Embed Size (px)
Citation preview

Evergreen: The First U.S. Veterans’Blind Rehabilitation Center
Gregory L. Goodrich1 and Tom Zampieri2
AbstractEvergreen was a World War I (WWI) adult, inpatient vocational rehabilitation facility forwar-blind soldiers, sailors, and marines in the United States. Although Evergreen sharedsimilarities with European war-blind rehabilitation organizations, it was novel in its philo-sophy and approach. It was also unlike any civilian blind rehabilitation program of its day.Although there are no comprehensive records known to us of how many troops becameblind or sustained vision loss during WWI, studying published reports of the veteransserved by Evergreen provides some insight into this population. As the United States’ onlyblind rehabilitation facility for adults, Evergreen achieved several firsts, including having anational scope, being racially integrated (at least to some degree), and innovating a resi-dential family training program. A role model of its day, it is now largely a footnote in thehistory of blind rehabilitation. We argue that the story of Evergreen contains lessons thatshould be remembered.
KeywordsArmed conflicts, blindness, history, veterans, vocational rehabilitation
World War I (WWI) began on July 28, 1914,
and pitted Germany and its allied nations
against the French and British and their allies.
The war ended on November 11, 1918. The
destruction of much of Europe was nearly
total and some 18 million people died with
an additional 41 million injured (World War
One Centennial Commission, 2017). The
United States entered the war later than its
allies, formally declaring war on April 2,
1917. During the 20 months that the United
States was involved, some 4.7 million
people served, 200,000 were injured, and
116,516 were killed (World War One
Centennial Commission, 2017). There are no
comprehensive records known to us of how
many troops became blind or sustained vision
loss during WWI. Evergreen came into exis-
tence to provide rehabilitation for U.S. war-
blind troops returning from Europe.
1 American Foundation for the Blind, Arlington,VA 22202, USA2 Blinded Veterans Association, Alexandria, VA22314, USA
Corresponding author:Gregory L. Goodrich, PhD, 1540 Ocean Avenue,Unit 14, Seabright, NJ 07760, USA.Email: [email protected]
Journal of VisualImpairment & Blindness
1-14ª American Foundation
for the Blind 2019Article reuse guidelines:
sagepub.com/journals-permissionsDOI: 10.1177/0145482X19845706
journals.sagepub.com/home/jvb

England, France, Belgium, and other Eur-
opean countries addressed their war-blind by
opening rehabilitation facilities, some gov-
ernment run and some private (Farrell,
1956). St. Dunstan’s in England, a private
charity headed by Sir Arthur Pearson, served
some 3,000 blind troops. In France, the gov-
ernment turned to the historic Hospice des
Quinze-Vingts (founded by Louis IX in
1260) and military hospitals to treat their
estimated 6,000 blind troops (Farrell,
1956). These European blind rehabilitation
facilities were well established by the time
the United States entered into the war and
provided useful models the United States
could draw upon to design its facility
(Salvante, 2015; Weed, 1923), which became
known as Evergreen.
According to Bonfiglioi, Tomba, Vigano,
Zati, and Benedetti (2015), WWI marked a
historic change in medicine with the idea that
medical care did not end with just the healing
of the wound, but that it extended to the reha-
bilitation needed to restore function and
independence to the degree possible for the
individual. Arguably, modern concepts of
occupational and physical therapy, as well
as prosthetics, saw their beginnings in the
treatment of WWI casualties. And, as Koes-
tler (2004) noted, WWI had a profound effect
on American society’s view of blindness and
visual impairment.
Formation
As blind troops began to return to the United
States from Europe, the first steps in the U.S.
development of a blind rehabilitation program
were undertaken by the office of the Surgeon
General of the Army, and a Committee on
Ophthalmology under the Council of National
Defense in October 1917 was convened. The
committee created a three-step plan: (1) eye
injuries would be treated in military hospitals,
(2) those who had permanent vision loss were
admitted to a vocational rehabilitation pro-
gram, and (3) once the rehabilitation was com-
pleted, the veteran who was blind would
transition back to civilian life (Farrell, 1956).
As with many plans, listing the steps was far
easier than implementing them.
To implement the last two steps of the
committee’s three-step plan, Army General
Hospital #7 was founded on a privately
owned 99-acre estate called Evergreen (see
Figure 1), which was leased to the Army for
US$1.00 per year by Mrs. T. Harrison Garrett
(Farrell, 1956; Weed, 1923; Woods, 1943).
The hospital was a first in a number of
respects: it was the only federal hospital
devoted exclusively to blind rehabilitation,
and its primary purpose was not to provide
medical care but to provide vocational reha-
bilitation to blind soldiers, sailors, marines,
and veterans. In fact, the hospital was more
school than hospital (Weed, 1923), and the
war-blind admitted were deemed “students”
not “patients.” Despite the fact the hospital
was an Army facility, it was responsible for
rehabilitation of soldiers, sailors, and mar-
ines. In addition to the main building, the
estate had other facilities including an indoor
swimming pool and bowling alley (see
Figure 2). The American Red Cross, which
leased a 2-acre property adjacent to Ever-
green, played an initial role by providing
social and recreational activities (Red Cross
Institute for the Blind, 1918; Weed, 1923).
There were two other agencies that played
important roles at Army General Hospital #7.
One was the Bureau of War Risk Insurance
(established by Congress in 1914) that
provided disability payments to disabled vet-
erans. The other was the Federal Board for
Vocational Education (FBVE), which was
established by Congress under the Smith–
Hughes Act of February 23, 1917 (Carleton,
2002; Office of Medical History, 2017).
FBVE provided vocational rehabilitation
across the United States to individuals with
2 Journal of Visual Impairment & Blindness XX(X)

various disabilities including blindness. Its
authority, in addition to creating vocation
rehabilitation programs and partnering with
existing programs, included the ability to
pay agencies for rehabilitation and to pay
individuals stipends while they were in
rehabilitation.
To help direct the operation of the hospi-
tal, an advisory committee was created with
membership including James Bordley and
M. C. Migel among others (Red Cross Insti-
tute for the Blind, 1920b). Dr. Bordley, a
Baltimore ophthalmologist, had taken an
early interest in war-blind troops and visited
rehabilitation facilities in Europe. Given his
profession and interests, Dr. Bordley, an
Army lieutenant colonel, was placed in
charge of the hospital (Woods, 1943). M.
C. Migel, an inductee into the Blindness Hall
of Fame: Leaders and Legends of the
Blindness Field, was a successful business
man, headed the Commission on Uniform
Type for the Blind, helped found both the
American Foundation for the Blind and the
World Conference on Work for the Blind
(now the World Blind Union), to list only a
few of his accomplishments (Tuttle & Tuttle,
2010).
Army General Hospital #7 formally
opened in April 1918, although new con-
struction on the site was not completed until
November 1918 (Miyagawa, 1999), which
required that the first arrivals to be housed
and taught in whatever existing buildings
were serviceable. Initially, the rehabilitation
program at Evergreen languished. In April
1919, however, Sir Arthur Pearson visited
the hospital and described the methods used
at St. Dunstan’s. The fact that St. Dunstan’s
successful program was run not by a
Figure 1. Estate house at Evergreen. The estate consisted of a large mansion with other buildingsincluding an indoor swimming pool and bowling alley. Courtesy of Perkins School for the BlindArchives.
Goodrich and Zampieri 3

government agency but by a more flexible
private agency was an important factor in
demilitarizing the hospital and turning
administration over to the Red Cross,
although Evergreen remained under the aus-
pices of the Army (Outlook for the Blind,
1918; Weed, 1923).
Among the problems that had cropped up
were the following:
� low morale among the troops who are
blind, in part because they were still on
active duty and their pay was signifi-
cantly lower than it would have been
if they had been discharged with a
service-connected disability (Miyagawa,
1999; “The past year,” 1920);
� the Army’s effort lacked strong leader-
ship unlike St. Dunstan’s (Farrell, 1956);
� living conditions were styled after mil-
itary barracks, and the military regimen
was not well suited to rehabilitation
(“The past year,” 1920);
� the rehabilitation programs that were
offered were rudimentary and left
troops with significant amounts of
unproductive free time (“The past
year,” 1920); and
� as Alan C. Woods (1943), an ophthal-
mologist who served at Evergreen,
noted, “the education and rehabilitation
of the blind is scarcely the function of a
Department whose fundamental duty is
to wage war” (p. 1021).
To resolve these problems, the administra-
tive and rehabilitation responsibilities were
transferred from the Army to the Red Cross
and FBVE. The hospital was renamed the
Red Cross Institute for the Blind. More
commonly, the institute was known as
“Evergreen,” after the name of the Garrett
Figure 2. The bowling alley at Evergreen. Two students are shown bowling. Courtesy of PerkinsSchool for the Blind Archives.
4 Journal of Visual Impairment & Blindness XX(X)

estate. The Red Cross was responsible for
the administration of Evergreen and the reha-
bilitation program. FBVE paid the Red Cross
for running the facility at the rate of
US$100.00 per month per student and an
additional US$6.50 per month per student for
supplies and equipment (FBVE, 1917).
When administrative control changed, the
soldiers who were blind at the hospital were
discharged and began collecting disability
payments from the War Risk Insurance
Board. The change in administration and
rehabilitation model quickly paid off: morale
improved and once-idle hours filled with
educational and vocational training (Half-
penny, 1920).
Since Evergreen remained an Army
facility, Dr. Bordley was assigned by the
Army as its director, in large part to ensure
satisfactory liaison between the Army, the
Red Cross, and FBVE. Dr. Bordley (1919)
strongly believed that vocational rehabili-
tation would allow blind troops to avoid
the unemployment that was typical of indi-
viduals with visual impairments in the
United States.
Demographics of the veterans whoare blind
The veterans at Evergreen were mostly
enlisted men who came from a variety of
backgrounds. About 65% had little formal
education and, prior to the war, were
employed as farmers or laborers. Over half
had lost vision because of wounds or the
effects of gas, and almost 20% had vision
loss attributable to disease such as spinal
meningitis or measles. Venereal disease or
toxic poisoning accounted for about 13% of
cases, and congenital defects such as retinitis
pigmentosa, myopia, or keratitis that were
aggravated by service in the war accounted
for about 8%. In about 4% of cases, the cause
of vision loss was unknown (FBVE, 1917).
These statistics should be treated with cau-
tion, since the exact numbers likely changed
over time as more individuals blinded in the
war were identified. In addition, only about
half of the total number of war blind were
seen at Evergreen (Ostermeier, 2010), and
the nature of vision injuries for the remaining
50% is unknown. About half of the students
served between the opening of Evergreen
and 1921 were totally blind, and the remain-
ing 50% had low vision. The degree of vision
loss was rated as the percentage loss from
typical vision, but this measure was not
viewed as an adequate determination for
eligibility for vocational training. “First, no
definite percentage of vision could be taken
as an index as to whether a man should be
referred” and referrals of “any man who had
difficulty in ‘carrying on’” were referred for
training at Evergreen (FBVE, 1921, p. 425).
Further confounding the issue was a lack of
confidence in the reliability of the military’s
ratings of vision when discharging troops
(U.S. Congress, 1920).
The total number of students served at
Evergreen is a matter of some debate. Woods
(1943), who served as an ophthalmologist at
Evergreen, estimated in 1943 that about 400
were treated there. This number is similar to
the 350 estimated by Farrell (1956) in his
book The Story of Blindness. The total num-
ber of WWI war–blind is even more difficult
to state with any precision, in large part,
because some report only those blinded in
combat, while others also report those
blinded by accident, disease, or aggravation
of existing eye disorders while in military
service. Another impediment to assessing the
number of WWI war–blind is that many fam-
ilies refused to allow their sons to receive
blind rehabilitation in the belief that the fam-
ily could best care for them (Bordley, 1919),
and the number of these cases was not
recorded. Not all identified war-blind were
referred to Evergreen, since FBVE also had
Goodrich and Zampieri 5

a policy of referring war-blind to community-
based agencies for blind people where avail-
able (FBVE, 1921). As Ostermeier (2010)
noted, only about half of those with eye
wounds or impaired eyesight as the result
of the war were treated at Evergreen. Collec-
tively, these reports suggest that some 800–
1,000 individuals became visually impaired
(i.e., they were blinded or became legally
blind) because of their service in WWI.
These numbers are largely speculative, given
the record keeping of the day and the fact that
we are examining events that occurred some
100 years ago.
Evergreen, under the Red Cross, may have
been a racially integrated facility, making it
relatively unique within the U.S. military
(and general society) of the day. The primary
evidence for integration is a photo in the
Perkins School for the Blind collections of
an African American student at Evergreen.
However, whether this individual repre-
sented a unique case or not is an open ques-
tion since race and segregation were not
specifically discussed in any Red Cross Insti-
tute for the Blind publication (or those relat-
ing to it) that we researched. Evergreen,
when it transferred from Red Cross to the
Veterans Bureau, appears to have been seg-
regated. Veterans Bureau testimony to Con-
gress states that African American veterans
blinded in WWI were not provided training
at Evergreen, but that they were referred to
other agencies including the Maryland
Workshop for the Blind in Baltimore and the
School for Colored Deaf and Blind in Austin,
TX (Director United States Veterans Bureau,
1922, 1923).
Injuries causing blindness in war time
often cause other significant injuries. Ampu-
tations, lingering effects of gas attacks, and
other injuries were not uncommon. The
Evergreen Review (archived within the New
Outlook for the Blind at http://www.perkin
s.org/history/archives/collections/outlook-
for-the-blind) was a monthly publication of
the Red Cross Institute for the Blind pub-
lished for only 1 year (1920). It contained
program descriptions and interesting facts
about Evergreen, including information
about distinguished visitors and stories about
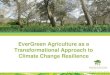
students. One particularly interesting case
serves as an illustration. Carl Bronner was a
sailor who, while on a recreational outing
ashore in Italy, picked up what he thought
was a naval metal polish can. It was, in fact,
an improvised hand grenade that exploded in
his hand. The accident resulted in the death
of Mr. Bronner’s companion, and Mr. Bron-
ner became totally blind and lost both of his
hands at the wrists. Despite these handicaps,
Mr. Bronner, while at Evergreen, was able to
complete his high school education, learn to
write braille, and use a specially adapted
typewriter to compose correspondence,
including independently folding papers and
inserting them into envelopes. The typewri-
ter was operated by a combination of wrist
controls and foot pedals (see Figure 3;
Bronner, 1921; “The story of Carl Bronner,”
1920). Unfortunately, to our knowledge,
there is no extant record of how the typewri-
ter was constructed, although it is shown in
Figure 3 in use by Mr. Bronner.
Philosophy and rehabilitationpractices
The philosophy of the institute heavily
emphasized vocational training with the goal
that as many men as possible would become
independent (Red Cross Institute for the
Blind, 1920c), but social and recreational
activities were not neglected. On the contrary,
social interactions and recreational activities
were viewed as being integral to the rehabili-
tation process. In fact, social and recreational
activities were listed as formal departments
within the rehabilitation curriculum (Red
Cross Institute for the Blind, 1920c, 1920g).
6 Journal of Visual Impairment & Blindness XX(X)

The Evergreen estate already had a swimming
pool and bowling alley, and these were pop-
ular recreational activities (see Figure 2).
Three principles guided the selection of
vocational courses offered at Evergreen.
First, consideration should be given to any
vocation that offered potential possibilities
to the blinded soldier. Second, these voca-
tions should provide an opportunity that
required only a small capital outlay to start
the business for the blind soldier who wanted
to start his own business. Third, the vocation
should provide the largest employment and
remunerative possibilities for those who
sought paid employment rather than starting
their own business (Red Cross Institute for
the Blind, 1920c). A partial list of vocational
courses is provided in Table 1.
The Evergreen estate provided plentiful
space for vocational training, including a
poultry farm. Buildings and equipment were
provided by the Army and Red Cross to sup-
port training including wood working, poul-
try farming, and machine shops, among other
training areas. A store was also built for stu-
dents to gain practice in setting up and run-
ning small businesses. To help orient new
students and visitors to the grounds, a braille
and tactile map (see Figure 4) was made by
John Benson, one of the students who previ-
ously worked as a stonecutting draftsman
(Red Cross Institute for the Blind, 1920a).
One of the most innovative aspects of the
Evergreen rehabilitation program was the
encouragement of wives and family mem-
bers to participate in the therapy their loved
ones received (Red Cross Institute for the
Blind, 1920a). This encouragement extended
to providing larger quarters for families and
including them in meals and social activities.
Since students who had only limited edu-
cation required prevocational subjects such
Figure 3. Carl Bronner using his adapted typewriter. Photo courtesy of American National Red Crossphotograph collection (Library of Congress; DLC) 2009632518.
Goodrich and Zampieri 7

as spelling, mathematics, reading, and other
educational topics, courses were developed
as part of the training options. In addition,
courses in braille and typewriting were pro-
vided both for personal reading and corre-
spondence and to facilitate vocational
training (see Figure 5). Since training alone
would not guarantee employment, FBVE had
offices across the country that contacted
potential employers to arrange for students
to be employed once their training at Ever-
green was completed (“Survey of Work,”
1920).
The ultimate goal of vocational training is
competitive employment, whether the stu-
dent was to open an independent store in the
community or work in a commercial setting.
To ensure that students would be compet-
itive, scientific time and motion studies were
made of sighted experts in selected vocations
(Lohrke, 1993; “Time-study motion picture,”
1919). Experts in a task were filmed at work,
and the films were analyzed to determine the
sequence of steps involved and how long
each step took. These studies allowed
instructors to precisely lay out the steps
involved in a given task, so that they could
more easily be learned by students. It also
provided a way to measure the student’s
Table 1. Education departments and partial listof courses offered at Evergreen.
Educationaldepartment Partial list of courses
Academic BrailleBusiness correspondenceCommercial arithmeticSpellingTypewritingAmerican historyCivicsEnglish literature
Massage andanatomy
MassageAnatomy
Commercial MerchandizingStore practiceEvery-day business and business
administrationInsurance salesSalesmanshipCommercial law and business
practicesIndustrial
departmentWoodworkingWeavingNovelty workTire vulcanizing (tire repair)Vulcanizing managementGarage managementMachine shop practiceCigar makingCigar making management
Poultrydepartment
Poultry husbandryPoultry house construction
and equipmentPoultry feeding, breeding,
diseasesPoultry classificationEgg productionIncubator operation
Musicdepartment
Elementary (voice, piano, string,wind, and percussioninstruments)
Advanced course for musicas a vocation
(continued)
Table 1. (continued)
Educationaldepartment Partial list of courses
Avocationalcourses
BookbindingBasketryBee keepingChair caning, rug weaving,
hammock makingDepartment of
physicaland socialeducation
BowlingSwimmingGymnasiumDance and entertainment
activities
8 Journal of Visual Impairment & Blindness XX(X)

productivity in relation to expectations in
competitive employment. The vocational
activities explored went well beyond ele-
mentary tasks and included typical jobs
in metalworking and woodworking (see
Figure 6). The instructors at Evergreen were
drawn from civilian blind rehabilitation
organizations, and commercial specialists in
various fields were hired as necessary
(Woods, 1943).
Evergreen was widely viewed as a unique
and innovative program in the blindness
field. The 25th biennial convention of the
American Association of Workers for the
Blind that was held near Evergreen in Over-
lea, MD, devoted a half day to visit, so that
the attendees could have lunch with the staff
members and students and take a tour of the
facility (Red Cross Institute for the Blind,
1920d). The prominence of Evergreen was
also enhanced by visits from distinguished
individuals including Elisabeth, Queen of
Belgium (Red Cross Institute for the Blind,
1920h); General John Pershing, who gave an
address to the students and faculty (Red
Cross Institute for the Blind, 1920e); and Kel-
ler (1919), who also addressed the students
and later wrote an article on her visit (Red
Cross Institute for the Blind, 1920f). All vis-
itors lauded the heroism of the students for
both serving their country and the way they
were learning to adjust to their vision loss.
They also praised the innovative rehabilitation
program that was developed at Evergreen.
Missing elements of rehabilitation
It may seem odd that nowhere in the educa-
tional or vocational curricula were low vision
or orientation and mobility mentioned. In
fact, neither existed at Evergreen nor any-
where else at the time. The field of low vision
did not begin to develop until 1924, when the
Figure 4. Braille and tactile map of Evergreen. Courtesy of Perkins School for the Blind Archives.
Goodrich and Zampieri 9

American Foundation for the Blind began
providing telescopes and referring patients
to eye care providers, and it was not until
1953 that formalized low vision clinics came
into existence (Goodrich, Arditi, Rubin,
Keeffe, & Legge, 2008). Similarly, O&M
would not become a discipline until its devel-
opment in 1944 at Valley Forge Army
Hospital (Koestler, 2004). Students at Ever-
green did learn to travel independently, and
canes were available, but travel skills were
not specifically mentioned in the curriculum.
Keller (1919) recalled that during her visit to
Evergreen, a student invited her for tea, and
she described “the ‘tap-tap’ of his cane being
music to [her] feet” as he guided her from the
barracks to the Red Cross House (p. 36). At
Evergreen, independent travel seems to have
been learned as a by-product of everyday life
and recreational activities. No records from
Evergreen mention how, or if, mobility canes
were formally distributed. Staff members
and experienced students would lead new
students to orient them to the grounds, and
gradually students learned to get around on
their own.
The closing of Evergreen
By 1924, the number of blind veterans being
referred to Evergreen began to decrease. The
Veterans Bureau was created in 1921, in
large part to consolidate the functions of the
Bureau of Pensions, FBVE, and the military
medical department (Farrell, 1956). The
three agencies were difficult for soldiers and
sailors to navigate, and the integration of the
three into one department offered a single
agency with which they needed to interact
(Farrell, 1956).
Figure 5. Braille and typing instruction. Two students, one reading braille and one using a typewriterare shown seated at a table with their instructor. Courtesy of Perkins School for the Blind Archives.
10 Journal of Visual Impairment & Blindness XX(X)

In 1922, responsibility for Evergreen was
transferred to the Veterans Bureau, which
continued the program until Evergreen was
formally closed on June 1, 1925 (Farrell,
1956; Ostermeier, 2010). The closure had
been anticipated for several years as the
number of combat injured troops decreased,
and the quality of staff members working at
the facility declined as the ones with the most
experience sought more permanent positions
elsewhere. As a result, the quality of rehabi-
litation at Evergreen declined (Woods,
1943). The Veterans Bureau was not man-
dated to continue the Evergreen facility, and
its responsibility to blind veterans became
limited to the payment of disability pensions.
The closing of Evergreen was also spurred by
a belief that the military would not need such
a facility in the future. That belief was
dashed only 19 years later when war-blind
troops serving in Europe and the Pacific
forced the military to open blind rehabilita-
tion facilities at Valley Forge, PA, and Let-
terman General Hospital in San Francisco,
CA (Farrell, 1956). The extent to which the
program at Evergreen influenced the opening
of the Veterans Administration (VA) Blind
Rehabilitation Center at the Edmond Hines,
Jr. Hospital in 1948 appears to be limited,
since the Evergreen blind rehabilitation pro-
gram oriented on vocational training, while
the Hines program focused on training for
personal independence that included O&M.
The success of any rehabilitation program
should be measurable; however, at the time
Evergreen was closed, there does not seem to
have been any comprehensive compilation of
data. The individual student reports pub-
lished in Evergreen Review paint a positive
image, as do the reports of FBVE (1917,
Figure 6. Student working on a lathe in the metal shop with his instructor observing. Courtesy ofPerkins School for the Blind Archives (Goodrich 18-0003 article).
Goodrich and Zampieri 11

1921). A less positive image was provided by
C. Warren Bledsoe, who interviewed 336
WWI blinded veterans residing in veterans’
homes (Miyagawa, 1999). Most of these vet-
erans were described as leading sedentary,
solitary lives, and only three used indepen-
dent mobility. Bledsoe did not report
whether these blind veterans had been stu-
dents at Evergreen or not; thus, it is unknown
whether or not their experiences reflected the
results of the Evergreen rehabilitation pro-
gram. In short, it appears that there is no
more than anecdotal eviendence upon which
to evaluate the success of Evergreen. This
lack of outcome evidence, however, should
not detract from the many accomplishments
made by the Evergreen board and staff
members, although it should be viewed as
a “case study” on the importance of sys-
tematic data gathering by rehabilitation and
other agencies.
Evergreen was a remarkable achieve-
ment. It was created in a very short time
following the entry into WWI of the
United States, and it became an efficient,
well-run blind rehabilitation facility (Woods,
1943) that was praised by many within and
outside the blindness community. Ever-
green under the Red Cross appears to have
been a racially integrated facility that
would make it unique within the U.S. mil-
itary (and general society) of the day.
Although the evidence for this integration
is sparse, and Veterans Bureau documents
suggest that in later years, at least, it was
racially segregated.
Evergreen also developed a science-based
vocational curriculum, a remarkable
achievement for the only blind rehabilitation
facility for adults in the United States. Its
primary focus was vocational rehabilitation;
however, the program recognized the impor-
tance of recreational and social activities
and the importance of family. Whenever
possible, families were accommodated and
provided living quarters so they could partic-
ipate in training alongside their war-blind
veteran. Baltimore offered a rich environ-
ment for social outings, and these were
enjoyed, as well. A basic tenant of the pro-
gram was that although all students had a loss
of vision, each student was recognized as an
individual, and each student’s rehabilitation
program was individually tailored.
Acknowledgment
The authors gratefully acknowledge the support
of the Perkins School for the Blind in obtaining
photographs that informed this manuscript and
the American Printing House for the Blind for
their consent to utilize the resources of the
M. C. Migel Library.
Declaration of conflicting interests
The author(s) declared no potential conflicts of
interest with respect to the research, authorship,
and/or publication of this article.
Funding
The author(s) received no financial support for
the research, authorship, and/or publication of
this article.
References
Bonfiglioi, S. S., Tomba, P., Vigano, A., Zati, A.,
& Benedetti, M. G. (2015). The First World
War drives rehabilitation toward the modern
concepts of disability and participation. Eur-
opean Journal of Physical Rehabilitation and
Medicine, 51, 331–336.
Bordley, J. (1919). Reeducation of the blind sol-
diers. International Record of Medicine and
General Practice Clinics, 109, 703–704.
Bronner, C. (1921). Carl Bronner. Outlook for the
Blind, XV(3), 123–124.
Carleton, D. (2002). The Smith-Hughes act
(February 23, 1917). In D. Carleton (Ed.),
Landmark congressional laws on education
(p. 227). Westport, CT: Greenwood Publish-
ing Group.
12 Journal of Visual Impairment & Blindness XX(X)

“Director United States Veterans Bureau.”
(1922). Annual report of the United States
Veterans’ Bureau. Retrieved from https://
babel.hathitrust.org/cgi/pt?id¼hvd.32044100
867647;view¼1up;seq¼9
“Director United States Veterans Bureau.”
(1923). Annual report of the United States
Veterans’ Bureau. Retrieved from https://
babel.hathitrust.org/cgi/pt?id¼mdp.390150
14437498;view¼1up;seq¼208
Farrell, G. (1956). The story of blindness (2nd ed.).
Cambridge, England: Harvard University
Press.
Federal Board for Vocational Education. (1917).
Methods employed in rehabilitation of the war
blind. Washington, DC: Author.
Federal Board for Vocational Education. (1921).
Fifth annual report to congress. Washington,
DC: Author.
Goodrich, G. L., Arditi, A., Rubin, R., Keeffe, J.,
& Legge, G. E. (2008). The low vision time-
line: An interactive history. Visual Impairment
Research, 10, 67–75.
Halfpenny, A. K. (1920). Evergreen. Evergreen
Review, 1, 27–28.
Keller, H. (1919). O! Brave new world that has
such people in’t. Red Cross Magazine, XIV,
31–38, 73–74.
Koestler, F. A. (2004). The unseen minority: A
social history of blindness in the United States.
New York, NY: AFB Press.
Lohrke, F. T. (1993). Motion study for the
blind: A review of the Gilbreths’s work
with the visually handicapped. Interna-
tional Journal of Public Administration,
16, 667–782.
Miyagawa, S. (1999). Journey to excellence:
Development of the military and VA blind
rehabilitation programs in the 20th century.
Lakeville, MN: Galde Press.
Office of Medical History. (2017). Nonmilitary
governmental departments concerned with
continuing the rehabilitation of disabled sol-
diers. Author. Retrieved from http://history.
amedd.army.mil/booksdocs/wwi/VolXIII/Sec
tionVIrev.htm
Ostermeier, M. (2010). History of guide dog
use by veterans. Military Medicine, 175,
587–593.
Outlook for the Blind. (1918). Sir Arthur Pear-
son’s visit to America. Outlook for the Blind,
Winter, 93–94.
“The past year at the Red Cross Institute for
the Blind.” (1920). Evergreen Review, 1,
52–56.
Red Cross Institute for the Blind. (1918). Red
Cross Institute for the Blind. Baltimore, MD:
Author.
Red Cross Institute for the Blind. (1920a). Braille
map of Evergreen. Evergreen Review, 1, 2.
Red Cross Institute for the Blind. (1920b). Com-
mittee of direction. Evergreen Review, 1, 19.
Red Cross Institute for the Blind. (1920c).
Courses of instruction. Evergreen Review, 1,
84–88.
Red Cross Institute for the Blind. (1920d). Ever-
green review. Evergreen Review, 1, 3.
Red Cross Institute for the Blind. (1920e). Gen-
eral Pershing’s talk at the Red Cross. Ever-
green Review, 1, 44.
Red Cross Institute for the Blind. (1920f). Helen
Keller’s address at Evergreen. Evergreen
Review, 1, 36–37.
Red Cross Institute for the Blind. (1920g). Snap-
shots at Evergreen field day sports. Evergreen
Review, 1, 75–77.
Red Cross Institute for the Blind. (1920h).
Visit of the Queen of Belgium. Evergreen
Review, 1, 1.
Salvante, M. (2015). Thanks to the Great War
the blind gets the recognition of his ability to
act: The rehabilitation of blinded servicemen
in Florence. First World War Studies, 6,
21–35.
The story of Carl Bronner. (1920). The Voca-
tional Summary, III(3), 38–39.
“Survey of Work.” (1920). Survey of work for the
blind. The Vocational Summary, III, 3–4.
Goodrich and Zampieri 13

“Time-study motion picture.” (1919). Blind
Americans at Evergreen. The Modern Hospi-
tal, XII, 206–207.
Tuttle, D., & Tuttle, N. (2010). Moses Charles
(M.C.) Migel. Retrieved from http://www.
aph.org/hall/inductees/migel/
U.S. Congress. (1920). Charges against the fed-
eral board for vocational education. Washing-
ton, DC: U.S. Government Printing Office.
Weed, F. (1923). General Hospital No. 7, Balti-
more, MD. In C. Lynch, F.W. Weed, & L.
McAfee (Eds.), The medical department of the
United States Army in the World War (Vol. V,
pp. 511–513). Washington, DC: U.S. Army
Surgeon General’s Office.
Woods, A. C. (1943). The story of the Red Cross
Institute for the Blind (1918-1925) in relation
to the present problem of the war blinded.
American Journal of Ophthalmology, 26,
1011–1023.
World War One Centennial Commission.
(2017). We honor. Retrieved from
http://www.worldwar1centennial.org/index.
php
14 Journal of Visual Impairment & Blindness XX(X)