Embed Size (px)
Citation preview

Clinical Radiology (1989) 40, 518-519
Experience with the Merck Small Bowel Enema Tube A. J. CHIPPINDALE* and S. DESAI~
*Department of Diagnostic Radiology, Stopford Medical Building, Oxford Road, Manchester and ~Department of Diagnostic Radiology, Royal Albert Edward Infirmary, Wigan Lane, Wigan
We describe our experience using the Merck 10 French small bowel enema tube in 50 patients. Small bowel intubation was quick and easy to perform, and the tube was well tolerated by our patients. Kinking of the Merck tube was correctable, but prolonged the examination. The examination had to be abandoned in 6% of cases due to retrograde movement of the tube back into the stomach.
Since the first description of a complete examination of the small bowel by barium infusion (Pesquera, 1929), there ha,,e been a number of technical developments which have lead to the increasing popularity of small bowel enema. Duodenal intubation was facilitated, first by the co-axial tube system (Scott Harden et al., 1960) and then by the 14 French gauge Bilbao Dotter tube (Bilbao et al., 1967). Sellink (1974) emphasised the importance of both adequate bowel preparation and the administration of large volumes of appropriate density contrast medium to ensure rapid transit and adequate distension of bowel loops. Nolan and Cadman (1987) have described the routine use of a 12 French gauge Sellink modified Bilbao Dotter tube (Nolan tube) in over 2000 patients.
However, intubation and positioning of the tube remains a problem, both in terms of discomfort and time involved. We describe our experience of 50 patients undergoing this examination using a new 10 French small bowel enema tube.
PATIENTS AND M E T H O D S
Between November 1987 and June 1988 we performed small bowel enemas in 50 patients, 26 male and 24 female (mean age 39.7 years, range 16 to 73 years). The clinical indication for small bowel enema was Crohn's disease (26 patients), abdominal pain (6 patients), small bowel obstruction (1 patient), malabsorption (6 patients), diarr- hoea (8 patients) and gastrointestinal bleeding (3 patients).
Small bowel enema was performed using the Merck 10 French 140 cm weighted small bowel enema tube in 10 patients with the Corsafe tip, and in 40 with the Silk tip, (Merck L t d Alton, Hampshire). The examination was explained to the patient and local anaesthetic spray applied to the pharynx. All intubations were performed by one operator (SD), who had substantial experience of the Nolan tube. The Merck tube was passed by mouth with the patient in the sitting position. Duodenal intuba- tion was achieved using the techniques described by Nolan and Cadman (1987), the tube being advanced over a stiff guidewire whose tip lay proximal to the pylorus. The tip of the tube was positioned so that the side holes were beyond the ligament of Treitz. A dilute barium suspension (Micropaque diluted to 20% weight to
volume) was infused from a plastic enema bag under gravity to achieve adequate small bowel distension.
RESULTS
Intubation was successful in all patients. Subjectively it appeared easier to intubate the duodenum with the Merck tube than with the Nolan tube. Three of our patients had experience of small bowel enema using both tubes. One of these patients was unable to tolerate the Nolan tube, but intubation with the Merck tube was possible during the same session. All three patients volunteered that the Merck tube was more acceptable.
A satisfactory flow rate was achieved in all Completed examinations, with the bag of barium approximately 1 metre above the table top.
In 8 of 50 patients (16%) the Merck tube became kinked in the small bowel, preventing barium flow (Fig. 1). Manoeuvres to straighten the tube were successful, but the resultant repositioning prolonged room occupancy and increased screening time.
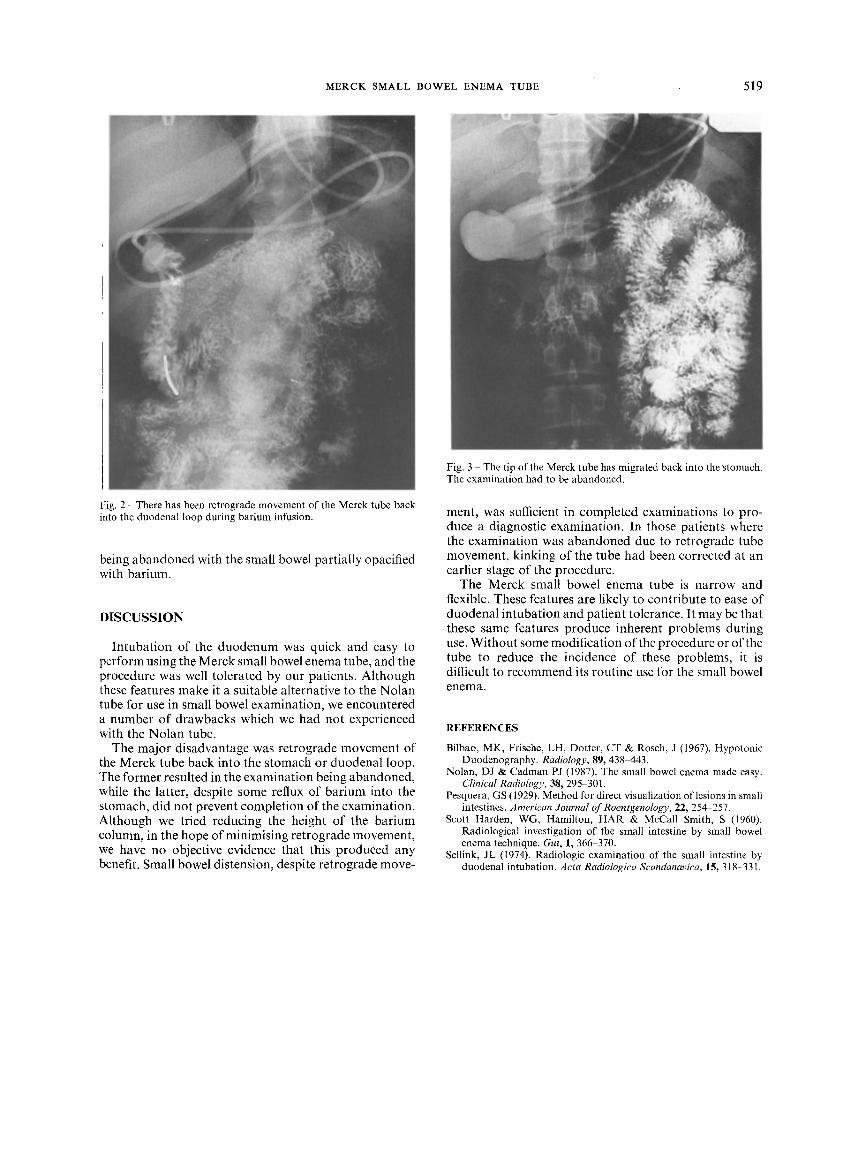
Retrograde movement of a satisfactorily placed tube was observed in 10 patients (20%). In seven (14%), this retrograde movement brought the tip of the tube back into the duodenal loop (Fig. 2). Reflux of barium into the stomach was observed in these patients, although small bowel distension was adequate. In three cases (6%), retrograde movement brought the tip of the tube back into the stomach (Fig. 3) resulting in the examination
Correspondence to: S. Desai, Consultant Radiologist, Royal Albert Fig. 1 The Merck tube kinked in the proximal small bowel prior to Edward Hospital, Wigan Lane, Wigan. barium infusion.
MERCK SMALL BOWEL ENEMA TUBE 519
Fig. 2 - There has been retrograde movement of the Merck tube back into the duodenal loop during barium infusion.
being abandoned with the small bowel partially opacified with barium.
DISCUSSION
Intubation of the duodenum was quick and easy to perform using the Merck small bowel enema tube, and the procedure was well tolerated by our patients. Although these features make it a suitable alternative to the Nolan tube for use in small bowel examination, we encountered a number of drawbacks which we had not experienced with the Nolan tube.
The major disadvantage was retrograde movement of the Merck tube back into the stomach or duodenal loop. The former resulted in the examination being abandoned, while the latter, despite some reflux of barium into the stomach, did not prevent completion of the examination. Although we tried reducing the height of the barium column, in the hope of minimising retrograde movement, we have no objective evidence that this produced any benefit. Small bowel distension, despite retrograde move-
Fig. 3 - The tip of the Merck tube has migrated back into the stomach. The examination had to be abandoned.
ment, was sufficient in completed examinations to pro- duce a diagnostic examination. In those patients where the examination was abandoned due to retrograde tube movement, kinking of the tube had been corrected at an earlier stage of the procedure.
The Merck small bowel enema tube is narrow and flexible. These features are likely to contribute to ease of duodenal intubation and patient tolerance. It may be that these same features produce inherent problems during use. Without some modification of the procedure or of the tube to reduce the incidence of these problems, it is difficult to recommend its routine use for the small bowel enema.
REFERENCES
Bilbao, MK, Frisehe, LH, Dotter, CT & Rosch, J (1967). Hypotonic Duodenography. Radiology, 89, 438 443.
Nolan, DJ & Cadman PJ (1987). The small bowel enema made easy. Clinical Radiology, 38, 295 301.
Pesquera, GS (1929). Method for direct visualization of lesions in small intestines. American Journal t?fRoentgenology, 22, 254 257.
Scott Harden, WG, Hamilton, HAR & McCall Smith, S (1960). Radiological investigation of the small intestine by small bowel enema technique. Gut, 1, 366 370.
Setlink, JL (1974). Radiologic examination of the small intestine by duodenal intubation. Acta Radiologica Scandanavica, 15, 318-331.

















![Enema Administration[1]](https://img.dokumen.tips/doc/110x75/55289a1f49795921048b4a43/enema-administration1.jpg)











