-
Hemostasis
-
HemostasisBlood must be fluidMust coagulate (clot) at
appropriate timeRapidLocalizedReversible
-
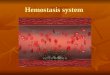
Normal HemostasisA well regulated processMaintains blood in a
fluid, clot free state in normal vessels Induces the rapid
formation of a localized hemostatic plug at the site of vascular
injury
-
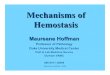
Normal sequence of Hemostasis (4 steps)1. Arteriolar
vasoconstriction (transient)Reflex neurogenic mechanismsBleeding
would resume after vasoconstriction if it werent for the activation
of platelets or coagulation systems
-
2. Exposure of subendothelial ECM when there is endothelial
injuryECM, especially collagen, is highly thrombogenicPlatelets
adhere and become activatedChange in shapeRelease of secretory
productsAggregation of platelets forms hemostatic plugThis is
primary hemostasis
-
First two steps of normal hemostasis
-
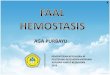
Normal hemostasis continued3. Tissue factor released at the site
of injury (by endothelial cells)Works with secreted platelet
factorsActivates coagulation cascadeA series of proteins where
thrombin is activatedInduces further platelet recruitment and
granule releaseEnds in fibrin depositionCalled secondary
hemostasis
-
Normal hemostasis continued4. Formation of permanent
plugPrevents further hemorrhagePolymerized fibrin and platelet
aggregationCounter regulatory mechanisms (t-PA) limit the plug to
the site of the injury
-
Steps 3 and 4
-
The Main Players in HemostasisEndothelial
cellsPlateletsCoagulation cascade
-
Endothelial CellsProduce vWF (vonWillebrand factor)A product of
normal endothelium found in the plasmaessential for platelet
binding to collagen and other surfacesSecrete Tissue factorinduced
by cytokines (TNF, IL-1)activates the extrinsic clotting
pathway
-
Endothelial Cells have Prothrombotic EffectVia vWF and tissue
factor factors that depress fibrinolysis factors needed for the
clot are not destroyed before clot formsCollagen is
highlythrombogenic
-
PlateletsExpress glycoprotein receptors on membranes. Gp
Ib,IIb/IIIaHave three types of granulesAlpha granulesFibrinogen,
fibronectin, factor V and VIII, PDGF, TGFbDense bodies or delta
granulesATP/ADP, ionized calcium, histamine, serotonin,
epinephrineLysosomal granules
-
PlateletsHyalomere and granulomere
-
Platelets continuedUpon encountering the ECM, platelets undergo
three general reactions:1. Adhesion and shape change mediated by
vWF and glycoprotein Ib2. Secretion (release reaction)calcium
required in coagulation cascadeADP as mediator of platelet
aggregationSurface expression of phospholipid complexBinding site
for calcium ions and coagulation factors
-
Platelets continued3. AggregationADP and TXA2 (vasoconstrictor
thromboxane A2) are the stimuli for the formation of the primary
hemostatic plugAspirin inhibits synthesis of TXA2Fused mass of
plateletsCreated by coagulation cascade that produces thrombin
Thrombin also converts fibrinogen to fibrin cementing platelets in
place
-
PEMBEKUAN DARAH /SISTEM KOAGULASIProses koagulasi merupakan
rangkaian reaksi enzimatik yg melibatkan : protein plasma sbg
faktor koagulasi fosfolipid Ca 2+Produk akhir jendalan fibrin
-
Faktor koagulasi
FactorCommon name(s)IFibrinogenIIProthrombinIIITissue Factor,
Tissue ThromboplastinIVCalsium IonVLabile Factor,
ProaccelerinVIVIIStable Factor, ProconvertinVIIIHemophilia A
factorIXChristmas Factor, Hemophilia B Factor, Plasma
Thromboplastin ComponentXStuart Prower FactorXIHemophilia C factor,
Plasma Thromboplastin Antecedent (PTA) XIIHageman Factor, Contact
FactorXIIIFibrin Stabilizing Factor, Laki-Lorand
FactorPKPrekallekrein, Fletcher FactorHMWKHigh Molecular Weight
Kininogen, Fitzgerald Factor
-
Jalur Intrinsik Jalur Ekstrinsik XII VII Kontak XIIa Ca++ HMWK
PK K Tromboplastin jaringan XI XIa
IX Ixa VIIa PF3 VIII Tenase Complex Ca ++
Jalur Bersama X Xa V PF3 Prothrombin Converting Complex Ca++
Fibrinogen Protrombin Trombin Fibrin Monomer
Fibrin Polimer Soluble XIII XIIIa Ca++ Fibrin Polimer
Insoluble
-
FibrinogenFibrinThrombinProthrombinXaVaVIIaTFExtrinsic
PathwayIXaVIIIaXIaXIIaIntrinsic pathwayXIIIaSoft clotFibrinHard
clotVVIII
-
FibrinogenFibrin
-
FibrinogenFibrinThrombin
-
FibrinogenFibrinThrombinProthrombinXaVa
-
FibrinogenFibrinThrombinProthrombinXaVaVIIaTFExtrinsic
Pathway
-
FibrinogenFibrinThrombinProthrombinXaVaVIIaTFExtrinsic
PathwayIXaVIIIaXIaXIIaIntrinsic pathwayXIIIaSoft clotFibrinHard
clot
-
FibrinogenFibrinThrombinProthrombinXaVaVIIaTFExtrinsic
PathwayIXaVIIIaXIaXIIaIntrinsic pathwayXIIIaSoft clotFibrinHard
clotVVIII
-
Hemophilia A
Deficiency of/nonfunctional VIII
Hemophilia BDeficiency of /nonfunctional IX
Why do they bleed?
-
FibrinogenFibrinThrombinProthrombinXaVaVIIaTFExtrinsic
PathwayIXaVIIIaXIaXIIaIntrinsic pathwayXIIIaSoft clotFibrinHard
clotVVIII
-
FIBRINOLISISProses penghancuran deposit fibrin oleh sistem
fibrinolitik aliran darah terbuka kembaliSistem Fibrinolitik, td :-
Plasminogen- Aktifaktor Plasminogen- Inhibitor PlasminSistem
Fibrinolitik dicetuskan oleh adanya aktivator plasminogen memecah
plasminogen plasmin
Aktivasi plasminogen :jalur intrinsik jalur ekstrinsik jalur
eksogen
-
FibrinFibrin Split Products (FSP)PlasminFibrinolysis
-
FibrinFibrin Split Products (FSP)PlasminPlasminogen
tPAFibrinolysis
-
Skema Fibrinolisis Intrinsik Ekstrinsik Eksogen (XIIa,Kalikrein)
(t-PA) (Urokinase Streptokinase)
Aktivator Plasminogen
Plasminogen Terikat Plasmin Terikat Fibrin FDP
Plasminogen Bebas Plasmin Bebas Fibrinogen V VIII Anti
Plasmin
-
Inhibitors of fibrinolysis
Plasminogen activator inhibitors (PAIs)
a2-antiplasmin (serpin)
-
PEMERIKSAAN LABORATORIUM HEMOSTASIS1. Rumple Leed (RL)2.
Bleeding time / masa perdarahan3. Clotting time / masa
penjendalan4. Jumlah trombosit5. Protrombin Time (PT) / Plasma
Protrombin Time (PPT)6. Activated Partial Tromboplastin Time
(APTT)7. Trombin Time
-
2. BLEEDING TIME/MASA PERDARAHANTujuan : menilai faktor
hemostasis yg letaknya ekstravaskulerMetoda : Ivy - voler lengan
bawah (T 40 mmHg) tusuk lancet sedalam 3 mm isap dg kertas saring
tiap 30 detik - N : 1 6 menit Duke - telinga - N : 1 3 menit
-
3. CLOTTTING TIME / MASA PENJENDALANTujuan : Mendeteksi kualitas
dan kuantitas faktor koagulasi scr keseluruhanNilai normal : 9 15
menit Gelas arloji : 2 6 menit
-
4. JUMLAH TROMBOSITTujuan : mengetahui kuantitas trombositCara :
Langsung Manual : Brecher Herweden Semi otomatik Otomatik Tak
langsung FonioNilai normal : 150.000 400.000 / mm3
-
5. PROTROMBIN TIME (PT) / PLASMA PROTROMBIN TIME (PPT)Tujuan :
Menguji faktor koagulasi jalur ekstrinsik (VII) & jalur bersama
(V, X) Memonitor terapi anti koagulan oralCara :Plasma + Ca 2+ +
tromboplastin jaringan terbentuk jendalan dideteksi dgn
fotodetektor (37 0C)Waktu yg diperlukan utk pembentukan jendalan
PTNilai normal : 11 -15 detik ( atau beda dgn kontrol 2 detik )
-
6. ACTIVATED PARTIAL TROMBOPLASTIN TIME (APTT)Tujuan : Menguji
faktor koagulasi jalur intrinsik (VIII, IX, XI, XII) & bersama
(V, X) Memonitor terapi heparinCara :Plasma + Ca 2+ + tromboplastin
jaringan terbentuk jendalan dideteksi dgn fotodetektor (37 0C)Waktu
yg diperlukan utk pembentukan jendalan APTT
Nilai normal : 20 - 40 detik
-
7. THROMBIN TIME (TT)Tujuan : menguji perubahan fibrinogen
menjadi fibrinCara : plasma + reagen trombin bekuan (370 C)Nilai
normal : 16 20 detik
-
Conditions Causing BleedingIncomplete hemostasis is most common
cause of bleeding.Vitamin K deficiency severe coagulation
defectRequired for synthesis of prothrombin and factors VII, IX and
XParenchymal diseases of the liverLiver synthesizes several
coagulation factors
-
Hereditary deficienciesHemophilia A--factor VIII
deficiencySex-linked recessive30% due to new mutations and dont
have family linkHemarthroses common (spontaneous bleeding in
joints)Infuse patient with factor VIII from human blood or
cryoprecipitate.Need 100% levels preop, keep at 30% postop.
Hemophilia B--factor IX deficiencyClinically indistinguishable
from Hemophilia ASex-linked recessiveNeed 50%
preoperativelyProlonged PTT, normal PTTX: Factor IX or FFP
-
Von Willebrands DiseaseVon Willebrands Disease- Most common
congenital bleeding disorder.Types I, II, and III.PT normal PTT
normal or elevatedProlonged bleeding timeType I most common (70%)
with mild sx.Type III causes most bleedingType I and III- reduced
quantity of vWFTX: Cryo, DDAVPType II- defect in vWF molecule,
enough of it but doesnt work well. TX: Cryo
-
Platelet DisordersAcquired-H2 blockers, heparin.Bernard-Soulier,
a Gp1b receptor deficiency (cant bind to each other)Uremia-Inhibits
Gp1b, vWF. TX: dialysis, DDAVP, cryo, plts.Ticlopidine- decreases
ADP in platelets, prevents exposure of Gp1b/IIIa
receptors.Dipyramidole- decreases ADP induced plt
aggregation.Plavix-ADP receptor antagonist.Pentoxifyllin- inhibits
plt aggregation
-
Platelet DisordersHeparin induced thrombocytopenia
(HIT)Antiplatelet antibodies results in platelet destruction.Also
causes aggregation and thrombosis.Low doses of heparin.LMWH may
have less risk.
DICDecreased plts, prolonged PT, PTT.Low fibrinogen, high fibrin
split products, high D-dimersOften initiated by tissue factor.Treat
underlying cause
-
ThrombiPlatelet aggregatesFibrinTrapped erythrocytes and
leucocytesNot part of this hemostatic processThis is a deep vein
thrombosisPostoperative patients confined to bed
-
Endothelial injury is dominant influenceHeart and arterial
circulationHypercholesteremia, cigarette smoke productsRadiation,
bacterial endotoxinsResults in exposure of subendothelial collagen,
adherence of platelets, release of tissue factor and local
depletion of prostacyclin (antithrombin)
-
Alterations in normal blood flowTurbulenceinjures
endotheliumAtherosclerotic plaquesStasis Can create venous
thrombiAneurysms cause local stasisDeformed cells of Sickle cell
anemia cause vascular occlusions
-
Stasis and TurbulenceDisrupt laminar flow (cells in middle)Bring
platelets into contact with endotheliumPrevent dilution of
activated clotting factors by fresh-flowing bloodRetard inflow of
clotting factor inhibitors
-
HypercoagulabilityLeiden Factor- 30% spontaneous venous
thrombosis.Most common congenital disorder.Resistance to Protein C,
defect on factor VTX: heparin, warfarin.Protein C, S deficiency-5%
venous thromboses. TX: heparin, warfarin.
- HypercoagulabilityAntithrombin III deficiency- 2-3% thrombosis.
Heparin doesnt work. Can develop after previous heparin
exposure.TX: ATIII concentrate, FFP(highest conc) followed by
heparin.Polycythemia- defect in platelet function, usually
thrombotic, but can bleed. Keep HCT
-
HypercoagulabilityLupus Anticoagulant- antiphospholipid
antibodies. Not all patients have SLE. A procoagulant (prolonged
PTT but hypercoagulable).Diagnose by seeing prolonged PTT, false
positive RPR test for syphilis.TX: heparin, warfarin.
-
HypercoagulabilityCardiopulmonary Bypass- factor XII activated,
results in hypercoagulable state. TX: heparin, warfarin.Warfarin
induced skin necrosis- Occurs when coumadin started before heparin.
Due to a decrease in protein S,C making patient transiently
hypercoagulable. Patients with Protien C deficiency highly
susceptible.
-
HypercoagulabilityMay be genetic or acquiredGenetic mutations in
the factor V geneMutant factor V is resistant to anticoagulant
effect of activated protein CSmoking, obesity and ageLate pregnancy
and postpartum amniotic fluid infusion into circulationDisseminated
cancers tumors release procoagulantsAdvanced age, bed rest and
immobilization
-
Hematologic DrugsWarfarin- prevents Vit K dependent
decarboxylation of glutamic residues on Vit K dependent
factors.Dextran- inhibits platelets and coagulation
factors.Sequential compression devices-improve venous return but
also induce fibrinolysis with compression (release of tPA).
-
Hematologic DrugsHeparin- activates antithrombin III.Reversed
with protamine (1-1.5 protamine per 100u of heparin).Half-life
60-90 min.Long term heparin use causes osteoporosis, alopecia. Does
not cross BBB.Protamine side-effects are hypotension, bradycardia,
decreased heart function.
- Hematologic DrugsHirudin- leeches, thrombin inhibitor.Ancrod-
Malayan pit viper venom, stimulates tPA
release.Amicar-antifibrinolytic, procoagulant, inhibits plasmin.
Used in DIC, persistent bleeding following CABG, thrombolytic
overdoses.Streptokinase, tPA-need to follow fibrinogen levels,
levels
-
Fate of thrombusPropagationAccumulate more platelets and fibrin
and obstruct a critical vesselEmbolizationDislodge thrombi and
transported to other sites in vasculature
-
Fate of thrombus, continuedDissolution/resolutionRemoved by
fibrinolytic activityOrganization Induce inflammation and fibrosis
and may reopen and allow blood flow
-
Fates continuedRecanalizationOpenings and even blood vessels
created in thrombus