management
enerGy Burned from BAsAL metABoLism,
dAiLy Activities, physicAL Activity
1 g fat provides 9 Calories1 g carbohydrate provides 4 Calories1 g protein provides 4 Calories1 g alcohol provides 7 Calories
Energy consumed = Energy burned Weight maintenanceEnergy consumed < Energy burned Weight lossEnergy consumed > Energy burned Weight gain
figure 1 – Calorie counting and energy balance for weight management
20

22 23
fact: heart disease (22%) and stroke (10%) cause one-third of all female deaths in singapore.
fallacy: only 9% of women named heart disease as a leading cause of death.
fact: women can do much to reduce their risk of heart attacks.
fallacy: 35% believed they were at low risk and could do nothing to prevent heart attacks.
fact: every risk factor adds risk. Controlling one risk factor still leaves the person at increased risk from the others.
fallacy: 40% of women believed cholesterol did not matter if blood pressure was controlled.
fact: Lifestyle measures and, if necessary, medicine, can control high blood pressure and cholesterol levels, but they will recur if not maintained.
fallacy: 30% of women believed they could stop medication when they achieved control.
In the long run however, low carbohydrate diets are not recommended for losing weight.
portion sizes, high-fat or calorie dense foods and decreased physical activity.
how much carbohydrates are required?
Carbohydrates should form about 45-65% energy of our diet, preferably from wholegrains. According to the Health Promotion Board healthy diet pyramid (refer figure 2), rice and alternatives form the base and provides the main source of energy for our daily activities, so try to have at least 5 to 7 servings every day.
Other sources of carbohydrate containing foods include fruits, starchy vegetables, dairy products and legumes. Starchy vegetables form part of the recommended 5 to 7 servings of rice and alternatives. Include two servings of fruits and
Melissa HoMelissa Ho is a Dietitian at Tan Tock Seng Hospital. She completed her Bachelor of Nutrition and Dietetics with Honours at Flinders University in Adelaide, Australia. She currently provides medical nutrition therapy to patients with conditions including obesity, diabetes, cardiovascular disease and malnutrition.
also some legumes that should make up the three servings in the meat and alternatives section.
tips for healthy carbohydrate intake • Have some carbohydrates at every
meal and choose wholegrains over refined grains. E.g. brown rice, wholemeal bread, oats or chappati.
• Have a fruit in between or with meals to prevent unhealthy snacking.
• Have a variety of vegetables and legumes each day.
• Avoid sweet drinks and sugary snacks which are high in refined carbohydrates. They are high in calories and often stimulate cravings for other unhealthy foods.
• Limit high fat foods that are high in calories e.g. oily fried rice or noodles, pastries, cakes, cookies, chips and fries.
Select Less
Select more
rice & ALternAtives(2-3 serVinGs shoULd Be
whoLe-GrAin prodUCts)
figure 2 – healthy diet pyramid for a balanced diet
fAts, oiLs, suGAr And sALtUse in sMALL AMoUnts
meAt & ALternAtives3 serVinGs
(½ a serving should come from dairy or other high calcium products)
fruit & veGetABLes2 serVinGs eACh
understanding Cholesterol and Heart disease
feAturefeAture
Q
Facts, fallacies and confusing information are responsible for creating much uncertainty and hesitation among women when faced with their high cholesterol levels. What actions should they take? What tests should they do. How far should they go? Women need to understand their risks and their options, to make the right choices.
m isconceptions about heart disease in women are common. in 2007
and 2009, the singapore heart foundation conducted surveys which
revealed several key gaps in women’s understanding of heart disease:
source: http://www.myheart.org.sg/heart-facts/statistics/

24 25
Dr Evelyn LeeDr Evelyn Lee is a Senior Consultant in Cardiology at Tan Tock Seng Hospital. Dr Lee trained in the UK, receiving her Bachelor of Medicine and Bachelor of Surgery from Cambridge University, and completed specialist training in Cardiology in 1999. She is a Fellow of the Royal College of Physicians (UK). Her interest is in Echocardiography.
my cholesterol level is high. my friends tell me once I start pill medication, it is life-long and there are side-effects. my brother had a heart attack last month. Is it true that women have a lower risk of heart disease? maybe I don’t need pills?– mrs A
feAturefeAture
harmless for many years, whereas over half of sudden deaths from heart attack are due to unstable minor narrowings whose inner linings crack, causing blood to clot and block the artery suddenly.
We can slow down arterial disease and promote stability by going back to basics and applying risk factor control.
the Conclusion?Mrs A decided the cost involved in undergoing additional tests would not impact her cholesterol management, and went home happier and more confident.
Women need to understand their risks and their options, to make the right choices.If women understood more about cholesterol and other cardiovascular risk factors, half our battle as doctors is won.
Adding to the confusion are recent articles highlighting side-effects of statins, a drug used to lower cholesterol, and a seemingly contradictory Norwegian study that linked high cholesterol levels with increased risk in men but lower risk in women.
Worldwide experience confirms the safety of statins. Severe complications such as liver or muscle damage are rare, and no more common than severe complications of drugs that is regarded as ‘safe’, like aspirin and penicillin. The evidence for statin-related forgetfulness is unclear, but side-effects, if any, were mostly unnoticeable without specific testing. Numerous research studies also provide clear and consistent evidence that statins save lives, particularly in high-risk individuals.
The Norwegian study was not, in fact, contradictory. It looked at lower-risk individuals, not the high
why do i not recommend any other tests?Additional tests are most helpful in symptomatic or moderate-risk patients where the need for treatment is unclear, but they are imperfect. Exercise tests detect major coronary artery blockages which impair blood supply to the heart, but not lesser blockages. CT scans measure coronary calcium (calcium scoring), which reflects extent of coronary disease, but not severity of blockages.
However, we have no tests for arterial stability, which is more important than narrowing.
It is a misconception that we must unblock arteries even if patients are well. Everyone gets some arterial disease with age. Unless narrowings are critical, unblocking arteries does not prolong life more than medicine. Arteries which are 80% blocked can stay stable, unchanged and
risk groups that clearly benefit from statin. It confirmed that total cholesterol, the traditional measurement, is unreliable in women. Many countries, including Singapore, now use better tests.
‘Total cholesterol’ includes both protective ‘good cholesterol’, High-density Lipoprotein (HDL), and harmful ‘bad cholesterol’, Low-density Lipoprotein (LDL). Pre-menopausal women have more HDL and a better balance between ‘good’ and ‘bad’. Unfortunately, post-menopausal women suffer heart attack and stroke, just like men, only their disease is delayed 10 years by pre-menopausal protection.
Statins lower LDL but are unable to raise HDL effectively. Hormone replacement therapy does not replicate the protection conferred by pre-menopausal female hormones and does not protect the heart. A sensible lifestyle is also safe and helpful, and is recommended for everyone regardless of risk.
so, back to Mrs A, what can i do for her? Firstly, there should be provision of sound knowledge for sensible decision-making.
Next, an overall risk-assessment should be made, looking at symptoms, medical history, age, blood pressure, diabetes, obesity, family history, smoking, diet, exercise and ECG of the person, not just cholesterol levels.
It turned out that both her LDL and HDL were slightly high, but the balance was good. Her brother, who suffered a heart attack, was obese and smoked heavily. She was a slim, pre-menopausal 40-year-old who swam regularly and a non-smoker. Her ECG was normal and overall risk was low. All she required was sensible diet and annual monitoring for changes in her risk factor profile with age.

26 27
many women who experience urinary leakage think of it as part of ageing. The incidence
of urinary incontinence, which is any involuntary leakage of urine, is under-reported as many women have grown to accept it as part of the norm.
There are several treatment options available which can bring about an improved quality of life and well-being.
There are several types of urinary incontinence:
1. Stress Urinary Incontinence There is leakage of urine upon straining such as with coughing, sneezing or laughing.
2. Urge Urinary IncontinenceUrinary leakage is accompanied by or immediately preceded by sense of urgency. Patients with this type of incontinence often report the need to rush to the bathroom.
Some women have mixed urinary incontinence, with combination symptoms of both mentioned.
3. Overflow Urinary Incontinence Urine leakage is associated with urinary retention. In some patients with neurological conditions or poorly controlled diabetes mellitus, neurological control in bladder storage and emptying is affected. This results in ‘overflow’ incontinence, in which bladder distension of the stored urine leaks out beyond a certain capacity.
4. Continuous Urinary Leakage This is seen in patients with fistulas such as a vesicovaginal fistula (VVF). These patients experience persistent leakage of urine from the vagina. These may be caused by complications of previous
surgeries or radiation therapy, and may be treated with appropriate corrective surgeries.
5. Overactive Bladder (OAB) These symptoms are complex, involving urgency, usually with frequency and nocturia. It can be a cause of incontinence.
Urinary incontinence may be temporary with identifiable, reversible causes or permanent ones. Different types of incontinence have different causes and treatment options.
It is not uncommon in women with previous childbirth to complain of urinary leakage when they cough or jog. The symptoms of such stress urinary incontinence may be of varying degree in different women, ranging from minimal staining to being pad dependent. These may have an onset many years post delivery, and with age or during the menopausal state.
The risk factors for stress urinary incontinence include previous pregnancy and vaginal delivery. Assisted delivery with forceps or other instruments, prolonged birth process and birth of large babies may increase the risk. Neurological conditions, ageing and obesity are also possible risk factors.
SEEKING TREATMENT – WHAT TO EXPECT
What should a patient expect when consulting a urologist? The Urologist will usually enquire about the nature, severity and duration of the urinary leakage. Gynecological and obstetrics history, along with the existence of previous
Treatment of incontinence depends very much of its type, and can range from conservative to surgical options. Importantly, the severity and patient’s expectations have to be taken into account when considering interventions.
surgeries are important points to note as well as the associated neurological or bowel dysfunction. Next, the effects of the condition to the lifestyle of the patient are determined.
A general abdominal and pelvic examination is usually done to look for any abdominal mass, or evidence of pelvic organ prolapse. The patient would usually be asked to cough or strain in an attempt to reproduce leakage. Targeted neurological examination will also performed.
What are some tests that the patient would have to undertake? Basic investigations would usually include urinalysis to screen for any urine infection, an abdominal ultrasound scan would be done to estimate residual urine, and a voiding diary would be created.
A voiding diary is a form of charting of urine voids done by the patient herself over three consecutive days. It looks at frequency of daytime and night voids, as well as voided volumes, incidence of leakages, which gives us an idea of severity of the incontinence. Daily fluid intake is also charted for evaluation.
Specialised tests like urodynamics, can reinforce the diagnosis and assess the severity of the condition but is usually reserved for selected patients
for consideration of more invasive therapeutic options.
What are the treatment options for urinary incontinence? Treatment of incontinence depends very much on the type of incontinence, and can range from conservative to surgical options. Importantly, the severity and patient’s expectations have to be taken into account when considering interventions.
Conservative treatment includes behavioural and lifestyle modifications such as healthy weight loss, reducing intake of irritants like caffeine and alcohol, and appropriate fluid intake. Bladder training is useful in urge incontinence and OAB and involves techniques to increase voiding intervals, decrease frequency and small voids. Pelvic floor exercises which improve symptoms by strengthening pelvic floor muscles to resist leakages can be useful, especially in mild to moderate stress urinary incontinence in women with previous childbirth experiences.
There are surgical options for stress urinary incontinence for patient with more severe symptoms should the conservative therapies fail. Such procedures aim to treat stress incontinence by correcting anatomical problems, such as using tapes and sling insertions and urethral bulking agents.
feAturefeAture
involuntary urine leakage in women is prevalent and often brushed off as a normal sign of aging. with
medical and technological advancements, there are varied ways that urinary incontinence can be treated.
Fix THe Leak:
Urinary Incontinence

28 29
Tension-free vaginal tape (TVT) and transobturator tape (TOT) are well-known tape procedures performed for stress incontinence. It involves a vaginal incision and placement of a tape to support the mid-urethra, and the ends of the tape are pulled through bilateral incisions at the lower abdomen (TVT) or inner thigh (TOT). This is usually done as a day surgery procedure with no external scars, quick recovery and satisfactory results.
For OAB and urge incontinence, there are medications available to help. However, antimuscarinics
often have side effects of dry eyes, blurring of vision and dry mouth. Injection of Botulinum toxin A into multiple sites in the bladder through a scope can also be performed and this injection has garnered high patient satisfaction.
It was a joyous occasion when Susan (not her real name) gave birth to her daughter in 1997. A year later, however, the 54-year-old administrator found that she had difficulty controlling her bladder.
“Whenever I cough, or run for the bus, I would wet myself.”
Susan’s condition got worse through the years and because of this she had to avoid exercises such as jogging as she was afraid that the impact and movement would cause urine to leak out. She resorted to wearing sanitary pads daily from then.
“Sometimes, I would have to change my pad several times a day as the whole pad would be soaked after several hours. It was troublesome but I could not tell anyone as this is an embarrassing condition.”
Susan lived with urinary incontinence for 14 years from 1998 to 2012, keeping her condition to
herself. It was not until May 2012 when she underwent a pre-employment check-up, that she finally plucked up the courage to mention her condition to the attending doctor who then referred her to Dr Gerald Tan, Consultant Urologist at Tan Tock Seng Hospital’s Department of Urology.
Following detailed checks and diagnoses by Dr Tan, Susan underwent minimally-invasive surgery in May 2012 to her condition. The procedure was completed and Susan was warded for a night.
“I was very afraid that there would be much pain after the operation, but it was very bearable. Dr Tan and the nurses at Tan Tock Seng Hospital also provided very clear explanations which kept me at ease.”
Post-surgery, Susan’s urine leakage problem abated, and she is now able to go about her daily life with
Suffering in Silence
Sometimes, I would have to change my pad several times a day as the whole pad would be soaked after several hours. It was troublesome but I could not tell anyone as this is an embarrassing condition.
Dr Yeo Eu Kiang, Sharon Dr Yeo Eu Kiang, Sharon is an Associate Consultant at the Department of Urology at Tan Tock Seng Hospital. She is also a Clinical Lecturer with the Yong Loo Lin School of Medicine. Dr Yeo received her Bachelor of Medicine and Bachelor of Surgery, and Master of Medicine (Surgery) from the National University of Singapore. She is a member of the Royal College of Surgeons of Glasgow, UK and a Fellow of Academy of Medicine Singapore.
poise and confidence. She has since started to jog regularly which she was unable to do so in the past.
With other women suffering from the same condition, Susan shared, “I had let this condition affect my life for more than a decade. Don’t be like me and let embarrassment get in the way of seeking early treatment.”
However, patients may require repeat injections between 6 to 12 months. Other surgical options like sacral neuromodulators are available, as are radical surgeries, but they are reserved for severe cases and less often done.
The use of pretty footwear with high heels is popular amongst the ladies in Singapore. In the pursuit of elegance and style, many young women opt to forego comfort and ignore the looming possibility of podiatric problems later in life. Learn about the common ‘high-heel related’ conditions that a podiatrist manages, along with prevention and treatment options.
feAturefeAture
A Patient's Journey
High Heels and You: A Podiatrist’s Perspective
“The most common conditions women suffer from, that are
exacerbated by the use of high heels, can be categorised according to the area of the anatomy that it affects. These problems are not confined to
the lower limb, and pain can reach as high as the lower back and spine.”
30 31
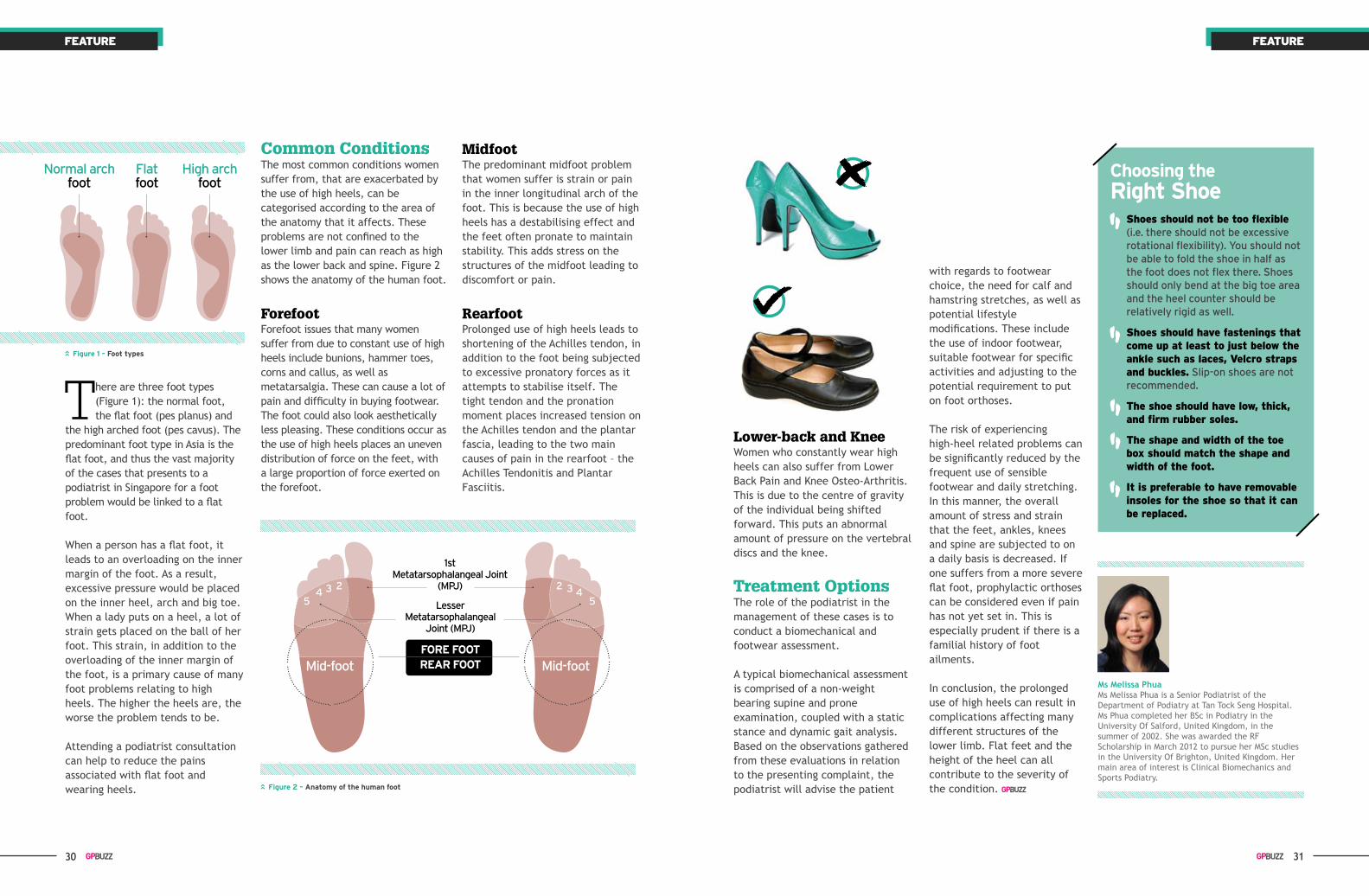
Flat foot
High arch foot
there are three foot types (Figure 1): the normal foot, the flat foot (pes planus) and
the high arched foot (pes cavus). The predominant foot type in Asia is the flat foot, and thus the vast majority of the cases that presents to a podiatrist in Singapore for a foot problem would be linked to a flat foot.
When a person has a flat foot, it leads to an overloading on the inner margin of the foot. As a result, excessive pressure would be placed on the inner heel, arch and big toe. When a lady puts on a heel, a lot of strain gets placed on the ball of her foot. This strain, in addition to the overloading of the inner margin of the foot, is a primary cause of many foot problems relating to high heels. The higher the heels are, the worse the problem tends to be.
Attending a podiatrist consultation can help to reduce the pains associated with flat foot and wearing heels.
Common ConditionsThe most common conditions women suffer from, that are exacerbated by the use of high heels, can be categorised according to the area of the anatomy that it affects. These problems are not confined to the lower limb and pain can reach as high as the lower back and spine. Figure 2 shows the anatomy of the human foot.
ForefootForefoot issues that many women suffer from due to constant use of high heels include bunions, hammer toes, corns and callus, as well as metatarsalgia. These can cause a lot of pain and difficulty in buying footwear. The foot could also look aesthetically less pleasing. These conditions occur as the use of high heels places an uneven distribution of force on the feet, with a large proportion of force exerted on the forefoot.
midfootThe predominant midfoot problem that women suffer is strain or pain in the inner longitudinal arch of the foot. This is because the use of high heels has a destabilising effect and the feet often pronate to maintain stability. This adds stress on the structures of the midfoot leading to discomfort or pain.
RearfootProlonged use of high heels leads to shortening of the Achilles tendon, in addition to the foot being subjected to excessive pronatory forces as it attempts to stabilise itself. The tight tendon and the pronation moment places increased tension on the Achilles tendon and the plantar fascia, leading to the two main causes of pain in the rearfoot – the Achilles Tendonitis and Plantar Fasciitis.
1st Metatarsophalangeal Joint
(MPJ)2 23 34 45 5Lesser
Metatarsophalangeal Joint (MPJ)
Mid-foot Mid-footfore footreAr foot
Lower-back and kneeWomen who constantly wear high heels can also suffer from Lower Back Pain and Knee Osteo-Arthritis. This is due to the centre of gravity of the individual being shifted forward. This puts an abnormal amount of pressure on the vertebral discs and the knee.
Treatment OptionsThe role of the podiatrist in the management of these cases is to conduct a biomechanical and footwear assessment.
A typical biomechanical assessment is comprised of a non-weight bearing supine and prone examination, coupled with a static stance and dynamic gait analysis. Based on the observations gathered from these evaluations in relation to the presenting complaint, the podiatrist will advise the patient
Choosing the right shoe
shoes should not be too flexible (i.e. there should not be excessive
rotational flexibility). You should not be able to fold the shoe in half as the foot does not flex there. Shoes should only bend at the big toe area and the heel counter should be relatively rigid as well.
• shoes should have fastenings that come up at least to just below the ankle such as laces, velcro straps and buckles. Slip-on shoes are not recommended.
• the shoe should have low, thick, and firm rubber soles.
• the shape and width of the toe box should match the shape and width of the foot.
• it is preferable to have removable insoles for the shoe so that it can be replaced.
Ms Melissa Phua Ms Melissa Phua is a Senior Podiatrist of the Department of Podiatry at Tan Tock Seng Hospital. Ms Phua completed her BSc in Podiatry in the University Of Salford, United Kingdom, in the summer of 2002. She was awarded the RF Scholarship in March 2012 to pursue her MSc studies in the University Of Brighton, United Kingdom. Her main area of interest is Clinical Biomechanics and Sports Podiatry.
Normal arch foot
with regards to footwear choice, the need for calf and hamstring stretches, as well as potential lifestyle modifications. These include the use of indoor footwear, suitable footwear for specific activities and adjusting to the potential requirement to put on foot orthoses.
The risk of experiencing high-heel related problems can be significantly reduced by the frequent use of sensible footwear and daily stretching. In this manner, the overall amount of stress and strain that the feet, ankles, knees and spine are subjected to on a daily basis is decreased. If one suffers from a more severe flat foot, prophylactic orthoses can be considered even if pain has not yet set in. This is especially prudent if there is a familial history of foot ailments.
In conclusion, the prolonged use of high heels can result in complications affecting many different structures of the lower limb. Flat feet and the height of the heel can all contribute to the severity of the condition.
feAturefeAture
figure 1 – foot types
figure 2 – Anatomy of the human foot

32 33
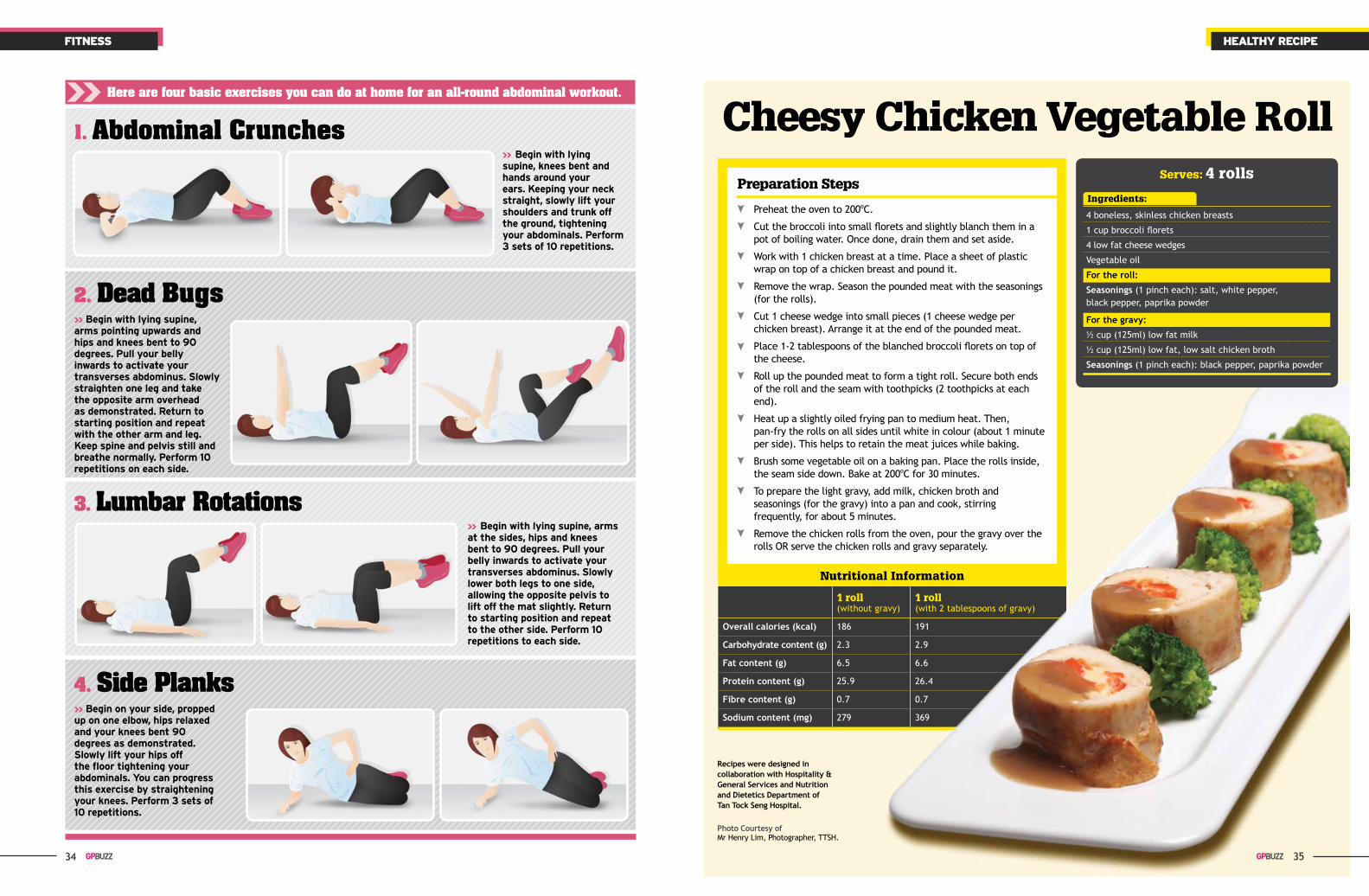
Abdominal exercises are a vital component to any exercise regime. Not only
are they fantastic to get your body in great shape, they are effective in protecting your lower back and preventing injuries in your upper and lower limbs. In our increasingly sedentary lifestyles, prolonged sitting increases the stress on the joints and the disks in the spine of our lower back. Strong abdominals will help you maintain a good posture and offload the stress on the spine, preventing back pain.
The abdominals consist of four main muscles. The rectus abdominus or the ‘six pack’ muscle runs vertically along the front of the abdomen. This muscle is responsible in bending the trunk forward and plays an important role in keeping an upright posture. The external and internal obliques are diagonally directed muscles located at the sides of the abdomen. Their primary function is to allow rotation of the trunk, sideways and forward bending.
zaki HairodinZaki Hairodin is a Senior Physiotherapist in the Physiotherapy Department and Sports Medicine and Surgery Clinic at Tan Tock Seng Hospital. He attends to musculoskeletal and sports injuries. A graduate in Physiotherapy with Honours from La Trobe University, Australia in 2008, his main clinical interests are in Clinical Pilates and low back pain in sports.
Work your Abdominals Right!Abdominal exercises are essential in building up a toned body and in preventing lower back injuries. However, they are ineffective in reducing excess fat around your waist. understand the major muscles around your abdomen and learn simple strengthening exercises you can do at home without the need of gym equipment.
fitnessfitness
The transverses abdominus forms the deepest layer of muscle of the abdomen. It has horizontally-directed fibres that wraps around the trunk similar to a corset. It plays a stabilising role for the spine as well as assisting in breathing and expiration and supporting the internal organs.
34
Begin with lying supine, arms at the sides, hips and knees bent to 90 degrees. pull your belly inwards to activate your transverses abdominus. slowly lower both legs to one side, allowing the opposite pelvis to lift off the mat slightly. return to starting position and repeat to the other side. perform 10 repetitions to each side.
Begin on your side, propped up on one elbow, hips relaxed and your knees bent 90 degrees as demonstrated. slowly lift your hips off the floor tightening your abdominals. you can progress this exercise by straightening your knees. perform 3 sets of 10 repetitions.
3. Lumbar Rotations
4. Side Planks
2. Dead Bugs
Begin with lying supine, knees bent and hands around your ears. Keeping your neck straight, slowly lift your shoulders and trunk off the ground, tightening your abdominals. perform 3 sets of 10 repetitions.
Begin with lying supine, arms pointing upwards and hips and knees bent to 90 degrees. pull your belly inwards to activate your transverses abdominus. slowly straighten one leg and take the opposite arm overhead as demonstrated. return to starting position and repeat with the other arm and leg. Keep spine and pelvis still and breathe normally. perform 10 repetitions on each side.
1. Abdominal Crunches
heALthy recipefitness
Preparation Steps
Preheat the oven to 200oC.
Cut the broccoli into small florets and slightly blanch them in a pot of boiling water. Once done, drain them and set aside.
Work with 1 chicken breast at a time. Place a sheet of plastic wrap on top of a chicken breast and pound it.
Remove the wrap. Season the pounded meat with the seasonings (for the rolls).
Cut 1 cheese wedge into small pieces (1 cheese wedge per chicken breast). Arrange it at the end of the pounded meat.
Place 1-2 tablespoons of the blanched broccoli florets on top of the cheese.
Roll up the pounded meat to form a tight roll. Secure both ends of the roll and the seam with toothpicks (2 toothpicks at each end).
Heat up a slightly oiled frying pan to medium heat. Then, pan-fry the rolls on all sides until white in colour (about 1 minute per side). This helps to retain the meat juices while baking.
Brush some vegetable oil on a baking pan. Place the rolls inside, the seam side down. Bake at 200oC for 30 minutes.
To prepare the light gravy, add milk, chicken broth and seasonings (for the gravy) into a pan and cook, stirring frequently, for about 5 minutes.
Remove the chicken rolls from the oven, pour the gravy over the rolls OR serve the chicken rolls and gravy separately.
Cheesy Chicken Vegetable Roll
Recipes were designed in collaboration with Hospitality & General Services and Nutrition and Dietetics Department of Tan Tock Seng Hospital.
Photo Courtesy of Mr Henry Lim, Photographer, TTSH.
Ingredients:
4 boneless, skinless chicken breasts
1 cup broccoli florets
4 low fat cheese wedges
Vegetable oil
For the roll:
Seasonings (1 pinch each): salt, white pepper, black pepper, paprika powder
For the gravy:
½ cup (125ml) low fat milk
½ cup (125ml) low fat, low salt chicken broth
Seasonings (1 pinch each): black pepper, paprika powder
Serves: 4 rolls
35
Here are four basic exercises you can do at home for an all-round abdominal workout.
Nutritional Information
1 roll(without gravy)
1 roll(with 2 tablespoons of gravy)
Overall calories (kcal) 186 191
Carbohydrate content (g) 2.3 2.9
Fat content (g) 6.5 6.6
Protein content (g) 25.9 26.4
Fibre content (g) 0.7 0.7
Sodium content (mg) 279 369
CliniC B1B– Orthopaedic Surgery– Rheumatology, Allergy and Immunology
CliniC 2B– Gastroenterology and Hepatology
Our sub-specialties include: • General Gastroenterology • Hepatology (Liver) Service • Inflammatory Bowel Disease • Gastrointestinal Endoscopy • Pancreato-Biliary Diseases • Upper Gastrointestinal Motility • Nutrition
– General Surgery Our sub-specialties include: • General Surgery • Colorectal Service • Bariatric and Weight Management Services • Upper Gastrointestinal Service • Head and Neck Surgical Services • Endocrine Service • Liver, Pancreas and Biliary Services
• Vascular Service • Veins Service • Thoracic Service • Plastics, Reconstructive and Aesthetics Services
– Urology Our sub-specialties include: • General Urology • Andrology and Men’s Health • Adrenal Surgery • Continence and Voiding Dysfunction • Endo-Urology and Stone Surgery • Female Urology • Minimally Invasive Surgery and Laparoscopic Surgery • Neuro-Urology • Prostate Surgery • Reconstructive Urology • Robotic Surgery • Subfertility and Sexual Dysfunction • Urologic Cancer Surgery
– Endoscopy Services• Colonoscopy• Flexible Cystoscopy• Gastroscopy
CliniC 4B– Diabetes and Endocrine – General Medicine – Haematology – Infectious Disease – Pain Management – Psychological Medicine – Renal Medicine – Respiratory and Critical Care Medicine
Multi-disCipinary speCialist Care
TTSH PEARL’s suite of clinics and services is guided by the four pillars
of care through Evidence Care, Destination Care, Team Care and
Personalised Care. We remain committed to delivering a higher level of patient care as we value
our patients most.
CliniC B1BOrthopaedic Surgery Tel: (65) 6889 4055 Email: [email protected]
Rheumatology, Allergy and Immunology Tel: (65) 6889 4027 Email: [email protected]
CliniC 2B Tel: (65) 1800-PEARL-00 Email: [email protected]
(65) 1800-73275-00
CliniC 4B Tel: (65) 1800-PEARL-00 Email: [email protected]
(65) 1800-73275-00





























