Embed Size (px)
Citation preview

Neurosurg Focus / Volume 33 / August 2012
Neurosurg Focus 33 (2):E7, 2012
1
The posterior petrosal approach has met with con-siderable success in the management of complex neoplastic and cerebrovascular lesions.1–3,9,13,27,28,30,
31,33,34,36 At the mere expense of meticulous bone work to preserve the labyrinth and skeletonize the sigmoid sinus, this approach affords a wide exposure, minimizing opera-tive distance and brain retraction, and affording multiple working angles to the neurosurgical target and adjacent vascular anatomy.1–3,9,13 These advantages are only fully realized by the division of the tentorium and superior pe-trosal sinus and mobilization of a completely skeleton-ized sigmoid sinus. This contrasts with early work in the otolaryngology literature in which the exposure was lim-ited superiorly by the tentorium and posteriorly by the sigmoid sinus.12,18,19 To add exposure, some have divided the sigmoid sinus;8,11,17,19,32 however, with meticulous skeletonization and mobilization of the sinus as in the petrosal approach, this potentially dangerous maneuver can be avoided.3,28 In addition, retraction of the dural ve-nous sinuses and temporal lobe is performed in one unit, in contrast to nonpetrosal approaches (such as the com-bined retrosigmoid-subtemporal approach) that place added traction on the vein of Labbé with retraction.3,28 In this article, we review the history of the posterior petrosal approach, from its predecessors in the early otolaryngol-ogy literature through its evolution as a combined supra-
and infratentorial exposure with modern extensions and modifications.
Early WorkEarly petrous bone work dates back to 1904, when a
translabyrinthine approach in combination with a suboc-cipital craniectomy was performed to expose an acoustic nerve neoplasm.10 Unfortunately, due to excessive blood loss and infection risks this approach was largely aban-doned over the ensuing decades, until it was revived in the otolaryngology literature in the 1960s.12,19 Over the ensuing 2 decades, the literature clearly recognized 3 variants of the petrosectomy—a lateral petrosectomy that spared the labyrinth entirely (retrolabyrinthine),12,18 a translabyrinthine approach,12,19 and a complete petrosec-tomy or transcochlear approach.21 The latter, described by House and Hitselberger in 1976, entailed transposition of the facial nerve with the petrosectomy. This was soon modified by Jenkins and Fisch22 in 1980, who kept the nerve skeletonized in its bony canal without transposi-tion to potentially mitigate the risk of postoperative facial nerve palsy (transotic approach). These approaches are summarized in Table 1.
Early additions to the standard translabyrinthine ap-
Evolution of the posterior petrosal approach
Bradley a. Gross, M.d., daryoush Tavanaiepour, M.d., rose du, M.d., ph.d., ossaMa al-MefTy, M.d., and ian f. dunn, M.d.Department of Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts
In this article, the authors review the history of the posterior petrosal approach. The early foundation of the ret-rolabyrinthine lateral petrosectomy has its roots in the otolaryngology literature. These early approaches were limited in exposure by the tentorium superiorly and the sigmoid sinus posteriorly. Although the concept of a transtentorial approach was originally combined with a complete labyrinthectomy, Hakuba and colleagues described the expansive exposure afforded by sectioning the tentorium and superior petrosal sinus and mobilizing a skeletonized sigmoid sinus. This maneuver serves as the key step in allowing for the full, combined supra- and infratentorial exposure that the posterior petrosal approach provides. In contrast to Hakuba et al.’s approach, which used a partial labyrinthec-tomy, modern approaches often preserve the entire labyrinth (retrolabyrinthine approach). For added exposure, the latter can be combined with the anterior petrosal approach, allowing for the preservation of hearing and an enhanced view of the surgical target. The authors review the evolution of the petrosal approach and highlight its applicability.(http://thejns.org/doi/abs/10.3171/2012.6.FOCUS12133)
Key Words • transpetrosal approach • retrolabyrinthine approach • presigmoid approach • petrosal approach • combined approach • skull base
1
B. A. Gross et al.
2 Neurosurg Focus / Volume 33 / August 2012
proach included its combination with a suboccipital cra-niectomy10,17 and, importantly, opening of the tentorium, as described by King26 in 1970. The latter was a key step in the evolution of the modern petrosal approach, provid-ing an expanded, combined supra- and infratentorial ex-posure.
Evolution to the Modern Posterior Petrosal Approach
In 1977, Hakuba et al.16 expanded on the concept of a combined supra- and infratentorial exposure, describ-ing 1 case in a patient with a clival meningioma that was approached via a combined supra- and infratentorial pe-trosal approach with partial labyrinthectomy. The patient these authors described did well postoperatively without hearing loss. Crucial maneuvers in the description includ-ed the meticulous complete skeletonization and mobiliza-tion of the sigmoid sinus after division of the tentorium and superior petrosal sinus; these steps serve as the key foundation of the modern posterior petrosal approach. Hakuba’s description essentially served as a predecessor to the modern transcrusal (partial labyrinthectomy) ap-proach;6,20,35 although hearing is not obligately sacrificed as in the complete labyrinthectomy, hearing loss is seen in up to 42% of cases.6 In contrast, Al-Mefty et al.’s1 poste-rior petrosal approach entails skeletonization of the semi-circular canals without sacrifice of the labyrinth. This presigmoid, retrolabyrinthine approach has served as the backbone in the approach to innumerable neoplastic and vascular lesions over the past 3 decades.1–3,9,27,28,30,31,33,34,36
The Posterior Petrosal ApproachThe posterior petrosal approach is performed with
the patient positioned supine, with the head turned 40°–60° after placing a roll under the ipsilateral shoulder. The head is extended to ensure that the petrous bone is the highest point in the field. After fixation in a Mayfield head holder, monitoring leads are placed for somatosen-sory evoked potentials, brainstem auditory evoked poten-tials, and select cranial nerves.
An incision is fashioned from the zygoma just ante-
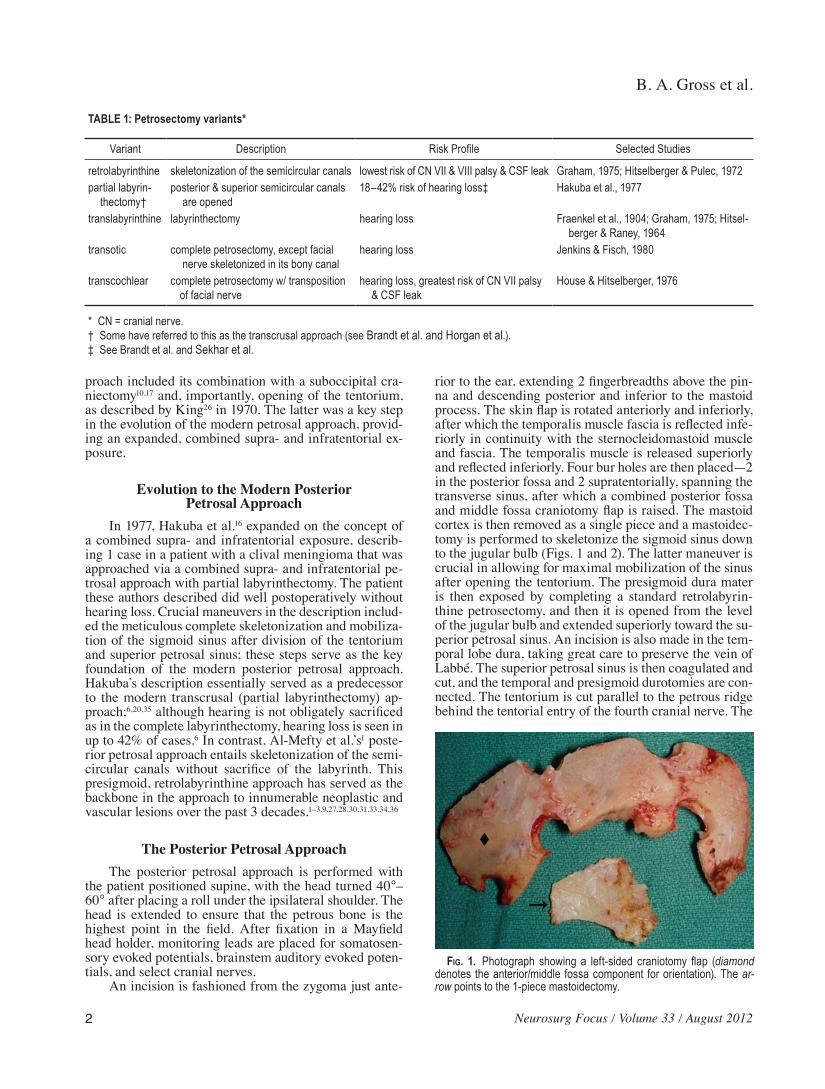
rior to the ear, extending 2 fingerbreadths above the pin-na and descending posterior and inferior to the mastoid process. The skin flap is rotated anteriorly and inferiorly, after which the temporalis muscle fascia is reflected infe-riorly in continuity with the sternocleidomastoid muscle and fascia. The temporalis muscle is released superiorly and reflected inferiorly. Four bur holes are then placed—2 in the posterior fossa and 2 supratentorially, spanning the transverse sinus, after which a combined posterior fossa and middle fossa craniotomy flap is raised. The mastoid cortex is then removed as a single piece and a mastoidec-tomy is performed to skeletonize the sigmoid sinus down to the jugular bulb (Figs. 1 and 2). The latter maneuver is crucial in allowing for maximal mobilization of the sinus after opening the tentorium. The presigmoid dura mater is then exposed by completing a standard retrolabyrin-thine petrosectomy, and then it is opened from the level of the jugular bulb and extended superiorly toward the su-perior petrosal sinus. An incision is also made in the tem-poral lobe dura, taking great care to preserve the vein of Labbé. The superior petrosal sinus is then coagulated and cut, and the temporal and presigmoid durotomies are con-nected. The tentorium is cut parallel to the petrous ridge behind the tentorial entry of the fourth cranial nerve. The
TABLE 1: Petrosectomy variants*
Variant Description Risk Profile Selected Studies
retrolabyrinthine skeletonization of the semicircular canals lowest risk of CN VII & VIII palsy & CSF leak Graham, 1975; Hitselberger & Pulec, 1972partial labyrin- thectomy†
posterior & superior semicircular canals are opened
18–42% risk of hearing loss‡ Hakuba et al., 1977
translabyrinthine labyrinthectomy hearing loss Fraenkel et al., 1904; Graham, 1975; Hitsel- berger & Raney, 1964
transotic complete petrosectomy, except facial nerve skeletonized in its bony canal
hearing loss Jenkins & Fisch, 1980
transcochlear complete petrosectomy w/ transposition of facial nerve
hearing loss, greatest risk of CN VII palsy & CSF leak
House & Hitselberger, 1976
* CN = cranial nerve.† Some have referred to this as the transcrusal approach (see Brandt et al. and Horgan et al.). ‡ See Brandt et al. and Sekhar et al.
Fig. 1. Photograph showing a left-sided craniotomy flap (diamond denotes the anterior/middle fossa component for orientation). The ar-row points to the 1-piece mastoidectomy.
Neurosurg Focus / Volume 33 / August 2012
Posterior petrosal approach
3
sigmoid sinus is then reflected posteriorly and the tempo-ral lobe gently retracted with the tentorium.3,9,28
The senior author has used the standard posterior pe-trosal approach in more than 160 cases spanning a period of 3 decades. Although most often used for meningiomas, this approach has been applied to numerous schwanno-mas, epidermoid lesions, chordomas, craniopharyngio-mas, paragangliomas, aneurysms, and brainstem cavern-ous malformations. Crucial technological elements of this technique include the adjunctive use of neuromoni-toring, neuronavigation, and the application of advances in neuroanesthesia.
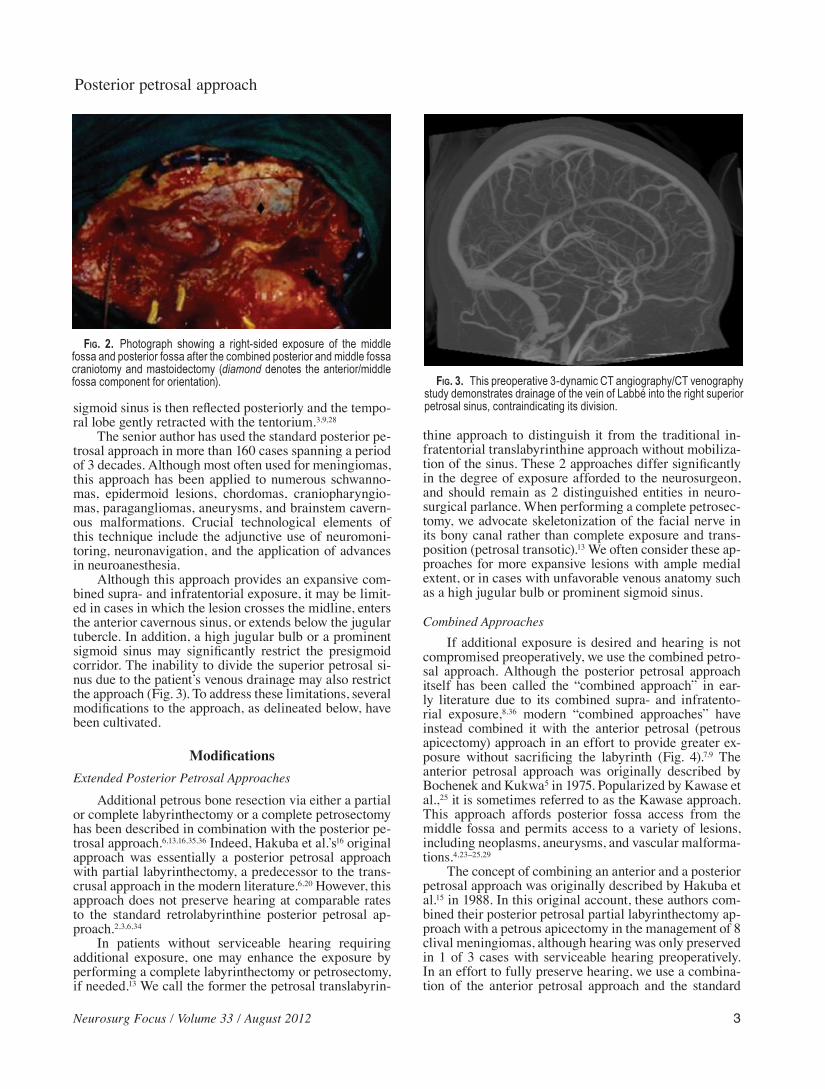
Although this approach provides an expansive com-bined supra- and infratentorial exposure, it may be limit-ed in cases in which the lesion crosses the midline, enters the anterior cavernous sinus, or extends below the jugular tubercle. In addition, a high jugular bulb or a prominent sigmoid sinus may significantly restrict the presigmoid corridor. The inability to divide the superior petrosal si-nus due to the patient’s venous drainage may also restrict the approach (Fig. 3). To address these limitations, several modifications to the approach, as delineated below, have been cultivated.
ModificationsExtended Posterior Petrosal Approaches
Additional petrous bone resection via either a partial or complete labyrinthectomy or a complete petrosectomy has been described in combination with the posterior pe-trosal approach.6,13,16,35,36 Indeed, Hakuba et al.’s16 original approach was essentially a posterior petrosal approach with partial labyrinthectomy, a predecessor to the trans-crusal approach in the modern literature.6,20 However, this approach does not preserve hearing at comparable rates to the standard retrolabyrinthine posterior petrosal ap-proach.2,3,6,34
In patients without serviceable hearing requiring additional exposure, one may enhance the exposure by performing a complete labyrinthectomy or petrosectomy, if needed.13 We call the former the petrosal translabyrin-
thine approach to distinguish it from the traditional in-fratentorial translabyrinthine approach without mobiliza-tion of the sinus. These 2 approaches differ significantly in the degree of exposure afforded to the neurosurgeon, and should remain as 2 distinguished entities in neuro-surgical parlance. When performing a complete petrosec-tomy, we advocate skeletonization of the facial nerve in its bony canal rather than complete exposure and trans-position (petrosal transotic).13 We often consider these ap-proaches for more expansive lesions with ample medial extent, or in cases with unfavorable venous anatomy such as a high jugular bulb or prominent sigmoid sinus.
Combined ApproachesIf additional exposure is desired and hearing is not
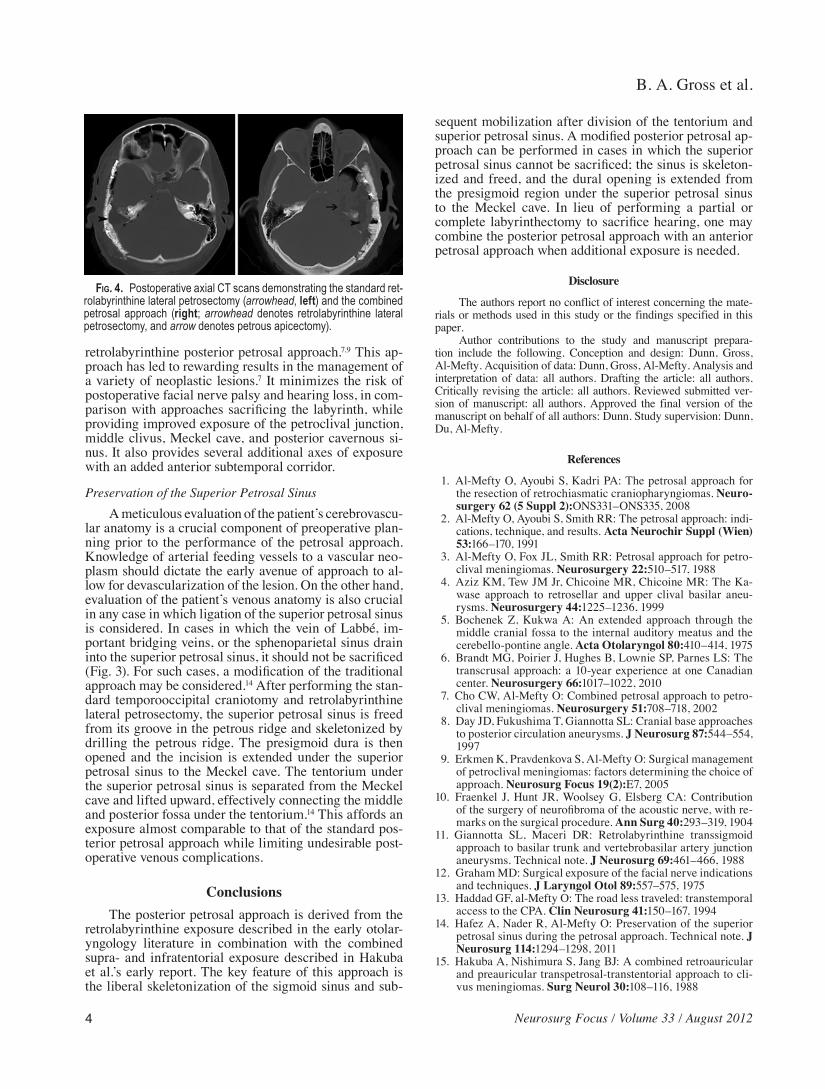
compromised preoperatively, we use the combined petro-sal approach. Although the posterior petrosal approach itself has been called the “combined approach” in ear-ly literature due to its combined supra- and infratento-rial exposure,8,36 modern “combined approaches” have instead combined it with the anterior petrosal (petrous apicectomy) approach in an effort to provide greater ex-posure without sacrificing the labyrinth (Fig. 4).7,9 The anterior petrosal approach was originally described by Bochenek and Kukwa5 in 1975. Popularized by Kawase et al.,25 it is sometimes referred to as the Kawase approach. This approach affords posterior fossa access from the middle fossa and permits access to a variety of lesions, including neoplasms, aneurysms, and vascular malforma-tions.4,23–25,29
The concept of combining an anterior and a posterior petrosal approach was originally described by Hakuba et al.15 in 1988. In this original account, these authors com-bined their posterior petrosal partial labyrinthectomy ap-proach with a petrous apicectomy in the management of 8 clival meningiomas, although hearing was only preserved in 1 of 3 cases with serviceable hearing preoperatively. In an effort to fully preserve hearing, we use a combina-tion of the anterior petrosal approach and the standard
Fig. 2. Photograph showing a right-sided exposure of the middle fossa and posterior fossa after the combined posterior and middle fossa craniotomy and mastoidectomy (diamond denotes the anterior/middle fossa component for orientation). Fig. 3. This preoperative 3-dynamic CT angiography/CT venography
study demonstrates drainage of the vein of Labbé into the right superior petrosal sinus, contraindicating its division.
B. A. Gross et al.
4 Neurosurg Focus / Volume 33 / August 2012
retrolabyrinthine posterior petrosal approach.7,9 This ap-proach has led to rewarding results in the management of a variety of neoplastic lesions.7 It minimizes the risk of postoperative facial nerve palsy and hearing loss, in com-parison with approaches sacrificing the labyrinth, while providing improved exposure of the petroclival junction, middle clivus, Meckel cave, and posterior cavernous si-nus. It also provides several additional axes of exposure with an added anterior subtemporal corridor.
Preservation of the Superior Petrosal SinusA meticulous evaluation of the patient’s cerebrovascu-
lar anatomy is a crucial component of preoperative plan-ning prior to the performance of the petrosal approach. Knowledge of arterial feeding vessels to a vascular neo-plasm should dictate the early avenue of approach to al-low for devascularization of the lesion. On the other hand, evaluation of the patient’s venous anatomy is also crucial in any case in which ligation of the superior petrosal sinus is considered. In cases in which the vein of Labbé, im-portant bridging veins, or the sphenoparietal sinus drain into the superior petrosal sinus, it should not be sacrificed (Fig. 3). For such cases, a modification of the traditional approach may be considered.14 After performing the stan-dard temporooccipital craniotomy and retrolabyrinthine lateral petrosectomy, the superior petrosal sinus is freed from its groove in the petrous ridge and skeletonized by drilling the petrous ridge. The presigmoid dura is then opened and the incision is extended under the superior petrosal sinus to the Meckel cave. The tentorium under the superior petrosal sinus is separated from the Meckel cave and lifted upward, effectively connecting the middle and posterior fossa under the tentorium.14 This affords an exposure almost comparable to that of the standard pos-terior petrosal approach while limiting undesirable post-operative venous complications.
ConclusionsThe posterior petrosal approach is derived from the
retrolabyrinthine exposure described in the early otolar-yngology literature in combination with the combined supra- and infratentorial exposure described in Hakuba et al.’s early report. The key feature of this approach is the liberal skeletonization of the sigmoid sinus and sub-
sequent mobilization after division of the tentorium and superior petrosal sinus. A modified posterior petrosal ap-proach can be performed in cases in which the superior petrosal sinus cannot be sacrificed; the sinus is skeleton-ized and freed, and the dural opening is extended from the presigmoid region under the superior petrosal sinus to the Meckel cave. In lieu of performing a partial or complete labyrinthectomy to sacrifice hearing, one may combine the posterior petrosal approach with an anterior petrosal approach when additional exposure is needed.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript prepara-tion include the following. Conception and design: Dunn, Gross, Al-Mefty. Acquisition of data: Dunn, Gross, Al-Mefty. Analysis and interpretation of data: all authors. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted ver-sion of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Dunn. Study supervision: Dunn, Du, Al-Mefty.
References
1. Al-Mefty O, Ayoubi S, Kadri PA: The petrosal approach for the resection of retrochiasmatic craniopharyngiomas. Neuro-surgery 62 (5 Suppl 2):ONS331–ONS335, 2008
2. Al-Mefty O, Ayoubi S, Smith RR: The petrosal approach: indi-cations, technique, and results. Acta Neurochir Suppl (Wien) 53:166–170, 1991
3. Al-Mefty O, Fox JL, Smith RR: Petrosal approach for petro-clival meningiomas. Neurosurgery 22:510–517, 1988
4. Aziz KM, Tew JM Jr, Chicoine MR, Chicoine MR: The Ka-wase approach to retrosellar and upper clival basilar aneu-rysms. Neurosurgery 44:1225–1236, 1999
5. Bochenek Z, Kukwa A: An extended approach through the middle cranial fossa to the internal auditory meatus and the cerebello-pontine angle. Acta Otolaryngol 80:410–414, 1975
6. Brandt MG, Poirier J, Hughes B, Lownie SP, Parnes LS: The transcrusal approach: a 10-year experience at one Canadian center. Neurosurgery 66:1017–1022, 2010
7. Cho CW, Al-Mefty O: Combined petrosal approach to petro-clival meningiomas. Neurosurgery 51:708–718, 2002
8. Day JD, Fukushima T, Giannotta SL: Cranial base approaches to posterior circulation aneurysms. J Neurosurg 87:544–554, 1997
9. Erkmen K, Pravdenkova S, Al-Mefty O: Surgical management of petroclival meningiomas: factors determining the choice of approach. Neurosurg Focus 19(2):E7, 2005
10. Fraenkel J, Hunt JR, Woolsey G, Elsberg CA: Contribution of the surgery of neurofibroma of the acoustic nerve, with re-marks on the surgical procedure. Ann Surg 40:293–319, 1904
11. Giannotta SL, Maceri DR: Retrolabyrinthine transsigmoid approach to basilar trunk and vertebrobasilar artery junction aneurysms. Technical note. J Neurosurg 69:461–466, 1988
12. Graham MD: Surgical exposure of the facial nerve indications and techniques. J Laryngol Otol 89:557–575, 1975
13. Haddad GF, al-Mefty O: The road less traveled: transtemporal access to the CPA. Clin Neurosurg 41:150–167, 1994
14. Hafez A, Nader R, Al-Mefty O: Preservation of the superior petrosal sinus during the petrosal approach. Technical note. J Neurosurg 114:1294–1298, 2011
15. Hakuba A, Nishimura S, Jang BJ: A combined retroauricular and preauricular transpetrosal-transtentorial approach to cli-vus meningiomas. Surg Neurol 30:108–116, 1988
Fig. 4. Postoperative axial CT scans demonstrating the standard ret-rolabyrinthine lateral petrosectomy (arrowhead, left) and the combined petrosal approach (right; arrowhead denotes retrolabyrinthine lateral petrosectomy, and arrow denotes petrous apicectomy).

Neurosurg Focus / Volume 33 / August 2012
Posterior petrosal approach
5
16. Hakuba A, Nishimura S, Tanaka K, Kishi H, Nakamura T: Clivus meningioma: six cases of total removal. Neurol Med Chir (Tokyo) 17:63–77, 1977
17. Hitselberger WE, House WF: A combined approach to the cer-ebellopontine angle. A suboccipital-petrosal approach. Arch Otolaryngol 84:267–285, 1966
18. Hitselberger WE, Pulec JL: Trigeminal nerve (posterior root) retrolabyrinthine selective section. Operative procedure for intractable pain. Arch Otolaryngol 96:412–415, 1972
19. Hitselberger WE, Raney AA: Transtemporal bone microsur-gical removal of acoustic neuromas. Neurosurgical thoughts comparing suboccipital and translabyrinthine approaches. Arch Otolaryngol 80:754–756, 1964
20. Horgan MA, Anderson GJ, Kellogg JX, Schwartz MS, Spektor S, McMenomey SO, et al: Classification and quantification of the petrosal approach to the petroclival region. J Neurosurg 93:108–112, 2000
21. House WF, Hitselberger WE: The transcochlear approach to the skull base. Arch Otolaryngol 102:334–342, 1976
22. Jenkins HA, Fisch U: The transotic approach to resection of difficult acoustic tumors of the cerebellopontine angle. Am J Otol 2:70–76, 1980
23. Kawase T, Bertalanffy H, Otani M, Shiobara R, Toya S: Surgi-cal approaches for vertebro-basilar trunk aneurysms located in the midline. Acta Neurochir (Wien) 138:402–410, 1996
24. Kawase T, Shiobara R, Toya S: Anterior transpetrosal-trans-tentorial approach for sphenopetroclival meningiomas: surgi-cal method and results in 10 patients. Neurosurgery 28:869–876, 1991
25. Kawase T, Toya S, Shiobara R, Mine T: Transpetrosal ap-proach for aneurysms of the lower basilar artery. J Neurosurg 63:857–861, 1985
26. King TT: Combined translabyrinthine-transtentorial approach to acoustic nerve tumours. Proc R Soc Med 63:780–782, 1970
27. King WA, Black KL, Martin NA, Canalis RF, Becker DP: The petrosal approach with hearing preservation. J Neurosurg 79: 508–514, 1993
28. Klimo P Jr, Browd SR, Pravdenkova S, Couldwell WT, Walker ML, Al-Mefty O: The posterior petrosal approach: technique
and applications in pediatric neurosurgery. Clinical article. J Neurosurg Pediatr 4:353–362, 2009
29. MacDonald JD, Antonelli P, Day AL: The anterior subtemporal, medial transpetrosal approach to the upper basilar artery and ponto-mesencephalic junction. Neurosurgery 43:84–89, 1998
30. Nanda A, Javalkar V, Banerjee AD: Petroclival meningiomas: study on outcomes, complications and recurrence rates. Clini-cal article. J Neurosurg 114:1268–1277, 2011
31. Origitano TC, Anderson DE, Tarassoli Y, Reichman OH, al-Mefty O: Skull base approaches to complex cerebral aneu-rysms. Surg Neurol 40:339–346, 1993
32. Rosenberg SI, Flamm ES, Hoffer ME, Schwartz DM: The retrolabyrinthine transsigmoid approach to midbasilar artery aneurysms. Laryngoscope 102:100–104, 1992
33. Samii M, Ammirati M, Mahran A, Bini W, Sepehrnia A: Sur-gery of petroclival meningiomas: report of 24 cases. Neuro-surgery 24:12–17, 1989
34. Seifert V, Raabe A, Zimmermann M: Conservative (laby-rinth-preserving) transpetrosal approach to the clivus and petroclival region—indications, complications, results and lessons learned. Acta Neurochir (Wien) 145:631–642, 2003
35. Sekhar LN, Schessel DA, Bucur SD, Raso JL, Wright DC: Partial labyrinthectomy petrous apicectomy approach to neo-plastic and vascular lesions of the petroclival area. Neurosur-gery 44:537–552, 1999
36. Spetzler RF, Daspit CP, Pappas CTE: The combined supra- and infratentorial approach for lesions of the petrous and clival regions: experience with 46 cases. J Neurosurg 76:588–599, 1992
Manuscript submitted April 15, 2012.Accepted June 27, 2012.Please include this information when citing this paper: DOI:
10.3171/2012.6.FOCUS12133.Address correspondence to: Ian F. Dunn, M.D., Department of
Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School, 75 Francis Street, Boston, Massachusetts 02115. email: [email protected].