Embed Size (px)
Citation preview

1
Ikuo Hirano, MDGastroenterology DivisionNorthwestern University Medical School
CSGNA Fall into GI Conference
Evaluation and Management of Dysphagia
Dysphagia Management
1. Evaluation of dysphagia
2. Dilation methods: pros and cons
3. Specific disease examples
1. Schatzki ring
2. Achalasia
3. Eosinophilic esophagitis
4. Refractory strictures
Dysphagia
Structural
Solid DysphagiaSolid & Liquid
Dysphagia
Motility
Esophageal
Dysphagia
Dysphagia localized to
chest or neck, food
impaction
Dysphagia localized to
neck, nasal regurgitation,
aspiration, associated ENT
symptoms
Oropharyngeal
Dysphagia
Esophageal Dysphagia:
Motility Disorders
Achalasia
Diffuse Esophageal Spasm
Scleroderma
Polymyositis
Esophageal Dysphagia Structural Etiologies
Schatzki ring
Eosinophilic esophagitis
Peptic stricture
Iatrogenic (radiation, surgery,
endoscopic therapy)
Esophageal neoplasm
Caustic injury
Esophageal diverticula
Esophageal web
Congenital esophageal stenosis
Diagnostic Testing for Esophagus
• Upper GI Series/Esophagram/Barium swallow
• Endoscopy
• Esophageal manometry
• Esophageal impedance manometry
• Impedance planimetry
• Endoscopic ultrasonography
2
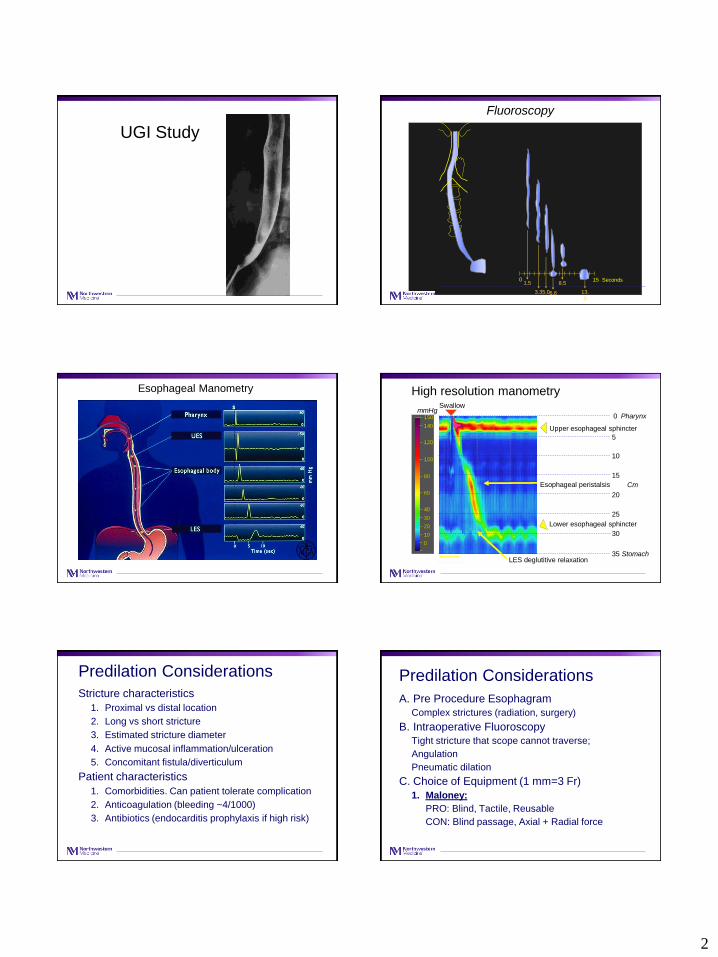
UGI Study
0 15 Seconds1.5
3.35.06.6
8.5
13.
0
Fluoroscopy
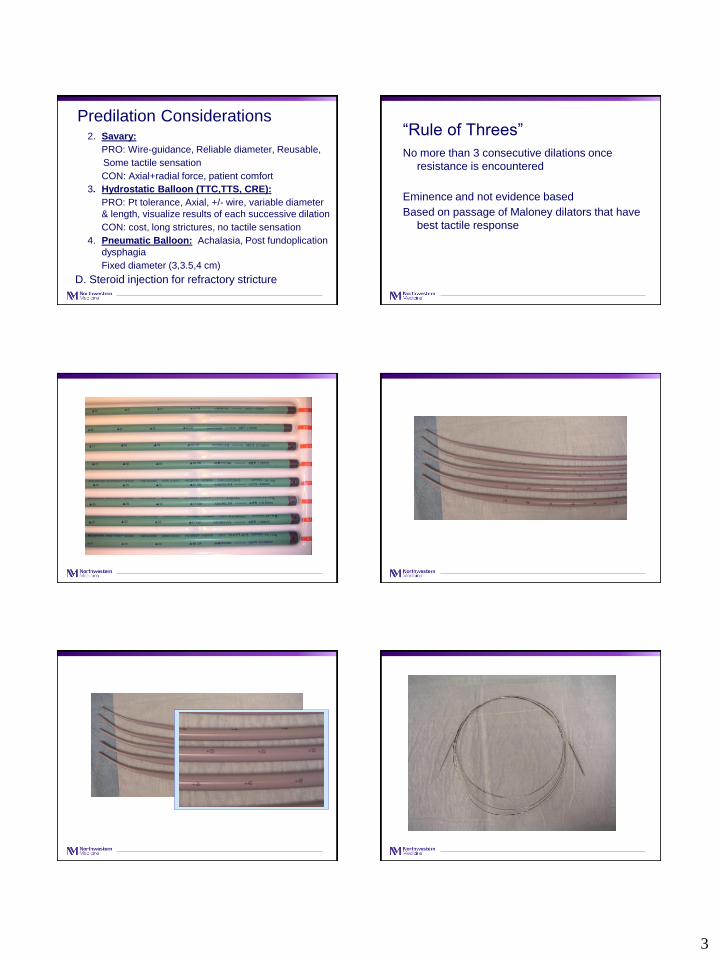
Esophageal Manometry High resolution manometry
20 seconds
Swallow
Esophageal peristalsis
LES deglutitive relaxation
Upper esophageal sphincter
Lower esophageal sphincter
0
5
10
15
20
25
30
35
Pharynx
Stomach
Cm
140
120
100
80
60
40
30
20
10
0
150mmHg
Predilation Considerations
Stricture characteristics
1. Proximal vs distal location
2. Long vs short stricture
3. Estimated stricture diameter
4. Active mucosal inflammation/ulceration
5. Concomitant fistula/diverticulum
Patient characteristics
1. Comorbidities. Can patient tolerate complication
2. Anticoagulation (bleeding ~4/1000)
3. Antibiotics (endocarditis prophylaxis if high risk)
Predilation Considerations
A. Pre Procedure Esophagram
Complex strictures (radiation, surgery)
B. Intraoperative Fluoroscopy
Tight stricture that scope cannot traverse;
Angulation
Pneumatic dilation
C. Choice of Equipment (1 mm=3 Fr)
1. Maloney:
PRO: Blind, Tactile, Reusable
CON: Blind passage, Axial + Radial force
3
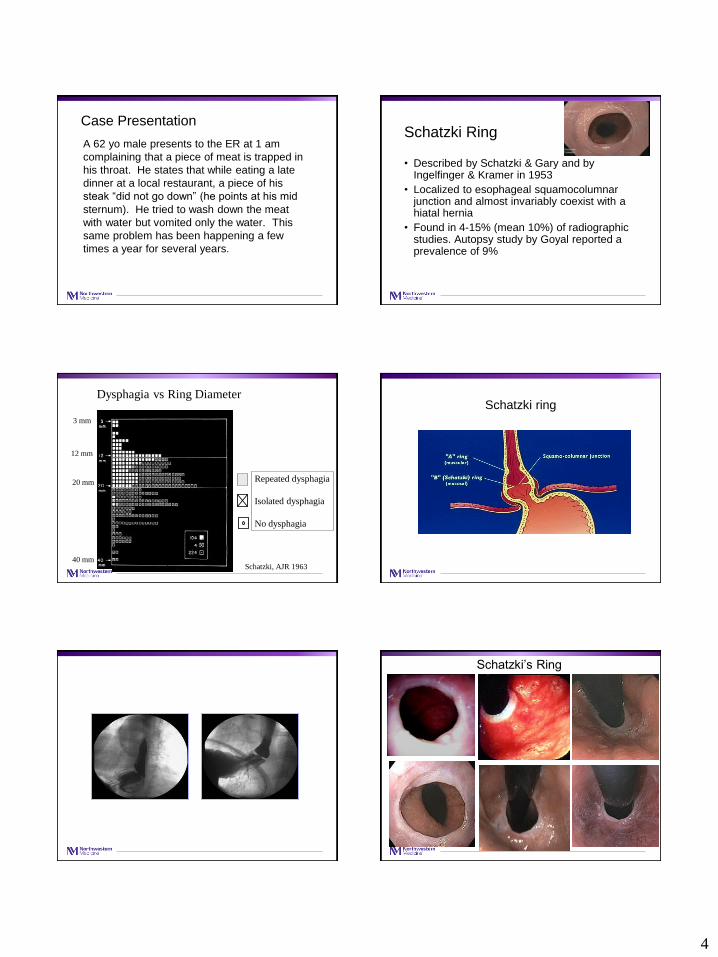
Predilation Considerations2. Savary:
PRO: Wire-guidance, Reliable diameter, Reusable,
Some tactile sensation
CON: Axial+radial force, patient comfort
3. Hydrostatic Balloon (TTC,TTS, CRE):
PRO: Pt tolerance, Axial, +/- wire, variable diameter
& length, visualize results of each successive dilation
CON: cost, long strictures, no tactile sensation
4. Pneumatic Balloon: Achalasia, Post fundoplication
dysphagia
Fixed diameter (3,3.5,4 cm)
D. Steroid injection for refractory stricture
“Rule of Threes”
No more than 3 consecutive dilations once
resistance is encountered
Eminence and not evidence based
Based on passage of Maloney dilators that have
best tactile response
4
Case Presentation
A 62 yo male presents to the ER at 1 am
complaining that a piece of meat is trapped in
his throat. He states that while eating a late
dinner at a local restaurant, a piece of his
steak “did not go down” (he points at his mid
sternum). He tried to wash down the meat
with water but vomited only the water. This
same problem has been happening a few
times a year for several years.
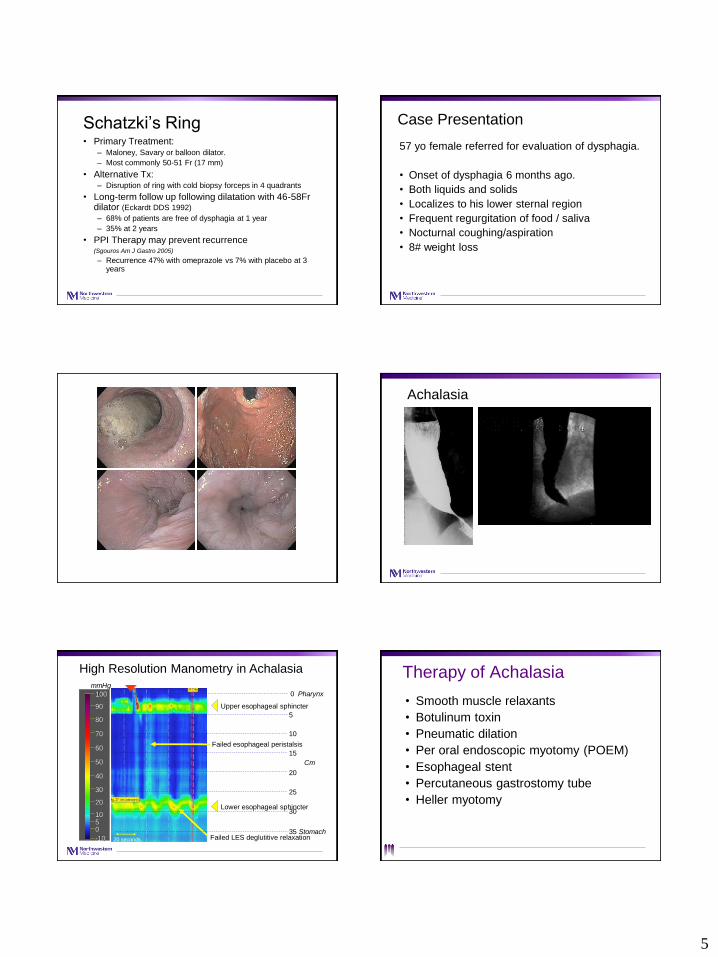
Schatzki Ring
• Described by Schatzki & Gary and by Ingelfinger & Kramer in 1953
• Localized to esophageal squamocolumnar junction and almost invariably coexist with a hiatal hernia
• Found in 4-15% (mean 10%) of radiographic studies. Autopsy study by Goyal reported a prevalence of 9%
Schatzki, AJR 1963
Dysphagia vs Ring Diameter
Repeated dysphagia
Isolated dysphagia
No dysphagia
3 mm
12 mm
20 mm
40 mm
Schatzki ring
Schatzki’s Ring
5
Schatzki’s Ring• Primary Treatment:
– Maloney, Savary or balloon dilator.
– Most commonly 50-51 Fr (17 mm)
• Alternative Tx: – Disruption of ring with cold biopsy forceps in 4 quadrants
• Long-term follow up following dilatation with 46-58Fr dilator (Eckardt DDS 1992)
– 68% of patients are free of dysphagia at 1 year
– 35% at 2 years
• PPI Therapy may prevent recurrence (Sgouros Am J Gastro 2005)
– Recurrence 47% with omeprazole vs 7% with placebo at 3 years
Case Presentation
57 yo female referred for evaluation of dysphagia.
• Onset of dysphagia 6 months ago.
• Both liquids and solids
• Localizes to his lower sternal region
• Frequent regurgitation of food / saliva
• Nocturnal coughing/aspiration
• 8# weight loss
Achalasia
QuickTime™ and aYUV420 codec decompressor
are needed to see this picture.
High Resolution Manometry in Achalasia
20 seconds
Swallow
Failed LES deglutitive relaxation
90
80
70
60
50
30
20
1050
-10
100
mmHg
40
Upper esophageal sphincter
Lower esophageal sphincter
0
5
10
15
20
25
30
35
Pharynx
Stomach
Cm
Failed esophageal peristalsis
Therapy of Achalasia
• Smooth muscle relaxants
• Botulinum toxin
• Pneumatic dilation
• Per oral endoscopic myotomy (POEM)
• Esophageal stent
• Percutaneous gastrostomy tube
• Heller myotomy
6
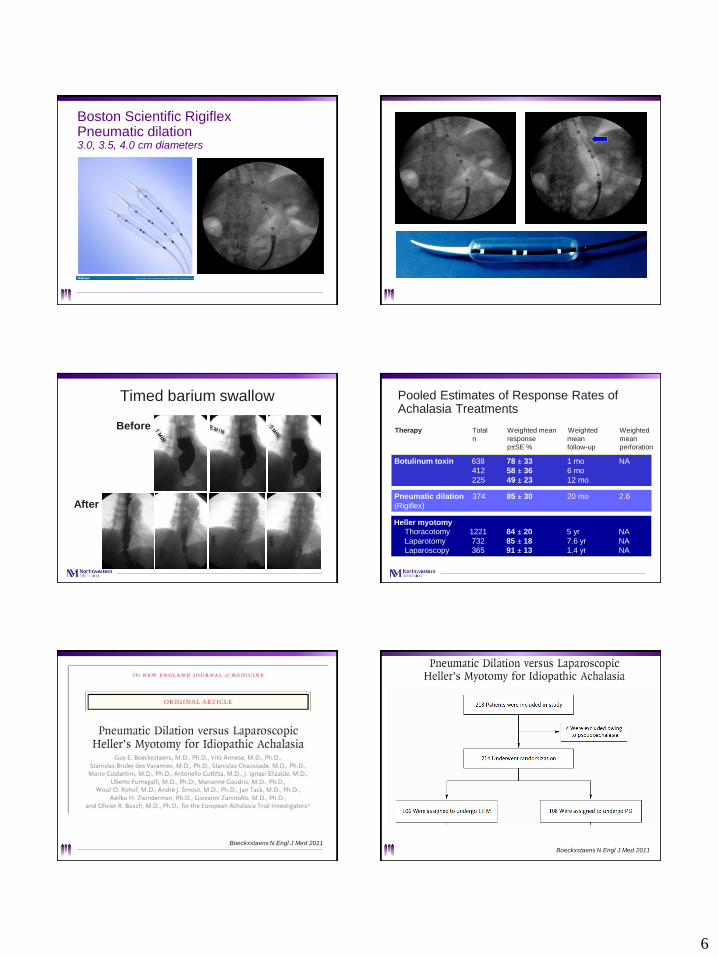
Boston Scientific RigiflexPneumatic dilation3.0, 3.5, 4.0 cm diameters
Before
After
Timed barium swallow Pooled Estimates of Response Rates of Achalasia Treatments
Therapy Total Weighted mean Weighted Weighted
n response mean mean
p±SE % follow-up perforation
Botulinum toxin 638 78 ± 33 1 mo NA
412 58 ± 36 6 mo
225 49 ± 23 12 mo
Pneumatic dilation 374 85 ± 30 20 mo 2.6
(Rigiflex)
Heller myotomy
Thoracotomy 1221 84 ± 20 5 yr NA
Laparotomy 732 85 ± 18 7.6 yr NA
Laparoscopy 365 91 ± 13 1.4 yr NA
Boeckxstaens N Engl J Med 2011Boeckxstaens N Engl J Med 2011

7
Boeckxstaens N Engl J Med 2011
Effectiveness of pneumatic dilation is comparable to laparoscopic Heller myotomy IF allow for
repeated dilations and accept risk of esophageal perforation
Case Presentation• 42 year old male presents with 12 years of intermittent
dysphagia for solids that localizes to his mid sternum. Symptoms have been progressive; now occurring on a daily basis. He has had repeated food impactions after eating meat or bread that last up to 1 hour. He was seen in the ER on 2 occasions for endoscopic disimpaction.
It takes the patient over an hour to complete his meals. He is embarrassed when he needs to leave the table during meals to vomit up food that he cannot swallow.
The patient was previously diagnosed with GERD and esophageal spasm.
PMH includes childhood asthma and allergic rhinitis.
Eosinophilic Esophagitis 2011
Liacouras et al. Eosinophilic Esophagitis Updated Consensus Recommendation.
J Allergy Clin Immunol 2011
EoE is a clinicopathologic disease
• Clinically, EoE is characterized by symptoms related to
esophageal dysfunction
• Pathologically, 1 or more biopsy specimens must show
eosinophil-predominant inflammation. With few exceptions,
15 eos/hpf is considered a minimum threshold for the
diagnosis of EoE
• The disease is isolated to the esophagus, and other
causes of esophageal eosinophilia should be excluded
EoE is increasing over past 2 decades in both children and adults worldwide
Prasad Clin Gastro Hepatol 2009; Hruz J Allergy Clin Immunol 2011;
DeBrosse J Allergy Clin Immunol 2010; Dellon Aliment Pharm Ther 2015
Olmstead County, MN (peds/adults) Olten County, Switzerland
Hamilton County, OH (peds) Denmark
Epidemiology of EoE in USHealth insurance database 2009-11 of 11.5 million;
Prevalence based on ICD9 (530.13) 57/100,000
Dellon Clin Gastro Hep 2014; 12 (4): 589
Eosinophilic Esophagitis
Clinical Features in Adults
• Male predominant ~70%
• Age at diagnosis: 35-40
• Atopy (asthma, allergic rhinitis, atopic dermatitis): ~70%
• Primary symptoms: dysphagia, food impaction
• Secondary symptoms: heartburn, chest pain
• Symptom duration prior to diagnosis: 5 years

8
Etiology of Dysphagia Retrospective Study 1371 Adults Undergoing EGD for dysphagia
Kidambi, Toto, Hirano World J Gastro 2012
1999 2009
EoE
GERD GERD
The 2 am “Wake up” Call!
EoE identified in 11-55% of adults with food impaction
Desai Furuta Gastrointest Endosc 2005;61:795
Gonsalves Sanger Zhang Hirano Am J Gastro 2006;101, S66
Kerlin Jones Remedios Campbell J Clin Gastro 2007;41:256
Byrne Peterson Fang Dig Dis Sci 2007; 52: 717
Sengupta Lembo Aliment Pharm Therap 2015; 42; 91
Hirano Am J Gastro 2016
Role of Endoscopy in EoEClassify and grade severity of characteristic findings of
Edema, Rings, Exudates, Furrows, Strictures (EREFS)
Hirano Moy Heckman Thomas Gonsalves Achem. Gut. 2012.
Normal Eosinophilic Esophagitis
Edema (loss vascular markings)Grade 0: Distinct vascularityGrade 1: Decreased Grade 2: Absent
Rings (trachealization)Grade 0: NoneGrade 1: Mild (ridges)Grade 2: Moderate (distinct rings)Grade 3: Severe (not pass scope)
Exudate (white plaques)Grade 0: NoneGrade 1: Mild (<10% surface area)Grade 2: Severe (>10% surface area)
Furrows (vertical lines)Grade 0: NoneGrade 1: Mild Grade 2: Severe (depth)
StrictureGrade 0: AbsentGrade 1: Present
Grade 0 Grade 1 Grade 2 Grade 3EoE Endoscopic Reference Score (EREFS)
Hirano Gut. 2013
Complications of EoE:Narrow caliber esophagus
Hirano Aceves Gastro Clin North Am 2014;43(2):297-316.
EoE inflammation+ Fibrosis
EoE FibrosisEoE inflammation
. .
Normal
EGD
Histo
EoE: A Conceptual Model of Clinical Subtypes Based On Inflammation and Tissue Remodeling
DilationMedical/Diet Therapy
Hirano Aceves Gastro Clin North Am 2014;43(2):297-316.

9
3 D’s of Treatment for EoE• Drugs
– Topical steroids
– Systemic steroids
– Leukotriene antagonists (montelukast)
– Mast cell stabilizers (cromolyn sodium)
– Immunomodulators (CRTH2 antagonist, azathioprine)
– Biologics (anti IL5, anti IL13, anti TNF, anti IgE)
• Dietary Therapy
– Empiric elimination diet
– Allergy testing directed elimination diet
– Elemental diet
• Dilation (Endoscopic therapy)
Suggested Algorithm for ManagementOf Eosinophilic Esophagitis
Suspected EoE
PPI x 8 wks
EGD with Bx
“PPI Responsive Esophageal Eosinophilia” (EoE vs GERD)
Symptom relief &Normal histology
EoE
> 15 Eos/hpf
Topical steroidDietary therapy
EGD with Bx
Elimination diet
↑ Dose topical
Systemic steroid
Biologic therapy ?
Persistent Symptoms and Pathology
Esophageal
dilation
Persistent dysphagiawith stricture
Consider Maintenance Therapy
Symptom relief &Normal histology
Hirano. Eosinophilic Esophagitis (Liacouras Ed). 2011
Esophageal Dilation in EoE Prior to 2008High risk of Esophageal Complications
8 cases; 3 dilations
1 perforation with EGD
5 dilations
5 large lacerations
with EGD or dilation
1 dilation
1 perforation
6 dilations
3 perforations
Esophageal Dilation in EoE 2012:Low risk of Esophageal Complications
474 dilations
0 perforations
70 dilations
0 perforations
15 dilations
0 perforations
293 dilations
3 perforations
• Retrospective study of 474 dilations in 207 adults
• 63 patients treated with dilation alone
• 93% of patients reported slight or no dysphagia after dilation
• Esophageal diameter increased from 11 mm pre to 16 mm post dilation
• 3 mm incremental dilation per session; median 2 sessions per patient (range 1-13)
• Median duration symptom improvement: 15 mos
• No perforations
Schoepfer AM, et al. Am J Gastroenterol 2010;105:1062-70
Esophageal Dilation in EoE: Effectiveness, Safety and Impact on Underlying Inflammation
121
104
0
50
100
150
(n=63)
Pre-Dilation
Post-Dilation
Peak e
osi
nophil
/ hpf
Esophageal Dilation Does Not Affect the Underlying Esophageal Inflammatory ProcessDilation without anti-eosinophil therapy
Schoepfer AM, et al. Am J Gastroenterol 2010;105:1062-70
10
Schoepfer AM, et al. Am J Gastroenterol 2010;105:1062-70
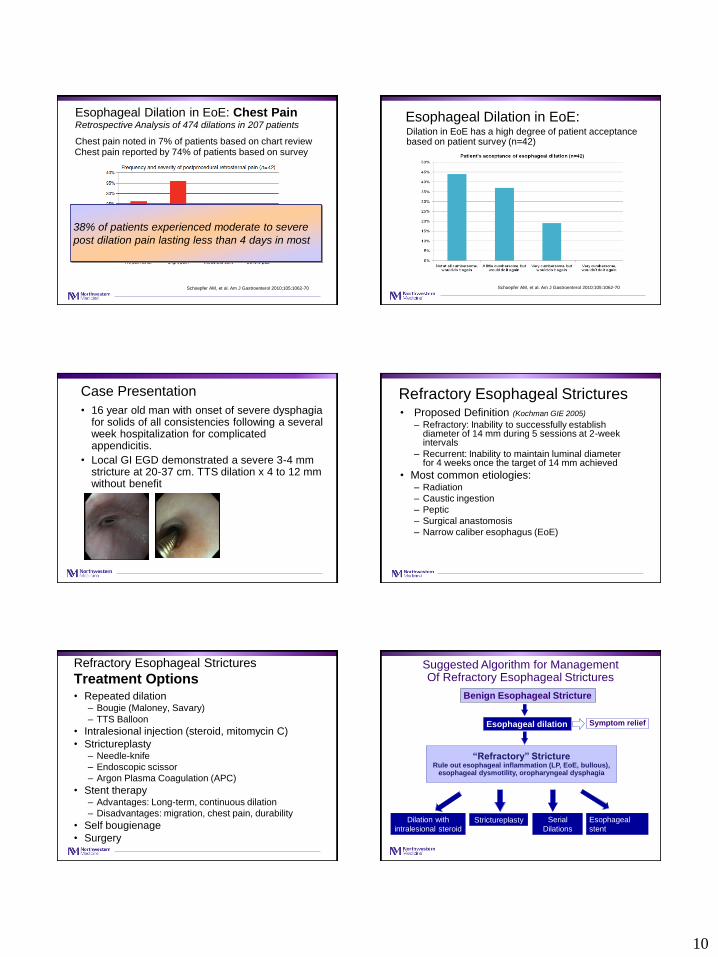
Chest pain noted in 7% of patients based on chart reviewChest pain reported by 74% of patients based on survey
Esophageal Dilation in EoE: Chest Pain Retrospective Analysis of 474 dilations in 207 patients
38% of patients experienced moderate to severe
post dilation pain lasting less than 4 days in most
Schoepfer AM, et al. Am J Gastroenterol 2010;105:1062-70
Dilation in EoE has a high degree of patient acceptance based on patient survey (n=42)
Esophageal Dilation in EoE:
Case Presentation
• 16 year old man with onset of severe dysphagia for solids of all consistencies following a several week hospitalization for complicated appendicitis.
• Local GI EGD demonstrated a severe 3-4 mm stricture at 20-37 cm. TTS dilation x 4 to 12 mm without benefit
Refractory Esophageal Strictures• Proposed Definition (Kochman GIE 2005)
– Refractory: Inability to successfully establish diameter of 14 mm during 5 sessions at 2-week intervals
– Recurrent: Inability to maintain luminal diameter for 4 weeks once the target of 14 mm achieved
• Most common etiologies:– Radiation
– Caustic ingestion
– Peptic
– Surgical anastomosis
– Narrow caliber esophagus (EoE)
Siersema Wijkerslooth Gastroint Endosc 2009
Refractory Esophageal Strictures
Treatment Options
Siersema Wijkerslooth Gastroint Endosc 2009
• Repeated dilation– Bougie (Maloney, Savary)
– TTS Balloon
• Intralesional injection (steroid, mitomycin C)
• Strictureplasty– Needle-knife
– Endoscopic scissor
– Argon Plasma Coagulation (APC)
• Stent therapy – Advantages: Long-term, continuous dilation
– Disadvantages: migration, chest pain, durability
• Self bougienage
• Surgery
Suggested Algorithm for ManagementOf Refractory Esophageal Strictures
Benign Esophageal Stricture
Esophageal dilation Symptom relief
Dilation with
intralesional steroidStrictureplasty Esophageal
stent
Serial
Dilations
“Refractory” StrictureRule out esophageal inflammation (LP, EoE, bullous),
esophageal dysmotility, oropharyngeal dysphagia
11
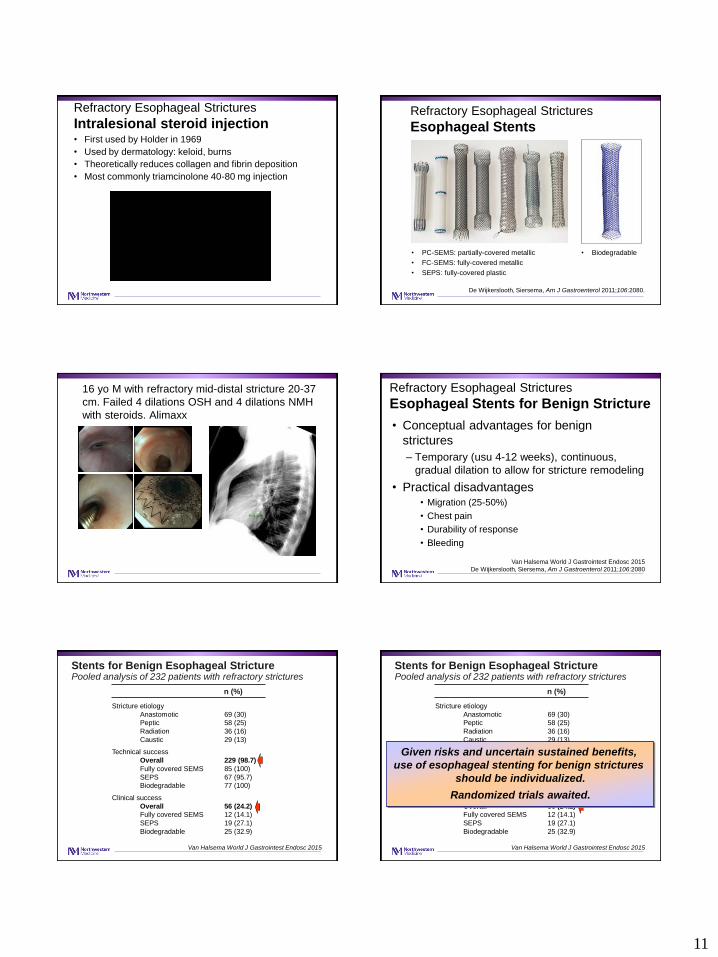
Refractory Esophageal Strictures
Intralesional steroid injection• First used by Holder in 1969
• Used by dermatology: keloid, burns
• Theoretically reduces collagen and fibrin deposition
• Most commonly triamcinolone 40-80 mg injection
Refractory Esophageal Strictures
Esophageal Stents
Siersema Wijkerslooth Gastroint Endosc 2009
• PC-SEMS: partially-covered metallic
• FC-SEMS: fully-covered metallic
• SEPS: fully-covered plastic
De Wijkerslooth, Siersema, Am J Gastroenterol 2011;106:2080.
• Biodegradable
Siersema Wijkerslooth Gastroint Endosc 2009
16 yo M with refractory mid-distal stricture 20-37
cm. Failed 4 dilations OSH and 4 dilations NMH
with steroids. Alimaxx
Refractory Esophageal Strictures
Esophageal Stents for Benign Stricture
Siersema Wijkerslooth Gastroint Endosc 2009
• Conceptual advantages for benign
strictures
– Temporary (usu 4-12 weeks), continuous,
gradual dilation to allow for stricture remodeling
• Practical disadvantages• Migration (25-50%)
• Chest pain
• Durability of response
• Bleeding
Van Halsema World J Gastrointest Endosc 2015
De Wijkerslooth, Siersema, Am J Gastroenterol 2011;106:2080
Stents for Benign Esophageal StricturePooled analysis of 232 patients with refractory strictures
n (%)
Stricture etiology
Anastomotic 69 (30)
Peptic 58 (25)
Radiation 36 (16)
Caustic 29 (13)
Technical success
Overall 229 (98.7)
Fully covered SEMS 85 (100)
SEPS 67 (95.7)
Biodegradable 77 (100)
Clinical success
Overall 56 (24.2)
Fully covered SEMS 12 (14.1)
SEPS 19 (27.1)
Biodegradable 25 (32.9)
Van Halsema World J Gastrointest Endosc 2015
Stents for Benign Esophageal StricturePooled analysis of 232 patients with refractory strictures
n (%)
Stricture etiology
Anastomotic 69 (30)
Peptic 58 (25)
Radiation 36 (16)
Caustic 29 (13)
Technical success
Overall 229 (98.7)
Fully covered SEMS 85 (100)
SEPS 67 (95.7)
Biodegradable 77 (100)
Clinical success
Overall 56 (24.2)
Fully covered SEMS 12 (14.1)
SEPS 19 (27.1)
Biodegradable 25 (32.9)
Van Halsema World J Gastrointest Endosc 2015
Given risks and uncertain sustained benefits,
use of esophageal stenting for benign strictures
should be individualized.
Randomized trials awaited.

12
Management of
Esophageal Strictures
Steroid injection and stents may reduce frequency of dilation for benign stricture
Esophageal stents are an option for refractory strictures but sustained resolution in < 25%
Pneumatic dilation is highly effective for treatment of achalasia and equivalent to surgical myotomy IF allow for aggressive dilation protocol
Esophageal dilation is safe and effective for esophageal strictures in eosinophilic esophagitis





























