Embed Size (px)
Citation preview

Evaluation of Burn Unit GBPT Performance from 2006-2008 (Iswinarno Doso Saputro, Badriyatut Dini)
1
EVALUATION OF BURN UNIT GBPT PERFORMANCE FROM 2006-2008. A RETROSPECTIVE STUDY Iswinarno Doso Saputro, Badriyatut Dini Department of Plastic Surgery, Airlangga University School of Medicine Dr Soetomo Hospital Surabaya ABSTRAK Luka bakar adalah salah satu kasus yang mematikan masih merupakan masalah kesehatan utama. Perawatan yang kompleks dan terbaik disampaikan dalam sebuah pusat spesialis oleh pribadi terlatih. Fasilitas yang diperlukan untuk pengobatan cedera sedang dan berat tidak tersedia di pusat-pusat banyak. Survival adalah salah satu dari beberapa kriteria untuk mengevaluasi kualitas manajemen bakar yang dipengaruhi oleh beberapa faktor termasuk usia pasien, memperpanjang dan menyebabkan luka bakar. Tujuan dari penelitian ini adalah untuk mendapatkan data dasar yang komprehensif untuk review berikutnya terutama setelah lahirnya unit luka bakar di rumah sakit dan untuk menganalisa korelasi kematian karena memperpanjang, disebabkan dari luka bakar. Ini dua tahun (antara Oktober 2006-September 2008) penelitian retrospektif pasien yang terluka bakar diterima di unit luka bakar GBPT RS Dr Soetomo. Data dikumpulkan dari catatan medis pasien dan dianalisis secara statistik. Sebanyak 213 pasien dirawat di unit luka bakar Rumah Sakit Dr.Soetomo sejak periode 137 (64%) dari mereka adalah laki-laki sementara 76 (35,7%) adalah perempuan, memberikan laki-laki: perempuan rasio 2:1. 189 (89,7%) pasien sembuh dan 24 (11,7%) pasien mati. Penyebab paling umum dari cedera ini adalah api 102 pasien (47,9%). Ada korelasi signifikan antara extenof mati terbakar (p = 0,0001; r = 0.498).. Kesimpulannya, kejadian luka bakar dari Oktober 2006 hingga September 2008 di Rumah Sakit Dr Soetomo 213 pasien, proporsi kasus kematian 11,3%. Ada korelasi signifikan antara tingkat dan menyebabkan cedera mati terbakar. ABSTRACT Burn injury is one of the deadly case remains a major health problem. The treatment is complex and best delivered in a specialist center by trained personnel. The facility that needed for the treatment of moderate and severe injury is not available in many centers. Survival is one of some criteria for evaluating quality of burn management which is influenced by some factors including age of patient, extend and caused of burn. The aim of this study is to obtain a comprehensive baseline data for subsequent review especially following the inception of a burn unit in the hospital and to analyze correlation to death due to extend, caused of burn injury. These two year (between October 2006-September 2008) Retrospective study of burn injured patient admitted in the burn unit GBPT Dr Soetomo Hospital. Data was collected from medical record of patient and was analyzed statistically. A total of 213 patient admitted in the burn unit Dr.Soetomo Hospital since that period 137 (64%) of them were males while 76 (35.7%) were females, giving a male : female ratio of 2:1. 189 (89.7%) patients were cured and 24 (11.7%) patients were die. The most common cause of these injury was fire 102 patients (47.9%). There were significant correlation between extent of burn to death (p=0.0001; r = 0.498). In conclusion, the incidence of burn injury from October 2006 to September 2008 at Dr Soetomo Hospital was 213 patients, proportion of death case were 11.3%. There were significant correlation between extent and caused of burn injury to death. Keywords: burn injury, burn unit, survival, burn management, Dr Soetomo Hospital Correspondence: Iswinarno Doso Saputro, Department of Plastic Surgery, Airlangga University School of Medicine, Dr Soetomo Hospital, Jl. Prof dr Moestopo 6-8, Surabaya 60131 INTRODUCTION Burn and related injuries are a major cause of death and disability in the United States. An estimated 1.1 million burn injuries require medical attention annually in the United States. Of those injured, about 50,000 require hospitalization and about 4,500 die annually from burn injuries. The introduction of burn centers in the 1960s and 1970s provide a truly multidisciplinary approach to care. Almost 95% of the patients admitted to burn centers in the U.S. now survive, and over one half of them return to pre-burn levels of physical and social
functioning within 12 to 24 months following injury (James 2006, Matthew 2007). The quality of burn care is no longer measured only by survival, but also by long term function and appearance. The surgeon’s goal for any burn is well healed, durable skin with normal function and near normal appearance (McCauley 2000, Hunt & Purdue 2000). Facilities that are needed for treatment of burn have not available yet in many health centers. For this reason, the basis for regional specialty treatment centers is provided. Early evaluation is safer if being done directly after trauma although distance and time to referral to burn center are the problems (Arvind

Folia Medica Indonesiana Vol. 47 No. 1 January - March 2011 : 1-5
2
2004). There are 3 burn centers in Indonesia, burn center RSUPN Dr. Cipto Mangunkusumo Jakarta, RSUD Dr Soetomo Surabaya and RSU Sanglah Denpasar. Burn center RSUD Dr Soetomo established since November 1999 for minimizing morbidity, mortality and disability rate because of burn and as referral center of burn in East Indonesia. Because of high incidence of burn and it morbidity and mortality, it is important to know quality of burn center RSUD Dr Soetomo Surabaya. The aim of this study is to know description of burn patients in burn center RSUD Dr Soetomo Surabaya and quality of burn center RSUD Dr Soetomo Surabaya. MATERIALS AND METHODS The study use observational analytic design. Data was collected retrospectively from medical record of patients admitted in burn center GBPT RSUD Dr Soetomo in the period of October 2006 until September 2008. This study uses total sampling of all patients in burn center RSUD Dr. Soetomo Surabaya in the period of October 2006 until September 2008. The population is all burn patients came to emergency room RSUD Dr Soetomo Surabaya in that period. The data include age, sex, domicile, cause, extent of burn, treatment duration and outcome. Data are explained descriptively. The statistic test are Fisher exact test and Symmetric measure test with α < 0.05. RESULTS There are 213 burn patients admitted in burn center GBPT RSUD Dr Soetomo in the period of October 2006 - September 2008. Total patients from Surabaya are 84 (39.3%) and outside Surabaya are 129 (60.7%) (Table 1). Table 1. Domicile distribution of burn patients in burn
center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Domicile Total
Surabaya 84 (39.3%) Outside Surabaya 129 (60.7%)
Total 213 (100%) Most of burn patients are male 137 (64.3%) and the other are female 76 (35.7%) , give the ratio (table 2).
Table 2. Sex and age distribution of burn patients in burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Sex Age
(years old) Total < 15 15-50 >50
Male 26 99 12 137 12.2 % 46.5 % 5.6 % 64.3 % Female 11 53 12 76 5.2 % 24.9 % 5.6 % 35.7 %
Total 37 152 24 213 17.4 % 71.4 % 11.3 % 100%
Table 2 shows that the most of patients are age of 15-50 years old consist of 152 patients (71.4%). Most of patients in this age group are male, consist of 99 (46.5%) and female are 53 patients (24.9%).
Figure 1. Cause and age distribution of burn patients in
burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Figure 1 shows that fire is the most common cause of burn, consist of 102 patients (47.9%), the other are scald, electrical and chemical consist of 56 patients (26.3%); 51 patients (23.9%) and 4 patients (1.9%).
Evaluation of Burn Unit GBPT Performance from 2006-2008 (Iswinarno Doso Saputro, Badriyatut Dini)
3
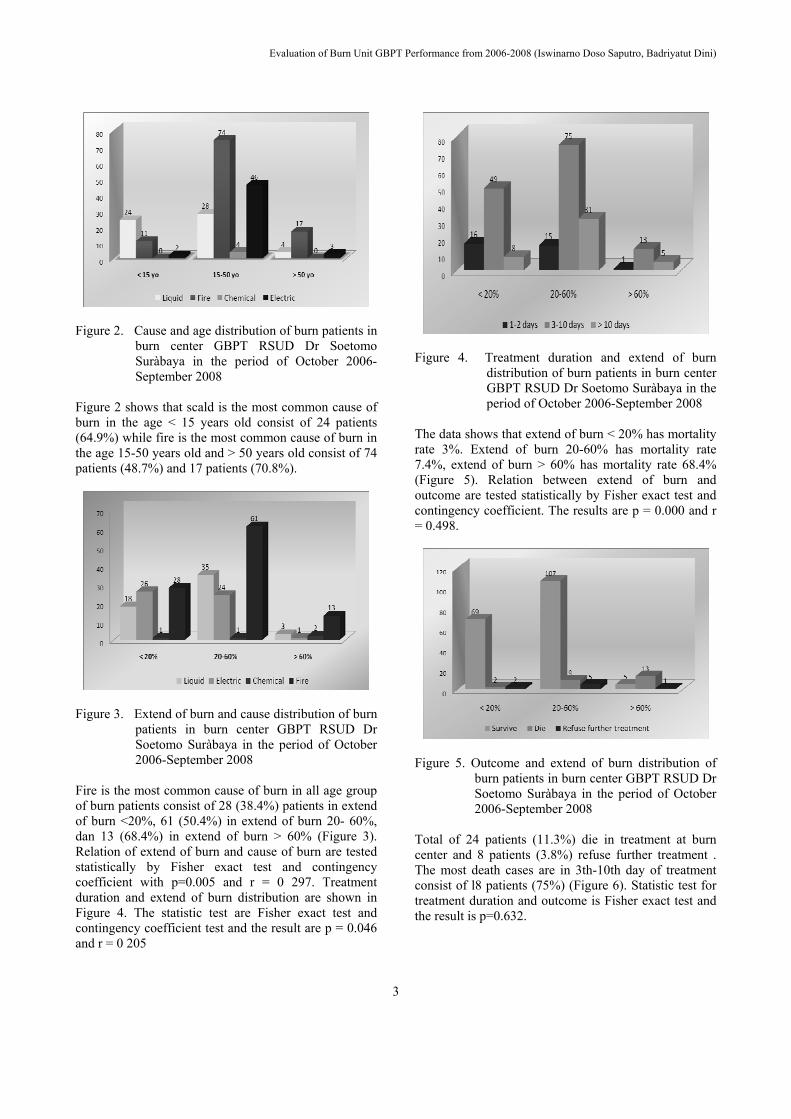
Figure 2. Cause and age distribution of burn patients in
burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Figure 2 shows that scald is the most common cause of burn in the age < 15 years old consist of 24 patients (64.9%) while fire is the most common cause of burn in the age 15-50 years old and > 50 years old consist of 74 patients (48.7%) and 17 patients (70.8%).
Figure 3. Extend of burn and cause distribution of burn
patients in burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Fire is the most common cause of burn in all age group of burn patients consist of 28 (38.4%) patients in extend of burn <20%, 61 (50.4%) in extend of burn 20- 60%, dan 13 (68.4%) in extend of burn > 60% (Figure 3). Relation of extend of burn and cause of burn are tested statistically by Fisher exact test and contingency coefficient with p=0.005 and r = 0 297. Treatment duration and extend of burn distribution are shown in Figure 4. The statistic test are Fisher exact test and contingency coefficient test and the result are p = 0.046 and r = 0 205
Figure 4. Treatment duration and extend of burn
distribution of burn patients in burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
The data shows that extend of burn < 20% has mortality rate 3%. Extend of burn 20-60% has mortality rate 7.4%, extend of burn > 60% has mortality rate 68.4% (Figure 5). Relation between extend of burn and outcome are tested statistically by Fisher exact test and contingency coefficient. The results are p = 0.000 and r = 0.498.
Figure 5. Outcome and extend of burn distribution of
burn patients in burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
Total of 24 patients (11.3%) die in treatment at burn center and 8 patients (3.8%) refuse further treatment . The most death cases are in 3th-10th day of treatment consist of l8 patients (75%) (Figure 6). Statistic test for treatment duration and outcome is Fisher exact test and the result is p=0.632.

Folia Medica Indonesiana Vol. 47 No. 1 January - March 2011 : 1-5
4
Figure 6. Outcome and treatment duration distribution
of burn patients in burn center GBPT RSUD Dr Soetomo Suràbaya in the period of October 2006-September 2008
DISCUSSION Prevalence and pattern of burn injury different in everywhere, depends on culture, daily activities, and technology, industry development. Adult burn injury may also result from an industrial or work-related accident or occur as a result of suicide attempt and assault. A large urban population will have an increased frequency of burn-trauma injuries. Table 1 shows that most of the domiciles are outside of Surabaya. The ratio of outside Surabaya and Surabaya is 3:2. It is different with the ratio before, it possibly due to many information of burn center RSUD dr. Soetomo. Talkshows, media information of burn injury can decrease burn incidence in Surabaya (Thomas 2003, Deirdre 2006) In this study, table 2 shows that the incidence of burn is higher in male. Male-to-female ratio is 1.8:1. Male is more active than female, may cause that. In addition, productive age is also affect higher incidents of this burn injury significantly, 71.4% of all burn injury cases in male and female at burn center RSUD dr. Soetomo. At Figure 1 shows fire is the most cause 47.9%. This mostly happened in children caused by carelessness of parents and babysitter at home. Matthew and John wrote that burn injuries result from a variety of causes. Scald burns are the most common cause of burn injury in the civilian population. Flame burns, the next most common cause of burn injury, typically result from house fires, campfires, and the burning of leaves or trash (Hunt & Purdue 2000, Matthew 2007)
At Figure 2 shows scald is the most common cause of age group < 15 years old (64.9%). Olivia wrote that scald burns are the leading cause of pediatric burn admissions and related morbidity, as well as a major cause of pediatric death.1–4 These injuries disproportionately affect the 0- to 4-year age group with the vast majority occurring in the home. Fire is the most common cause in age group 15-50 years old and age > 50 years (48.7%) and (70.8%). Assault and child abuse are significant contributory factors to burn-trauma injuries in this population (Hunt & Purdue 2000, Olivia 2003, Thomas 2003, James 2006, Mathew 2007) Figure 3 shows that fire is the most common of all extend of burn group. Relation between extend of burn and cause of burn are tested statistically by Fisher exact test and contingency coefficient and the results are p=0.005, r= 0 297. There is significant relation between extend of burn and cause of burn. Fire causes burn injury wider and deeper of wound than hot liquid which is caused, Thermal trauma from fire can reach hundred even thousand degree Celcius, also explosion effect can attack on face, so increase possibility inhalation trauma and affect prognosis of patients. Thermal injury causes coagulation necrosis of the skin and underlying tissues to a variable depth. Burn injury also exerts deleterious effects on all other organ systems (Garner 2000, Hunt & Purdue 2000, Matthew 2007) On this study, electric causes wide of burn injury under 15% and fire cause wider than 15%. This shows, electric doesn’t cause wide burn injury but affect damage of tissues more progressive and deeper, so burn injury by electric ended up with extremity amputation and rehabilitation handle important role in this case. Electric can destructs body tissue by conversion to thermal energy along the tissue so the tissue damage cannot be identified clinically only. (Hunt & Purdue 2000, McCauley 2000, Matthew 2007) At Figure 4 shows distribution of treatment duration and wide of burn injury have significant correlation with p=0.046, r=0 205. The more extend of burn injury the more extend of tissue damage that happened. This is also affect damage of body system more complex. In the end, this is caused duration of treatment were needed in patient’s management (Matthew 2007) Figure 5 shows that extend of burn > 60% has the highest mortality rate (68.4%). Correlation between wide of burn injury between outcome shows significant correlation with p=0.001, r=0.498. Many factors became the parameter of burn injury prognosis, wide of burn injury isn’t the only factor in determination of patient’s management. In this study, mostly all patients that has burn injury over 60% could not survive. Marc wrote that

Evaluation of Burn Unit GBPT Performance from 2006-2008 (Iswinarno Doso Saputro, Badriyatut Dini)
5
extend of burn > 40% is the survival limit while Arvind wrote the survival limit is the extend of burn > 75% (Nathan 2000, Sheridan 2000, Arvind 2004, Marc 2008) In this study, 11.3% of patients die in the treatment and 3.8% refuse further treatment at burn center GBPT. It is lower than amount in last year that reached 20%. The most death case in day 3-10 treatment comprised 18 patients (75%) and all dead patients (Figure 6). Significant test of correlation between duration of treatment and outcome shows that there is no significant correlation, p= 0.632. Both of them were related with many factors such as wide of burn injury and age that influenced prognoses. In North America, burn injury is one of the main causes of injury deaths, particularly in children under the age of 14 years. Increased mortality rates for young children are associated with increased cardiac work and impaired cardiac function but not with the inflammatory and hypermetabolic responses. The highest fatality rates occur among children 4 years of age or younger and adults over the age of 55 years. Burn-related deaths in these two age groups account for more than two-thirds of all fire deaths. Males are twice as likely to die of burn-related injury as females. Recent advances in burn care, such as metabolic support, control of infections, resuscitation, early excision and grafting of the burn wounds, and treatment of inhalation injury have improved outcomes for severely burned children and adults. The essence of successful burn care is the team. No individuals capable of meeting the many acute and long-term needs of the burn patient. Consequently, burn care is best delivered in a specialized burn center where experienced physicians, nurses, physical and occupational therapists, nutritionists, psychologists, and social workers can all participate in the care of the individual (Deirdre 2006, Matthew 2007, Marc 2008). CONCLUSION The proportion of burn death 2006-2008 is 11,3%. Burn incidence occurs twice more frequent in male than in female, with the ratio of 1,8. Fire is the most common cause of burn in productive age. Cause of burn affects
the extent of burn significantly, while the latter has significant effects on treatment duration and outcome. Whereas, duration of treatment has no significant effect on the outcome. REFERENCES 1. Arvind N P, Maria Siemionow. Burns. Handbook
of Plastic Surgery. 2004. P 175-86. 2. Deirdre C et al, Burn Wound Infections. Clinical
Microbiology Reviews, 19 (2). 2006 , p. 403–434. 3. Garner W. Thermal Burns. In: Russel RC, editor.
Plastic Surgery. Indication, Operations and Outcomes. St.Louis: Mosby; 2000. p.357-73.
4. James H et al. Burns. Schwartz’s Manual of Surgery Eight Edition. 2006. P 138-64
5. Hunt JL, Purdue GF. Burns: Acute Burns, Burn Surgery, and Postburn Reconstruction. Selected Readings in Plactic Surgery; 9(12). 2000. P 1-30
6. Marc G et al. Age Differences in Inflammatory and Hypermetabolic Postburn Responses. Pediatrics. 121 (3), 2008, p 497-507. Available from http://www.pediatrics.org
7. Matthew B. Klein, Thermal, Chemical and Electrical Injuries. Grabb and Smith's Plastic Surgery, Sixth Edition. Lippincott Williams & Wilkins; 2007. p.132-49.
8. McCauley R, Barret J. Electrical Injuries. In: Russel RC, editor. Plastic Surgery. Indication, Operations and Outcomes. St.Louis: Mosby; 2000. p.375-385
9. Nathan A et al, A Model of Infected Burn Wounds Using Escherichia coli O18:K1:H7 for the Study of Gram-Negative Bacteremia and Sepsis. Infection and Immunity. 68 (6). 2000, p 3349-51
10. Olivia T, Baxter AL. Accidental Scald Burns in Sinks. Pediatrics. 111 (2), 2003, p 191- 4. Available from http://www.pediatrics.org
11. Sheridan RL et al. Long-term Outcome of Children Surviving Massive Burns. JAMA. 283 (1), 2000, p 69-73. Available from http://jama.amaassn.org
12. Thomas K et al. Frequency of Burn-Trauma Patients in an Urban Setting. Arch Surg. 13, 2003, p 1292-96. Available from www.archsurg.com
13.





























