Embed Size (px)
Citation preview

EXTERNAL LATERAL DISLOCATION OF THE ELBOW*
WELLINGTON D. GRIBEMER, M.D., P.A.C.S.
Chief of Fracture and Orthopedic Service, St. Joseph’s HospitaI
READING, PENNSYLVANIA
D ISLOCATIONS and fractures in or about the eIbow are frequent and, because of the commonIy resuIting
deformities and disabiIities, are a constant chaIIenge to the surgeon. In spite of accumulated experience and a weaIth of Iiterature, many probIems, invoIved in these injuries, remain to be soIved. Having encountered, within a short time, severa exampIes of a rather unusua1 type of eIbow disIocation, it seems that a study and review of that type might be justified.
It is the purpose of this articIe to present the resuIts of a study of externa1 IateraI disIocation of the eIbow, with case reports. DisIocation of both bones at the eIbow can occur in any one of four or more directions, i.e., anterior, posterior, IateraI, mediaI, and divergent. There are, of course, variations in these genera1 types. There seems to have been some confusion in describing IateraI disIocations, some writers considering the dispIacement of the humerus as the basis for distinction. In this discussion, the direction in which the uIna and radius are dispIaced is used to differentiate between the Iesions.
DisIocations are probabIy the most fre- quent of eIbow injuries, exceeding fractures in most series; in one of these they con- stituted 20 per cent of the cases.l The simpIe posterior disIocation is the most frequent; this is foIIowed in order by the posterior with fracture; disIocation of the head of the radius; interna IateraI, or medi- a1; and the externa1 IateraI type. In a study of a series of disIocations by Geist and Henry,2 externa1 IateraI disIocations oc- curred in onIyo.7 per cent. A review of other studies aIso shows that the externa1 IateraI type is rather rare. NeweII,3 in a series of
I,I 14 cases of e’lbow injuries, records twenty-one disIocations none of which were IateraI. The case reports of this variety of disIocation, as reveaIed by a fairIy extensive review of the Iiterature, are appended.
ExternaI Iateral disIocations of the eIbow may be either partia1 or compIete. Tinker4 stated, “ PartiaI outward disIocation of the eIbow joint is so unusua1 that every case seems worth recording.” He reported two cases of partia1 disIocation, one of which was compound. Stimson,’ in discussing externa1 IateraI disIocation, referred to onIy thirteen cases of partiaI dislocation, incIuding one of his own, and beIieved that this represented the entire number reported up to that time. Concerning compIete outward disIocation, he states, “These dislocations, of which the first observation was reported by Dupuytren in 1807, aIthough the form had been described by Petit nearIy one hundred years before, were apparentIy so rare that MaIgaigne couId coIIect onIy ten reported cases. Of Iate, reports have so muItipIied that, excIuding irreguIar cases, those of which the description is not suficientIy detaiIed and those which seem more properIy to belong among disIocations backward, the number of those avaiIabIe for study and generaIization is about twenty-five.” Wilson1 reported three IateraI disIocations in a series of ninety-three patients with dis- Iocations, not indicating the type. Armitage and Armitage5 state, “ External Iateral disIocation of both bones of the forearm is very rare.”
WinsIow’j in reporting his onIy case of compIete externa1 IateraI disIocation de- scribes three varieties. He makes the foIIow- ing statement: “Owing to the anatomic
* Department of Orthopedics, St. Joseph’s HospitaI.
57

58 American Journal of Surgery Griesemer-EIbow Didocation JANUARY, ,940
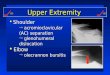
FIG. I. Case I. Anteroposterior view of incompIete externa1 late& disIoca- tion. (August 5, 1935.)
FIG. 3A. Case I. Anteroposterior view after reduction, showing fragment of epitrochlea in proper position. (October 29, 1935.)
FIG. 2. Same case, showing detached placed portion of epitrochIea.
and dis-
FIG. 3n. Same case, showing complete reduc- tion.

NEW SERIES VOL. XLVII, No. I Grresemer-Elbow DisIocation American Journal of Surgery 59
compIexity of the eIbow joint, complete latera dislocations are of extreme rarity.” His cIassification is as foIIows:
I. Directly outward, without rotation of forearm.
2. SubepicondyIar, with elbow flexed nearIy or entirely to a right angle with forearm pronated, the radius being pIaced somewhat anteriorIy to the &a. The great sigmoid cavity is Iocated just beIow the externa1 condyle.
3. Supra-epicondyIar, the forearm being flexed in pronation. The bones of the fore- arm are pIaced above the externa1 epi- condyIe, with considerabIe shortening of the arm, which constitutes the most marked type.
Mechanism. A study of this injury indicates that it is produced by a very unusua1 degree or type of vioIence. It apparentIy resuIts in most cases from a faI1 on the outstretched hand, aIthough it is said to have foIIowed a faI1 on the inner side of the eIbow, or from a direct bIow upon the forearm. Tinker4 beIieved that this disIoca- tion scarceIy ever occurs in a norma aduIt. He further stated that it occurs onIy in
NicoIadoni quoted by Tinker, beIieved that in most cases, evuIsion of the interna condyIe or epitrochIea in these disIocations
FIG. 4. LateraI view in same case after reduction.
FIG. 5. Case II. Antrroposterior view, showing FIG. 6. Lateral view of same cast, showing dis- compIete external Iateral dislocation with pIacement of both bones and fracture at upper radius and ulna impinged on the supinator end of the radius. ridge. (August 12, 1935.)
persons who have an abnorma1 weakness is caused through the tension on the of the capsule and interna IateraI Iigament attached flexor muscIes. In chiIdren, this is of the elbow joint. This no doubt probabIy an epiphysea1 separation. Tinker accounts for the infrequency of the Iesion. attributed this condition to the puI1 on the

60 American Journal of Surgery Griesemer-EIbow DisIocation JANUARY, ,940
interna IateraI Iigament. He produced the disIocation experimentaIIy by abduction of the compIeteIy extended and pronated
FIG. 7. Case II, immediately after reduction, showing improved position of head of radius. (August 12, 1935.)
forearm. Rotation on the humeroradia1 articuIation as a center causes the rupture of the internal IateraI Iigament, thus
of the trochIea, sIiding over the outer ridge of this process, occupying a position vary- ing from the groove between this ridge and the capiteIIum, in the incomplete form, to a position upon the supinator ridge or epicondyIe, in the compIete form.
Physical Signs. Examination usuaIIy shows the forearm in a position between extension and right angIe ffexion, with a variance of anguIation depending on the individua1 case. Pronation of the forearm is common and is due to pressure under the muscIes which take attachment from the externa1 condyIe and are made tense. When the hand of the injured extremity hangs at the side, with the forearm adducted, the axis of the humerus is pointed downward and inward. The norma angIe of the humerus is more downward and outward. The nterna1 condyIe is made prominent, the skin being made very tense over it and it may have a rough edge if the epitrochIea has been avuIsed. There is increased protuberance of the oIeocranon, because the ridge of the sigmoid cavity interIocks in the deep groove between the outer margin of the trochIear surface and the
FIG. 8. Case III. Anteroposterior view, showing partia1 external lateral dislocation, with dis- placement of epitrochlea down- ward and backward. (August 11, 1935)
FIG. 9. LateraI view in same case, showing displaced epitrochIea.
opening the joint. The sigmoid cavity of capiteIIum. The externa1 condyIe is usuaIIy the uIna is then separated from the trochIea not prominent, but may be identified by and its mid-ridge escapes from the groove making strong pressure above the head of

NEW SERVES VOL. XLVII, No. I Griesemer-EIbow Dislocation American Journal of Surgery 61
the radius, behind the extensor muscIes. The very definite widening of the trans- verse diameter of the joint is the most prominent sign. The triceps tendon stands out as a very tense band.
Complications. These disIocations may be compound and comphcated by severe injuries to soft and osseous tissues. Exten- sive Iaceration of the capsuIe and overIying soft tissues, particuIarly the musculature, may occur. The chief vesseIs and nerve trunks may be seriousIy injured, aIthough this compIication is not frequent in the Iiterature. Jeanneney and VieIIag cite a case in which such trauma occurred and was foIIowed by the VoIkmann syndrome. Juvara, in 1930, quoted by Papin,‘O re- ported a case in which there was a paraIysis of the cubita nerve. These complications of the soft parts may be so extensive as to require amputation. Gant,l’ in 1866, re- ported a case of externa1 Iatero-anguIar disIocation in which this operation became
FIG. I IA. Case IV. Anterior-posterior view, showing partial external IateraI dis- Iocation, with evidence of disturbance of external condyIe and dispIacement of epitrochIea into olecranon fossa of humerus. (October 28, 1935.)
imperative on account of the extensive damage to the soft parts. Gerdes,* 1863, reported a case of compIete external
FIG. 10. Case III, showing reduction, with epitrochIea stil1 displaced, but in improved position. (September 8, ‘935.)
FIG. I IB. Diagrammatic representation of Case Iv.

62 American Journal of Surgery Griesemer-Elbow DisIocation JANUARY, 1940
lateral disIocation, with such extensive trauma to the soft parts, that, in spite of non-injury to chief vesseIs and nerve
Diagnosis. Prompt and accurate diag- nosis of injuries invoIving the eIbow region is urgent, for upon it depends the seIection
FIG. 12. Case IV. LateraI view, showing cpitrochIea dispktced into olecranon- fossa of humerus.
trunks, remova of the limb was deemed necessary. Th ese amputations probabIy might have been avoided by the more modern dkbridement and aseptic technique.
The interna condyIe or epitrochIea is frequentIy fractured or avuIsed and may become interposed in the disturbed joint. This condition increases the diffIcuIties of both diagnosis and treatment. The Iocation of the fragment may cause an external appearance of the parts, simuIating frac- ture of the oIecranon (Papin’O). The externa1 condyle may aIso be traumatized, ahhough this does not seem to increase the difficuIty of reduction. In addition to fractures in or about the eIbow joint, there may be such injuries at the Iower IeveIs of the forearm, CoIIes’ fractures probabIy being the most frequent. The additiona fractures are no doubt due to the unusua1 type and degree of vioIence necessary to produce this dislocation.
FIG. 13. Case IV. Anteroposterior view after reduction. In flexion. Showing repIacement of epitrochlea and indi- cating damage to external condyle. (October 28, 1935.)
of the method of treatment. Treatment must vary with the kind of injury. Favor- able prognosis is contingent upon adequate treatment. These are pertinent factors in caring for the disIocation under discussion. The correct diagnosis may be very evident from the physical signs, btit carefu1 x-ray examination shouId be made to establish a more accurate presentation of the condi- tions invoIved. The whole forearm shouId be incIuded in this study, especiaIIy when there is evidence of gross injury in the eIbow region. In two of the cases to be reported, CoIIes’ fracture was present and added to the diffIcuIties of treatment and prognosis.
Treatment. WhiIe our experience in the treatment of these externa1 IateraI disIoca- tions is Iimited, certain points gathered from it and from a review of the reported case histories seem worthy of consideration. Injuries to the soft parts, especiaIIy to the chief nerve trunks and vesseIs, shouId receive carefu1 attention before any manip- uIation is undertaken. In some cases, these injuries may be more important than the underIying fracture or disIocation. As these complications are not pecuIiar to the dislocation under discussion, their manage-

NEW SEI RIES VOL. XLVII, No. I
ment will not be further elaborated upon. should be made promptly. Thi s can be Atten lpt at reduction should not be de- accomplished in the operating rot 3rn bef ‘ore Iayed , for early reposition must be obtained sphnting. Hospitalization of such cases for
Griesemer-Elbow Dislocation American Journal of Su r3-y 63
FIG. 14. Case IV. Anteroposterior view, show- FIG. IS. Same case, showing ing evidence of union of epitrochIea to further union of cpitrochIea. humerus and reparative process of ex- (March g, 1936.) terna condvle with thickening of adjacent periosteum.*(December 2, I&S.) ’
to secure a favorable end result, and also, because reduction becomes more difficult if delayed. Older cases should have at least one attempt at closed reduction. Those eight to ten days old are difficult and are rarely reduced without operation.
General anesthesia to obtain complete relaxation is usually required, for without it effective manipulation is painful and difficult because of muscle spasm. Reduc- tion will usually be obtained by manipulat- ing the forearm into strong pronation, at the same time extending it and continuing with lateral flexion and supination. After reposition, the arm is put into acute Aexion, depending in degree upon the severity of the swelling about the joint. Early reduction often obviates the diffr- culty of swelling. These cases are usually retained by a posterior moulded plaster splint, extending from mid-humerus to the distal ends of the metacarpaIs, with the forearm in supination. An x-ray check
several days is a wise precaution in order to facilitate observation of peripheral nerve function and circulation.
Reduction may be comparatively easy and perhaps may not require any pre- scribed technique other than straight trac- tion, followed by flexion. However, certain cases may be resistant, the cause of this resistance not being evident in the x-ray plates. In these, continued or repeated forceful attempts at reduction should not be made for fear of added damage to the soft parts, especially nerves and vessels that may be atheromatous.
If closed reduction fails in competent hands, we agree with Winslow6 and Papin’O that open operation should be done at once, for, while there is risk of infection in open reduction, the importance of obtaining prompt reposition is so great that, under proper conditions, it seems worthwhile to assume this risk. Cases showing interposi- tion of the displaced epitrochlea or other

64 American Journal of Surgery Griesemer-EIbow DisIocation
fragments. indicate earIy surgica1 inter- ference, if manipuIation does not attain proper reposition. An interposed epitroch-
FIG. 16. Case v. Anteroposterior view showing compIete external latera dis- location in SubepicondyIar position. (September 30, 1935.)
Iea shouId be dislodged and the elbow reduced; then if Iarge, it may be fixed at its proper position; if smaI1, it may be removed entireIy. In one case, not person- aIIy treated but reported with this paper, open operation was done three weeks after the injury, but no attempt was made to repIace the epitrochIea. Postoperative x-ray showed that the *reduction had been main- tained but with a fair-sized epitrochIea stiI1 wideIy dispIaced, with no interposition. This condition apparentIy has not inter- fered with the end resuIt. However, we beIieve it wise to dea1 definiteIy with this process of bone, even if it is not interposed. Guerin, quoted by Papin,‘O cites a case in which the epitrochIea came out of the articuIation, anteriorIy. By means of a bodkin thrust through the skin, he repIaced the epitrochlea into position.
Open operation affords an opportunity for inspecting the joint with respect to disturbing eIements such as interposed tissues or smaI1 bone fragments, which may have been missed in the x-ray picture. It aIIows for the carefu1 remova of bIood cIots that might Iater undergo osseous
changes and disturb joint function. This inspection of the joint cavity must be most carefu1, with a minimum of manipuIation, and should never incIude digita examina- tion. In one case presented, in which cIosed reduction faiIed, earIy operation revealed conditions which wouId have resisted any further manipulations in attempting cIosed reduction, and which no doubt wouId have resuIted in further damage to soft .parts. Unreduced cases wiI1 usuaIIy resuIt in disabIed and painfu1 joints, requiring radica1 treatment Iater. OccasionaIIy an oId unreduced case may have a degree of function which does not warrant any attempt at improvement.
If there is much skin damage or sweIIing about the joint, operation must be deIayed. However, this is a matter of circumstance and judgment. We feel that under proper conditions, patients seen within three hours after the accident and considered operative, may be operated upon at once with com- parative safety, for within this period it is beIieved that damaged tissues retain a definite resistance to infection.
Active motion, with arm supported in spIint shouId be started early-within twenty-four hours in cases treated by cIosed reduction and in thirty-six hours in cases which have received operative treat- ment. At first this active motion must be carefuIIy guarded and be limited to ffexion, depending upon the degree of pain and sweIIing. Under strict supervision, prona- tion and supination with Aexion should foIIow, so that within three or four weeks satisfactory function shouId be attained in most uncomplicated cases. The more com- plicated cases wiI1 aIso show a better percentage of good resuIts, if early, properIy supervised active motion is instituted. Proper physiotherapy is aIso an aid to recovery, but should not be depended upon to the excIusion of the patient’s obn motion. One of the causes of unsatisfactory resuIts in eIbow joint cases has been pro- longed immobilization. Some of the earIier writers recognized this factor which has been too much overIooked in Iater years.

NEW SERIES VOL. XLVII, No. I Griesemer-EIbow DisIocation American Journnl of Surgery 6s
F. M. Johnson,r2 in 1880, caIIed attention to the danger of fixing joints for too Iong a
and end resu1t.s cannot aIways be ascer-
period, citing an eIbow case with resulting tained. However, we beIieve that, if earIy reduction is accomphshed in these disloca-
FIG. 17. Case v. Lateral view, showing Iateral FIG. 18. Same case, showing reduction, with displacement with a spIinter fracture of slight upward displacement of fragment the ulna. (September 30, 1935.) of ulna. (October I, 1935.)
ankyIosis from such a procedure. He advocated passive motion. However, we fee1 that carefu1 active motion is the better method. H. J. BigeIow,13 in 1868, spoke of the “genera1 impropriety of passive motion in treatment of fractures and disIocations of the elbow joint.”
tions, whether simple or compIicated, the resuIts wiI1 be much improved.
CASE REPORTS
Prognosis. Prognosis must aIways be guarded in these cases as in any injury invoIving the eIbow joint. Even though compIete and earIy reduction has been obtained in a simple case, secondary joint changes may take pIace and cause more or Iess disability. The causes of these dis- abIing aIterations have not been entireIy expIained. Certain writers beIieve that, because of the numerous centers of ossifica- tion in the eIbow region, an injury in- voIving them may cause irritation with resulting excessive ossifying changes in the fracture lines, as we11 as ossification of bIood cIots and damaged muscIe tissues. Such changes may occur in the absence of demonstrated fracture lines.
CASE I. A. G., aged IO years, entered the hospita1 August 5, rg35 at 8 P.M., immediateIy after a faI1 on his outstretched hand. Examina- tion showed a deformity of the right elbow with marked widening. The forearm was held in extension, with sIight pronation. The diagnosis was an unusua1 disIocation of the elbow, with possibIe fracture. There was no disturbance of the peripheral circulation or nerve function. X-ray examination (Figs. 1-4) showed an in- compIete external Iateral dislocation of the elbow joint, with avuIsion of the epitrochIea.
These cases shouId have adequate foI- low-up treatment and observation and be IinalIy rated as to result at the end of a year. This procedure is not aIways possible
Treatment. Under genera1 anesthesia, an attempt at reduction was made immediatery. This was unsuccessfu1 and, as further effort seemed useless, it was abandoned for fear of causing added injury to the soft parts. The cause of faiIure was not evident on further examination or in a study of the x-ray pIates. Consent for immediate operation could not be obtained. The patient was put to bed, with forearm in traction; this treatment was main- tained’for twelve hours. It was hoped that this traction might overcome the muscIe spasm and perhaps aIIow reduction. A second effort to reduce was unsuccessful and permission for

66 American Journal of Surgery Griesemer-EIbow DisIocation JANVARY, r940
operation was given. The operation was per- formed about thirteen hours after the accident. A posteroIatera1 incision exposed the interior
FIG. 19. Case v. Showing compIete reduction. (Octo- ber I, 1935.1
of the joint, revealing a situation that wouId have defied any attempt at closed reduction. The radius was dispIaced anteriorly with its head forced upward through the orbicular ligament and the anterior portion of the joint capsule. It was firmIy fixed in this position by a constricting band around it, immediately beIow the head. Before reduction couId be accompIished, this band required incision. The joint was then carefuIIy flushed with norma saIine solution, removing a moderate amount of partially cIotted bIood. After reduction of the joint and replacement of the epitrochIea, the torn orbicuIar Iigament, joint capsuIe and other injured tissues were repaired with catgut. The skin was closed with siIkworm gut tied over smaI1 rubber tension tubes. Retention of posi- tion was obtained by use of a posterior moulded pIaster spIint, extending from the middIe of the upper arm to the distal ends of the metacarpals, with elbow flexed sIightIy Iess than 90 degrees, forearm being placed in supination.
Postoperative Course. This was uneventful, with no rise of temperature or other complica- tion. SIight active motion in spIint was started within twenty-four hours. This was increased as conditions permitted. The wound heaIed normaIIy and the patient Ieft the hospita1 on the tenth day. The spIint was removed entirely at the end of the third week. Motion at this time was fair in a11 directions. Restriction in extension was the most marked impairment.
Three months after the injury a11 functions of the elbow were recovered, with the exception of complete extension, and this returned in an additiona two weeks. One year after the injury, there was no impairment of any of the functions of the elbow joint.
CASE II. Mrs. H. M., aged 79 years, entered the hospita1 August IZ, 1935, shortIy after having faIlen on her outstretched right hand. Examination showed gross deformity of both right wrist and elbow, with a smaI1 bIeed- ing wound over the uIna about 2 inches beIow the olecranon. There was marked discoIoration and sweIIing of the upper third of the forearm and about the elbow. No disturbance of the peripheral circuIation or nerve function was noticed. The eIbow was considerabIy widened with prominence of the interna condyIe of the humerus. The forearm was pronated and definiteIy shortened. Diagnosis of externa1 IateraI disIocation of the eIbow, with a CoIIes’ fracture and a compounding wound of the uIna was made. X-ray study (Figs. 5-7) showed a compIete externa1 IateraI disIocation of the elbow, with a fracture of the head of the radius. In addition, a CoIIes’ fracture with marked displacement was noted.
Treatment. Under gas-oxygen anesthesia, the disIocation was easily reduced by using straight traction foIIowed by ffexion. The wound, which was not deep, was treated and tetanus antitoxin given. The ColIes’ fracture was manipuIated into satisfactory position, and anterior and posterior mouIded pIaster spIints were applied to the forearm. On account of the sweIIing about the elbow, the spIints were not made to incIude that joint. The arm was pIaced
in 90 degrees fI exion. X-ray (Fig. 7) showed compIete reduction of the dislocation, with
satisfactory position of the bones invoIved in the CoIIes’ fracture. The position of the head
of the radius, while not entireIy satisfactory, was considered to be the best that couId be accomplished at the time.
The sweIIing receded rapidIy and the wound caused no troubIe. Guarded active motion was begun at the elbow on the second day and at the wrist on the third day. The patient Ieft the hospita1 on the fifth day. Two months after the injury, there was good motion at the wrist with slight restriction in extension of the eIbow. FIexion was compIete. Supination of the fore- arm was somewhat restricted.

NEW SERIES VOL.. XLVII, No. I Griesemer-Elbow DisIocation American Journal of Surgery 67
By February, 1936 there was compIete plete external IateraI disIocation of the eIbow, restoration of function at the wrist and eIbow complicated by avulsion of the epitrochIea. except for restriction of supination. In August Treatment. SeveraI unsuccessfu1 attempts
FIG. 20. Case VI. LateraI view showing marked comminution.
FIG. 21. Case VI. Anteroposterior view showing partial externa1 latera dislocation in subepicondylar position with a large fracture of externa1 con- dyIe and dispIacement of a smaIIer unidentified fragment beIow joint.
there was the same restriction of supination as at the previous examination. However, the function of the wrist and elbow was generalty satisfactory, considering the injury encoun- tered and the age of the patient. She was able to do Iight work about the house and was satisfied with the outcome.
Comment. This case is an exampIe of the complete supra-epicondyIar type and iIIustrates easy reduction, in spite of comphcating factors, which adverseIy affected the outcome.
CASE III. M. S., aged 52 years, was ad- mitted August 9, 1935, shortly after having fallen down a flight of five steps, landing on the Ieft side with the entire weight of her body on the Ieft forearm. Examination showed a deformity of the Ieft wrist and marked sweIIing and widening of the elbow. There were aIso muItipIe lacerations about this region. No disturbance of periphera1 circuIation or nerve function was evident. The wrist had been fractured severa years before, sIight impair- ment resuhing. X-ray examination (Figs. 8 and 9) showed a fracture of the distal end of the radius with position fair, and aIso an incom-
at reduction under the fluoroscope were made. Open operation was advised, but was deIayed because of the condition of the skin about the eIbow. On August 30, 1935, three weeks after the accident, open operation was performed. A posterior Kocher incision was used to expose the area. After cIeaning out the oIecranon fossa, reduction was easiIy obtained. No at- tempt was made to replace the epitrochIea. Position was maintained by the use of a posterior anguIar splint.
The postoperative course was uneventfu1, with no evidence of infection. EarIy motion of the wrist and elbow was started. On the patient’s discharge from the hospita1 two and one-half weeks after operation, there was a fair degree of function, with, however, some limitation of Aexion and extension.
Seven months after the injury, the patient was able to do her usua1 housework. Flexion of the elbow was compIete, and extension was 74 per cent of normal. Pronation was compIete with 74 per cent of normal supination. There was sIight pain in the wrist. In August 1936, there was genera1 improvement of all

68 American Journal of Surgery Griesemer-Elbow DisIocation Jarwmu, I$W
functions, although there was still sIight after considerabIe difficulty. Excessive force restriction of supination. was not used. X-ray (Fig. I 3) showed reduction
Comment. This case iIIustrates the type due compIete, with the fragment of the internal
FIG. 22. Case VI. LateraI view after reduction showing con- siderable anterior dispIace- ment of externa1 condyle. Later views indicated im- provement.
to a faI1 directIy on the elbow and forearm. We do not fee1 that the severa attempts at reduction under the fluoroscope were wise, as the sweIIing and skin Iacerations about the joint were aggravated, thus proIonging the preoperative period. AIso we think it wouId have been more judicious to have deaIt more definiteIy with the avuIsed epitrochIea.
CASE IV. J. I., aged 14 years, was admitted October 28, 1933, shortIy after sustaining a faI1 on his Ieft eIbow. Examination showed considerabIe discoIoration, with widening and marked sweIIing of the eIbow joint. The arm was heId in moderate pronation. PeripheraI nerve function and circuIation were not dis- turbed. The diagnosis of externa1 IateraI disIocation of the elbow, with possibIe fracture of the oIecranon, was made. X-ray study (Figs. I I and 12) reveaIed a partia1 externa1 IateraI disIocation of the eIbow, with a cornminuted fracture of the externa1 condyIe, a fragment of the interna condyIe Iay in the oIecranon fossa of the humerus.
Treatment. Under genera1 anesthesia, ap- parentIy satisfactory reduction was obtained
FIG. 23. Case VI. Anteroposte- rior view after reduction.
condyIe in good position. Because of the marked swelling, no attempt at splinting the elbow was made. The patient was put to bed with his forearm heId at right angIe flexion. Heat was applied and slight active motion was aIlowed on the second day. On the third day the sweIIing had subsided suffIcientIy to aIIow the application of a posterior mouIded pIaster spIint, with a sIight increase of fIexion. The pa- tient was discharged the same day, reporting to the Out-Patient Department two days Iater when increasing active motion was started.
At the end of the fourth week, motions of the joint were norma except for sIight restric- tion of extension. Four and three-fourths months after the injury, examination showed compIete return of function, with union of the repIaced fragment of the internal condyle. (Fig. IS.)
Comment. This is an exampIe of the type of injury due to a direct faI1 on the elbow. It indicates that, even in the presence of an inter- posed fragment, satisfactory cIosed reduction may at times be accompIished and that such a replaced fragment may become firmIy re- united to the contiguous portion of the humerus.
CASE v. S. D., aged 36 years, was admitted September 30, 1933, severa hours after a

NEW SERIES VOL. XLVII. No. I Griesemer-EIbow DisIocation American Journal of Surgery 69
fall on the outstretched left hand. There was deformity, with marked widening of the Ieft elbow. A diagnosis of externa1 Iateral disIoca- tion was made. No disturbance of the periphera1 circulation or nerve distribution was found. X-ray (Figs. 16 and I 7) showed a compIete externa1 Iateral disIocation of the elbow, with a spIinter fracture of the oIecranon.
Treatment. Under general anesthesia, reduc- tion was obtained without any d&cuIty, by using straight traction folIowed by flexion. X-ray check (Fig. 18) indicated complete reduction of the disIocation with the fragment of the olecranon in fair position. A posterior mouIded pIaster spIint was appIied with arm in acute ffexion. Patient refused to be admitted to the hospita1 and was sent to her home some distance from the city. No further record was obtainabIe, so that the end resuIts cannot be known. However, with the prompt and satis- factory reduction, we believe that a usefu1 result was obtained.
This case represented the subepicondyIar
type. CASE VI. Mrs. H. W., age 33 years, was
first seen JuIy 9, 1938, twenty-two hours after a faI1 on the right elbow and after an unsuccess- ful attempt at reduction. A description of the origina deformity cannot be given. The origina x-ray plate showed an externa1 latera disloca- tion, and a fracture of the externa1 condyIe with dispIacement of a Iarge fragment IateraIIy and a smaIIer unidentified fragment Iying some distance below the joint. The unusua1 type of disIocation had not been recognized. At the time of examination there was no disturbance of periphera1 circuIation or nerve function.
Treatment. Under genera1 anesthesia, strong traction with pronation followed by supination and Aexion was made. Retake in operating room showed satisfactory reduction. Fixation in pIaster splints, in acute Aexion was appIied. The patient was discharged the next day, with instructions as to earIy active motion. On August 16, function was good, with slight re- striction of extension. By December recovery was compIete.
Comment. This was a case of the sub- epicondyIar type. In spite of deIayed reduction, a good resuIt was obtained.
SUMMARY
I. A study of externa1 IateraI disIoca- tion of the eIbow is presented, indicating
that reported cases of both compIete and incompIete disIocations are infrequent.
2. This type of disIocation is often compIicated by fractures, in or about the elbow and at the Iower IeveIs of the fore- arm. Therefore, an x-ray study of the whoIe forearm shouId aIways be a part of the examination.
3. As earIy recognition is of importance, the chief of service shouId see such cases promptly.
4. Reduction, under genera1 anesthesia, should be attempted at once, but the force exerted shouId be gentIe.
5. If earIy cIosed reduction faiIs, open operation shouId be performed at once, especiaIIy if there is interposition of bone fragments.
6. Extensive skin Iacerations and joint sweIIing, as a ruIe, contraindicate opera- tion. However, operation may be con- sidered in these cases if they are seen within three hours after accident, as tissues retain a resistance to infection within this period.
7. Open reduction permits inspection of the joint and remova of interposed tissues and extravasated bIood, whiIe reducing the possibiIities of Iater joint changes.
8. Fixation shouId be maintained in supination with flexion to such an acute angIe as may be permitted by the sweIIing.
g. It is a wise precaution to hospitaIize these patients severa days for observation.
IO. EarIy active motion is essentia1 in either open or cIosed reduction to obtain earIy restoration of joint function.
I I. As in a11 eIbow injuries, prognosis must be guarded.
12. Adequate foIIow-up supervision is indicated for a proper rating of end resuIts.
13. Six case reports are given.
REFERENCES
I. WILSON, P. D. Fractures and dislocations in region of eIbow. Surg., Gynec. CT Obst., 56: 335-359,
‘933. z. GEIST, E. S., and HENRY, M. 0. DisIocations and
simpIe fractures of elbow. Minnesota Med., I I : 509-513, 1928.

70 American Journal of Surgery Griesemer-EIbow Didocation JANUARY, ,940
3. NEWELL, E. T. Fractures, epiphysea1 separations and disIocations; r&sum& of I I 14 cases. Soutb. M. J., 19: 688-690, 1926.
4. TINKER, M. B. OId compound partiat outward dis- location of the elbow and resection. Am. Med., 4: 539-541, 1902.
5. ARMITAGE, H. M., and ARMITACE, G. L., JR. Treatment of injuries in the vicinity of the elbow joint. Ann. Surg., 63: 596-605, 1916.
6. WINSLOW, R. CompIete external dislocation at the eIhow. Ann. h-g., 31: 595-599, Igoo.
7. STIMSON, L. A. Fractures and DisIocations, 3rd ed. New York and PhiIa., Igoo. Lea Bros. & Co.
8. GERDES. CompIete Luxation des EIIbogengeIenks nach aussen. COT.-Bl. j. d. Aerzte u. Apoth. d. Grossherz., 2: 289-292, 1863.
g. JEANNENEY and VIELLE. Luxation du coude chez un homme de 22 ans. Rupture de I’artere et de Ia
veine hum&raIes. Syndrome de Volkmann. J. de mbd. de Bordeaux, 57: 522-524, 1927.
IO. PAPIN, EDOUARD. Luxation externe du coude avec fracture de I’CpitrochICe. J. de mkd. de Bordeaux, Iog: 25-26, 1932.
I I. GANT, F. J. An externa1 Iatero-anguIar disIocation of the right eIbow-joint; a new form of dis- Iocation, with dissection of the limb. Brit. PP For. M.-Cbir. Rev., 37: 195-201, 1866. Proc. Roy. Med. Ed Cbir. Sot. Lond., 5 : 102, 1864- I 867.
12. JOHNSON, F. M. CompIete outward disIocation of radius and uIna. Tr. M. A. Missouri, 23: 33, 1880.
I 3. BIGELOW, H. J. PracticaI views of the treatment of fractures and dislocations of the elbow-joint, and on the genera1 impropriety of passive motion. Boston M. ti S. J., 78: zag-21 I, 1868.
I HAVE many times seen a doctor whose muscIes are not 50 per cent as
strong as the muscIes of his patient, trying to reduce a fracture with his own hands without any form of mechanica contrivance to help him.
From-“Fractures” by PauI B. Magnuson, third edition (Lippincott).