Embed Size (px)
Citation preview
Abstract of thesis entitled
“Evidence-based guideline on Home-based exercise for the prevention of
treatment related lymphoedema on breast cancer patients”
Submitted by
Lam Hoi Yuk
for the degree of Master of Nursing
at the University of Hong Kong
In July 2015
Lymphoedema following breast cancer surgery remains a common and serious
treatment complication for cancer survivors, affecting their physical, psychological
and social well-being. Current evidences indicated that Home-based exercise (HBE),
a low cost and time-saving everyday exercise at home, does prevent lymphoedema
but is yet to be widely adopted in Hong Kong. This translational research proposal is
aimed at formulating a Home-based exercise programme (HBEP) for preventing
treatment related lymphoedema on breast cancer patients based on the best available
research evidences. The objectives are to evaluate the literatures on the efficacy of
HBE in preventing lymphoedema, identify essential components in implementing a
HBEP and develop an evidence-based guideline on HBEP as well as to develop an

implementation and evaluation plan for the HBEP guideline and determine its
transferability to other settings.
In evaluating the effectiveness of HBE in preventing lympohoedema due to breast
cancer treatment, an integrated and systematic review of literatures was carried out.
Eight relevant studies were identified and critically appraised by the Scottish
Intercollegiate Guidelines Network (SIGN) checklist on randomized control trial. The
findings indicated HBE had a significant effect on the prevention of breast cancer
related lymphoedema. An evidence-based guideline on HBEP was developed with
recommendations on patient recruitment, intervention and evaluation. All
recommendations were graded according to the SIGN guideline. The implementation
potential of the proposed intervention in the designated clinical setting was assessed
in terms of transferability, feasibility and cost-benefit ratio. Results of the assessment
indicated the proposed guideline is feasible to implement in the designated unit.
Furthermore, to facilitate the adoption of the innovation, a concrete and effective
communication plan, 2-month pilot study and evaluation plan were subsequently
established.
From bringing better patient outcome to reducing medical expenses, it is worth
and essential to implement this evidence-based guideline of Home-based exercise to
prevent life-long patients suffering and guide a safe and coherence nursing practice.

Evidence-based guideline on Home-based Exercise for the prevention
of treatment related lymphoedema on breast cancer patients
by
Lam Hoi Yuk
BN, RN
A thesis submitted in partial fulfilment of the requirements for the degree of
Master of Nursing at The University of Hong Kong.
July 2015

i
Declaration
I declare that this thesis represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualifications.
_____________________
Lam Hoi Yuk
July 2015

ii
Acknowledgements
No major undertaking is accomplished alone, my supervisor, my family and my
friends are invaluable when working with my dissertation in this two years. I would
like to express my deep appreciation and the warmth thanks to my supervisor Dr.
Joyce Oi-Kwan Chung, Lecturer, for her enlightenment, ongoing guidance and
invaluable support and assistance in the past two years.
I am also grateful to my classmate of the Master of Nursing Programme 2015, my
colleagues and my friends Dominic Chow and Vivian Yuen for their generosity,
understanding and support throughout the years.
Finally, I would like to express my gratitude to my family for their unending love,
encouragement and invaluable support throughout my life.

iii
Contents
Declaration…………………………………………………………………………….i
Acknowledgements………………………………………………………….…………ii
Table of Contents…………………………………………………...…………………iii
List of Appendice………….............................................................................………..vi
Chapter 1 Introduction
Background………………………………………………………………………1
Affirming the need……………………………………………………………….3
Objectives and Significance…………………………………………….………..5
Chapter 2 Critical Appraisal
Search and Appraisal Strategies
Identification of studies………………………………………………………8
Inclusion/ exclusion criteria………………………………………………….8
Data extraction & appraisal strategies……………………………………......9
Results
Characteristics of selected studies……………………………………….….10
Methodology quality………………………………………………….…….12
Summary and Synthesis……………………………………………………...…14
iv
Chapter 3 Translation and Application
Implementation potential
Target audiences and setting…….………………………………………..…21
Transferability of the findings
Comparability of target audiences and setting………………….……….….22
Philosophy of care……………………………………………………..……23
Number of clients benefit from the innovation………………………….…24
Estimated timing for implementation and evaluation………………………24
Feasibility
Freedom of implementation………………………………………….……..25
Interfere on current staff function…………………………………………..26
Administrative support…………………………………………………..…27
Consensus with other healthcare professionals……………………….…….27
Staff development & resources needed……………………………….……28
Available evaluation tools…………………………………………..………29
Cost-benefit ration of the innovation
Possible risks and benefits……………………………………….…………29
Cost…………………………………………………………………………31
Evidence-based practice guideline/protocol……………………………………32

v
Chapter 4 Implementation Plan
Communication plan with potential users
Identification of stakeholders……………………………………………....33
Communication process…………………………………………………….35
Pilot study plan…………………………………………………………………37
Patient recruitment strategies……………………………………………….38
Intervention evaluation……………………………………………………...38
Outcome measurement…………………………………………………...…39
Evaluation plan………………………………………………………………….40
Patient outcomes……………………………………………………………40
Staff outcomes………………………………………………………………42
System outcomes……………………………………………………………42
Nature and number of clients…………………………………………….…43
Data collection and analysis…..………………………………………...…..44
Basis for practice effectiveness…………………………………………..…45
Chapter 5
Conclusion……………………………………………………………..……47
Appendices………………………………………………………………………..…48
References…………………………………………………………………….……..79

vi
List of Appendices
Appendix 1
Search Table……………………………………………………………………..48
Appendix 2
Tables of Evidence………………………………………………………………49
Appendix 3
Quality assessments of studies………………………………………………..…52
Appendix 4
Timeline of HBEP………………………………………………………..………68
Appendix 5
Estimated total cost of implementing HBEP…………………………….……….69
Appendix 6
Estimated total cost of not implementing HBEP………………………………...71
Appendix 7
Evidence-based guideline of HBEP………………………………..…………….72
1
Chapter 1
Introduction
1.1 Background
Breast cancer is the second most common cancer in the world and remains as the
top cancer in women causing around 521,000 of deaths worldwide in 2012 (IARC,
2014). Comparing to other Asian countries, Hong Kong especially has the highest
incidence rate of 61 per 100,000 people while that of China was only 22.1
(Sankaranarayanan, Swaminathan & Lucas, 2011). In Hong Kong, the annual number
of breast cancer cases diagnosed has tripled in the past two decade, as it dramatically
increased from 1152 cases diagnosed in 1993 to 3419 cases in 2011 (Hong Kong
Cancer Registry, 2013). Despite the high incident rate and rising trend of breast
cancer in Hong Kong, the 5-year survival rate was the highest among Asia with
almost 90% (Sankaranarayanan, Swaminathan & Lucas, 2011). The phenomenon may
attribute to the early detection of breast cancer in recent years from increasing public
awareness and education on self-examination, as well as the availability of advanced
surgical and oncological management.
Management strategies on breast cancer include surgery, radiotherapy, systemic
hormonal therapy and chemotherapy (HA Central Oncology Committee, 2009).
Surgery is widely considered as the primary and standard treatment for early breast

2
cancer, aimed at tumour resection and clearance of involved marginal lymph node in
minimizing the chance of recurrence (HA Central Oncology Committee, 2009;
National Cancer Institute, 2013a).
Despite the survival chance of patients were greatly increased, cancer survivors
still have a long journey to live with the subsequent problems arise from the
symptoms of breast cancer related lymphoedema, emotional effects as well as side
effect from adjuvant therapy etc. (Britton & Purushotham,2009; National Cancer
Institute, 2013b).
Breast cancer related lymphoedema (BCRL) is the disturbance on the lymphatic
system causing chronic swelling over upper limb after excision of axillary lymph
node and adjuvant therapy, affecting up to 28-34% of patients (Britton &
Purushotham,2009; Rinder, 2013). Empirical studies supported that treatments on
breast cancer are highly related to lymphoedema, removal of axillary lymph node may
lower the lymph carrying capacity of fluid, axillary dissection may increase blood
flow, altered axillary vessels and overloading the lymphatic system (Britton &
Purushotham,2009; National Cancer Institute, 2013a). More, adjuvant radiotherapy
would cause lymph node fibrosis and lead to lymphatic system obstruction (Britton &
Purushotham, 2009; Rinder, 2013). With the growing numbers of patient being
diagnosed and offered surgery, it can be estimated that the incidence of developing
3
BCRL will be further increase; therefore it is worth to review the existing
management of the issue.
Recently, there is a new trend of implementing Home-based exercise (HBE)
rehabilitation programme on preventing lymphoedema in foreign countries but is yet
to be widely adopted in Hong Kong (Box et al., 2002; Kilgour, Jones & Keyserlingk,
2008; Kilbreath et al., 2013). Therefore, this paper will discuss about the
evidence-based practice of HBE on breast cancer survivors at risk for lymphoedema,
aims to provide better patient outcomes.
1.2 Affirming the need
In caring breast cancer patient in a surgical unit, patients usually discharge on the
next day of operation if there is no post-operative complication after an over-night
observation. They will have routine follow-up for wounds and afterwards
chemotherapy as well as radiotherapy. Patients underwent mastectomy with axillary
lymph node excision will be offered an extra and elective session by physiotherapists
on introducing manual drainage, exercise and after surgery care, charged for $150 for
an hours. Since, patient with only an hour session of exercise programme, they may
not able to understand well about the aims, importance and steps of exercise. Due to
the low awareness on the issue, some of them may even not willing to attend the

4
session by spending extra time and money or even think it is just helpless. Current
practices on preventing BCRL are clearly inefficient and hence causing a low
participation rate as well as poor compliance of preventive exercise.
Increasing numbers of patients admitted for BCRL associated pain, swelling,
reducing range-of-motion in these years, treatments are usually unimpressive while
oedematous conditions are always irreversible from increasing swelling to developing
blister, wounds and infections. Numerous studies revealed that BCRL not only
affecting cancer survivor’s physical mobility, self-caring ability but also putting
additional psychological disturbance related to poor self-image, chronic pain, hence
reducing their quality-of-life and causing lots of suffers at their cancer journey
(Britton & Purushotham, 2009; National Cancer Institute, 2013b; Gautam, Maiya &
Vidyasagar, 2011; Pusic et al., 2013). In order to better managing the incurable BCRL,
to prevent is always better than control. With increasing trend of patients diagnosed
with breast cancer and offered management, it is estimated that greater numbers of
cancer survivors will be suffered from BCRL. There is a pressing need for implement
a standardized and evidence-based programme.
Numerous studies revealed that exercise increase lymphatic drainage by
enhancing lymph flow from extremities to proximal body, hence is effective in
managing BCRL (National Cancer Institute, 2013b; Stuiver et al., 2012). In recent

5
years, foreign countries are introducing Home-based exercise in promoting low cost
and time-saving everyday exercise at home (Jeff & Wiseman,2012; Gautam, Maiya &
Vidyasagar, 2011). Nurses play an essential role on disease prevention by educating
patients on post-operative exercise, knowledge of lymphoedema and the awareness of
its early sign (Sisman et al., 2012). Information leaflets are given to patients whereas
exercise classes are held to introduce simple exercise, enabling patients can do it at
home safely and freely (Box, 1998; Kilbreath et al., 2013).
In view of its beneficial effects on patients’ outcome, it is worth and essential to
evaluate this intervention and hence develop an evidence-based guidelines for guiding
safe and consistent nursing practice.
1.3 Objectives and Significance
The clinical question of this study is “What is the effect of home-based exercise
programme (HBEP) compared with usual care on the incidence of lymphoedema for
women with breast cancer?”
The objectives of this dissertation targeting women at risk for BCRL are:
1. To examine the effect of HBE on the incidence of lymphoedema
2. To identify the essential components in implementing the HBEP
3. To develop an evidence-based guideline for HBE

6
4. To develop an implementation plan for the HBE guideline
5. To determine the transferability of the evidence-based guideline to other settings
As aforementioned, BCRL is a prevalence and serious complications for breast
cancer survivors, affecting their physical and psychological well-being. Introducing
an effective HBEP could benefit the patient, nurses and the institution.
For patients, development of BCRL causing long term sufferings and
inconveniences, greatly affecting their quality-of-life. From minimizing the incidence
of developing BCRL to bringing better patient outcomes, its worth for implementing
this simple, time-saving and costless intervention to prevent life-long suffering.
As stated in the Vision and Mission of the Hospital Authority (2014), healthcare
providers should dedicate ourselves to provide high quality services on patients to
empower them to regain and stay healthy. In view of the long-term suffering on
patients with lymphoedema, nurses should be innovative and active to participate on
for example education, follow up and management on implementing HBE for better
patient outcomes. Nurses could empower themselves and develop professionalism
through implementing a nurse-led programme.
For institutes, patients with BCRL usually admitted repeatedly due to pain, wound
infection, progressively increase swelling etc. Due to its incurable nature, treatments

7
in hospital mainly focused on symptom control by analgesics, antibiotics and offering
wound dressing as well as fitting pressure garment by occupational therapist and
providing pneumatic pumping or manual drainage by physiotherapist. Patients with
symptoms alleviated will be discharged and most of them will be relapsed and
admitted repeatedly. Multiple team consultations, long length-of-stays and repeatedly
admission put a huge impact on especially the health care system in Hong Kong by
increasing medical expenses. With effective intervention on lowering the incidence of
BCRL, the cost can be reduced.
Therefore, a newly, safely, low-cost intervention on prevention of BCRL should
be evaluated and later bring into practice to give better patient outcome and help
reducing medical expenses. A clear and evidence-based guideline should be
developed for guiding a safe and coherence nursing practice.

8
Chapter 2
Critical Appraisal
2.1 Search and Appraisal Strategies
2.11 Identification of studies
The electronic databases used for searching include PubMed, CINAHL PLUS
(EBSCOHOST), Cochrane Library (Trials) and ProQuest.
Four groups of keywords related to breast cancer (tumor, neoplasm, carcinoma,
malignancy), breast surgery (mastectomy, lumpectomy, lymph node dissection),
lymphoedema (swelling, edema, edematous, arm circumference, limb circumference)
and exercise (physical activity, physical therapy, physiotherapy, rehabilitation,
training, breathing, aerobic, stretching, weightlifting, weight bearing, flexibility,
resistance) were used and combined for searching relevant studies from the electronic
databases.
The titles and abstracts of the retrieved articles were screened. Articles that
fulfilled the inclusion criteria were selected. The Reference lists of these selected
articles were screened to identify additional relevant studies.
2.12 Inclusion/ exclusion criteria
The inclusion criteria are (1) interventional studies evaluating Home-based
9
exercise on breast cancer patient in preventing lymphoedema, (2) patients underwent
breast surgery (mastectomy, modified radical mastectomy, lumpectomy, breast
conserving surgery +/- lymph node dissection), (2) written in English, (3) retrievable
in full-text. Subjects with (1) age >80, (2) men and (3) women with existing
lymphoedema were excluded.
2.13 Data extraction & appraisal strategies
Data extracted from the selected studies were summarized in the Table of
Evidence (attached in the appendix 2) and presented in the descendant order of
publication year. The following data of each studies were recorded: The citation,
study type, evidence level, population, sample & design, length of follow-up, outcome
measures and effect size.
In assessing the quality of the studies, the Scottish Intercollegiate Guidelines
Network (SIGN) checklist on randomized control trial was used. It was developed in
1993, which assists healthcare professionals in evaluating the methodology of
literatures systemically, hence guiding the best evidence for developing practical
guidelines (SIGN, 2014). All selected studies were then rated with the hierarchy of
evidence according to this guideline.

10
2.2 Results
The search was carried out from the early February to 18 of September in 2014, a
total of 34,898 potential relevant studies were identified after initial keyword searches
through the four databases. Among these, 595 studies met all the inclusion and
exclusion criteria. Upon screening the topics and abstracts, 56 studies were identified
for further consideration. The full-text review of these studies led to the inclusion of
17 studies. However, 10 studies were excluded due to duplication but an additional
study was identified through the review of reference lists. Finally, a total of 8 eligible
studies (Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012;
Cinar et al., 2008; Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008; Box et al.,
2002; Wingate, 1985) were selected for this review. The search history was attached
in Appendix 1.
2.21 Characteristics of selected studies
Of the eight selected studies, five of them were randomized controlled trials (RCT)
(Kilbreath et al., 2013; Cinar et al., 2008; Kilgour, Jones & Keyserlingk, 2008; Todd
et al., 2008; Box et al., 2002) and the others were quasi experiments (Singh, Vera &
Campbell, 2013; Scaffidi et al., 2012; Wingate, 1985). They were published between
1985 and 2013, and originated from six countries, including two from Australia

11
(Kilbreath et al., 2013; Box et al., 2002), two from Canada (Singh, Vera & Campbell,
2013; Kilgour, Jones & Keyserlingk, 2008) and one each from Italy (Scaffidi et al.,
2012), Turkey (Cinar et al., 2008), United Kingdom (Todd et al., 2008) and United
State (Wingate, 1985). All studies included women who had scheduled or undergone
breast surgery of modified radical mastectomy, simple mastectomy, lumpectomy or
breast conserving surgery with or without axillary lymph node dissection as the
subjects. Women with cognitive and neurological deficit as well as having underlying
shoulder problems including sustained fracture and with previous surgery were
commonly excluded. The mean age of participants ranged from 50 to 60 years. The
study data were extracted and tabulated in Appendix 2 for a quick summary.
The major outcomes of all studies were incidence of lymphoedema and shoulder
range-of-motion. Others less frequently assessed outcomes were quality-of-life, pain
and upper limb function, as well as length-of-stay in hospital. The incidence of
lymphoedema was an objective measurement determined by arm circumference
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et
al., 2008; Kilgour, Jones & Keyserlingk, 2008; Box et al., 2002; Wingate, 1985),
water displacement method (Todd et al., 2008; Box et al., 2002) and multi-frequency
bioimpedance analysis (Box et al., 2002; Kilbreath et al., 2013). Box et al., (2002)
was the only study compared the three methods and multi-frequenct bioimedance

12
analysis was considered as the most reliable method with 100% consistency with
clinical significant, while the other two methods might underestimate the incidence by
33% to 42%. Shoulder range-of-motion was measured by the Goniometer (Singh,
Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et al., 2008; Kilgour, Jones &
Keyserlingk, 2008; Todd et al., 2008; Wingate, 1985). The upper limb function was
measured using the Constant & Murley Score (Scaffidi et al., 2012), Disabilities of
Arm, Shoulder and Hand Score (DASH) (Singh, Vera & Campbell, 2013) and the
functional questionnaire developed by Wingate (1985) (Cinar et al, 2008; Wingate,
1985). Quality-of-life was evaluated using the Functional Assessment of Cancer
Therapy- Breast (FACT-B+4) (Singh, Vera & Campbell, 2013; Todd et al., 2008). Pain
level was measured by the Visual Analogue Scale (Singh, Vera & Campbell, 2013)
and the Borg’s Category Scale (Kilgour, Jones & Keyserlingk, 2008).
2.22 Methodology quality
As aforementioned, appraisal assessments were conducted on each selected
studies using the SIGN checklist and the details were attached in Appendix 3. All
studies did address the research question appropriately and clearly. In three RCTs,
subjects were randomized using the random number table or computerized random
number list (Kilbreath et al., 2013; Kilgour, Jones & Keyserlingk, 2008; Todd et al.,

13
2008), however the methods of randomization were not indicated in the other two
RCTs (Cinar et al., 2008; Box et al., 2002) and hence whether the assignments were
truly random were unable to verify. Of the two quasi experiments with acceptable
rating, subjects allocated to groups according to the time period (Scaffifi et al., 2012),
which were before and after the renovation of rehabilitation service and according to
the location (Singh, Vera & Campbell, 2012), where were two different sites within
the same authority. The baseline characteristics between the study groups of these
studies were similar. Detail report on demographic data and health history was
included in all studies except on the study of Wingate (1985). In this study, patient
assignment was made by the preference of physician (Wingate, 1985). Subjects in the
intervention group had significantly greater number of axillary lymph node being
removed, which may higher the incidence of lymphedema, adding an associated risk
of bias on the study outcomes.
Moreover, only two studies used opaque, sealed envelopes and employed an
objective third person for groups allocation to ensure adequate concealment
(Kilbreath et al., 2013; Todd et al., 2008). Blinding on subjects was uncommon in all
studies. Owing to the nature of the study, patient blinding was not clinically feasible
and unethical. There is an indication for explaining the possible risks of the study and
obtaining informed consent for this new intervention. Instead, blinding on investigator
14
was possible in minimizing bias in measuring the study outcomes and was attempted
in five studies (Kilbreath et al., 2013; Cinar et al., 2008; Kilgour, Jones & Keyserlingk,
2008; Todd et al., 2008; Box et al., 2002). All outcomes were measured with reliable
tools and in a standard and valid way. The percentage of participant dropout from the
studies were ranged from 0 to 12%, which is far below the considerable level of 20%.
After performing quality assessments in all studies, only the study of Wingate
(1985) was rejected, as it committed significant flaws in the study design by
convenience sampling and recruited subjects with significant between group
differences, which was likely affecting the study outcomes. All the others studies had
minor flaws in the design correlated to a low risk of bias were ranked as acceptable
with methodologically moderate to strong in quality.
2.3 Summary and Synthesis
In summary, six out of eight studies examined the effect of HBE. For the other
two studies, one study compared the effects of early and delay HBE on lymphoedema
(Todd et al., 2008) and the other study compared the differences between supervised
and Home-based exercises (Cinar et al., 2008). Cinar et al. (2008) indicated that
supervised exercise and HBE had only small difference in maintaining shoulder ROM
and upper limb function on patients. In addition, there were no significant difference
15
in arm circumference and incidence of developing lymphoedema. Supervised group
received 15 exercise sessions while the control group received HBE with return
demonstration during hospitalization. The result indicated that HBE shares the same
effectiveness in preventing lymphoedema and is feasible when clear instructions of
HBE were given with return demonstration.
HBE was effective in preventing lymphoedema, maintaining and improving
shoulder ranged-of-motion and upper limb function on breast cancer patients.
However, there were no difference between groups on quality-of-life and pain level.
Three studies reported an associated risk of developing lymphoedema in the HBE
group was significantly decreased by 2.6 to 3.8 times. (Kilbreath et al., 2013; Box et
al., 2002; Scaffidi et al., 2012). That means women in the control group had more
than two times the risk of developing lymphoedema compared with those in the HBE
group. A study with moderate methodological quality also reported the risk of
developing lymphoedema was 3.9 times greater in the non-HBE group but was unable
to achieve a statistical significance (Singh, Vera & Campbell, 2013). Women
underwent axillary dissection was not an inclusion criteria in this study, only half of
the included subjects had 5 or more lymph node being dissected. These subjects were
of lower risk of lymphoedema and therefore the reducing number of incidence may
influence the result in reaching a statistical significance. Another RCT reported small
16
but statistically significant decrease of arm circumference for a two-week programme
(Kilgour, Jones & Keyserlingk, 2008), showing that the immediate effect on
lymphoedema was not obvious. The study of Wingate (1985) was the only study that
reported an increase of arm circumference in the HBE group. As aforementioned, the
study had significant methodological flaws affecting the study outcomes, therefore the
contraindicated result of this study should be abandoned.
For the short to long term effect of HBE, the results were consistent as the
intervention significantly reduced the incidence of BCRL (Kilbreath et al., 2013; Box
et al., 2002; Scaffidi et al., 2012; Singh, Vera & Campbell, 2013). The baseline
characteristics of patients enrolled in these studies were similar and with no
significant difference. All studies were common in delivering “a package of”
home-based exercise programme, which comprised of preoperative education,
postoperative exercise and instruction on performing continuous HBE as well as
regular follow-up in monitoring the progress of HBE.
In these selected studies, preoperative education was given verbally or in written
booklets. The contents were similar and comprised of education on lymphoedema,
possible risk of developing lymphoedema and introduction of postoperative exercise.
Postoperative exercise from these studies varies from the starting time to the type of
exercise. In most studies, postoperative exercise was introduced by either

17
physiotherapists or nurses and started on postoperative day 1 to day 4 during
hospitalization (Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al.,
2012; Todd et al., 2008; Box et al., 2002).
Various types of exercise were introduced, including deep breathing exercise
(Singh, Vera & Campbell, 2013; Scaffidi et al., 2012), stretching exercise (Kilbreath
et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et al., 2008;
Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008), range-of-motion (ROM)
exercise (Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et al., 2008;
Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008; Box et al., 2002; Wingate,
1985), and resistance exercise (Kilbreath et al., 2013; Wingate, 1985).
Deep breathing exercise in both studies were started on postoperative day one
(Singh, Vera & Campbell, 2013; Scaffidi et al., 2012). For stretching exercise,
Kilbreath et al. (2013) implemented three stretches of shoulder flexion to elevate the
arm overhead, arm abduction to 90˚and 135˚ in supine position. Each stretch was
instructed to maintain 5 to 15 minutes. And the stretching exercise introduced by the
other studies was focused on the side flexion of neck muscles, elevation and
abduction of shoulder limited by 90˚ as well as flexion and extension of elbow, three
times a day for around 15 to 30 minutes in each session or 10 repetitions for each
stretch (Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et al., 2008;

18
Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008). Two studies in additionally
introduced advanced stretching exercise of raising arms overhead and wall climbing
hand exercise after drain removal or when drain output was less than 100ml per day
(Singh, Vera & Campbell, 2013; Box et al., 2002). For the range-of-motion exercise,
studies were common in commencing neck, hand and elbow exercise. Shoulder ROM
exercise was taken into caution and was introduced on postoperative day three to
seven (Singh, Vera & Campbell, 2013; Cinar et al., 2008; Todd et al., 2008; Box et al.,
2002). And the study by Todd et al. (2008) further explained that patients performing
active, vigorous full-shoulder exercise on day two after operation had 2.7 times
greater risk of developing lymphoedema when compared with patients undertaking
shoulder exercise limited by 90˚on movement in the first week after operation.
Subjects of these study were advised to perform the whole set of range-of-motion
exercise for two to three times in each day and stay pain-free. More, Kilbreath et al.
(2013) introduced resistance exercise by using Thera-band and obtained significant
results. Wingate (1985) suggested resistance exercise for HBEP had adversely
increased the incidence of developing lymphoedema, however whether the result was
attributed to the methodological flaw or the intervention itself was unknown.
Breathing, stretching and range-of-motion exercise are considered as low risk
when compared with vigorous, resistance exercise. Employing exercise with lower

19
risk may secure the safety of patients performing daily HBE. Introducing early
exercise and delayed full shoulder range-of-motion exercise during hospitalization
were beneficial to the subjects.
Except the study performed by Singh, Vera & Campbell (2013), all studies
provided written information of steps and safety reminders of HBE to patients while
the programme performed by Kilgour, Jones & Keyserlingk (2008) in additionally
distributed video for guidance. Except the two weeks HBEP of Kilgour, Jones &
Keyserlingk (2008), all studies included regular follow-ups in monitoring the progress
and checking the accuracy and safety of the HBE. For the HBEP lasted for 6 to 7
months, 1 to 2 follow-up sessions were offered to participants, while for 2-years
exercise programme and programme introduced resistance exercise, 8 follow-up
sessions were given.
Other than the study performed by Box et al. (2002) & Kilbreath et al. (2013), all
studies measured the interventional effects on arm or shoulder range-of-motion. Four
studies found a statistically significant increase in range-of-motion over the exercise
group when compared with the control group and ranged from 4.92 to 32 degree
(Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Kilgour, Jones & Keyserlingk,
2008; Wingate, 1985). The results showed that HBE was not only useful in preventing
lymphoedema, but also helpful in improving the shoulder range-of-motion.

20
To conclude, the outcomes of these studies were significant and their contents
were consistent, which is feasible and transferrable to my clinical setting in
preventing the incidence of lymphoedema.
21
Chapter 3
Translation and Application
Integrated review in the previous chapter supported that Home-based exercise
programme (HBEP) is safe and effective in preventing breast cancer related
lymphoedema to give better patient outcome. In view of its potential transferability to
the local clinical setting, it is essential to assess the implementation potential of this
intervention before implementing it. The assessment includes examining the
transferability of findings, the feasibility and the cost-benefit ratio of the innovation
for patient in a breast surgical unit (Polit & Beck, 2014).
3.1 Implementation potential
3.1.1 Target audiences and setting
The Home-based exercise programme is considered to be implemented in the
breast surgical unit of a regional hospital in Hong Kong. It is a teaching hospital for
local universities and regarded as a leading hospital among its cluster. The setting
consists of twenty-four beds and is shared between breast and two other surgical
teams. It is an integrated surgical unit with a multipurpose room and an interview
room for counselling and education.
The unit admits patients clinically for scheduled operation and emergency cases
22
from the Accident & Emergency Department. In this setting, the majority of breast
patients are admitted for operation while the others are admitted for the new case
work up or management of disease complications. The target audiences of the HBEP
are those who scheduled surgery for breast cancer.
3.1.2 Transferability of the findings
According to Polit & Beck (2014), transferability of findings means to which
extent the innovations fit in the new settings. In assessing the suitability of
implementing the HBEP in the target setting, the demographic characteristics of the
target audiences and setting would be compared with the reviewed studies. In addition,
the Philosophy of care, the number of clients could be benefited and the timing of
implementation and evaluation would be discussed.
3.1.2.1 Comparability of target audiences and setting
According to the data extracted from the CMS system of the Hospital Authority,
the mean age range of the target audience was 45 to 60 years which is similar to the
range of 50 to 60 years in the reviewed studies. In line with the evidence, the target
audience of the intervention are women who scheduled for breast cancer surgery
including mastectomy, modified radical mastectomy (MRM) and lumpectomy with

23
axillary lymph node dissection. The Home-based exercise programmes from all the
reviewed studies were conducted in hospital-based clinical setting, which are similar
to the target setting of a surgical unit in a public hospital.
Although all of the reviewed studies were performed in Western countries, the
effect of exercising should be the same across cultures. The characteristics of target
audiences and settings are similar to the selected studies, therefore the programmes
are considered to be suitable for applying in the target setting.
3.1.2.2 Philosophy of care
The Vision and Mission of the Hospital Authority (2014) stated that healthcare
providers should dedicate ourselves to provide high quality services on patients to
empower them to regain and stay health. The HBEP is of sufficiently high quality that
can prevent breast cancer related lymphoedema and thus preventing life-long
suffering (Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012;
Kilgour et al., 2008; Box et al., 2002).
With respect to the guideline for specialty nursing service in the target unit, nurses
need to provide holistic and continuity care to patients. The philosophy of care
underlying the intervention is to empower nurses to provide holistic perioperative care
to patients in preventing lymphoedema, thus is consensus with the Vision and Mission

24
of the Hospital Authority and the nursing service guideline of the target setting.
3.1.2.3 Number of clients benefit from the innovation
The target surgical setting admits around 300 patients with breast disease annually.
Among the total number of admissions, over 70% of them are admitted clinically for
scheduled operation, which is around 210 patients in each year. Of these,
approximately around 150 patients (3 to 4 cases per week) undergo breast cancer
operation. Therefore, the estimated number of patients meeting the inclusion and
exclusion criteria, willing to participate in the 12 months HBEP and being recruited in
first 5 months will be 55.
With the increasing number of patients being diagnosed at early stage and offered
surgery as discussed before, it can be estimated that the number of clients requiring
the home-based exercise service will be further increase. Thus, there is sufficiently
large number of clients can benefit from the innovation.
3.1.2.4 Estimated timing for implementation and evaluation
All selected studies delivered “a package of” HBEP including preoperative
education and counselling, postoperative education on performing daily home-based
exercise, and regular face-to-face and phone follow-up in monitoring the progress of

25
the home-based exercise. The recommended duration for implementing the
programme was at least six months to a year in showing the positive result (Singh,
Vera & Campbell, 2013; Scaffidi et al, 2012; Cinar et al., 2008; Kilbreath et al., 2013;
Todd et al., 2008). Therefore, it will take around 24 months to implement and evaluate
the proposed programme including 3 months for preparation and communication, 2
months for pilot test and evaluation and then another 19 months for actual
implementation of the programme and evaluation. The proposed timeline was
attached in Appendix 4.
In evaluating the process of the programme, the number of patients utilizing the
service and the satisfaction feedback on the programme would be considered. The
outcomes could be evaluated by the incident rate of lymphoedema, quality of life and
the adherence and admission rate of lymphoedema cases.
3.1.3 Feasibility
3.1.3.1 Freedom of implementation
The World Health Organization (2015) stated that “Nursing” is using the
autonomy and collaborative care in promoting health and prevention of illness. In the
target unit, by providing sufficient evidence in highlighting the significance of the
innovation and gaining support from the colleagues and the administrative level,

26
nurses do have the autonomy to implement innovation. An example of utilizing the
research innovation in the setting is the implementation of the drain care education to
postoperative breast patients advocated by the Breast Nurse in a few years ago. For
this year, a Registered Nurse identified there was no protocol in caring the chest drain
in the unit. With reference to the protocol from the Cardiothoracic Unit and the latest
literatures, an update and clear guideline was developed and put into practice. With
sufficient quality evidences and clear guidelines, nurses in this setting do have the
freedom of implementing innovation.
3.1.3.2 Interfere on current staff function
At this stage, the implementation of the Home-based exercise programme will
involve the Breast Nurse, a Registered Nurse, ward nurses and a clerical staff. Breast
Nurse will be invited to provide expert opinion, guidance and support on the
intervention. Minimal time will be needed to minimize conflicts with her current
duties.
The current nurse-to-patient ratio of the target setting is 1:6 to 8. Involving ward
nurses in the programme and assigning a full-time Registered Nurse in coordinating
and administrating the programme from the unit may increase the workload of the
current staffs, the cost-effectiveness of the programme must be evaluated.

27
The clerical staff in the target setting will be assigned to help the programme for a
half-day on Saturday without interfering the working time and nature. Thus, the
influence on implementing the programme on current staff function are minimal.
3.1.3.3 Administrative support
Being a teaching hospital for local universities, the setting provides a research
ground for healthcare professionals. The Department Head of the target unit
consistently emphasizes the mission of the department is to conduct clinical research
and transform the discoveries into innovative techniques and procedures, and bring
them to benefit patients. The Division Head of the breast surgery is also open for both
translational and clinical research in the area of breast cancer (Department of Surgery,
2014). The Department Operation Manager and Ward Manager are open-minded to
promote and implement new practices on enhancing service quality. This shows that
adequate support could be granted from the administrative level.
3.1.3.4 Consensus with other healthcare professionals
In the preparation phase, the programme coordinator will invite the surgeon,
breast nurse and physiotherapist to give vulnerable advice in planning the content of
the Home-based exercise programme. Holding communication meeting in addressing

28
the concern of different parties could promote multidisciplinary collaboration.
3.1.3.5 Staff development & resources needed
Most of the nurses in the target units are degree holders. The chosen programme
coordinator should be experienced and equipped with specialty and postgraduate
qualification in breast and surgical nursing. Additional trainings on staff mainly focus
on familiarizing the steps of the proposed exercise and programme, communication
skills and evaluation skills.
Apart from staffing, the venue, education materials and evaluation equipment are
needed in implementing the innovation. The multipurpose room could be utilized for
implementing the programme. The room is spacious enough for both group and
individual education session, exercise and return demonstration, which also equipped
with a CMS system accessible computer, projector and chairs facilitating education
and documentation. Education materials including PowerPoint, video and pamphlets
will be prepared in the preparation phase. For evaluation, equipment such as
measuring tape and goniometer for lymphoedema measurement are needed.
Measuring tape is available in the setting and the goniometer would be purchased to
place in the room.

29
3.1.3.6 Available evaluation tools
Evaluation plays a significant role in effective implementation, continuous
improvement and allocation of resources. For the outcomes evaluation, the
circumferential measurement used in the selected studies is easy, appropriate and
sensitive in determining the incidence of lymphoedema. The goniometer is widely
known as a standard tool in measuring the range-of-motion. The Function Assessment
of Cancer Therapy- Breast (FACT-B+4), which includes four specific questions on
evaluating arm symptoms will be used for assessing the quality of life (Singh, Vera &
Campbell, 2013). All the evaluation tools used are readily available.
3.1.4 Cost-benefit ratio of the innovation
3.1.4.1 Possible risks and benefits
In patient aspect
Exercise is widely recognized as a safe practice and has significant benefits to
health. Home-based exercise is of relatively low risk to patients compared with other
invasive or pharmacological interventions. The exercise educated in the programme
are of low intensity and proved to be safe and effective in preventing lymphoedema
from the integrated review. The programme is of low and insignificant risk of injury,
pain and formation of seroma (Wintage, 1985; Singh, Vera & Campbell, 2013). To

30
further minimize the risk, clear instructions and guideline for exercise will be given,
every exercise will be instructed with return demonstration and follow-up sessions
will be given in monitoring the progress.
According to the reviewed studies, the implementation of the HBEP reduced the
incidence of lymphoedema by 2.6 to 3.9 times (Kilbreath et al, 2013; Box et al., 2002;
Scaffidi et al., 2012; Singh, Vera & Campbell, 2013). Breast cancer related
lymphoedema causing chronic and incurable suffering from pain and swelling,
reducing patients’ physical mobility, affecting their self-caring ability and altering
self-image hence reducing their quality-of-life. The implementation of programme
prevents patients from long-term suffering and hence promotes health.
In staff and institution aspect
The low participation rate and exercise adherence rate of the current practice
indicated that providing an hour of physiotherapy session solely after operation could
not prevent patients from BCRL effectively. Increasing number of breast cancer
patients developing lymphoedema will increase the workload of staffs and cause a
huge financial burden on especially the institution.
On the contrary, implementing the innovation could bring various benefits to both
the staffing and institution. For the staff, nurses could empower themselves and

31
promote professionalism through implementing the nurse-led programme, hence
increasing staff morale and job satisfaction. For institutes, the innovation could reduce
medical cost for managing patients with lymphoedema and the increase of service
quality could bring good reputation to the hospital.
3.1.4.2 Cost
The total cost of implementing the Home-based exercise programme in serving 55
patients will be approximately HKD$233,286. The details were illustrated in
Appendix 5. The cost is estimated in terms of manpower, training and materials cost.
In this programme, the manpower cost are mainly considered as the time for staffs to
prepare the materials, coordinate and implement the programme.
The target setting provides a free venue and equipment including computers,
stationary and projector for meetings, trainings and programme implementation.
Therefore, the material cost for implementing the programme are mainly the printing
cost for education materials, log books and documents and the production cost for
education video and goniometer (tool for evaluation).
If the Home-based exercise programme is not implemented, around 30 patients
may develop lymphoedema in the 12 months period by estimation. Most of them
readmitted in every four to five months and the average length-of-stay is seven days.

32
The estimated total cost for the management of lymphoedema is HKD$3,823,290,
which is 16 times much higher than the cost of implementing the innovation. The
details were provided in Appendix 6.
The programme could effectively reduce the overall medical expenses of the
institution. Together with the non-material cost of improving patients’ quality of life
by preventing the disease and enhancing staff morale by advocating nursing
professionalism, it is worth to implement the programme in the target setting.
In summary, the potential benefits on patients, nurses and institutions outweigh
the risk of implementation. The Home-based exercise programme is transferable to
the target audience and feasible to implement in the target setting.
3.2 Evidence-based practice guideline/protocol
Developing an evidence-based guideline for the innovation is essential for guiding
quality, safe and consistent nursing practice. The evidence-based guideline for the
Home-based exercise programme in preventing breast cancer related lymphoedema
was attached in Appendix 7.
The recommendations from the selected reviews were extracted and graded
according to The Scottish Intercollegiate Guideline Network (SIGN) guideline in
relation to the strength of the available evidence (SIGN, 2011).

33
Chapter 4
Implementation plan
4.1 Communication plan with potential users
The implementation assessment in previous chapter supported the new practice of
Home-based exercise programme (HBEP) and thus an evidence-based guideline was
developed. The next crucial steps are to initiate and facilitate the adoption of
innovation by developing a concrete and effective communication plan (Stetler, 2001;
Schmidt & Brown, 2008). Rogers’ model on Diffusion of Innovation was adopted in
developing the plan in light of its effectiveness in facilitating the practice of an
innovation (Rogers, 2003).
4.1.1 Identification of stakeholders
According to the model of Diffusion of Innovation, communicating with members
of a social system is a key element towards success (Rogers, 2003). Members of the
social system are those influencing and being affected by the new practice, including
the administrators, opinion leaders, operators and users (Lobiondo-wood & Haber,
2002; Rogers, 2003).
Administrators stand on a highly influential position in the system, which exert
either positive or negative influence on the implementation (Lobiondo-wood & Haber,

34
2002). In this setting, the Chief of Service (COS), the Division Chief of Breast
Surgery, the Department Operations Manager of Surgery (DOM) and the Ward
Manager (WM) are considered as the administrators. They are at an upper level that
possesses the authority power to approve the adoption of a new practice and provide
financial support to set-up and operate an innovation, while the Ward Manager, in
addition, is responsible for daily operations in ward and duty arrangement of staff.
Opinion leaders are also a key member within the social systems, who plays a
significant role in providing expert opinions and advice about the practice (Rogers,
2003; Lobiondo-wood & Haber, 2002). In the breast unit, the surgeons, the Advanced
Practice Nurse (Breast specialist) and the physiotherapists are identified as the
opinion leaders. They are specialists in the concerned area, technically competent and
experienced to evaluate the proposed innovation and provide practical feedbacks. The
Breast specialist, who is in additionally work as a partner with the development team
in planning, implementing and monitoring the programme as well as communicating
the innovation to administrators and frontline staffers. With the support of the opinion
leaders, an active adoption of the practice can be led, posing a positive influence on
the implementation.
The mostly affected members in the system are the operators and users (Schmidt
& Brown, 2008; Lobiondo-wood & Haber, 2002). Operators of the programme are the

35
Breast Specialist, co-ordinating nurse and all Registered Nurses in the breast unit,
who frequently contact patients for promoting and implementing the programme. On
the other side of the coin, nurses who are reluctant to change, or who perceive that the
innovation would increase their workload may lead an active opposition and
contribute to negative outcome.
Users of the innovation are patients with breast cancers. The HBEP is carried out
to prevent breast cancer-related lymphoedema. Patients’ understanding and perception
on the innovation would affect the participation and adherence to the programme
(Kilgour, Jones & Keyserlingk, 2008).
4.1.2 Communication process
Effective communication with every member in the systems could enhance mutual
understanding and co-operation in adopting a new practice (Lobiondo-wood & Haber,
2002; Rogers, 2003). The entire communication process is a very social process and
the strategies are again based on Roger’s model of Diffusion of Innovations.
Homophilous communication is the most effective strategy for initiating
information exchange, which is the sharing of ideas between individuals with similar
beliefs and interests (Rogers, 2003). To begin with, the co-ordinating nurse will
introduce the benefits, cost-effectiveness and feasibility of the new practice to the

36
Breast Specialist (APN) and surgeons informally. These opinion leaders share the
same visions and interests with the co-ordinating nurse in providing quality breast
services to patients, who are most likely to be convinced and are also able to provide
expert opinion on the innovation. Thereafter, the co-ordinating nurse will share the
ideas with the Ward Manager in an informal meeting. By valuing the innovation,
providing operational feedbacks and supports on the new practice, he is an essential
stakeholder in marking the program a reality for the unit.
With initial support from the opinion leaders and WM, the co-ordinator will work
with the Breast Specialist to develop a detailed proposal comprising the reviewed
evidence, implementation potentials and proposed guidelines of the HBEP with
tentative timeline and a concise implementation plan to seek administrative approval.
The proposal will be illustrated clearly with PowerPoint presentation with tables in a
formal meeting to the COS, Division Chief of Breast surgery, DOM and WM in
addressing their concerns. The necessity for adoption, significances, cost and benefits
of the programme will be emphasized in gaining their support.
Upon approval from the administrative level, the co-ordinating nurse will
integrate various expert opinions in planning the programme, preparing the necessary
materials for operation and then begin to communicate with the frontline staff.
Frontline staffers are potential operators involved in giving advice and education on
37
HBEP to patients during hospitalization. Knowledge and persuasion are essential to
them for adopting an innovation (Rogers, 2003). Holding semi-formal ward meetings
to share the reviewed evidence, significance and details of the new practice among
peers with printouts could enhance their understanding and interest. Performing
further persuasion actions such as emphasizing the benefits of HBEP on patients,
answering individual’s concerns and clarifying uncertainties could promote their
support to the adoption of new practice.
This communication and preparation process may take approximately three
months. By getting into the implementation phase, the co-ordinating nurse will
perform interval process evaluation in the first and every four months for monitoring.
The comments and information are valuable and practical in guiding the revision of
the guideline. Throughout the whole preparation and implementation period, every
members of the system will be kept abreast of the progress of the HBEP via internal
email bi-monthly.
4.2 Pilot study plan
Piloting an innovation has positive influence on adoption of new practice for
testing its feasibility and the acceptability among staffs and patients (Lobiondo-wood
& Haber, 2002; Rogers, 2003). Before actual implementation, piloting the HBEP for

38
two months in the unit aimed at identifying unexpected difficulties, reviewing the
logistics and feasibility of the programme and hence modifying the guideline when
necessary. Several aspects including the patient recruitment strategies, implementation
process, evaluation methods and outcomes will be reviewed.
4.2.1 Patient recruitment strategies
Potential participants were screened from the scheduled lists of operation by the
co-ordinating nurse and being informed of the study during their pre-operative
assessment visit. Physicians are advised to encourage patients to participate in the
HBEP actively. Patients who fulfilled inclusion and exclusion criteria of the
programme and provided informed consent will be recruited in the pilot scheme. Five
cases are expected to be recruited in two weeks. The co-ordinating nurse will record
the number of cases approached, number of cases successfully recruited and barriers
encountered for process evaluation.
4.2.2 Intervention evaluation
The proposed HBEP comprising preoperative education, postoperative skills
revision and pre-discharge education as well as follow-ups in monitoring the progress.
Additional guides including pamphlet, CD and logbook will be given for references

39
and record. Ward nurses are mainly responsible for skills revision and education to
hospitalized patients.
Pilot test is necessary to identify flaws and problems during implementation
process (LoBiondo-Wood & Haber, 2002). In evaluating the workflow, the
co-ordinating nurse will hold a focus group with frontline staff in the week after
implementation to identify problems encountered, collect feedbacks and evaluate
staff’s perception and satisfaction towards the practice.
After piloting the HBEP, the co-ordinating nurse will conduct unstructured
interviews with individual participants in reviewing the appropriateness of the venue,
timing, the quality of education sessions and materials as well as their perception and
satisfaction on the programme.
4.2.3 Outcome measurements
All measurements will be undertaken by the co-ordinator and Breast nurse. The
study outcomes will be measured on the day before operation (baseline), at a week
and three weeks after the operation to determine the short-term effect of the practice
and most importantly to test the appropriateness of the data-collection tools and
workflow. Patients’ outcomes include measuring the limb circumference by tape, the
shoulder range-of-motion (ROM) by goniometer and assessing the psychosocial
40
aspects with questionnaire (FACT-B+4). Apart from monitoring the patient outcomes
and their safety, logistics workflow for outcome measurement including the feasibility
of using these evaluation methods in the setting, the accuracy and time spent are
examined.
In summary, by reviewing the recruitment strategies, outcome measurement and
integrating both patients and staffs’ opinions on the workflow in the pilot, the
co-ordinator could make further improvements and modifications on the guideline and
logistics arrangement for a better programme.
4.3 Evaluation plan
Evaluation plays a significant role in health programmes for effective planning,
continuous improvement and appropriate resource allocation (Lobiondo-wood &
Haber, 2002). It is vital to evaluate the quality and effectiveness of an innovation,
hence provides objective information necessary to ensure its sustainability. The
outcomes measure to be evaluated are identified as patient outcomes, staff outcomes
and system outcomes.
4.3.1 Patient outcomes
Previous research synthesis demonstrated that HBEP effectively reduces the
41
incidence of lymphoedema, thus the primary patient outcome for innovation efficacy
is the incidence of lymphoedema. The presence of lymphoedema will be identified
using non-invasively measurement on arm size. By using circumferential tape,
measurements will be taken with both arms supported on a flat surface at six points
(mid-point of the third metacarpophalangeal joint, the ulnar styloid process and at 10,
20, 30 and 40cm proximal from the ulnar styloid process). An increase of 2cm or
more and >10% comparing to the unoperated arm at any of the six measurement
points indicate lymphoedema (Kilbreath et al., 2013; Singh, Vera & Campbell, 2013;
Cinar et al., 2008; Box et al., 2002).
Secondary patient outcomes are the shoulder range of motion (ROM) and quality
of life (QOL). Shoulder ROM (flexion, abduction and external rotation) will be
assessed using a universal goniometer in a sitting position. According to the reviewed
studies, HBEP significantly improves shoulder ROM and takes effect in short term
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Cinar et
al., 2008; Kilgour, Jones & Keyserlingk, 2008). This outcome is a vital motivator to
positively reinforce patients the adherence of daily HBE.
Patient’ QOL will be evaluated using the Functional Assessment of Cancer
Therapy- Breast questionnaire with for additional questions on arm symptoms
(FACT-B+4). It has a high sensitivity and specificity in assessing outcome in patients

42
with lymphoedema and breast cancer, thus showing excellent statistically and
clinically reliable result (Singh, Vera & Campell, 2013; Todd et al., 2008).
4.3.2 Staff outcomes
Nurses are key persons to conduct the innovation, therefore the staff outcomes are
an equally important part of the evaluation. The satisfaction and confidence level of
nurses in operating the program will be assessed after training and programme
implementation using self-reviewing questionnaire and focus group discussion to
evaluate the effectiveness of training sessions and identify barriers and difficulties in
the operating process for process evaluation.
4.3.3 System Outcome
System outcomes measure the system effectiveness through assessing patients’
adherence to the program, adverse events encountered and costs. Patients’ adherence
reflect the efficacy of proposed guideline and will be assessed using logbook and in
follow-ups. Any adverse events encountered in carrying out the program should be
carefully considered to ensure the safety and effectiveness of practice by continuously
monitoring in every follow-ups and self-reports from participants. The operational
cost will be reviewed and monitored in every four months for regular financial reports

43
to the administrators.
4.3.4 Nature and number of clients
In line with the reviewed literatures, pilot and proposed clinical guideline in
previous chapters, the nature of clients in actual implementation are women aged 18
to 80 years old who had scheduled for breast cancer surgery and will admit to the
target breast unit without any underlying shoulder problems, existing lymphoedema
and physical, cognitive and neurological deficits.
With reference to the study of Kilbreath et al. (2013), the standard deviation for
change in arm circumference at 9 months after surgery was 4. The sample size
estimated by an online computer program is approximately 44 (Lenth, 2006-9). This
will give 90% power to detect a different of 2cm for arm circumference with a
significance level of 5% for a two-tailed t-test. Allowing an attrition rate of 20% due
to mortality and loss to follow-up on especially a 12 months program, the actual
number of samples required for evaluation is 55.
In the target unit, the average admission rate of patient undergo breast cancer
surgery is approximately 12 patients in each month. Therefore, the proposed period
for patient recruitment in actual implementation is five months. The minimum
available number of potential cases should be 60.

44
4.3.5 Data collection
All measurements will be collected by the co-ordinating nurse and Breast Nurse.
Based on the table of evidence, the recommended duration for functional and physical
outcomes to take effect was 3 weeks (shoulder ROM) to 18 months (QOL) and 6
months to a year (Incidence of lymphoedema) respectively. In this study, variables
will be measured on the day before operation as baseline, at 3 weeks, 6 months and 12
months after operation to determine the short, intermediate and long term effect of the
innovation. Demographic data of patients will be obtained from patients’ medical
records and collected at the baseline assessment.
4.3.6 Data analysis
For a longitudinal study with four time-points, the data will be analyzed for the
short term, intermediate and long term effect. For the primary outcome measure, the
change from baseline and unoperated arm for arm circumference will be determined
to indicate a reduction in the incidence of lymphoedema. The mean change will be
compared by two-tailed paired t-test.
For measure of shoulder ROM, the data will be analyzed in the same way as the
primary outcomes to determine if the ROM is improved. For quality of life score, the
mean change from baseline will be compared with different time-points using

45
two-tailed paired t-test to test if the score is increased.
For other aspects of staff and system outcomes, data will be collected using
qualitative method of unstructured interviews and self-reviewing questionnaire, then
followed by coding the data into categories and theme for further analysis and
interpretation.
4.3.7 Basis for practice effectiveness
The innovation is regarded as effective only if the patient outcomes, staff
outcomes and system outcomes fulfill the bases that synthesized from the reviewed
studies. For primary patient outcome, the programme is considered as effective with a
significant reduction on the incidence of lymphoedema by 30%. Such criteria is in
line with the literatures that HBEP reduced the risk of lymphoedema by three times
(Kilbreath et al., 2013; Box et al., 2002; Scaffidi et al., 2012; Singh, Vera & Campbell,
2013). For secondary outcomes, the targets are achieving improvement in shoulder
ROM by more than 10 degree and QOL score with FACT-B+4 by 2 points.
With respect to the staff outcomes, the objectives are over 80% of nurses show
positive satisfaction and confidence in operating the practice, which can be identified
in both questionnaire and focus group.
For system outcomes, the target adherence rate to achieve is over 70% for

46
programme efficacy. Regarding the cost, the estimated operational cost for serving 55
patients in 24 months (12months for each patient) is HKD$148,161. The objective is
to keep reviewing and maintaining the cost below HKD$ 160,000.

47
Chapter 5
Conclusion
Based on the reviewed evidence, Home-based exercise programme is effective in
reducing the incidence of lymphoedema, improving shoulder range of motion and
quality of life of breast cancer patients following surgeries. No specific side effect
was indicated among the studies. Other than reducing medical expenses of institution,
the adoption of this innovation prevents patients from life-long sufferings and
conveniences of breast cancer-related lymphoedema. In view of its beneficial effects
on patients and institution, an evidence-based guideline, the implementation and
evaluation plan of HBEP was developed to facilitate the adoption of practice in the
unit. It is hoped that the evidence-based guideline of HBEP could be useful in guiding
safe and consistence nursing practice.

48
Appendix 1 – Search history
PubMed
CINAHL Plus Cochrane Library
(Trials) ProQuest
I I I I
By keyword search:
1. breast cancer OR breast tumor OR breast neoplasm OR breast carcinoma OR breast malignancy
2. breast surgery OR mastectomy OR lumpectomy OR lymph node dissection
3. Lymphedema OR swelling OR edema OR edematous OR arm circumference OR limb circumference
4. exercise OR physical activity OR physical therapy OR physiotherapy OR training OR breathing
OR rehabilitation OR aerobic OR stretching OR weightlifting OR weight bearing OR flexibility
OR resistance
I I
I
PubMed
899 articles
CINAHL Plus
260 articles
ProQuest
33601 articles
I I I
Limits (English
clinical trials,
humans)
Limits (English,
academic journals)
Cochrane Library
138 articles
Limits (Clinical trial,
controlled clinical trial,
RCT, English; excluded
news, review and study
on men & age >80)
I I I
PubMed
145 articles
CINHAL Plus
142 articles
ProQuest
170 articles
I I I
Reviewed by titles and abstracts
I I I I
PubMed
16 articles
CINHAL PLUS
13 articles
(8 articles from
google scholar)
Cochrane Library
23 articles
ProQuest
4 articles
I I I I
Reviewed by full paper
I I I I
PubMed
4 articles
CINHAL PLUS
5 articles
Cochrane Library
6 articles
ProQuest
2 articles
I I I I
Total checklist for review after elimination of duplication: 7 + 1 (from reference list) = 8_

49
Appendix 2 - Table of evidence (Citation 1-3)
1. BCRL = Breast Cancer-related lymphedema; SM= Simple mastectomy; MRM = Modified radical mastectomy; AD = Axillary dissection; BCS = Breast Conserving Surgery
2. IG= Intervention group; CG= Control group; HBE= Home-based exercise; LE= lymphoedema; ROM = Range-of-motion
3. aRR= adjusted risk ratio of CG: IG, UL function = Upper limb function
4. Values given as differences in means (intervention/control-baseline); ∆Gp = Between group difference (intervention-control)
Citation Study type/
Evidence Populations1 Samples & Design2
Length of
follow-up Outcome measures3 Effect size4
1.
Kilbreath
et
al.,(2013)
RCT-
(multi-cente
r)
(1+)
N = 160
Mean age: 53
Women
underwent AD
within 6 weeks
IG: n= 81
1. Advice on daily HBE + UC
(resistance & stretching)
2. 8 FUs monitor HBE
CG: n= 79
1. Written info: post-op Ex &
prevent LE;
2. In patient: Assisted stretch
Post op
1, 3, 9 &
15 month
Primary:
(1) Incidence of LE (aRR)
(1) At 3 month: 2.6 (p<0.02;
95% CI 0.9-7.4)
2. Singh,
Vera &
Campbell,
(2013)
Quasi
experiment
– not
randomized
(2+)
N=72
Mean age: 60
Women scheduled
for MRM/ SM/
BCS
IG: n=41
1. Post op D1-7: Breathing,
stretching, ROM Ex
2. After D7: Shoulder Ex
3. HBE+ UC
CG: n-31 1. Pre-op management:
Exercise, LE & scar
Pre-op,
post op 7
month
Primary:
(1) Incidence of LE (%)
(2) Shoulder ROM
(degree)
Secondary:
(3) QOL (FACT-B+4
score)
(4) Post-op Pain (VAS)
(5) UL function (DASH
score)
(1) IG: 2.5; CG: 9.7(p=0.19)
(2) Flexion IG: +0.63; CG:-6.06(p=0.03)
(3) IG:+1.9; CG:-1.4(p=0.43)
(4) IG:+7.5; CG:+8.5(p=0.74)
(5) Not significant
3. Scaffidi
et al.,
(2012)
Quasi
experiment
– not
randomized
(2+)
N= 83
Mean age: 51
Women scheduled
for (lumpectomy/
SM +/- AD)
IG: n=58
1. Written info: post-op S/E
2. Post op: Deep breathing,
stretching exercise
3. Instruct +FU HBE
CG: n=25
1. Verbal info. on post-op S/E
Pre-op,
post-op
Day 60,
180
Primary:
(1) Incidence of LE (%)
(2) Arm ROM (%)
Secondary:
(3) UL function (Constant
& Murley score)
At 180-day
(1) IG: 5.2 ; CG: 20 (p=0.036)
(2) IG: -12 ; CG: -44 (p=0.001)
(3) IG: 92.3;CG:79.8(p=0.001)
50
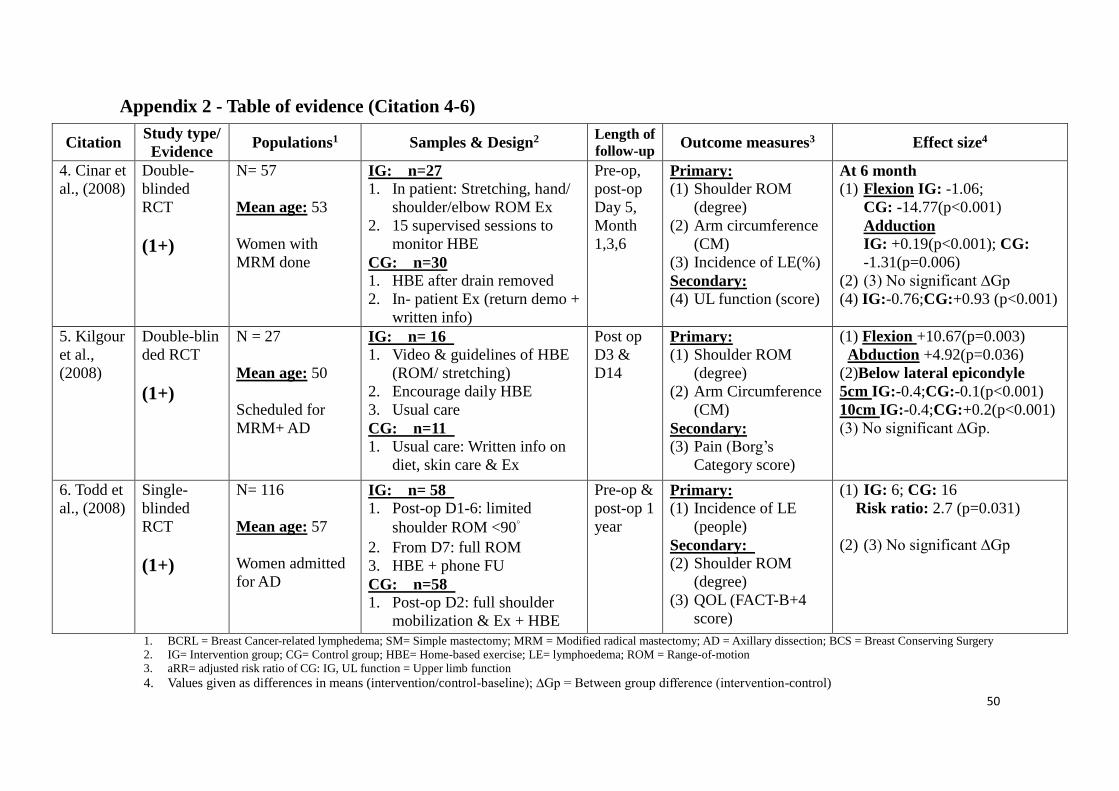
Appendix 2 - Table of evidence (Citation 4-6)
1. BCRL = Breast Cancer-related lymphedema; SM= Simple mastectomy; MRM = Modified radical mastectomy; AD = Axillary dissection; BCS = Breast Conserving Surgery
2. IG= Intervention group; CG= Control group; HBE= Home-based exercise; LE= lymphoedema; ROM = Range-of-motion
3. aRR= adjusted risk ratio of CG: IG, UL function = Upper limb function
4. Values given as differences in means (intervention/control-baseline); ∆Gp = Between group difference (intervention-control)
Citation Study type/
Evidence Populations1 Samples & Design2
Length of
follow-up Outcome measures3 Effect size4
4. Cinar et
al., (2008)
Double-
blinded
RCT
(1+)
N= 57
Mean age: 53
Women with
MRM done
IG: n=27 1. In patient: Stretching, hand/
shoulder/elbow ROM Ex
2. 15 supervised sessions to
monitor HBE
CG: n=30
1. HBE after drain removed
2. In- patient Ex (return demo +
written info)
Pre-op,
post-op
Day 5,
Month
1,3,6
Primary:
(1) Shoulder ROM
(degree)
(2) Arm circumference
(CM)
(3) Incidence of LE(%)
Secondary:
(4) UL function (score)
At 6 month
(1) Flexion IG: -1.06;
CG: -14.77(p<0.001)
Adduction
IG: +0.19(p<0.001); CG:
-1.31(p=0.006)
(2) (3) No significant ∆Gp
(4) IG:-0.76;CG:+0.93 (p<0.001)
5. Kilgour
et al.,
(2008)
Double-blin
ded RCT
(1+)
N = 27
Mean age: 50
Scheduled for
MRM+ AD
IG: n= 16
1. Video & guidelines of HBE
(ROM/ stretching)
2. Encourage daily HBE
3. Usual care
CG: n=11
1. Usual care: Written info on
diet, skin care & Ex
Post op
D3 &
D14
Primary:
(1) Shoulder ROM
(degree)
(2) Arm Circumference
(CM)
Secondary: (3) Pain (Borg’s
Category score)
(1) Flexion +10.67(p=0.003)
Abduction +4.92(p=0.036)
(2)Below lateral epicondyle
5cm IG:-0.4;CG:-0.1(p<0.001)
10cm IG:-0.4;CG:+0.2(p<0.001)
(3) No significant ∆Gp.
6. Todd et
al., (2008)
Single-
blinded
RCT
(1+)
N= 116
Mean age: 57
Women admitted
for AD
IG: n= 58
1. Post-op D1-6: limited
shoulder ROM <90˚ 2. From D7: full ROM
3. HBE + phone FU
CG: n=58
1. Post-op D2: full shoulder
mobilization & Ex + HBE
Pre-op &
post-op 1
year
Primary:
(1) Incidence of LE
(people)
Secondary:
(2) Shoulder ROM
(degree)
(3) QOL (FACT-B+4
score)
(1) IG: 6; CG: 16
Risk ratio: 2.7 (p=0.031)
(2) (3) No significant ∆Gp

51
Appendix 2 - Table of evidence (Citation 7-8)
1. BCRL = Breast Cancer-related lymphedema; SM= Simple mastectomy; MRM = Modified radical mastectomy; AD = Axillary dissection; BCS = Breast Conserving Surgery
2. IG= Intervention group; CG= Control group; HBE= Home-based exercise; LE= lymphoedema; ROM = Range-of-motion
3. aRR= adjusted risk ratio of CG: IG, UL function = Upper limb function
4. Values given as differences in means (intervention/control-baseline); ∆Gp = Between group difference (intervention-control)
Citation Study type/
Evidence Populations1 Samples & Design2
Length of
follow-up Outcome measures Effect size3
7. Box et
al., (2002)
Single-
blinded RCT
(1+)
N= 65
Mean age: 56
Women
scheduled for
(Local
excision
/MRM+ AD)
IG: n=32
1. Pre-op: Introduce LE/
HBE
2. Post-op: ROM Ex
3. Encourage HBE+UC+FU
CG: n=33
1. Usual care: Pamphlet
ofexercise
Pre-op,
post-op
Day5,
Month
1,3,6,12 &
24
Primary:
(1) Incidence of LE(%)
At month 24
(1) IG: 11 (95%CI,
0.7-22.9)
CG: 30 (95%CI,
13.6-46.4)
8.
Wingate,
(1985)
Quasi
experiment
-not
randomized
(2-0)
N= 90
Mean age: 57.3
Women
scheduled for
MRM
IG: n=49
In patient post-op:
1. daily ROM/resistance Ex
2. Instruct hand and arm
care
3. HBE for 8 weeks
CG: n=41
No treatment
Post op
Day 5 &
month 3
Primary:
(1) Arm Circumference
(cm)
(2) Shoulder ROM
(degree)
At 3 month
(1) At olecranon +0.5
7.5cm proximal -0.9
15cm proximal +0.5
(significant,ANOVA)
(2) Abduction
+15.7 (p<0.001)
Flexion +16.3(p<0.001)

52
Appendix 3 - Appraisal checklist
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Kilbreath, S. L., Lee, M-J., Refshauge, K. M., Beith, J. M., Ward, L. C., Simpson, J. M. et al. (2013). Transient
swelling versus lymphoedema in the first year following surgery of breast cancer. Support Care Cancer. 21: 2207-2215
Guideline topic: Home-based exercise of breast cancer related
lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study
design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled
clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Yes No
Can’t say (Computer generated randomisation list)
1.3 An adequate concealment method is used
Yes No
Can’t say (Use sealed opaque
envelopes & by a third person )
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation Yes No
Can’t say (Did not mentioned
whether the subjects were
blinded or not)
1.5 The treatment and control groups are similar at the start of the trial Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say

53
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes No
Can’t say (With reliable tools)
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
12% (Low compliance/time commitment, loss contact)
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes No
Can’t say Does not apply
(Treatment group was coded)
1.1
0
Where the study is carried out at more than one site, results are
comparable for all sites
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that
the overall effect is due to the study intervention?
Yes.
(Power analysis was calculated with 80% power,
considered also 20% mortality and loss of contact.)
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and
the extent to which it answers your question and mention any areas of uncertainty raised above.
- The study showed that lymphedema in the first year is likely to be transient and HBE reduce the
risk of developing swelling.
- The data of the risk factors (e.g. HBE, chemotherapy) were presented in a risk ratio with 95%
Confident interval & p-value.
- Whether the subjects were blinded to the group allocation were not mentioned.

54
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Singh, C., Vera, M. D. & Campbell, K. L. (2013). The effect of prospective monitoring and early
physiotherapy intervention on arm morbidity following surgery for breast cancer: A pilot study.
Physiotherapy Canada. 65(2): 183-191
Guideline topic: Home-based exercise of breast
cancer related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
3. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt,
check the study design algorithm available from SIGN and make sure you have the
correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not
relevant, and the study cannot be rated higher than 1+
4. Is the paper relevant to key question? Analyse using PICO (Patient or Population
Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES
complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please
specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is
randomised.
Yes No
Can’t say (according
to site)
1.3 An adequate concealment method is used.
Yes No
Can’t say (Not
mentioned)
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say (Single
blinded-
subject)
1.5 The treatment and control groups are similar at the start of
the trial.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say

55
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (With reliable
tools)
1.8 What percentage of the individuals or clusters recruited into
each treatment arm of the study dropped out before the study
was completed?
1.4% (Not complete 7
months program)
1.9 All the subjects are analysed in the groups to which they
were randomly allocated (often referred to as intention to
treat analysis).
Yes No
Can’t say Does not
apply
(Removed for
analysis)
1.1
0
Where the study is carried out at more than one site, results
are comparable for all sites.
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical
considerations, your evaluation of the
methodology used, and the statistical
power of the study, are you certain that the
overall effect is due to the study
intervention?
Yes.
(Subjects were allocated according to the
site.
? Not randomised. T-test was used to prove
the statistical significant.)
2.3 Are the results of this study directly
applicable to the patient group targeted by
this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment
of the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
- The study showed that physiotherapy programme and follow up on HBE reduce
arm morbidity following breast cancer surgery.
- Small sample size, the therapist and investigators were not blinded to the group
allocation.
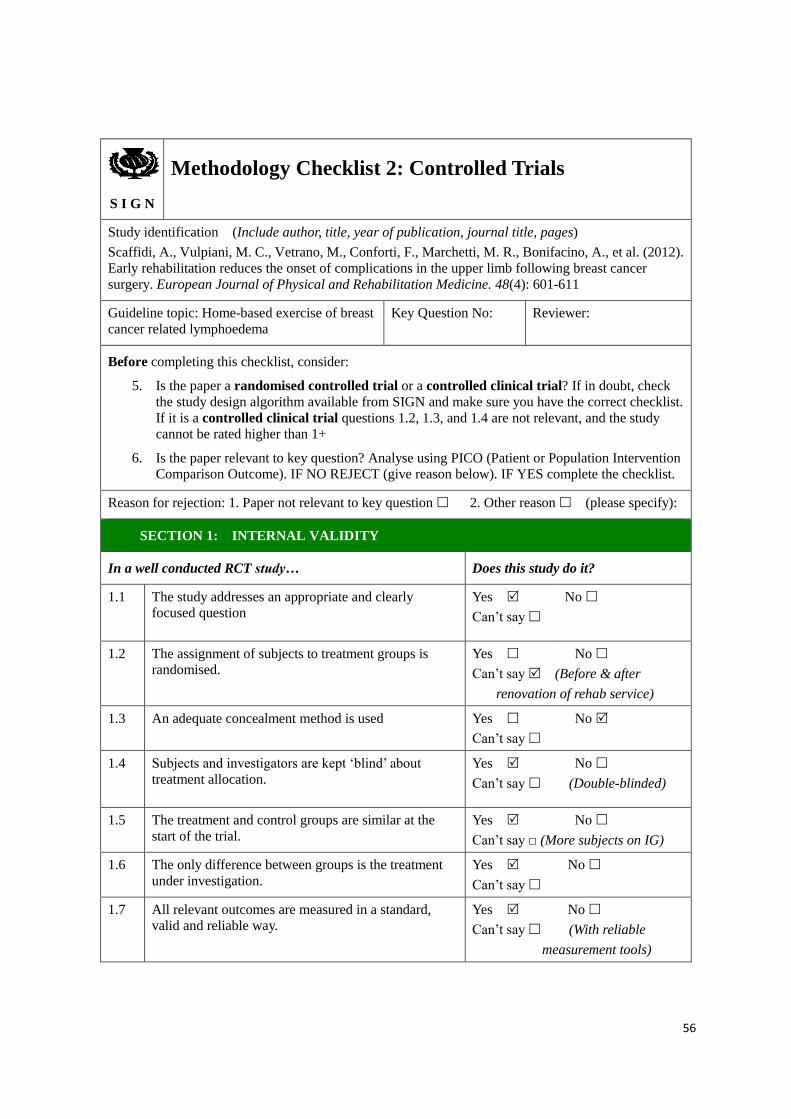
56
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Scaffidi, A., Vulpiani, M. C., Vetrano, M., Conforti, F., Marchetti, M. R., Bonifacino, A., et al. (2012).
Early rehabilitation reduces the onset of complications in the upper limb following breast cancer
surgery. European Journal of Physical and Rehabilitation Medicine. 48(4): 601-611
Guideline topic: Home-based exercise of breast
cancer related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
5. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check
the study design algorithm available from SIGN and make sure you have the correct checklist.
If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study
cannot be rated higher than 1+
6. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly
focused question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is
randomised.
Yes No
Can’t say (Before & after
renovation of rehab service)
1.3 An adequate concealment method is used
Yes No
Can’t say
1.4 Subjects and investigators are kept ‘blind’ about
treatment allocation.
Yes No
Can’t say (Double-blinded)
1.5 The treatment and control groups are similar at the
start of the trial.
Yes No
Can’t say □ (More subjects on IG)
1.6 The only difference between groups is the treatment
under investigation.
Yes No
Can’t say
1.7 All relevant outcomes are measured in a standard,
valid and reliable way.
Yes No
Can’t say (With reliable
measurement tools)

57
1.8 What percentage of the individuals or clusters
recruited into each treatment arm of the study dropped
out before the study was completed?
0% (Participants were excluded if
they were not fully adhere to the programme & FU.)
1.9 All the subjects are analysed in the groups to which
they were randomly allocated (often referred to as
intention to treat analysis).
Yes No
Can’t say Does not apply
1.10 Where the study is carried out at more than one site,
results are comparable for all sites
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to
minimise bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical
considerations, your evaluation of the
methodology used, and the statistical
power of the study, are you certain
that the overall effect is due to the
study intervention?
Yes. (Two treatment groups are Mann-Whitney was used to calculate the statistical significance.)
2.3 Are the results of this study directly
applicable to the patient group
targeted by this guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the
study, and the extent to which it answers your question and mention any areas of uncertainty
raised above.
- The study showed that rehabilitation programme that included HBE and in-patient
education following breast cancer surgery reduce the incidence of postoperative
side-effects, including lymphoedema.
- Participants enrolled in two period were then enrolled in two groups. No external
force influencing the allocation except the time they enrolled in the study.
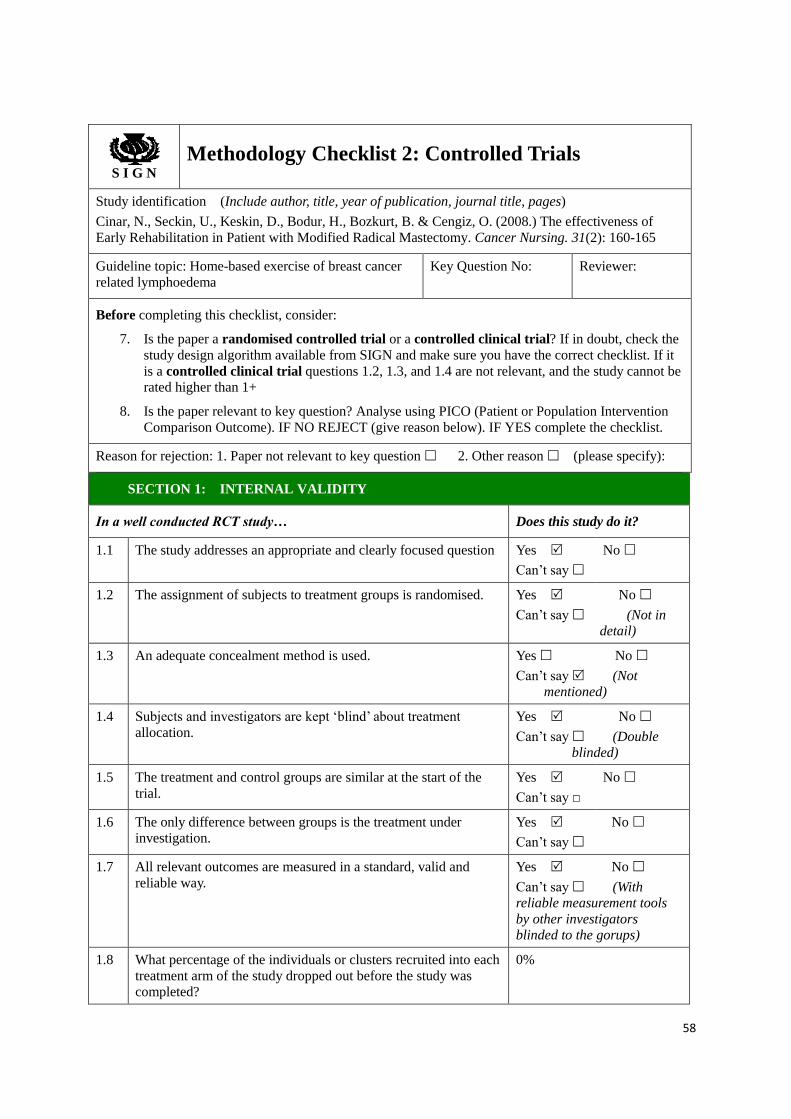
58
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Cinar, N., Seckin, U., Keskin, D., Bodur, H., Bozkurt, B. & Cengiz, O. (2008.) The effectiveness of
Early Rehabilitation in Patient with Modified Radical Mastectomy. Cancer Nursing. 31(2): 160-165
Guideline topic: Home-based exercise of breast cancer
related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
7. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it
is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be
rated higher than 1+
8. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Yes No
Can’t say (Not in
detail)
1.3 An adequate concealment method is used.
Yes No
Can’t say (Not mentioned)
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say (Double blinded)
1.5 The treatment and control groups are similar at the start of the
trial.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (With reliable measurement tools
by other investigators blinded to the gorups)
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
0%

59
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
Yes No
Can’t say Does not
apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations,
your evaluation of the methodology used, and
the statistical power of the study, are you
certain that the overall effect is due to the
study intervention?
Yes. (The randomisation and concealment
method were not clearly stated. T-test was used to calculate the significance of the study.)
2.3 Are the results of this study directly applicable
to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the
study, and the extent to which it answers your question and mention any areas of uncertainty
raised above.
- The study showed that early assisted rehabilitation programme improve shoulder
mobility after modified radical mastectomy.
- No significance different between the surprised exercise and HBE on the incidence of
lypmphoedema.

60
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Kilgour, R. D., Jones, D. H., & Keyserlingk, J. R. (2008). Effectiveness of a self-administered, home-based
exercise rehabilitation program for women following a modified radical mastectomy and axillary node
dissection: a preliminary study. Breast Cancer Research and Treatment. 109(2), 285-295.
Guideline topic: Home-based exercise of breast cancer
related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
9. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it is a
controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated
higher than 1+
10. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Yes No
Can’t say
(Computerized number list)
1.3 An adequate concealment method is used.
Yes No
Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say (Double
blinded, patients & therapists)
1.5 The treatment and control groups are similar at the start of the
trial.
Yes
Can’t say □
No
(Shown in
table)
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say (The HBE
program)
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (All outcomes were
stated clearly and measured
with reliable tools by experienced therapist.)

61
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
0%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
Yes
Can’t say
No
Does not
apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations,
your evaluation of the methodology used, and
the statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
2.3 Are the results of this study directly applicable
to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study,
and the extent to which it answers your question and mention any areas of uncertainty raised above.
- The study showed that the early onset and self-administered HBE programme improve
shoulder mobility and lymphedema after breast surgery.
- The sample size of this study is small, but it’s targeted on a vulnerable group of
participants who underwent mastectomy and also axillary node dissection. Power analysis
could be calculated to enhance the power of the study.
- The adherence rate of the program decrease with time and the reasons were also estimated
for future study or programme implementation.

62
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Todd, J., Scally, A., Dodwell, D., Horgan, K. & Topping, A. (2008). A Randomised controlled trail of two
programmes of shoulder exercise following axillary node dissection for invasive breast cancer.
Physiotherapy, 94, 265-273
Guideline topic: Home-based exercise of breast cancer
related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
11. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it is a
controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated
higher than 1+
12. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Yes No
Can’t say (Random
number table)
1.3 An adequate concealment method is used.
Yes No
Can’t say (sealed envelope & by an
objective third person)
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say (Single
blinded)
1.5 The treatment and control groups are similar at the start of the trial. Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (With
reliable measurement tools & confirmed by other
investigators)
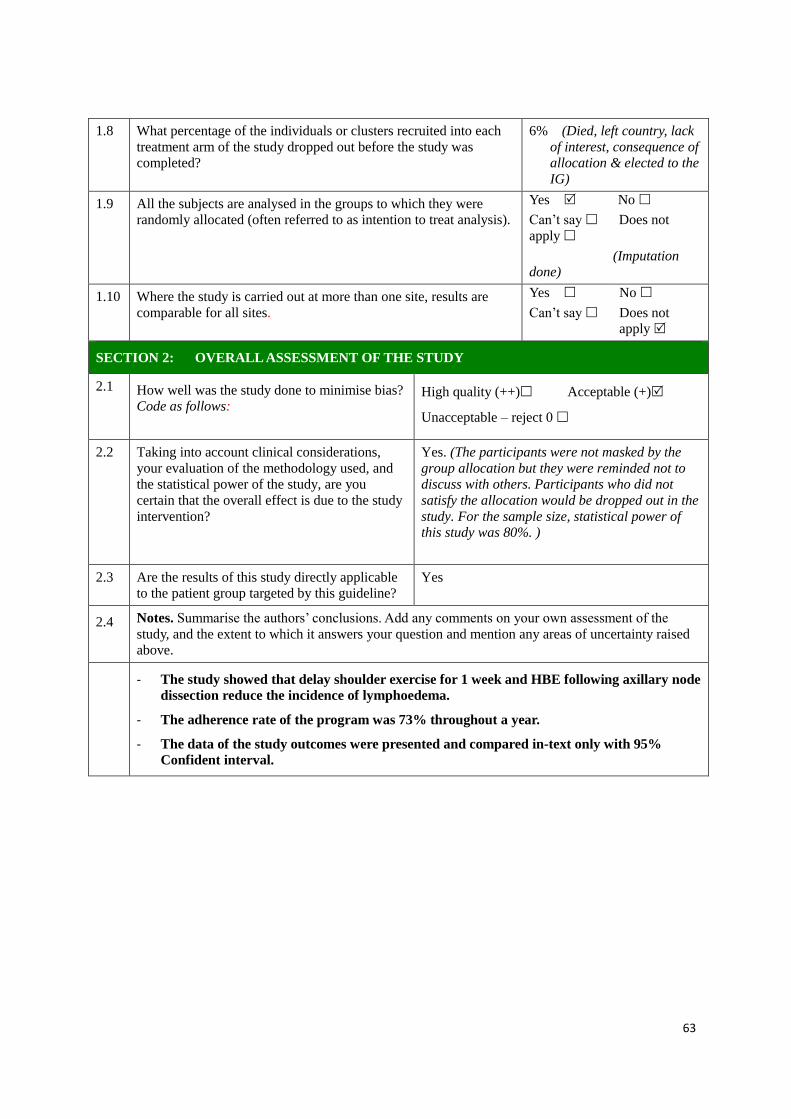
63
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
6% (Died, left country, lack
of interest, consequence of allocation & elected to the
IG)
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes No
Can’t say Does not
apply
(Imputation done)
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations,
your evaluation of the methodology used, and
the statistical power of the study, are you
certain that the overall effect is due to the study
intervention?
Yes. (The participants were not masked by the
group allocation but they were reminded not to discuss with others. Participants who did not
satisfy the allocation would be dropped out in the
study. For the sample size, statistical power of this study was 80%. )
2.3 Are the results of this study directly applicable
to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the
study, and the extent to which it answers your question and mention any areas of uncertainty raised
above.
- The study showed that delay shoulder exercise for 1 week and HBE following axillary node
dissection reduce the incidence of lymphoedema.
- The adherence rate of the program was 73% throughout a year.
- The data of the study outcomes were presented and compared in-text only with 95%
Confident interval.

64
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Box, R. C., Reul-Hirche, H. M., Bullock-Saxton, J. E., & Furnival, C. M. (2002). Physiotherapy after
breast cancer surgery: results of a randomised controlled study to minimise lymphoedema. Breast Cancer Research and Treatment. 75, 51-64.
Guideline topic: Home-based exercise of breast cancer
related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
13. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it
is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be
rated higher than 1+
14. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised. Yes
Can’t say
No
(Not in
detail)
1.3 An adequate concealment method is used.
Yes No
Can’t say (Not
mentioned)
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say
(Single blinded, taken remedial strategies to
minimize the bias.)
1.5 The treatment and control groups are similar at the start of the
trial.
Yes
Can’t say □
No
(Shown in
table)
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say
(The Exercise program)

65
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (with reliable measurement tools &
outcomes stated clearly)
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
9% (unavailable for review/ final assessment, death,
relocation, with subsequent
operation)
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
Yes
Can’t say
No
Does not
apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations,
your evaluation of the methodology used, and
the statistical power of the study, are you
certain that the overall effect is due to the
study intervention?
Yes.
(Although the sample size was small, the power
analysis was calculated to ensure the study with 90% power. Statistical power of the data were
clearly stated.)
2.3 Are the results of this study directly
applicable to the patient group targeted by this
guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the
study, and the extent to which it answers your question and mention any areas of uncertainty
raised above.
- The study showed that the physiotherapy intervention programme reduce the
development of secondary lymphoedema after breast surgery. The study was clinically
significant with 95% confident interval.
- The study included a structured exercise programme and followed for 24 months which
was a comparatively good study to examine the long term effect on the participants.
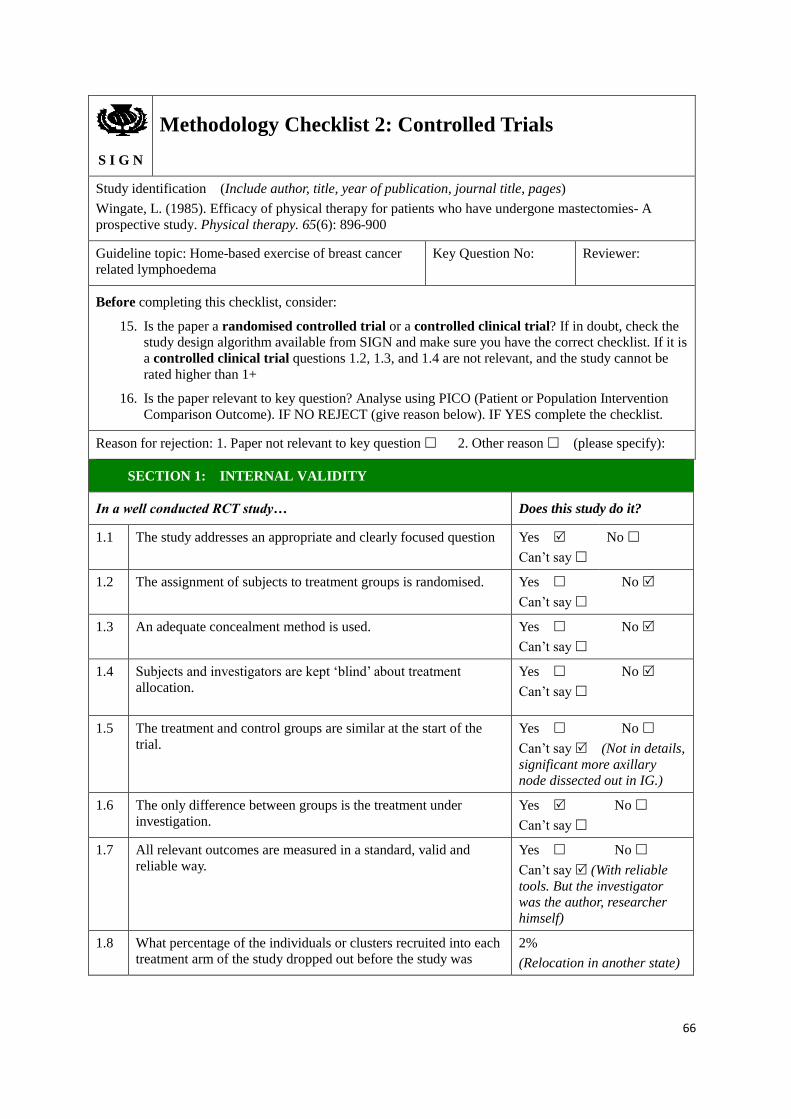
66
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Wingate, L. (1985). Efficacy of physical therapy for patients who have undergone mastectomies- A
prospective study. Physical therapy. 65(6): 896-900
Guideline topic: Home-based exercise of breast cancer
related lymphoedema
Key Question No: Reviewer:
Before completing this checklist, consider:
15. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it is
a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be
rated higher than 1+
16. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Yes No
Can’t say
1.3 An adequate concealment method is used.
Yes No
Can’t say
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes No
Can’t say
1.5 The treatment and control groups are similar at the start of the
trial.
Yes No
Can’t say (Not in details,
significant more axillary node dissected out in IG.)
1.6 The only difference between groups is the treatment under
investigation.
Yes No
Can’t say
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes No
Can’t say (With reliable
tools. But the investigator was the author, researcher
himself)
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
2%
(Relocation in another state)

67
completed?
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
Yes No
Can’t say Does not
apply
(Not mentioned)
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes
Can’t say
No
Does not
apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows
High quality (++) Acceptable (+)
Unacceptable – reject 0
2.2 Taking into account clinical considerations,
your evaluation of the methodology used, and
the statistical power of the study, are you
certain that the overall effect is due to the
study intervention?
Can’t say. (The study was designed, outcomes were measured and analysed by the author,
the same person. The data were analysed by t-test, chi-square test and ANOVA.)
2.3 Are the results of this study directly applicable
to the patient group targeted by this guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the
study, and the extent to which it answers your question and mention any areas of uncertainty
raised above.
- The study showed that physiotherapy enhance shoulder ROM on women underwent
mastectomies.
- No randomization, concealment, the outcomes were collected & analyzed by the author
himself.

68
Appendix 4 – Timeline of HBEP
Month Tasks 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Communication
meetings
Administrators
approval
Material preparation
Staff Training
Pilot - patient
recruitment (2 weeks)
Pilot test (5 weeks)
Pilot test- evaluation
Program amendment
Full implementation –
recruitment
Program
implementation
Interval program
evaluation
Whole program
evaluation

69
Appendix 5 – Estimated total cost of implementing HBEP (12 months for 55 patients)
Items Quantities
Cost/unit
(HKD)
Total cost
(HKD)
Set-up cost (For first 4 months)
Manpower cost
1 Experienced Registered Nurse
(RN as coordinator)
24hours/week
(Preparation)
$182/hour $69,888
1 Advanced Practice Nurse Breast
Nurse)
2 hours/week $260/hour $8,320
1 Clerical Staff 4 hours/ week $85/hour $5,440
Training Cost
Experienced Registered Nurse
(coordinator)
Communication course
Available in
hospital
/
2 hours training and
sharing session on
exercising
$182/hour $364
1 Breast Nurse $260/hour $520
1 Physiotherapist I $269/hour $538
Material Cost
Venue & stationary for training and meetings
Available in
hospital
/ Measuring tape for evaluation
Video marking – camera and software
Compact disc (CD) 5 sample disc $5/disc $25
Documents/pamphlets/ logbook/
handouts/ evaluation forms
Around 200 papers $0.15/A4paper $30
Total set-up cost: $85, 125

70
Operational cost (12 months, serving 55 patients)
Manpower Cost
Experienced Registered Nurse
Preparation/documentation 5hours/ week
$182/hour
$47,320
Education- Pre-op (group)/ Post-op
(individual)
4 hours/ week
(in first 6months)
$18,928
Face-to-face monitoring-
(Post-op 1 week & 2 week)
2times/15mins/
Patient
$5,005
Phone monitoring-
(Months 1-5; 7-11)
10 times/
10mins/patient
$16,683
Evaluation-
(Pre-op, Month 6 & 12)
3 times/
20mins/patient
$10,010
Program evaluation 10hours/week for last
2months
$14,560
1 Breast Nurse 4 hours/ month $260/hour $12,480
1 Clerical Staff 5 hours/ week $85/hour $22,100
Material Cost
Venue, computer, projector, stationary
Available
/
Evaluation tools- measure tape, tank /
Video CD 80 copies $5/disc $400
Pamphlets, handouts, log books &
evaluation forms
80 copies $0.15/A4 paper $600
Evaluation & Documents 500 papers $0.15/A4 paper $75
Total operation cost: $148,161

71
Appendix 6- Estimated total cost of not implementing HBEP for 12 months
(approximately 30 patients, readmitted for 4 episodes with 7 days each)
Items Quantities
Cost/unit
(HKD)
Total cost
(HKD)
Extra manpower cost (During hospitalization)
Daily limb Physiotherapy 20mins/day $153/hour $61,200
Occupational therapist for
pressure garment
3 hour/service $153/hour $13,770
Pain team consultation
(1 Doctor, 1 RN)
Once/admission
/ 30mins
$400/doctor/hour
+ $182/RN/hour
$34,920
Material Cost (During hospitalization)
Hospitalization cost 7days/ episode $4000/ day $3,360,000
Antibiotics (Injection/oral) 1course/episode $120/course $14,400
Dressing materials Daily $200/day $336,000
Pressure Garment once $100/piece $3000
Total cost for NOT implementing the HBEP: $3,823,290

72
Appendix 7 – Guideline of implementing Home-based exercise programme
(HBEP) for breast cancer patients
Aim and objectives
The aim of this guideline is to develop a clear and evidence-based protocol for guiding safe
and consistent nursing practice in implementing Home-based exercise programme on
prevention of breast cancer related lymphoedema among breast cancer patients.
The objectives of the guideline are:
1. To prevent lymphoedema among breast patients after breast cancer surgery
2. To assist nurses and healthcare professionals to deliver a safe Home-based exercise
programme
3. To summarize the evidence of the Home-based exercise programme
4. To standardize the content of the Home-based exercise programme
5. To promote quality holistic patient-based care for breast cancer patients
Target group
Target User:
This guideline is designed for nurses and other healthcare professionals on the care of
patients who scheduled for breast cancer surgery.
Target populations:
Women who are admitted to the unit and scheduled for breast cancer surgery.
Inclusion criteria
Women aged 18 to 80 years
Scheduled for breast cancer surgery

73
Exclusion criteria
Having underlying shoulder problems
Having existing lymphoedema
Having physical, cognitive and neurological deficit
Recommendations
Assessment & recruitment
1. All women after breast surgery are suggested to perform HBE. (Grade A)
Evidence: Findings from the reviewed studies supported that HBE is effective and
significant in preventing lymphoedema and improving shoulder range-of-motion.
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Kilgour et al.,
2008; Box et al., 2002) (1+; 2+; 2+; 1+; 1+)
2. Women underwent breast surgery having physical, cognitive and neurological deficit
should be excluded. (Grade B)
Evidence: Patients with these deficits may not able to engage in exercises and follow the
guideline (Kilbreath et al., 2013; Box et al., 2002) (1+; 1+)
3. Women with underlying shoulder problems (i.e. sustained fracture, previous shoulder or
upper limb surgery, shoulder dysfunction) should be excluded. (Grade B)
Evidence: Women with underlying shoulder problems are of higher risk of injury, safety
issue is a concern. (Kilbreath et al., 2013; Scaffidi et al., 2012; Kilgour, Jones &
Keyserlingk, 2008) (1+; 2+; 1+)
4. Women with existing limb lymphedema should be excluded. (Grade A)
Evidence: Women with existing lymphedema are excluded in all studies due to safety
concern and the aims of preventing lymphedema. (Kilbreath et al., 2013; Singh, Vera &
74
Campbell, 2013; Scaffidi et al., 2012; Kilgour, Jones & Keyserlingk, 2008; Box et al.,
2002; Cinar et al., 2008; Todd et al., 2008) (1+; 2+; 2+; 1+; 1+; 1+; 1+)
Intervention
5. HBEP can be carried out by nurses and physiotherapists. (Grade A)
Evidence: These selected programmes were provided by either nurses or physiotherapists.
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Kilgour,
Jones & Keyserlingk, 2008; Box et al., 2002; Cinar et al., 2008; Todd et al., 2008) (1+; 2+;
2+; 1+; 1+; 1+; 1+) The only HBEP administrated by doctor was failed to attain a clinical
and statistical significant result. (Wingate, 1985) (2-)
6. HBEP is suggested to start on the day after operation. (Grade A)
Evidence: Five studies started the HBEP on the day after operation (Singh, Vera &
Campbell, 2013; Scaffidi et al., 2012; Todd et al., 2008; Box et al., 2002) (2+; 2+; 1+; 1+),
while other programmes were started on day four and seven. (Kilgour, Vera & Campbell,
2008; Cinar et al., 2008) (1+; 1+) Only one study began the HBE on four weeks after
operation (Kilbreath et al., 2013) (1+).
7. HBEP should last for at least 6 months to a year. (Grade A)
Evidence: Three studies implemented HBEP for 6 to 7 months (Singh, Vera & Campbell,
2013; Scaffidi et al., 2012; Cinar et al., 2008) (2+; 2+; 1+), while the others programmes
lasted for 1 to 2 years (Kilbreath et al., 2013; Todd et al., 2008; Box et al., 2002) (1+; 1+;
1+).
8. HBEP should comprise of A) preoperative education, B) individualized postoperative
exercise sessions and C) regular follow-ups. (Grade A)
Evidence: A) +B) + C) These were the common composition of the HBEP in the quality
studies and shown significant reduction in the incidence of developing lymphoedema.

75
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Box et al.,
2002) (1+; 2+; 2+; 1+)
A) + B) Both elements were described in programme shown statically significant in
preventing BCRL. (Kilgour, Jones & Keyserlingk, 2008) (1+)
9. Preoperative education should A) include introduction on lymphoedema, possible risk of
developing lymphoedema and postoperative exercise; B) deliver verbally or in written
format. (Grade A)
Evidence: A) + B) The same contents were delivered by either one or both means
preoperatively in these studies and shown significant results. (Kilbreath et al., 2013;
Singh, Vera & Campbell, 2013; Scaffidi et al., 2012; Kilgour, Jones & Keyserlingk, 2008;
Box et al., 2002) (1+; 2+; 2+; 1+; 1+)
10. Deep breathing, stretching and ROM exercise should be performed on the day after
operation. (Grade A)
Evidence: These types of exercise were used in combination in the quality programmes
contributed to significant results. (Singh, Vera & Campbell, 2013; Scaffidi et al., 2012;
Cinar et al., 2008; Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008; Box et al., 2002)
(2+; 2+; 1+; 1+; 1+; 1+)
11. Stretching A) on neck muscles, elevation and abduction of shoulder below 90˚and flexion
and extension of elbow; B) maintains for 5 to 15 minutes for each stretch are suggested.
(Grade A)
Evidence: Stretching exercise was introduced by the quality selected studies and
contributed significant results. (Kilbreath et al., 2013; Scaffidi et al., 2012; Kilgour, Jones
& Keyserlingk, 2008) (1+; 2+; 1+)
12. Range-of-motion exercise on hands, elbow and shoulder movement limited by 90˚(in the

76
first week after operation) are suggested. (Grade A)
Evidence: ROM exercise was included in the selected studies. (Singh, Vera & Campbell,
2013; Cinar et al., 2008; Todd et al., 2008; Box et al., 2002) (2+; 1+; 1+; 1+) The use of
full shoulder ROM had shown negative effect on lymphoedema. (Todd et al., 2008) (1+)
13. Stretching and ROM exercise A) should be performed in 2- 3 times per day and B)
patients should be reminded to stay pain-free. (Grade A)
Evidence: Studies suggested to repeat each set of ROM exercise for 2 – 3 times per day.
(Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al., 2013; Todd et al,
2008; Box et al., 2002) (1+; 2+; 2+; 1+; 1+) It is also important to avoid injury and
interfere on wound healing by performing HBE comfortably and free from pain.
(Kilbreath et al., 2013; Scaffidi et al., 2013; Kilgour, Jones & Keyserlingk, 2008) (1+; 2+;
1+)
14. Pamphlet or video of steps and safety reminders should be distributed. (Grade A)
Evidence: Pamphlet or videos are important in guiding and facilitating correct and safe
HBE. (Kilbreath et al., 2013; Scaffidi et al., 2013; Cinar et al., 2008; Kilgour, Jones &
Keyserlingk, 2008; Todd et al, 2008; Box et al., 2002; Kilgour, Jones & Keyserlingk,
2008) (1+; 2+; 1+; 1+; 1+; 1+; 1+)
15. At least two sessions of face-to-face or telephone follow-ups should be offered.(Grade A)
Evidence: Face-to-face follow-ups are important in monitoring the progress of HBE,
ensuring the accuracy and safety of HBE. (Kilbreath et al., 2013; Singh, Vera & Campbell,
2013; Scaffidi et al., 2013; Box et al., 2002) (1+; 2+; 2+; 1+;1+) Telephone follow-up was
only used by Todd et al. (2008) (1+)
77
Evaluation
16. The multi-frequency bioimpedance analysis, water displacement method and arm
measurement can detect lymphoedema. (Grade A)
Evidence: All quality studies used either one to all of them in determining the incidence
of lymphoedema. (Kilbreath et al., 2013; Singh, Vera & Campbell, 2013; Scaffidi et al.,
2013; Cinar et al., 2008; Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008; Box et al.,
2002) (1+; 2+; 2+; 1+; 1+; 1+; 1+)
17. The range-of-motion alone can be measured by the Goniometer. (Grade A)
Evidence: In these studies, Goniometer was used in measuring the ROM and obtained
significant results. (Singh, Vera & Campbell, 2013; Scaffidi et al., 2013; Cinar et al., 2008;
Kilgour, Jones & Keyserlingk, 2008; Todd et al., 2008; Wingate, 1985) (2+; 2+; 1+; 1+;
1+; 2-)
18. The adherence rate and problems encountered should be recorded in the logbook. (Grade
B)
Evidence: It is essential for progress monitoring and programme evaluation. (Kilbreath et
al., 2013; Kilgour, Jones & Keyserlingk, 2008) (1+; 1+)
Summary
According to the graded recommendation, the flow of Home-based exercise programme is
summarized in the chart attached below.
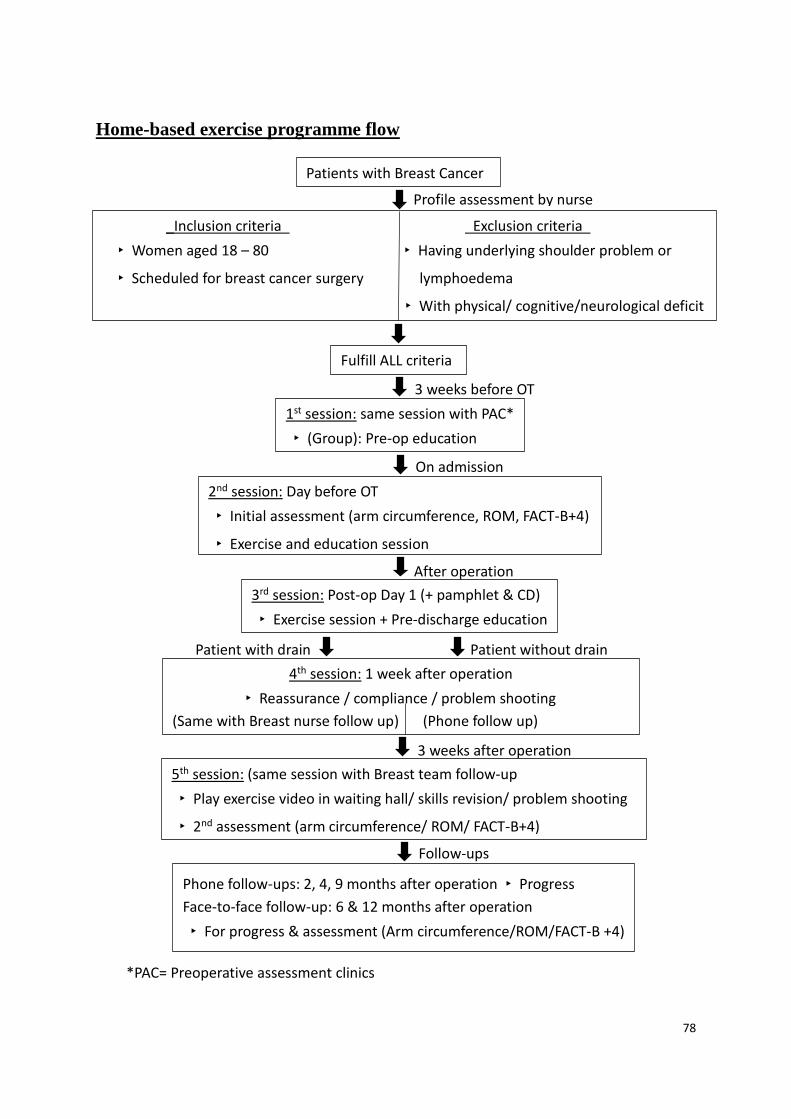
78
On admission
Home-based exercise programme flow
Profile assessment by nurse
Patients with Breast Cancer
_Inclusion criteria Exclusion criteria
‣ Women aged 18 – 80 ‣ Having underlying shoulder problem or
‣ Scheduled for breast cancer surgery lymphoedema
‣ With physical/ cognitive/neurological deficit
Fulfill ALL criteria
1st session: same session with PAC*
‣ (Group): Pre-op education
3 weeks before OT
After operation
2nd session: Day before OT
‣ Initial assessment (arm circumference, ROM, FACT-B+4)
‣ Exercise and education session
Patient with drain Patient without drain
3rd session: Post-op Day 1 (+ pamphlet & CD)
‣ Exercise session + Pre-discharge education
3 weeks after operation
4th session: 1 week after operation
‣ Reassurance / compliance / problem shooting
(Same with Breast nurse follow up) (Phone follow up)
Follow-ups
5th session: (same session with Breast team follow-up
‣ Play exercise video in waiting hall/ skills revision/ problem shooting
‣ 2nd assessment (arm circumference/ ROM/ FACT-B+4)
*PAC= Preoperative assessment clinics
Phone follow-ups: 2, 4, 9 months after operation ‣ Progress
Face-to-face follow-up: 6 & 12 months after operation
‣ For progress & assessment (Arm circumference/ROM/FACT-B +4)

79
References
Box, R. C. (1998). Women’s Health: A Text-book for physiotherapists. (2nd ed.). London: WB
Saunders.
Box, R. C., Reul-Hirche, H. M., Bullock-Saxton, J. E., & Furnival, C. M. (2002).
Physiotherapy after breast cancer surgery: results of a randomised controlled study to
minimise lymphoedema. Breast Cancer Research and Treatment. 75, 51-64.
Britton, T. M. B., & Purushotham, A.D. (2009). Understanding Breast Cancer-Related
Lymphoedema. Surgeon, 7(4), 120-124.
Cinar, N., Seckin, U., Keskin, D., Bodur, H., Bozkurt, B. & Cengiz, O. (2008). The
Effectiveness of Early Rehabilitation in Patients with Modified Radical Mastectomy.
Cancer Nursing. 31(2), 160-165.
Department of Surgery (2014). Division page of Breast Surgery. Retrieved January 1, 2015,
from http://www.surgery.hku.hk/br.php
Gautam, A. P., Maiya, A. G., & Vidyasagar, M. S. (2011). Effect of home-based exercise
program on lymphedema and quality of life in female postmastectomy patients: Pre-post
intervention and study. Journal of Rehabilitation Research & Development, 48(10),
1261-1268.
Hospital Authority (2014). Vision, Mission and Values. Retrieved September 1, 2014, from
http://www.ha.org.hk/visitor/ha_visitor_index.asp?Parent_ID=10004&
Content_ID=10009&Ver=HTML
Hospital Authority Central Oncology Committee (2009) HA Clinical Practice Guideline on
Management of Breast Cancer. Retrieved March 28, 2014, from CPG_Breast _Patient
version_ ENG 20090317_logo_revised20090331.pdf

80
Hong Kong Cancer Registry (2013). Hong Kong Cancer Registry, Hospital Authority.
Retrieved September 1, 2014, from http://www3.ha.org.hk/cancereg/statistics.html
International Agency for Research on Cancer (IARC) (2014). Cancer Factsheets- Globocan
2012 Section of Cancer Information. Retrieved March 28, 2014, from
http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx
Jeffs, E. & Wiseman, T. (2012). Randomised controlled trial to determine the benefit of daily
home-based exercise in addition to self-care in management of breast cancer-related
lymphedema: a feasibility study. Support Care Cancer, 21, 1013-1023.
Kilbreath, S. L., Lee, M., Refshauge, K. M., Beith, J. M., Ward, L. C., J., Simpson, J. M., &
Black, D. (2013). Transient swelling verus lymphoedema in the first year following
surgery for breast cancer. Support Care Cancer. 21, 2207-2215.
Kilbreath, S. L., Refshauge, K. M., Beith, J. M., Ward, L. C., Lee, M., Simpson, J. M. &
Hansen, R. (2012). Upper limb progressive resistance training and stretching exercises
following surgery for early breast cancer: a randomized controlled trial. Breast cancer
Research and Treatment. 133, 667-676.
Kilbreath, S. L., Refshauge, K. M., Beith, J. M., Ward, L. C., Simpson, J. M. & Hansen, R. D.
(2006). Progressive resistance and stretching following surgery for breast cancer: study
protocol for a randomised controlled trial. BMC Cancer. 6, 273.
Kilgour, R. D., Jones, D. H., & Keyserlingk, J. R. (2008). Effectiveness of a self-administered,
home-based exercise rehabilitation program for women following a modified radical
mastectomy and axillary node dissection: a preliminary study. Breast Cancer Research and
Treatment. 109(2), 285-295.
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [computer software].
Retrieved May 12, 2015, from http://www.stat.uiowa.edu/~rlenth/Power.

81
LoBiondo-Wood, G., & Haber, J. (2002). Nursing research: methods, critical appraisal, and
utilization (5th ed.). St. Louis: Mosby.
National Cancer Institute (2013a). Treatment Option Overview. Retrieved March 28, 2014,
from http://www.cancer.gov/cancertopics/pdq/treatment/breast/Patient
National Cancer Institute Breast Cancer Treatment (2013b). Coping with cancer: Supportive
and Palliative Care. Retrieved March 28, 2014, from
http://www.cancer.gov/cancertopics/coping
Polit, D. F. & Beck, C. T. (2014). Essentials of nursing research: appraising evidence for
nursing practice. (8th ed.). Philadelphia: Lippincott Williams & Wilkins.
Pusic, A. L., Cemal, Y., Klassen, A., Cano, S., Sulimanoff, I., Hernandez, M., et al. (2013).
Quality of life among breast cancer patient with lymphedema: a systematic review of
patient-reported outcome instruments and outcomes. Journal of Cancer Survivorship,
7(1), 83-92.
Rauschecker, H. H. F., Clarke, M. J., Gatzemeier, W., & Recht, A. (2001). Systemic therapy
for treating locoregional recurrence in women with breast cancer. The Cochrane Library,
4.
Ridner, S. H. (2013). Pathophysiology of Lymphedema. Seminars in Oncology Nursing,
29(1), 4-11.
Rogers, E. M. (2003). Diffusion of innovations (5th ed.). New York: Free Press.
Sankaranarayanan, R., Swaminathan, R., & Lucas, E. (2011). Cancer survival in Africa, Asia,
the Caribbean and Central America. International Agency for Research on Cancer.
Retrieved March 28, 2014, from http://survcan.iarc.fr/indexsurvcan1.php
Scaffidi, M., Vulpiani, M. C., Vetrano, M., Conforti, F., Marchetti, M. R., Bonifacino, A., et al.
(2012). Early rehabilitation reduces the onset of complications in the upper limb

82
following breast cancer surgery. European Journal of Physical and Rehabilitation
Medicine. 48(4), 601-611.
Schmidt, N. A., & Brown, J. M. (2009). Evidence-based practice for nurses: an appraisal
and application of research. Sudbury: Jones and Bartlett Publishers.
Scottish Intercollegiate Guideline Network (2014). Introduction to SIGN. Retrieved
September 16, 2014, from http://www.sign.ac.uk/about/introduction.html
Scottish Intercollegiate Guideline Network (2011). SIGN 50: A Guideline developer’s
handbook. Retrieved September 20, 2014 from
http://www.sign.ac.uk/guidelines/fulltext/50/index.html
Singh, C., Vera, M. D. & Campbell, K. L. (2013). The effect of Prospective Monitoring and
Early Physiotherapy Intervention on Arm Morbidity Following Surgery for Breast Cancer:
A Pilot Study. Physiotherapy Canada. 65(2), 183-191.
Sisman, H., Sahin, B., Dumann, B. B., & Tanriverdi, G. (2012). Nurse-assisted education and
exercise decrease the prevalence and morbidity of lymphedema following breast cancer
surgery. Journal of Balkan Union of Oncology, 17(3), 565-569.
Stetler, C. B. (2001). Updating the Stetler Model of research utilization to facilitate
evidence-based practice. Nursing Outlook, 49(6), 272-279.
Stuiver, M. M., Tusscher, M. R. T., Agasi-ldenburg, C.S., Lucas, S., Aaronson, N. K., &
Bossuyt, P. M. M. (2012). Conventional interventions for preventing clinically detectable
upper-limb lymphoedema in patients who are at risk of developing lymphoedema after
breast cancer therapy. The Cochrane Library, 4.
Todd, J., Scally, A., Dodwell, D., Horgan, K. & Topping, A. (2008). A randomised controlled
trial of two programmes of shoulder exercise following axillary node dissection for
invasive breast cancer. Physiotherapy. 94, 265-273.

83
Wingate, L. (1985). Efficacy of Physical Therapy for Patients Who Have Undergone
Mastectomies. Physical Therapy. 65(6), 896-900.
World Health Organization (2015). Health topics: Nursing. Retrieved January 1, 2015 from
http://www.who.int/topics/nursing/en/





























