Embed Size (px)
Citation preview

Everything you always wanted to know about TB…but were afraid to inhale?
Kevin Schwartzman MD, MPHRespiratory Division, MUHC
McGill Internal Medicine Resident Core TeachingMarch 29, 2012

Question
What is special about March 24?
http://www.youtube.com/watch?v=6tynGqZV1A0
www.theunion.org www.stoptb.org

Learner Objectives--1
To describe basic concepts in tuberculosis epidemiology
To recognize the spectrum of clinical and radiographic manifestations of active TB, in different patient populations
To describe the essential pathophysiology of latent and active TB
To identify and understand the rationale for evidence-based diagnostic strategies for active TB

Learner Objectives--2
To describe standard treatment for active TB
To identify indications, contraindications, and potential complications of this treatment
To identify key concepts in TB control, within and outside the hospital

Overview
Case presentations Epidemiology Pathophysiology Active TB:
Diagnosis Treatment, including special considerations Infection control
Key concepts in TB control
Jad Davenport, “Mural outside tuberculosis clinic, Dhaka”World Lung Foundation (http://worldlungfoundation.org)

Jad Davenport. “TB flourishes in crowded Dhaka shantytowns”World Lung Foundation (http://worldlungfoundation.org)

Pierre Virot, “A TB patient is examined by the doctor, Ghana”World Lung Foundation (http://worldlungfoundation.org)
www.nytimes.comOn May 24, 2007, Andrew Speaker, a 31 year-old lawyer from Atlanta, landed at Trudeau Airport on a flight from Prague, with a diagnosis of extensively drug-resistant (XDR) tuberculosis. He drove a rented car across the US border, and was apprehended. He had smear-negative TB, later determined not to be XDR.

Case 1
35 y.o. Inuit female Referred to MGH after trauma Smoker, no other past history No respiratory or constitutional symptoms Previously exposed to brother with active
TB Apparently did not receive treatment for latent
infection


Next steps?

Case 1
Underwent bronchoscopy BAL cytology negative BAL smear-negative for AFB
Discharged to the North with instructions for follow-up CXRs and clinical follow-up/other tests depending on results BAL ultimately culture-negative
Apparently lost to follow-up until she developed left arm and shoulder pain months later



Case 1
What would you recommend now?

Case 1
Bronchoscopy: some mucosal abnormalities seen on left side
BAL AFB smear negative BUT necrotizing granulomatous
inflammation and AFB seen on biopsy specimens
Patient is staying at Northern Module What would you recommend now?

Case 2
32 y.o. male refugee claimant from Congo, arrived in Canada < 1 week previously
Admitted to medical ward because of extensive herpes zoster in left V1 distribution, with probable bacterial superinfection
Wife known HIV-positive, no respiratory issues Patient found to be HIV-positive with CD4 70 Complains of minor hemoptysis


Case 2
What investigations (if any) would you now arrange?
Would you isolate this patient? What treatment (if any) would you
recommend?

Case 3
40 year-old female, Quebec-born, referred for persistent cough of 6 months’ duration
Smoker; also noticed ~10 lbs weight loss No travel history, no known HIV risks

Ms CL

Case 3
What would be your differential diagnosis? What would be your next steps?

“I thought TB had disappeared”
2010: WHO estimated 8.8 million new cases, vs. 8.3 million cases in 2000 and 6 million cases in 1990
40% in India and China, 24% in Africa Overall global incidence 128 per 100,000
annually, down from peak 142 in 2004 1.1 million deaths in HIV-negative individuals,
350,000 deaths in HIV-positive individuals 1/3 of world population believed to have latent
TB infection
http://www.who.int/tb/publications/global_report/en/index.html




Major Determinants
Basic elements of TB control e.g. diagnosis, consistent and appropriate treatment
Health system infrastructure e.g. national control programs, public vs. private providers etc.
General socioeconomic and health status, tobacco, alcohol, diabetes
HIV Drug resistance Obviously all these are interrelated

Bates et al, Arch Int Med 2007
Smoking and TB

Diabetes and TB
Jeon and Murray, PLoS Medicine 2008

HIV
Strongest known risk factor for TB disease Increases risk of progression/reactivation
of latent TB infection by 100-fold or more To date, impact on global epidemiology
most evident in sub-Saharan Africa, but concern re unknown magnitude of HIV-TB coinfection notably in India

Drug Resistance
In 2010, the estimated number of prevalent cases of multi-drug resistant TB was 650,000 (of 12 million prevalent cases of active TB overall)
Estimated that 3.4% of new cases and 20% of retreatment cases were MDR-TB
Defined as resistance to isoniazid AND rifampin, with or without resistance to other antibiotics
A marker of treatment program quality Poor prognosis, treatment complexity and
expense


WHO, Anti-Tuberculosis Drug Resistance in the World, 2008

WHO, Anti-Tuberculosis Drug Resistance in the World, 2008

TB in Canada
Ellis et al, Public Health Agency of Canada






Montreal
123 reported active TB cases in 2007; maximum was 209 in 1994
Corresponding decrease in incidence from 11.6 to 6.4 per 100,000
Consistently ~80% of cases involve foreign-born persons
DSP Montréal-Centre, Bureau de surveillance épidémiologique
http://www.santepub-mtl.qc.ca/Mi/surveillance/mado/archives/90-2005/incidence90-2007.pdf

Active Tuberculosis
Airborne Droplets
Inhalation by Others
Latent Infection
Case Finding (Passive or Active)
Effective Drug Treatment
Patient Behaviour (e.g. Cover Mouth)
Respiratory Isolation
Ventilation and Air Filtration
Ultraviolet Light
Progression or Reactivation
Antiretroviral Therapy for HIV
BCG Vaccination
Diagnosis and Treatment of Latent TB
Pathophysiology

Long and Schwartzman, Transmission and Pathogenesis of TB, Chapter 3, Canadian Tuberculosis Standards 2007

Clinical Manifestations
Pulmonary disease: 2/3 of cases in Canada Pleural TB and thoracic nodal disease ~ 10% Most common extrapulmonary site is peripheral lymph
nodes (~12%) Patients often asymptomatic when they have
less extensive disease (e.g. immigration screening)
Most frequent symptom: cough, usually for weeks to months—in symptomatic patients, virtually always present (even if not the symptom that precipitated the visit)

Clinical Manifestations
Other frequent symptoms: sputum, fever, malaise, loss of weight/appetite, night sweats, hemoptysis
Symptoms generally not very specific, hence the importance of the clinical and epidemiologic context
Timing of cough often used to estimate period of contagion
Physical exam generally not helpful; may show cachexia, fever, sometimes adenopathy

Questions to Ask
Place of birth, year of immigration (risk highest in years immediately after arrival)
Known history of TB disease, latent TB, exposure
Recent travel Visitors from abroad HIV issues Other past medical history

Chest Radiograph
The key first step in investigation A normal chest X-ray usually excludes the
diagnosis of pulmonary TB, except in some HIV-infected persons
Reactivation disease: usually upper zone airspace disease (infiltrate; “fluffy” appearance), may have cavities Involvement of other areas of lung, or contralateral
lung, suggests bronchogenic spread, and a higher bacterial load/potential for contagion
Beware of judging active vs. inactive TB on a CXR

Gary Hampton, “Paula Fujiwara of the IUATLD talks to the mother of a TB patient…” World Lung Foundation (http://worldlungfoundation.org)


Chest X-Ray
Primary disease (usually children, or persons with advanced HIV infection): lower zone disease, often dense consolidation, with or without cavitation May mimic bacterial pneumonia May be associated with intrathoracic
adenopathy
Miliary disease (rare)

Ms GL




Diagnosis of Active TB
For pulmonary disease, diagnosis hinges on growth of mycobacteria from respiratory secretions, i.e. sputum (spontaneous or induced), and/or bronchoalveolar lavage


Diagnosis
Culture of a single induced sputum has similar sensitivity to BAL culture for the diagnosis of pulmonary TB
3 induced sputa may have better sensitivity than BAL

Diagnosis
For other sites, biopsy (showing necrotizing granulomas, and ideally acid-fast bacteria) and/or culture according to the site Very low yield of fluid smear and culture for
serosal disease (pleural, pericardial, peritoneal)
Biopsies needed, with histology and culture

Diagnosis
For pulmonary TB, typically 50-60% smear-positive, though this will vary with clinical context Lower with HIV, or persons diagnosed
because of screening (e.g. immigration, contacts)
Higher with more advanced symptoms, more extensive radiographic abnormalities

Standard Nucleic Acid Amplification (PCR)
Limited use in diagnosis of smear-negative pulmonary TB, or extrapulmonary disease Sensitivity typically reported to be ~60% for
smear-negative pulmonary disease Lower for extrapulmonary disease A negative result cannot be used to exclude the
diagnosis Occasionally ordered under very specific
circumstances e.g. contact investigation that will start sooner if PCR positive

Menzies and Khan, Diagnosis of Tuberculosis Infection and Disease, Chapter 4, Canadian Tuberculosis Standards, 2007

Nucleic Acid Amplification
Now used as standard method to confirm that an isolate is M. tuberculosis AFB smear-positive specimens Cultures growing mycobacteria
Final confirmation is performed at the provincial reference laboratory

What’s new?
http://www.who.int/tb/features_archive/xpert_use_web/en/


Reporting
Once identified in the laboratory, reporting of active TB to public health authorities is mandatory by law “Double reporting” by laboratory and treating
physician Treating physician must report cases treated
on the basis of clinical diagnosis alone
Treatment of contagious tuberculosis is also required by law, and can be imposed

Tuberculin Skin Testing and Interferon-Gamma Release Assays
Are NOT appropriate diagnostic tests for active TB
A positive test may indicate TB infection, but cannot distinguish active from latent TB Pre-test probability of latent TB infection may
be 50% or higher, depending on the patient’s origin

Tuberculin Skin Testing and Interferon-Gamma Release Assays
Well-known false negative rate of ≥ 10% in active TB A negative TST or IGRA does not exclude the
diagnosis
False negatives also seen with HIV, other immune suppression e.g. in rheumatologic disease, transplant Anergy screens poorly reliable in this context

Initiating Treatment
Empiric treatment for active TB may sometimes be started without culture confirmation
This depends on the perceived likelihood of active TB, the potential consequences of waiting for confirmation, and the potential risks of treatment

Initiating Treatment
Treatment for latent TB should NEVER be started if active disease is a possibility If cultures have been sent, await results before
treating for latent TB (if appropriate)
However, it IS acceptable to initiate treatment for active TB, then modify if cultures are negative 4-month modified regimen for “culture-negative” TB
Also beware of treating pneumonia with a fluoroquinolone, if TB is a possibility

Treatment
Intensive phase: first 2 months Daily isoniazid, rifampin, pyrazinamide, and
ethambutol
Continuation phase: usually 4 additional months Daily or intermittent isoniazid and rifampin
• If intermittent, must be directly observed PZA stopped after 2 month intensive phase Ethambutol discontinued once drug susceptibility
confirmed

Treatment
Isoniazid: 5 mg/kg, to 300 mg max plus pyridoxine 25 mg daily
Rifampin: 10 mg/kg, to 600 mg max
Ethambutol: 15 mg/kg, to 1600 mg max
Pyrazinamide: 20 mg/kg, to 2000 mg max
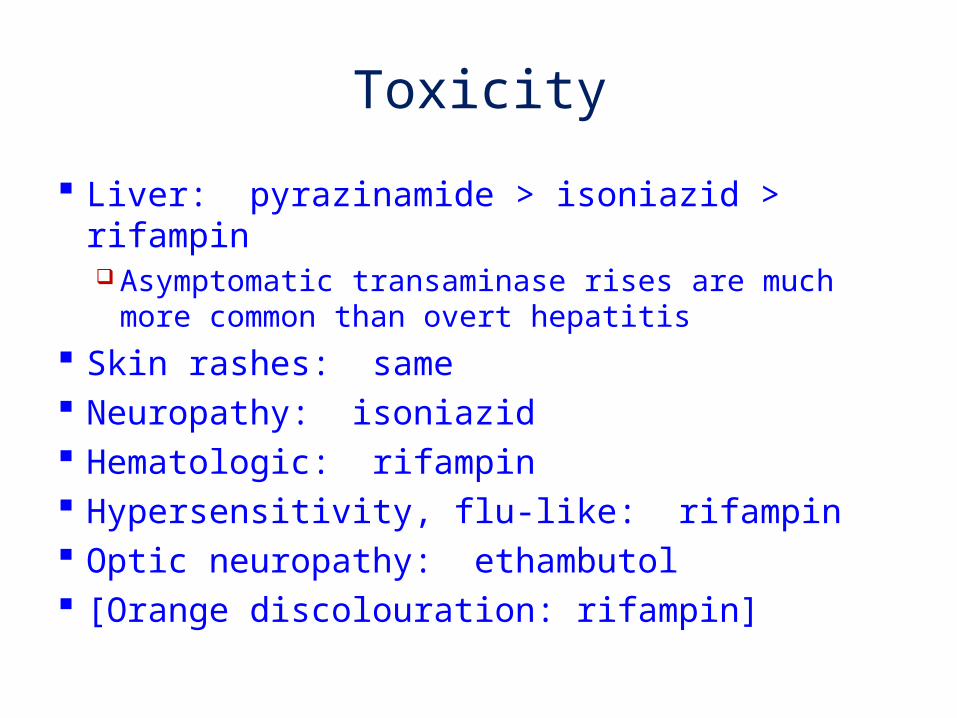
Toxicity
Liver: pyrazinamide > isoniazid > rifampin Asymptomatic transaminase rises are much more
common than overt hepatitis
Skin rashes: same Neuropathy: isoniazid Hematologic: rifampin Hypersensitivity, flu-like: rifampin Optic neuropathy: ethambutol [Orange discolouration: rifampin]

From Yee et al, Am J Respir Crit Care Med 2003. Bars show isoniazid, rifampin and PZA in that order, except for visual disturbance with ethambutol.
Standard definition of hepatitis was used, i.e. transaminases ≥ 3 x upper limit of normal with symptoms, or ≥ 5 x upper limit without symptoms

Special Considerations
Drug interactions Rifampin: potent P450 inducer
• Warfarin, antiretrovirals, cyclosporin, tacrolimus, oral contraceptives, anti-seizure medications, etc.
Isoniazid: increases phenytoin levels
Hepatic disease: close supervision May consider avoiding PZA, substituting
moxifloxacin
Active TB patients are usually seen at least monthly after discharge

Special Considerations
Renal dysfunction Dose adjustment for ethambutol Pyrazinamide is dialyzed Both given 3 times weekly for dialysis patients
Pregnancy INH, rifampin, ethambutol safe Safety of pyrazinamide undocumented, so
usually avoided No quinolones

Special Considerations
HIV Timing of antiretroviral therapy in patients with
new diagnosis of HIV concomitant with TB (Earlier appears better)
Immune reconstitution Drug-drug interactions Drug absorption Length of treatment

Length of Treatment
Usually 6 months Extended to 9 months if culture-positive at 2
months Also extended for bone or joint disease, CNS
disease (12 months)

Other Considerations
Adjunctive corticosteroids TB meningitis Pericardial TB
Therapeutic drug monitoring Clinical response slower than expected Concern about absorption or interactions
Direct observation Drug resistance

Infection Control
Most important: institution of appropriate isolation, diagnostics and treatment
Use of negative pressure room Use of N95 masks
Patients can use surgical masks when outside their rooms

Infection Control Smear-positive patients usually hospitalized
until repeatedly smear-negative Occasional exceptions for patients who live
alone and will remain at home
Smear-negative patients may be treated as outpatients, depending on the home situation and prospects for adherence Admission of patients with young children Admission of patients from congregate settings

Long and Schwartzman, Transmission and Pathogenesis of TB, Chapter 3, Canadian Tuberculosis Standards 2007

Contact Investigation
An important element of TB control in industrialized countries
“Concentric circle” approach for patients with pulmonary disease, beginning with household contacts
More extensive investigation for patients with smear-positive or laryngeal disease Also extended if there is evidence of significant
transmission, e.g. secondary active cases or excessive latent infection in contacts

Contact Investigation
One of the most cost-effective TB prevention strategies
Contacts diagnosed with latent TB infection are a high priority for treatment Active TB MUST be excluded

Key Concepts in TB Control
Priority is diagnosis and treatment of the most infectious patients WHO “DOTS” strategy focuses on diagnosis
using sputum smear microscopy Appropriate and complete drug treatment,
most often with direct supervision Monitoring and documentation of treatment
outcomes Major limitations include HIV, drug
resistance

Key Concepts in TB Control
Adjuncts to improve diagnostic yield Enhanced microscopy GeneXpert MTB/RIF® Availability of mycobacterial cultures in some settings
Linkage of TB and HIV control activities Rethinking empiric TB retreatment strategies to
deal with resistance Better MDR coverage Increasing the availability of drug susceptibility testing

Key Concepts in TB Control
In middle- and high-income countries, contact investigation with treatment of latent infection among contacts at risk
In the US and Canada, targeted testing and treatment for latent TB infection
Immigration-related screening activities Detection and treatment of active TB at time of
immigration Detection and potential treatment of “high-risk”
inactive TB

Summary
TB remains a major global health problem Although incidence has decreased in Canada
(and Montreal), we will continue to see it Foreign-born, Aboriginals, homeless,
immunosuppressed
Essential to keep the diagnosis of TB in mind, and pursue it using the right tools, in the appropriate clinical, radiographic, and epidemiologic context

Summary
Active TB Importance of microbiologic diagnosis;
biopsy/histology for extrapulmonary disease Standard treatment regimens Suitable respiratory isolation

THANK YOU! WHO/TBP/Jan van den Hombergh, Ethiopian girls in Assosa Mooi (World Lung Foundation)





























