Embed Size (px)
Citation preview
Evaluating the Hypoxic PatientEvaluating the Hypoxic Patient
Catherine J. Markin MDPulmonary and Critical CareNoon Conference 2004
GoalsGoals
Discuss mechanisms of hypoxia Explore clinical/lab tests for hypoxia Provide a “framework” for evaluation of
patients with hypoxia
You are called by a 7CVA nurse who is taking care of You are called by a 7CVA nurse who is taking care of patient LB. LB is a 52 y/o woman with rheumatoid patient LB. LB is a 52 y/o woman with rheumatoid arthritis and a TKA 3 days ago. The nurse reports that arthritis and a TKA 3 days ago. The nurse reports that LB is requiring 3L/min nc oxygen to maintain a SpOLB is requiring 3L/min nc oxygen to maintain a SpO22 of 89%, but is otherwise not distressed. The nurse of 89%, but is otherwise not distressed. The nurse comments that the only thing the patient is comments that the only thing the patient is complaining of is a sore throat for which prn cetacaine complaining of is a sore throat for which prn cetacaine spray is being used. The nurse thinks that the patient spray is being used. The nurse thinks that the patient might benefit from a bronchodilator and asks if you might benefit from a bronchodilator and asks if you would give her a verbal order.would give her a verbal order.
You are in the middle of dinner and are tempted to You are in the middle of dinner and are tempted to give the order. But instead you decide to give the order. But instead you decide to evaluate the patient yourself. As you are evaluate the patient yourself. As you are walking across the bridge, you are thinking walking across the bridge, you are thinking about the following clinical questions:about the following clinical questions:
1.1. Is the patient in respiratory distress and in Is the patient in respiratory distress and in need of immediate assistance in breathing?need of immediate assistance in breathing?
2.2. What is the differential diagnosis of What is the differential diagnosis of hypoxia in this patient?hypoxia in this patient?
3.3. What are the appropriate clinical tests that What are the appropriate clinical tests that can help sort out the cause of hypoxia?can help sort out the cause of hypoxia?
1.1. Is the patient in respiratory distress and in Is the patient in respiratory distress and in need of immediate assistance in breathing?need of immediate assistance in breathing?
2.2. What is the differential diagnosis of hypoxia in this What is the differential diagnosis of hypoxia in this patient?patient?
3.3. What are the appropriate clinical tests that can help What are the appropriate clinical tests that can help sort out the cause of hypoxia?sort out the cause of hypoxia?

HypoxiaHypoxia::– Inadequate utilization of oxygen by cellsInadequate utilization of oxygen by cells
HypoxemiaHypoxemia:: – Abnormally low oxygen in the bloodAbnormally low oxygen in the blood
Clinical Signs of HypoxiaClinical Signs of Hypoxia
Cyanosis Restlessness/agitation Tachypnea Tachycardia Confusion +/- Low SpO2
Indications for Endotracheal IntubationIndications for Endotracheal Intubation
Airway protection Relief of airway obstruction Shock Facilitation of suctioning/pulm toilet Reducing work of breathing Respiratory failure
Hypercapnic Hypoxic
Upon your arrival, pt is breathing 14/min and with Upon your arrival, pt is breathing 14/min and with complaints of vague chest constriction but no complaints of vague chest constriction but no pain. The nurse hands you an EKG that is pain. The nurse hands you an EKG that is significant only for ST 120 bpm. You note the significant only for ST 120 bpm. You note the patients patients cigarettescigarettes next to the bed and she has next to the bed and she has an an epidural in placeepidural in place. Lungs with faint bibasilar . Lungs with faint bibasilar crackles. The patient is crackles. The patient is obeseobese and you are and you are unsure of her JVP.unsure of her JVP.
1. Is the patient in respiratory distress and in need of immediate assistance in breathing?
2.2. What is the differential diagnosis of What is the differential diagnosis of hypoxia in this patient?hypoxia in this patient?
3. What are the appropriate clinical tests that can help sort out the cause of hypoxia?
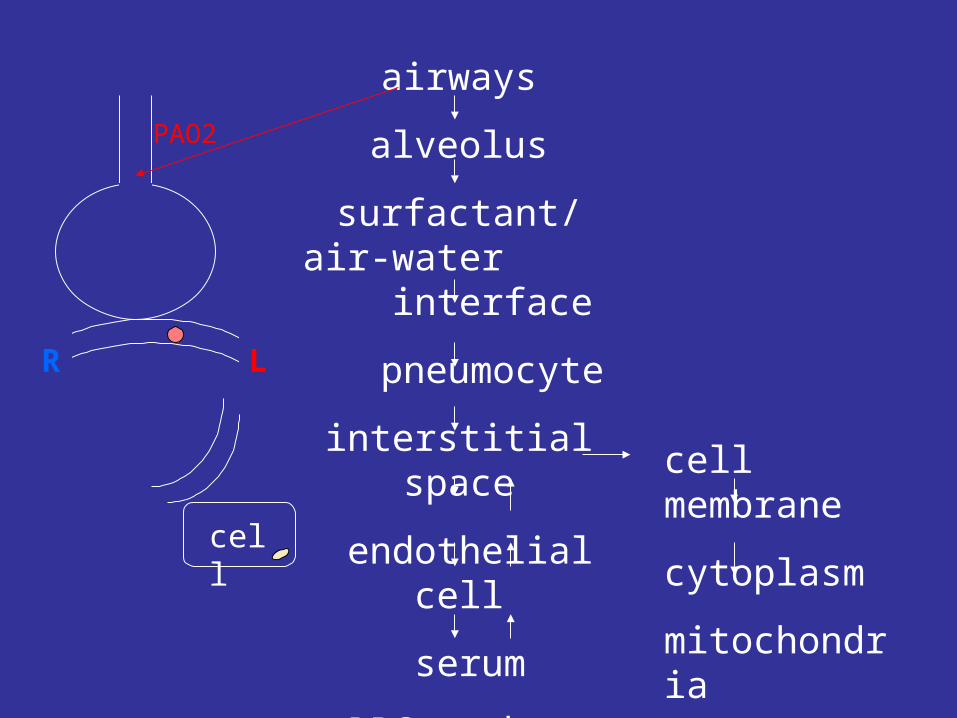
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Hypoventilation3. Low alveolar pressure4. Low FIO25. R to L Shunt (V>Q)6. Dead Space Ventilation (V<<Q) 7. Diffusion Impairment
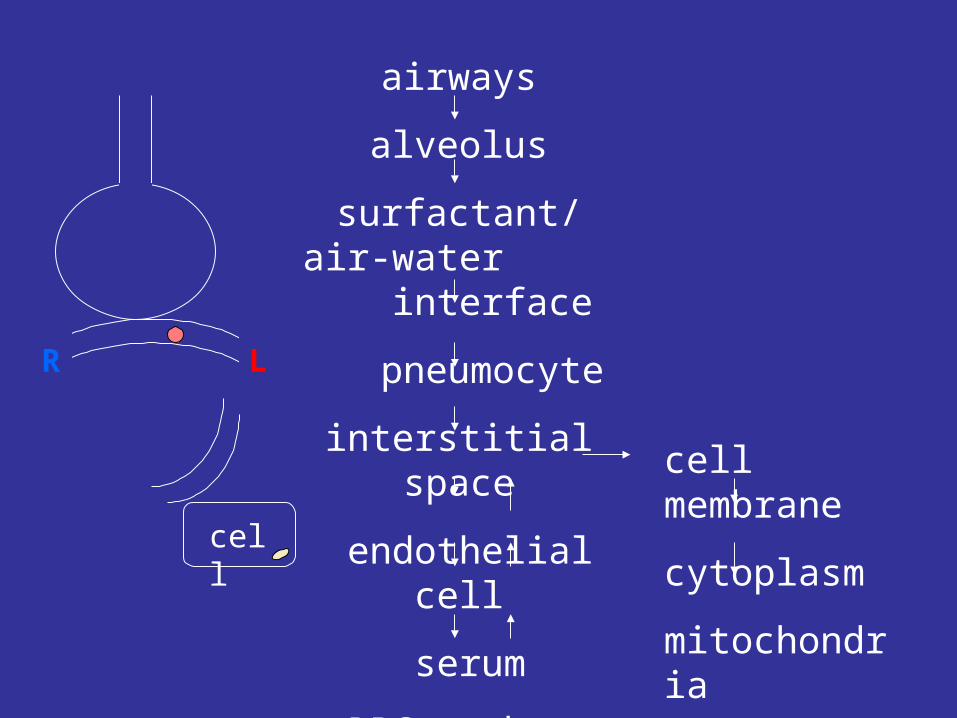
airways
alveolus
surfactant/air-water interface
pneumocyte
interstitial space
endothelial cell
serum
RBC membrane
hgb
cell membrane
cytoplasm
mitochondria
R LR
cell
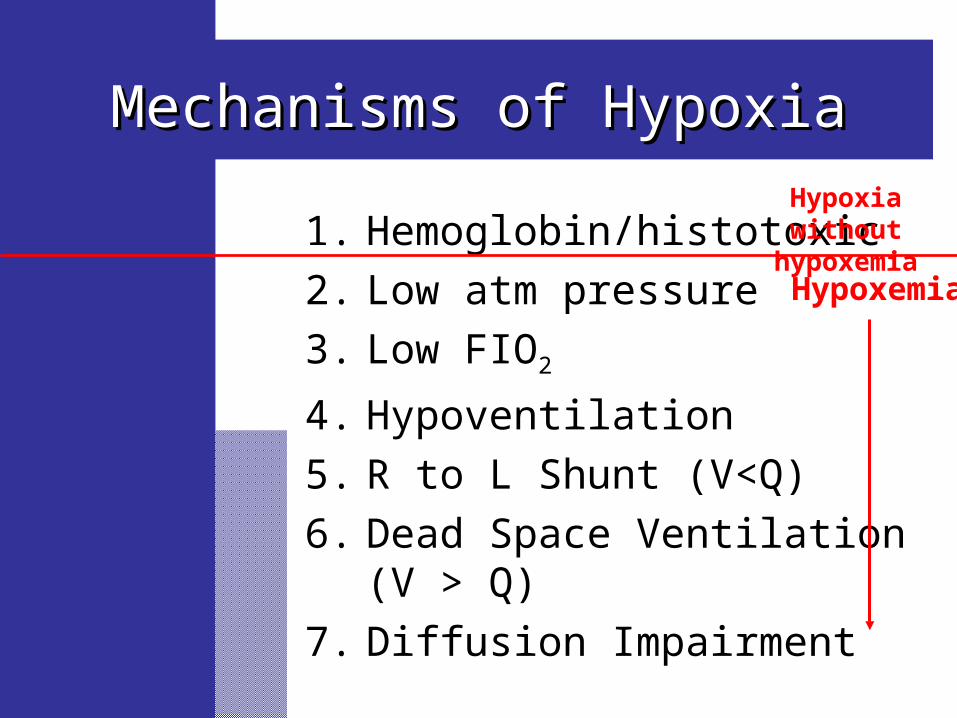
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V > Q) 7. Diffusion Impairment
Hypoxemia
Hypoxia without hypoxemia
Diagnosis of Hypoxia without Diagnosis of Hypoxia without HypoxemiaHypoxemia
– Physical or laboratory signs of Physical or laboratory signs of hypoxiahypoxia
– Adequate PaOAdequate PaO2 2 (>60 mmHg)(>60 mmHg)
– Normal or mildly abnormal SpONormal or mildly abnormal SpO22
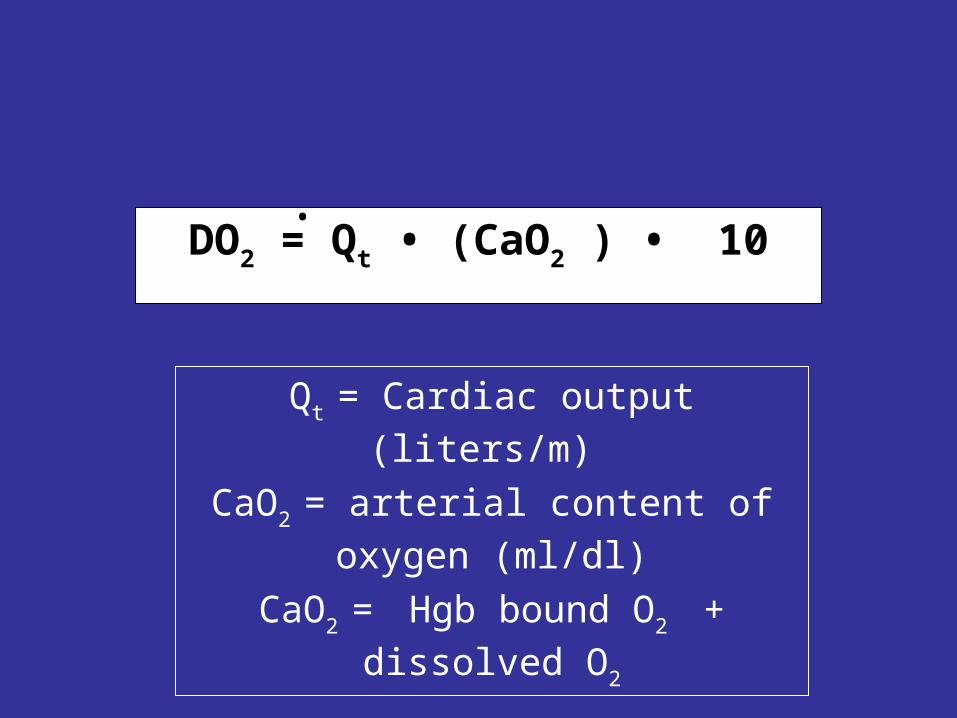
DO2 = Qt • (CaO2 ) • 10
Qt = Cardiac output (liters/m)
CaO2 = arterial content of oxygen (ml/dl)
CaO2 = Hgb bound O2 + dissolved O2
•
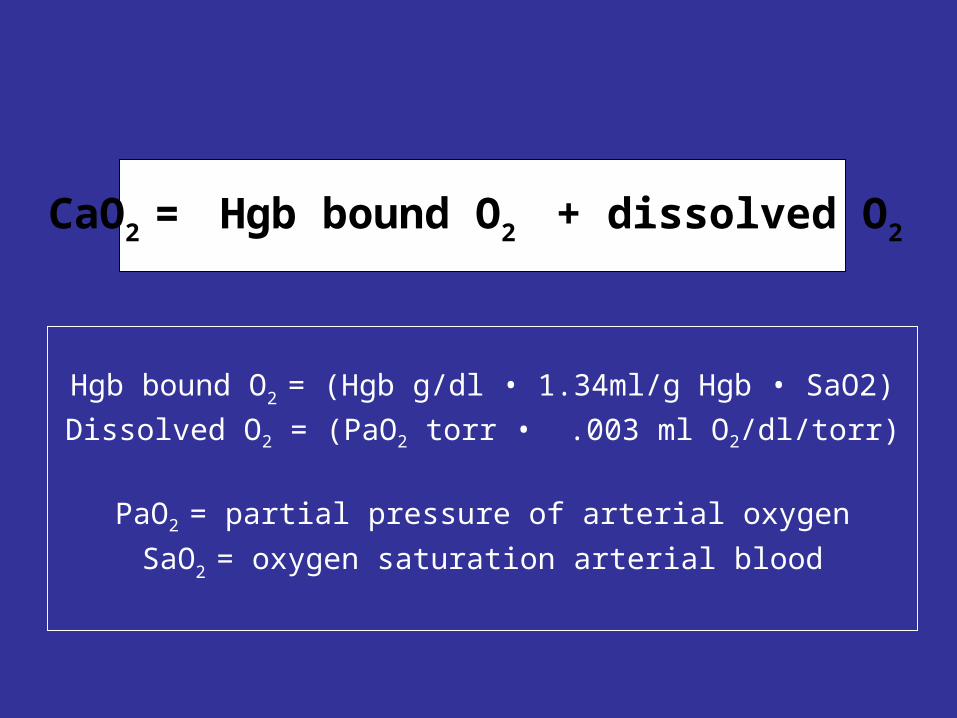
Hgb bound O2 = (Hgb g/dl • 1.34ml/g Hgb • SaO2)Dissolved O2 = (PaO2 torr • .003 ml O2/dl/torr)
PaO2 = partial pressure of arterial oxygenSaO2 = oxygen saturation arterial blood
CaO2 = Hgb bound O2 + dissolved O2
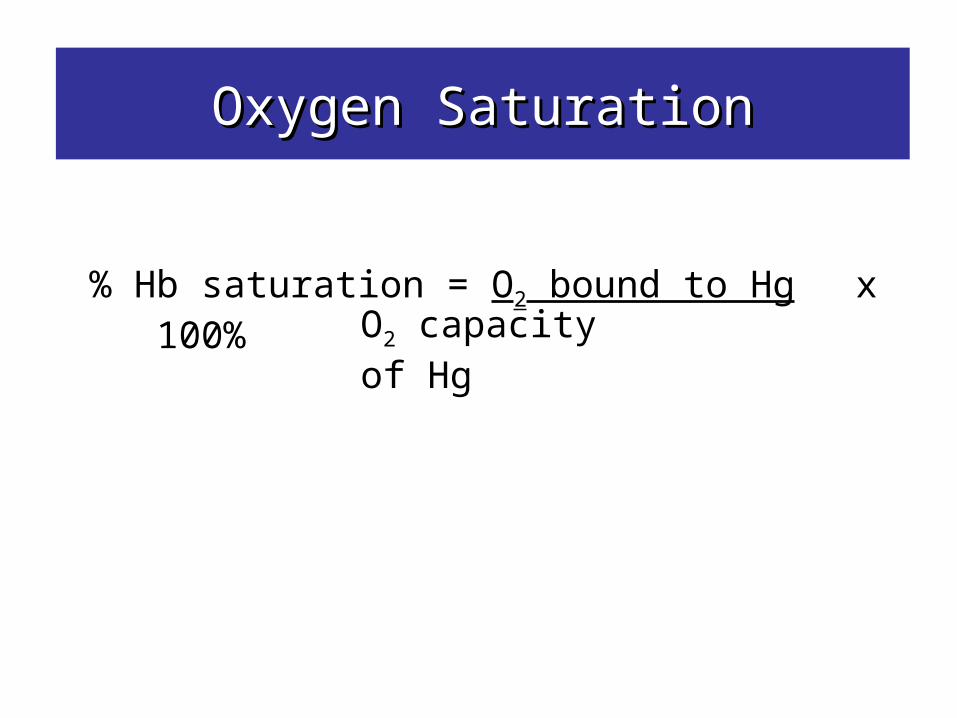
Oxygen SaturationOxygen Saturation
% Hb saturation = O2 bound to Hg x 100%O2 capacity of Hg
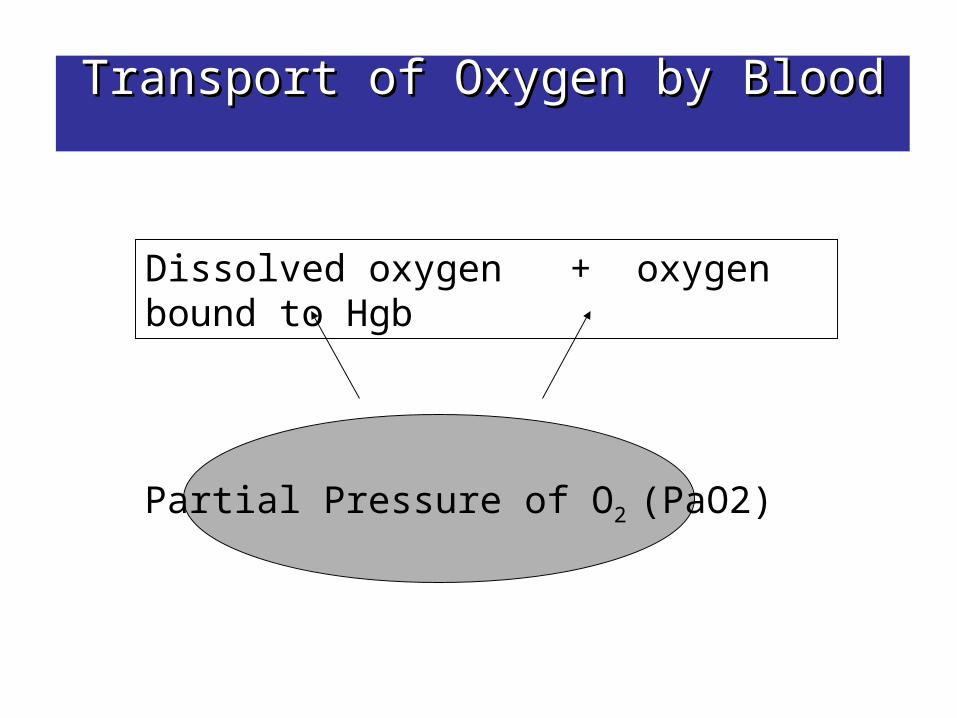
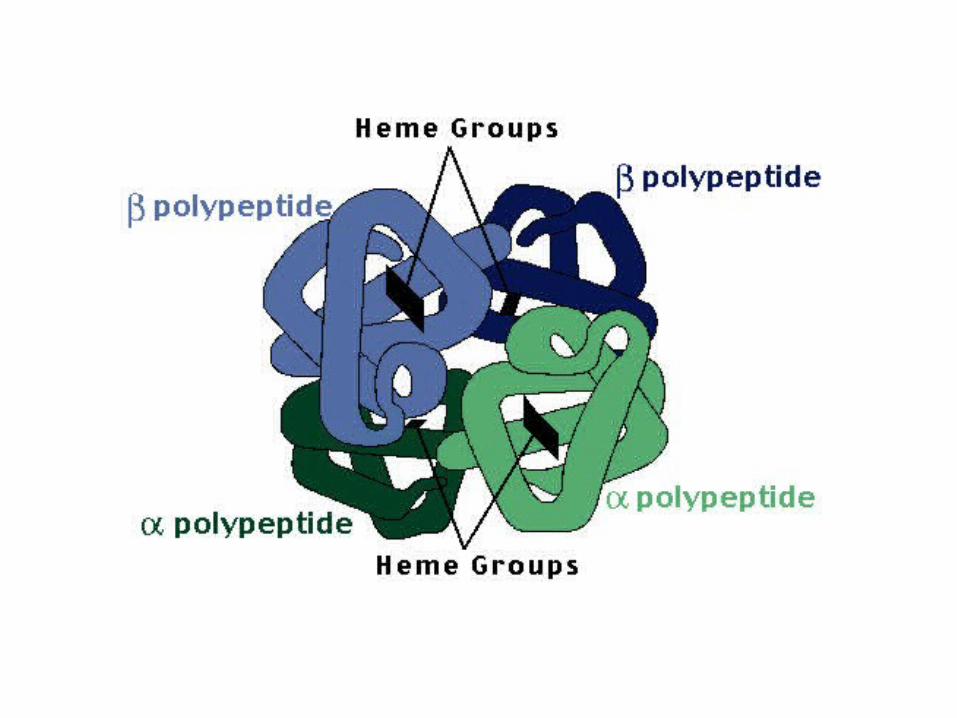
Transport of Oxygen by BloodTransport of Oxygen by Blood
Dissolved oxygen + oxygen bound to Hgb
Partial Pressure of O2 (PaO2)
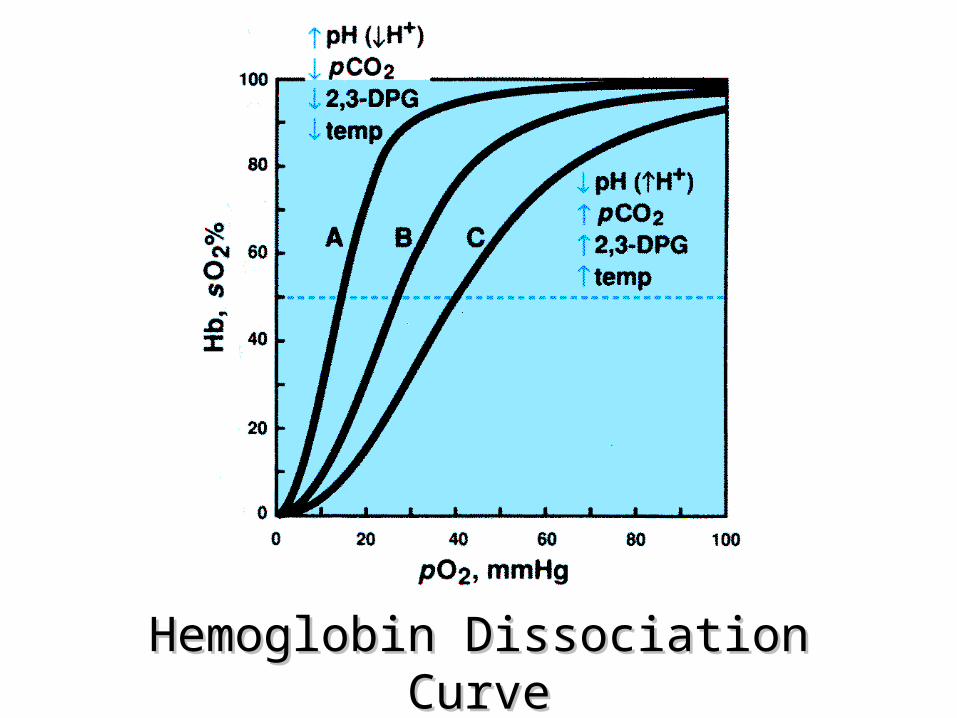
Hemoglobin Dissociation CurveHemoglobin Dissociation Curve
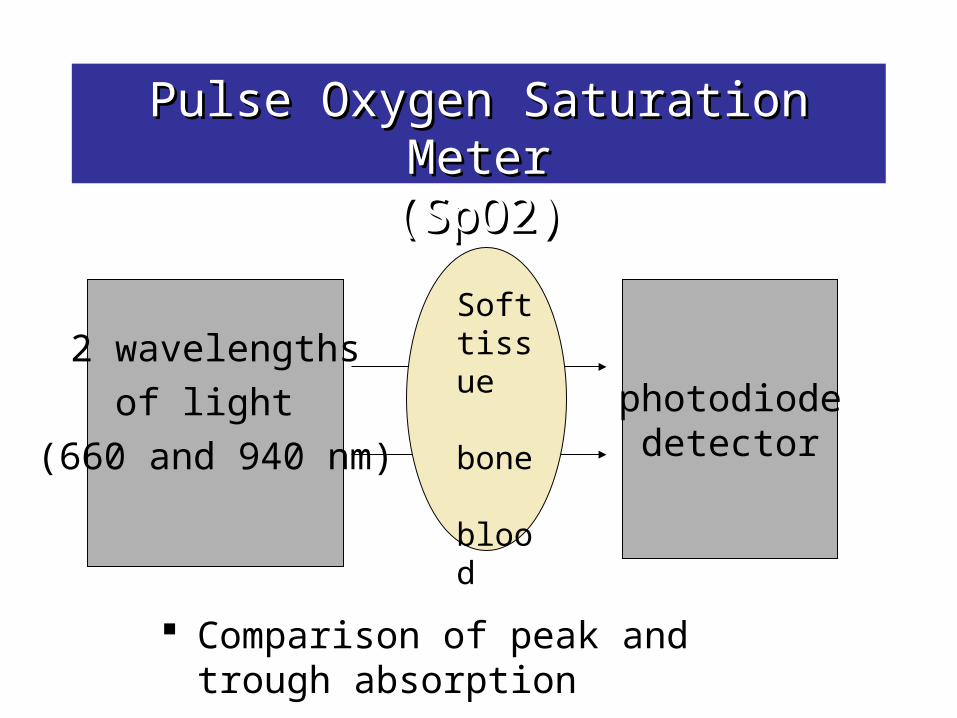
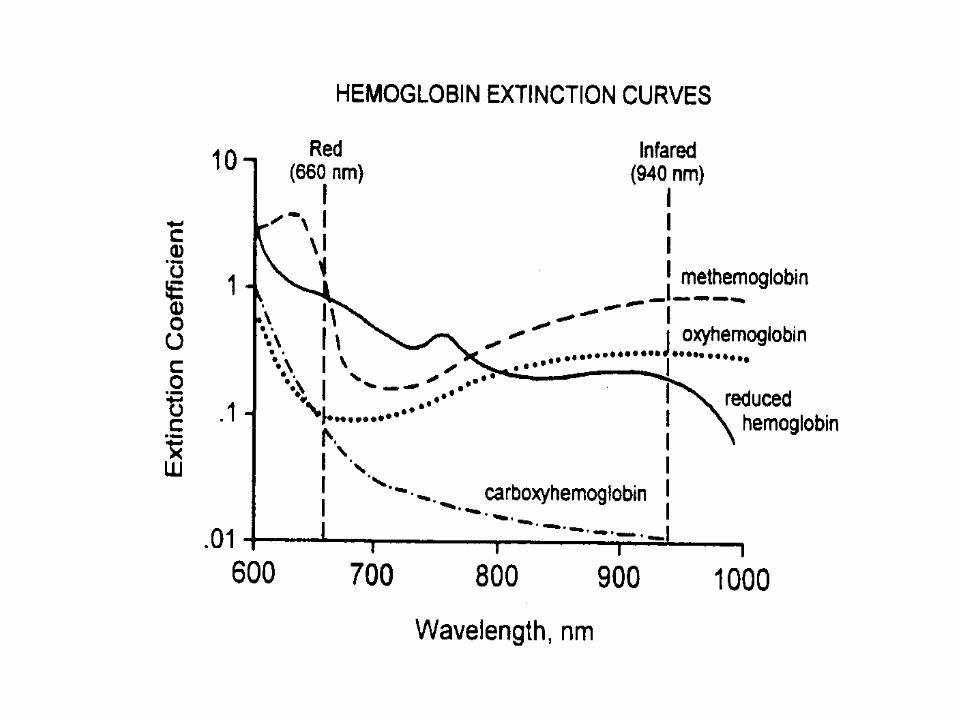
Pulse Oxygen Saturation MeterPulse Oxygen Saturation Meter(SpO2)(SpO2)
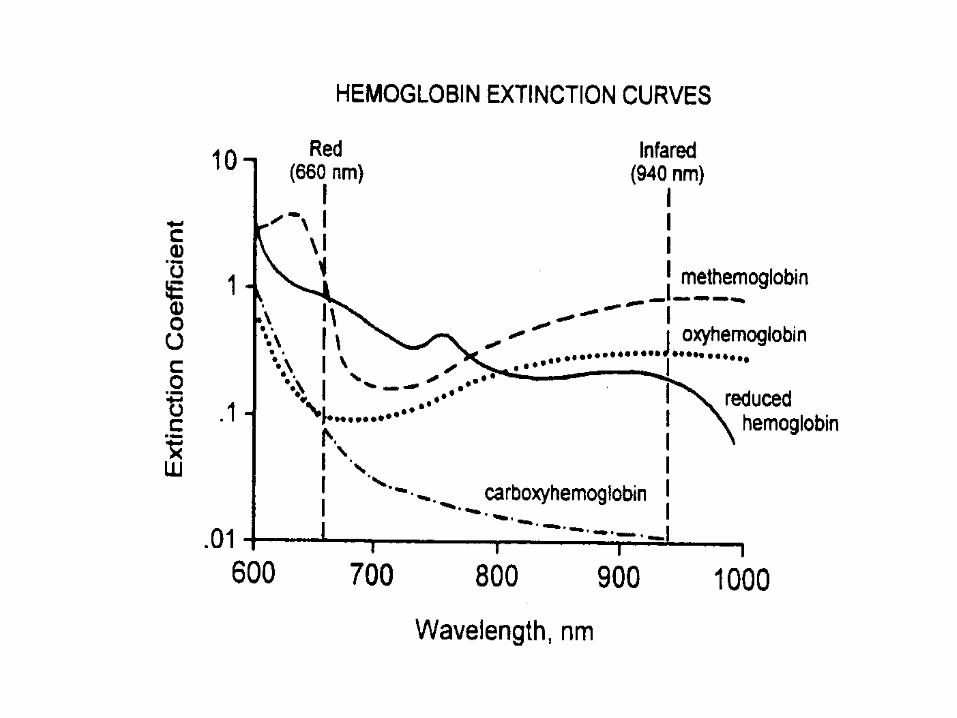
Comparison of peak and trough absorption
2 wavelengthsof light
(660 and 940 nm)
photodiodedetector
Soft tissue
bone
blood

pulsatile arterial blood
non-pulsatile arterial blood
venous and capillary blood
tissue

R = ratio
AC = pulsatile
DC = non pulsatile
2+
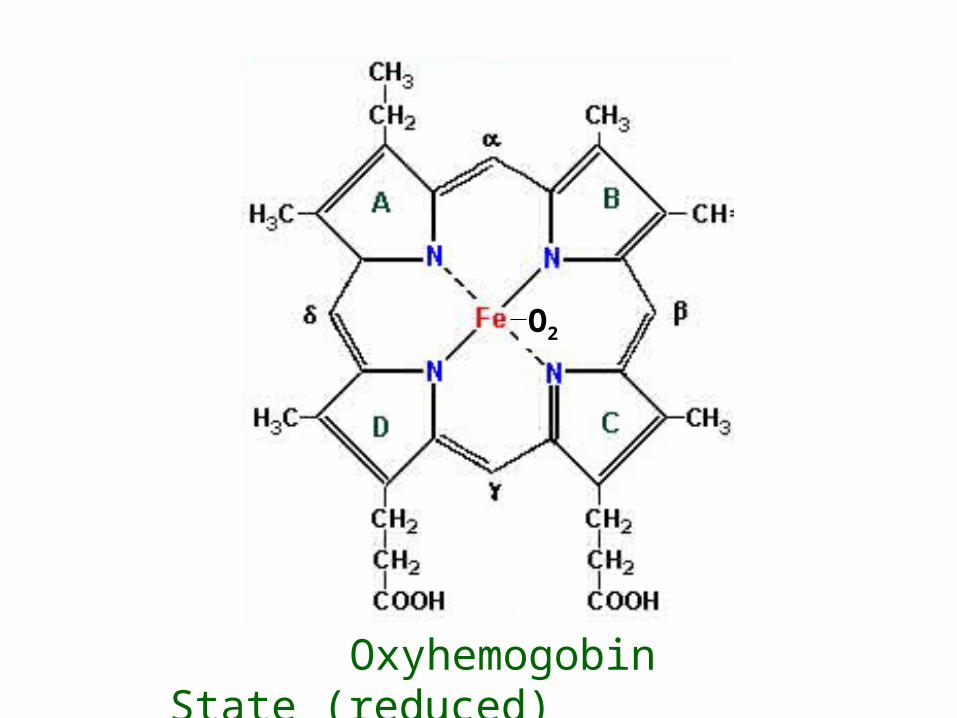
Heme Molecule in Ferrous State (reduced)
O2
Oxyhemogobin
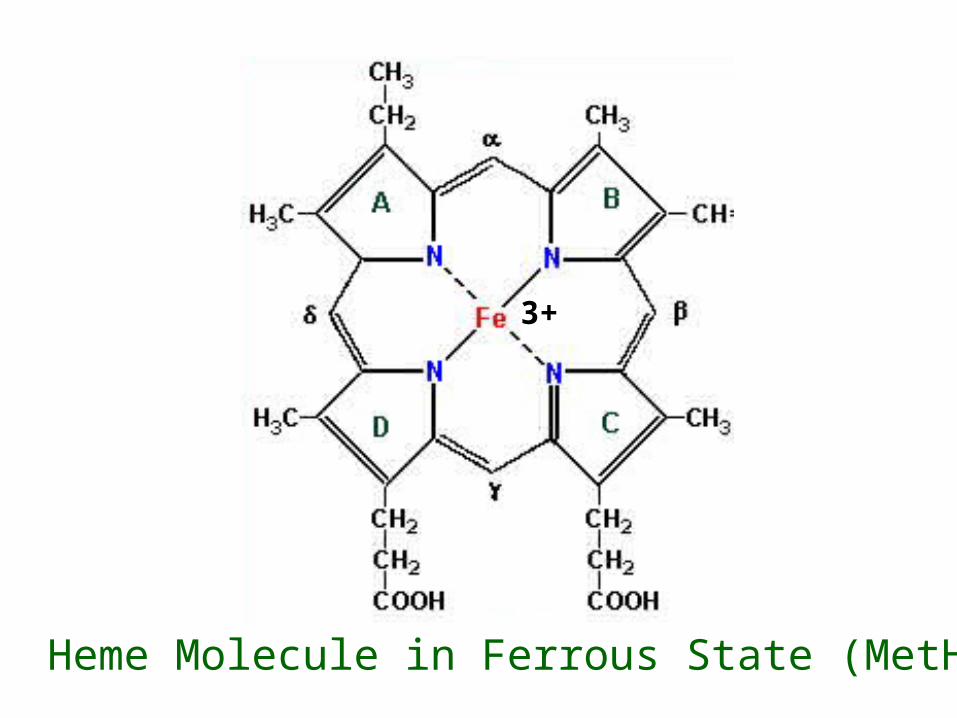
3+
Heme Molecule in Ferrous State (MetHgb)

MethemoglobinMethemoglobin
Heme in ferric (3+) state “Muddy brown” blood MetHgb saturation is 85% , SpO2 89% Absorption at 660 nm and 940 nm are equal Peak absorption 631 nm Causes: Congenital defect in enzyme metHgb
reductase, high level or chronic exposure to anoxidizing agent (benzocaine, dapsone, fava beans)
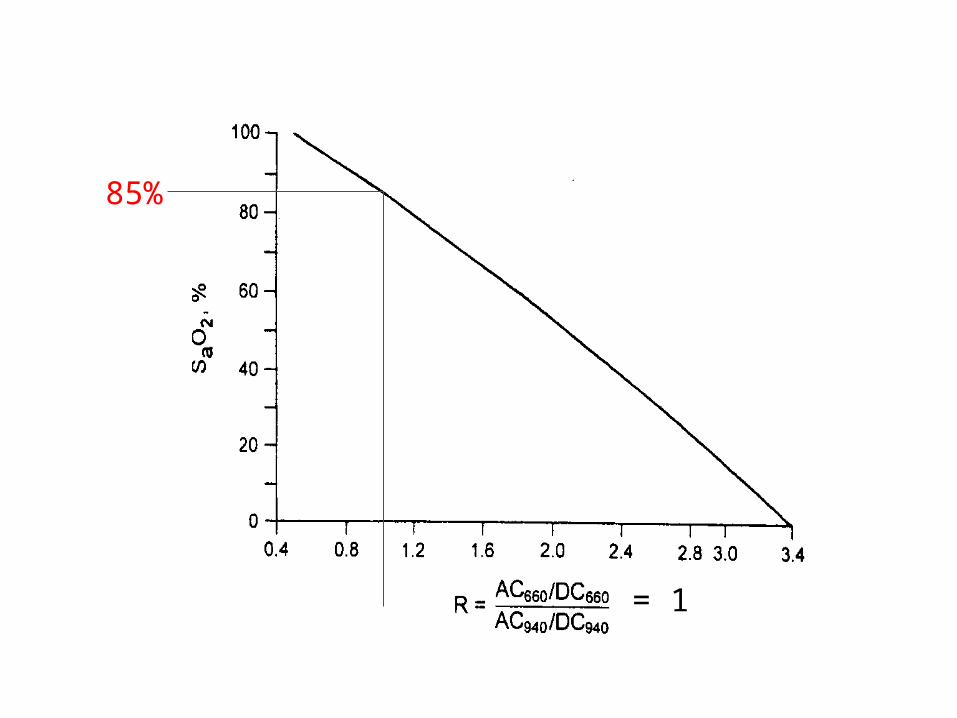
= 1
85%
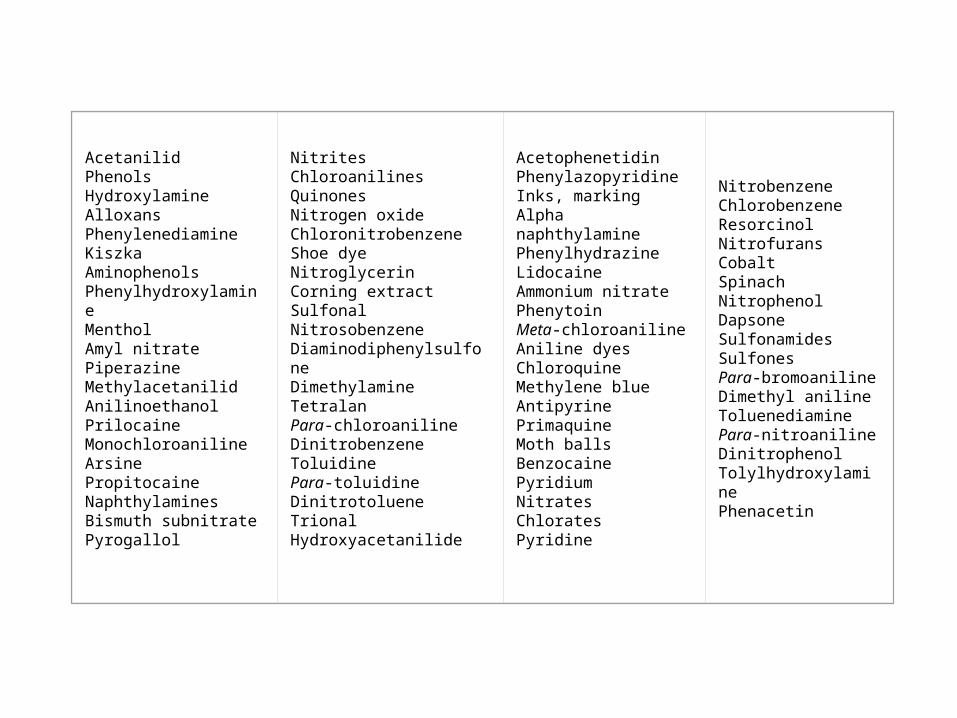
AcetanilidPhenolsHydroxylamineAlloxansPhenylenediamineKiszkaAminophenolsPhenylhydroxylamineMentholAmyl nitratePiperazineMethylacetanilidAnilinoethanolPrilocaineMonochloroanilineArsinePropitocaineNaphthylaminesBismuth subnitratePyrogallol
NitritesChloroanilinesQuinonesNitrogen oxideChloronitrobenzeneShoe dyeNitroglycerinCorning extractSulfonalNitrosobenzeneDiaminodiphenylsulfoneDimethylamineTetralanPara-chloroanilineDinitrobenzeneToluidinePara-toluidineDinitrotolueneTrionalHydroxyacetanilide
AcetophenetidinPhenylazopyridineInks, markingAlpha naphthylaminePhenylhydrazineLidocaineAmmonium nitratePhenytoinMeta-chloroanilineAniline dyesChloroquineMethylene blueAntipyrinePrimaquineMoth ballsBenzocainePyridiumNitratesChloratesPyridine
NitrobenzeneChlorobenzeneResorcinolNitrofuransCobaltSpinachNitrophenolDapsoneSulfonamidesSulfonesPara-bromoanilineDimethyl anilineToluenediaminePara-nitroanilineDinitrophenolTolylhydroxylaminePhenacetin
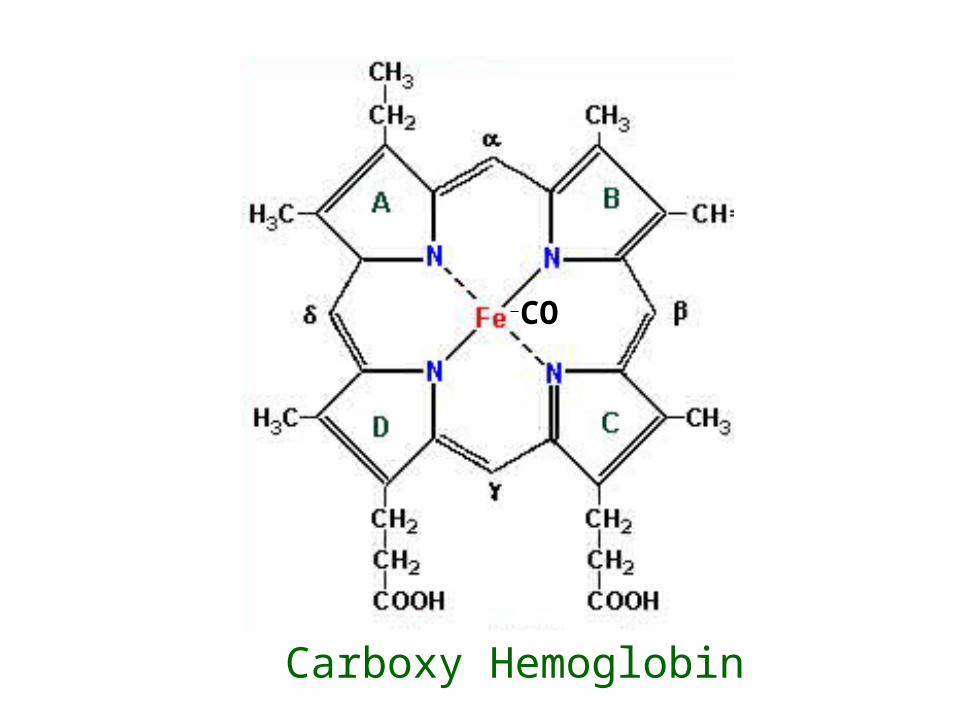
CO
Carboxy Hemoglobin

CarboxyhemoglobinCarboxyhemoglobin
Heme bound to CO “Cherry red” blood Absorbtion co-efficient similar to oxyhemoglobin—
falsely positive SpO2 Causes: Exposure to high levels of inhaled carbon
monoxide Normal levels: 0-3% non-smokers, up to 15%
smokers
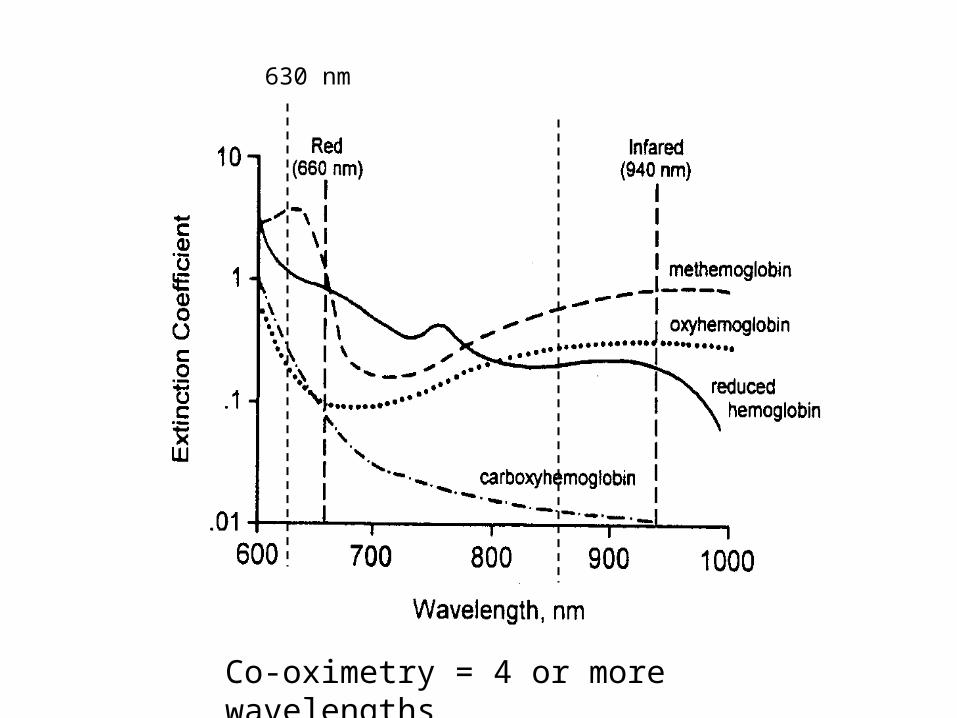
630 nm
Co-oximetry = 4 or more wavelengths
Mitochondrial Hypoxia
Cyanide poisoning Binds to ferric iron in cytochrome C oxidase Inhibits electron transport chain Low affinity for hgb Cellular anoxia, anaerobic metabolism,
lactic acidosis Exposures: Occupational exposure to
hydrogen cyanide (electroplating, photography, jewelry making), combustion of household materials, nitroprusside
Mitochondrial Hypoxia, cont.
Congenital disorders Mitochondrial genetic disorders
Sepsis
HAART therapy Nucleoside reverse transcriptase inhibitors
(stavudine, lamvudine, zidovudine)
Limitations of OLimitations of O22 Saturation Saturation +/- 2% between 70-100% Inaccuracies with:
– Poor perfusion– Venous pulsations– Nail polish– Hyperbilirubinemia– Methylene blue– Indigo and indocyanine green– Onchomycosis– Carboxy hemoglobin– Methemoglobin
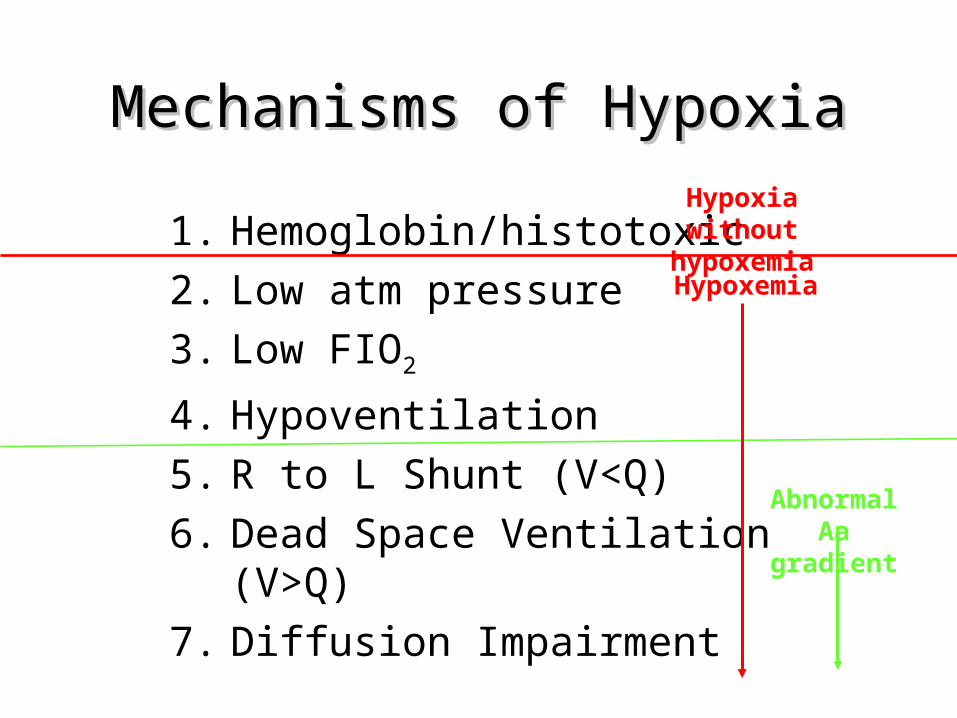
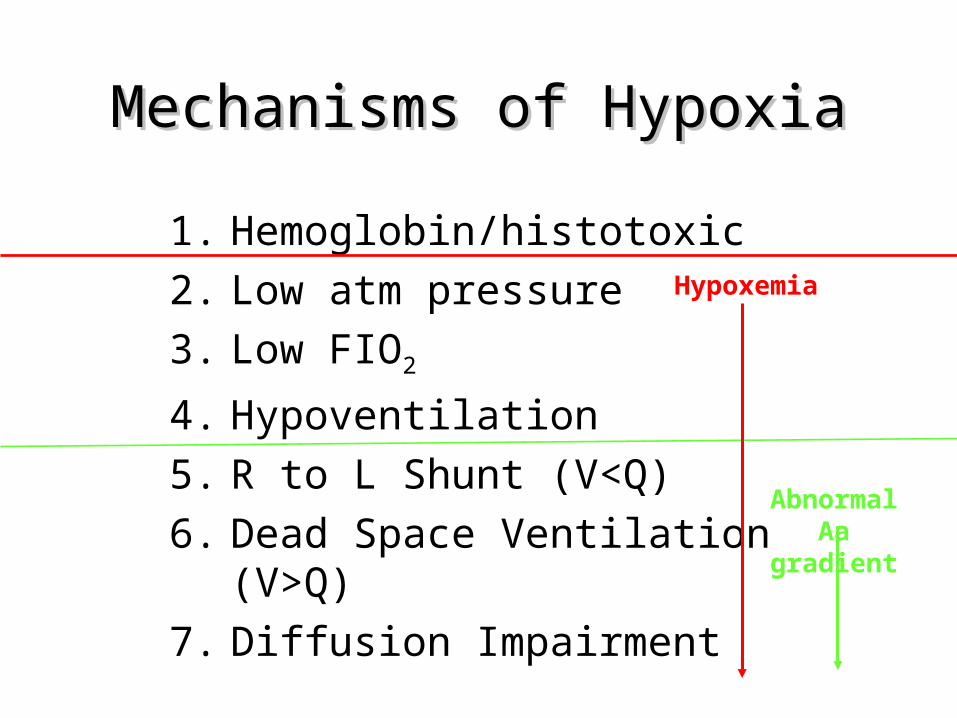
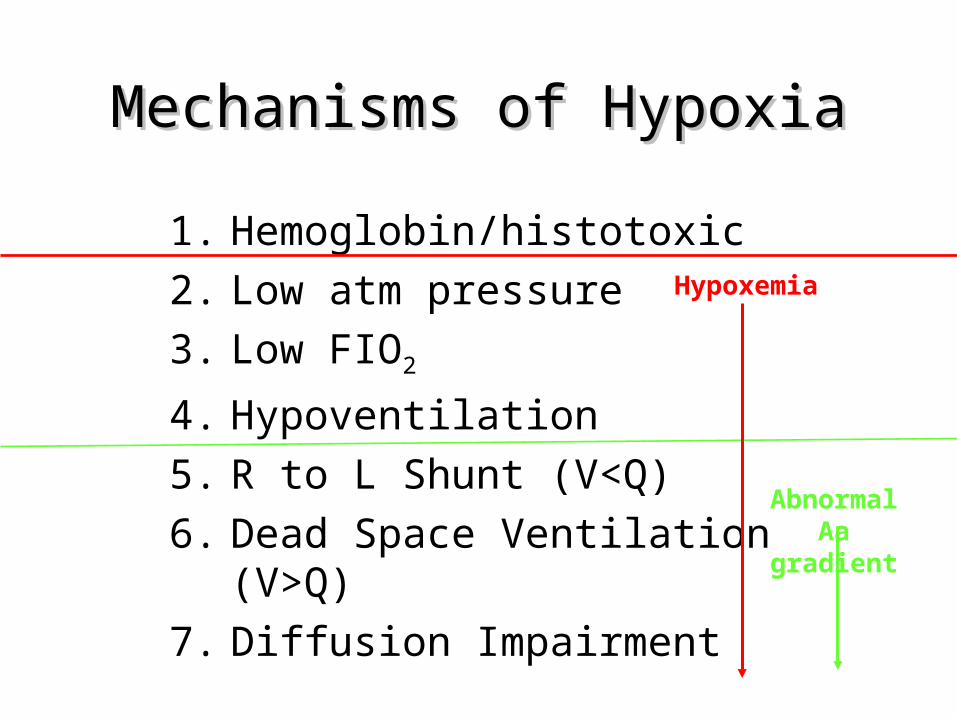
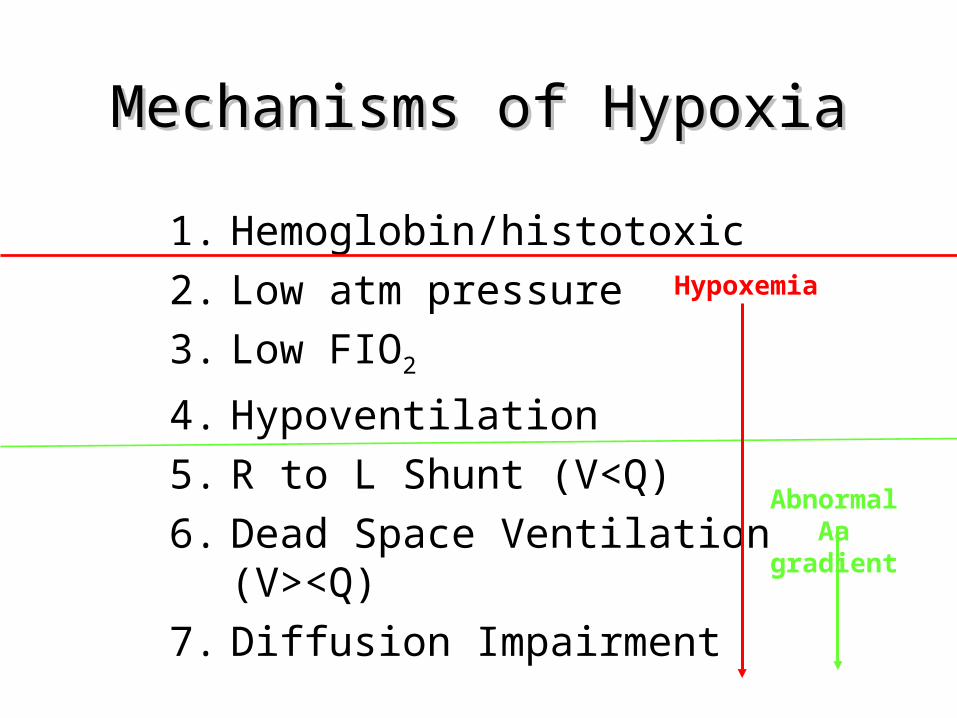
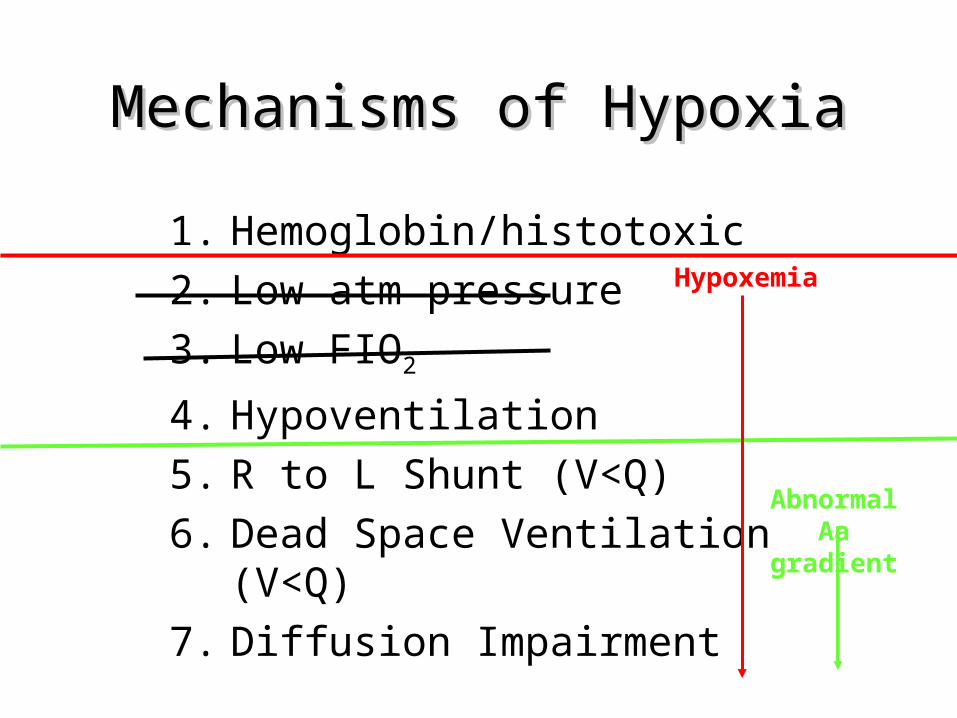
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V>Q) 7. Diffusion Impairment
Abnormal Aa gradient
Hypoxemia
Hypoxia without hypoxemia
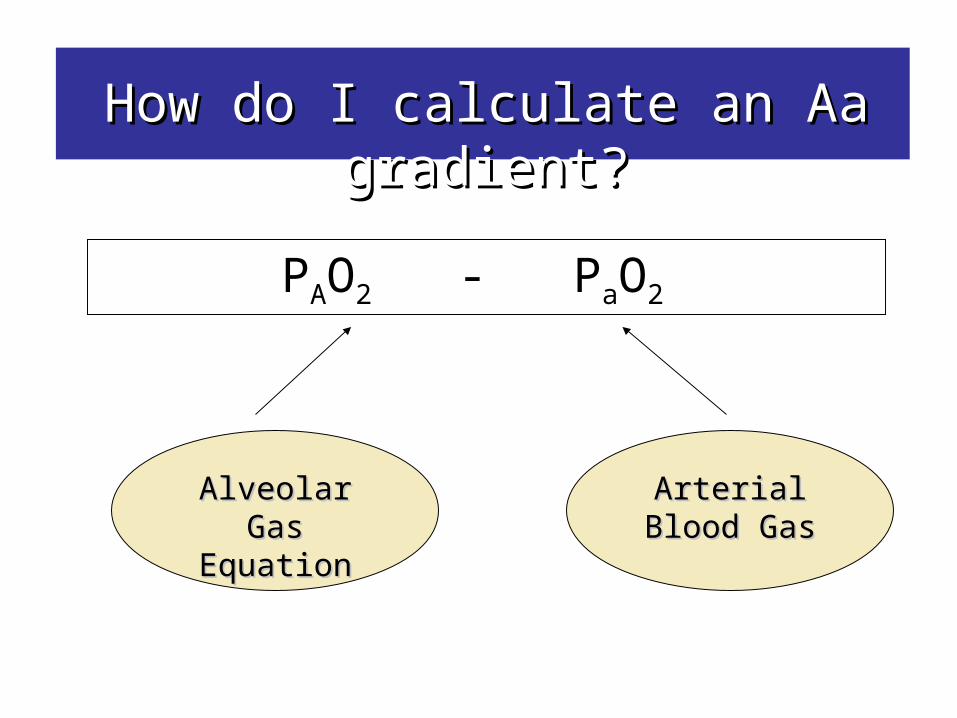
How do I calculate an Aa gradient?How do I calculate an Aa gradient?
PAO2 - PaO2
Alveolar Gas Alveolar Gas EquationEquation
Arterial Blood Arterial Blood GasGas
airways
alveolus
surfactant/air-water interface
pneumocyte
interstitial space
endothelial cell
serum
RBC membrane
hgb
cell membrane
cytoplasm
mitochondria
R LR
cell
PAO2
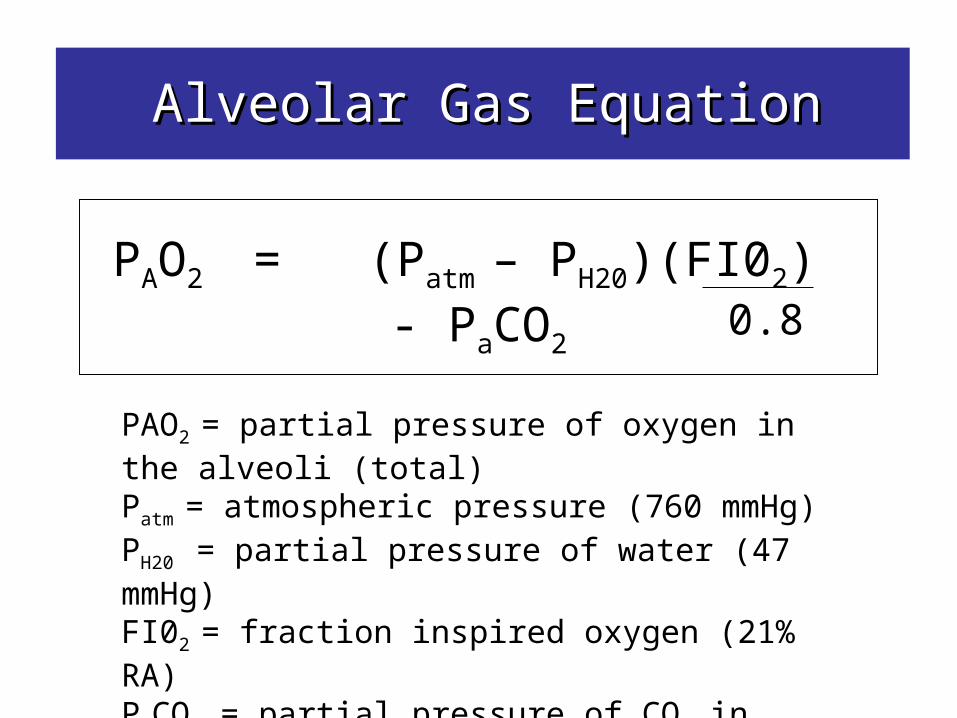
Alveolar Gas EquationAlveolar Gas Equation
PAO2 = (Patm – PH20)(FI02) - PaCO2
0.8
PAO2 = partial pressure of oxygen in the alveoli (total)Patm = atmospheric pressure (760 mmHg)PH20 = partial pressure of water (47 mmHg)FI02 = fraction inspired oxygen (21% RA)PaCO2 = partial pressure of CO2 in bloodO.8 = respiratory quotient
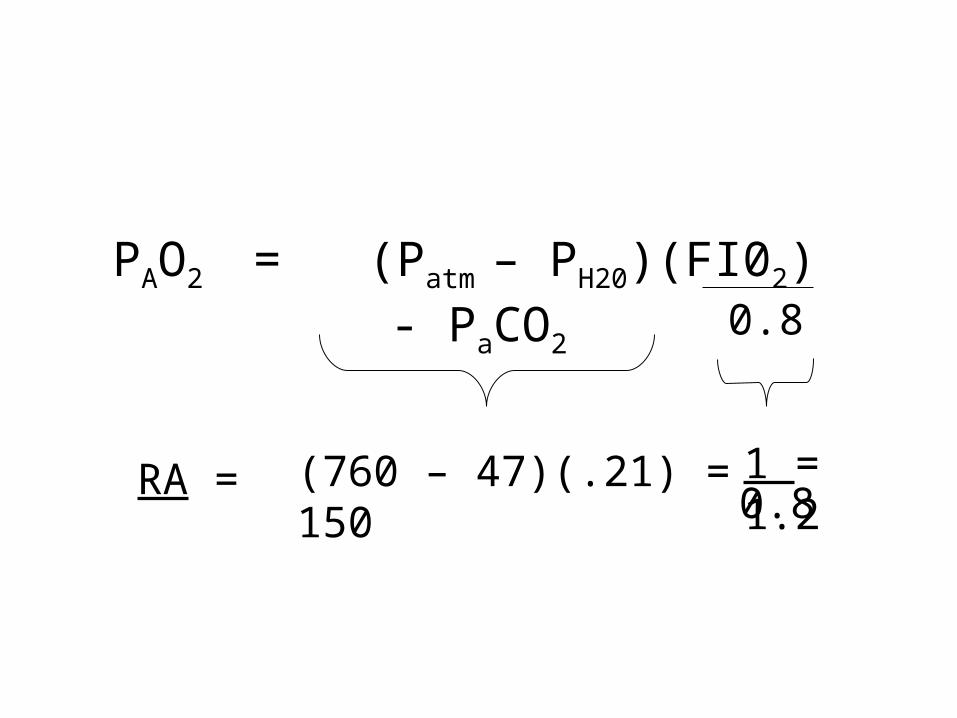
PAO2 = (Patm – PH20)(FI02) - PaCO2
0.8
(760 – 47)(.21) = 1501.0.8
1 = 1.2RA =

PAO2 (RA) = 150 - 1.2(PaCO2)
Remember this Formula!
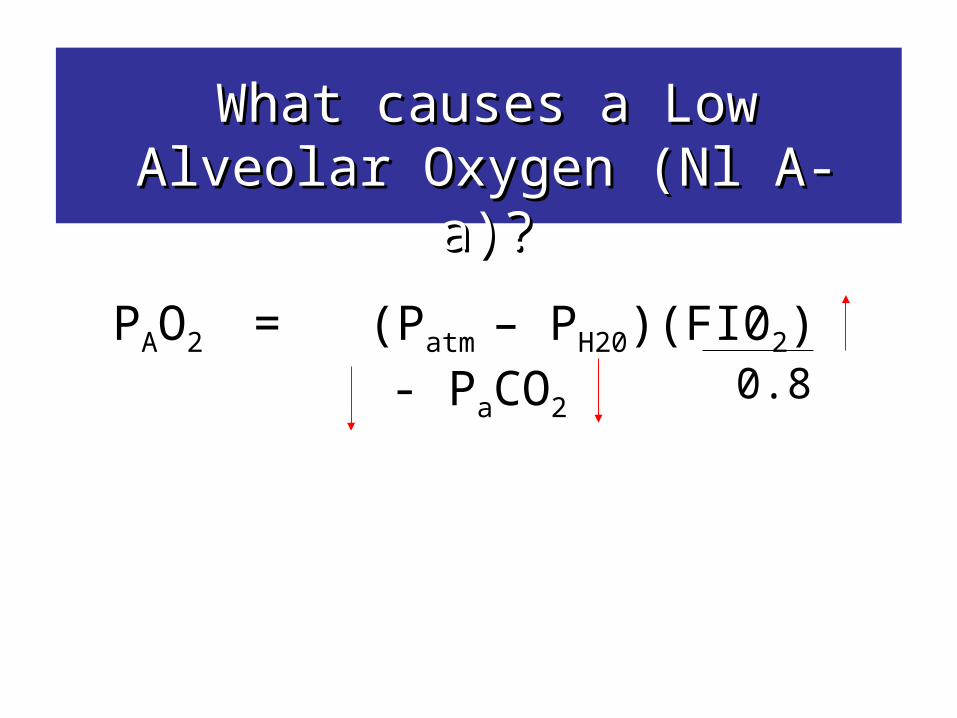
What causes a Low Alveolar What causes a Low Alveolar Oxygen (Nl A-a)?Oxygen (Nl A-a)?
PAO2 = (Patm – PH20)(FI02) - PaCO2
0.8
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V>Q) 7. Diffusion Impairment
Abnormal Aa gradient
Hypoxemia
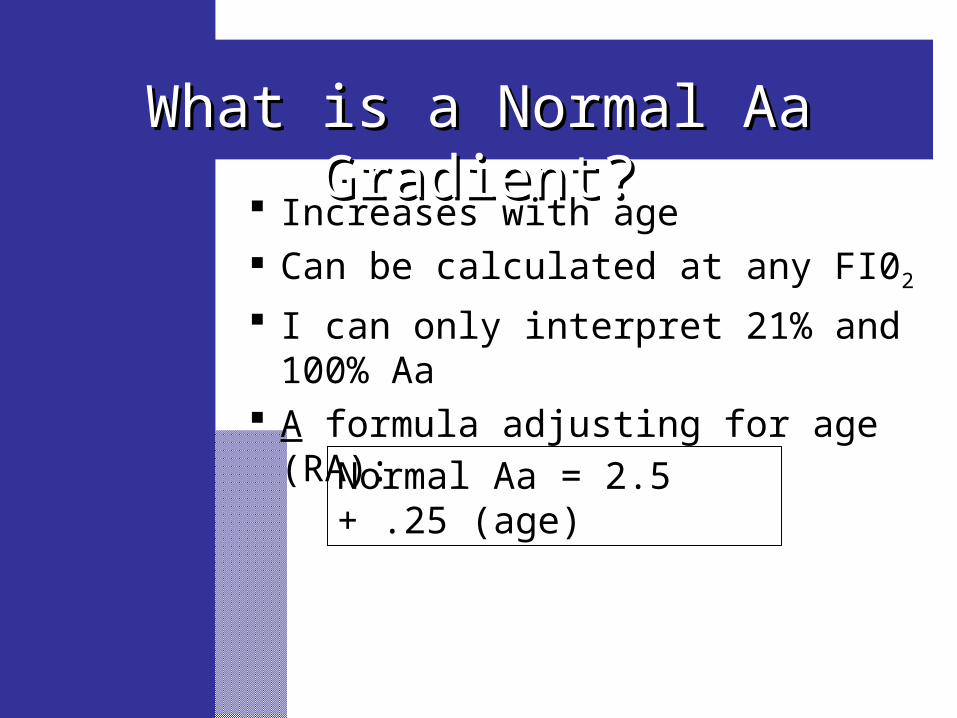
What is a Normal Aa Gradient?What is a Normal Aa Gradient?
Increases with age Can be calculated at any FI02
I can only interpret 21% and 100% Aa A formula adjusting for age (RA):
Normal Aa = 2.5 + .25 (age)
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V>Q) 7. Diffusion Impairment
Abnormal Aa gradient
Hypoxemia
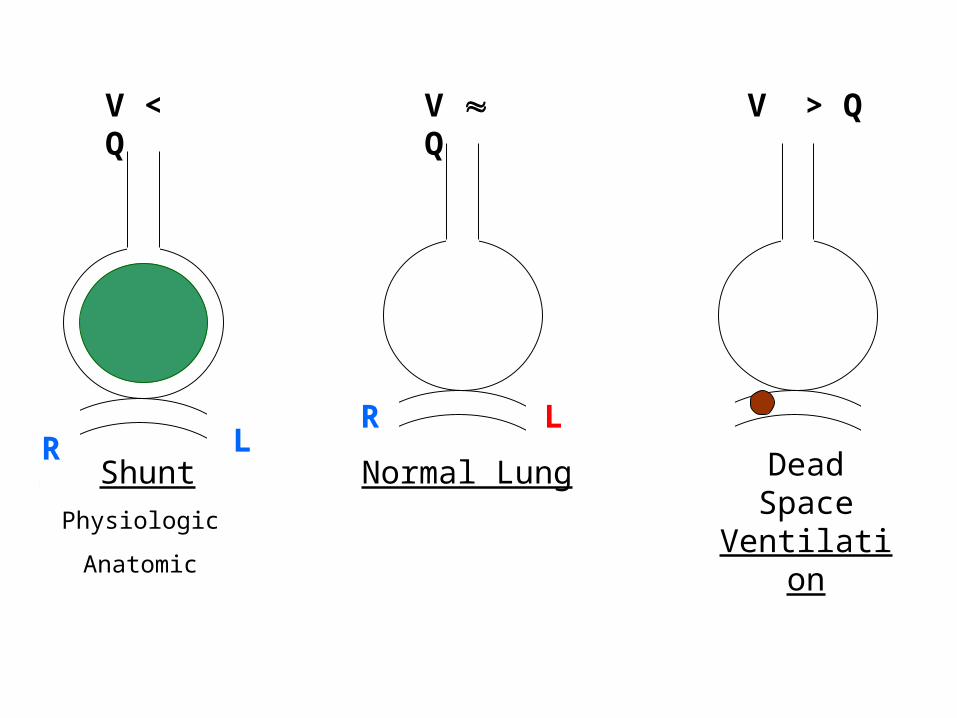
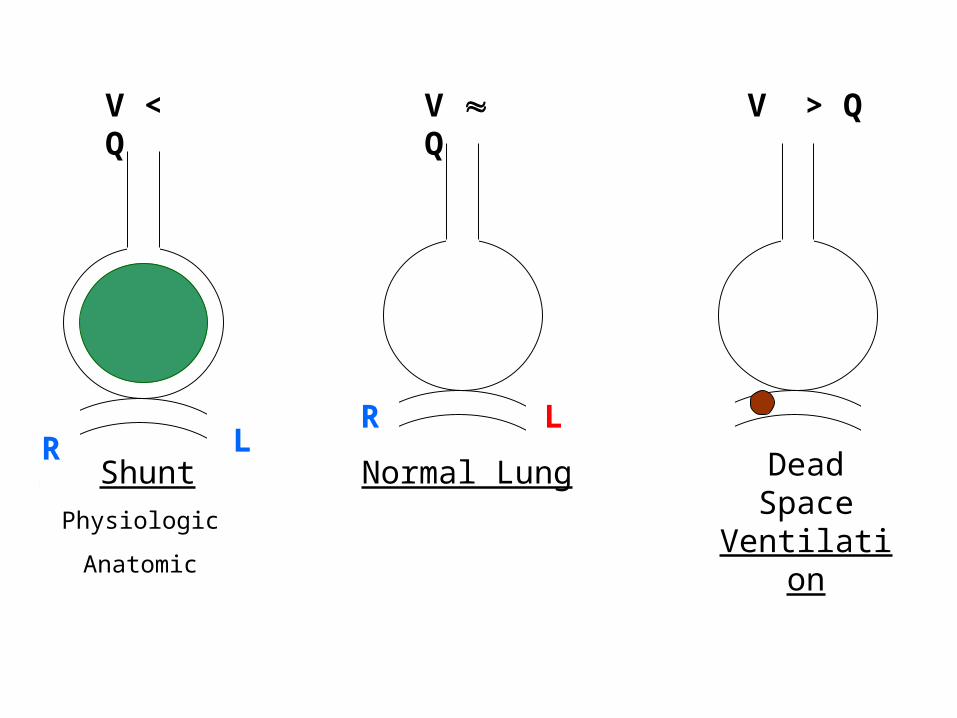
V QV < Q V > Q
Normal Lung Dead Space Ventilation
Shunt
Physiologic
Anatomic
R LR L
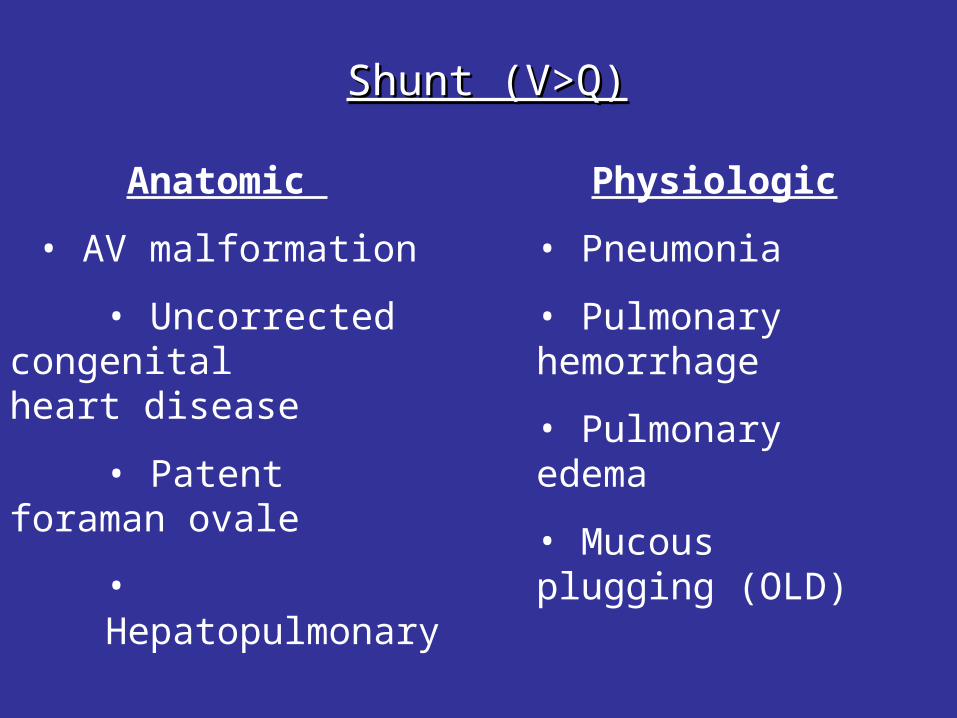
Anatomic
• AV malformation
• Uncorrected congenital heart disease
• Patent foraman ovale
• Hepatopulmonary syndrome
Shunt (V>Q)Shunt (V>Q)
Physiologic
• Pneumonia
• Pulmonary hemorrhage
• Pulmonary edema
• Mucous plugging (OLD)
V QV < Q V > Q
Normal Lung Dead Space Ventilation
Shunt
Physiologic
Anatomic
R LR L
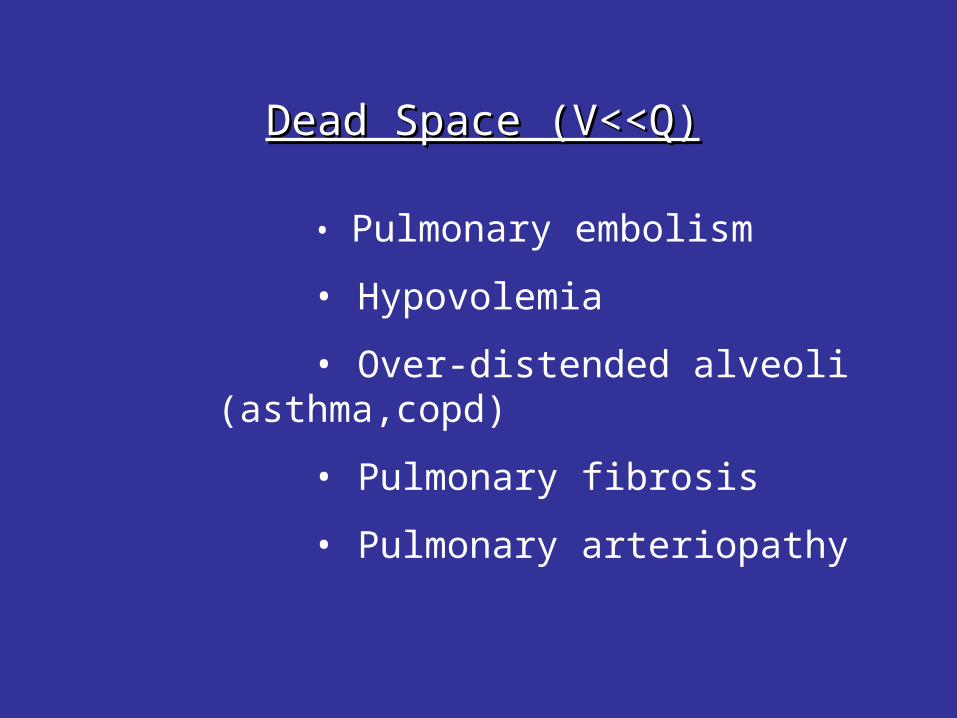
Dead Space (V<<Q)Dead Space (V<<Q)
• Pulmonary embolism
• Hypovolemia
• Over-distended alveoli (asthma,copd)
• Pulmonary fibrosis
• Pulmonary arteriopathy
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V><Q) 7. Diffusion Impairment
Abnormal Aa gradient
Hypoxemia
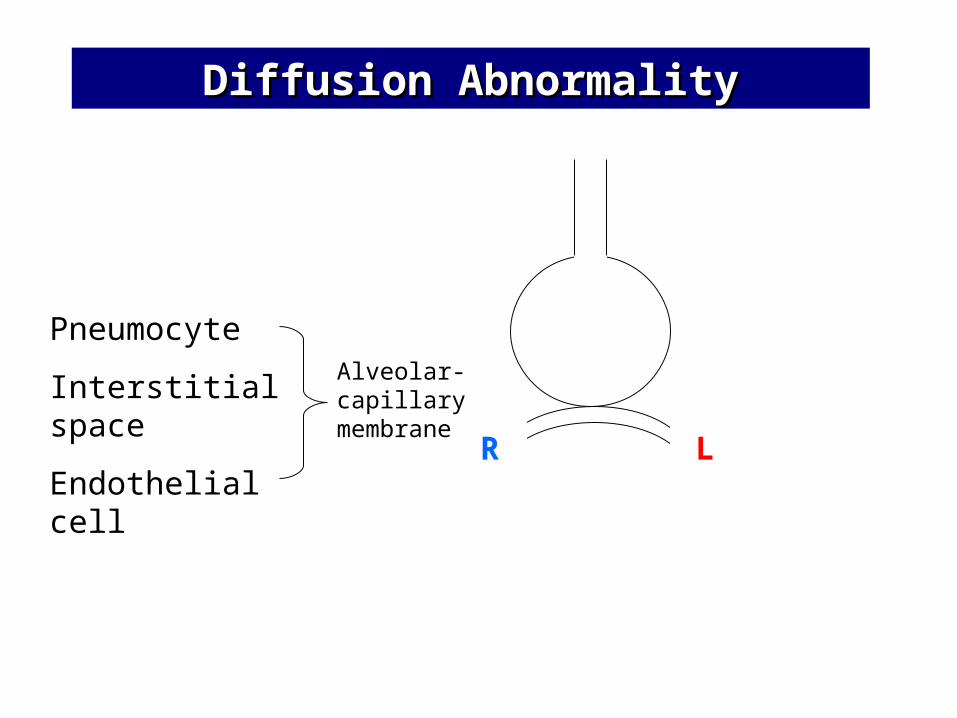
Diffusion AbnormalityDiffusion Abnormality
Pneumocyte
Interstitial space
Endothelial cell
Alveolar-capillary membrane
LR
Diffusion ImpairmentDiffusion Impairment
• Early interstitial lung disease
• Alveolar proteinosis
• Pneumocystis carinii pneumonia
• Hepatopulmonary syndrome
You are called by a 7CVA nurse who is taking care of You are called by a 7CVA nurse who is taking care of patient LB. LB is a patient LB. LB is a 52 y/o woman52 y/o woman with with rheumatoid rheumatoid arthritisarthritis and a and a TKA 3 daysTKA 3 days ago. The nurse reports that ago. The nurse reports that LB is requiring 3L/min nc oxygen to maintain a LB is requiring 3L/min nc oxygen to maintain a SpOSpO22 of 89%,of 89%, but is otherwise but is otherwise not distressednot distressed. The nurse . The nurse comments that the only thing the patient is comments that the only thing the patient is complaining of is a complaining of is a sore throatsore throat for which prn for which prn cetacaine cetacaine sprayspray is being used. The nurse thinks that the patient is being used. The nurse thinks that the patient might benefit from a might benefit from a bronchodilatorbronchodilator and asks if you and asks if you would give her a verbal order.would give her a verbal order.
Upon your arrival, pt is breathing 14/min and with Upon your arrival, pt is breathing 14/min and with complaints of vague chest constriction but no complaints of vague chest constriction but no pain. The nurse hands you an EKG that is pain. The nurse hands you an EKG that is significant only for ST 120 bpm. You note the significant only for ST 120 bpm. You note the patients patients cigarettescigarettes next to the bed and she has next to the bed and she has an an epidural in placeepidural in place. Lungs with faint bibasilar . Lungs with faint bibasilar crackles. The patient is crackles. The patient is obeseobese and you are and you are unsure of her JVP.unsure of her JVP.
Mechanisms of HypoxiaMechanisms of Hypoxia
1. Hemoglobin/histotoxic 2. Low atm pressure3. Low FIO2
4. Hypoventilation5. R to L Shunt (V<Q)6. Dead Space Ventilation (V<Q) 7. Diffusion Impairment
Abnormal Aa gradient
Hypoxemia
CXR shows mild plate-like atelectasis at the bases CXR shows mild plate-like atelectasis at the bases but is otherwise normal. ABG on RA 7.32/50/50. but is otherwise normal. ABG on RA 7.32/50/50. Co-oximetry: 3% carboxyhemoglobin, 2% Co-oximetry: 3% carboxyhemoglobin, 2% methemoglobin, oxyhemoglobin 85%methemoglobin, oxyhemoglobin 85%
Interpretation: Chronic respiratory acidosis, Interpretation: Chronic respiratory acidosis, moderate hypoxemia, Aa gradient = 40. moderate hypoxemia, Aa gradient = 40.
Predicted Aa gradient based on age is 16.Predicted Aa gradient based on age is 16.
Next Diagnostic Test?Next Diagnostic Test?
Chest CT Angiogram positive for PEChest CT Angiogram positive for PE
Clinical Tests Used in Work-up of Hypoxia SpO2
ABG (RA most helpful, don’t jeopardize well-being of patient)
CXR CT angiogram VQ scan Co-oximetry Hct Cyanide level Lactic acid
All Pts
What is most important to remember?What is most important to remember?
The DDX of hypoxia can be simplified based on the physiologic mechanisms Hypoxia with or without hypoxemia Hypoxemia with or without Aa gradient
Working through the physiologic based ddx will avoid missing important diagnoses
An ABG is not needed to identify the hypoxic patient but can be helpful in narrowing the DDX of hypoxia