Embed Size (px)
Citation preview

Evidence For A Novel Bone-Kidney Axis Regulating Systemic Phosphate Homeostasis
L. Darryl Quarles, M.D.
Summerfield Endowed Professor of Nephrology
University Of Kansas Medical Center
Learning Objectives
• Examine the role of hyperphosphatemia in vascular calcifications and mortality
• Discuss the functions of: – Phex– FGF23– Klotho
• Propose a model showing how these factors may participate in a novel bone-kidney axis regulating systemic phosphate homeostasis and mineralization.
• Examine the role of FGF23 in the pathogenesis of disordered mineral homeostasis in CKD.
Novel Genes Regulating Phosphate Homeostasis}
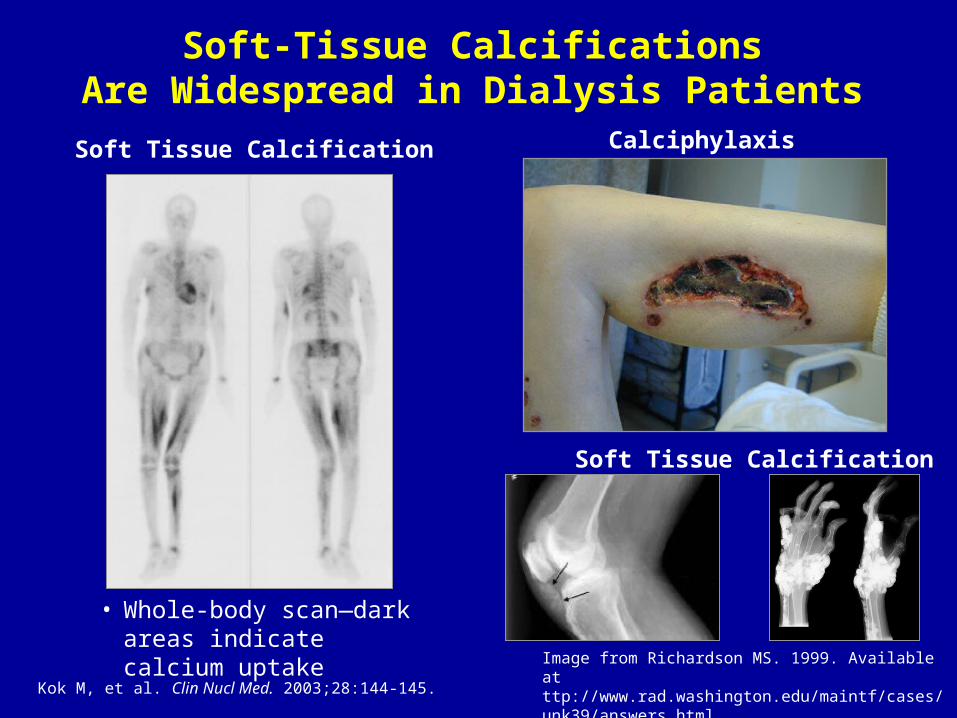
Soft-Tissue CalcificationsAre Widespread in Dialysis Patients
Calciphylaxis
Image from Richardson MS. 1999. Available at ttp://www.rad.washington.edu/maintf/cases/unk39/answers.html..Image from Block GA. 2004.
Soft Tissue Calcification
• Whole-body scan—dark areas indicate calcium uptake
Kok M, et al. Clin Nucl Med. 2003;28:144-145.
Soft Tissue Calcification

Coronary-Artery Calcification Is Prevalent in ESRD
A
B
Goodman WG et al N Engl J Med.342:1478-83, 2000.

London, G. M. et al. Nephrol. Dial. Transplant. 2003 18:1731-1740
Arterial Calcification Status Increases All-Cause (A) and Cardiovascular Mortality (B) in ESRD Patients
Uncertain Pathogenesis of Vascular Calcification in CKD
• Risk factors include:70% of increased CV risk accounted for by traditional factors
– Age
– Hypertension– Diabetes mellitus– Inflamation-C-reactive protein
CKD-related Factors– Time on dialysis– Hyperphosphataemia– Calcium intake– Treatment with Vitamin D?

Disturbances in Mineral Metabolism Are Associated With Increased Risk of Mortality in Hemodialysis
Adapted from Block GA, et al. J Am Soc Nephrol. 2004;15:2208-2218.
< 3.0
Serum Phosphorus (mg/dL)
Referent group
Serum Phosphorus
3.0–4.04.0–5.0
5.0–6.06.0–7.0
7.0–8.08.0–9.0 > 9.0
0.00.6
1.2
1.4
1.6
1.8
2.0
2.2
1.0
Rel
ativ
e R
isk
of D
eath
(n=4
0,53
8)
0.00.6
0.8
1.0
1.2
1.4
1.6
1.8
< 8.0
Corrected Serum Calcium (mg/dL)
Referent group
Serum Calcium
8.0–8.58.5–9.0
9.0–9.5
9.5–10.0
10.0–10.5
10.5–11.0> 11.0
Rel
ativ
e R
isk
of D
eath
(n=4
0,53
8)

Inorganic Phosphate But Not Calcium Concentration Affects Mineralization
[Ca]
von Kossa
[Ca]
[Pi]
Alizarin red
[Pi]
Murshed M, et al Unique coexpression in osteoblasts of broadly expressed genes accounts for the spatial restriction of ECM mineralization to bone. Genes Dev. 19:1093-104, 2005.

Murshed M, et al Unique coexpression in osteoblasts of broadly expressed genes accounts for the spatial restriction of ECM mineralization to bone. Genes Dev. 19:1093-104, 2005.
Genetic Rescue of the Mgp -/- Phenotype

• Consensus regarding role of hyperphosphatemia, but lack of prospective studies demonstrating that interventions to lower serum phosphate improves survival.
• Understanding of the hormonal cascades regulating phosphate homeostasis may provide insights into additional pathways affecting the systemic complications of hyperphosphatemia.
Vascular Calcification & Morbidity/Mortality in CKD
Regulation of Phosphorus Homeostasis
Is there a hormonal cascade regulating serum phosphorus concentrations independent of PTH?

PTH-Independent Hypophosphatemic Disorders
• Tumor-Induced Osteomalacia (TIO).• Autosomal Dominant Hypo-phosphatemic
Rickets (ADHR).• McCune-Albright/Bone Fibrous Dysplasia. • X-Linked Hypophosphatemic Rickets
(XLH).• Linear Nevus Sebaceous Syndrome.

X-Linked Hypophosphatemic Rickets (XLH):Clinical Features
• Most common inherited form of rickets.• X-linked dominant disorder. • Phenotype:
– Renal• Decreased renal tubular reabsorption of phosphate.
• Aberrant regulation of 1,25 (OH)2 Vitamin D3 production.
– Skeletal• Defective calcification of cartilage (rickets) and bone
(osteomalacia).• Growth retardation.

XLH:Genetic Abnormality
• PHEX gene (PHosphate regulating gene homologous to Endopeptidases on X Chr).
• Disease gene encodes a member of M13 family of Type II transmembrane zinc metallo-endopeptidase.
• Mutations have been identified in 86% of familial and 57% of sporadic cases of XLH.
• Phex substrates are likely responsible for renal and skeletal phenotypes in XLH.
• Phex could convert a prohormone to a phosphate- conserving factor, or inactivate a phosphaturic hormone and/or mineralization inhibitor (most likely).

Phex Function: Lesions from the Hyp mouse homologue of XLH
• Expresses the major phenotypic features of XLH. • Mouse Phex cDNA sequence is highly homologous to that
of humans.• Hyp has a 3' Phex deletion creating a truncated
endopeptidase lacking the catalytic domain.• Systemic/humoral phosphaturic factor (“Phosphatonin”)
identified by parabiosis and cross-transplant studies.• Autocrine/paracrine nascent defect in Hyp-derived
osteoblasts leading to impaired mineralization independent of hypophosphatemia, caused by inhibitor of mineralization (“Minhibin”).
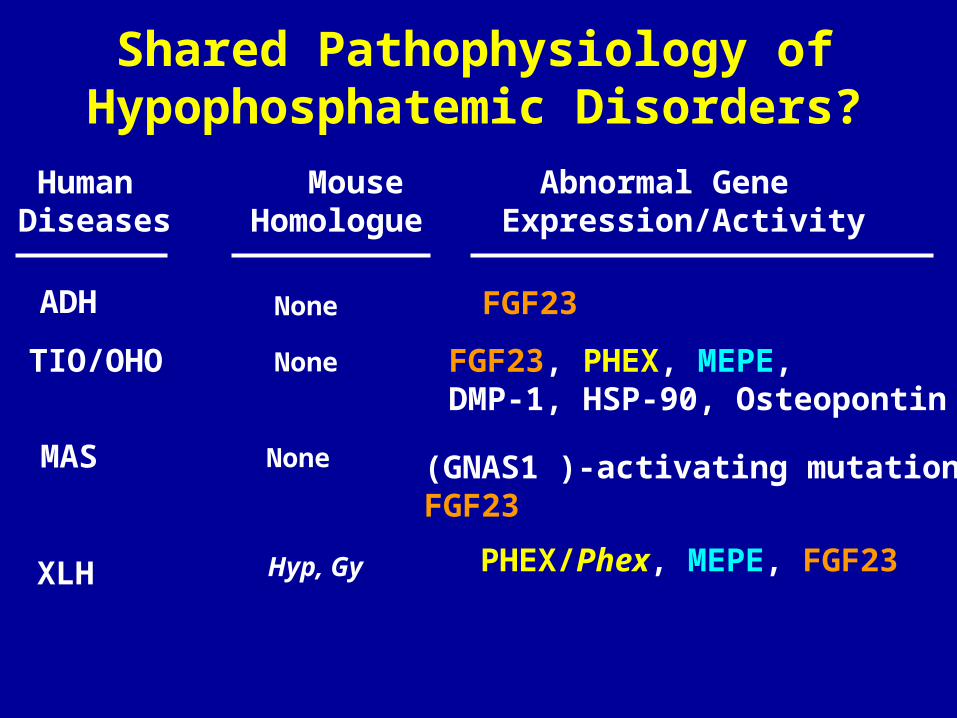
Shared Pathophysiology of Hypophosphatemic Disorders?
HumanDiseases
Mouse Homologue
Abnormal Gene Expression/Activity
ADH
TIO/OHO
XLH
None
None
Hyp, Gy
FGF23
FGF23, PHEX, MEPE,DMP-1, HSP-90, Osteopontin
PHEX/Phex, MEPE, FGF23
MAS None (GNAS1 )-activating mutations,FGF23

FGF23: A Candidate for Phosphatonin? • FGF23 is a ~32 kDa (251 amino
acids) protein with an N-terminal region containing the FGF homology domain and a novel 71 aa C-terminus that has phosphaturic activity in vivo.
• FGF23 is overproduced by tumors causing tumor-induced osteomalacia (TIO).
• Autosomal dominant hypophosphatemic rickets (ADHR) is caused by missense mutations of the 176-RXXR-179 motif in FGF-23 preventing its processing into inactive N- and C-terminal fragments.
• FGF23 is proposed to be a substrate for PHEX
Phex-Dependent Cleavage And Inactivation Of The Phosphaturic Hormone FGF23 Hypothesis

Is FGF23 Phosphatonin?
• To determine whether FGF23 is involved in the pathogenesis of XLH we:– Examined FGF23 levels in XLH and Hyp.– Confirmed that FGF23 has phosphaturic activity.– Determined whether FGF23 deficiency rescues
the hypophosphatemia in Hyp mice.– Assessed if FGF23 is a substrate for Phex.

Serum Phosphorus (A), Serum FGF23 (B) And Their Correlation (C) In Subjects With XLH
Weber T. Liu S, Quarles LD J Bone Mineral Res. 2003.

Increased Circulating fgf23 Levels in Hyp

Administration of FGF23 to Mice Induces Hypophosphatemia

Is FGF23 The Phosphaturic Factor In XLH/Hyp?
• To determined if FGF23 deficiency rescues the hypophosphatemia in Hyp mice, we:– Generated FGF23 null mice,– Transferred FGF23 deficiency onto the
Hyp mouse background to determine if superimposed FGF23 deficiency rescued the hypophosphatemia in Hyp mice.

Exon1 Exon3Exon2H
5’ Flanking
Fgf23 Gene
TK Neo
Short armEGFP
Long arm
Exon3Exon2H H
Targeted Allele
EGFP
Neo Exon3Exon2H H
5’ Flanking
N
SS
S S H
Targeting Strategy Used To Disrupt Fgf23 And Genotyping of Fgf23 Deficient Mice
TargetingConstruct
M
Neo (640bp)
Fgf23 (266 bp)
-/-+/-+/+ H2O
A
B
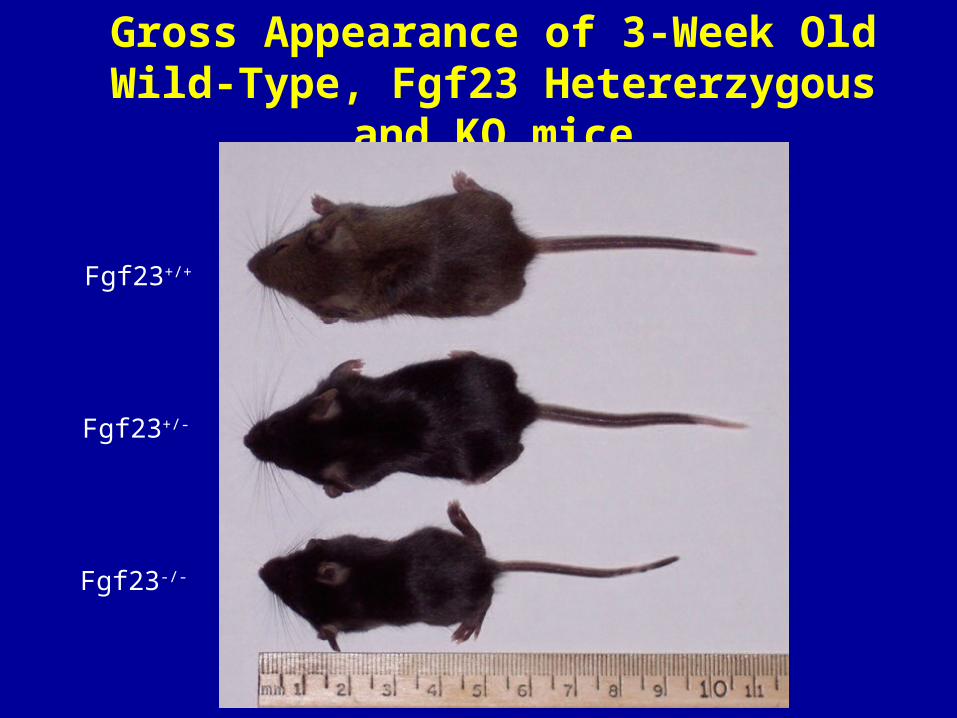
Fgf23+/+
Fgf23-/-
Gross Appearance of 3-Week Old Wild-Type, Fgf23 Hetererzygous and KO mice
Fgf23+/-

Genotypes
WT Het KO
Se
rum
1,2
5(O
H) 2
D3 C
on
ce
ntr
ati
on
s (
pM
)
0
200
400
600
800
1000
aa,b
b
B
WT Het KO
Se
rum
Ph
os
ph
oru
s C
on
ce
ntr
ati
on
(m
g/d
L)
0
2
4
6
8
10
12
14
16
18
a
b
c
Serum Pi, 1,25(OH)2D3 and Fgf23 levels in Wild-Type, Heterozygous and Homozygous
Fgf23-Deficient Mice
Genotypes
A
Se
rum
Fg
f23
Co
nc
en
tra
tio
ns
(p
g/m
l)
0
10
20
30
40
50
WT Het KO
Genotypes
C

Breeding Strategy/Study Design
Serum Phosphate, Calcium, fgf23, 1,25(OH)2D3, MicroCT
3 weeks
Fgf23+/+ Fgf23-/-
Fgf23-KO
Fgf23+/+/Hyp
Hyp
Fgf23-/-/Hyp
Fgf23-KO/HypWild-type
Fgf23+/-/XY (Heterozygous fgf23-KO males)
Fgf23+/-/HypX (Heterozygous fgf23-KO /Hyp females)
X

Serum Pi levels in Wild-Type, Fgf23-, Phex-, and combined Fgf23/Phex-Deficient Mice
WT Het KO Hyp Het/Hyp KO/Hyp
Ser
um
Ph
osp
ho
rus
Co
nce
ntr
atio
n (
mg
/dL
)
0
2
4
6
8
10
12
14
16
18
Genotypes
a
b
c c
dd
n > 5

Serum 1,25(OH)2D3 Levels in Wild-Type, Fgf23-, Phex-, and combined Fgf23/Phex-KO Mice
WT Het KO Hyp Het/Hyp KO/HypSer
um
1,2
5 (O
H)2
D3
Co
nce
ntr
atio
ns
(pM
)
0
200
400
600
800
1000
aa,b
b b
cc
Genotypes
n=4

Genotypes
WT Het KO Hyp Het/Hyp KO/Hyp
Ser
um
Fg
f23
Lev
els
(pg
/ml)
0
500
1000
1500
2000
2500
a a
b
c
n > 5
Serum Fgf23 levels in Wild-Type, Fgf23-, Phex-, and combined Fgf23/Phex-Deficient Mice
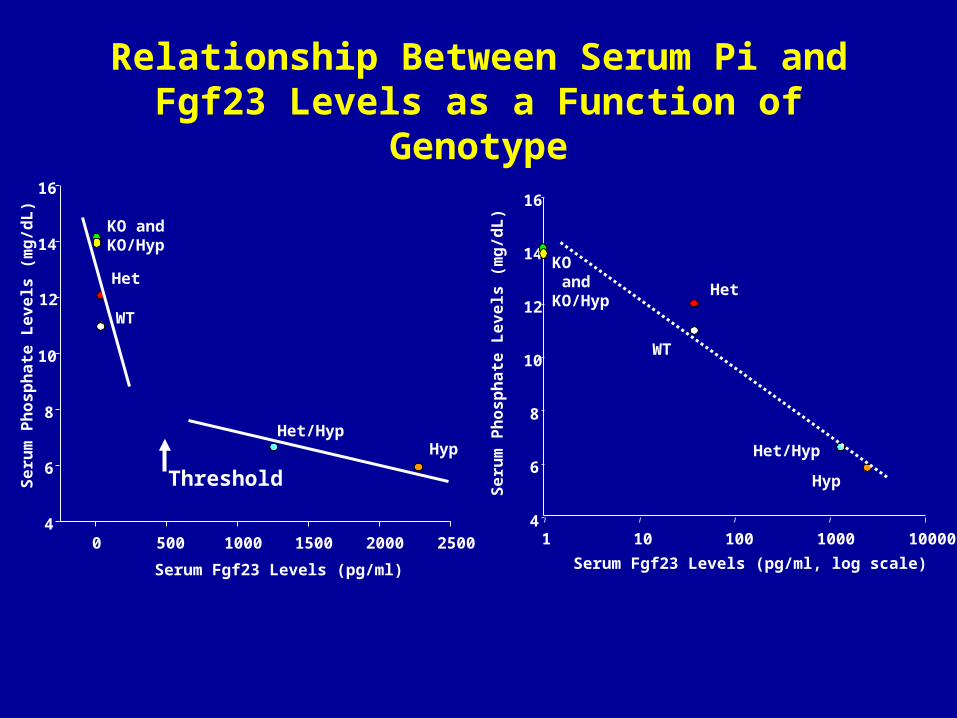
Serum Fgf23 Levels (pg/ml)
0 500 1000 1500 2000 2500
Se
rum
Ph
os
ph
ate
Le
ve
ls (
mg
/dL
)
4
6
8
10
12
14
16
HypHet/Hyp
WT
Het
KO and KO/Hyp
1 10 100 1000 10000
Se
rum
Ph
os
ph
ate
Le
ve
ls (
mg
/dL
)
4
6
8
10
12
14
16
Serum Fgf23 Levels (pg/ml, log scale)
Hyp
Het/Hyp
WT
Het
KO and KO/Hyp
Relationship Between Serum Pi and Fgf23 Levels as a Function of Genotype
Threshold
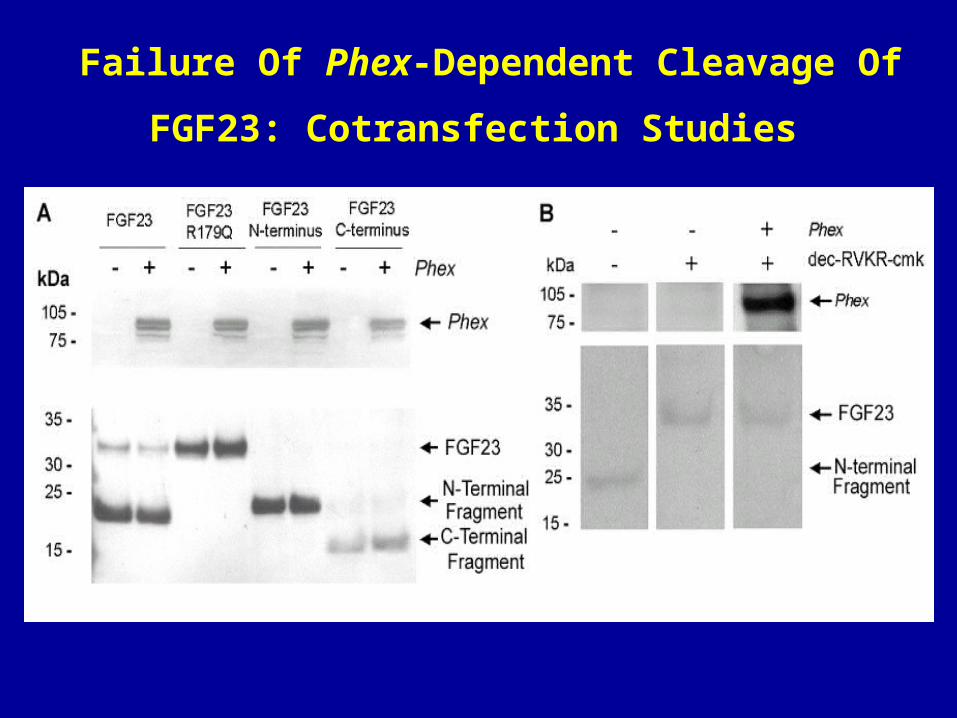
Failure Of Phex-Dependent Cleavage Of FGF23:
Cotransfection Studies

Expression of fgf23 mRNA levels in normal
and Hyp-derived bone and osteoblasts

Fgf23 +/+
BM
CB
GP
CB
BM
GP
Hyp/Fgf23 +/-
BM
GP
CB
Fgf23 +/-
Inactivating Phex mutations in Hyp increase FGF23 gene expression in bone of heterozyogous FGF23 knock-out/GFP knock-in mice

Role of fgf23 in Phex Deficiency• Superimposed fgf23 deficiency rescues hypophoshatemia in Hyp mice.• Fgf23 does not appear to be a substrate of Phex.• Phex-deficiency increases fgf23 expression through unknown
mechanisms.• An alternative hypothesis is needed to explain increments in
circulating fgf23 levels in association with inactivating Phex mutations.

What Is The Physiological Role of FGF23?
• Regulation of FGF23 expression.
• End-organ effects of FGF23:
– Kidney.
– Parathyroid gland.
– Other tissues.
• Role in CKD
• Isolation and characterization of mouse Fgf23 promoter.
• Evaluation of potenital regulators of Fgf23 promoter activity, including PTH, Vitamin D, calcium and phosphorus in vitro.
• Confirmation that these factors regulate serum Fgf23 levels in vivo.
Physiological Function of FGF23: Lesions From Studies of the Fgf23 Promoter
1 mM 2 mM 3 mM 4 mM
0.0
0.2
0.4
0.6
0.8
1.0
1.2
Phosphate Concentration
1 mM 2 mM 3 mM 5 mM0.0
0.2
0.4
0.6
0.8
1.0
1.2
Calcium Concentration
Luci
fera
se A
ctiv
ities
(F
irefly
/Ren
illa)
Luci
fera
se A
ctiv
ities
(F
irefly
/Ren
illa)
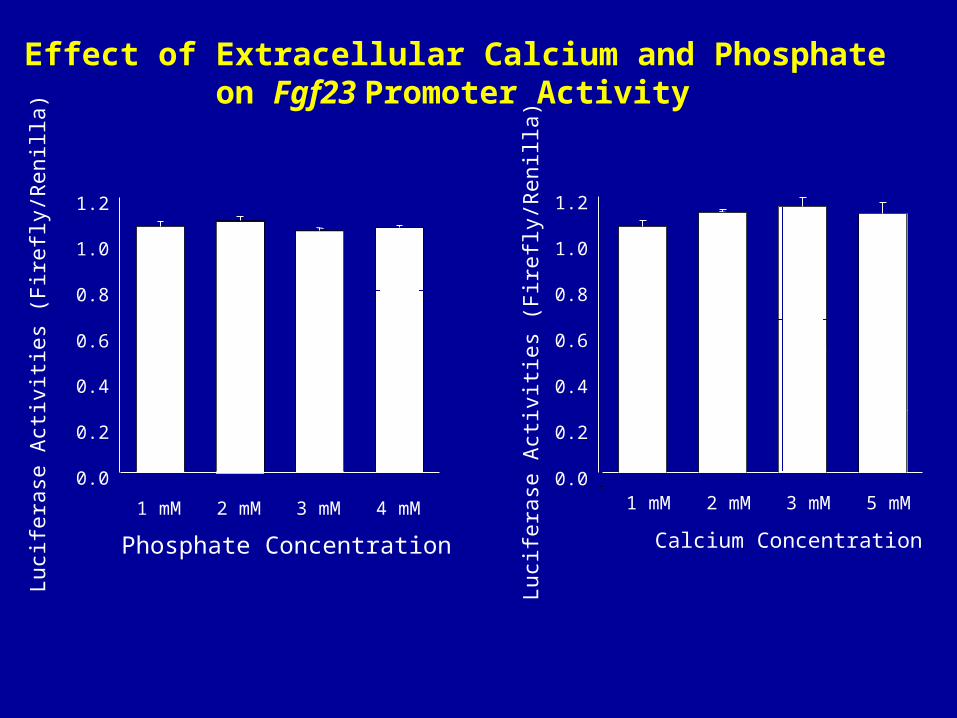
Effect of Extracellular Calcium and Phosphate on Fgf23 Promoter Activity

Lu
cife
rase
Act
ivit
ies
(Fir
efly
/Ren
illa)
1,25-(OH)2-vitamin D 3 Concentration
0.0
0.5
1.0
1.5
2.0
2.5
3.0
0 M 10-10 M 10-9 M 10-8 M
**
Effect of 1,25‑(OH)2D3 on Fgf23 Promoter Activity
Lu
cife
rase
Act
ivit
ies
(Fir
efly
/Ren
illa)
PTH Concentration
0 mM 1 mM 10 mM 100 mM
0.0
0.2
0.4
0.6
0.8
1.0
* * *
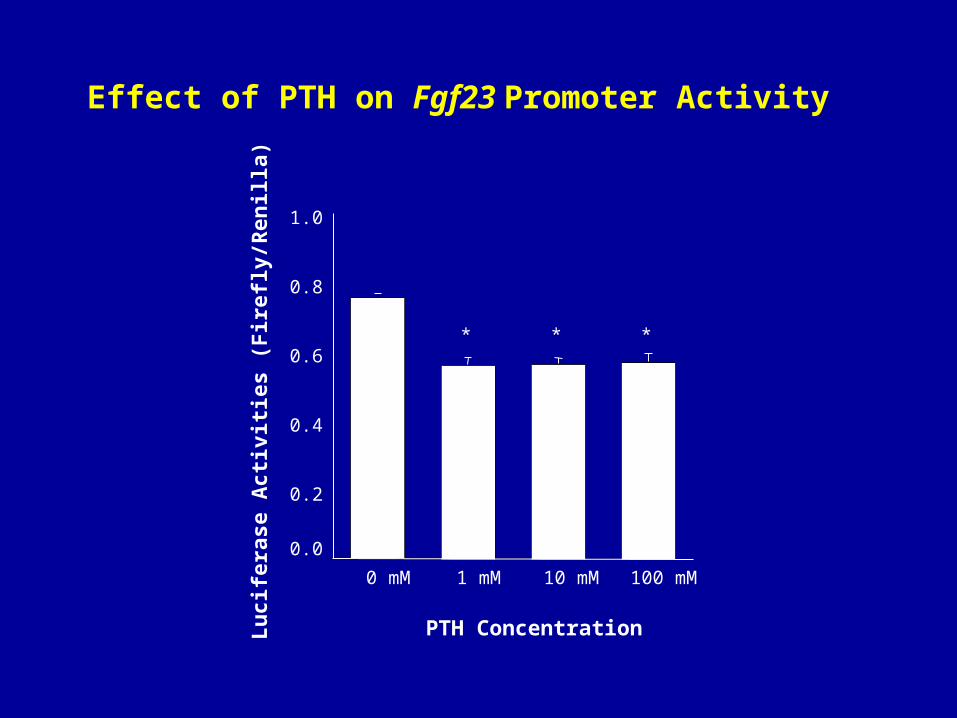
Effect of PTH on Fgf23 Promoter Activity
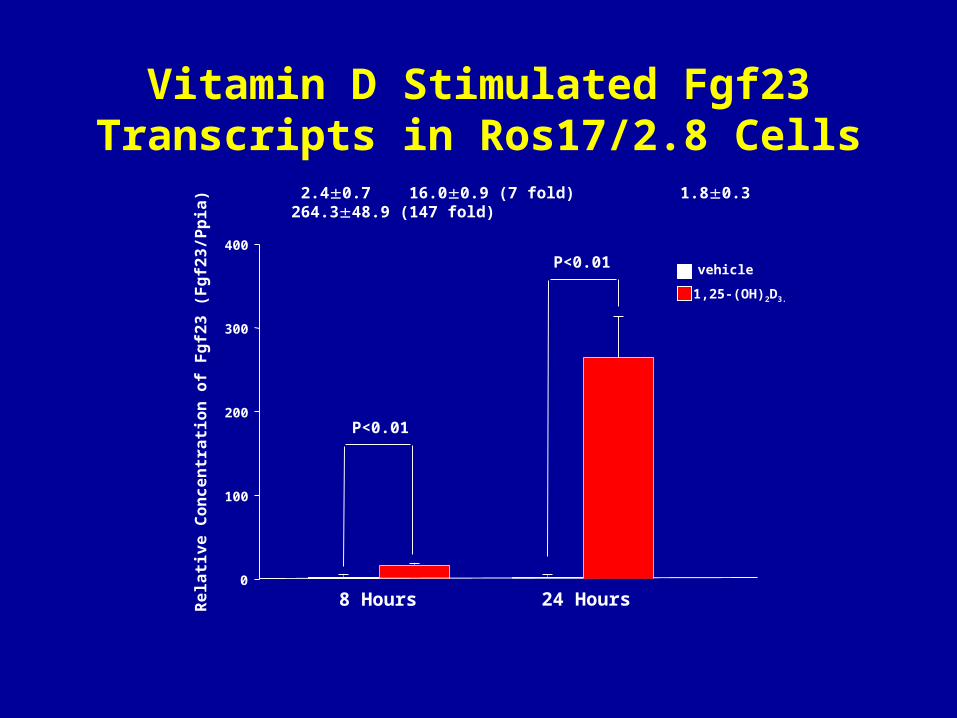
Vitamin D Stimulated Fgf23 Transcripts in Ros17/2.8 Cells
vehicle
Re
lati
ve
Co
nc
en
tra
tio
n o
f F
gf2
3 (
Fg
f23
/Pp
ia)
0
100
200
300
400
1,25-(OH)2D3.
8 Hours 24 Hours
2.40.7 16.00.9 (7 fold) 1.80.3 264.348.9 (147 fold)
P<0.01
P<0.01

Ser
um
In
tact
PT
H
(p
g/m
l)
Vehicle Calcitriol0
10
20
30
40
*
Vehicle Calcitriol
Ser
um
Cal
ciu
m
(mg
/dL
)
0
2
4
6
8
10
Vehicle Calcitriol
Ser
um
Ph
osp
ho
rus
(
mg
/dL
)
0
2
4
6
8
10
Ser
um
FG
F2
3
(p
g/m
l)
0
20
40
60
80
100
120
140
160
Vehicle Calcitriol
*A B
DC
Effect of 1,25‑(OH)2D3 on Serum Levels of Fgf23, PTH, Phosphorus and Calcium
100 ng/g/BW Calcitriol IP

Characteristics of Fgf23 Promoter
• The mouse Fgf23 promoter is characterized by:- A transcription start site 123 bp upstream of the initial ATG.- A TATA box 35 bp upstream of the transcription start site.- 67% homology with the human promoter over the first 800 bps.
• The 3.5kb 5' flanking region of the mouse Fgf23 gene has promoter activity in vitro.
• In ROS 17/2.8 osteoblasts, 1,25(OH)2D3 stimulates activity of the Fgf23 promoter/reporter construct, and alterations of extracellular phosphorus and calcium concentrations have no effect.
• Injection of calcitriol into wild-type mice increases serum Fgf23 levels from a basal level 90.0±8.9 pg/ml to 136.4 ± 8.7pg/ml (Mean ± SEM) at 24 hours after injection.
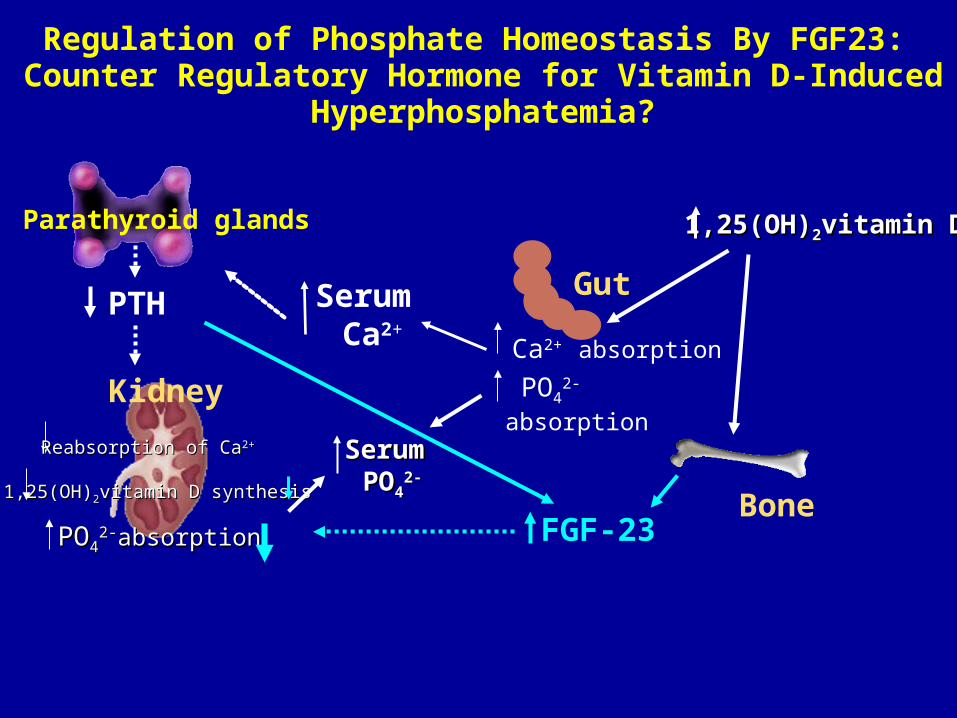
Regulation of Phosphate Homeostasis By FGF23: Counter Regulatory Hormone for Vitamin D-Induced
Hyperphosphatemia?
Bone
Kidney
Reabsorption of CaReabsorption of Ca2+ 2+
1,25(OH)1,25(OH)22vitamin D synthesisvitamin D synthesis
POPO442-2-absorptionabsorption
Parathyroid glands
PTHCa2+ absorption
Gut
PO42-absorption
Serum Serum POPO44
2-2-
FGF-23
Serum Ca2+
1,25(OH)1,25(OH)22vitamin Dvitamin D

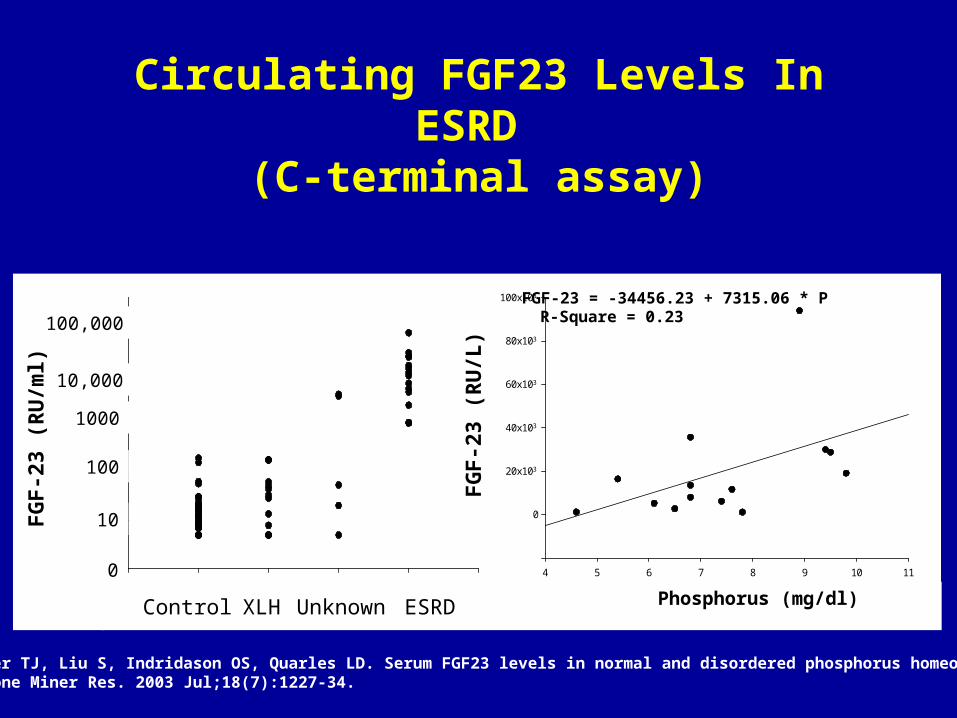
Uncertain Role of FGF23 in CKD
• Circulating levels of FGF23 are increased in CKD.
100
101
102
103
104
105
106
FG
F-2
3 (R
U/m
l)
Control XLH Unknown ESRD
0
10
100
1000
10,000
100,000
4 5 6 7 8 9 10 11
-20x103
0
20x103
40x103
60x103
80x103
100x103
Phosphorus (mg/dl)
FG
F-2
3 (R
U/L
)
FGF-23 = -34456.23 + 7315.06 * PR-Square = 0.23
Circulating FGF23 Levels In ESRD (C-terminal assay)
Weber TJ, Liu S, Indridason OS, Quarles LD. Serum FGF23 levels in normal and disordered phosphorus homeostasis. J Bone Miner Res. 2003 Jul;18(7):1227-34.
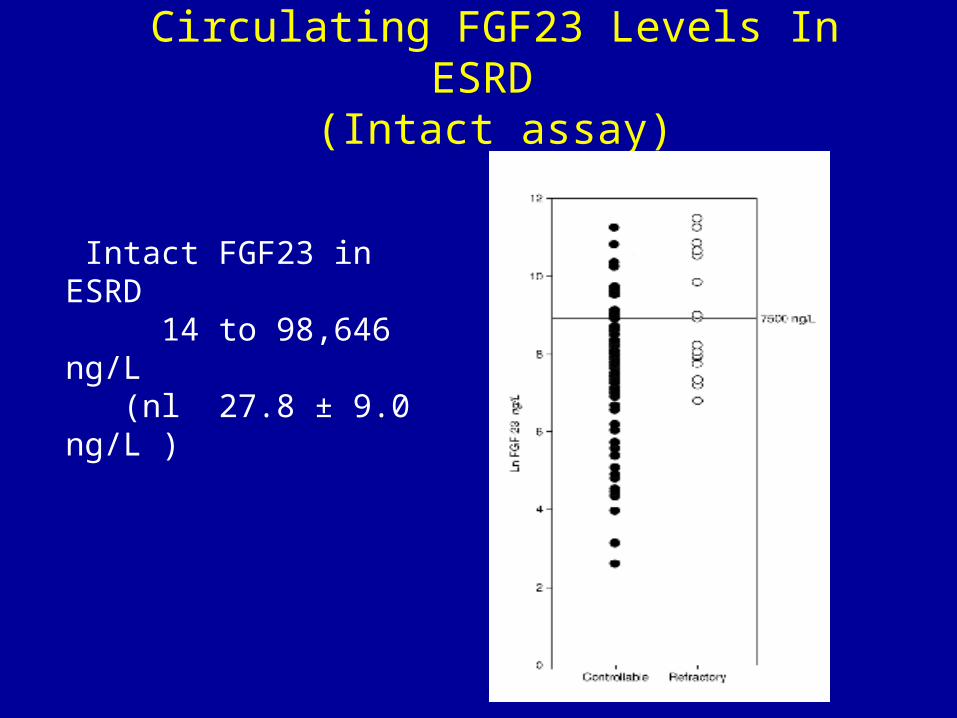
Intact FGF23 in ESRD 14 to 98,646 ng/L (nl 27.8 ± 9.0 ng/L )
Circulating FGF23 Levels In ESRD (Intact assay)

Fumihiko Koiwa, (2005) Sevelamer Hydrochloride and Calcium Bicarbonate Reduce Serum Fibroblast Growth Factor 23 Levels in Dialysis Patients. Therapeutic Apheresis and Dialysis 9:4, 336-339
Sevelamer Hydrochloride and Calcium Bicarbonate Reduce Serum Fibroblast Growth Factor 23 Levels in Dialysis Patients

Vitamin D Treatment Is Associated With Increased FGF23 Levels In Dialysis Patients
Shohei N et al. Kidney Intern 67:1171-1178, 2005

Uncertain Role of FGF23 in CKD
• Circulating levels of FGF23 are increased in CKD.• Evidence for a role in development of secondary HPT.
Cross-sectional clinical observations: Diminishes 1,25(OH)2D3 in kidney and stimulates PTH by parathyroid gland.

Factors Associated with FePO4
Full multivariate β P R2
model .50 log FGF23 5.2 0.009 log PTH 6.0 0.004 eGFR -.02 0.031 sP -1.0 0.615
FGF23 Mitigates Hyperphosphatemia in CKD
Gutierrez O JASN 2204-2205, 2005
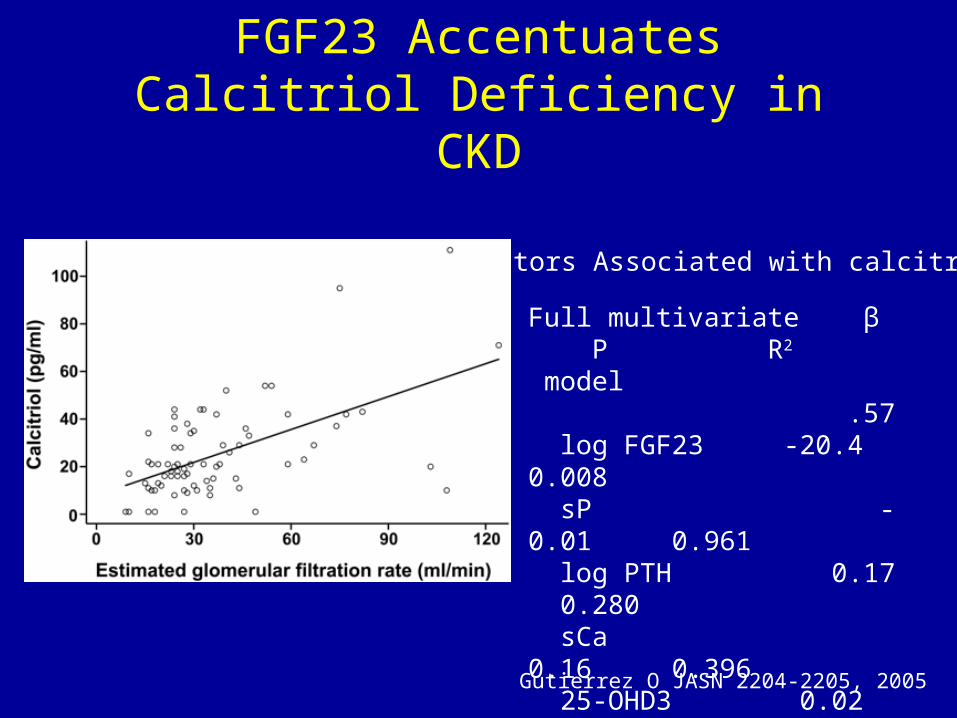
FGF23 Accentuates Calcitriol Deficiency in CKD
Factors Associated with calcitriol
Full multivariate β P R2
model .57 log FGF23 -20.4 0.008 sP -0.01 0.961 log PTH 0.17 0.280 sCa 0.16 0.396 25-OHD3 0.02 0.043 eGFR 0.01 0.067
Gutierrez O JASN 2204-2205, 2005

Uncertain Role of FGF23 in CKD
• Circulating levels of FGF23 are increased in CKD.• Evidence for a role in development of secondary HPT.
Cross-sectional clinical observations: Diminishes 1,25(OH)2D3 in kidney and stimulates PTH by parathyroid gland.
• Effects on other organ systems (positive vs negative?)– Vasculature– Pituitary– Pancreas?– Bone?

Hyperphosphatemic Familial Tumoral Calcinosis (HFTC; MIM211900)
• Autosomal recessive hyperphosphatemic disorder characterized by the progressive deposition of calcified masses in cutaneous and subcutaneous tissues.
• Caused by recessive mutations in at least two genes– GALNT3 (ppGalNacT3-mediated O-glycosylation
may protect normal FGF23 from proteolysis)
– FGF23 (destabilizing mutations)

S71G Missense Mutation in FGF23 Causes Tumoral Calcinosis
PO4 7.9-8.9 mg/dlTMP/GFR 3.5 mM/l 1,25(OH2)D3 65-85 pg/ml C-terminal FGF23 >1,800 Ru/mluCa 4.6 mg/kg BW
Tissue Calcification Serum Biochemistries
Mutation
Chefetz I, et al . A novel homozygous missense mutation in FGF23 causes Familial Tumoral Calcinosis associated with disseminated visceral calcification. Hum Genet. 2005 Sep 7;:1-6

Uncertain Role of FGF23 in CKD
• Circulating levels of FGF23 are increased in CKD.• Evidence for a role in development of secondary HPT.
Cross-sectional clinical observations: Diminishes 1,25(OH)2D3 in kidney and stimulates PTH by parathyroid gland.
• Effects on other organ systems (positive vs negative?)– Vasculature– Pituitary– Pancreas?– Bone?
IS A CO-FACTOR REQUIRED FOR FGF23 ACTIONS?

[Klotho]: Identification of Essential Molecule Responsible for Tissue Specific FGF23 Signaling
• FGF23 induced ERK/Egr-1 in kidney, parathyroid and pituitary, but not heart, lung, liver and spleen.
• Klotho purified from kidney as a FGF23 interacting protein.
• FGF23 responsiveness could be imparted to non-responding cells by overexpression of Klotho.
• Klotho is either a receptor for FGF23 or required for FGF23 activation of a cell surface receptor.
• FGF23 levels are markedly increased in Klotho null mice due to end-organ resistance?
Urakawa, I et al ASBMR M132, 2005.





























