Embed Size (px)
Citation preview
Ιωάννης Ν. Αναστασόπουλος MD,PhD
Συντονιστής Διευθυντής ΕΣΥ
B’ Ορθοπαιδική Κλινική
Παραμορφώσεις άκρων ποδών στα παιδιά
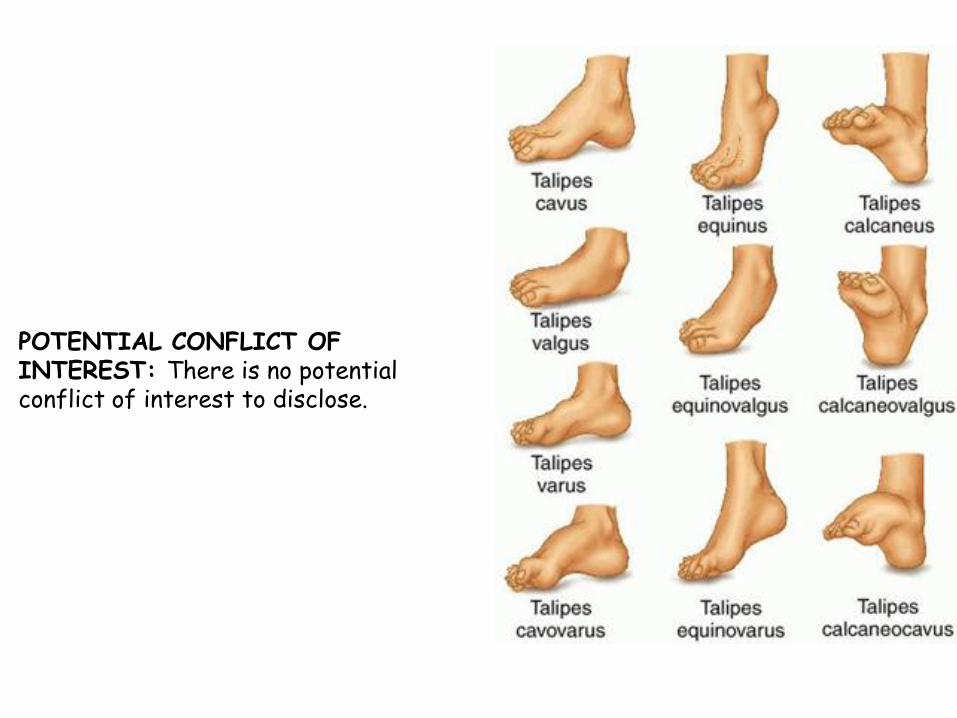
POTENTIAL CONFLICT OF INTEREST: There is no potential conflict of interest to disclose.
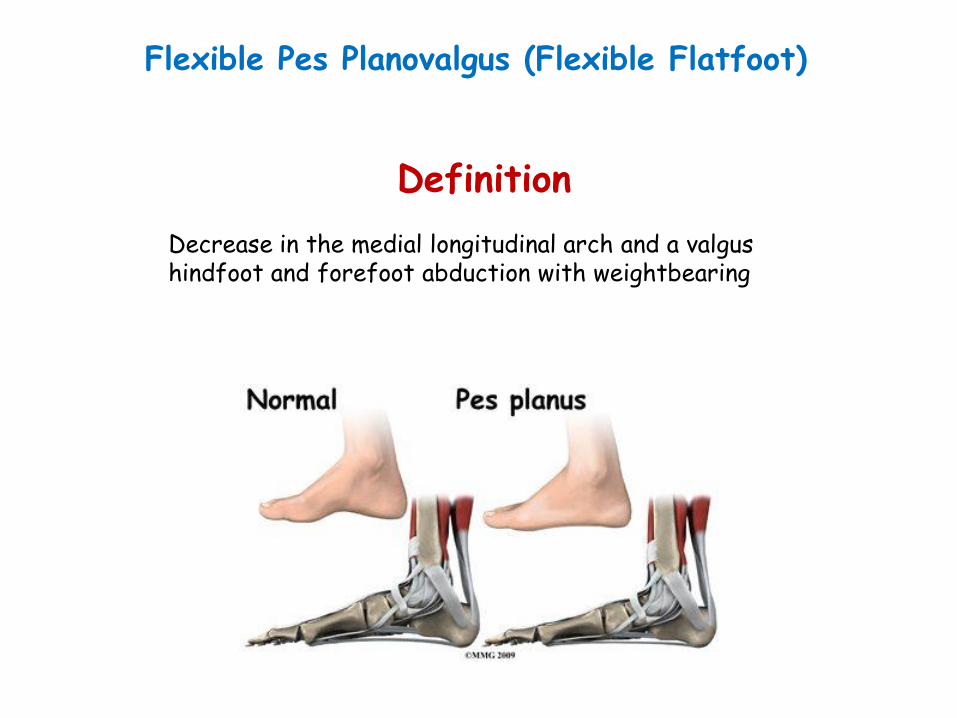
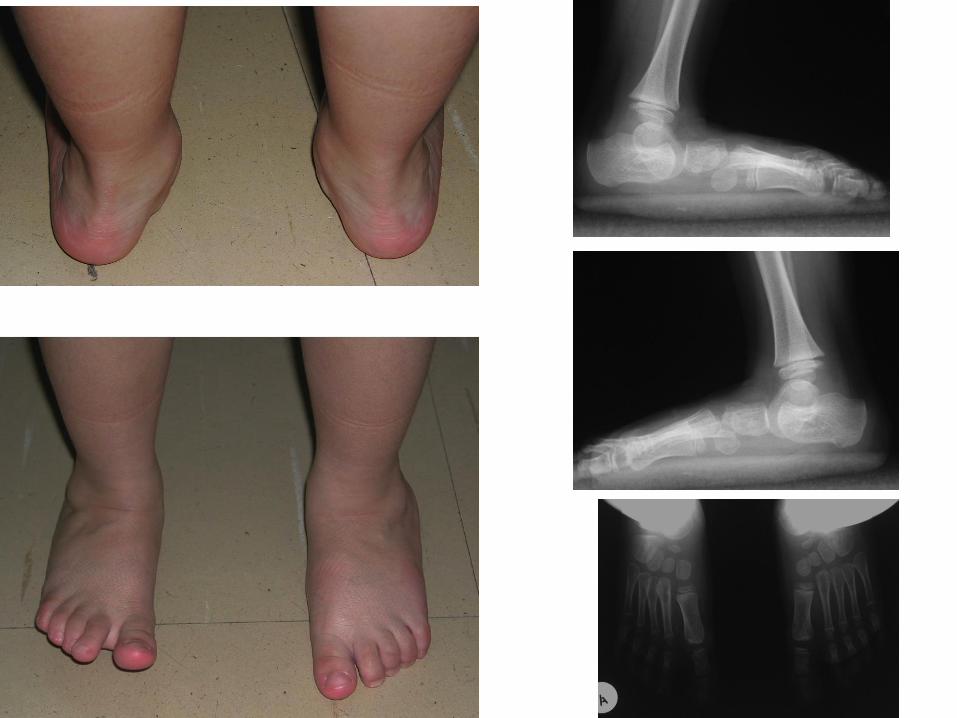
Flexible Pes Planovalgus (Flexible Flatfoot)
Definition Decrease in the medial longitudinal arch and a valgus hindfoot and forefoot abduction with weightbearing

Flat foot is the normal foot shape in the first few years of life Age Prevalence 2 years or younger 97% 6 years 26% 10 years 4% Ages 3 to 6 years may be a critical time period for the development of the medial longitudinal arch. Morley AJ. Knock-knee in children. BMJ. 1957;2(5051):976–979
Staheli LT, Chew DE, Corbett M. The longitudinal arch. A survey of eight hundred and eighty-two feet in normal children and adults. J Bone Joint Surg Am. 1987;69(3):426–428
Epidemiology

Male gender and obesity are associated with a higher risk of flatfoot in children aged 7 to 8 years. Chang JH, Wang SH, Kuo CL, Shen HC, Hong YW, Lin LC. Prevalence of flexible flatfoot in Taiwanese school aged children in relation to obesity, gender, and age. Eur J Pediatr. 2010;169(4):447–452
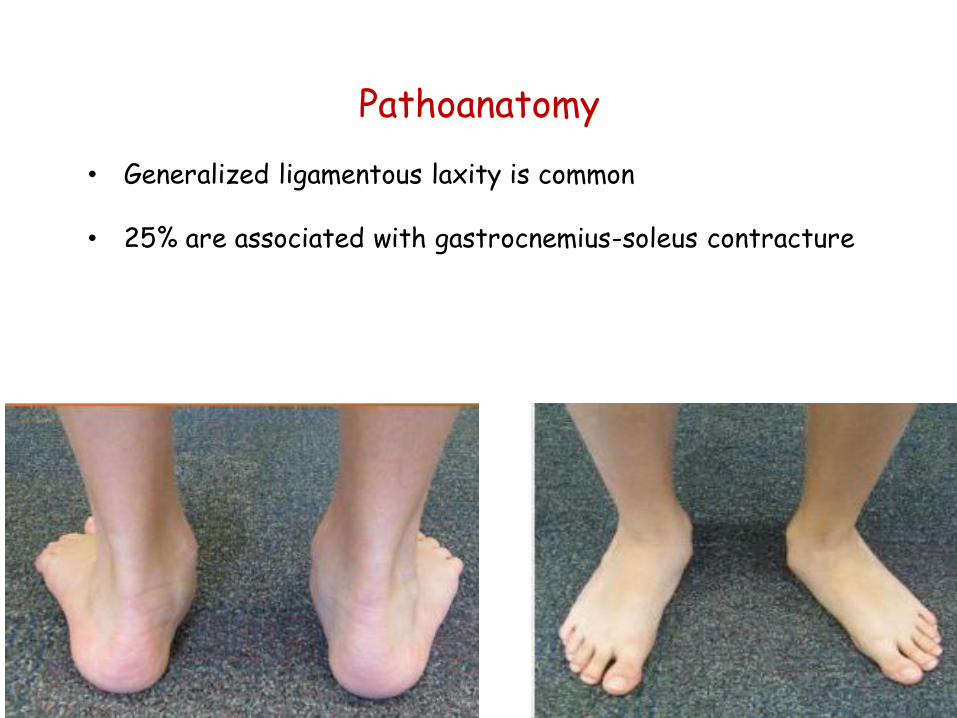
Pathoanatomy
• Generalized ligamentous laxity is common
• 25% are associated with gastrocnemius-soleus contracture

Clinical Features

Differential diagnosis •Tarsal coalition •Congenital vertical talus •Accessory navicular
“Young patients and their parents should be reassured that most flexible flatfeet are normal in childhood, and that the foot arch elevates over the first 10 years of age” Wenger DR Mauldin D, Speck G, Morgan D, Lieber RL. Corrective shoes and inserts as treatment for flexible flatfoot in infants and children. J Bone Joint Surg Am 1989; 71: 800-810
‘’Although orthotics are diffusely prescribed to alleviate symptoms, to date there is no evidence supporting the use of orthotics to correct the deformity’’ Whitford D, Esterman A. A randomized controlled trial of two types of in-shoe orthoses in children with flexible excess pronation of the feet. Foot Ankle Int. 2007;28(6):715–723
Treatment
1. Asymptomatic flat foot
‘’As a matter of fact some authors even suggest that insoles could cause more harm, leading to dependency and long-term negative psychological effects’’ Driano AN, Staheli L, Staheli LT. Psychosocial development and corrective shoewear use in childhood.
J Pediatr Orthop 1998;18 :346-349

Complaints • Activity-related pain. • Fatigue of the foot muscles. • Calluses to the medial foot. • Rapid shoe breakdown. • Recurrent ankle sprains.
Generic orthotic use can reduce pain in symptomatic flexible flat feet for some patients. Evans AM. The flat-footed child—to treat or not to treat: what is the clinician to do? J Am Podiatr Med Assoc. 2008;98(5):386–393
2. Symptomatic flat foot

Triple arthrodesis Arthroreisis
Koutsogiannis Osteotomy
Mosca lengthening
Surgery ?

• Current evidence suggests that it is safe and appropriate to simply observe an asymptomatic child with flat feet.
• Painful flexible flatfoot may benefit from orthopedic intervention, such as physical therapy, bracing, or even a surgical procedure.
• Orthotics, although generally unproven to alter the course of flexible flatfoot, may provide relief of pain when present.
Pediatric Pes Planus: A State of- the-Art Review James B. Carr II, MD, Scott Yang, MD, Leigh Ann Lather, MD PEDIATRICS Volume 1 37, number 3 , March 2016: e2 0151230
Summary

Definition
Α complex deformity that includes:
equinus cavus Heel varus adduction
Supination
Congenital clubfoot

CCF is a complex disease caused by both GENETIC AND ENVIRONMENTAL FACTORS
Idelberger, 1939: monozygotic twins: 32.5% dizygotic twins: 2.9% Engell et al., 2006: monozygotic twins: 16.6% dizygotic twins: 5% Wynne-Davies, 1965: risk to parents with a first-degree relative affected: 2.9%
Etiology
Positive family history in 15-23% (Cohen-Overbeek et al., 2006)
Pagnotta et al F.Ankle Jour.(4)2011:
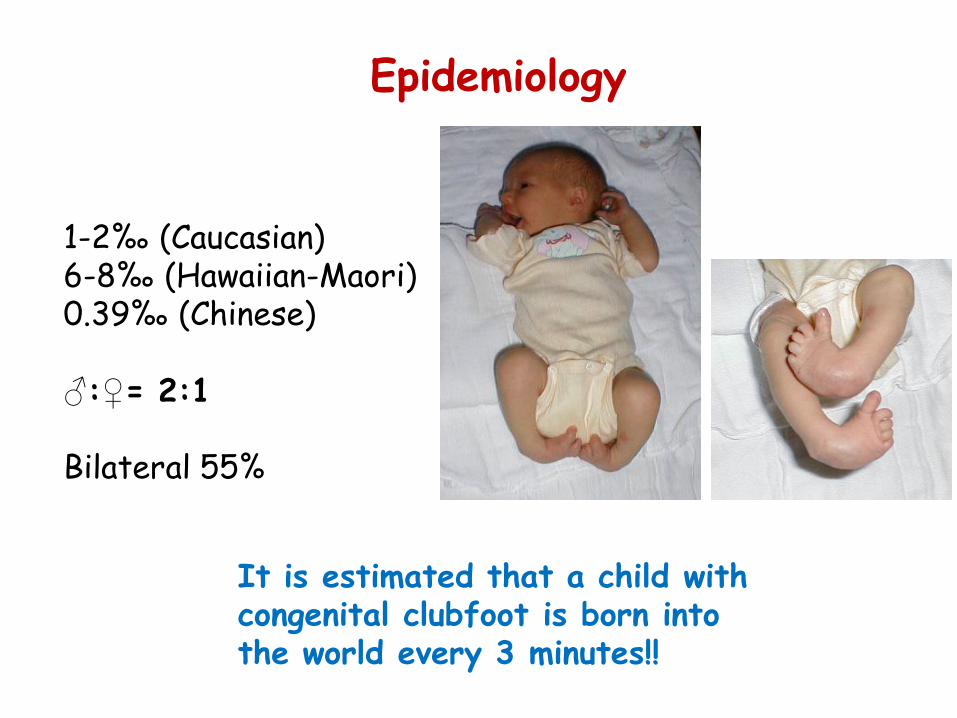
1-2‰ (Caucasian) 6-8‰ (Hawaiian-Maori) 0.39‰ (Chinese) ♂:♀= 2:1 Bilateral 55%
Epidemiology
It is estimated that a child with congenital clubfoot is born into the world every 3 minutes!!

Normal leg Club foot leg
Pathology

Pathogenesis
• Leg muscle atrophy already present at the end of the 14 week of intrautering life
• Pulling action of the shortened triceps surae and tibialis posterior
Waisbrod 1973
• These shortened muscles might cause the
deformity
• Muscle atrophy tends to increase by the growth Ippolito 2008
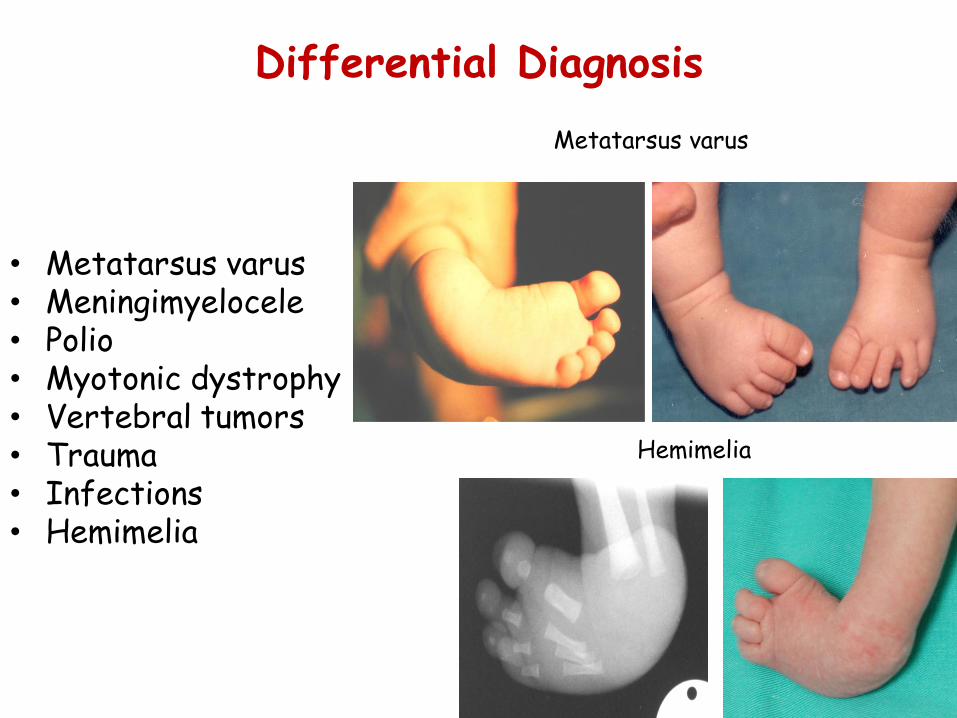
Differential Diagnosis
• Metatarsus varus • Meningimyelocele • Polio • Myotonic dystrophy • Vertebral tumors • Trauma • Infections • Hemimelia
Metatarsus varus
Hemimelia

Pre-natal Diagnosis
Trans vaginal 13-16 gestational week Trans abdominal 16-39 gestational week Difficult detection after 26-18 weeks
Sonography

20 weeks 15 weeks
Isolated club foot
Complex club foot
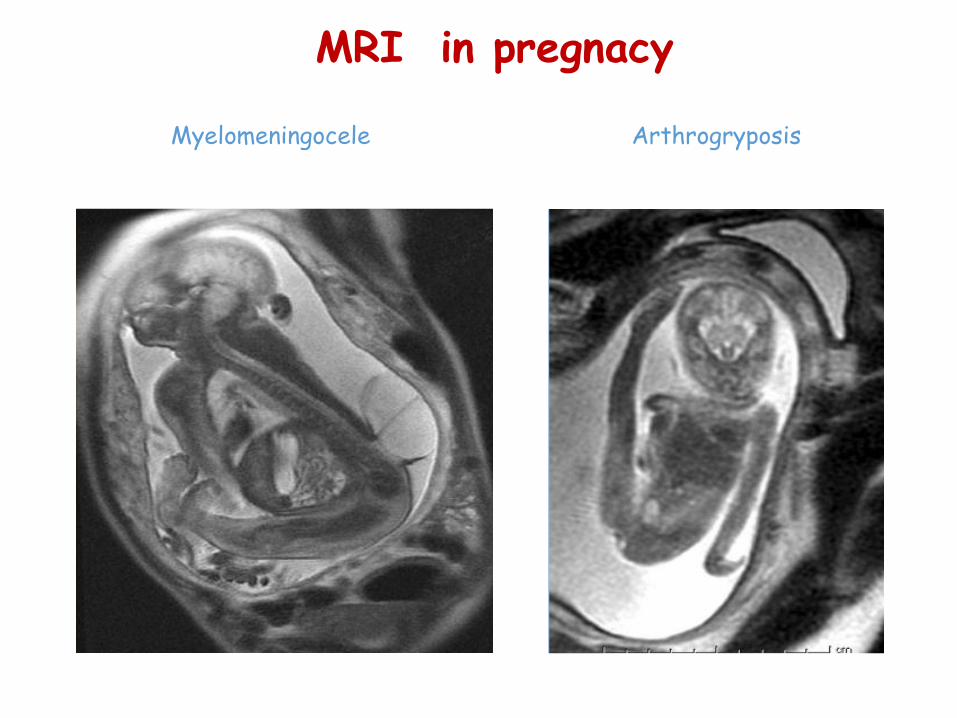
Myelomeningocele Arthrogryposis
MRI in pregnacy

Parents counseling
• U/S Operator • Gynaecologist • Geneticist • Orthopaedic Surgeon • Bioethicist • Psychologist
Advantages of prenatal diagnosis
• Karyotype • Spina bifida • Psychological support
to parents • Appropriate mode of
delivery • Appropriate perinatal
care
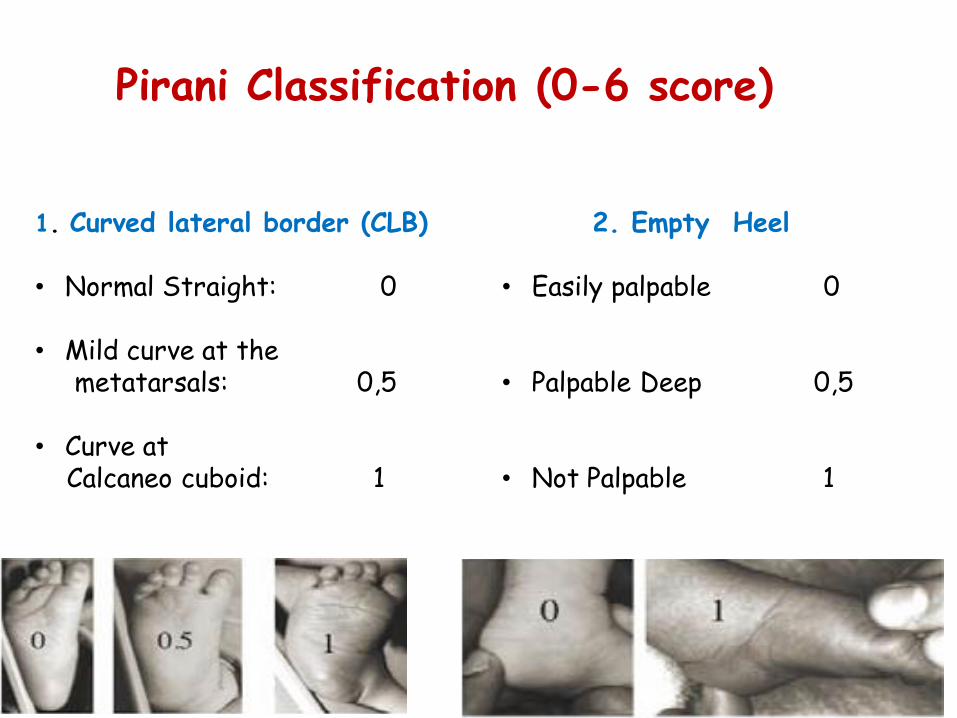
Pirani Classification (0-6 score)
1. Curved lateral border (CLB) • Normal Straight: 0 • Mild curve at the metatarsals: 0,5 • Curve at Calcaneo cuboid: 1
2. Empty Heel • Easily palpable 0 • Palpable Deep 0,5 • Not Palpable 1

Pirani Classification (0-6 score)
3. Rigid Equinus (RE) • 15 degrees beyond neutral: 0 • Extention to neutral: 0,5 • Extention short to neutral: 1
4. Medial Crease (MC)
• Normal arch 0
• Two deeper creases 0,5
• Single deep crease 1

Pirani Classification (0-6 score)
5. Talar head Palpability • None 0
• Partial 0,5
• Full 1
6. Posterior crease (PC)
• Multiple creses 0
• One or two deeper cereases 0,5 • Single deep crease 1

Surgical treatment
Gold standard in 20th century.
• Posterior release, Phelps 1891
• Postero-medial release Turco 1980
• (failure rate 25% - 50%)
• Cincinnati approach
• Postero – medial and lateral release (McKay)
• Carrolls (2 incisions technique)
• External fixators (Ilizarov)

Postero(+/-medial) release

Cincinnati approach

Poor results Pain Stiffness Deformity Relapse Early arthritis
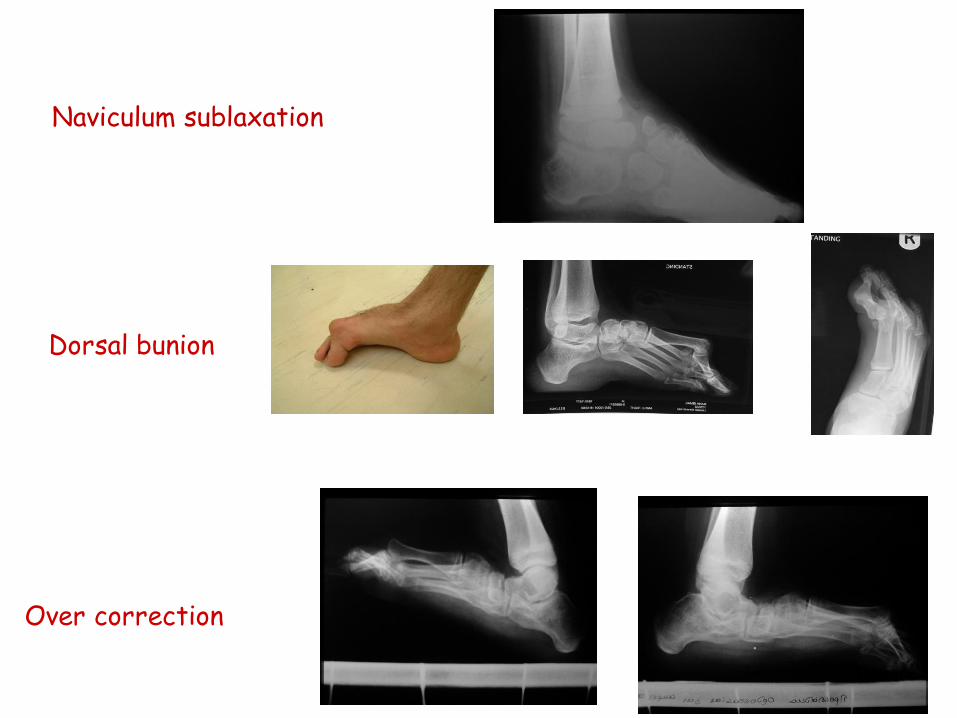
Over correction
Dorsal bunion
Naviculum sublaxation



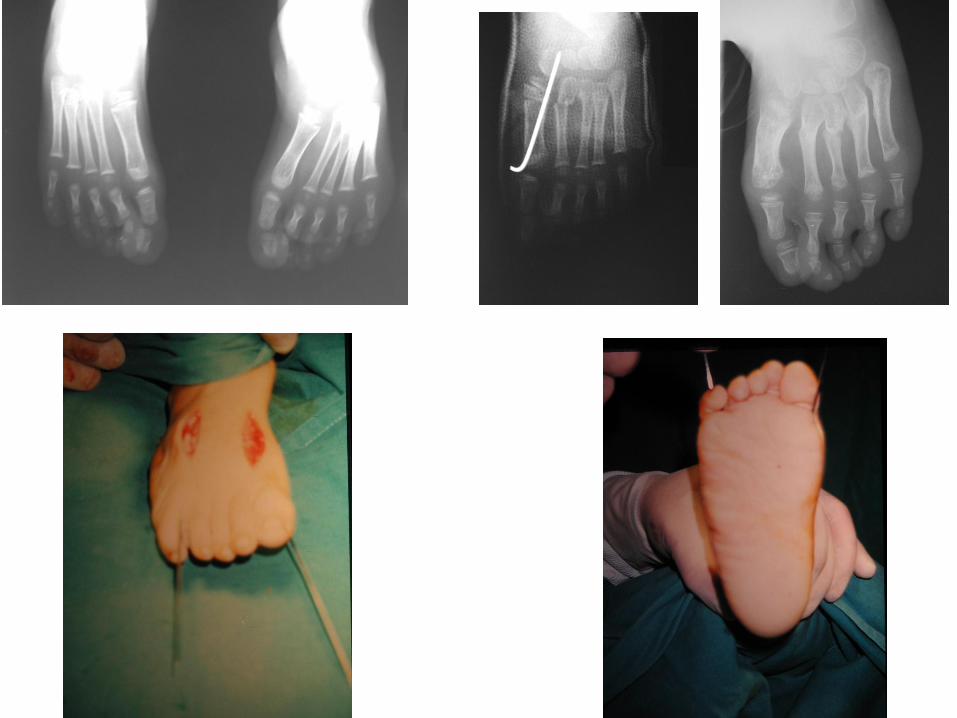

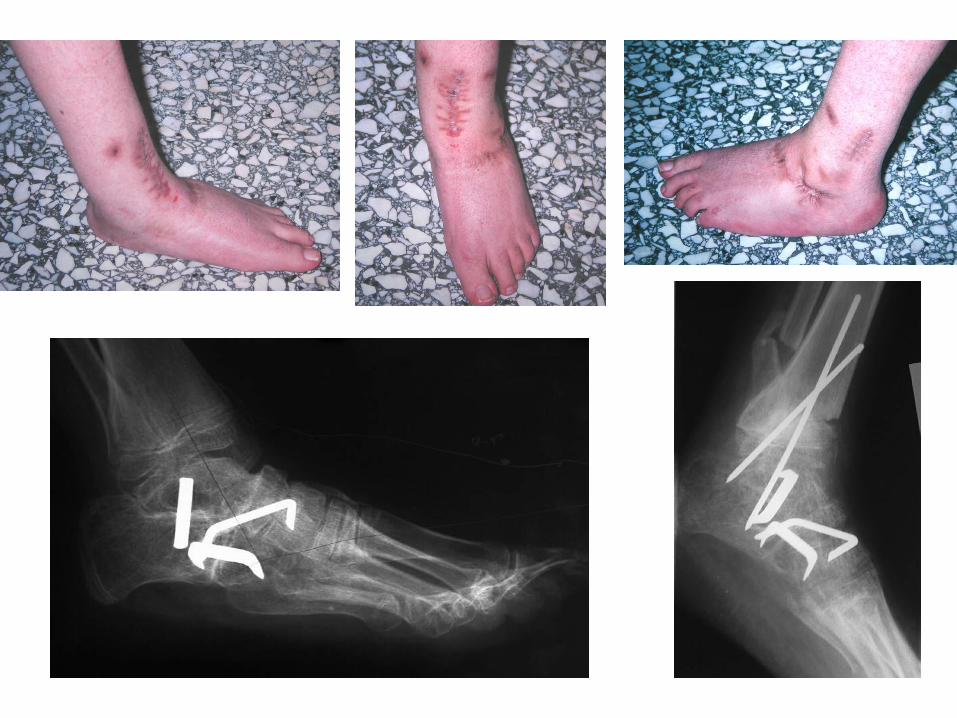

Relapsed or neglected clubfoot
• Ponseti I. Congenital clubfoot, Oxford, England: Oxford University Press, 1996.
• Dwyer FC. The treatment of relapsed club foot by insertion of a wedge into the calcaneum.
J Bone Joint Surg (Br) 1963;45-B:67-75. • Evans D. Relapsed club foot. J Bone Joint Surg (Br) 1961;43-B:722-33. • Triple arthrodesis.

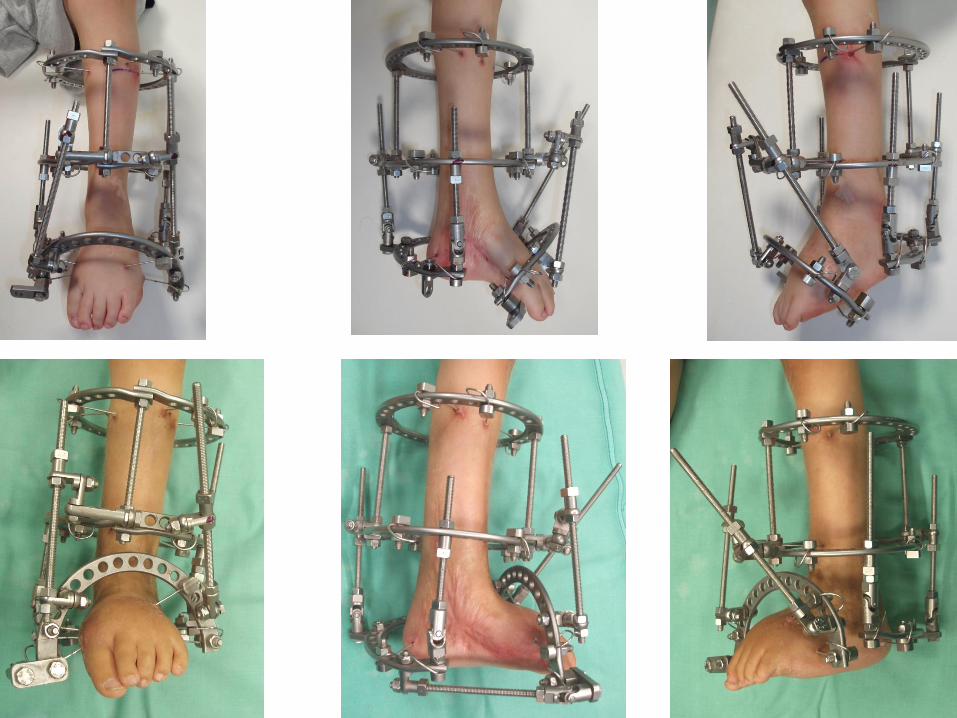
• “The Ilizarov distractor for the correction of relapsed or neglected clubfoot”
GRILL et al JBJS(Br) 1987
• “The Ilizarov technique in correction of complex foot deformities”
GRANT et al Clin. Orthop 1992
• “The treatment of recurrent arthrogrypotic clubfoot in children by the Ilizarov method”
CHOI et al JBJS (Br) 2001

U Osteotomy
V Osteotomy
Grant et al 1992

P. K. M 6y


P.H. M 4y






A. N. M
Age 5y


Ponseti Method of Treatment of Congenital Clubfoot
www.ponseti.info

Ponseti method
• The technique is based on the concept that less is surgical aggression, greater will be the future mobility of the foot.
• By contrast a congenital club foot extensively surgically treated, occur in adulthood rigid, inflexible in its synchondrosis, prolonged and painful to load, less appropriate for a sport.

Ponseti treatment
Reduction of talonavicular joint dislocation
Main step

Ponseti treatment



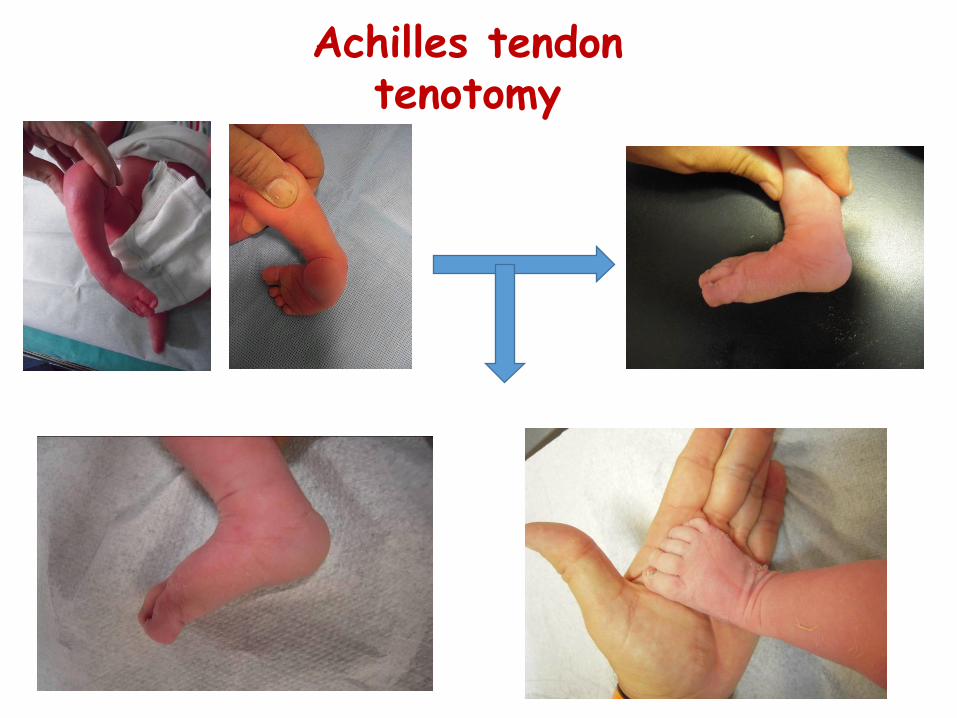
Achilles tendon tenotomy


Club Foot treatment pathway
3D ultrasound 2D ultrasound
1
2 3
4 5
Follow up Skeletal maturity
6
Ponseti serial casting


Ponseti treatment The recurrence
Causes
• Treatment poorly executed • Poor compliance to treatment • Poor adaptation of parents in treatment • Persistence of “noxious stimuli” cause of the
deformity
Treatment poorly executed
• Error performance of the cast • Error in correction • Error in surgical technique • Post-operative treatment is not carried out • Refusal of the tool in abduction

FAILED “PONSETI” Hospital “St Elsewhere”

Relapses
Clin Orthop Surg 2014 Sep;6(3):245-52. Zhao D et al., Relapse of clubfoot after treatment with the Ponseti
method and the function of the foot abduction orthosis.
Age > 2y Anterior tibialis transfer
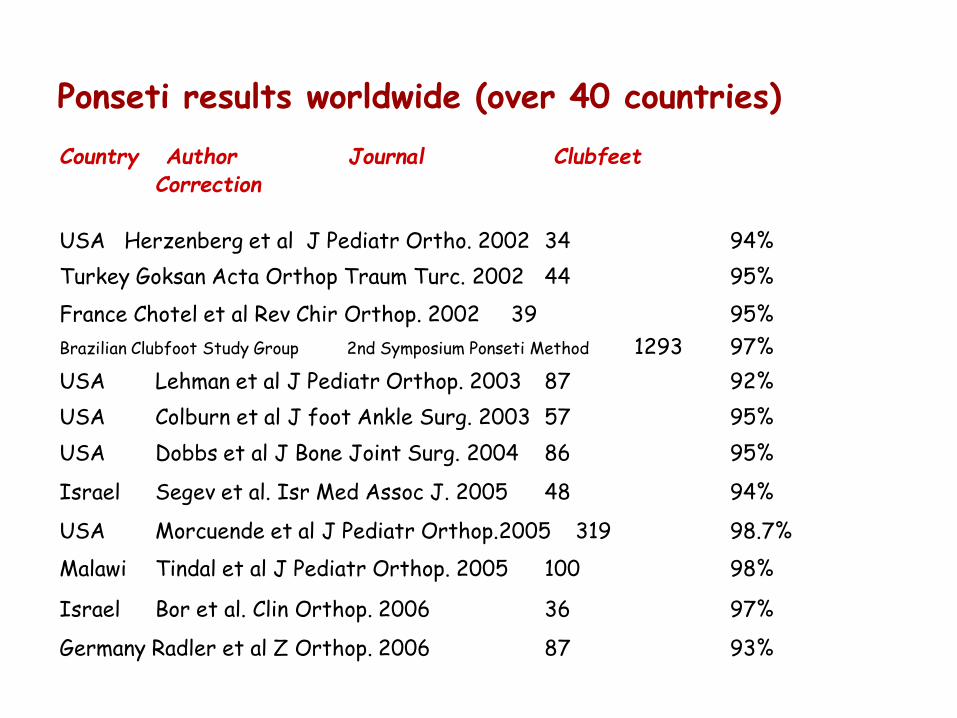
Country Author Journal Clubfeet Correction USA Herzenberg et al J Pediatr Ortho. 2002 34 94%
Turkey Goksan Acta Orthop Traum Turc. 2002 44 95%
France Chotel et al Rev Chir Orthop. 2002 39 95%
Brazilian Clubfoot Study Group 2nd Symposium Ponseti Method 1293 97%
USA Lehman et al J Pediatr Orthop. 2003 87 92%
USA Colburn et al J foot Ankle Surg. 2003 57 95%
USA Dobbs et al J Bone Joint Surg. 2004 86 95%
Israel Segev et al. Isr Med Assoc J. 2005 48 94%
USA Morcuende et al J Pediatr Orthop.2005 319 98.7%
Malawi Tindal et al J Pediatr Orthop. 2005 100 98%
Israel Bor et al. Clin Orthop. 2006 36 97%
Germany Radler et al Z Orthop. 2006 87 93%
Ponseti results worldwide (over 40 countries)

Remember, operate now a clubfoot is no more ethical Ignacio V. Ponseti
EPOS Mallorca 2005

Thank you





























